 Alejandra Aguilar-Latorre1
Alejandra Aguilar-Latorre1 Guillermo Pérez Algorta2
Guillermo Pérez Algorta2 Capilla Navarro-Guzmán3María J. Serrano-Ripoll4,5,6*
Capilla Navarro-Guzmán3María J. Serrano-Ripoll4,5,6* Bárbara Oliván-Blázquez1,7
Bárbara Oliván-Blázquez1,7- 1Primary Healthcare Center Arrabal, Institute for Health Research Aragón (IIS Aragón), Zaragoza, Spain
- 2Division of Health Research, Faculty of Health and Medicine, Lancaster University, Lancaster, United Kingdom
- 3Department of Psychology, University of the Balearic Islands, Palma, Spain
- 4Primary Care Research Unit of Mallorca, Balearic Islands Health Services, Palma, Spain
- 5Research in Preventive Activities and Promotion and in Cancer Illes Balears (GRAPP-CAIB), Balearic Islands Health Research Institute (IdISBa), Palma, Spain
- 6Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS), Barcelona, Spain
- 7Department of Psychology and Sociology, University of Zaragoza, Zaragoza, Spain
Background: Depression symptoms are prevalent in the general population, and their onset and continuation may be related to biological and psychosocial factors, many of which are related to lifestyle aspects. Health promotion and lifestyle modification programmes (LMPs) may be effective on reducing the symptoms. The objective of this study was to analyse the clinical effectiveness of a LMP and a LMP plus Information and Communication Technologies, when compared to Treatment as Usual (TAU) over 6 months. The interventions were offered as an adjuvant treatment delivered in Primary Healthcare Centers (PHCs) for people with depression symptoms.
Methods: We conducted an open-label, multicentre, pragmatic, randomized clinical trial. Participants were recruited from several PHCs. Those participants visiting general practitioner for any reason, who also met the inclusion criteria (scoring 10 to 30 points on the Beck II Self-Applied Depression Inventory) were invited to take part in the study. TAU+LMP consisted of six weekly 90-min group sessions focused on improving lifestyle. TAU+LMP + ICTs replicated the TAU+LMP format, plus the addition of a wearable smartwatch to measure daily minutes walked and sleep patterns. A total of 188 participants consented to participate in the study and were randomized. We used linear mixed models, with a random intercept and an unstructured covariance to evaluate the impact of the interventions compared to TAU.
Results: Both interventions showed a statistically significant reduction on depressive symptoms compared to TAU (TAU+LMP vs. TAU slope difference, b = −3.38, 95% CI= [−5.286, −1.474] p = 0.001 and TAU+LMP+ICTs vs. TAU slope difference, b = −4.05, 95% CI = [−5.919, −2.197], p < 0.001). These reductions imply a moderate effect size. In the TAU+LMP+ICTs there was a significant increase regarding minutes walking per week (b = 99.77) and adherence to Mediterranean diet (b = 0.702). In the TAU+LMP there was a significant decrease regarding bad sleep quality (b = −1.24).
Conclusion: TAU+LMPs administered in PHCs to people experiencing depression symptoms were effective on reducing these symptoms compared to TAU. They also have a positive impact on changing several lifestyle factors. These findings indicate that these interventions can be promising strategies for PHCs.
Introduction
It is estimated that 280 million people of all ages are currently experiencing depression symptoms and their impact (1). Due to its high prevalence in primary care settings (2), its treatment at this level of care is recommended (3, 4). One of the goals of primary care interventions is about educating people about healthy lifestyle habits (5). Lifestyle Modification Programmes (LMPs) can prevent the development of depression and are considered a successful treatment option (6–9). Regarding specific lifestyle factors, regular leisure-time exercise of any intensity has been shown to improve mental health and prevent depression (10, 11). Moreover, sleep disturbance is not only a manifestation of depression but can also be considered a prodromal symptom, therefore, its identification and treatment needs to be prioritized before, during and after experiencing depression (12, 13).
Spain has long been associated with the Mediterranean diet, which is regarded as one of the world's healthiest dietary patterns (14). This dietary pattern may be a safe and low-cost measure for depression prevention (15).
