
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Med. , 01 March 2023
Sec. Nuclear Medicine
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1070362
This article is part of the Research Topic Targeted Alpha Particle Therapy in Oncology View all 17 articles
 Stein Gunnar Larsen1*†
Stein Gunnar Larsen1*† Wilhelm Graf2,3
Wilhelm Graf2,3 Anthony Burton Mariathasan1Olaf Sørensen1Milan Spasojevic1Mariusz Adam Goscinski1
Anthony Burton Mariathasan1Olaf Sørensen1Milan Spasojevic1Mariusz Adam Goscinski1 Silje Selboe4
Silje Selboe4 Nadja Lundstrøm3,5
Nadja Lundstrøm3,5 Anne Holtermann1
Anne Holtermann1 Mona-Elisabeth Revheim4,6Øyvind Sverre Bruland6,7,8
Mona-Elisabeth Revheim4,6Øyvind Sverre Bruland6,7,8Background: Peritoneal metastasis (PM) from colorectal cancer carries a dismal prognosis despite extensive cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS-HIPEC). With a median time to recurrence of 11–12 months, there is a need for novel therapies. Radspherin® consists of the α-emitting radionuclide radium-224 (224Ra), which has a half-life of 3.6 days and is adsorbed to a suspension of biodegradable calcium carbonate microparticles that are designed to give short-range radiation to the serosal peritoneal surface linings, killing free-floating and/or tumor cell clusters that remain after CRS-HIPEC.
Methods: A first-in-human phase 1 study (EudraCT 2018–002803-33) was conducted at two specialized CRS-HIPEC centers. Radspherin® was administered intraperitoneally 2 days after CRS-HIPEC. Dose escalation at increasing activity dose levels of 1-2-4-7-MBq, a split-dose repeated injection, and expansion cohorts were used to evaluate the safety and tolerability of Radspherin®. The aim was to explore the recommended dose and biodistribution using gamma-camera imaging. The results from the planned safety interim analysis after the completion of the dose-limiting toxicity (DLT) period of 30 days are presented.
Results: Twenty-three patients were enrolled: 14 in the dose escalation cohort, three in the repeated cohort, and six in the expansion cohort. Of the 23 enrolled patients, seven were men and 16 were women with a median age of 64 years (28–78). Twelve patients had synchronous PM stage IV and 11 patients had metachronous PM [primary stage II; (6) and stage III; (5)], with a disease-free interval of 15 months (3–30). The peritoneal cancer index was median 7 (3–19), operation time was 395 min (194–515), and hospital stay was 12 days (7–37). A total of 68 grade 2 adverse events were reported for 17 patients during the first 30 days; most were considered related to CRS and/or HIPEC. Only six of the TEAEs were evaluated as related to Radspherin®. One TEAE, anastomotic leakage, was reported as grade 3. Accordion ≥3 grade events occurred in a total of four of the 23 patients: reoperation due to anastomotic leaks (two) and drained abscesses (two). No DLT was documented at the 7 MBq dose level that was then defined as the recommended dose. The biodistribution of Radspherin® showed a relatively even peritoneal distribution.
Conclusion: All dose levels of Radspherin® were well tolerated, and DLT was not reached. No deaths occurred, and no serious adverse events were considered related to Radspherin®.
Clinical Trial Registration: Clinicaltrials.gov, NCT 03732781.
Peritoneal metastasis from colorectal cancer (CRC) carries a worse prognosis than hepatic and lung metastases (1). Most patients with metastatic CRC (mCRC) cannot be cured, illustrated by a 5-year survival of 10–20% in study patients (2, 3), and with an even more grim prognosis in population-based registries reporting a median survival of 5–12 months and 5-year survival of 5–10% (4, 5). The incidence of peritoneal metastasis (PM) is approximately 4–10% at the time of diagnosis and 4–12% in patients with recurrence after primary curative resection (6–8).
In cases with limited peritoneal tumor load, improved and even long-term survival can be achieved by combining complete cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) as shown in a randomized controlled trial (9), case–control studies (10–12), meta-analysis (13), and several cohort studies (14, 15). Systemic chemotherapy alone has a limited effect on localized PM-CRC with a median survival of 13–16 months (1, 16). CRS-HIPEC aims to remove all macroscopic tumors and achieve high intraperitoneal concentrations of hyperthermic cytotoxic drugs (17).
The outcome of CRS-HIPEC is, however, highly variable, and most patients will experience disease recurrence with a 5-year overall survival (OS) reported in about 40% of CRS-HIPEC cases (13, 15). However, the 5-year disease-free survival (DFS) is only 18% with a median time to relapse between 11 and 12 months. At the moment of recurrence, two-thirds of patients suffer either from peritoneal relapse or peritoneal relapse and distant metastases together (18).
If PM recurrence after CRS-HIPEC occurs, the prognosis is dismal. Hence, there is a definite unmet medical need for novel treatments against abdominal cancer dissemination and novel therapeutic strategies that may help preserve the surgical complete response after CRS-HIPEC.
Intraperitoneal (IP) therapy with α-emitters may be beneficial for patients with PM-CRC since hallmarks of the disease include dissemination within the abdominal cavity and residual micrometastases in a substantial number of patients. Preclinical studies have tested α-emitting radioimmunoconjugates as IP treatment of ovarian cancer, and 211At and 212Pb conjugated to antibodies are in clinical development (19–22). Preclinical and clinical data indicate that α-emitters are well tolerated without dose-limiting toxicity (23, 24).
Radspherin® is a novel treatment principle especially designed to give local radiation to the surface of the abdominal cavity based on biodegradable microparticles with 224Ra adsorbed to the particle. By injection into the peritoneal cavity, the particles are distributed and emit internal α-particle radiation to the tissue of the peritoneal lining and potentially kill remaining free cancer cells and small cell clusters and hopefully will prevent the further spread of disease.
In this study, we report our first experience from a phase 1 study in patients with PM-CRC to evaluate the safety and toxicity of Radspherin®, determine the recommended, and/or establish a recommended dose for Radspherin® as a single IP or two repeated doses following CRS-HIPEC.
The study was approved by the National Ethics Committees in Norway and Sweden, the Norwegian Medicines Agency, and the Swedish Medical Products Agency. Data were registered in the Sponsors database (Viedoc eCRF).
A first-in-human, phase 1 study (EudraCT 2018–002803-33) was conducted at two specialized CRS-HIPEC centers in Oslo, Norway, and Uppsala, Sweden. Twenty-three patients were included between 11 May 2020 and 16 August 2021. Twenty-nine patients were screened. CRS was performed to remove all macroscopically visible tumors, involving peritonectomy procedures and organ resections as necessary. Peritoneal tumor distribution was classified using the peritoneal cancer index (PCI) (25), and the completeness of cytoreduction (CC) score (25) was used to evaluate residual tumor after CRS. All CC-0 cases were given HIPEC. All anastomoses were completed before the HIPEC procedure.
The synchronous PM was defined as a diagnosis at or within 6 months of primary surgery, and disease-free interval (DFI) was the time from primary surgery to diagnosis of PM. Postoperative complications (30-day morbidity and mortality) were classified according to Accordion (26).
