 Danielle Ní Chróinín
Danielle Ní Chróinín Evan Alexandrou1,2,3
Evan Alexandrou1,2,3- 1Liverpool Hospital, Liverpool, NSW, Australia
- 2South Western Sydney Clinical School, UNSW Sydney, Liverpool, NSW, Australia
- 3Centre for Applied Nursing Research, School of Nursing and Midwifery, Western Sydney University and Ingham Institute of Applied Medical Research, Liverpool, NSW, Australia
- 4School of Nursing, Faculty of Science, Medicine and Health, University of Wollongong, Wollongong, NSW, Australia
- 5SWS Nursing and Midwifery Research Alliance, Ingham Institute of Applied Medical Research, Liverpool, NSW, Australia
The burden of delirium in the intensive care setting is a global priority. Delirium affects up to 80% of patients in intensive care units; an episode of delirium is often distressing to patients and their families, and delirium in patients within, or outside of, the intensive care unit (ICU) setting is associated with poor outcomes. In the short term, such poor outcomes include longer stay in intensive care, longer hospital stay, increased risk of other hospital-acquired complications, and increased risk of hospital mortality. Longer term sequelae include cognitive impairment and functional dependency. While medical category of admission may be a risk factor for poor outcomes in critical care populations, outcomes for surgical ICU admissions are also poor, with dependency at hospital discharge exceeding 30% and increased risk of in-hospital mortality, particularly in vulnerable groups, with high-risk procedures, and resource-scarce settings. A practical approach to delirium prevention and management in the ICU setting is likely to require a multi-faceted approach. Given the good evidence for the prevention of delirium among older post-operative outside of the intensive care setting, simple non-pharmacological interventions should be effective among older adults post-operatively who are cared for in the intensive care setting. In response to this, the future ICU environment will have a range of organizational and distinct environmental characteristics that are directly targeted at preventing delirium.
Introduction
The burden of delirium in the intensive care setting is a global priority (1, 2). Delirium is an acute neurocognitive disorder that is characterized by a fluctuating level of consciousness with impaired attention and cognition (3). Delirium affects up to 80% of patients in intensive care units (4). An episode of delirium is often distressing to patients and their families, and in patients within, or outside of, the intensive care unit (ICU) setting, and it is associated with poor outcomes, in the short term, which includes longer stay in intensive care, longer hospital stay, and increased risk of hospital mortality in patients (5–11). Longer term sequelae include cognitive impairment and dependency in activities of daily living (6, 9, 12–16). In the Australian healthcare setting, it has been estimated that an episode of delirium increases hospital stay by, on average, 2.7 days (17), and in the ICU-based Deli I study, patients experiencing an acute episode of delirium stayed, on average, an extra 6 days longer in hospital (18).
Delirium in the intensive care setting
Each year, there are approximately 175,000 admissions to Australian adult intensive care units (ICUs); this number has been increasing by 6% each year since 2011 (19). While there is considerable variability in the intensive care unit admissions depending on geographic location (20), intensive care unit beds and usage appear to be increasing (20). The majority of patients admitted to intensive care will survive ICU (19, 20); however, as many as one in five patients will experience an acute episode of delirium (21), and being older and frail increases the risk (2, 11, 22–24). The direct healthcare costs associated with delirium and longer hospital stay alone would be approximately $255 million annually in the Australian intensive care setting, excluding the cost due to the loss of healthy life, which has been estimated to be double that of direct healthcare costs (17, 25).
While the medical category of admission may be a risk factor for poor outcomes (26, 27) in critical care populations, outcomes for surgical ICU admissions are not particularly optimistic, with dependency at hospital discharge exceeding 30% (28) and average in-hospital mortality in the order of approximately 2.5–5% but exponentially higher in older patients or those undergoing high-risk procedures (28–31). Thirty-day mortality among non-cardiac surgical patients reaches almost 40% (32); even higher mortality rates have been observed in resource-limited settings (33). A recent study indicated that 28% of 350,000 admissions across 238 ICUs in the United States represented a primary surgical diagnosis (28). While encouraging trends were noted in terms of mortality and length of stay for some surgical cohorts, functional decline appeared to be increasing over time (28). Factors such as delirium, prolonged immobilization, and mechanical ventilation may all contribute to functional decline and other poor outcomes in surgical and general ICU populations, exacerbated by underlying risk factors such as age, frailty, comorbidity, and cognitive impairment (28, 34–36). Although not specific to those requiring intensive care admission, post-operative delirium is reported in upward of 65% of patients (37, 38). Identification of those who have the highest risk may facilitate the implementation of targeted interventions (39). The risk for the development of post-operative delirium may be conceptualized as relating to pre-operative (baseline) factors, intra-operative factors related to the surgery and anesthetic, and post-operative factors (38). A recent study highlighted the potential to predict delirium in older (aged ≥70 years) surgical patients undergoing elective cardiovascular, orthopedic, or general surgery (40), with surgery type, multimorbidity, renal failure, polypharmacy, ASA, cut-to-suture time, and cognitive assessment allowing an ability to predict delirium with an AUC of 0.8 (40). This information is helpful not only just in planning care but also in discussing risk with patients and families and managing expectations. Furthermore, embedding assessment in formal multi-faceted structures such as comprehensive geriatric assessment (CGA) may reduce post-operative delirium in older patients such as those undergoing vascular or hip fracture surgery (41, 42).