Additionally, facilitators of adherence to interventions, such as the use of Information and Communication Technologies (ICTs), should be considered in LMPs (16). In previous studies, the practice of monitoring behaviors in daily life has been useful to promote lifestyle changes in depressed people in primary care (17, 18). More specifically, wearable devices have been proven to be feasible and acceptable for use among overweight people with severe mental illness (19). These devices allow for monitoring behaviors in real-time in an unobtrusive way, enabling people to monitor and change their own activity (20).
Therefore, specifically, and as a novelty of this study, we combined and promoted several healthy lifestyles together (physical activity, sleep patterns and diet) in a face-to-face group format at the primary healthcare level with a longitudinal follow-up at 6 months in order to evaluate the effectiveness of the interventions over time.
The main objective is to analyse the clinical effectiveness of a TAU+LMP and an TAU+LMP with ICTs, when compared to Treatment as Usual (TAU) over 6 months, delivered in the context of in Primary Healthcare Centers (PHCs) as an adjuvant treatment for people experiencing depression symptoms. The second objective is to analyse if both interventions are similarly effective in improving the results of the lifestyle variables when compared to TAU.
Methods and analysis
Study design
An open-label, multicentre, pragmatic, randomized clinical trial (RCT) in three parallel groups was carried out: TAU as a control group, and TAU+LMP and TAU+LMP+ICTs as intervention groups in several PHCs.
Sample size
To estimate the sample needed for this study, a Spanish study conducted with primary care patients with depression was considered as a proxy reference (18). Serrano-Ripoll et al. (18) reported an average score in BDI-II (21) at baseline of 24.5 points (SD 7.84). Following Button et al. (22) recommendation of considering a 17.5% reduction in the BDI-II as clinically relevant, we determined that a decrease of at least 4.28 points would be clinically significant and beneficial for people in Spain. Accepting a risk of 0.05 and a risk of 0.20 in a bilateral contrast, each treatment group required 35 participants. A final sample size of 42 people per each group was considered, with consideration of having a possible 20% withdrawal rate. The total sample size required was 126.
Recruitment and participants
Participants were chosen from among those who visited a general practitioner (GP) at one of the participating PHCs for any reason and who also met the inclusion criteria described below. The recruiting time was 7 months (starting in April 2020 and finishing in October 2020). By the end of the study, 188 patients from PHCs in two locations in Spain (Zaragoza and Mallorca) with subclinical, mild or moderate depression (scoring 10 to 30 points on the BDI-II) (21) were recruited for the study. Further details about the inclusion and exclusion criteria are available in the published protocol (23).
A computer-generated random number (24) administered by an independent researcher was used to allocate participants. All the study centers randomized patients to all conditions.
Intervention development and evaluation
All participants received a general medical care from their GPs, which means that they received the care they usually get in PHC, which typically does not mean care from clinicians specialized in delivering mental health care (25). In Spain general medical care could be usual antidepressant treatment with psychological advice and / or psychotropic drugs by the GP (26).
Those allocated to TAU+LMP received 90-min session per week for 6 weeks conducted by an expert psychologist, which were also supplemented with PowerPoint presentations. The following topics were covered: 1) Psychoeducation on depression; 2) Behavior activation; 3) Sleep hygiene habits and careful exposure to sunlight; 4) Physical activity; 5) Adherence to the Mediterranean diet; and 6) Summary of previous sessions. TAU+LMP+ICTs replicated the TAU+LMP format, plus the addition that participants were given a wearable smartwatch and instructed to wear it to measure daily minutes walked and sleep patterns. Those participants not assigned to either of the two interventions were considering as part of TAU group (25).
A blinded research assistant gathered patient data by administering questionnaires at baseline (T0), immediately after the intervention (T1), and at six-month follow-up session (T2).
Outcomes and measures
Data about gender, age, marital status, level of education, occupation and economic level were collected. Chronic comorbidities with prevalences >5% were also considered (arrhythmias, heart failure, ischemic cardiopathy, dyslipidemia, obesity, excess weight, vein and artery disease, cerebrovascular disease, diabetes, chronic bronchitis, chronic obstructive pulmonary disease (COPD), asthma, chronic kidney disease, hypo and hyperthyroidism, tobacco use, alcoholism, insomnia, attempted suicide, anemia, neoplasia, dementia, deafness, cataracts, glaucoma, arthrosis, osteoporosis, and back pain) (27).
