 Pei Lu1†
Pei Lu1† Junyan Pu
Junyan Pu Zijie Wang
Zijie Wang Min Gu
Min Gu- 1Department of Urology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
- 2Department of Urology, The Affiliated Yixing Hospital of Jiangsu University, Yixing, China
Since 1969, an herbal medicine extracted from Quercus salicina Blume/Quercus stenophylla Makino (QS) has been clinically used for the management of urolithiasis in Japan. Historically, the decoction of leaves and shoots of QS trees was popularly utilized as a folk prescription to remove urinary calculi. This study was designed to perform a brief review of the updated progress of QS extract for urinary stones based on previous studies. A comprehensive literature search was conducted in multiple electronic databases, including Web of Science, PubMed, and EMBASE, and relevant data on QS extract were extracted. As a result, the major mechanism of QS extract for urolithiasis is observed to be closely related to the anti-oxidative activities according to recent studies, leading to inhibition of the accumulation of renal calcium and prevention of stone formation and recurrence of stones. As for the effect of discharging stones, loosening the upper urinary tract has also been noticed recently. More extensive studies are still necessary to systemically evaluate the individual dosage, drug safety, and targeted stone types.
Introduction
Urolithiasis is one of the common and detrimental diseases, affecting about 10–15% of the population around the world (1). In Asia, the prevalence is about 1–19.1%, varying with different social conditions and geographical positions. While the prevalence of urolithiasis keeps increasing these years, the recurrence rate reaches up to 21–53% after 3–5 years, and the lifetime risk of recurrence rate is about 60–80% (2). As a result, the urinary stone disease is a great burden for the health care system, which reminds us to pay attention to such disease (3).
According to the latest guidelines (4–7), current urinary stone management was generally classified into two types of treatments: surgical treatment and conservative treatment. For stones larger than 10 mm in diameter, surgical treatment is recommended according to international guidelines, such as percutaneous nephrolithotomy (PCNL), retrograde intrarenal surgery (RIRS), extracorporeal shockwave lithotripsy (ESWL), and ureteroscopic lithotripsy. The final selection of these operative methods is mostly determined by the positions and sizes of the stones. Aside from these operative treatments, conservative treatment is recommended for the spontaneous expulsion of ureteral stones, especially those smaller than 10 mm in diameter. Conservative treatment includes medical expulsion therapy (MET) and periodic follow-up, conventional oral drugs utilized in MET are alpha-blockers, calcium channel blockers, and PDE5 inhibitors, which can help relax ureteral passage and discharge stones.
In the 1960s, the extract of Quercus Salicina entered clinical application in Japan as a new oral administration for urolithiasis. Some controlled studies conducted in Japan proved that QS extract could exert its biological function by discharging upper urinary tract calculi (8, 9), while a series of randomized controlled clinical studies were carried out later to evaluate the efficacy and safety of the QS extract in the management of patients with kidney ureteral calculi, indicating that QS extract could significantly improve stone discharge rate, shorten the calculi discharge time and relieve back pain symptom (10–14). In cases of patients with larger kidney stones (larger than 10 mm in diameter), QS extract was also utilized after operative treatment, such as ureteroscopic lithotripsy, to increase the lithagogue rate (15, 16). Subsequently, a few studies involved the specific mechanism about the function of curing and preventing urolithiasis of QS extract were performed, indicating that the medical properties of QS are mostly due to its antioxidative capacity (17, 18).
To date, the administration of QS extract was limited in East Asian countries, while the biological function and its molecular mechanisms remain greatly lacking extensive research. Furthermore, various clinical issues were noticed in clinical use, hindering its wide application. Thus, this review focuses exclusively on the current progress of applications of QS based on its biological functions, especially on the clinical use for urolithiasis and related mechanisms.
Materials and methods
A comprehensive literature search was conducted in multiple electronic databases, including Web of Science, PubMed, and EMBASE, and relevant data on QS extract were extracted.