The good news is that high-quality evidence suggests that at least 30% of episodes of hospital-acquired delirium are preventable, including, for example, in post-operative hip fracture cohorts (3, 43, 44). Multi-component, multidisciplinary interventions have been shown to reduce the incidence of delirium, in general wards, post-operative, and aged care settings (3, 45–48). However, evidence for the effectiveness of interventions to reduce the burden of delirium in the intensive care has been inconclusive (49–54), and none of these intensive care studies focused purely on post-operative populations. Gaps are in part attributable to a lack of focus on the effective implementation and dissemination of evidence into practice (55–57). There is a lack of good evidence supporting the use of pharmacological interventions to prevent delirium in the intensive care setting. A recent Cochrane systematic review (45) concluded that “the effects of other pharmacological, sedation, environmental, and preventive nursing interventions is unclear and warrants further investigation,” while a meta-analysis of bundle interventions likewise failed to show an association with delirium prevalence or duration (58). Nonetheless, previous trials, systematic reviews, and meta-analyses have shown promise in terms of the effectiveness of non-pharmacological interventions to reduce the burden of delirium in the hospital and critical care settings (43–47, 52).
A recent review of pharmacological therapy in the ICU highlighted the significant limitations of existing trials, with heterogeneity in terms of agents used, primary outcome measures, timing of treatment, and delirium diagnosis (59). Among the available pharmacological agents, dexmedetomidine has some evidence supporting its benefit in reducing post-operative delirium in older patients undergoing elective non-cardiac surgery (60). A slightly more recent meta-analysis of 14 melatonin/ramelteon studies suggested that these formulations might significantly reduce delirium in surgical (49% risk reduction) and ICU (34%) patient groups (61), but optimum duration, dosing, and formulation are yet to be identified.
In addition to delirium prevention, early recognition of delirium is key. Improving detection through the use of screening tools (3, 62, 63) may facilitate improved diagnosis, which can in turn trigger prompts to guide investigation and management (3, 64, 65). Simple screening tools may in fact be utilized to assist in the diagnosis of delirium in the intensive care setting. The Confusion Assessment Method (CAM) and its ICU version have been validated as a reliable (kappa = 0.96; 95% CI 0.91–0.99) and valid (sensitivity 0.81–0.82 and specificity 0.99) tool to diagnose delirium in the intensive care setting (66–68). Hypoactive delirium, which is common in older patients, is associated with a poorer prognosis than the hyperactive form (3) but is more likely to be under-recognized (69), highlighting the need to maintain an appropriate index of suspicion in older patients. While DSM-V criteria for the diagnosis of delirium no longer explicitly refer to the level of arousal for the diagnosis of delirium, the level of arousal is fundamental to the assessment of attention and cognition and should be included in the assessment of the potentially delirious patient (70). The issue of coma is also pertinent to the ICU setting, and it is worth noting that a diagnosis of delirium is precluded in patients with a severely reduced level of arousal such as coma (71).
Thus, a practical approach to delirium prevention and management in the ICU setting is likely to require a multi-faceted approach. Some examples of non-pharmacological interventions to reduce the risk of delirium are presented in the Table 1. Environmental factors may also be a focus of risk-reduction strategies, with design modifications potentially targeting sound and light, floor planning, and room arrangement, aiming to reduce stressors and positively influence the patient experience (4). Harnessing the expertise and manpower of family members, to assist with aspects of care such as orientation and memory cueing, cognitive stimulation, and sensory checks, may also be feasible and acceptable (72).