The primary outcome was the severity of depressive symptoms, measured by the BDI-II. It consists of 21 questions, with higher scores indicating more severe depressive symptomatology (28). The internal consistency of the BDI-II in our sample was acceptable at baseline (α = 0.71).
Secondary outcomes
To analyse the effectiveness of the intervention in modifying lifestyles, physical activity was measured using the International Physical Activity Questionnaire-Short Form (IPAQ-SF) (29). It assesses the activity over the last seven days (30) and contains seven items. In our analysis, we use the minutes walking per week and the minutes seated per day.
Adherence to the Mediterranean diet was assessed using the 14-item Mediterranean Diet Adherence Screener (MEDAS), developed by the PREDIMED study group (31). It includes items related to food consumption and consumption habits. Higher scores indicate higher level of adherence (32).
Sleep quality and sleep patterns were measured using the Pittsburgh Sleep Quality Index (PSQI) (33), which consists of 19 questions about subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, sleep medication use and daytime dysfunction over the previous month. Higher scores indicate worse sleep quality (34). The internal consistency of the PSQI in our sample was acceptable at baseline (α = 0.75).
Ethics approval
Ethics approval was granted by the Research Ethics Committee of Aragón (CEICA, PI18/286) and the Research Ethics Committee of the Balearic Islands (IB3950/19 PI). The study was developed following the Helsinki Declaration. All of the subjects signed an informed consent form; their data were anonymized and were only used for the purposes of the study.
Statistical analysis
Firstly, a descriptive analysis (frequencies for categorical variables; means and standard deviation for continuous variables) and a univariate analysis (one-way ANOVA for age, BDI-II, IPAQ-SF, PSQI, and MEDAS, and Chi-Square test for the remaining variables) were used to examine the data and tested whether there were baseline differences between groups after randomization. Secondly, to answer the main objective – whether there were differences between treatment groups regarding their effectiveness in reducing depression—we used Linear Mixed-Effects Models (LMEMs) (35). We specified a model with a random intercept and unstructured covariance. The parameter of interest was the interaction effect of treatment and time in a model that also included age as a covariate because it was the only baseline variable that was significantly different between groups. Cohen's d (d) is calculated from the estimated mean values of BDI-II and its standard deviations (SD) at baseline (36).
Moreover, to answer the second question—whether there were differences between treatment groups with respect to the improvement of lifestyle variables—we used LMEMs with the same previous components.
The statistical analysis was carried out per intention-to-treat analysis (ITT) (i.e., all participants who were randomized were included in the statistical analysis and were analyzed according to the group to which they were originally assigned) (37). The results from the trial were presented as a regression coefficient for predicting change in primary and secondary outcomes with 95% confidence intervals. LMEMs were tested against a Bonferroni-adjusted alpha level of 0.01 (0.05/5) (38). A statistical analysis was performed using the SPSS software (version 25.0) (39).
Results
A total of 246 participants were evaluated for eligibility, with 14 of them failing to meet the inclusion criteria, 6 declining to participate because they were not interested, and 38 declining to participate because they had time incompatibility. Of the 246 initial participants, 58 (23.58%) did not participate. Finally, 188 participants were included (Figure 1).

Figure 1. Flowchart of the study: randomization, sampling and monitoring of patients. GP, General Practitioner; TAU, Treatment as Usual; LMP, Lifestyle Modification Programme; ICTs, Information and Communication Technologies; ITT, Intention-to-treat.
Firstly, the descriptive analysis showed that of the 188 participants, 162 were female and 26 were male, and all participants were between 20 to 83 years old (mean age = 53.32, SD = 13.07). The univariate analysis subsequently revealed significant differences between the groups (p = 0.014) regarding age, specifically between the TAU and TAU+LMP+ICTs groups (p = 0.018), with the TAU+LMP+ICT participants being older. However, no significant differences were found between the groups in the other variables (Table 1).