Quercus salicina Blume extracts
Quercus trees are oak species native to Japan and Korea. Aside from the resource for food and construction, researchers analyzed the components of Quercus species and found out that, especially, Quercus salicina Blume, were rich in phenolic compounds (19). Through the extraction of QS, 5 main components were isolated, named: (1) D-threo-guaiacylglycerol 8-O-β-D-(6'-O-galloyl)glucopyranoside, (2) 9-methoxy-D-threo-guaiacylglycerol8-O-β-D-(6'-O-galloyl)glu copyranoside, (3) 6"-O-galloyl salidroside, (4) methyl gallate, and (5) quercetin (20). The first four components are all phenolic compounds, generally consisting of phenolic acids and flavonoids, which have the property of antioxidation. Antioxidants are indispensable to defend against the damage of oxidative stress, caused by free radicals and reactive oxygen species (ROS), which can be classified into two categories: preventive antioxidants, including superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GTx), and radical scavenging antioxidants, including vitamin C, and flavonoid (21). As mentioned above, QS extract comprises large amounts of flavonoids, which belong to radical scavenging antioxidants, so QS extract prevents the injury caused by free radicals.
At present, QS extract has been mainly used in the fields of medicine, cosmetics, and food, the applications are listed in Table 1 (23–28). Basically, the majority of biological functions are related to antioxidation.
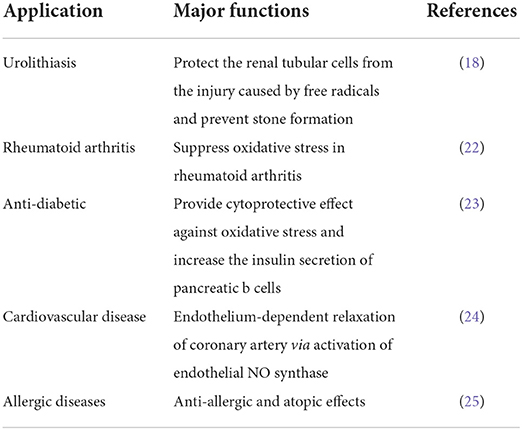
Table 1. Major medical functions and applications of QS extract.
Clinical applications of QS extracts in the treatment of urolithiasis
Nowadays, QS extract has been applied to clinical treatment alone or combined with operative management as oral administration. We have summarized studies conducted to testify to the therapeutic efficacy of urinary stones, and the results were systematically shown in Table 2.
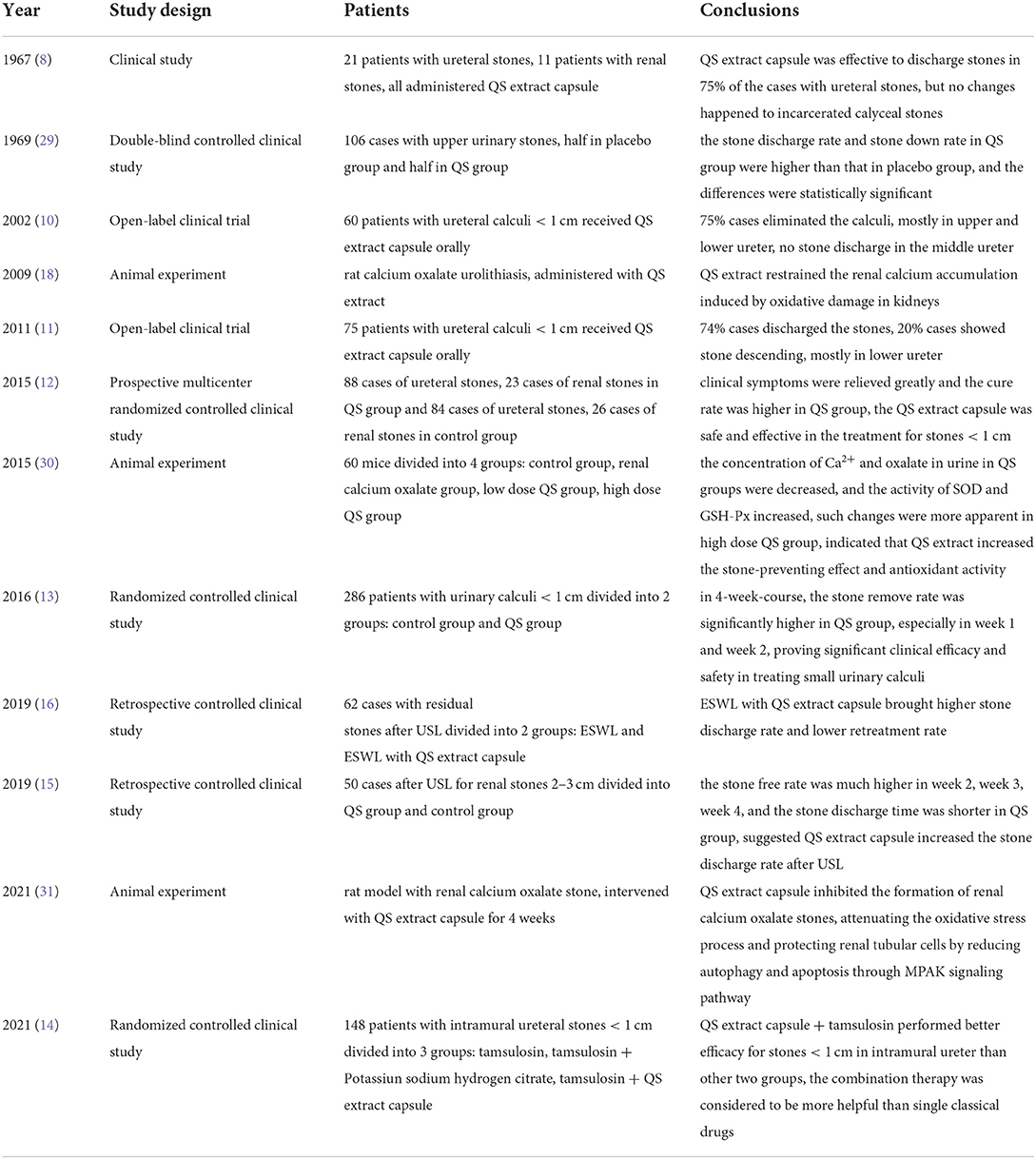
Table 2. Results of major research concerning the efficacy of urocalun for urinary stones.
Patients with kidney ureteral calculi that are less than 10 mm in diameter are considered to be able to pass stones by medication, while one prospective multicenter randomized controlled clinical study evaluated the efficacy of QS extract by providing a 4-week-treatment for these patients (12). A total of 111 patients in the experiment group administered QS extract capsules, 2 pills every time, 3 times a day, and 110 patients in the control group administered lithagogue powder, 1 bag