 Marta Calatroni
Marta Calatroni
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Med., 09 January 2023
Sec. Rheumatology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.990252
This article is part of the Research TopicSarcoidosis and Autoimmunity: from Bench to BedsideView all 8 articles
Sarcoidosis is a systemic inflammatory disease of unknown etiology. Kidney involvement in sarcoidosis may be present in up 25–30% of cases. An early diagnosis and prompt treatment with corticosteroids can improve the prognosis but rarely renal sarcoidosis can lead to kidney failure needing renal replacement therapy (RRT). Acute kidney injury (AKI) in sarcoidosis may be caused by granulomatous interstitial nephritis (GIN) or hypercalcemia. These disorders are usually clinically silent and may lead end stage renal disease (ESKD) if not diagnosed or detected too late. In patients with ESKD, dialysis and renal transplantation can offer results comparable to those observed in patients with other causes of kidney failure. Based on a review of literature, we present an overview of RRT in patients with AKI or chronic kidney disease (CKD) caused by sarcoidosis.
Sarcoidosis is an inflammatory systemic disease of unknown etiology characterized by abnormal collections of inflammatory cells that form granulomas. Sarcoidosis usually occurs between the ages of 20 and 50 years and women are 30% more affected than men (1). The disease occurs worldwide with an estimated prevalence of 10–160 per 100,000 population. However, there are significant differences in the various geographical regions of the world with higher prevalence in Afro-Americans, Caribbean, and in Northern countries (2–7). The diagnosis of sarcoidosis is difficult and the disease may remain undetected in several cases. In the absence of standardized criteria, a panel of the American Thoracic Society proposed to use three major criteria: a compatible clinical presentation, finding non-necrotizing granulomatous inflammation in one or more tissue samples, and the exclusion of alternative causes of granulomatous disease (8). Sarcoidosis may affect multiple organs. The lungs are the affected organ in >90% of cases and pulmonary sarcoidosis may be responsible of progressive respiratory disease, that remains a leading cause of death and disability (9, 10). Renal involvement in patients with sarcoidosis occurs in up to 25–43% (11, 12). A wide spectrum of renal diseases has been reported in patients with sarcoidosis, including granulomatous interstitial nephritis (GIN), several subtypes of glomerulonephritis, renal stones and nephrocalcinosis (13–15) (Table 1). Kidney involvement may be severe, leading to kidney failure in acute and in chronic disease. Only case reports and few small retrospective studies have been reported in literature and little information is available about treatment and prognosis of patients with kidney failure. Notwithstanding, an early recognition of these diseases is important to start early the treatment and to establish the prognosis. In this descriptive review, we will consider the available data on cases of acute kidney injury (AKI) and chronic kidney disease (CKD) in sarcoidosis, requiring renal replacement therapy (RRT).
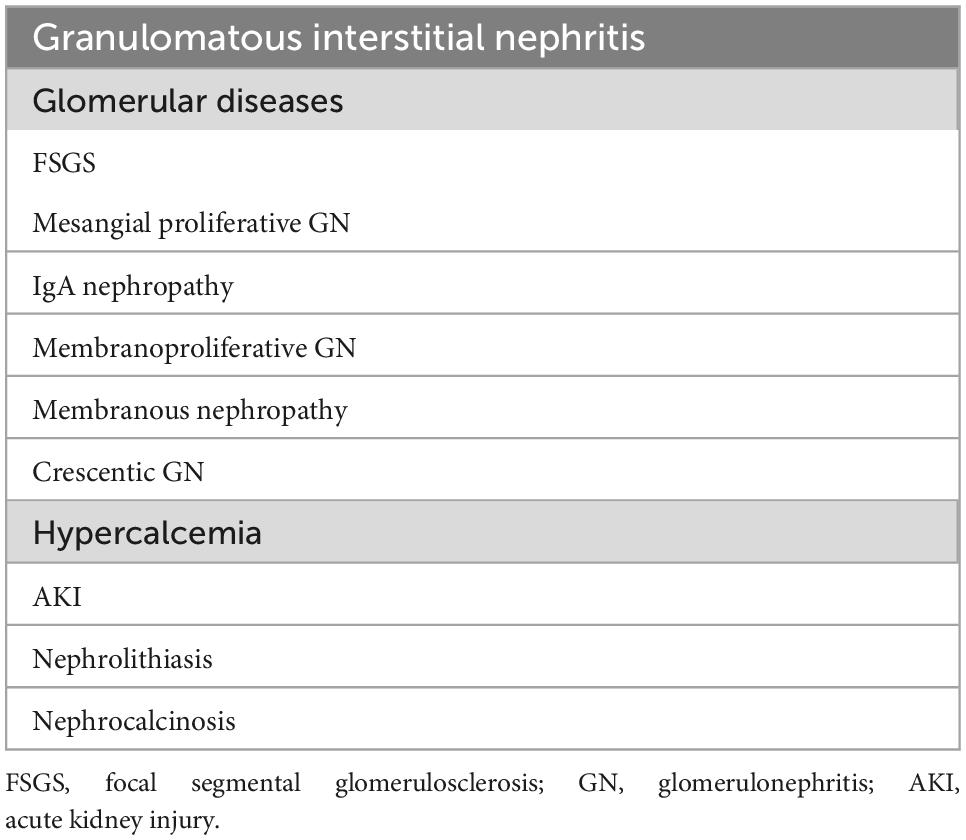
Table 1. Main renal diseases reported in patients with sarcoidosis.