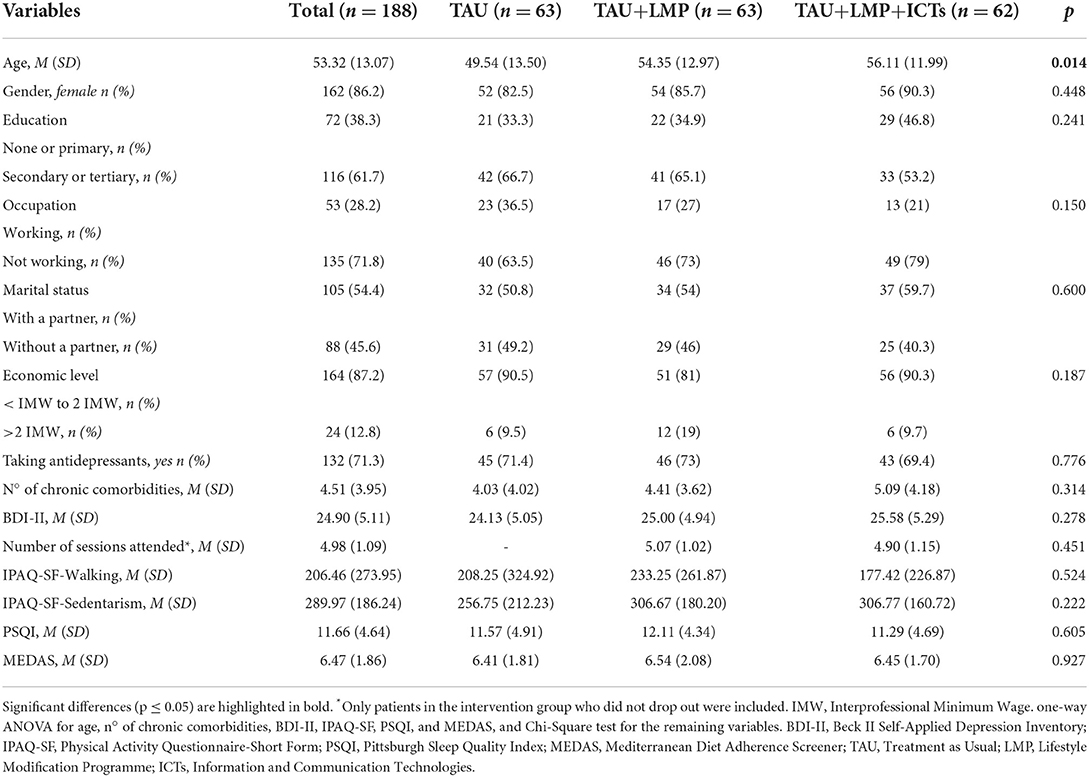
Table 1. Sociodemographic and clinical characteristics of the sample.
Considering the raw scores of both intervention groups, there was a decrease in BDI-II at 6 months compared to baseline levels (TAU+LMP mean difference = −5.48, SD = 9.50 and TAU+LMP+ICTs mean difference = −7.71, SD = 11.52). Also, an increase in IPAQ–SF–Walking (TAU+LMP mean difference = 123.56, SD = 251.74 and TAU+LMP+ICTs mean difference = 189.88, SD = 350.99), a decrease in IPAQ–SF–Sedentarism (TAU+LMP mean difference = −2.56, SD = 167.48 and TAU+LMP+ICTs mean difference = −32.62, SD = 189.61), a decrease in PSQI (TAU+LMP mean difference = −3.21, SD = 4.36 and TAU+LMP+ICTs mean difference = −1.52, SD = 5.13) and a decrease and an increase in MEDAS (TAU+LMP mean difference = −0.21, SD = 2.15 and TAU+LMP+ICTs mean difference =0.92, SD = 1.64) (Table 2).