every time, 3 times a day. After a 4-week-treatment, some clinical symptoms of patients in the experiment group, like low back pain or/and painful urination, and urinary frequency, were greatly relieved, and evaluating indexes like stone discharge rate, stone down rate, and stone expelling failure rate were 56.8, 12.6, 30.6, 39.1, 10, and 50.9% in experiment group and control group, respectively. The patients' conditions greatly improved in the experimental group, the total effective rate was 69.4%, much higher than in the control group, which was 49.1%, proving the overall efficiency of the QS extract capsule. In another study, the stone removal rate increased from 27 to 74% as the medication time was prolonged, and the stone removal rate was also variant on account of different positions in the urinary tract based on results of the plain film of kidney-ureter-bladder; it seemed to be most helpful for lower ureteral calculi (11), but it is still to be testified as the cases contained in this study were not enough.
Apart from monotherapy, combined treatments, including QS extract capsules and other conventional drugs or QS extract capsules administered after surgical management, were also reported. Conventional drugs, like a1-blockers, are recommended for urinary stones (< 10 mm) expulsion as they decrease the ureteral peristaltic frequency, smooth muscle tonus, contractile force, and increase ureteral flow. In a recent Chinese study, the author compared the effectiveness in 3 groups: the observation group used tamsulosin (a1-blocker) alone, the control group used tamsulosin and Potassium Sodium Hydrogen Citrate Granules, and the experiment group used tamsulosin and QS extract capsule. The stone discharge rates in the observation group, control group, and experiment group were 36, 78, and 82%, indicating that the combined treatment, tamsulosin and QS extract capsule, was the most effective (14). The clinical efficacy of QS extract was also confirmed in patients with kidney stones (2 to 3 cm) after receiving ureteroscopic lithotripsy, the effect of expediting stone discharge was better in the QS extract capsule group than that in the lithagogue powder group (15). Oral administration of QS extract capsule combined with ESWL (extracorporeal shock-wave lithotripsy) was also reported as a treatment for residual stones after ureteroscopic lithotripsy, the study concluded that such combination therapy was much more efficient than ESWL alone, not only increasing the stone-free rate but also decreasing the retreatment rate (16).