Hyperthermic intraperitoneal chemotherapy was administrated using a closed technique with an open abdomen in Norway (27), whereas the closed abdomen technique was used in Sweden (28). In Norway, the HIPEC regimen contained mitomycin, 35 mg/m2 (maximum 70 mg), given in three fractions for 90 min (50% initially, 25%/30 min, and 25%/60 min), whereas in Sweden, oxaliplatin 460 mg/m2 or irinotecan 460 mg/m2 were both given in 30 min.
Following the CRS-HIPEC, an in-dwelling peritoneal Blake catheter was placed anteriorly in the upper abdominal cavity. The catheter was obliquely tunneled, clamped, and fixed to the abdominal wall to reduce the risk of leakage or displacement.
The dose escalation was performed as a 3 + 3 design (Figure 1), increasing dose levels starting at 1 MBq followed by 2, 4, and 7 MBq or until eventual dose-limiting toxicity (DLT) was observed. The repeated injection cohort included three subjects for the highest dose level that has been declared safe (explored as a split dose of two separate injections given 1 week apart). The study also involved an expansion cohort with six subjects at the highest safe activity dose safe. Radspherin® was injected in the abdominal cavity through a catheter 2 days after CRS-HIPEC for patients to have stabilized after the complex surgery. Each subject was followed until disease progression in the abdominal cavity or for 12 months (18 months after the highest dose level) after the administration of Radspherin®. The results from the safety interim analysis after the completion of the pre-defined DLT period of 30 days are presented.
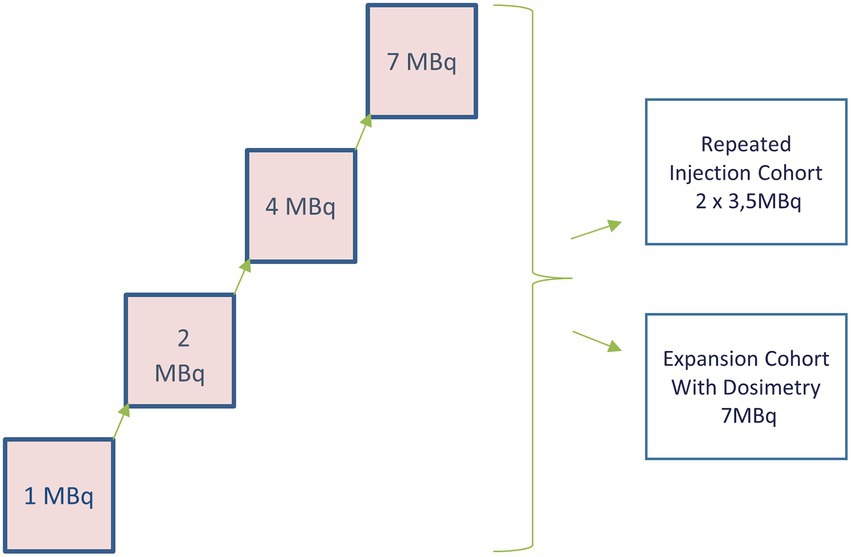
Figure 1. Dose escalation aimed to define the recommended dose on 3 + 3 subjects (12). Thereafter, a repeated injection cohort (3) and an expansion cohort were performed (6).
Dose-calibrated Radspherin® (up to 10 mL containing 0.7–1 g of particles) was prepared at the nuclear medicine department at the site and administered as a single bolus injection via a three-way Luer lock connected to the inserted peritoneal catheter. After the injection, the catheter was flushed with about 250 ml of isotonic solution, and in all instances, all drains were kept clamped for a minimum of 72 h, except in one patient where a laparotomy was performed after 65 h. The patient moved from side to side in the bed regularly for the first 2 h after installation. For repeated injections, the same in-dwelling peritoneal catheter was used and then removed 3–4 days later.
The peritoneal distribution of Radspherin® particles was examined by single-photon emission computed tomography/computed tomography (SPECT/CT) gamma-camera imaging performed on days 1, 2, and 3 (Day 6 for the dosimetry cohort). The patients were followed closely during the hospital stay and later at pre-scheduled intervals to discover complications such as suspected unexpected serious adverse reactions (SUSARs), serious adverse effects (SAEs), and adverse effects (AEs). The EMA “Guideline on strategies to identify and mitigate risks for first-in-human and early clinical trials with investigational medicinal products” (EMEA/CHMP/SWP/28367/07 Rev. 1) has been considered for the assessment of factors of risk.
The primary objectives of the study were to investigate the safety and toxicity of Radspherin® and to determine the recommended dose of Radspherin®, among the four suggested doses of 1, 2, 4, and 7 MBq following CRS and HIPEC (Figure 1).
The secondary objectives of the study were to establish a recommended dose of Radspherin® as a single IP injection or two repeated IP injections following CRS and HIPEC and to describe the biodistribution of Radspherin®.
According to national guidelines, adjuvant chemotherapy was not routinely given. In the case of synchronous PM with locoregional lymph node metastasis, adjuvant chemotherapy was recommended after CRS-HIPEC/Radspherin®, otherwise not.
All data were recorded in the eCRF, and external study monitoring and source data verification were performed. The study was reviewed by an Independent Data Monitoring Committee. Categorical variables were described using frequencies/percentages, and continuous variables were described with median/range. Safety evaluations were based on the incidence, intensity, and type of AEs, and clinically significant changes in the subjects’ vital signs and clinical laboratory results.
Twenty-nine patients were screened for the study (Figure 2). Totally, there were six screening failures due to the extent of metastasis (PCI > 20; 3), other previous malignant diseases (2), or peroperative bleeding (1) leading to exclusion from the study before the decision on giving Radspherin®. Accordingly, 23 patients were given Radspherin®. Of the 23 patients, 19 patients were treated at Oslo University Hospital and four at Uppsala Academic Hospital in Sweden. The study had a dose escalation cohort (14 pts.) with increasing doses from 1 MBq (4 pts.) to 2 MBq (3 pts.), 4 MBq (4 pts.), and 7 MBq (3 pts.), a repeated cohort (3 pts.) with 3.5 MBq given two times with 1-week interval, and an expansion cohort on highest dose level 7 MBq with additional six patients (Figure 1).
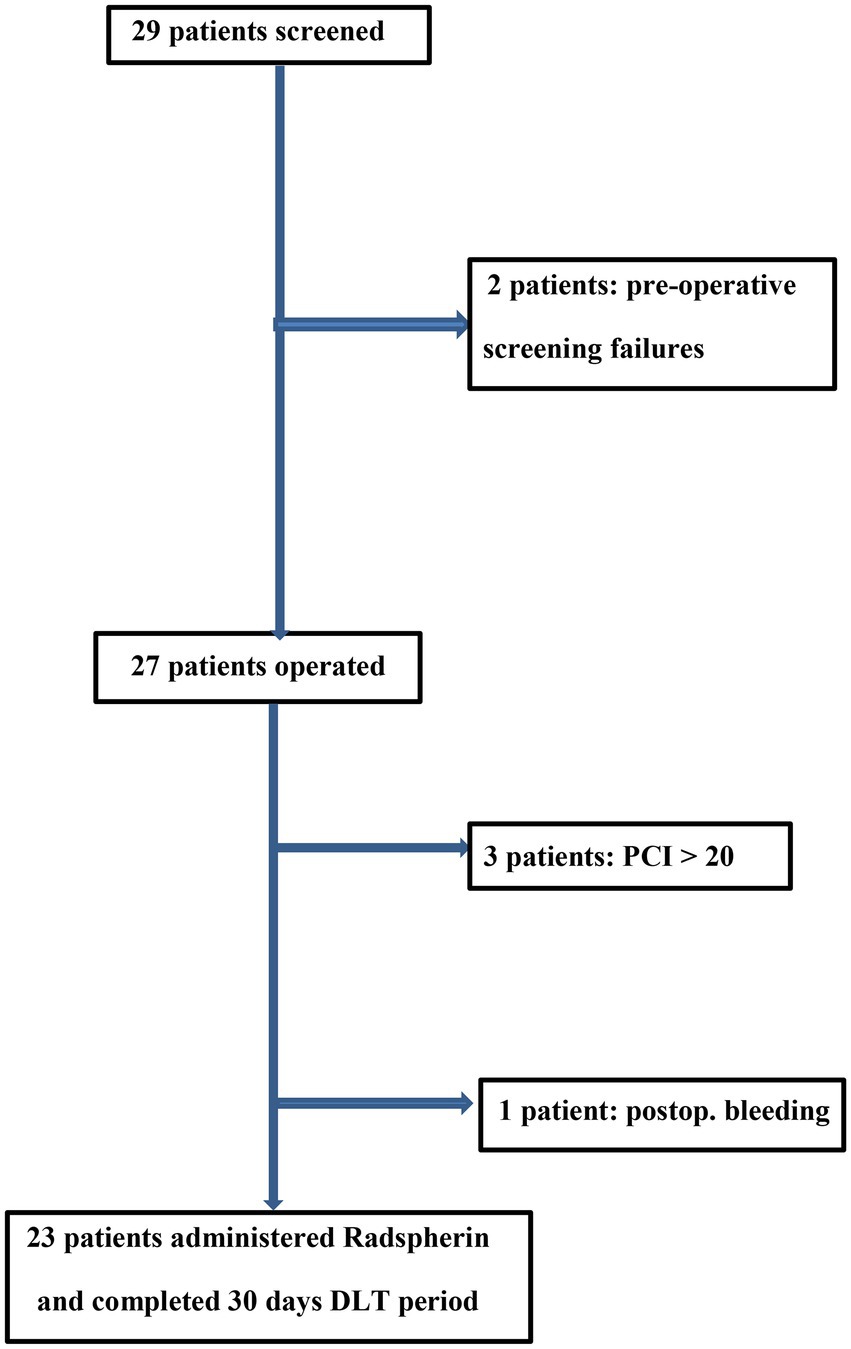
Figure 2. Consort flow diagram of the study patients (n = 23).
Table 1 summarizes the clinicopathological characteristics of the study cohort, which comprised 16 women (70%) and seven men (30%) with a median age of 64 years (28–78). Twelve patients were diagnosed with IUCC stage IV disease after primary surgery. Metachronous metastasis occurred after a disease-free interval (DFI) of median of 11 months (range 3–30). Approximately 43% had received chemotherapy at some point before CRS-HIPEC. Performance status was in most cases ECOG 0, while only one patient was in ECOG 1. One patient in the 7 MBq cohort received neoadjuvant irradiation therapy. Lymph node metastasis was present in 15 patients (65%) of the primary cases.
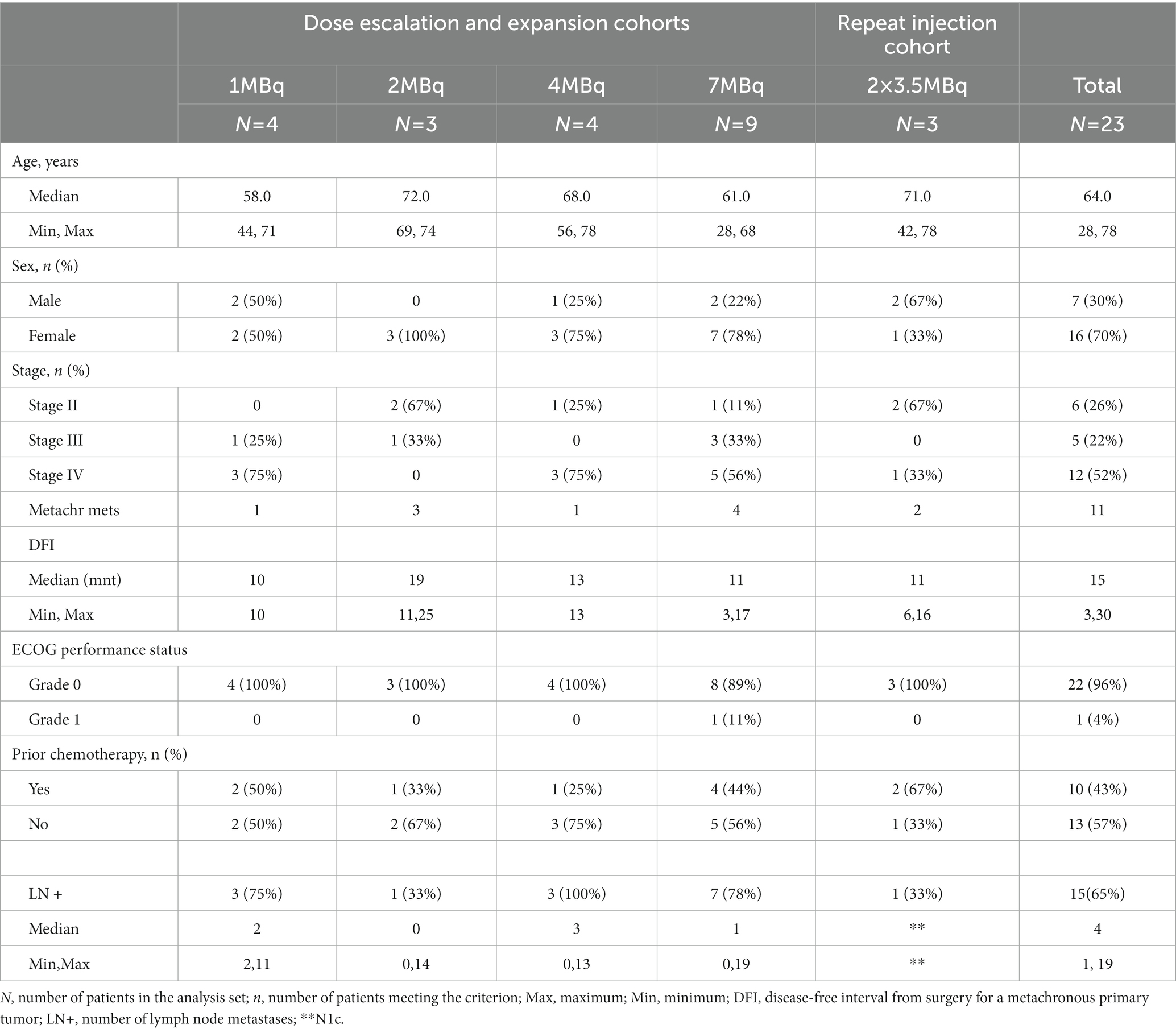
Table 1. Clinicopathological characteristics after CRS-HIPEC (n = 23).
The median PCI at the time of CRS-HIPEC was 7 (3–19; Table 2). The median duration of surgery was 374 min (266–508). The median peroperative bleeding was 300 mL (50–1,000 mL). In-hospital time was 11 days (7–37). At Norwegian Radium Hospital, HIPEC is performed with mitomycin C, 35 mg/m2 up to 70 mg, median 63 mg (57–70), and given in a closed perfusion circuit with open abdomen; duration 90 min; and intra-abdominal temperature median 42.0°C. In Uppsala, oxaliplatin 460 mg/m2 or irinotecan 460 mg/m2 was perfused for 30 min. Accordingly, the total operation time was reduced by 60 min compared to the Norwegian site. The knife time is then median more than 4 h before HIPEC in this study with complex surgery for PM.
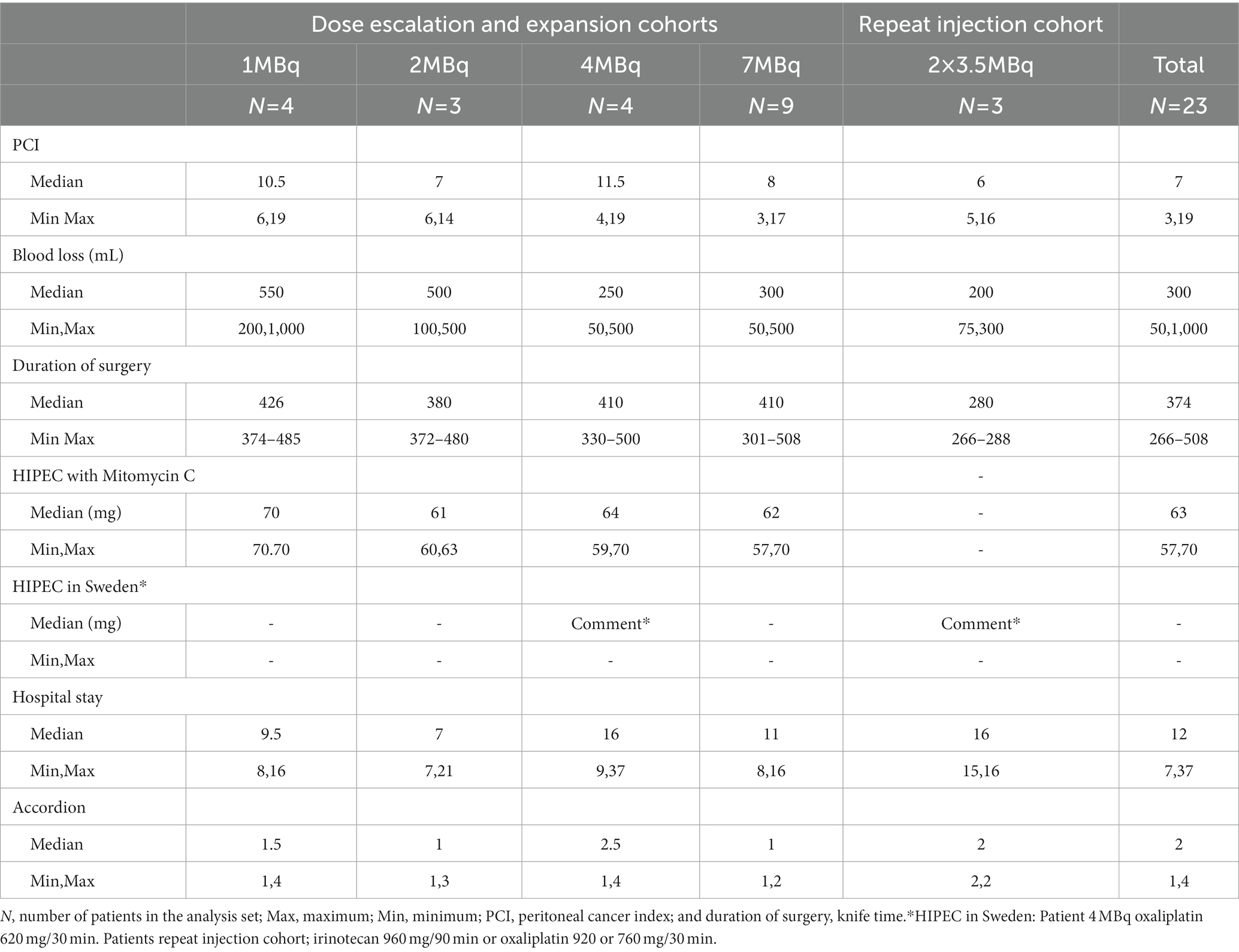
Table 2. Characteristics after CRS-HIPEC (n = 23).
The highest dose escalation level 4, the 7 MBq dose, was selected as recommended dose, as no DLT was observed. The incidence of DLTs, TEAEs, and SAEs is summarized in Table 3. The actual amount of Radspherin® administered is shown in Table 4. All 23 patients were included in the safety population. A total of 68 TEAEs were reported for 17 patients (74%) during the first 30 days. Of these, 23 of grade 2 before Radspherin® installation and 45 of grade 2 in the time period after Radspherin® installation (Days 1–30) were reported in 16 patients. There was one grade 3 TEAE which was reported as SAE but unrelated to Radspherin®. The most frequently reported AEs were vomiting, pyrexia, nausea, and decreased appetite, and the majority were considered related to CRS and/or HIPEC. Only six of the TEAEs were evaluated as related to Radspherin® and laboratory test abnormalities [platelet count increased, blood alkaline phosphatase increased, hemoglobin decreased (n = 2), monocyte count increased, and hepatic enzyme abnormal]. All these TEAEs were resolved with no actions taken and no need for additional treatment.
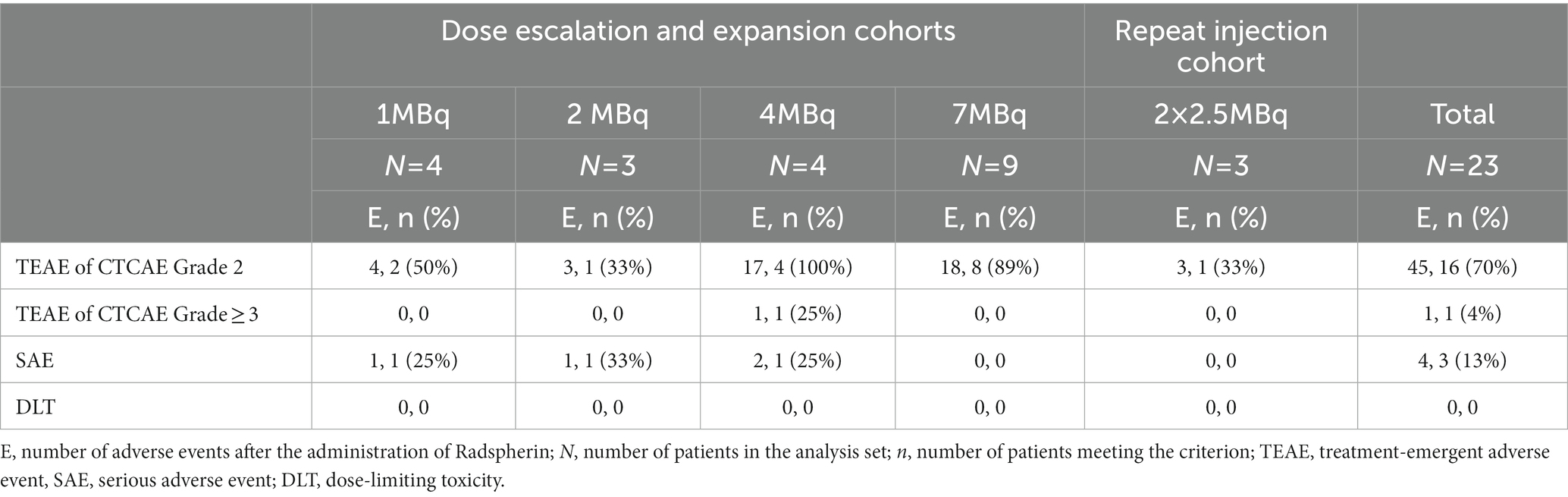
Table 3. Number of treatment-emergent adverse events in the time period of 1–30 days.
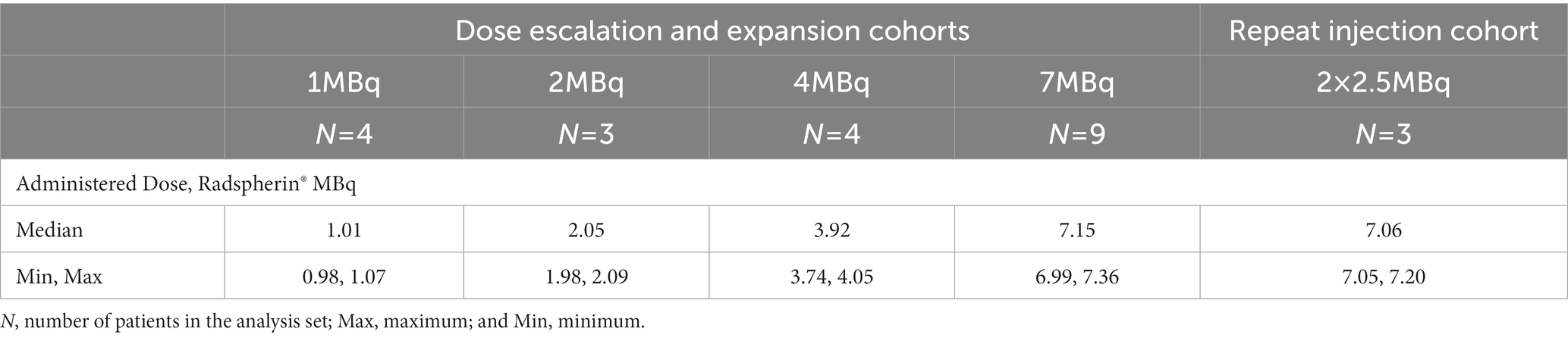
Table 4. Administered dose and compliance.
Four SAEs within 30 days were reported for three patients, and all were considered unrelated to Radspherin®. These SAEs included one anastomotic leak (grade 3), which was reoperated on Day 2, two abdominal infections (grade 2) that required a drain on Day 10, and an anastomotic leak that required reoperation on Day 10 and a drain on Day 15 (see the section “Discussion”). During reoperations, abdominal fluid was drained before opening the abdomen, washed out with physiological saline solution liquid, and removed as irradiation waste. No patients in the repeat injection cohort had any SAE. No deaths or study discontinuations due to TEAEs or SAEs were reported during the 30 days.
Corresponding Accordion grade 3 events occurred in two of the 23 patients (draining of abscesses) and Accordion grade 4 events in two (reoperation due to anastomotic leaks; Table 3). There were no deaths within 100 days. The biodistribution of Radspherin® showed a relatively even peritoneal distribution, and an example is shown in Figure 3.
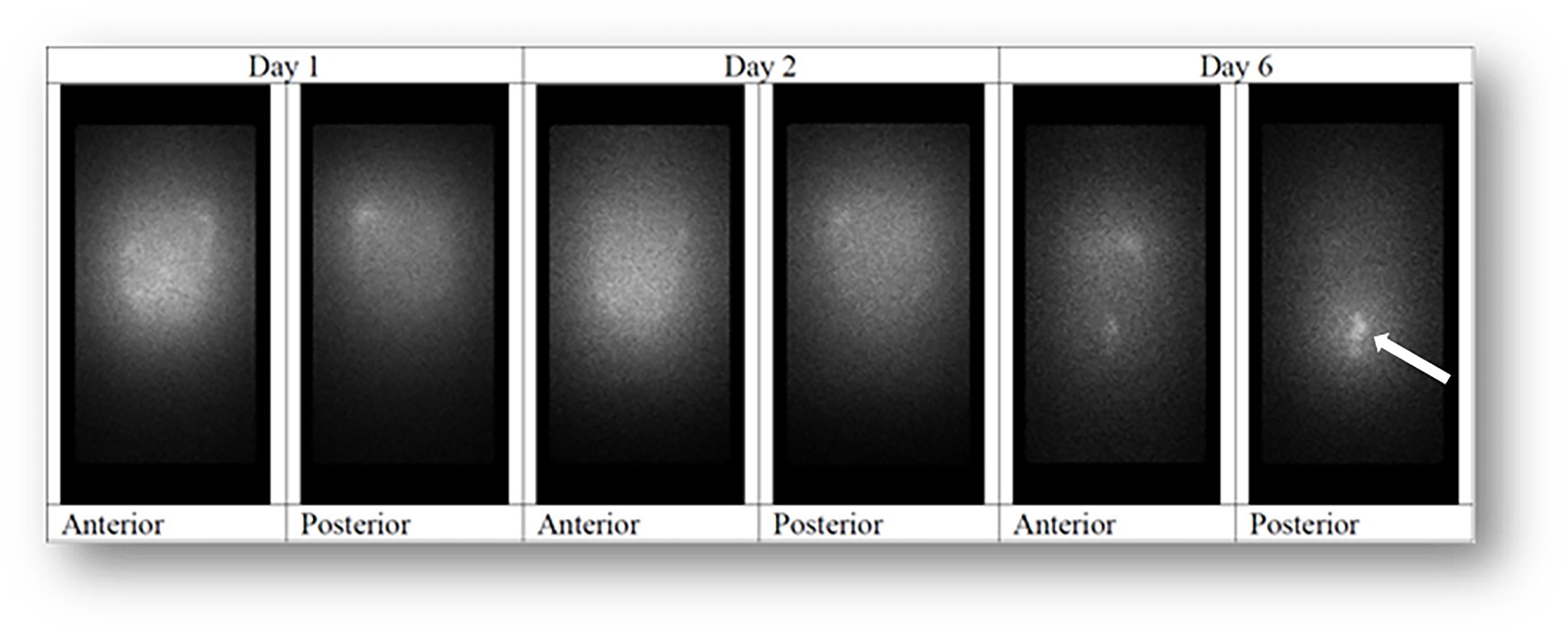
Figure 3. 224Ra-labeled microparticles for patient at 7 MBq were evenly distributed in the abdominal cavity both in the anterior and posterior images. In this subject, an area with a slightly higher activity was observed in the left upper region. No areas with low levels of activity were observed. At a late time point, uptake was observed in the distal large intestine (arrow).
The CRS-HIPEC procedure is well known to be associated with postoperative complications (29), and significantly higher incidences of severe postoperative complications (i.e., fistulas and anastomotic leaks) have been observed in patients treated with HIPEC than in patients treated without HIPEC (30).
In the current study, there was no 30-day mortality. The incidence of severe postoperative complications (Accordion 3), the need for drainage or parenteral nutrition occurring in five of the 23 patients (22%), and the reoperation rate of 9% (two of 23 patients) were all as expected and suggest that the treatment with Radspherin® is well tolerated and safe. The first patient with anastomotic leakage in the study experienced an increase in white blood cells to 18.7 × 109/L and a moderate elevation of C-reactive protein (CRP) to 61 the day after surgery and the day before Radspherin® installation, followed by antibiotics the next day and reoperation with the verification of anastomotic leakage 2 days after Radspherin®. The other patient also experienced an increase in white blood cells to 16.7 × 109/L and a moderate CRP increase to 58 the day after surgery and received Radspherin® the following day. Five days later, intravenous antibiotics were started due to an infection. Anastomotic leakage was diagnosed on Day 10, and a laparotomy with resection and stoma was performed. Both cases were considered caused by infection before Radspherin® and to be related to the CRS and HIPEC procedures.
In other larger patient series, postoperative mortality between 0.7 and 7.7% has been reported (29, 31, 32) with reoperation rates varying between 4 and 20.8% (13). Oslo University Hospital has previously reported corresponding numbers of 0% (mortality), 15% (Accordion ≥3), and 8% (reoperation rate) (14) with CRS-HIPEC and without Radspherin®.
Norwegian Radium Hospital recently performed a dose-escalating phase I trial with intraperitoneal (IP) MOC31PE immunotoxin in PM-CRC after CRS-HIPEC (33) showing promising results for better control of PM. The hospital has used radium and α-emitters for the treatment of metastatic cancer with Xofigo®, a 223Ra radiopharmaceutical. Xofigo® was approved by the FDA and EMEA in 2013 for the treatment of symptomatic bone metastasis from prostate cancer.
Because of the short range and high linear energy transfer of α-particle emitters, there is a much higher relative biological effectiveness of the radiation from Radspherin® than from β-particle emitting radiopharmaceuticals previously used. Thereby, α-particle emitters are theoretically more efficient in treating micrometastases and killing chemotherapy-resistant tumor cells. The much shorter radiation range prevents the radiation of tissue in deeper regions of sensitive abdominal organs (i.e., small intestine), which was the prime reason for abandoning the β-particle emitting radiopharmaceuticals, giving a discrete surface irradiation of just the serosal lining of the peritoneal cavity.
This favorable safety profile in the current study is in line with documentation from other preclinical and clinical studies with other related alpha-emitting compounds administered intraperitoneally. Safety and effect of IP administration have been demonstrated in animal models both with colloids/particles and antibodies as carriers of a range of radionuclides: 211At polymers (34, 35), bismuth-213 (213Bi) antibodies (36), 211At antibodies (37, 38), 212Pb antibodies (21, 39, 40), thorium-227 (227)Th antibodies (41), and actinium-225 (225Ac) antibodies (42).
All dose levels of Radspherin® were well tolerated with DLT not reached. No deaths occurred, and no SAEs were considered related to Radspherin®. The biodistribution of Radspherin® showed a good peritoneal distribution of the radiolabeled microparticles. Long-term safety, dosimetry, and first efficacy results of Radspherin® will be reported after 18 months of the follow-up period.
All dose levels of Radspherin® were well tolerated with DLT not reached. No deaths occurred, and no SAEs were considered related to Radspherin®. The biodistribution of Radspherin® showed a good peritoneal distribution of the radiolabeled microparticles.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by National Ethics Committees in Norway and Sweden. The patients/participants provided their written informed consent to participate in this study.
SL, M-ER, and ØB: conceptualization. SL, WG, M-ER, and ØB: study design and drafting the manuscript and revising it critically for important intellectual content. SL, WG, and ØB: data analysis. SL, WG, SS, NL, AH, M-ER, and ØB: interpretation of results. All authors contributed to the article and approved the submitted version.
This study was funded by Oncoinvent AS and Innovation Norway.
The authors thank the sponsor Oncoinvent AS for their teams involved in Radspherin® production and clinical trial support. We also thank the other members on the delegation log for their collaboration (Lars Tore Gyland Michalsen, Benedicte Haug Olsen, Ayca Muftuler Løndalen, Gasha Rashid, Anders Tulipan, Ebbe Billmann Thorgersen, Simen Grønningsæter, and Ingrid Vedaa Skåla) and the nurse staffs in both hospitals.
ØB is a clinical consultant to and holds ownership in Oncoinvent AS.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that this study received funding from Oncoinvent AS. Oncoinvent AS was involved in the study design, collection, analysis, interpretation of data and the decision to submit this article for publication.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1.Franko, J, Shi, Q, Meyers, JP, Maughan, TS, Adams, RA, Seymour, MT, et al. Prognosis of patients with peritoneal metastatic colorectal cancer given systemic therapy: an analysis of individual patient data from prospective randomised trials from the analysis and research in cancers of the digestive system (ARCAD) database. Lancet Oncol. (2016) 17:1709–19. doi: 10.1016/S1470-2045(16)30500-9
2.Kopetz, S, Chang, GJ, Overman, MJ, Eng, C, Sargent, DJ, Larson, DW, et al. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. J Clin Oncol. (2009) 27:3677–83. doi: 10.1200/JCO.2008.20.5278
3.Tveit, KM, Guren, T, Glimelius, B, Pfeiffer, P, Sorbye, H, Pyrhonen, S, et al. Phase III trial of cetuximab with continuous or intermittent fluorouracil, leucovorin, and oxaliplatin (Nordic FLOX) versus FLOX alone in first-line treatment of metastatic colorectal cancer: the NORDIC-VII study. J Clin Oncol. (2012) 30:1755–62. doi: 10.1200/JCO.2011.38.0915
4.Sorbye, H, Cvancarova, M, Qvortrup, C, Pfeiffer, P, and Glimelius, B. Age-dependent improvement in median and long-term survival in unselected population-based Nordic registries of patients with synchronous metastatic colorectal cancer. Ann Oncol. (2013) 24:2354–60. doi: 10.1093/annonc/mdt197
5.Abdel-Rahman, O. A real-world, population-based study of the outcomes of patients with metastatic colorectal cancer to the peritoneum treated with or without cytoreductive surgery. Int J Color Dis. (2020) 35:719–25. doi: 10.1007/s00384-020-03525-x
6.Segelman, J, Granath, F, Holm, T, Machado, M, Mahteme, H, and Martling, A. Incidence, prevalence and risk factors for peritoneal carcinomatosis from colorectal cancer. Br J Surg. (2012) 99:699–705. doi: 10.1002/bjs.8679
7.Koppe, MJ, Nagtegaal, ID, de Wilt, JH, and Ceelen, WP. Recent insights into the pathophysiology of omental metastases. J Surg Oncol. (2014) 110:670–5. doi: 10.1002/jso.23681
8.Confuorto, G, Giuliano, ME, Grimaldi, A, and Viviano, C. Peritoneal carcinomatosis from colorectal cancer: HIPEC? Surg Oncol. (2007) 16:S149–52. doi: 10.1016/j.suronc.2007.10.026
9.Verwaal, VJ, Bruin, S, Boot, H, van Slooten, G, and van Tinteren, H. 8-year follow-up of randomized trial: cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer. Ann Surg Oncol. (2008) 15:2426–32. doi: 10.1245/s10434-008-9966-2
10.Elias, D, Lefevre, JH, Chevalier, J, Brouquet, A, Marchal, F, Classe, JM, et al. Complete cytoreductive surgery plus intraperitoneal chemohyperthermia with oxaliplatin for peritoneal carcinomatosis of colorectal origin. J Clin Oncol. (2009) 27:681–5. doi: 10.1200/JCO.2008.19.7160
11.Franko, J, Ibrahim, Z, Gusani, NJ, Holtzman, MP, Bartlett, DL, and Zeh, HJ 3rd. Cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion versus systemic chemotherapy alone for colorectal peritoneal carcinomatosis. Cancer. (2010) 116:3756–62. doi: 10.1002/cncr.25116
12.Mahteme, H, Hansson, J, Berglund, A, Pahlman, L, Glimelius, B, Nygren, P, et al. Improved survival in patients with peritoneal metastases from colorectal cancer: a preliminary study. Br J Cancer. (2004) 90:403–7. doi: 10.1038/sj.bjc.6601586
13.Mirnezami, R, Mehta, AM, Chandrakumaran, K, Cecil, T, Moran, BJ, Carr, N, et al. Cytoreductive surgery in combination with hyperthermic intraperitoneal chemotherapy improves survival in patients with colorectal peritoneal metastases compared with systemic chemotherapy alone. Br J Cancer. (2014) 111:1500–8. doi: 10.1038/bjc.2014.419
14.Froysnes, IS, Larsen, SG, Spasojevic, M, Dueland, S, and Flatmark, K. Complete cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for colorectal peritoneal metastasis in Norway: prognostic factors and oncologic outcome in a national patient cohort. J Surg Oncol. (2016) 114:222–7. doi: 10.1002/jso.24290
15.Larsen, SG, Goscinski, MA, Dueland, S, Steigen, SE, Hofsli, E, Torgunrud, A, et al. Impact of KRAS, BRAF and microsatellite instability status after cytoreductive surgery and HIPEC in a national cohort of colorectal peritoneal metastasis patients. Br J Cancer. (2022) 126:726–35. doi: 10.1038/s41416-021-01620-6
16.Franko, J, Shi, Q, Goldman, CD, Pockaj, BA, Nelson, GD, Goldberg, RM, et al. Treatment of colorectal peritoneal carcinomatosis with systemic chemotherapy: a pooled analysis of north central cancer treatment group phase III trials N9741 and N9841. J Clin Oncol. (2012) 30:263–7. doi: 10.1200/JCO.2011.37.1039
17.Brucher, BL, Piso, P, Verwaal, V, Esquivel, J, Derraco, M, Yonemura, Y, et al. Peritoneal carcinomatosis: cytoreductive surgery and HIPEC--overview and basics. Cancer Investig. (2012) 30:209–24. doi: 10.3109/07357907.2012.654871
18.Elias, D, Gilly, F, Boutitie, F, Quenet, F, Bereder, JM, Mansvelt, B, et al. Peritoneal colorectal carcinomatosis treated with surgery and perioperative intraperitoneal chemotherapy: retrospective analysis of 523 patients from a multicentric French study. J Clin Oncol. (2010) 28:63–8. doi: 10.1200/JCO.2009.23.9285
19.Andersson, H, Cederkrantz, E, Back, T, Divgi, C, Elgqvist, J, Himmelman, J, et al. Intraperitoneal alpha-particle radioimmunotherapy of ovarian cancer patients: pharmacokinetics and dosimetry of (211)at-MX35 F(ab')2--a phase I study. J Nucl Med. (2009) 50:1153–60. doi: 10.2967/jnumed.109.062604
20.Milenic, DE, Molinolo, AA, Solivella, MS, Banaga, E, Torgue, J, Besnainou, S, et al. Toxicological studies of 212Pb intravenously or intraperitoneally injected into mice for a phase 1 trial. Pharmaceuticals (Basel). (2015) 8:416–34. doi: 10.3390/ph8030416
21.Kasten, BB, Azure, MT, Schoeb, TR, Fisher, DR, and Zinn, KR. Imaging, biodistribution, and toxicology evaluation of 212Pb-TCMC-trastuzumab in nonhuman primates. Nucl Med Biol. (2016) 43:391–6. doi: 10.1016/j.nucmedbio.2016.04.001
22.Meredith, R, Torgue, J, Shen, S, Fisher, DR, Banaga, E, Bunch, P, et al. Dose escalation and dosimetry of first-in-human alpha radioimmunotherapy with 212Pb-TCMC-trastuzumab. J Nucl Med. (2014) 55:1636–42. doi: 10.2967/jnumed.114.143842
23.Cederkrantz, E, Andersson, H, Bernhardt, P, Back, T, Hultborn, R, Jacobsson, L, et al. Absorbed doses and risk estimates of (211)at-MX35 F(ab')2 in intraperitoneal therapy of ovarian cancer patients. Int J Radiat Oncol Biol Phys. (2015) 93:569–76. doi: 10.1016/j.ijrobp.2015.07.005
24.Meredith, S, Hilliard, J, and Vaillancourt, R. Evaluation of a rapid hydration protocol: safety and effectiveness. J Oncol Pharm Pract. (2017) 23:249–54. doi: 10.1177/1078155216631406
25.Jacquet, P, and Sugarbaker, PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat Res. (1996) 82:359–74. doi: 10.1007/978-1-4613-1247-5_23
26.Strasberg, SM, Linehan, DC, and Hawkins, WG. The accordion severity grading system of surgical complications. Ann Surg. (2009) 250:177–86. doi: 10.1097/SLA.0b013e3181afde41
27.Benoit, L, Cheynel, N, Ortega-Deballon, P, Giacomo, GD, Chauffert, B, and Rat, P. Closed hyperthermic intraperitoneal chemotherapy with open abdomen: a novel technique to reduce exposure of the surgical team to chemotherapy drugs. Ann Surg Oncol. (2008) 15:542–6. doi: 10.1245/s10434-007-9635-x
28.Goldenshluger, M, Zippel, D, Ben-Yaacov, A, Dux, J, Yalon, T, Zendel, A, et al. Core body temperature but not intraabdominal pressure predicts postoperative complications following closed-system Hyperthermic intraperitoneal chemotherapy (HIPEC) administration. Ann Surg Oncol. (2018) 25:660–6. doi: 10.1245/s10434-017-6279-3
29.Cashin, PH, Graf, W, Nygren, P, and Mahteme, H. Cytoreductive surgery and intraperitoneal chemotherapy for colorectal peritoneal carcinomatosis: prognosis and treatment of recurrences in a cohort study. Eur J Surg Oncol. (2012) 38:509–15. doi: 10.1016/j.ejso.2012.03.001
30.Baratti, D, Kusamura, S, Laterza, B, Balestra, MR, and Deraco, M. Early and long-term postoperative management following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. World J Gastrointest Oncol. (2010) 2:36–43. doi: 10.4251/wjgo.v2.i1.36
31.Simkens, GA, van Oudheusden, TR, Braam, HJ, Luyer, MD, Wiezer, MJ, van Ramshorst, B, et al. Treatment-related mortality after Cytoreductive surgery and HIPEC in patients with colorectal peritoneal Carcinomatosis is underestimated by conventional parameters. Ann Surg Oncol. (2016) 23:99–105. doi: 10.1245/s10434-015-4699-5
32.Yonemura, Y, Canbay, E, and Ishibashi, H. Prognostic factors of peritoneal metastases from colorectal cancer following cytoreductive surgery and perioperative chemotherapy. ScientificWorldJournal. (2013) 2013:978394. doi: 10.1155/2013/978394
33.Froysnes, IS, Andersson, Y, Larsen, SG, Davidson, B, Oien, JT, Olsen, KH, et al. Novel treatment with intraperitoneal MOC31PE immunotoxin in colorectal peritoneal metastasis: results from the ImmunoPeCa phase 1 trial. Ann Surg Oncol. (2017) 24:1916–22. doi: 10.1245/s10434-017-5814-6
34.Larsen, RH, Hoff, P, Vergote, IB, Bruland, OS, Aas, M, De Vos, L, et al. Alpha-particle radiotherapy with 211At-labeled monodisperse polymer particles, 211At-labeled IgG proteins, and free 211At in a murine intraperitoneal tumor model. Gynecol Oncol. (1995) 57:9–15. doi: 10.1006/gyno.1995.1093
35.Vergote, I, Larsen, RH, de Vos, L, Nesland, JM, Bruland, O, Bjorgum, J, et al. Therapeutic efficacy of the alpha-emitter 211At bound on microspheres compared with 90Y and 32P colloids in a murine intraperitoneal tumor model. Gynecol Oncol. (1992) 47:366–72. doi: 10.1016/0090-8258(92)90141-5
36.Milenic, D, Garmestani, K, Dadachova, E, Chappell, L, Albert, P, Hill, D, et al. Radioimmunotherapy of human colon carcinoma xenografts using a 213Bi-labeled domain-deleted humanized monoclonal antibody. Cancer Biother Radiopharm. (2004) 19:135–47. doi: 10.1089/108497804323071904
37.Elgqvist, J, Andersson, H, Back, T, Hultborn, R, Jensen, H, Karlsson, B, et al. Therapeutic efficacy and tumor dose estimations in radioimmunotherapy of intraperitoneally growing OVCAR-3 cells in nude mice with 211At-labeled monoclonal antibody MX35. J Nucl Med. (2005) 46:1907–15.
38.Palm, S, Back, T, Claesson, I, Danielsson, A, Elgqvist, J, Frost, S, et al. Therapeutic efficacy of astatine-211-labeled trastuzumab on radioresistant SKOV-3 tumors in nude mice. Int J Radiat Oncol Biol Phys. (2007) 69:572–9. doi: 10.1016/j.ijrobp.2007.06.023
39.Milenic, DE, Garmestani, K, Brady, ED, Albert, PS, Ma, D, Abdulla, A, et al. Alpha-particle radioimmunotherapy of disseminated peritoneal disease using a 212Pb-labeled radioimmunoconjugate targeting HER2. Cancer Biother Radiopharm. (2005) 20:557–68. doi: 10.1089/cbr.2005.20.557
40.Boudousq, V, Bobyk, L, Busson, M, Garambois, V, Jarlier, M, Charalambatou, P, et al. Comparison between internalizing anti-HER2 mAbs and non-internalizing anti-CEA mAbs in alpha-radioimmunotherapy of small volume peritoneal carcinomatosis using 212Pb. PLoS One. (2013) 8:e69613. doi: 10.1371/journal.pone.0069613
41.Heyerdahl, H, Abbas, N, Sponheim, K, Mollatt, C, Bruland, O, and Dahle, J. Targeted alpha therapy with 227Th-trastuzumab of intraperitoneal ovarian cancer in nude mice. Curr Radiopharm. (2013) 6:106–16. doi: 10.2174/18744710113069990018
42.Essler, M, Gartner, FC, Neff, F, Blechert, B, Senekowitsch-Schmidtke, R, Bruchertseifer, F, et al. Therapeutic efficacy and toxicity of 225Ac-labelled vs. 213Bi-labelled tumour-homing peptides in a preclinical mouse model of peritoneal carcinomatosis. Eur J Nucl Med Mol Imaging. (2012) 39:602–12. doi: 10.1007/s00259-011-2023-6
Keywords: metastatic colorectal cancer, peritoneal metastasis, cytoreductive surgery, hyperthermic intraperitoneal chemotherapy, 224Ra, alpha emitter, targeted alpha particle therapy
Citation: Larsen SG, Graf W, Mariathasan AB, Sørensen O, Spasojevic M, Goscinski MA, Selboe S, Lundstrøm N, Holtermann A, Revheim M-E and Bruland &S (2023) First experience with 224Radium-labeled microparticles (Radspherin®) after CRS-HIPEC for peritoneal metastasis in colorectal cancer (a phase 1 study). Front. Med. 10:1070362. doi: 10.3389/fmed.2023.1070362
Edited by:
Aditi Bhatt, Zydus Hospitals, IndiaReviewed by:
Vikas Prasad, Washington University, United StatesCopyright © 2023 Larsen, Graf, Mariathasan, Sørensen, Spasojevic, Goscinski, Selboe, Lundstrøm, Holtermann, Revheim and Bruland. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stein Gunnar Larsen, c3RsQG91cy1oZi5ubw==
†ORCID: Stein Gunnar Larsen https://orcid.org/0000-0002-9831-1995
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.