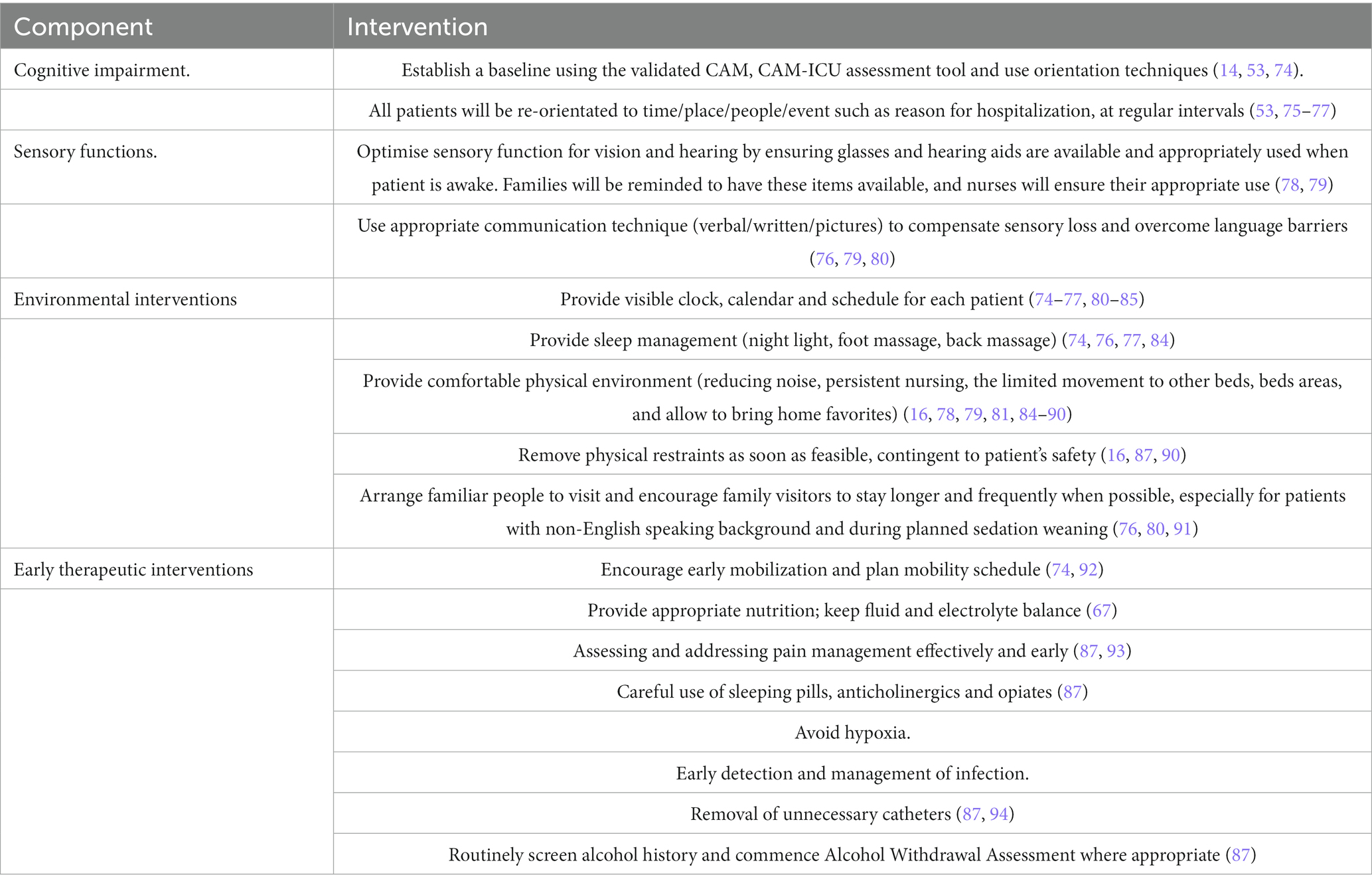
Table 1. Non-pharmacological interventions reduce the risk of delirium.
Implications for clinical practice
Good quality evidence suggests that at least 30% of episodes of delirium among older adults admitted to the hospital are preventable, with interventions being delivered by an interdisciplinary team of nursing, medical, and allied health clinicians (3). There is consistent evidence that these multi-component interventions are effective in preventing delirium, in general wards and aged care settings (43, 45). However, evidence for the effectiveness of interventions to reduce the burden of delirium in the intensive care has been inconclusive. While and small single-site, non-pharmacological multi-component interventional studies have shown promising results (45), larger studies, often among patients at high risk, have not shown a clear benefit (43, 49). In particular, older cardiothoracic surgery patient appears to be resistant to intervention in the ICU, even when other similar-aged surgical patients can have the risk of reduced post-operative delirium (43). Importantly, several significant organizational and design changes to the intensive care setting have been proposed, as “the future of intensive care: delirium should no longer be an issue” (73).
Conclusion
Given the good evidence for the prevention of delirium among older post-operative outside of the intensive care setting, simple non-pharmacological interventions should be effective among older adults post-operatively cared for in the intensive care setting. In response to this, the future ICU environment will have a range of organizational and distinct environmental characteristics that are directly targeted at preventing delirium.