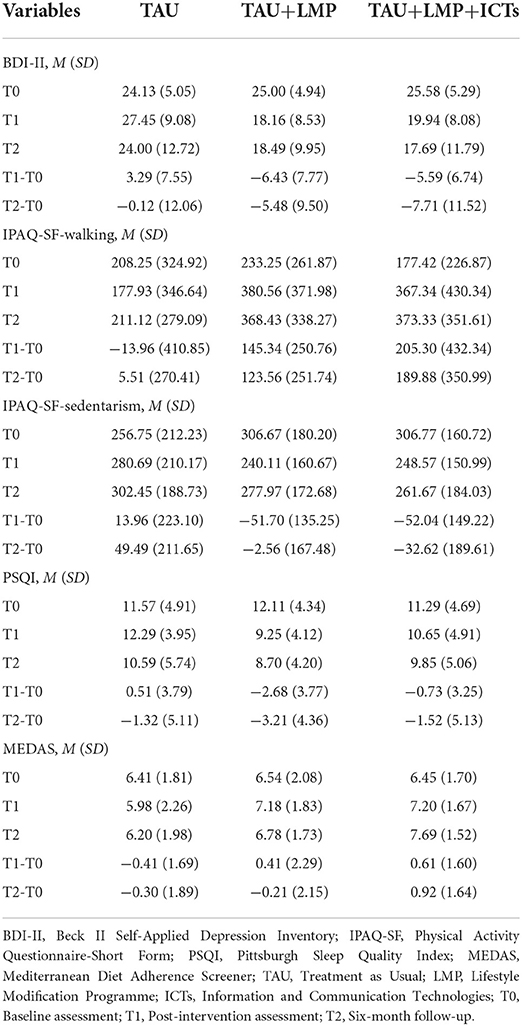
Table 2. Outcome variables of each group in each measurement.
Secondly, the LMEM evidenced that both interventions could be clinically effective compared to TAU, as there was a significant interaction effect for both treatments and time on BDI–II (TAU+LMP vs. TAU slope difference: b = −3.38, 95% CI= [−5.286, −1.474] p =0.001; and TAU+LMP+ICTs vs. TAU slope difference: b = −4.06, 95% CI= [−5.919, −2.197], p <0.001) (Table 3). That reduction in BDI–II implies a moderate effect size in both TAU+LMP and TAU+LMP+ICTs groups (d =0.671 and d =0.779, respectively).
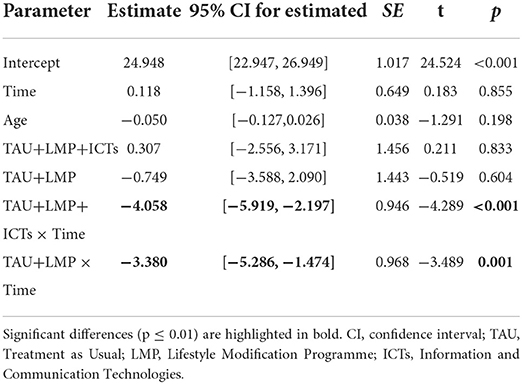
Table 3. Estimates of Fixed Effects in BDI-II.
Moreover, LMEMs showed that the variables that measure lifestyle (IPAQ–SF–Walking, IPAQ–SF–Sedentarism, PSQI and MEDAS) changed differently when comparing TAU to the intervention group. Specifically, regarding IPAQ–SF–Walking, there was a significant increase in the TAU+LMP+ICTs group (TAU+LMP+ICTs vs. TAU slope difference: b = 99.778, 95% CI= [30.530, 169.026], p = 0.005) (Supplementary Table 1). That increase in IPAQ-SF-Walking implies a small effect size in the TAU+LMP+ICTs group (d = 0.310). Regarding IPAQ-SF-Sedentarism, there were no significant changes in any group (Supplementary Table 2). Regarding PSQI, there was a significant reduction in the TAU+LMP group (TAU+LMP vs. TAU slope difference: b = −1.240, 95% CI= [−2.126, −0.354], p = 0.006) (Supplementary Table 3). That decrease in PSQI implies a small effect size in the TAU+LMP group (d = 0.268). Finally, regarding MEDAS, there was a significant increase in the TAU+LMP+ICTs group (TAU+LMP+ICTs vs. TAU slope difference: b = 0.702, 95% CI= [.337, 1.066], p < 0.001) (Supplementary Table 4). That increase in MEDAS implies a small effect size in the TAU+LMP+ICTs group (d = 0.040).
Discussion
The findings of this study indicate that over 6 months, TAU+LMPs were effective in decreasing depressive symptoms. Also, TAU+LMPs helped in the adoption of several healthier lifestyle behaviors when compared to TAU.
The findings of this study are consistent with other Spanish RCTs on psychoeducational group interventions delivered by PHC nurses for people with depression and physical comorbidity (40, 41). Furthermore, they are also consistent with a multidisciplinary online programmes that integrates evidence-based tactics from the fields of lifestyle medicine (42), as well as with a recent pilot RCT about a group-based lifestyle medicine for depression (43).
Recent meta-analyses of RCTs concluded that multi-component LMPs (with three lifestyle factors such as physical activity, nutritional advice, and sleep management) appeared to be effective in mitigating depressive symptoms (44, 45). A recent Spanish longitudinal cohort study (46), a cross-sectional study about health conditions, lifestyle factors and depression (47) and a recent meta-analysis of observational studies (48) have all shown that healthy lifestyles are associated with a reduced risk of depressive symptoms.
Regarding changes on lifestyle, reflecting a long-lasting effect of the interventions, people receiving the TAU+LMP+ICTs group significantly increased their total weekly minutes of walking (approximately, 1 h and three quarters) when compared to TAU. Participants following the TAU+LMP also increased their minutes of walking (approximately 1 h), but those results only showed a certain trend toward significance. A systematic review and a meta-analysis analyzing RCTs about the treatment effect of exercise on depression (49, 50) concluded that physical exercise is an effective intervention for depression. Moreover, evidence suggests that it is not only necessary to be physically active but also to limit the number of hours spent being sedentary (51). In the same line, in a cross-sectional study with primary care patients, depression symptoms were associated with physical inactivity (52). Participants from the TAU+LMP+ICTs group reduced their total daily minutes seated (~45 min) almost significantly. This lack of relationship found between sedentary lifestyle and depression may be due to the fact that what the participants did while sitting was not controlled. Therefore, time spent being sedentary could have been used doing pleasant leisure activities (i.e., watching TV, reading or using the computer) (53).
An RCT associated physical activity with elevated mood and with a significant reduction in the severity of insomnia symptoms (54). In our study, there was a significant reduction in bad sleep quality among the participants from the TAU+LMP. In a recent cross-sectional study, inadequate sleep was associated with most health disabilities and major depression (55). Furthermore, a meta-analysis concluded that a lack of good sleep quality is significantly associated with depression in older adults (56), and another meta-analysis stated that certain sleep disorders (nightmares and insomnia) increase the risk of suicidal behavior in depressed patients (57).
A recent cross-sectional study observed positive associations between a healthy diet and sleep with mental health (58). Participants from the TAU+LMP+ICTs group significantly increased their adherence to the Mediterranean diet. A recent RCT determined that adherence to the Mediterranean diet was related to fewer depressive symptoms (59). A meta-analysis of RCTs determined that dietary interventions significantly reduced depressive symptoms (60). Moreover, meta-analyses of observational studies indicated that adults following a healthy dietary pattern have fewer depressive symptoms and a lower risk of developing depressive symptoms (61). In particular, adhering to the Mediterranean diet appeared to reduce the risk of depression (62).
The differences found between both interventions (TAU+LMP and TAU+LMP+ICTs) could be due to the use of the wearable smartwatch for monitoring. We have found the following advantages of its use. Firstly, the patients from the TAU+LMP+ICTs group had a more remarkable reduction in their depression and, as previously stated, this reduction of depression might be clinically relevant. Secondly, these patients had significantly increased the minutes of walking per week and they also increased their adherence to the Mediterranean diet. However, participants from this group did not have a significant improvement in their sleep quality, whereas the participants from the TAU+LMP improved their sleep. These results may have been influenced by the individual use of the smartwatch. Most of the patients from the TAU+LMP+ICTs group were very excited about using this device, however, most of them did not wear it during the night. As such, feedback about their sleep was not available. This underuse of the smartwatch could have been due to the patients' acceptance of technologies (63).
Regarding the limitations and strengths of the study, the first strength was the study's design; a pragmatic RCT with sample homogeneity between groups. As the study was developed in primary care conditions, the research results are easily transferable to practice. Another advantage is that since the randomization was blind, the evaluations and the statistical analysis provided greater validity to the results. Furthermore, and as a new characteristic, numerous aspects of healthy lifestyles were considered together and no adverse effects from the interventions were reported. In this regard, the group intervention format offered social support, a sense of belonging and the opportunity to share common difficulties (64). Finally, the participant profile was similar to regular PHC patients.
One limitation was the overlap with COVID-19 since participants found it difficult to properly implement the lifestyle guidelines during this time (65). Despite session attendance being high (5 out of the 6 sessions), another issue was the dropout rate, which was mostly due to time incompatibility or a lack of interest in answering the questionnaires during the follow-up. Furthermore, the sample was predominantly female and, as such, no analysis by gender could be performed. Finally, due to the nature of the intervention, both the psychologist who led the sessions and the participants were aware of the assigned intervention during the RCT.
Future trials with larger sample sizes could plan for subgroup analyses. For example, analyzing the effectiveness of an TAU+LMP for the different severities of depression (i.e., subclinical, mild, moderate and even severe). Moreover, recruiting more men may be beneficial to be able to make gender comparisons. Furthermore, adherence strategies (i.e., sending text messages) (66) may be considered in future RCTs. In addition, qualitative studies should be carried out to investigate the specific causes of dropout. Regarding the use of ICTs, more studies are needed to determine how to improve adherence and compliance rates so that people can wear wearable devices continuously for 24 h (20).
Conclusion
TAU+LMPs administered in PHCs to people suffering from mainly moderate depression were effective in reducing depressive symptomatology comparing to TAU. The use of ICTs resulted in a greater improvement in depression and in several lifestyle factors (weekly minutes of walking and adherence to the Mediterranean diet). More research is needed to enhance adherence. These promising programmes could be easily implemented in PHCs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Research Ethics Committee of Aragón (CEICA, PI18/286). The patients/participants provided their written informed consent to participate in this study.
Author contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas, took part in drafting, revising or critically reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Funding
This work was supported by Carlos III Health Institute grant number PI18/01336. The funders have no role in study design, data collection and analysis, decision to publish or manuscript preparation. The funding organization will audit trial conduct once a year.
Acknowledgments
We wish to thank the Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS, RD21/0016/0005) that is part of the Results-Oriented Cooperative Research Networks in Health (RICORS) (Carlos III Health Institute), the Primary Health Care Research Group of Aragon (GAIAP – B21-20R) of the Department of Science, University and Knowledge Society of the government of Aragon (Spain) and Feder Funds “Another way to make Europe”. This research has been developed during a short-research term of A-AL at Lancaster University supported by Campus de Excelencia Internacional del Valle del Ebro (Campus Iberus), “Convenio de subvención Erasmus+ Educación Superior para prácticas Consorcio Iberus+”, and Universidad de Zaragoza, Fundación Bancaria Ibercaja y Fundación CAI “Programa Ibercaja-CAI de Estancias de Investigación”, grant number CM 9/21.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.954644/full#supplementary-material
References
1. World Health Organization (WHO). Depression. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/depression
3. Aguilera-Martín Á, Gálvez-Lara M, Cuadrado F, Moreno E, García-Torres F, Venceslá JF, et al. Cost-effectiveness and cost-utility evaluation of individual vs. group transdiagnostic psychological treatment for emotional disorders in primary care (PsicAP-Costs): a multicentre randomized controlled trial protocol. BMC Psychiatry. (2022) 22, 1–15. doi: 10.1186/s12888-022-03726-4
4. WHO. International Statistical Classification of Diseases and Related Health Problems, 10th Revision ICD-10: Tabular List. Geneva: World Health Organization (2016).
5. Malhi GS, Outhred T, Hamilton A, Boyce PM, Bryant R, Fitzgerald PB, et al. Royal australian and New Zealand college of psychiatrists clinical practice guidelines for mood disorders: Major depression summary. Medical J Australia. (2018) 208:175–80. doi: 10.5694/mja18.00351
6. Aguilar-Latorre A, Serrano-Ripoll MJ, Oliván-Blázquez B, Gervilla E, Navarro C. Associations between severity of depression, lifestyle patterns, and personal factors related to health behavior: secondary data analysis from a randomized controlled trial. Front Psychol. (2022) 13. doi: 10.3389/fpsyg.2022.856139
7. Forsyth A, Deane FP, Williams P. A lifestyle intervention for primary care patients with depression and anxiety : a randomised controlled trial. Psychiatry Res. (2015) 1–8. doi: 10.1016/j.psychres.2015.10.001
8. García-Toro M, Ibarra O, Gili M, Serrano MJ, Oliván B, Vicens E, et al. Four hygienic-dietary recommendations as add-on treatment in depression A randomized-controlled trial. J Affect Disord. (2012) 140:200–3. doi: 10.1016/j.jad.2012.03.031
9. Lopresti AL, Hood SD, Drummond PD. A review of lifestyle factors that contribute to important pathways associated with major depression: Diet, sleep and exercise. J Affect Disord. (2013) 148:12–27. doi: 10.1016/j.jad.2013.01.014
10. Harvey SB, Overland S, Hatch SL, Wessely S, Mykletun A, Hotopf M. Exercise and the prevention of depression: results of the HUNT cohort study. Am J Psychiatry. (2018) 175. doi: 10.1176/appi.ajp.2017.16111223
11. Lin CY, Kim B, Liao Y, Park JH. Personal, behavioral, and perceived environmental factors associated with late-life depression in older men and women. Psychol Res Behav Manag. (2019) 12:641–50. doi: 10.2147/PRBM.S214524
12. Asarnow LD, Soehner AM, Harvey AG. Basic sleep and circadian science as building blocks for behavioral interventions: a translational approach for mood disorders. Behav Neurosci. (2014) 128:360–70. doi: 10.1037/a0035892
13. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. (2019) 23:2324–32. doi: 10.1111/jcmm.14170
14. González-García S, Green RF, Scheelbeek PF, Harris F, Dangour AD. Dietary recommendations in Spain –affordability and environmental sustainability? J Clean Prod. (2020) 254. doi: 10.1016/j.jclepro.2020.120125
15. Pano O, Martínez-Lapiscina EH, Sayón-Orea C, Martinez-Gonzalez MA, Martinez JA, Sanchez-Villegas A. Healthy diet, depression and quality of life: A narrative review of biological mechanisms and primary prevention opportunities. World J Psychiatry. (2021) 11:997–1016. doi: 10.5498/wjp.v11.i11.997
16. NICE. Behaviour Change: Individual Approaches. (2014). Avavilable onlilne at: www.nice.org.uk/guidance/ph49 (accessed December 1, 2021).
17. Olivan-Blázquez B, Montero-Marin J, García-Toro M, Vicens-Pons E, Serrano-Ripoll MJ, Castro-Gracia A, et al. Facilitators and barriers to modifying dietary and hygiene behaviours as adjuvant treatment in patients with depression in primary care: A qualitative study. BMC Psychiatry. (2018) 18:1–12. doi: 10.1186/s12888-018-1779-7
18. Serrano-Ripoll MJ, Oliván-Blázquez B, Vicens-Pons E, Roca M, Gili M, Leiva A, et al. Lifestyle change recommendations in major depression: Do they work? J Affect Disord. (2015) 183. doi: 10.1016/j.jad.2015.04.059
19. Naslund JA, Aschbrenner KA, Barre LK, Bartels SJ. Feasibility of popular m-health technologies for activity tracking among individuals with serious mental Illness. Telemed E-Health. (2015) 21:213–6. doi: 10.1089/tmj.2014.0105
20. Lee S, Kim H, Park MJ, Jeon HJ. Current advances in wearable devices and their sensors in patients with depression. Front Psychiat. (2021) 12:1–8. doi: 10.3389/fpsyt.2021.672347
21. Beck A, Steer R, Ball R, Ranieri W. Comparison of beck depression 1 in psychiatric inventories−1a and - outpatients. J Pers Assess. (1996) 67:588–97. doi: 10.1207/s15327752jpa6703_13
22. Button K, Kounali D, Thomas L, Wiles N, Peters T, Welton N, et al. Minimal clinically important difference on the Beck Depression Inventory - II according to the patient's perspective. