 Jacqueline So
Jacqueline So Ann-Sophie De Craemer
Ann-Sophie De Craemer Dirk Elewaut
Dirk Elewaut Lai-Shan Tam
Lai-Shan Tam
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Med. , 08 September 2022
Sec. Rheumatology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.988532
This article is part of the Research Topic Precision Medicine in Spondyloarthritis: Reality or Utopia? View all 6 articles
Spondyloarthritis (SpA) is a family of heterogenous diseases consisting of different phenotypes. The exact disease mechanism remains unclear but evidence shows the complex pathophysiology with interplay between genome, microbiome, and immunome. Biologic DMARDs have markedly improved patients' disease control and quality of life. However, treatment response varies among patients. There is a growing need to identify biomarkers for the diagnosis, prognosis, prevention, and treatment of SpA. Genomic studies have been the research focus in the past two decades and have identified important genes involved in SpA. In recent years, emerging evidence supports the link between gut and joint inflammation in SpA, in which the role of gut microbiome in SpA is of great interest. Herein, potential genetic and gut microbial biomarkers for predicting treatment response are discussed. Novel strategies targeting dysbiosis in SpA are also summarized. These results represent a significant step toward precision medicine for patients with SpA.
Spondyloarthritis (SpA) is a group of seronegative inflammatory diseases characterized by spondylitis, peripheral arthritis and enthesitis. Axial spondyloarthritis (axSpA) is the prototypical form of SpA which includes non-radiographic axSpA and radiographic axSpA [also known as ankylosing spondylitis (AS)]. Other diseases in this family include psoriatic arthritis (PsA), reactive arthritis, enteropathic arthritis related to inflammatory bowel diseases (IBD) and undifferentiated SpA. Diseases in the SpA family share common clinical features including sacroiliitis, peripheral arthritis, enthesitis and dactylitis. Some patients may also have extra-musculoskeletal manifestations such as uveitis, IBD and psoriasis. Currently, the management of SpA is based on disease subtypes and manifestations. Non-steroidal anti-inflammatory drugs (NSAIDs) have been the mainstay of treatment for spondylitis for decades. However, the efficacy of NSAIDs in axSpA was suboptimal with 30–35% response rate only (1, 2). Majority of patients suffered from suboptimal disease control with persistent and debilitating back pain.
The introduction of biologic disease modifying anti-rheumatic drugs (DMARDs), which target inflammatory cytokines or their receptors, was a major medical breakthrough in the treatment of SpA. Biologic DMARDs including anti-tumor necrosis factor (TNF), anti-interleukin (IL) 17 and anti-IL23 and targeted synthetic DMARDs have significantly improved treatment outcomes and the quality of life of SpA patients (3–5). However, there is not one drug that fits all patients. The current approach in choosing among biologics is mainly based on disease subtypes and concurrent manifestations such as monoclonal anti-TNF, but not recombinant TNF receptor- Fc fusion protein etanercept, for patients with concomitant axSpA and uveitis and anti-IL17 or anti-IL23 for PsA patients with severe psoriasis (6, 7). Yet, clinical response to biologic DMARDs varies among patients. There is a substantial group of SpA patients who are poor responders or non-responders to biologic DMARDs (8). Also, clinical trials have showed that some biologics could be beneficial in one aspect of the disease while harmful or ineffective in another, for example, anti-IL17 might increase risk of exacerbation or even new onset of Crohn's disease and anti-IL23 is effective in treating PsA but not in axSpA (9, 10). These demonstrate the immunological heterogenicity in different disease subtypes. Many studies attempted to investigate the use of serum cytokines including IL-6, IL-17, IL-23, and TNF-α in predicting treatment response. However, the results were inconclusive (11). Twin studies showed that the concordance rates of AS in monozygotic and dizygotic twin were 50–75 and 20–27%, respectively (12, 13). This signifies that SpA is not entirely genetically determined, but is a result of the complex interplay of genetic and environmental factors (13) (Figure 1). With the medical advancement in SpA, are we ready to practice precision medicine according to molecular phenotyping such as genomics, metabolomics and microbiomics?
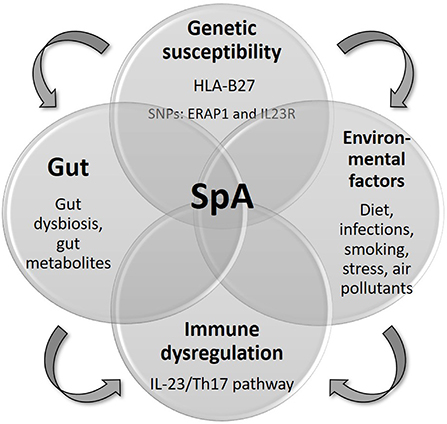
Figure 1. Pathogenesis of SpA.
Human Leukocyte Antigen (HLA)-B27 is a Class I Major Histocompatibility Complex (MHC) molecule that strongly increases genetic susceptibility to SpA and accounts for one-fifth of the AS heritability (14), and to a lesser extent PsA. The pathogenesis of SpA remains uncertain but there are several hypotheses of HLA-B27 related SpA pathogenesis. First, antigen peptide processing generates highly immunogenic peptide- MHC complexes that trigger T-cell immune response. Second, HLA-B27 free heavy chain homodimers may become targets for natural killer cells. Third, misfolding of HLA-B27 in the endoplasmic reticulum (ER) results in activation of an unfolded protein response and the production of IL-23(15, 16). The prevalence of HLA-B27 in axSpA patients varies among different ethnicities. Around 70–80% of Caucasian patients with axSpA are positive for HLA-B27 while HLA-B27 is only present in 20–60% of axSpA patients in Latin America, Middle East, and Japan (17–19). Animal model in the early 90s showed that HLA-B27/β2 microglobulin transgenic rats with high transgene copy numbers developed spontaneous spondyloarthritis-like phenotype while those with low transgene copy numbers remain healthy (20). This showed that the effect of one gene itself is not sufficient to cause SpA.
Genome-wide association studies (GWAS) have identified 113 single nucleotide polymorphism (SNP)s that contribute to disease susceptibility for AS including two major discoveries: Endoplasmic reticulum aminopeptidase 1 (ERAP1) variant and IL23-receptor (IL23R) (21, 22). ERAP1 encodes the aminopeptidase involved in trimming peptides to the optimal length in order to be presented on MHC Class I molecules in the ER, which is a key molecular mechanism involved in AS (23). In vivo, inhibition of ERAP1 also reduced the expansion of Th17 and production of IL-2 and IL-17A (24). However, further clinical studies are needed to prove the therapeutic role of ERAP1 inhibition in axSpA. Identification of IL-23R, a gene involved in the IL-23/Th17 axis, is another important finding in GWAS (23). IL-23 is a pro-inflammatory cytokine that drives the differentiation of Th17 lymphocytes, which in turns produce IL-17 and other proinflammatory cytokines involved in SpA. Animal studies showed that overexpression of IL-23 could induce SpA features (25). The important role of the IL-23/Th17 axis in SpA has been vastly supported by genetic studies, animal models, and therapeutic trials (26). Other overlapping genes involved in the IL-23/Th17 pathway for axSpA and PsA include IL-12B, STAT3, and CARD9.
Could genotyping guide therapeutic choices in SpA? A systematic review on genetic variants in relation to treatment response showed inconclusive results (27). Polymorphisms of the TNF receptor superfamily 1A and 1B (TNFRSF1A/1B) gene were most commonly investigated to predict treatment response of anti-TNF in SpA (Table 1). The study conducted by Seitz et al. showed that TNF-α−308 G/G genotype was associated with better response to anti-TNF compared to patients with A/A or A/G genotype in AS and PsA patients (28). Another study in Italy also found that TNFα−308 A allele and IL-6−174GG homozygosis were good predictors of drug-survival of the first anti-TNF in SpA (29). However, Murdaca et al. did not find a positive correlation between TNF-α−308 or−238 genotype and anti-TNF treatment response in PsA (33). Another two studies in AS did not confirm the association between TNF-α−308 or-238 and anti-TNF treatment response neither (30, 31). Whereas, a study of 106 AS patients in China found that TNF-α−857 C/C genotype and TNF-α−1031 T/T genotype were associated with better treatment response to anti-TNF therapy (30). TNFAIP3 polymorphism rs6920220 and rs610604 were associated with better quality of life after 3 months of anti-TNF use in PsA (32). SNP + 489 GG and GA genotype of the TNF-α gene may predict good treatment response to etanercept in PsA (33). Apart from TNF receptor family, V allele of the SNP rs396991 (V158F) in FCGR3A gene showed better response to infliximab (anti-TNF) at 6 months in axSpA (34). A recently published pilot study showed that 12 interferon regulated genes might predict magnetic resonance imaging (MRI) response to anti-TNF treatment in AS (35). There are studies that showed TNF polymorphisms may predict poor response to treatment too. Aita et al. showed that TNFRSF1A c.625 + 10A>G was associated with late response to infliximab in SpA (36) and TNFRSF1B polymorphism rs1061622 genotype was associated with non- response to a first-line anti-TNF treatment in AS (37).

Table 1. Studies on gene expression profiling for response prediction in SpA.
Currently, there is no conclusive evidence showing that TNF polymorphism or other SNPs could predict clinical response to anti-TNF in SpA. However, different populations with various genetic compositions and environmental exposure were involved in different studies which may account for the non-replicable results. With the emergence of more biologic and targeted synthetic DMARDs, more studies are required to explore potential pharmacogenomic markers to guide personalized treatment.
There is growing evidence supporting the pathogenic mechanism of the gut-joint axis in SpA (38). Mielants et al. performed ileocolonoscopic studies in patients with SpA in the 1980s and found that two-thirds of the patients with SpA had subclinical gut inflammation (39, 40). Clinical disease activity also correlated with the degree of gut inflammation (41). Those with chronic gut inflammation were also at higher risk of developing IBD (42). The GIANT (Ghent Inflammatory Arthritis and spoNdylitis cohort) confirmed these findings with nearly half of the patients with SpA showing subclinical gut inflammation; 6.5% of them developed clinically overt IBD over 5 years (43). The degree of bone marrow edema on sacroiliac joint MRI in patients with SpA also positively correlated with gut inflammation (44). These observations support the link between the gut and the joint in SpA.
Gut dysbiosis, an imbalance of microbiota, could increase gut permeability and trigger inflammatory responses, leading to auto-inflammatory diseases such as IBD and asthma (45, 46). Alterations in the gut microbiome are also observed in rheumatic diseases (47). HLA-B27 transgenic germ-free rats fail to develop arthritis and colitis (48). However, they develop disease phenotype after reintroduction of commensal bacteria (49). Also, SKG mice develop spondyloarthritis and colitis after intraperitoneal injection of curdlan (a major component of bacterial and fungal wall) (50). These animal findings underscore the importance of the gut microbiome and mycobiome in SpA. In humans, a recently published systemic review and meta-analysis showed a high inconsistency of the intestinal microbial composition in SpA reported in different studies (47). Costello et al. first identified a distinct microbial composition in the terminal ileum of AS patients, with an increased abundance of 5 families of bacteria (Lachnospiraceae, Ruminococcaceae, Rikenellacea, Porphyromonadaceae, and Bacteroidaceae) and a decreased abundance of 2 families of bacteria (Veillonellaceae and Prevotellaceae) (51). Later, Tito et al. found the abundance of genus Dialister in ileal biopsies correlated with Ankylosing Spondylitis Disease Activity Score (ASDAS) in SpA patients (52). Also, there was an increase in abundance of Ruminococcus gnavus (53) and a decreased abundance of anti-inflammatory F. prausnitzii A2-165 in fecal samples of SpA patients (54). Metagenomic sequencing of fecal samples of patients with AS in China showed an expansion of Prevotella melaninogenica, Prevotella copri, Prevotella sp. C561 and a relative reduction of Bacteroides spp, compared to healthy controls (55). Whereas, Manasson et al. showed an increased abundance of order Clostridiales and Erysioekotrichales and a decreased abundance of order Bacteroidales in fecal samples of PsA/SpA patients compared to healthy controls (56). The only study that specifically investigated gut microbiome in PsA showed a decreased abundance in Akkermansia, Ruminococcus, and Pseudobutyrivobrio in fecal samples of PsA patients, which resembles IBD dysbiosis (57).
Apart from bacterial microbiota, studies from IBD showed that fungal and viral microbiota are also important in regulating host immunity and maintaining gut homeostasis. A reduction of fungal diversity was observed in IBD patients (58). Also, the Ascomycota to Basidiomycota ratio was lowered in IBD patients compared to healthy individuals, with an expansion of Candida albicans and a reduction of Saccharomyces cerevisiae. Similarly, a pilot study showed distinct fecal mycobiota pattern in AS patients characterized by an increased abundance of Ascomycota (mainly the class of Dothideomycetes) and decreased abundance of Basidiomycota (mainly Agaricales) (59). Also, an increase abundanced of Saccharomyces in AS patients was associated with worse radiographic damage (59). In AS patients receiving biologic agents anti-TNF and anti-IL17 (56, 59), on top of bacterial dysbiosis, there were expansion of Saccharomyetales and C. albicans in post treatment fecal samples. Perturbation of gut virome was also observed in IBD patients. Studies showed an increased relative abundance of Caudovirales bacteriophages and Microviridae bacteriophages in fecal samples of IBD patients compared to healthy individuals (60). However, gut virome study in SpA is lacking. Future studies should comprehensively investigate the complex gut ecosystem including microbiome, mycobiome, and virome to improve our understanding of disease pathogenesis.
Perturbation in the gut microbial composition was observed in SpA. However, there is a great variability of microbiome profile between studies. This discrepancy could be related to different genetic backgrounds and environmental exposures. Also, sampling methods, DNA extraction protocol and analysis methods could affect the accuracy of the microbiome analysis. Confounding factors such as diet, antibiotic use and smoking should be taken into account in microbiome analysis. Further large- scale studies are needed to establish the SpA-specific, and ideally phenotype-specific, microbial communities. With the advance in sequence- based screening, metagenomic studies should be conducted which may provide the functional properties of SpA-specific microbes.
With the increasing association of gut dysbiosis and SpA, studies were also performed to identify potential microbial biomarkers to predict treatment response (Table 2). Manasson et al. investigated the change in gut microbiome in fecal samples of PsA/SpA patients after anti-TNF or anti-IL17 treatment, and found a distinctive microbial shift in patients receiving different treatments. The abundance of Clostridiales increased and Bacteroidales decreased after anti-TNF. In contrast, there was a significant reduction in abundance of Clostridiales and increased abundance of Bacteriodales after anti-IL17 (56). Perturbation in the fungal microbiota was also noted after anti-TNF and anti-IL-17 treatment, in particular an expansion of Candida and C. albicans after anti-IL17. Another pilot study of 20 AS patients also showed the dynamic variation of gut microbiome composition after anti-TNF treatment (61). There was an expansion in abundance of genus Collinsella, genus Dialister, genus Escherichina-Shigella, family Actinomycetaceae, family Coriobactereriaceae, family Prevotellaceae and a decrease in abundance of genus Bacteriodes, genus Parasutterella and family Burkholderiaceae and family Lachnospiraceae in AS fecal samples compared to healthy controls. The relative abundance of genus Escherichina-Shigella and Klebsiella positively correlated with Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) while the relative abundance of Lachnospiraceae negatively correlated with BASDAI. This dynamic change in gut microbial abundance in association with disease activity suggests the potential use of some microbes as indicators for disease activity. Another study of 18 SpA patients showed that higher proportions of Burkholderiales in fecal samples at baseline could predict clinical response to anti-TNF at 3 months (62). Whereas, higher proportion of genus Dialister and genus Salmonella in fecal samples of SpA patients after 3 months of anti-TNF distinguished between good and poor responder to anti-TNF respectively (62). However, these studies were limited by small sample size and the lack of healthy controls in the latter one. Chen et al. showed that 6-month use of adalimumab (anti-TNF) restored gut microbiome in AS patients (63). Also, high abundance of Comamonas in fecal samples might predict poor response to adalimumab (63). Future studies are required to confirm the specific bacteria and their mechanism involved which contribute to treatment success or failure in SpA. Larger, longitudinal studies should be performed in order to validate the potential microbial markers in predicting treatment response.
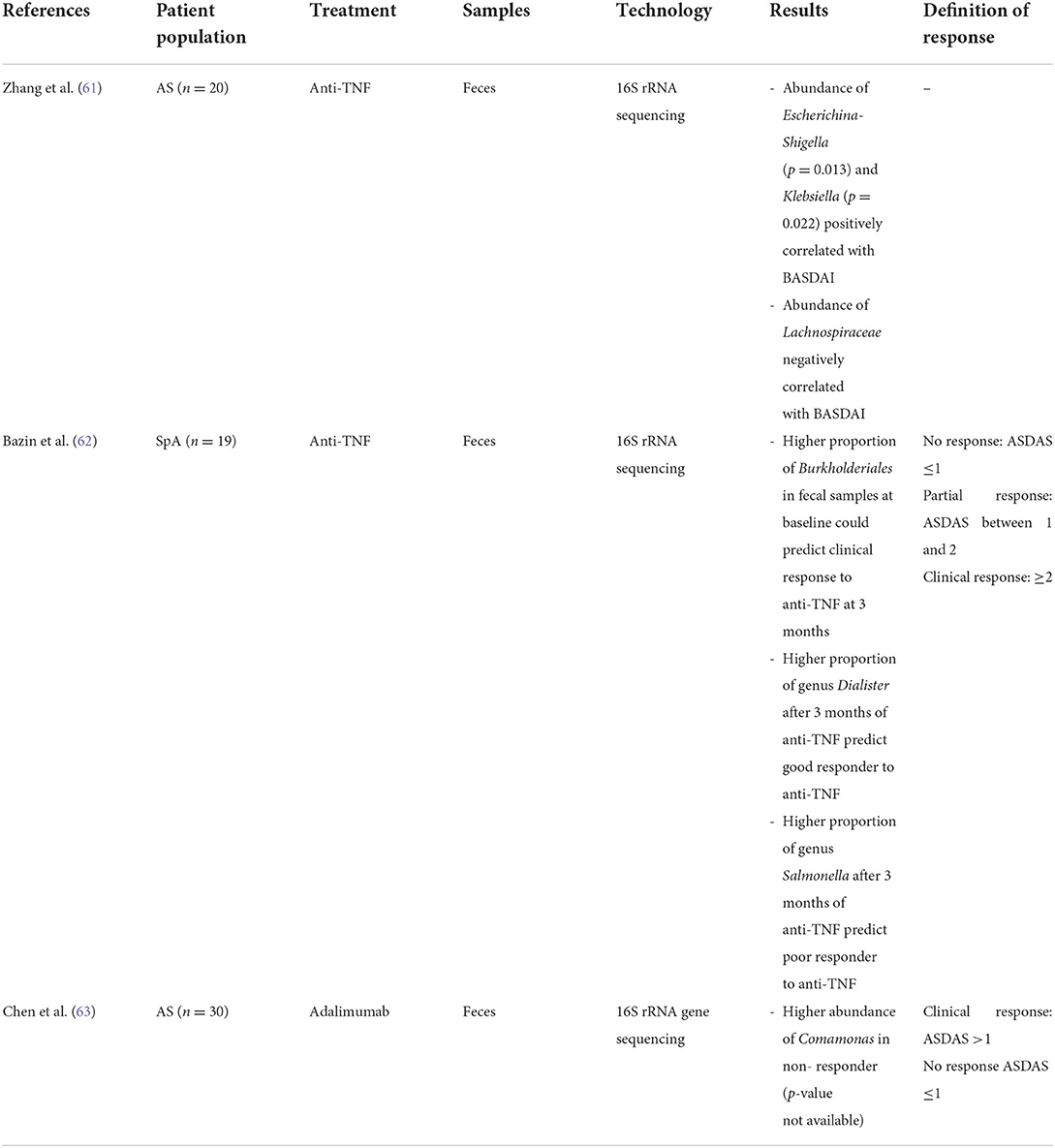
Table 2. Studies on gut microbial abundances between responders and non-responders in SpA.
There is a growing interest in modulation of the gut microbiome composition in SpA by prebiotics, probiotics, antibiotics, dietary modifications or fecal microbiota transplantation (FMT) in order to restore the normal gut microbiota. Prebiotics long-chain inulin and fructooligosaccharides both effectively ameliorated colitis in HLA-B27/β2 microglobulin transgenic rats (64, 65). Administration of probiotic and prebiotic mixture containing Lactobacillus acidophilus La-5, Bifidobactrium lactis Bb-12 and inulin to HLA-B27/β2 microglobulin transgenic rats also significantly increased gut microbial diversity, stimulated growth of Bifidobacterium animalis and attenuated colonic inflammation (66). However, there is no clinical trial of prebiotic use in SpA patients and the use of probiotics to modify dysbiosis in AS patients is so far discouraging. A pilot study using the combination of probiotics Lactobacillus Acdiophilus and Lactobacillus Salivarius in eighteen quiescent ulcerative colitis patients with active SpA showed improvement in disease activity (67). However, another study using specific probiotics composed of two Lactobacillus and two Bifidobacterium did not show improvement of disease activity or bowel symptoms in patients with SpA (68). A randomized controlled trial (RCT) comparing the use of probiotic combinations of Streptococcus salivarius, Bifidobacterium lactis LAFTI B94, and Lactobacillus acidophilus LAFTI L10 with placebo in active SpA patients again failed to show its efficacy (69). The results of probiotic use in PsA were conflicting too (70, 71). The use of the antibiotic rifaximin has been studied in proteoglycan-induced AS mice and showed promising results in reducing AS disease severity, inhibiting production of inflammatory cytokines, and promoting growth of beneficial intestinal bacteria in the gut (72). Yet, future clinical studies on the use of antibiotics in treating SpA patients are required. FMT is effective in treating Clostridium difficile infection and IBD by restoration of normal gut microbiome composition. A case report showed resolution of peripheral arthritis in a PsA patient after FMT for Clostridium difficile infection (73). However, a RCT (the FLORA study) showed that the use of FMT was inferior to sham in treating peripheral PsA (74).
Diets could alter gut microbiota composition. Protective effects of dietary patterns and supplements in SpA have been studied (75). Low starch diet has been proposed in AS patients as high dietary starch might promote the growth of Klebisella pneumoniae, which is possibly associated with the development of AS, in the bowel (75). A longitudinal study of 35 AS patients showed improvement in disease severity with low-starch diet (76). Also, diary-free diet was found to be effective in lowering disease activity and reducing use of NSAID in a pilot study of AS patients (77). However, systemic review concluded that there were insufficient evidence showing the beneficial effects of low starch and dairy-free diet in AS patients (78). Mediterranean diet has anti-inflammatory properties. Recently published observational study by Ometto et al. showed greater improvement in disease activity in axial SpA patients receiving Mediterranean diet nutritional advice (79). Another cross-sectional observational study of 211 PsA patients showed low adherence to Mediterranean diet was associated with higher PsA activity (80). Nonetheless, more studies are needed to conclude the beneficial impact of specific diet pattern in SpA patients. On the other hand, 1,25 dihydrovitamin D 1,25 (OH)2D is involved in regulating the production of pro-inflammatory cytokines. Meta-analysis showed that lower vitamin D level was associated with higher disease activity in AS (81). However, the beneficial effect of vitamin D supplementation in AS is lacking. Whereas, limited data support the use of vitamin D in decreasing disease activity in PsA (82). Fish oil supplement marine n-3 polyunsaturated fatty acids (PUFA) have anti-inflammatory effects and could improve arthritis. A RCT showed high dose PUFA significantly reduced the use of analgesics in PsA patients although there was no significant improvement in disease activity (83). Yet, current evidence is insufficient to draw a clear conclusion on the effectiveness of gut microbiome modulation in SpA given the knowledge gaps in microbiome of SpA. With the increase in understanding of dysbiosis in SpA, tailored intervention on gut microbiota may hopefully reshape gut microbiota and bring SpA into a cure.
Various gut microbial metabolites including short chain fatty acids (SCFAs), tryptophan and vitamin B derivates are important in maintaining gut barrier integrity and immune response in AS (84). SCFAs such as acetate, propionate and butyrate, are generated by the bacterial fermentation of dietary fibers. SCFAs promote regulatory T cell (Treg) differentiation which in turn suppresses Th17 cell differentiation and reduces production of pro-inflammatory cytokines (84). The association of altered gut microbiota and reduction in beneficial fatty acids is observed in some immune- mediated diseases such as IBD and asthma (85, 86). Notably, butyrate is crucial in maintaining gut permeability through upregulation of tight junction protein (84). Dysbiosis with lower butyrate-producing bacteria was observed in IBD patients (87, 88). Evidence showed that Faecalibacterium prausnitzii, a major butyrate producer in the gut, may affect SCFAs production (87). The fecal level of SCFAs including butyrate and proprionate were lower in AS patients (89). Reduction in fecal medium chain fatty acids was also observed in patients with PsA compared to healthy controls (57).
Animal models showed that modulation of SCFAs could suppress systemic inflammation. Administration of SCFAs and fiber-rich diets could suppress lymphocyte driven systemic inflammation and ameliorate inflammatory arthritis (90, 91). Administration of SCFA propionate to HLA-B27/β2 microglobulin - transgenic rats also significantly reduced colonic inflammation and expression of inflammatory cytokines (92). The use of indole-3-acetic acid (microbial tryptophan metabolite) in proteoglycan-induced AS mice also ameliorated disease severity, dampened inflammatory response and restored the balance of gut microbiome composition (93). However, translational research on gut metabolites modulation in human is still lacking.
There are some challenges in gut metabolites research. Similar to studies on gut microbiome, gut metabolites are heavily influenced by genetic and environmental factors. Dietary intake of carbon and fibers have a strong deterministic effect on gut metabolites. Also, there is an interplay between gut microbiome and gut metabolites. Fluctuation in disease activity may result in dynamic variation in gut microbiome and metabolites. Standardization of sample collection and preparation methods is another key obstacle which may hinder the research development in gut metabolites. Future studies are required to broaden our understanding of microbial community and microbial metabolic pathways in SpA.
SpA is a heterogenous group of diseases of overlapping phenotypes which involves the complex interplay between genetic and environmental factors. Genomic studies have increased our understanding on genetic predisposition in SpA. However, further research is required to translate these genomic findings into clinical practices for disease phenotyping and drug response prediction. Emerging evidence on gut-joint axis in SpA is promising and has shed new insights into the pathogenesis of SpA. Currently there is a huge knowledge gap regarding gut microbiomics and metabolomics in SpA. The development in this field is nascent but has been expanding rapidly. Future multi-omic studies may improve our understanding toward SpA and walk toward precision medicine by identifying new biomarkers and treatments.
JS: manuscript preparation. A-SD, DE, and L-ST: critical comments and manuscript revision. All authors contributed to this article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cinar M, Dinc A, Simsek I, Erdem H, Koc B, Pay S, et al. Evaluation of the short-term efficacy of NSAIDs on patients with active ankylosing spondylitis in daily practice: a 3-month, longitudinal, observational study. Rheumatol Int. (2010) 30:331–40. doi: 10.1007/s00296-009-0963-y
2. Baraliakos X, Kiltz U, Peters S, Appel H, Dybowski F, Igelmann M, et al. Efficiency of treatment with non-steroidal anti-inflammatory drugs according to current recommendations in patients with radiographic and non-radiographic axial spondyloarthritis. Rheumatology. (2017) 56:95–102. doi: 10.1093/rheumatology/kew367
3. Callhoff J, Sieper J, Weiss A, Zink A, Listing J. Efficacy of TNFalpha blockers in patients with ankylosing spondylitis and non-radiographic axial spondyloarthritis: a meta-analysis. Ann Rheum Dis. (2015) 74:1241–8. doi: 10.1136/annrheumdis-2014-205322
4. Mease P. Emerging immunomodulatory therapies and new treatment paradigms for axial spondyloarthritis. Curr Rheumatol Rep. (2019) 21:35. doi: 10.1007/s11926-019-0830-0
5. Liu W, Wu YH, Zhang L, Liu XY, Bin X, Bin L, et al. Efficacy and safety of TNF-α inhibitors for active ankylosing spondylitis patients: multiple treatment comparisons in a network meta-analysis. Sci Rep. (2016) 6:32768. doi: 10.1038/srep32768
6. Ward MM, Deodhar A, Gensler LS, Dubreuil M, Yu D, Khan MA, et al. 2019 Update of the American college of rheumatology/spondylitis association of America/spondyloarthritis research and treatment network recommendations for the treatment of ankylosing spondylitis and nonradiographic axial spondyloarthritis. Arthritis Care Res. (2019) 71:1285–99. doi: 10.1002/acr.24025
7. Gossec L, Baraliakos X, Kerschbaumer A, de Wit M, McInnes I, Dougados M, et al. Eular recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann Rheum Dis. (2020) 79:700–12. doi: 10.1136/annrheumdis-2020-217159corr1
8. Wang EA, Suzuki E, Maverakis E, Adamopoulos IE. Targeting IL-17 in psoriatic arthritis. Eur J Rheumatol. (2017) 4:272–7. doi: 10.5152/eurjrheum.2017.17037
9. Fauny M, Moulin D, D'Amico F, Netter P, Petitpain N, Arnone D, et al. Paradoxical gastrointestinal effects of interleukin-17 blockers. Ann Rheum Dis. (2020) 79:1132–8. doi: 10.1136/annrheumdis-2020-217927
10. Baeten D, Ostergaard M, Wei JC, Sieper J, Jarvinen P, Tam LS, et al. Risankizumab, an IL-23 inhibitor, for ankylosing spondylitis: results of a randomised, double-blind, placebo-controlled, proof-of-concept, dose-finding phase 2 study. Ann Rheum Dis. (2018) 77:1295–302. doi: 10.1136/annrheumdis-2018-213328
11. Lorenzin M, Ometto F, Ortolan A, Felicetti M, Favero M, Doria A, et al. An update on serum biomarkers to assess axial spondyloarthritis and to guide treatment decision. Ther Adv Musculoskelet Dis. (2020) 12:1759720X20934277. doi: 10.1177/1759720X20934277
12. Jarvinen P. Occurrence of ankylosing spondylitis in a nationwide series of twins. Arthritis Rheum. (1995) 38:381–3. doi: 10.1002/art.1780380313
13. Brown MA, Kennedy LG, MacGregor AJ, Darke C, Duncan E, Shatford JL, et al. Susceptibility to ankylosing spondylitis in twins: the role of genes, HLA, and the environment. Arthritis Rheum. (1997) 40:1823–8. doi: 10.1002/art.1780401015
14. International International Genetics of Ankylosing Spondylitis Consortium (IGAS), Cortes A, Hadler J, Pointon JP, Robinson PC, Karaderi T, et al. Identification of multiple risk variants for ankylosing spondylitis through high-density genotyping of immune-related loci. Nat Genet. (2013) 45:730–8. doi: 10.1038/ng.2667
15. Colbert RA, DeLay ML, Klenk EI, Layh-Schmitt G. From HLA-B27 to spondyloarthritis: a journey through the ER. Immunol Rev. (2010) 233:181–202. doi: 10.1111/j.0105-2896.2009.00865.x
16. Chen B, Li J, He C, Li D, Tong W, Zou Y, et al. Role of HLA-B27 in the pathogenesis of ankylosing spondylitis (Review). Mol Med Rep. (2017) 15:1943–51. doi: 10.3892/mmr.2017.6248
17. Ziade NR. HLA B27 antigen in Middle Eastern and Arab countries: systematic review of the strength of association with axial spondyloarthritis and methodological gaps. BMC Musculoskelet Disord. (2017) 18:280. doi: 10.1186/s12891-017-1639-5
18. Arevalo M, Gratacos Masmitja J, Moreno M, Calvet J, Orellana C, Ruiz D, et al. Influence of HLA-B27 on the ankylosing spondylitis phenotype: results from the regisponser database. Arthritis Res Ther. (2018) 20:221. doi: 10.1186/s13075-018-1724-7
19. Bakland G, Nossent HC, Gran JT. Incidence and prevalence of ankylosing spondylitis in Northern Norway. Arthritis Rheum. (2005) 53:850–5. doi: 10.1002/art.21577
20. Hammer RE, Maika SD, Richardson JA, Tang JP, Taurog JD. Spontaneous inflammatory disease in transgenic rats expressing HLA-B27 and human beta 2m: an animal model of HLA-B27-associated human disorders. Cell. (1990) 63:1099–112. doi: 10.1016/0092-8674(90)90512-D
21. Zhang Z, Dai D, Yu K, Yuan F, Jin J, Ding L, et al. Association of HLA-B27 and ERAP1 with ankylosing spondylitis susceptibility in Beijing Han Chinese. Tissue Antigens. (2014) 83:324–9. doi: 10.1111/tan.12334
22. Wellcome Trust Case Control, Australo-Anglo-American Spondylitis, Burton PR, Clayton DG, Cardon LR, Craddock N, et al. Association scan of 14,500 nonsynonymous SNPs in four diseases identifies autoimmunity variants. Nat Genet. (2007) 39:1329–37. doi: 10.1038/ng.2007.17
23. Costantino F, Breban M, Garchon HJ. Genetics and functional genomics of spondyloarthritis. Front Immunol. (2018) 9:2933. doi: 10.3389/fimmu.2018.02933
24. Chen L, Ridley A, Hammitzsch A, Al-Mossawi MH, Bunting H, Georgiadis D, et al. Silencing or inhibition of endoplasmic reticulum aminopeptidase 1 (ERAP1) suppresses free heavy chain expression and Th17 responses in ankylosing spondylitis. Ann Rheum Dis. (2016) 75:916–23. doi: 10.1136/annrheumdis-2014-206996
25. Sherlock JP, Joyce-Shaikh B, Turner SP, Chao CC, Sathe M, Grein J, et al. IL-23 induces spondyloarthropathy by acting on ROR-gammat+ CD3+CD4-CD8- entheseal resident T cells. Nat Med. (2012) 18:1069–76. doi: 10.1038/nm.2817
26. Smith JA, Colbert RA. Review: the interleukin-23/interleukin-17 axis in spondyloarthritis pathogenesis: Th17 and beyond. Arthritis Rheumatol. (2014) 66:231–41. doi: 10.1002/art.38291
27. Ortolan A, Cozzi G, Lorenzin M, Galozzi P, Doria A, Ramonda R. The genetic contribution to drug response in spondyloarthritis: a systematic literature review. Front Genet. (2021) 12:703911. doi: 10.3389/fgene.2021.703911
28. Seitz M, Wirthmuller U, Moller B, Villiger PM. The−308 tumour necrosis factor-alpha gene polymorphism predicts therapeutic response to TNFalpha-blockers in rheumatoid arthritis and spondyloarthritis patients. Rheumatology. (2007) 46:93–6. doi: 10.1093/rheumatology/kel175
29. Fabris M, Quartuccio L, Fabro C, Sacco S, Lombardi S, Ramonda R, et al. The−308 TNFalpha and the−174 IL-6 promoter polymorphisms associate with effective anti-TNFalpha treatment in seronegative spondyloarthritis. Pharmacogenomics J. (2016) 16:238–42. doi: 10.1038/tpj.2015.49
30. Tong Q, Zhao DB, Bajracharya P, Xu X, Kong RN, Zhang J, et al. TNF-α−857 and−1031 polymorphisms predict good therapeutic response to TNF-α blockers in Chinese Han patients with ankylosing spondylitis. Pharmacogenomics. (2012) 13:1459–67. doi: 10.2217/pgs.12.133
31. Nossent JC, Sagen-Johnsen S, Bakland G. Tumor necrosis factor-alpha promoter−308/238 polymorphism association with less severe disease in ankylosing spondylitis is unrelated to serum TNF-α and does not predict TNF inhibitor response. J Rheumatol. (2014) 41:1675–82. doi: 10.3899/jrheum.131315
32. Ovejero-Benito MC, Munoz-Aceituno E, Reolid A, Fisas LH, Llamas-Velasco M, Prieto-Perez R, et al. Polymorphisms associated with anti-TNF drugs response in patients with psoriasis and psoriatic arthritis. J Eur Acad Dermatol Venereol. (2019) 33:e175–e7. doi: 10.1111/jdv.15431
33. Murdaca G, Gulli R, Spano F, Lantieri F, Burlando M, Parodi A, et al. TNF-α gene polymorphisms: association with disease susceptibility and response to anti- TNF-α treatment in psoriatic arthritis. J Invest Dermatol. (2014) 134:2503–9. doi: 10.1038/jid.2014.123
34. Morales-Lara MJ, Conesa-Zamora P, Garcia-Simon MS, Pedrero F, Santaclara V, Perez-Guillermo M, et al. Association between the FCGR3A V158F polymorphism and the clinical response to infliximab in rheumatoid arthritis and spondyloarthritis patients. Scand J Rheumatol. (2010) 39:518–20. doi: 10.3109/03009741003781969
35. Harrison SR, Burska AN, Emery P, Marzo-Ortega H, Ponchel F. Interferon-related gene expression in response to TNF inhibitor treatment in ankylosing spondylitis patients: a pilot study. Rheumatology. (2021) 60:3607–16. doi: 10.1093/rheumatology/keaa817
36. Aita A, Basso D, Ramonda R, Moz S, Lorenzin M, Navaglia F, et al. Genetics in TNF-TNFR pathway: a complex network causing spondyloarthritis and conditioning response to anti-TNFalpha therapy. PLoS ONE. (2018) 13:e0194693. doi: 10.1371/journal.pone.0194693
37. Schiotis R, Sanchez A, Escudero A, Bartolome N, Szczypiorska M, Font P, et al. Candidate's single-nucleotide polymorphism predictors of treatment nonresponse to the first anti-TNF inhibitor in ankylosing spondylitis. Rheumatol Int. (2014) 34:793–801. doi: 10.1007/s00296-013-2913-y
38. So J, Tam LS. Gut microbiome and its interaction with immune system in spondyloarthritis. Microorganisms. (2020) 8:1727. doi: 10.3390/microorganisms8111727
39. Mielants H, Veys EM, Cuvelier C, de Vos M. Ileocolonoscopic findings in seronegative spondylarthropathies. Br J Rheumatol. (1988) 27:95–105. doi: 10.1093/rheumatology/XXVII.suppl_2.95
40. Mielants H, Veys EM, Cuvelier C, De Vos M, Goemaere S, De Clercq L, et al. The evolution of spondyloarthropathies in relation to gut histology. II Histological aspects. J Rheumatol. (1995) 22:2273–8.
41. Mielants H, Veys EM, Cuvelier C, De Vos M, Goemaere S, De Clercq L, et al. The evolution of spondyloarthropathies in relation to gut histology. III Relat Between Gut Joint. J Rheumatol. (1995) 22:2279–84.
42. De Vos M, Cuvelier C, Mielants H, Veys E, Barbier F, Elewaut A. Ileocolonoscopy in seronegative spondylarthropathy. Gastroenterology. (1989) 96:339–44. doi: 10.1016/0016-5085(89)91557-6
43. Van Praet L, Van den Bosch FE, Jacques P, Carron P, Jans L, Colman R, et al. Microscopic gut inflammation in axial spondyloarthritis: a multiparametric predictive model. Ann Rheum Dis. (2013) 72:414–7. doi: 10.1136/annrheumdis-2012-202135
44. Van Praet L, Jans L, Carron P, Jacques P, Glorieus E, Colman R, et al. Degree of bone marrow oedema in sacroiliac joints of patients with axial spondyloarthritis is linked to gut inflammation and male sex: results from the GIANT cohort. Ann Rheum Dis. (2014) 73:1186–9. doi: 10.1136/annrheumdis-2013-203854
45. Sartor RB, Wu GD. Roles for intestinal bacteria, viruses, and fungi in pathogenesis of inflammatory bowel diseases and therapeutic approaches. Gastroenterology. (2017) 152:327–39e4. doi: 10.1053/j.gastro.2016.10.012
46. Nakatsuji T, Gallo RL. The role of the skin microbiome in atopic dermatitis. Ann Allergy Asthma Immunol. (2019) 122:263–9. doi: 10.1016/j.anai.2018.12.003
47. Wang Y, Wei J, Zhang W, Doherty M, Zhang Y, Xie H, et al. Gut dysbiosis in rheumatic diseases: a systematic review and meta-analysis of 92 observational studies. EBioMed. (2022) 80:104055. doi: 10.1016/j.ebiom.2022.104055
48. Wain WH, Price MF, Brayton AR, Cawson RA. Macromolecular syntheses during the cell cycles of yeast and hyphal phases of Candida albicans. J Gen Microbiol. (1976) 97:211–7. doi: 10.1099/00221287-97-2-211
49. Rath HC, Herfarth HH, Ikeda JS, Grenther WB, Hamm TE, Balish E, et al. Normal luminal bacteria, especially Bacteroides species, mediate chronic colitis, gastritis, and arthritis in HLA-B27/human beta2 microglobulin transgenic rats. J Clin Invest. (1996) 98:945–53. doi: 10.1172/JCI118878
50. Ruutu M, Thomas G, Steck R, Degli-Esposti MA, Zinkernagel MS, Alexander K, et al. Beta-glucan triggers spondylarthritis and Crohn's disease-like ileitis in SKG mice. Arthritis Rheum. (2012) 64:2211–22. doi: 10.1002/art.34423
51. Costello ME, Ciccia F, Willner D, Warrington N, Robinson PC, Gardiner B, et al. Brief report: intestinal dysbiosis in ankylosing spondylitis. Arthritis Rheumatol. (2015) 67:686–91. doi: 10.1002/art.38967
52. Tito RY, Cypers H, Joossens M, Varkas G, Van Praet L, Glorieus E, et al. Brief report: dialister as a microbial marker of disease activity in spondyloarthritis. Arthritis Rheumatol. (2017) 69:114–21. doi: 10.1002/art.39802
53. Breban M, Tap J, Leboime A, Said-Nahal R, Langella P, Chiocchia G, et al. Faecal microbiota study reveals specific dysbiosis in spondyloarthritis. Ann Rheum Dis. (2017) 76:1614–22. doi: 10.1136/annrheumdis-2016-211064
54. Stoll ML, Weiss PF, Weiss JE, Nigrovic PA, Edelheit BS, Bridges SL, et al. Age and fecal microbial strain-specific differences in patients with spondyloarthritis. Arthritis Res Ther. (2018) 20:14. doi: 10.1186/s13075-018-1510-6
55. Wen C, Zheng Z, Shao T, Liu L, Xie Z, Le Chatelier E, et al. Quantitative metagenomics reveals unique gut microbiome biomarkers in ankylosing spondylitis. Genome Biol. (2017) 18:142. doi: 10.1186/s13059-017-1352-6
56. Manasson J, Wallach DS, Guggino G, Stapylton M, Badri MH, Solomon G, et al. Interleukin-17 inhibition in spondyloarthritis is associated with subclinical gut microbiome perturbations and a distinctive interleukin-25-driven intestinal inflammation. Arthritis Rheumatol. (2020) 72:645–57. doi: 10.1002/art.41169
57. Scher JU, Ubeda C, Artacho A, Attur M, Isaac S, Reddy SM, et al. Decreased bacterial diversity characterizes the altered gut microbiota in patients with psoriatic arthritis, resembling dysbiosis in inflammatory bowel disease. Arthritis Rheumatol. (2015) 67:128–39. doi: 10.1002/art.38892
58. Yue B, Luo X, Yu Z, Mani S, Wang Z, Dou W. Inflammatory bowel disease: a potential result from the collusion between gut microbiota and mucosal immune system. Microorganisms. (2019) 7:440. doi: 10.3390/microorganisms7100440
59. Li M, Dai B, Tang Y, Lei L, Li N, Liu C, et al. Altered bacterial-fungal interkingdom networks in the guts of ankylosing spondylitis patients. mSystems. (2019) 4:e00176–18. doi: 10.1128/mSystems.00176-18
60. Norman JM, Handley SA, Baldridge MT, Droit L, Liu CY, Keller BC, et al. Disease-specific alterations in the enteric virome in inflammatory bowel disease. Cell. (2015) 160:447–60. doi: 10.1016/j.cell.2015.01.002
61. Zhang F, Ma C, Zhang B. Dynamic variations in gut microbiota in ankylosing spondylitis patients treated with anti- TNF-α for six months. Ann Clin Lab Sci. (2020) 50:99–106. doi: 10.1007/s10067-020-05032-4
62. Bazin T, Hooks KB, Barnetche T, Truchetet ME, Enaud R, Richez C, et al. Microbiota composition may predict anti-tnf alpha response in spondyloarthritis patients: an exploratory study. Sci Rep. (2018) 8:5446. doi: 10.1038/s41598-018-23571-4
63. Chen Z, Zheng X, Wu X, Wu J, Li X, Wei Q, et al. Adalimumab therapy restores the gut microbiota in patients with ankylosing spondylitis. Front Immunol. (2021) 12:700570. doi: 10.3389/fimmu.2021.700570
64. Hoentjen F, Welling GW, Harmsen HJ, Zhang X, Snart J, Tannock GW, et al. Reduction of colitis by prebiotics in HLA-B27 transgenic rats is associated with microflora changes and immunomodulation. Inflamm Bowel Dis. (2005) 11:977–85. doi: 10.1097/01.MIB.0000183421.02316.d5
65. Koleva PT, Valcheva RS, Sun X, Ganzle MG, Dieleman LA. Inulin and fructo-oligosaccharides have divergent effects on colitis and commensal microbiota in HLA-B27 transgenic rats. Br J Nutr. (2012) 108:1633–43. doi: 10.1017/S0007114511007203
66. Schultz M, Munro K, Tannock GW, Melchner I, Gottl C, Schwietz H, et al. Effects of feeding a probiotic preparation (SIM) containing inulin on the severity of colitis and on the composition of the intestinal microflora in HLA-B27 transgenic rats. Clin Diagn Lab Immunol. (2004) 11:581–7. doi: 10.1128/CDLI.11.3.581-587.2004
67. Sanges M, Valente G, Rea M, Della Gatta R, de Franchis G, Sollazzo R, et al. Probiotics in spondyloarthropathy associated with ulcerative colitis: a pilot study. Eur Rev Med Pharmacol Sci. (2009) 13:233–4.
68. Brophy S, Burrows CL, Brooks C, Gravenor MB, Siebert S, Allen SJ. Internet-based randomised controlled trials for the evaluation of complementary and alternative medicines: probiotics in spondyloarthropathy. BMC Musculoskelet Disord. (2008) 9:4. doi: 10.1186/1471-2474-9-4
69. Jenks K, Stebbings S, Burton J, Schultz M, Herbison P, Highton J. Probiotic therapy for the treatment of spondyloarthritis: a randomized controlled trial. J Rheumatol. (2010) 37:2118–25. doi: 10.3899/jrheum.100193
70. Haidmayer A, Bosch P, Lackner A, D'Orazio M, Fessler J, Stradner MH. Effects of probiotic strains on disease activity and enteric permeability in psoriatic arthritis-a pilot open-label study. Nutrients. (2020) 12:2337. doi: 10.3390/nu12082337
71. Grinnell M, Ogdie A, Wipfler K, Michaud K. Probiotic use and psoriatic arthritis disease activity. ACR Open Rheumatol. (2020) 2:330–4. doi: 10.1002/acr2.11143
72. Yang L, Liu B, Zheng J, Huang J, Zhao Q, Liu J, et al. Rifaximin alters intestinal microbiota and prevents progression of ankylosing spondylitis in mice. Front Cell Infect Microbiol. (2019) 9:44. doi: 10.3389/fcimb.2019.00044
73. Selvanderan SP, Goldblatt F, Nguyen NQ, Costello SP. Faecal microbiota transplantation for Clostridium difficile infection resulting in a decrease in psoriatic arthritis disease activity. Clin Exp Rheumatol. (2019) 37:514–5.
74. Kragsnaes MS, Kjeldsen J, Horn HC, Munk HL, Pedersen JK, Just SA, et al. Safety and efficacy of faecal microbiota transplantation for active peripheral psoriatic arthritis: an exploratory randomised placebo-controlled trial. Ann Rheum Dis. (2021) 80:1158–67. doi: 10.1136/annrheumdis-2020-219511
75. Popa SL, Dumitrascu DI, Brata VD, Duse TA, Florea MD, Ismaiel A, et al. Nutrition in spondyloarthritis and related immune-mediated disorders. Nutrients. (2022) 14:1278. doi: 10.3390/nu14061278
76. Ebringer A, Wilson C. The use of a low starch diet in the treatment of patients suffering from ankylosing spondylitis. Clin Rheumatol. (1996) 15:62–6. doi: 10.1007/BF03342649
77. Appelboom T, Durez P. Effect of milk product deprivation on spondyloarthropathy. Ann Rheum Dis. (1994) 53:481–2. doi: 10.1136/ard.53.7.481
78. Macfarlane TV, Abbood HM, Pathan E, Gordon K, Hinz J, Macfarlane GJ. Relationship between diet and ankylosing spondylitis: a systematic review. Eur J Rheumatol. (2018) 5:45–52. doi: 10.5152/eurjrheum.2017.16103
79. Ometto F, Ortolan A, Farber D, Lorenzin M, Dellamaria G, Cozzi G, et al. Mediterranean diet in axial spondyloarthritis: an observational study in an Italian monocentric cohort. Arthritis Res Ther. (2021) 23:219. doi: 10.1186/s13075-021-02600-0
80. Caso F, Navarini L, Carubbi F, Picchianti-Diamanti A, Chimenti MS, Tasso M, et al. Mediterranean diet and psoriatic arthritis activity: a multicenter cross-sectional study. Rheumatol Int. (2020) 40:951–8. doi: 10.1007/s00296-019-04458-7
81. Cai G, Wang L, Fan D, Xin L, Liu L, Hu Y, et al. Vitamin D in ankylosing spondylitis: review and meta-analysis. Clin Chim Acta. (2015) 438:316–22. doi: 10.1016/j.cca.2014.08.040
82. Gaal J, Lakos G, Szodoray P, Kiss J, Horvath I, Horkay E, et al. Immunological and clinical effects of alphacalcidol in patients with psoriatic arthropathy: results of an open, follow-up pilot study. Acta Derm Venereol. (2009) 89:140–4. doi: 10.2340/00015555-0555
83. Kristensen S, Schmidt EB, Schlemmer A, Rasmussen C, Johansen MB, Christensen JH. Beneficial effect of n-3 polyunsaturated fatty acids on inflammation and analgesic use in psoriatic arthritis: a randomized, double blind, placebo-controlled trial. Scand J Rheumatol. (2018) 47:27–36. doi: 10.1080/03009742.2017.1287304
84. Scalise G, Ciancio A, Mauro D, Ciccia F. Intestinal microbial metabolites in ankylosing spondylitis. J Clin Med. (2021) 10:3354. doi: 10.3390/jcm10153354
85. Machiels K, Joossens M, Sabino J, De Preter V, Arijs I, Eeckhaut V, et al. A decrease of the butyrate-producing species Roseburia hominis and Faecalibacterium prausnitzii defines dysbiosis in patients with ulcerative colitis. Gut. (2014) 63:1275–83. doi: 10.1136/gutjnl-2013-304833
86. Thorburn AN, McKenzie CI, Shen S, Stanley D, Macia L, Mason LJ, et al. Evidence that asthma is a developmental origin disease influenced by maternal diet and bacterial metabolites. Nat Commun. (2015) 6:7320. doi: 10.1038/ncomms8320
87. Miquel S, Martin R, Bridonneau C, Robert V, Sokol H, Bermudez-Humaran LG, et al. Ecology and metabolism of the beneficial intestinal commensal bacterium Faecalibacterium prausnitzii. Gut Microbes. (2014) 5:146–51. doi: 10.4161/gmic.27651
88. Kumari R, Ahuja V, Paul J. Fluctuations in butyrate-producing bacteria in ulcerative colitis patients of North India. World J Gastroenterol. (2013) 19:3404–14. doi: 10.3748/wjg.v19.i22.3404
89. Shao TJ, He ZX, Xie ZJ, Li HC, Wang MJ, Wen CP. Characterization of ankylosing spondylitis and rheumatoid arthritis using 1HNMR-based metabolomics of human fecal extracts. Metabolomics. (2016) 12:70. doi: 10.1007/s11306-016-1000-2
90. Lucas S, Omata Y, Hofmann J, Bottcher M, Iljazovic A, Sarter K, et al. Short-chain fatty acids regulate systemic bone mass and protect from pathological bone loss. Nat Commun. (2018) 9:55. doi: 10.1038/s41467-017-02490-4
91. Mizuno M, Noto D, Kaga N, Chiba A, Miyake S. The dual role of short fatty acid chains in the pathogenesis of autoimmune disease models. PLoS ONE. (2017) 12:e0173032. doi: 10.1371/journal.pone.0173032
92. Asquith M, Davin S, Stauffer P, Michell C, Janowitz C, Lin P, et al. Intestinal metabolites are profoundly altered in the context of HLA-B27 expression and functionally modulate disease in a rat model of spondyloarthritis. Arthritis Rheumatol. (2017) 69:1984–95. doi: 10.1002/art.40183
Keywords: spondyloarthritis precision medicine, genetics, microbiome, metabolomics, spondyloarthritis
Citation: So J, De Craemer A-S, Elewaut D and Tam L-S (2022) Spondyloarthritis: How far are we from precision medicine? Front. Med. 9:988532. doi: 10.3389/fmed.2022.988532
Received: 07 July 2022; Accepted: 16 August 2022;
Published: 08 September 2022.
Edited by:
Huji Xu, Tsinghua University, ChinaReviewed by:
Tejpal Gill, Oregon Health and Science University, United StatesCopyright © 2022 So, De Craemer, Elewaut and Tam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lai-Shan Tam, bHN0YW1AY3Voay5lZHUuaGs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.