Author contributions
DN, EA, and SF were responsible for drafting, editing, and finalization of the manuscript. All authors agreed to be accountable for the content of the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. La Cour, KN, Andersen-Ranberg, NC, Weihe, S, Poulsen, LM, Mortensen, CB, Kjer, CKW, et al. Distribution of delirium motor subtypes in the intensive care unit: a systematic scoping review. Crit Care. (2022) 26:53. doi: 10.1186/s13054-022-03931-3
2. Salluh, JI, Wang, H, Schneider, EB, Nagaraja, N, Yenokyan, G, Damluji, A, et al. Outcome of delirium in critically ill patients: systematic review and meta-analysis. BMJ. (2015) 350:h2538. doi: 10.1136/bmj.h2538
3. Inouye, SK, Westendorp, RG, and Saczynski, JS. Delirium in elderly people. Lancet. (2014) 383:911–22. doi: 10.1016/S0140-6736(13)60688-1
4. Luetz, A, Grunow, JJ, Mörgeli, R, Rosenthal, M, Weber-Carstens, S, Weiss, B, et al. Innovative ICU Solutions to Prevent and Reduce Delirium and Post-Intensive Care Unit Syndrome. Seminars in respiratory and critical care medicine. (2019) 40:673–86. doi: 10.1055/s-0039-1698404
5. Dolan, MM, Hawkes, WG, Zimmerman, SI, Morrison, RS, Gruber-Baldini, AL, Hebel, JR, et al. Delirium on hospital admission in aged hip fracture patients: prediction of mortality and 2-year functional outcomes. J Gerontol A Biol Sci Med Sci. (2000) 55:M527–34. doi: 10.1093/gerona/55.9.M527
6. Ely, EW, Shintani, A, Truman, B, Speroff, T, Gordon, SM, Harrell, FE Jr, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. (2004) 291:1753–62. doi: 10.1001/jama.291.14.1753
7. Kennedy, M, Helfand, BKI, Gou, RY, Gartaganis, SL, Webb, M, Moccia, JM, et al. Delirium in older patients with COVID-19 presenting to the emergency department. JAMA Netw Open. (2020) 3:e2029540. doi: 10.1001/jamanetworkopen.2020.29540
8. Ní Chróinín, D, Francis, N, Wong, P, Kim, YD, Nham, S, and D'amours, S. Older trauma patients are at high risk of delirium, especially those with underlying dementia or baseline frailty. Trauma Surg Acute Care Open. (2021) 6:e000639. doi: 10.1136/tsaco-2020-000639
9. Ouimet, S, Kavanagh, BP, Gottfried, SB, and Skrobik, Y. Incidence, risk factors and consequences of ICU delirium. Intensive Care Med. (2007) 33:66–73. doi: 10.1007/s00134-006-0399-8
10. Radinovic, K, Markovic-Denic, L, Dubljanin-Raspopovic, E, Marinkovic, J, Milan, Z, and Bumbasirevic, V. Estimating the effect of incident delirium on short-term outcomes in aged hip fracture patients through propensity score analysis. Geriatr Gerontol Int. (2015) 15:848–55. doi: 10.1111/ggi.12358
11. Sanchez, D, Brennan, K, Al Sayfe, M, Shunker, SA, Bogdanoski, T, Hedges, S, et al. Frailty, delirium and hospital mortality of older adults admitted to intensive care: the Delirium (Deli) in ICU study. Crit Care. (2020) 24:609. doi: 10.1186/s13054-020-03318-2
12. Abelha, FJ, Luís, C, Veiga, D, Parente, D, Fernandes, V, Santos, P, et al. Outcome and quality of life in patients with postoperative delirium during an ICU stay following major surgery. Crit Care. (2013) 17:R257–7. doi: 10.1186/cc13084
13. Andrews, L, Silva, SG, Kaplan, S, and Zimbro, K. Delirium monitoring and patient outcomes in a general intensive care unit. Am J Crit Care. (2015) 24:48–56. doi: 10.4037/ajcc2015740
14. Balas, MC, Deutschman, CS, Sullivan-Marx, EM, Strumpf, NE, Alston, RP, and Richmond, TS. Delirium in older patients in surgical intensive care units. J Nurs Scholarsh. (2007) 39:147–54.
15. Hideaki, S, Subrina, J, Takeshi, U, Taro, M, and Hiroko, K. Severity of delirium in the ICU is associated with short term cognitive impairment. A prospective cohort study. Intensive Crit Care Nurs. (2015) 31:250–7. doi: 10.1016/j.iccn.2015.01.001
16. Mehta, S, Cook, D, Devlin, JW, Skrobik, Y, Meade, M, Fergusson, D, et al. Prevalence, risk factors, and outcomes of delirium in mechanically ventilated adults*. Crit Care Med. (2015) 43:557–66. doi: 10.1097/CCM.0000000000000727
17. Pezzullo, L, Streatfeild, J, Hickson, J, Teodorczuk, A, Agar, MR, and Caplan, GA. Economic impact of delirium in Australia: a cost of illness study. BMJ Open. (2019) 9:e027514. doi: 10.1136/bmjopen-2018-027514
18. Brennan, K, Sanchez, D, Hedges, S, Al Sayfe, M, Shunker, SA, Bogdanoski, T, et al. A nurse-led intervention to reduce the incidence and duration of delirium among adults admitted to intensive care: A stepped-wedged cluster randomised trial. Austr Crit Care. (2022). doi: 10.1016/j.aucc.2022.08.005
19. Australian and New Zealand Intensive Care Society. Centre for outcome and resource evaluation 2020 report. Camberwell, Australia: Australian and New Zealand Intensive Care Society (2020).