As we know, calcium oxalate has constituted the majority of urinary stones in recent years (32) and previous studies showed that the urinary oxalate levels of patients with urolithiasis were higher, meanwhile, increasing lipid peroxides and urinary tubular enzymes were found, indicating that the exposure to oxalate could result in lipid peroxidation and tubular cells injuries, primarily the proximal tubular cells (33). Such changes in the oxidant-antioxidant balance might be due to the toxic substance brought by the exposure to oxalate initially, and in the late stage, leukocytes infiltrated and antioxidant enzyme activities decreased, causing the kidney to remain under excessive oxidative stress (34). Free radical production elicited by peroxidation was related to the concentration of oxalate, but some researchers proposed that even though there was a tiny increase in urinary oxalate levels, it might still contribute to the progression of renal diseases (35). Later studies demonstrated that oxalate-induced free radical production in renal tubular epithelial cells was through the activation of NAD(P)H oxidase via cytokine TGF-β1 induction, and free radical scavengers could make this peroxide production decrease noticeably (36). These researches provide us the evidence that antioxidant therapy can prevent oxalate-mediated peroxidation and cell injuries caused by peroxidation; therefore, there would be less cellular debris for calcium oxalate crystal nucleation and aggregation, suspending the kidney stone formation and preventing stone recurrence. That is how QS extract works as lithophytic agent. Animal experiments have provided evidence that QS extract can inhibit the formation of renal calcium oxalate stone and the oxidative process. The researchers established the model mice with renal calcium oxalate stones by Glycol, and the administration of QS extract could decrease the concentration of Ca2+ and oxalate in the urine, and increase the activity of SOD and GSH-Px (30). Further mechanism illustrated that QS extract capsule inhibited the oxidative process induced by calcium oxalate crystallization and reduced the phosphorylation of MPAK signaling pathway, then the process of autophagy and apoptosis through MPAK signaling pathway was attenuated (31), which could protect the renal tubular epithelial cells and prevent the calcium oxalate crystal adhesion.
Safety
Mild side events, including nausea and vomiting, occurred in several cases, whereas there were no significant differences in incidence between the intervention group and control group in all these studies; after symptomatic treatment, these reactions were eased, and there were no indications of drug withdrawal. No severe side effects happened in these clinical trials yet. Furthermore, researchers did not exclude the possibility that such reactions might be related to nephrocolic instead of the medication. It remains to be investigated whether there are specific side effects of QS extract.
Japanese researchers also made a study of clinical equivalence of two different formulations of QS extract, capsule, and tablet, to examine whether these formulations would have an impact on the medicine potency. Results pointed out that both formulations exerted the same clinical effectiveness, while the miniaturized tablet might be better for medication compliance since it is more convenient for swallowing (37).
Limitations
As mentioned above, a 4-week treatment of QS extract capsule was usually contained, but no studies adopted a shorter or longer treatment period, although the stone discharge rate of patients administering QS extract capsule was higher, there was no significant difference in week 3 and week 4 (13). Therefore, the duration of QS extract capsule treatment needs to be further investigated whether a shorter course is efficient enough or a longer course is required to ensure the clearance of stones. Second, the dosage of the QS extract capsule in these studies was 450 mg taken 3 times per day. It is still unknown if there is a cytotoxic effect of QS extract capsule in clinical dosage and whether it would cause a medicament liver lesion or other damage when a longer course is required.
Importantly, no drug use report for children, pregnant, or lactating women was reported up to now. Moreover, the QS extract capsule performed different strengths on discharging stones in different positions of the urinary tract, which requires more investigation to clarify the concrete differences such medicine could bring about. Except for calcium oxalate calculus, urinary calculi include cystine calculus, magnesium ammonium phosphate calculus, and calcium phosphate calculus; the effect of the QS extract capsule on these stones remains to be studied to provide a clinical guide as an individualized treatment for patients with different types of stones.
As to the mechanism of QS extract capsule on the formation of urinary calculi, the protection for renal tubular epithelial cells through antioxidant activity against oxidative stress damage is considered as the main factor, inhibiting the crystals accumulation and stone formation. The researchers also found that acute renal tubular injury was relieved, and if intervened with a QS extract capsule in rat model with renal calcium oxalate stones (31), the concentration of Cr, BUN was decreased (30), suggesting that once the QS extract capsule could improve the renal function, there might be other ways for QS extract capsule to influence the renal tubular epithelial cells beside from antioxidation, and the corrected mechanism is under discussion, which could provide a new insight for the prevention and measures of urolithiasis.
Conclusions
QS extract has been utilized for the management of urolithiasis for several years, while most of the effects were attributed by its medical properties to the antioxidative activities. Clinical studies and animal experiments have proven that QS extract is of high efficacy and safety in the treatment of urinary calculi when used alone or in combination therapy. Taken together, QS extract improves the stone-free rate and resubmission rate in urolithiasis. With the advance in medical technology, the treatment for urolithiasis has improved dramatically, but its prevention still lacks effective medicine. The role of renal tubular cells' protection of QS extract by antioxidation may paint a fascinating and incomplete picture to take measures in preventing the calcium oxalate stone formation and recurrence.
Author contributions
PL: substantial contributions to the conception and design of the work, interpretation of data for the work, and manuscript revision. JP: the acquisition, analysis, and interpretation of data for the work and drafting the work. YZ: substantial contributions to the conception and design of the work and manuscript revision. ZW: manuscript revision and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy. PH: agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy and integrity of any part of the work are appropriately investigated and resolved. MG: substantial contributions to the conception and final approval of the version to be published. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the National Natural Science Foundation of China [Grant Nos. 82170769 and 81870512], Project of Jiangsu Province for Important Medical Talent [Grant No. ZDRCA2016025], the 333 High-Level Talents Project in Jiangsu Province [Grant No. BRA2016514], and the Standardized Diagnosis and Treatment Research Program of Key Diseases in Jiangsu Province [Grant No. BE2016791].
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Desai M, Sun Y, Buchholz N, Fuller A, Matsuda T, Matlaga B, et al. Treatment selection for urolithiasis: percutaneous nephrolithomy, ureteroscopy, shock wave lithotripsy, and active monitoring. World J Urol Mar. (2017) 35:1395–9. doi: 10.1007/s00345-017-2030-8
2. Liu Y, Chen Y, Liao B, Luo D, Wang K, Li H, et al. Epidemiology of urolithiasis in Asia. Asian J Urol Oct. (2018) 5:205–14. doi: 10.1016/j.ajur.2018.08.007
3. Ziemba JB, Matlaga BR. Epidemiology and economics of nephrolithiasis. Investig Clin Urol Sep. (2017) 58:299–306. doi: 10.4111/icu.2017.58.5.299
4. Kausman JY, Patel B, Marks SD. Standard dosing of tacrolimus leads to overexposure in pediatric renal transplantation recipients. Pediatr Transpl. (2008) 12:329–35. doi: 10.1111/j.1399-3046.2007.00821.x
5. Assimos D, Krambeck A, Miller NL, Monga M, Murad MH, Nelson CP, et al. Surgical Management of Stones: American Urological Association/Endourological Society Guideline, PART I. J Urol Oct. (2016) 196:1153–60. doi: 10.1016/j.juro.2016.05.090
6. Assimos D, Krambeck A, Miller NL, Monga M, Murad MH, Nelson CP, et al. Surgical Management of Stones: American Urological Association/Endourological Society Guideline, PART II. J Urol Oct. (2016) 196:1161–9. doi: 10.1016/j.juro.2016.05.091
7. Taguchi K, Cho SY, Ng AC, Usawachintachit M, Tan YK, Deng YL, et al. The Urological Association of Asia clinical guideline for urinary stone disease. Int J Urol Jul. (2019) 26:688–709. doi: 10.1111/iju.13957
8. Goto K, Ito S, Otani F, Liu J. Clinical effects of Urocalun for the upper urinary urolithiasis. Acta Urologica Japonica Aug. (1967) 13:628–31.
9. Inada T, Kitayama T. Use of Urocalun in patients with urolithiasis in the upper urinary tracts. Acta Urologica Japonica Jun. (1967) 13:470–4.