We conducted a literature search from ’70s to May 2022 in PubMed, Medline, and Embase, and from reference list of retrieved articles. During searching, we used these terms and keywords: renal sarcoidosis, acute kidney injury, chronic kidney disease, renal replacement therapy, granulomatous interstitial nephritis, hypercalcemia, nephrocalcinosis, and renal transplantation. Study quality and recommendations were assessed based on importance of the published studies.
Severe acute renal failure requiring dialysis may occur in sarcoidosis. It is mainly due to granulomatous interstitial nephritis, hypercalcemia, and/or hypergammaglobulinemia. Many patients with renal sarcoidosis are affected by non-caseating GIN, a disorder that responds to corticosteroids and immunosuppressive drugs. Clinically, GIN may be silent or may present with abnormal urine analysis such as microscopic hematuria, mild proteinuria or sterile leukocyturia sometimes associated with high serum creatinine levels and low glomerular filtration rate (GFR). GIN may also be severe and lead to AKI and requiring dialysis (16–23). In some cases, AKI is the first manifestation of sarcoidosis (24, 25). In a retrospective study on 12 cases of sarcoidosis complicated by AKI renal biopsies showed tubule-interstitial nephritis in all patients, with granuloma in six patients and giant cells in two cases. Five patients (40%) needed hemodialysis for severe renal impairment. All patients received prednisone 1 mg/kg/day with gradual improvement of renal function, normalization of serum creatinine levels and no renal recurrence of AKI after 5 years (16).
The differential diagnosis between AKI due to granulomatous interstitial nephritis or other diseases may be difficult without renal biopsy. Cases of AKI caused by IgA nephritis (26) or associated with elevated levels of anti-glomerular basement antibodies (27) in patients with sarcoidosis have been reported. In addition, cases of sarcoidosis with ANCA-positive crescentic glomerulonephritis have been described (28). Prompt diagnosis and treatment may result in partial or complete recovery but late diagnosis can result in irreversible kidney damage. Another cause of AKI is represented by hypercalcemia. It is defined by a total serum calcium concentration >10.4 mg/dl (>2.60 mmol/L) or ionized serum calcium >5.2 mg/dl (>1.30 mmol/L). Depending on the population studied, about 2–63% of sarcoidosis patients show hypercalcemia (29). Elevated levels of serum calcium are probably due to overproduction of activated polarized macrophages expressing very high levels of the 25(OH)D-1α-hydroxylase that convert 25(OH)D into 1,25(OH)2D3 (30). Mild hypercalcemia (<11.5 mg/dl) is often asymptomatic or may be associated with aspecific gastrointestinal troubles. An acute increase in serum calcium over 12 mg/dl (3.00 mmol/L) may lead to AKI through different mechanisms (i) hypercalcemia causes intracellular calcium overload and tubular obstruction by calcium precipitates (31, 32), (ii) hypercalcemia increases renal vascular resistance and reduces GFR (33), (iii) hypercalcemia induces renal resistance to vasopressin leading to polyuria, dehydration, and hypovolemia (34). Severe hypercalcemia (>14 up to 18 mg/dl) can cause neuromuscular symptoms, hyporeflexia, dehydration, confusion, and acute renal failure. A shortened QTc interval is shown on electrocardiogram and arrhythmias may occur. Acute hypercalcemia is a rare event in sarcoidosis, but several cases of hypercalcemia-related acute renal failure have been reported (35–41). In a few cases, the concomitance of hypercalcemia and acute renal failure may be caused by peritoneal sclerosis (42). Hypercalcemia is often asymptomatic and may remain undetected if it is not measured routinely. Hypercalciuria is even more frequent. It is often associated with interstitial inflammation and may predict a good response to immunosuppressive therapy (43). Treatment of hypercalcemia depends on the severity of the disorder. Mild hypercalcemia can be managed with corticosteroids, thiazide diuretics, hydroxychloroquine, or ketoconazole. In intermediate cases (serum calcium between 12 and 14 mg/dl) corticosteroids, bisphosphonates, or denosumab are indicated. Severe hypercalcemia is a life-threatening complication and needs an emergency treatment. The more effective and safest management consists in dialysis. If dialysis is not possible saline infusion, calcitonin and intravenous bisphosphonates, and denosumab are indicated. Some patients with sarcoidosis and myeloma may present AKI, associated with hypergammaglobulinemia, normal albuminemia and hypercalcemia. In these cases, the differential diagnosis between sarcoidosis and multiple myeloma may be difficult (44, 45). Bone marrow biopsy, showing non-caseating granulomas or prompt improvement of hypercalcemia and kidney function after corticosteroid administration may lead to a correct diagnosis (46).
Granulomatous interstitial nephritis is often clinically silent and but may be complicated and lead to end stage kidney disease (ESKD) if not diagnosed or detected too late. Sarcoidosis-associated glomerular diseases, including focal and segmental glomerulosclerosis (47), IgA nephropathy (48), and membranous nephropathy (49) may also progress to ESKD. In a retrospective study of 2009, The French Sarcoidosis Group described 47 adults with renal sarcoidosis and reported that more than 60% of them had a GFR <60 ml/min per 1.73 m2 and two patients needed hemodialysis after a median follow-up of 24 months (50). In that study the long-term renal function was inversely related to the initial fibrosis score at kidney biopsy and patients with an extensive interstitial fibrosis were unresponsive to treatment. Similar results have been found by Rajakariar et al. (51) and by Berliner et al. (52). In the past, the most frequent cause of CKD in sarcoidosis was nephrocalcinosis, a disorder characterized by the deposition of calcium salts in the kidney parenchyma and tubules, that may lead silently to ESKD (53–56). More recently, a systematic renal screening in sarcoidosis, including instrumental diagnosis with abdominal x ray, ultrasonography and/or computed tomography, allowed to detect and manage silent stones and calcium deposits in the kidney and to prevent their progression to ESKD. However, a small number of patients with long-term asymptomatic hypercalcemia and hypercalciuria may still develop nephrocalcinosis and require RRT (57–59). In many instances, patients needing regular dialysis for unknown causes develop asymptomatic or oligosymptomatic hypercalcemia which reveal the presence of an underlying sarcoidosis (60, 61). Both periodic hemodialysis and continuous ambulatory peritoneal dialysis have been successfully used in patients with uremic sarcoidosis. However, peritoneal dialysis can be ineffective in patients with peritoneal sarcoidosis, a possible, although unusual, presentation of the disease (62–64). A main issue in sarcoidotic patients on regular dialysis is represented by hypercalcemia. In uremic patients, there is usually hyperphosphatemia, hypocalcemia, and the poor kidney conversion from 25(OH) to the active 1,25(OH)2D3. These abnormalities stimulate an excessive production of parathyroid hormone (PTH) leading to secondary hyperparathyroidism and progressive development of uremic osteodystrophy, characterized by osteitis fibrosa, and a high turnover bone disease (65). A decreased expression in α-Klotho, a transmembrane protein expressed in the kidney that serves as a co-receptor for fibroblast growth factor 23 (FGF-23) (66), and a corresponding increase in FGF-23, a bone hormone that regulates phosphate homeostasis in the kidney along with active vitamin D and parathyroid hormone (67) concur to the production of secondary hyperparathyroidism (68) and hypercalcemia (69). The large use of pharmacological therapies, such as calcimimetics and antiresorptive agents, can inhibit the production of parathyroid hormone. However, these medications, together with inflammation, oxidative stress, and malnutrition, may also produce an excessive suppression of parathyroid hormone eventually leading to an adynamic bone disease, which is now the most predominant form of uremic osteodystrophy (70). In adynamic bone disease there is a reduced bone turnover, which limits the capacity of bone to release or store calcium, resulting in normo-, hypo- or hyper-calcemia (71). Thus, in dialysis patients with sarcoidosis hypercalcemia can result from many possible sources, including the underlying disease, an autonomous secondary hyperparathyroidism, an adynamic bone disease, an inappropriate use of medications such as calcium carbonate, vitamin D and derivate, or the use of high dialysate calcium concentrations (72–75). Other rare causes of hypercalcemia should also be considered, such as immobilization (76), adrenal insufficiency (77, 78), tuberculosis (79) and malignancy (80, 81). The fact that hypercalcemia may occur in anephric patients, demonstrates that calcitriol may be generated by extra-renal sources (82, 83). The development of hypercalcemia is often enhanced by the administration of vitamin D3. Some nephrologists feel that measurement of 25-OH vitamin D is sufficient to assess the deficit of Vitamin D. In sarcoidosis serum levels of 25-OH vitamin D are often low. This finding may encourage the clinician to prescribe vitamin D supplementation. However, this apparent hypovitaminosis is the result of an overproduction of 1α-hydroxylase that converts 25(OH) to the active 1,25(OH)2D3. Supplementation of vitamin D may aggravate hypercalcemia in these cases (84, 85). Although the most used test to measure vitamin D is based on 25-OH vitamin D, in dialysis patients we recommend to measure 1-25(OH)2 vitamin D3 to prevent iatrogenic toxicity. In a series of 101 cases of calcitriol-mediated hypercalcemia, sarcoidosis represented the most common etiology, being involved in 49% of cases (86). Whatever the cause, chronic hypercalcemia may lead to vascular calcifications which are associated with an increased risk of cardiovascular disease and mortality (87). Identifying the causes of hypercalcemia in sarcoidosis patient on dialysis is critical. In difficult cases, bone biopsy can provide important information. It may indicate or rule out the presence and severity of osteitis fibrosa, osteomalacia, malignancy, or chronic infection. Histomorphometric analysis can evaluate the bone and trabecular volumes, the ratio osteoid surface per bone surface volume and fibrous volume giving information on the presence of high turnover bone disease or adynamic kidney disease.
There is little information about the results of kidney transplantation in patients with sarcoidosis. From a theoretical point of view, sarcoidosis patents with ESKD should be considered good candidates to a successful kidney transplantation. Indeed, many patients are young or middle-aged adults and in advanced renal sarcoidosis, corticosteroids and other immunomodulatory treatments may attenuate disease activity. Good outcome was reported by single centers. Sarcoidosis recurred in some patients (88, 89). However, it is difficult to assess the risk of recurrence since the follow-up was too short (90–95). A few cases of de novo sarcoidosis developing after kidney transplantation have been described (96, 97). In a multicenter French study of 2010, 18 patients with sarcoidosis who underwent renal transplantation were reported. After a median follow-up of 42 months, patient and death-censored graft survival were 94.4% and the mean GFR was 60 ml/min per 1.73 m2. Recurrence of sarcoidosis occurred in 5 patients (27.5%) in median after 13 months; extra-renal involvement occurred in two patients and renal involvement in three patients (16,5%) leading to impairment of graft function. When the period between the last episode of sarcoidosis and renal transplantation was short, recurrence was more frequent (98). In summary, the available data indicate that survival and complication rates of kidney transplant in sarcoidosis are similar to those of patients undergoing transplantation for other indications. Immunosuppressive therapy including corticosteroids could control hypercalcemia. However, renal or extra renal recurrences of sarcoidosis are frequent and little information is available about the long-term results. With these limitations, kidney transplantation can be considered an acceptable treatment for sarcoidosis patients with ESKD.
Kidney involvement in sarcoidosis is often clinically silent but may be severe if not diagnosed or detected too late. In this descriptive review, we have reported the main case reports and retrospective studies available in literature about RRT in patients affected by renal sarcoidosis. Dialysis may be required in sarcoidosis for acute and chronic disease and both hemodialysis and peritoneal dialysis can be used, although a peritoneal sarcoidosis could be the clinical presentation of the disease and the cause of ineffective peritoneal dialysis. Based on literature data, kidney transplantation is also an accepted treatment for uremic sarcoidosis patients and complication rates of kidney transplant seem to be similar to those of patients undergoing transplantation for other indications. An early recognition of kidney diseases in sarcoidosis is crucial to reduce the risk of complications, the progression of kidney disease and to establish the prognosis.
A systematic screening of renal function including serum creatinine, urine analysis, and serum calcium levels should be part of diagnostic test in sarcoidosis patients to detect early kidney involvement and start treatment. Further larger studies are needed to confirm these clinical results and to better investigate treatment and prognosis of patients with renal sarcoidosis.
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Brito-Zerón P, Sellarés J, Bosch X, Hernández F, Kostov B, Sisó-Almirall A. Epidemiologic patterns of disease expression in sarcoidosis: age, gender and ethnicity-related differences. Clin Exp Rheumatol. (2016) 34:380–8.
2. Larsson J, Graff P, Bryngelsson I, Vihlborg P. Sarcoidosis and increased risk of comorbidities and mortality in Sweden. Sarcoidosis Vasc Diffuse Lung Dis. (2020) 37:104–35.
3. Hena K. Sarcoidosis epidemiology: race matters. Front Immunol. (2020) 11:537382. doi: 10.3389/fimmu.2020.537382
4. Sikjær M, Hilberg O, Ibsen R, Løkke A. Sarcoidosis: a nationwide registry-based study of incidence, prevalence and diagnostic work-up. Respir Med. (2021) 187:106548. doi: 10.1016/j.rmed.2021.106548
5. Arkema EV, Cozier Y. Sarcoidosis epidemiology: recent estimates of incidence, prevalence and risk factors. Curr Opin Pulm Med. (2020) 26:527–34. doi: 10.1097/MCP.0000000000000715
6. Yoon H, Kim H, Kim Y, Song J. Prevalence and incidence of sarcoidosis in Korea: a nationwide population-based study. Respir Res. (2018) 19:158. doi: 10.1186/s12931-018-0871-3
7. Pietinalho A, Hiraga Y, Hosoda Y, Löfroos A, Yamaguchi M, Selroos O. The frequency of sarcoidosis in Finland and Hokkaido, Japan. A comparative epidemiological study. Sarcoidosis. (1995) 12:61–7.
8. Crouser E, Maier L, Wilson K, Bonham C, Morgenthau A, Patterson K, et al. Diagnosis and detection of sarcoidosis. An official american thoracic society clinical practice guideline. Am J Respir Crit Care Med. (2020) 201:e26–51. doi: 10.1164/rccm.202002-0251ST
9. Gbd Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. (2020) 8:585–96.
10. Belperio J, Shaikh F, Abtin F, Fishbein M, Weigt S, Saggar R, et al. Diagnosis and treatment of pulmonary sarcoidosis: a review. JAMA. (2022) 327:856–67. doi: 10.1001/jama.2022.1570
11. Bergner R, Löffler C. Renal sarcoidosis: approach to diagnosis and management. Curr Opin Pulm Med. (2018) 24:513–20. doi: 10.1097/MCP.0000000000000504
12. Gorsane I, Zammouri A, Hajji M, Sallemi N, Aoudia R, Barbouch S, et al. [Renal involvement in sarcoidosis: prognostic and predictive factors]. Nephrol Ther. (2022) 18:52–8. doi: 10.1016/j.nephro.2021.08.001
13. Stehlé T, Joly D, Vanhille P, Boffa J, Rémy P, Mesnard L, et al. Clinicopathological study of glomerular diseases associated with sarcoidosis: a multicenter study. Orphanet J Rare Dis. (2013) 8:65. doi: 10.1186/1750-1172-8-65
14. Löffler C, Löffler U, Tuleweit A, Waldherr R, Uppenkamp M, Bergner R. Renal sarcoidosis: epidemiological and follow-up data in a cohort of 27 patients. Sarcoidosis Vasc Diffuse Lung Dis. (2015) 31:306–15.
15. Calatroni M, Moroni G, Reggiani F, Ponticelli C. Renal sarcoidosis. J Nephrol. (2022). [Online ahead of print]. doi: 10.1007/s40620-022-01369-y
16. Mahfoudhi M, Mamlouk H, Turki S, Kheder A. Systemic sarcoidosis complicated of acute renal failure: about 12 cases. Pan Afr Med J. (2015) 22:75. doi: 10.11604/pamj.2015.22.75.6237
17. Agrawal V, Crisi G, D’Agati V, Freda B. Renal sarcoidosis presenting as acute kidney injury with granulomatous interstitial nephritis and vasculitis. Am J Kidney Dis. (2012) 59:303–8. doi: 10.1053/j.ajkd.2011.09.025
18. El-Reshaid K, Al-Khaldi E, Madda J. Granulomatous interstitial nephritis and acute renal failure due to renal-limited sarcoidosis. Saudi J Kidney Dis Transpl. (2000) 11:48–52.
19. Ikeda S, Hoshino T, Nakamura T. A case of sarcoidosis with severe acute renal failure requiring dialysis. Clin Nephrol. (2014) 82:273–7. doi: 10.5414/CN107717
20. Kikuchi H, Mori T, Rai T, Uchida S. Acute kidney injury caused by sarcoid granulomatous interstitial nephritis without extrarenal manifestations. CEN Case Rep. (2015) 4:212–7. doi: 10.1007/s13730-015-0171-4
21. Harzallah A, Kaaroud H, Boubaker K, Barbouch S, Goucha R, Ben Hamida F. Acute kidney injury with granulomatous interstitial nephritis and vasculitis revealing sarcoidosis. Saudi J Kidney Dis Transpl. (2017) 28:1157–61. doi: 10.4103/1319-2442.215120
22. Horino T, Matsumoto T, Inoue K, Ichii O, Terada Y. A case of acute kidney injury caused by granulomatous interstitial nephritis associated with sarcoidosis. CEN Case Rep. (2018) 7:34–8. doi: 10.1007/s13730-017-0287-9
23. Sadek B, Sqalli Z, Al Hamany Z, Benamar L, Bayahia R, Ouzeddoun N. [Renal failure in sarcoidosis]. Rev Pneumol Clin. (2011) 67:342–6. doi: 10.1016/j.pneumo.2011.01.004
24. Rema J, Carvalho M, Vaz R, Fonseca M, Sampaio S, Praça A, et al. Acute renal failure as a form of presentation of sarcoidosis in a young adult: a case report. J Med Case Rep. (2014) 8:274. doi: 10.1186/1752-1947-8-274
25. Rajkumar T, Lea-Henry T, Chacko B. Acute kidney injury as the presenting manifestation of sarcoidosis: a case series and review of literature. Nephrology (Carlton). (2018) 23:597–600. doi: 10.1111/nep.13176
26. Akbari R, Shahani M, Ranae M. Acute renal failure due to IgA nephropathy in sarcoidosis. Iran J Kidney Dis. (2019) 13:340–2.
27. Yoshinori K, Arata A, Osamu H, Kensuke J. A case of acute kidney injury caused by granulomatous tubulointerstitial nephritis associated with sarcoidosis and concomitant presence of anti-glomerular basement membrane antibody. Sarcoidosis Vasc Diffuse Lung Dis. (2016) 32:368–71.
28. Auinger M, Irsigler K, Breiteneder S, Ulrich W. Normocalcaemic hepatorenal sarcoidosis with crescentic glomerulonephritis. Nephrol Dial Transplant. (1997) 12:1474–7. doi: 10.1093/ndt/12.7.1474
29. Ackermann D. [Hypercalcemia in sarcoidosis–case report, prevalence, pathophysiology and therapeutic options]. Therap Umschau Rev Ther. (2007) 64:281–6. doi: 10.1024/0040-5930.64.5.281
30. Lopez D, Al-Jaberi F, Woetmann A, Ødum N, Bonefeld C, Kongsbak-Wismann M, et al. Macrophages control the bioavailability of vitamin D and vitamin D-regulated T cell responses. Front Immunol. (2021) 12:722806. doi: 10.3389/fimmu.2021.722806
31. Hilderson I, van Laecke S, Wauters A, Donck J. Treatment of renal sarcoidosis: is there a guideline? Overview of the different treatment options. Nephrol Dial Transplant. (2014) 29:1841–7. doi: 10.1093/ndt/gft442
32. Manjunath V, Moeckel G, Dahl N. Acute kidney injury in a patient with sarcoidosis: hypercalciuria and hypercalcemia leading to calcium phosphate deposition. Clin Nephrol. (2013) 80:151–5. doi: 10.5414/cn107258
33. Hamdy N, Kanis J. Hypo-hypercalcemia. 3rd ed. In: Oxford Textbook of Clinical Nephrology. Oxford: Oxford University Press (2005). p. 269–86.
35. Ohashi N, Yonemura K, Hirano M, Takahashi S, Kato A, Fujigaki Y, et al. A patient with sarcoidosis presenting with acute renal failure: implication for granulomatous interstitial nephritis and hypercalcemia. Intern Med. (2002) 41:1171–4. doi: 10.2169/internalmedicine.41.1171
36. Moysés-Neto M, Guimarães F, Ayoub F, Vieira-Neto O, Costa J, Dantas M. Acute renal failure and hypercalcemia. Ren Fail. (2006) 28:153–9. doi: 10.1080/08860220500531005
37. Karnchanasorn R, Sarikonda M, Aldasouqi S, Gossain VV. Severe hypercalcemia and acute renal failure: an unusual presentation of sarcoidosis. Case Rep Med. (2010) 2010:423659. doi: 10.1155/2010/423659
38. Deepa A, Padegal V, Chandra K, Santhosh H. Gastric and pulmonary sarcoidosis complicated by hypercalcemia and acute renal failure: case report and literature review. Lung India. (2017) 34:380–2. doi: 10.4103/lungindia.lungindia_276_15
39. Volpicelli G, Mussa A, Frascisco M. A case of severe hypercalcemia with acute renal failure in sarcoidosis: a diagnostic challenge for the emergency department. Eur J Emerg Med. (2005) 12:320–1. doi: 10.1097/00063110-200512000-00015
40. O’Riordan K, Mohyuddin T, Moloney M. Unusual presentation of sarcoidosis, requiring a positron emission tomography/CT (PET/CT) for diagnosis. BMJ Case Rep. (2021) 14:e237424. doi: 10.1136/bcr-2020-237424
41. Rahimi C, Stroemel M, Andeen NK. AKI and hypercalcemia in a patient with weakness and fatigue. Kidney360. (2020) 1:1328–9. doi: 10.34067/KID.0002282020
42. Bachmeyer C, Belaube N, Loi V, Wendum D, Gauthé M, Haymann J. Hypercalcemia and acute renal failure indicating peritoneal sarcoidosis. Am J Med. (2021) 134:e571–2. doi: 10.1016/j.amjmed.2021.06.023
43. Zhao, T, Yu X, Wang S, Yang L, Su T. Hypercalciuria may predict better response to immunosuppressive therapy in renal sarcoidosis: a case series. J Nephrol. (2022). doi: 10.1007/s40620-022-01360-7 [Epub ahead of print].
44. Tiago Serra J, Martinho A, Paixao Duarte F, Aldomiro F. Sarcoidosis and multiple myeloma: a case report and literature review. Case Rep Hematol. (2019) 2019:4586265. doi: 10.1155/2019/4586265
45. Learned B, Nasiri-Ahad W, Davis J, Desai A, Chang A. Rare association between sarcoidosis and smoldering multiple myeloma: a case report. Cancer Invest. (2021) 39:880–4. doi: 10.1080/07357907.2021.1988633
46. El-Husseini A, Sabucedo A, Lamarche J, Courville C, Peguero A. Atypical sarcoidosis diagnosed by bone marrow biopsy during renal workup for possible multiple myeloma. CEN Case Rep. (2013) 2:102–6. doi: 10.1007/s13730-012-0052-z
47. Altiparmak M, Oygar D, Bilir M, Kiliçarslan I, Serdengeçti K. A rare cause of focal segmental glomerulosclerosis: sarcoidosis. Nephron. (2002) 90:211–2. doi: 10.1159/000049044
48. Kahn A, Hodges N, Lord M. A case of sarcoidosis in a patient with IgA nephropathy. MedGenMed. (2005) 7:7.
49. Stehlé T, Audard V, Ronco P, Debiec H. Phospholipase A2 receptor and sarcoidosis-associated membranous nephropathy. Nephrol Dial Transplant. (2015) 30:1047–50. doi: 10.1093/ndt/gfv080
50. Mahévas M, Lescure F, Boffa J, Delastour V, Belenfant X, Chapelon C, et al. Renal sarcoidosis: clinical, laboratory, and histologic presentation and outcome in 47 patients. Medicine. (2009) 88:98–106. doi: 10.1097/MD.0b013e31819de50f
51. Rajakariar R, Sharples E, Raftery M, Sheaff M, Yaqoob M. Sarcoid tubulo-interstitial nephritis: long-term outcome and response to corticosteroid therapy. Kidney Int. (2006) 70:165–9. doi: 10.1038/sj.ki.5001512
52. Berliner A, Haas M, Choi M. Sarcoidosis: the nephrologist’s perspective. Am J Kidney Dis. (2006) 48:856–70. doi: 10.1053/j.ajkd.2006.07.022
53. Bossuyt A, Verbeelen D, Jonckheer M, Six R. Usefulness of 99mTc-methylene diphosphonate scintigraphy in nephrocalcinosis. Clin Nucl Med. (1979) 4:333–4. doi: 10.1097/00003072-197908000-00005
54. Muther R, McCarron D, Bennett W. Renal manifestations of sarcoidosis. Arch Intern Med. (1981) 141:643–5. doi: 10.1001/archinte.141.5.643
55. Nocton J, Stork J, Jacobs G, Newman A. Sarcoidosis associated with nephrocalcinosis in young children. J Pediatr. (1992) 121:937–40. doi: 10.1016/S0022-3476(05)80347-6
56. Wachtell K, Molzen A, Hansen F. [Nephrocalcinosis and urolithiasis as primary symptoms in Boeck’s sarcoidosis]. Ugeskr Laeger. (1996) 158:1685–6.
57. Demetriou E, Pietras S, Holick M. Hypercalcemia and soft tissue calcification owing to sarcoidosis: the sunlight-cola connection. J Bone Miner Res. (2010) 25:1695–9. doi: 10.1002/jbmr.51
58. Chrysaidou K, Sargiotis G, Karava V, Liasis D, Gourvas V, Moutsanas V, et al. Subcutaneous fat necrosis and hypercalcemia with nephrocalcinosis in infancy: case report and review of the literature. Children (Basel). (2021) 8:374. doi: 10.3390/children8050374
59. Shavit L, Jaeger P, Unwin R. What is nephrocalcinosis? Kidney Int. (2015) 88:35–43. doi: 10.1038/ki.2015.76
60. Kwon A, Koh E, Chung S, Kim Y. Sarcoidosis as a cause of unappreciated hypercalcaemia in a patient with end-stage renal disease on peritoneal dialysis. BMJ Case Rep. (2013) 2013:bcr2013010017. doi: 10.1136/bcr-2013-010017
61. Huart A, Kamar N, Lanau J, Dahmani A, Durand D, Rostaing L. Sarcoidosis-related hypercalcemia in 3 chronic hemodialysis patients. Clin Nephrol. (2006) 65:449–52. doi: 10.5414/cnp65449
62. Uthman I, Bizri A, Khalifeh M. Peritoneal sarcoidosis. Semin Arthritis Rheum. (2002) 31:353. doi: 10.1053/sarh.2002.32548
63. Lee S, Lee M, Lee J, Choi S, Yi B, Jung J. Peritoneal sarcoidosis: a case report. Medicine. (2019) 98:e16001. doi: 10.1097/MD.0000000000016001
64. Panaccio P, Bellobono M, Esposito L, Ricciardiello M, Cinalli S, Cotellese R. Peritoneal sarcoidosis mimicking peritoneal carcinomatosis. Ann Ital Chir. (2019) 8:S2239253X19029803.
65. Komaba H, Ketteler M, Cunningham J, Fukagawa M. Old and new drugs for the management of bone disorders in CKD. Calcif Tissue Int. (2021) 108:486–95. doi: 10.1007/s00223-020-00788-y
66. Neyra J, Hu M, Moe O. Klotho in clinical nephrology: diagnostic and therapeutic implications. Clin J Am Soc Nephrol. (2020) 16:162–76. doi: 10.2215/CJN.02840320
67. Rausch S, Föller M. The regulation of FGF23 under physiological and pathophysiological conditions. Pflugers Archiv Eur J Physiol. (2022) 474:281–92.
69. Iwazu Y, Kuro-O M, Miura Y, Takeda S, Yamada T, Nagata D. Calciprotein particles and fibroblast growth factor 23 contribute to the pathophysiology of hypercalcemia in a patient with renal sarcoidosis. Clin Kidney J. (2021) 14:421–3. doi: 10.1093/ckj/sfz086
70. Haarhaus M, Evenepoel P, European Renal Osteodystrophy (EUROD) Workgroup, Chronic Kidney Disease Mineral and Bone Disorder (CKD-MBD) Working Group of the European Renal Association–European Dialysis and Transplant Association [ERA-EDTA]. Differentiating the causes of adynamic bone in advanced chronic kidney disease informs osteoporosis treatment. Kidney Int. (2021) 100:546–58. doi: 10.1016/j.kint.2021.04.043
71. Peugh J, Khalil A, Chan M, Hansen K. Teriparatide treatment for hypercalcemia associated with adynamic bone disease. JBMR Plus. (2019) 3:e10176. doi: 10.1002/jbm4.10176
72. Wei Y, Kong X, Li W, Wang Z. Effect of calcium carbonate combined with calcitonin on hypercalcemia in hemodialysis patients. Ther Apher Dial. (2014) 18:618–22. doi: 10.1111/1744-9987.12178
73. Malihi Z, Wu Z, Lawes C, Scragg R. Adverse events from large dose vitamin D supplementation taken for one year or longer. J Steroid Biochem Mol Biol. (2019) 188:29–37. doi: 10.1016/j.jsbmb.2018.12.002
74. Kilpatrick R, Danese M, Belozeroff V, Smirnakis K, Goodman W, Rothman K. The association of vitamin D use with hypercalcemia and hyperphosphatemia in hemodialysis patients: a case-crossover study. Pharmacoepidemiol Drug Saf. (2011) 20:914–21. doi: 10.1002/pds.2183
75. Janssen M, van der Kuy A, ter Wee P, van Boven W. Aluminum hydroxide, calcium carbonate and calcium acetate in chronic intermittent hemodialysis patients. Clin Nephrol. (1996) 45:111–9.
76. Madureira R, Callas S, Caires R, Ferraz Crispilho S, Ayroza Galvão P, Moysés R. Continuous renal replacement therapy might mask immobilization-induced hypercalcemia in critically ill patients. Blood Purif. (2020) 49:129–31. doi: 10.1159/000502679
77. Sakao Y, Sugiura T, Tsuji T, Ohashi N, Yasuda H, Fujigaki Y, et al. Clinical manifestation of hypercalcemia caused by adrenal insufficiency in hemodialysis patients: a case-series study. Intern Med. (2014) 53:1485–90. doi: 10.2169/internalmedicine.53.1104
78. Oyama Y, Iwafuchi Y, Narita I. A case of hypercalcemia because of adrenal insufficiency induced by glucocorticoid withdrawal in a patient undergoing hemodialysis. CEN Case Rep. (2022) 11:73–8. doi: 10.1007/s13730-021-00619-5
79. Werion A, Ponlot E, Lhommel R, Komuta M, Coubeau L, Goffin E. An unusual cause of hypercalcaemia in a home haemodialysis patient: peritoneal tuberculosis. Int J Infect Dis. (2021) 104:222–3. doi: 10.1016/j.ijid.2020.12.053
80. Kundu S, Jha S, Rivera A, Flores Monar GV, Islam H, Puttagunta S, et al. Multiple myeloma and renal failure: mechanisms, diagnosis, and management. Cureus. (2022) 14:e22585. doi: 10.7759/cureus.22585
81. Hu M. Hypercalcemia of malignancy. Endocrinol Metab Clin North Am. (2021) 50:721–8. doi: 10.1016/j.ecl.2021.07.003
82. Barbour G, Coburn J, Slatopolsky E, Norman A, Horst R. Hypercalcemia in an anephric patient with sarcoidosis: evidence for extrarenal generation of 1,25-dihydroxyvitamin D. N Engl J Med. (1981) 305:440–3. doi: 10.1056/NEJM198108203050807
83. Kalantar-Zadeh K, Neumayer H, Wünsch P, Luft F. Hypercalcaemia and sarcoidosis in an anephric dialysis patient. Nephrol Dial Transplant. (1994) 9:829–31.
84. Sodhi A, Aldrich T. Vitamin D supplementation: not so simple in sarcoidosis. Am J Med Sci. (2016) 352:252–7. doi: 10.1016/j.amjms.2016.05.027
85. Thapa S, Sandhu J, Sah B. An uncommon cause of severe hypercalcemia: vitamin D supplementation in sarcoidosis. Am J Med. (2021) 134:e555–6. doi: 10.1016/j.amjmed.2021.04.037
86. Donovan P, Sundac L, Pretorius C, d’Emden M, McLeod D. Calcitriol-mediated hypercalcemia: causes and course in 101 patients. J Clin Endocrinol Metab. (2013) 98:4023–9. doi: 10.1210/jc.2013-2016
87. Podestà M, Cucchiari D, Ciceri P, Messa P, Torregrosa J, Cozzolino M. Cardiovascular calcifications in kidney transplant recipients. Nephrol Dial Transplant. (2021) 37:2063–71. doi: 10.1093/ndt/gfab053
88. Shen S, Hall-Craggs M, Posner J, Shabazz B. Recurrent sarcoid granulomatous nephritis and reactive tuberculin skin test in a renal transplant recipient. Am J Med. (1986) 80:699–702. doi: 10.1016/0002-9343(86)90828-4
89. Brown J, Jos V, Newstead C, Lawler W. Sarcoid-like granulomata in a renal transplant. Nephrol Dial Transplant. (1992) 7:173. doi: 10.1093/oxfordjournals.ndt.a092094
90. Hakaim A, Stilmant M, Kauffman J, Schmitt G, Joshi P, Carpinito G, et al. Successful renal transplantation in a patient with systemic sarcoidosis and renal failure due to focal glomerulosclerosis. Am J Kidney Dis. (1992) 19:493–5. doi: 10.1016/s0272-6386(12)80961-9
91. Schmidt R, Bender F, Chang W, Teba L. Sarcoidosis after renal transplantation. Transplantation. (1999) 68:1420–3.
92. Cochat P, Fargue S, Mestrallet G, Jungraithmayr T, Koch-Nogueira P, Ranchin B, et al. Disease recurrence in paediatric renal transplantation. Pediatr Nephrol. (2009) 24:2097–108. doi: 10.1007/s00467-009-1137-6
93. Mann D, Fyfe B, Osband A, Lebowitz J, Laskow D, Jones J, et al. Sarcoidosis within a renal allograft: a case report and review of the literature. Transplant Proc. (2013) 45:838–41. doi: 10.1016/j.transproceed.2012.11.008
94. Bagnasco S, Gottipati S, Kraus E, Alachkar N, Montgomery R, Racusen L, et al. Sarcoidosis in native and transplanted kidneys: incidence, pathologic findings, and clinical course. PLoS One. (2014) 9:e110778. doi: 10.1371/journal.pone.0110778
95. Kono M, Hasegawa J, Wakai S, Ishiwatari A, Abe Y, Endo M, et al. Living kidney donation from a donor with pulmonary sarcoidosis: a case report and review of the literature. Transplant Proc. (2017) 49:1183–6. doi: 10.1016/j.transproceed.2017.03.025
96. Shinzato T, Kubo T, Shimizu T, Nanmoku K, Yagisawa T. Sarcoidosis in the renal allograft of a recipient whose primary disease was autosomal dominant polycystic kidney disease. CEN Case Rep. (2019) 8:79–82. doi: 10.1007/s13730-018-0369-3
97. Kisner T, Pfister R, Engels M, Benzing T, Michels G. [De novo sarcoidosis after kidney transplantation]. Dtsch Med Wochenschr. (2012) 137:476–8. doi: 10.1055/s-0031-1298981
Keywords: end-stage kidney disease, renal replacement therapy, granulomatous interstitial nephritis, hypercalcemia, nephrocalcinosis, renal transplantation
Citation: Calatroni M, Moroni G and Ponticelli C (2023) Renal replacement therapy in sarcoidosis. Front. Med. 9:990252. doi: 10.3389/fmed.2022.990252
Received: 09 July 2022; Accepted: 16 December 2022;
Published: 09 January 2023.
Edited by:
Miriana d’Alessandro, University of Siena, ItalyReviewed by:
Laura Bergantini, University of Siena, ItalyCopyright © 2023 Calatroni, Moroni and Ponticelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marta Calatroni,  bWFydGEuY2FsYXRyb25pQGh1bmltZWQuZXU=
bWFydGEuY2FsYXRyb25pQGh1bmltZWQuZXU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.