20. Wunsch, H, Angus, DC, Harrison, DA, Collange, O, Fowler, R, Hoste, EA, et al. Variation in critical care services across North America and Western Europe. Critical care medicine. (2008) 36:2787–e9. doi: 10.1097/CCM.0b013e318186aec8
21. Ankravs, MJ, Udy, AA, Byrne, K, Knowles, S, Hammond, N, Saxena, MK, et al. A multicentre point prevalence study of delirium assessment and management in patients admitted to Australian and New Zealand intensive care units. Crit Care Resusc. (2020) 22:355–60. doi: 10.51893/2020.4.OA8
22. Bagshaw, SM, Stelfox, HT, Mcdermid, RC, Rolfson, DB, Tsuyuki, RT, Baig, N, et al. Association between frailty and short- and long-term outcomes among critically ill patients: a multicentre prospective cohort study. CMAJ. (2014) 186:E95–E102. doi: 10.1503/cmaj.130639
23. Darvall, JN, Bellomo, R, Paul, E, Subramaniam, A, Santamaria, JD, Bagshaw, SM, et al. Frailty in very old critically ill patients in Australia and New Zealand: a population-based cohort study. Med J Aust. (2019) 211:318–23. doi: 10.5694/mja2.50329
24. Flaatten, H, De Lange, DW, Morandi, A, Andersen, FH, Artigas, A, Bertolini, G, et al. The impact of frailty on Icu and 30-day mortality and the level of care in very elderly patients (>/= 80 years). Intensive Care Med. (2017) 43:1820–8.
25. Caplan, GA, Teodorczuk, A, Streatfeild, J, and Agar, MR. The financial and social costs of delirium. European geriatric medicine. (2020) 11:105–12. doi: 10.1007/s41999-019-00257-2
26. Le Gall, JR, Lemeshow, S, and Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA. (1993) 270:2957–63. doi: 10.1001/jama.270.24.2957
27. Zimmerman, JE, Kramer, AA, McNair, DS, and Malila, FM. Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today’s critically ill patients. Critical care medicine. (2006) 34:1297–310. doi: 10.1097/01.CCM.0000215112.84523.F0
28. Vakayil, V, Ingraham, NE, Robbins, AJ, Freese, R, Northrop, EF, Brunsvold, ME, et al. Epidemiological trends of surgical admissions to the intensive care unit in the United States. The journal of trauma and acute care surgery. (2020) 89:279–88. doi: 10.1097/TA.0000000000002768
29. Lamarche, Y, Elmi-Sarabi, M, Ding, L, Abel, JG, Sirounis, D, and Denault, AY. A score to estimate 30-day mortality after intensive care admission after cardiac surgery. The Journal of thoracic and cardiovascular surgery. (2017) 153:1118–1125.e4. doi: 10.1016/j.jtcvs.2016.11.039
30. Reis, P, Lopes, AI, Leite, D, Moreira, J, Mendes, L, Ferraz, S, et al. Predicting mortality in patients admitted to the intensive care unit after open vascular surgery. Surgery today. (2019) 49:836–42. doi: 10.1007/s00595-019-01805-w
31. Sanchez, D, Brennan, K, Sayfe M., AL, Shunker, SA, Bogdanoski, T, Hedges, S, et al. Frailty, delirium and hospital mortality of older adults admitted to intensive care: the Delirium (Deli) in ICU study. Crit Care. (2020) 24:609.
32. Ekeloef, S, Thygesen, LC, and Gögenur, I. Short- and long-term mortality in major non-cardiac surgical patients admitted to the intensive care unit. Acta anaesthesiologica Scandinavica. (2019) 63:639–46. doi: 10.1111/aas.13319
33. Bunogerane, GJ, and Rickard, J. A cross sectional survey of factors influencing mortality in Rwandan surgical patients in the intensive care unit. Surgery. (2019) 166:193–7. doi: 10.1016/j.surg.2019.04.010
34. Bagshaw, SM, Stelfox, HT, Mcdermid, RC, Rolfson, DB, Tsuyuki, RT, Baig, N, et al. Association between frailty and short- and long-term outcomes among critically ill patients: a multicentre prospective cohort study. CMAJ. (2014) 186:E95–102.
35. Guidet, B, de Lange, DW, Boumendil, A, Leaver, S, Watson, X, Boulanger, C, et al. The contribution of frailty, cognition, activity of daily life and comorbidities on outcome in acutely admitted patients over 80 years in European ICUs: the VIP2 study. Intensive care medicine. (2020) 46:57–69. doi: 10.1007/s00134-019-05853-1
36. Menges, D, Seiler, B, Tomonaga, Y, Schwenkglenks, M, Puhan, MA, and Yebyo, HG. Systematic early versus late mobilization or standard early mobilization in mechanically ventilated adult ICU patients: systematic review and meta-analysis. Critical care (London, England). (2021) 25:16. doi: 10.1186/s13054-020-03446-9
37. Inouye, SK. Delirium after hip fracture: to be or not to be? Journal of the American Geriatrics Society. (2001) 49:678–9. doi: 10.1046/j.1532-5415.2001.49133.x
38. Bilotta, F, Lauretta, MP, Borozdina, A, Mizikov, VM, and Rosa, G. Postoperative delirium: risk factors, diagnosis and perioperative care. Minerva anestesiologica. (2013) 79:1066–76.
39. Wilson, S, Sutherland, E, Razak, A, O’Brien, M, Ding, C, Nguyen, T, et al. Implementation of a Frailty Assessment and Targeted Care Interventions and Its Association with Reduced Postoperative Complications in Elderly Surgical Patients. Journal of the American College of Surgeons. (2021) 233:764–775.e1. doi: 10.1016/j.jamcollsurg.2021.08.677
40. Eschweiler, GW, Czornik, M, Herrmann, ML, et al. Presurgical Screening Improves Risk Prediction for Delirium in Elective Surgery of Older Patients: The PAWEL RISK Study. Front Aging Neurosci. (2021) 13:679933. Published 2021 Jul 27. doi: 10.3389/fnagi.2021.679933
41. Partridge, JS, Harari, D, Martin, FC, Peacock, JL, Bell, R, Mohammed, A, et al. Randomized clinical trial of comprehensive geriatric assessment and optimization in vascular surgery. The British journal of surgery. (2017) 104:679–87. doi: 10.1002/bjs.10459
42. Shields, L, Henderson, V, and Caslake, R. Comprehensive Geriatric Assessment for Prevention of Delirium After Hip Fracture: A Systematic Review of Randomized Controlled Trials. Journal of the American Geriatrics Society. (2017) 65:1559–65. doi: 10.1111/jgs.14846
43. Deeken, F, Sanchez, A, Rapp, MA, Denkinger, M, Brefka, S, Spank, J, et al. Outcomes of a delirium prevention program in older persons after elective surgery: a stepped-wedge cluster randomized clinical trial. JAMA Surg. (2022) 157:e216370. doi: 10.1001/jamasurg.2021.6370
44. Chuan, A, and Sanders, RD. The use of dexmedetomidine to prevent delirium after major cardiac and non-cardiac surgery. Anaesthesia. (2021) 76:1296–9. doi: 10.1111/anae.15494
45. Burton, JK, Craig, L, Yong, SQ, Siddiqi, N, Teale, EA, Woodhouse, R, et al. Non-pharmacological interventions for preventing delirium in hospitalised non-Icu patients. Cochrane Database Syst Rev. (2021) 11:Cd013307. doi: 10.1002/14651858.CD013307.pub2
46. Hshieh, TT, Yang, T, Gartaganis, SL, Yue, J, and Inouye, SK. Hospital elder life program: systematic review and meta-analysis of effectiveness. Am J Geriatr Psychiatry. (2018) 26:1015–33. doi: 10.1016/j.jagp.2018.06.007
47. Hshieh, TT, Yue, J, Oh, E, Puelle, M, Dowal, S, Travison, T, et al. Effectiveness of multicomponent nonpharmacological delirium interventions: a meta-analysis. JAMA Intern Med. (2015) 175:512–20. doi: 10.1001/jamainternmed.2014.7779
48. Chuan, A, Zhao, L, Tillekeratne, N, Alani, S, Middleton, PM, Harris, IA, et al. The effect of a multidisciplinary care bundle on the incidence of delirium after hip fracture surgery: a quality improvement study. Anaesthesia. (2020) 75:63–71. doi: 10.1111/anae.14840
49. Bannon, L, Mcgaughey, J, Verghis, R, Clarke, M, Mcauley, DF, and Blackwood, B. The effectiveness of non-pharmacological interventions in reducing the incidence and duration of delirium in critically ill patients: a systematic review and meta-analysis. Intensive Care Med. (2019) 45:1–12. doi: 10.1007/s00134-018-5452-x
50. Girard, TD, Exline, MC, Carson, SS, Hough, CL, Rock, P, Gong, MN, et al. Haloperidol and Ziprasidone for treatment of delirium in critical illness. N Engl J Med. (2018) 379:2506–16. doi: 10.1056/NEJMoa1808217
51. Herling, SF, Greve, IE, Vasilevskis, EE, Egerod, I, Bekker Mortensen, C, Moller, AM, et al. Interventions for preventing intensive care unit delirium in adults. Cochrane Database Syst Rev. (2018) 11:Cd009783. doi: 10.1002/14651858.CD009783.pub2
52. Kang, J, Lee, M, Ko, H, Kim, S, Yun, S, Jeong, Y, et al. Effect of nonpharmacological interventions for the prevention of delirium in the intensive care unit: a systematic review and meta-analysis. J Crit Care. (2018) 48:372–84. doi: 10.1016/j.jcrc.2018.09.032
53. Moon, KJ, and Lee, SM. The effects of a tailored intensive care unit delirium prevention protocol: a randomized controlled trial. Int J Nurs Stud. (2015) 52:1423–32. doi: 10.1016/j.ijnurstu.2015.04.021
54. Rood, PJT, Zegers, M, Ramnarain, D, Koopmans, M, Klarenbeek, T, Ewalds, E, et al. The impact of nursing delirium preventive interventions in the ICU: a multicenter cluster-randomized controlled clinical trial. Am J Respir Crit Care Med. (2021) 204:682–91. doi: 10.1164/rccm.202101-0082OC
55. Eccles, MP, and Mittman, BS. Welcome to implementation science. Implement Sci. (2006) 1:1. doi: 10.1186/1748-5908-1-1
56. Fixsen, D, Naoom, S, Blase, K, Friedman, R, and Wallace, F. Implementation research: A synthesis of the literature. Tamps, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute, National Implementation Research Network (2005).
57. Proctor, EK, Powell, BJ, and Mcmillen, JC. Implementation strategies: recommendations for specifying and reporting. Implement Sci. (2013) 8:139. doi: 10.1186/1748-5908-8-139
58. Zhang, S, Han, Y, Xiao, Q, Li, H, and Wu, Y. Effectiveness of Bundle Interventions on ICU Delirium: A Meta-Analysis. Critical care medicine. (2021) 49:335–46. doi: 10.1097/CCM.0000000000004773
59. Korenoski, A, Li, A, Kane-Gill, SL, Seybert, AL, and Smithburger, PL. Pharmacologic Management of Delirium in the ICU: A Review of the Literature. Journal of intensive care medicine. (2020) 35:107–17. doi: 10.1177/0885066618805965
60. Janssen, TL, Alberts, AR, Hooft, L, Mattace-Raso, F, Mosk, CA, and van der Laan, L. Prevention of postoperative delirium in elderly patients planned for elective surgery: systematic review and meta-analysis. Clinical interventions in aging. (2019) 14:1095–117. doi: 10.2147/CIA.S201323
61. Khaing, K, and Nair, BR. Melatonin for delirium prevention in hospitalized patients: A systematic review and meta-analysis. Journal of psychiatric research. (2021) 133:181–90. doi: 10.1016/j.jpsychires.2020.12.020
62. Kean, J, and Ryan, K. Delirium detection in clinical practice and research: critique of current tools and suggestions for future development. Journal of psychosomatic research. (2008) 65:255–9. doi: 10.1016/j.jpsychores.2008.05.024
63. Australian Commission on Safety and Quality in Healthcare, 2006. Delirium Clinical Care Standard. [Internet]. Sydney.
64. ACSQHC, 2021. Available at: https://www.safetyandquality.gov.au/sites/default/files/2021-11/delirium_clinical_care_standard_2021.pdf
65. Fu, S, Lopes, GS, Pagali, SR, Thorsteinsdottir, B, LeBrasseur, NK, Wen, A, et al. Ascertainment of Delirium Status Using Natural Language Processing From Electronic Health Records. The journals of gerontology. Series A, Biological sciences and medical sciences. (2022) 77:524–30. doi: 10.1093/gerona/glaa275
66. Ely, EW, Inouye, SK, Bernard, GR, Gordon, S, Francis, J, May, L, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA. (2001) 286:2703–46. doi: 10.1001/jama.286.21.2703
67. Inouye, SK, Van Dyck, CH, Alessi, CA, Balkin, S, Siegal, AP, and Horwitz, RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. (1990) 113:941–8. doi: 10.7326/0003-4819-113-12-941
68. Shi, Q, Warren, L, Saposnik, G, and Macdermid, JC. Confusion assessment method: a systematic review and meta-analysis of diagnostic accuracy. Neuropsychiatr Dis Treat. (2013) 9:1359–70. doi: 10.2147/NDT.S49520
69. Hoch, J, Bauer, JM, Bizer, M, Arnold, C, and Benzinger, P. Nurses' competence in recognition and management of delirium in older patients: development and piloting of a self-assessment tool. BMC Geriatr. (2022) 22:879. doi: 10.1186/s12877-022-03573-8
70. European Delirium Association, & American Delirium Society. The DSM-5 criteria, level of arousal and delirium diagnosis: inclusiveness is safer. BMC medicine. (2014) 12:141. doi: 10.1186/s12916-014-0141-2
71. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing (2013).
72. Mitchell, ML, Kean, S, Rattray, JE, Hull, AM, Davis, C, Murfield, JE, et al. A family intervention to reduce delirium in hospitalised ICU patients: A feasibility randomised controlled trial. Intensive & critical care nursing. (2017) 40:77–84. doi: 10.1016/j.iccn.2017.01.001
73. Kotfis, K, Van Diem-Zaal, I, Williams Roberson, S, Sietnicki, M, Van Den Boogaard, M, Shehabi, Y, et al. The future of intensive care: delirium should no longer be an issue. Crit Care. (2022) 26:200. doi: 10.1186/s13054-022-04077-y
74. Balas, MC, Vasilevskis, EE, Olsen, KM, Schmid, KK, Shostrom, V, Cohen, MZ, et al. Effectiveness and safety of the awakening and breathing coordination, delirium monitoring/management, and early exercise/mobility (ABCDE) bundle. Crit Care Med. (2014) 42:1024–36. doi: 10.1097/CCM.0000000000000129
75. Colombo, R, Corona, A, Praga, F, Minari, C, Giannotti, C, Castelli, A, et al. A reorientation strategy for reducing delirium in the critically ill. Results of an interventional study. Minerva Anestesiol. (2012) 78:1026–33.
76. Guo, Y, and Fan, Y. A preoperative, nurse-led intervention program reduces acute postoperative delirium. J Neurosci Nurs. (2016) 48:229–35. doi: 10.1097/JNN.0000000000000220
77. Patel, J, Baldwin, J, Bunting, P, and Laha, S. The effect of a multicomponent multidisciplinary bundle of interventions on sleep and delirium in medical and surgical intensive care patients. Anaesthesia. (2014) 69:540–9. doi: 10.1111/anae.12638
78. Allen, J, and Alexander, E. Prevention, recognition, and management of delirium in the intensive care unit. Aacn Adv Crit Care. (2012) 23:5–11; quiz 12–3.
79. Zaubler, TS, Murphy, K, Rizzuto, L, Santos, R, Skotzko, C, Giordano, J, et al. Quality improvement and cost savings with multicomponent delirium interventions: replication of the Hospital Elder Life Program in a community hospital. Psychosomatics. (2013) 54:219–26. doi: 10.1016/j.psym.2013.01.010
80. Guo, Y, Sun, L, Li, L, Jia, P, Zhang, J, Jiang, H, et al. Impact of multicomponent, nonpharmacologic interventions on perioperative cortisol and melatonin levels and postoperative delirium in elderly oral cancer patients. Arch Gerontol Geriatr. (2016) 62:112–7. doi: 10.1016/j.archger.2015.10.009
81. Brummel, NE, and Girard, TD. Preventing delirium in the intensive care unit. Crit Care Clin. (2013) 29:51–65. doi: 10.1016/j.ccc.2012.10.007
82. Elliott, R, Mckinley, S, Cistulli, P, and Fien, M. Characterisation of sleep in intensive care using 24-hour polysomnography: an observational study. Crit Care. (2013) 17:R46. doi: 10.1186/cc12565
83. Hu, RF, Jiang, XY, Chen, J, Zeng, Z, Chen, XY, Li, Y, et al. Non-pharmacological interventions for sleep promotion in the intensive care unit. Cochrane Database Syst Rev. (2015) 2018:CD008808. doi: 10.1002/14651858.CD008808.pub2
84. Stuck, A, Clark, MJ, and Connelly, CD. Preventing intensive care unit delirium: a patient-centered approach to reducing sleep disruption. Dimens Crit Care Nurs. (2011) 30:315–20. doi: 10.1097/DCC.0b013e31822fa97c
85. Young, J, Murthy, L, Westby, M, Akunne, A, and O'mahony, R, Guideline Development Group. Diagnosis, prevention, and management of delirium: summary of NICE guidance. BMJ. (2010) 341:c3704. doi: 10.1136/bmj.c3704
86. Barr, J, Fraser, GL, Puntillo, K, Ely, EW, Gelinas, C, Dasta, JF, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. (2013) 41:263–306. doi: 10.1097/CCM.0b013e3182783b72
87. Devlin, JW, Skrobik, Y, Gélinas, C, Needham, DM, Slooter, AJ, Pandharipande, PP, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. (2018) 46:e825–73. doi: 10.1097/CCM.0000000000003299
88. Kamdar, BB, King, LM, Collop, NA, Sakamuri, S, Colantuoni, E, Neufeld, KJ, et al. The effect of a quality improvement intervention on perceived sleep quality and cognition in a medical ICU. Crit Care Med. (2013) 41:800–9. doi: 10.1097/CCM.0b013e3182746442
89. Mistraletti, G, Pelosi, P, Mantovani, ES, Berardino, M, and Gregoretti, C. Delirium: clinical approach and prevention. Best Pract Res Clin Anaesthesiol. (2012) 26:311–26. doi: 10.1016/j.bpa.2012.07.001
90. Vidan, MT, Sanchez, E, Alonso, M, Montero, B, Ortiz, J, and Serra, JA. An intervention integrated into daily clinical practice reduces the incidence of delirium during hospitalization in elderly patients. J Am Geriatr Soc. (2009) 57:2029–36. doi: 10.1111/j.1532-5415.2009.02485.x
91. Bellelli, G, Moresco, R, Panina-Bordignon, P, Arosio, B, Gelfi, C, Morandi, A, et al. Is delirium the cognitive harbinger of frailty in older adults? A review about the existing evidence. Front Med. (2017) 4:188. doi: 10.3389/fmed.2017.00188
92. Schweickert, WD, Poholman, MC, Pohlman, AE, Nigos, C, Pawlike, AJ, Esbrook, CL, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. (2009) 373:1874–82. doi: 10.1016/S0140-6736(09)60658-9
93. Smith, M, and Meyfroidt, G. Critical illness: the brain is always in the line of fire. Intensive Care Med. (2017) 43:870–3. doi: 10.1007/s00134-017-4791-3
Keywords: delirium, post-operative, intensive care unit, nursing, multidisciplinary, cognitive impairment
Citation: Ní Chróinín D, Alexandrou E and Frost SA (2023) Delirium in the intensive care unit and its importance in the post-operative context: A review. Front. Med. 10:1071854. doi: 10.3389/fmed.2023.1071854
Edited by:
Zhongheng Zhang, Sir Run Run Shaw Hospital, ChinaReviewed by:
Jesus Rico-Feijoo, Hospital Universitario Río Hortega, SpainCopyright © 2023 Ní Chróinín, Alexandrou and Frost. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Danielle Ní Chróinín, RGFuaWVsbGUuTmlDaHJvaW5pbkBoZWFsdGgubnN3Lmdvdi5hdQ==