10. Xiaochun Z, Yanqun N. Treatment of calculus in ureter with Urocalun (report of 60 cases). Chin J Urol. (2002) 23:696–7. doi: 10.3760/j:issn:1000-6702.2002.11.019
11. Lixia Z, Feiyuan L, Li'e D. Experiences of treatment of urolithiasis with urocalun. Med Innov China. (2011) 8:141–2. doi: 10.3969/j.issn.1674-4985.2011.27.088
12. Hu H, Xuhui Z, Xiaochun Z, et al. Quercus salicina extract capsules in the management of kidney ureteral calculi: a prospective multicenter randomized controlled clinical study. Chin J Urol. (2015) 36:533–7. doi: 10.3760/cma.j.issn.1000-6702.2015.07.015
13. Jianyu X, Jiaxun L, Jianpeng Y. The Clinical Efficacy ofQuercus Salicina Extract Capsules on Urinary Calculi. J Mod Urol. (2016) 21:793–5. doi: 10.3969/j.issn.1009-8291.2016.10.014
14. Shuai Y, Wenjin Z, Jingyu W, Yangang Z. Clinical Efficacy of Quercus Salicina Extract Capsules and Potassium Sodium Hydrogen Citrate on Stones in the Intramural Ureter. Chin Remed Clin. (2021) 21:108–10. doi: 10.11655/zgywylc2021.01.051
15. Tengfei G, Dengyang M, Ting C, Jing S. Effect of urocalun on renal stones from 2 to 3 cm after ureteroscopic lithotripsy. Zhejiang Practical Medicine. (2019) 24:434–5. doi: 10.16794/j.cnki.cn33-1207/r.2019.06.015
16. Kang P, Jie L, Hao W, Xiaofei D. Clinical study of treatment of stone residue after flexible ureteroscopy with urocalun and ESWL. Electronic J Clin Med Literature. (2019) 6:82. doi: 10.16281/j.cnki.jocml.2019.97.053
17. Moriyama MT, Miyazawa K, Noda K, Oka M, Tanaka M, Suzuki K. Reduction in oxalate-induced renal tubular epithelial cell injury by an extract from Quercus salicina Blume/Quercus stenophylla Makino. Urol Res. (2007) 35:295–300. doi: 10.1007/s00240-007-0114-4
18. Moriyama MT, Suga K, Miyazawa K, Tanaka T, Higashioka M, Noda K, et al. Inhibitions of urinary oxidative stress and renal calcium level by an extract of Quercus salicina Blume/Quercus stenophylla Makino in a rat calcium oxalate urolithiasis model. Int J Urol. (2009) 16:397–401. doi: 10.1111/j.1442-2042.2009.02268.x
19. Jong JK, Bimal KG, Hyeun CS, Kyung JL Ki SS, Young SC, et al. Comparison of phenolic compounds content in indeciduous Quercus species. J Med Plants Res. (2012) 6:5228–39. doi: 10.5897/JMPR12.135
20. Kim JI, Kim HH, Kim S, Lee KT, Ham IH, Whang WK. Antioxidative compounds from Quercus salicina Blume stem. Arch Pharm Res Mar. (2008) 31:274–8. doi: 10.1007/s12272-001-1152-2
21. Antolovich M, Prenzler PD, Patsalides E, McDonald S, Robards K. Methods for testing antioxidant activity. The Analyst. (2002) 127:183–98. doi: 10.1039/b009171p
22. Min-Soo LE, Myung-Hee JE, Jin-Sun HE, Jong-Bok KI, Jongwon CH. Protective effects of Quercus salicina Blume against FCA-induces oxidative stress in rheumatoid arthritis (abstract no. P7-9). In: Proceedings of International Congress of Korean Federation of Pharmaceutical Societies April 19-21, International Convention Center, Jeju, Korea The Pharmaceutical Society of Korea, Seoul, Korea. (2012).
23. Song JL, Zhao X, Wang Q. Protective effects of Quercus salicina on alloxan-induced oxidative stress in HIT-T15 pancreatic beta cells. Exp Ther Med Mar. (2013) 5:947–51. doi: 10.3892/etm.2013.885
24. Park SH, Kim HJ, Yoon JS, Lee HW, Park GC Yi E, et al. The Effect of Quercus salicina Leaf Extracts on Vascular Endothelial Function: Role of Nitric Oxide. J Nanosci Nanotechnol Feb. (2016) 16:2069–71. doi: 10.1166/jnn.2016.11930
25. Bak JP. Screening and Compound Isolation from Natural Plants for Anti-allergic Activity. Journal of the Korean Society for Applied Biological Chemistry. (2011) 54:367–75. doi: 10.3839/jksabc.2011.058
26. Aung T, Bibat MAD, Zhao CC, Eun JB. Bioactive compounds and antioxidant activities of Quercus salicina Blume extract. Food Sci Biotechnol Apr. (2020) 29:449–58. doi: 10.1007/s10068-020-00755-1
27. Yue WG, Yin S, Ding Y, Lin Z, Li Y. Quercus salicina Blume: Research progress in chemistry and pharmacodynamics (1959-2021). Exp Ther Med. (2013) 5:947–51.
28. Lee HJ, Park SN. Antioxidative effect and active component analysis of quercus salicina blume extracts. J Soc Cosmet Scientists Korea. (2011) 37:143–52. doi: 10.1002/cbdv.202100777
29. Kato T, Takahashi Y, Fukuyama T, Oka N, Hasegawa T. Urocalun for upper urinary stones–investigation of its effect on stone passage by means of simultaneous control study in double blind method. Acta Urol Japonica. (1969) 15:460–70.
30. Hui L, JianWen Z, ShengPing Z, HongLiang W, Rui S, Fan Z, et al. Excluding stone efficiency of quercus salicina extract capsules on renal calcium oxalate mouse without renal function damage. J Trop Med. (2015) 15:886–9.
31. Pei L, Rijin S, Wei Z, et al. The effect and mechanism of urocalum on the formation of renal calcium oxalate crystals. J Nanjing Med Univ Nov. (2021) 41:1569–73.
32. Hali A, Bhatti KH, Boeri L, Cloutier J, Davidoff K, Elqady A, et al. Stone composition of renal stone formers from different global regions. Arch Ital Urol Androl. (2021) 93:307–12. doi: 10.4081/aiua.2021.3.307
33. Huang H-S, Ma M-C, Chen C-F, Chen J. Lipid peroxidation and its correlations with urinary levels of oxalate, citric acid, and osteopontin in patients with renal calcium oxalate stones. Urology. (2003) 62:1123–8. doi: 10.1016/S0090-4295(03)00764-7
34. Huang H-S, Ma M-C, Chen J, Chen C-F. Changes in the oxidant-antioxidant balance in the kidney of rats with nephrolithiasis induced by ethylene glycol. J Urol. (2002) 167:2584–93. doi: 10.1016/S0022-5347(05)65042-2
35. Scheid C, Koul H, Hill WA, Luber-Narod J, Kennington L, Honeyman T, et al. Oxalate toxicity in LLC-PK1 cells: Role of free radicals. Kidney Int. (1996) 49:413–9. doi: 10.1038/ki.1996.60
36. Rashed T, Menon M, Thamilselvan S. Molecular mechanism of oxalate-induced free radical production and glutathione redox imbalance in renal epithelial cells: effect of antioxidants. Am J Nephrol Sep-Oct. (2004) 24:557–68. doi: 10.1159/000082043
Keywords: Quercus salicina extract, urolithiasis, anti-oxidative, stone formation, clinical application
Citation: Lu P, Pu J, Zong Y, Wang Z, Han P and Gu M (2022) Application of Quercus salicina extract in the management of urolithiasis. Front. Med. 9:960292. doi: 10.3389/fmed.2022.960292
Received: 02 June 2022; Accepted: 29 August 2022;
Published: 20 September 2022.
Edited by:
Dongyuan Chang, First Hospital, Peking University, ChinaReviewed by:
Andrea Angeletti, Giannina Gaslini Institute (IRCCS), ItalySajid Sultan, Sindh Institute of Urology and Transplantation, Pakistan
Copyright © 2022 Lu, Pu, Zong, Wang, Han and Gu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min Gu, bGFuY2V0Z3VAYWxpeXVuLmNvbQ==
†These authors have contributed equally to this work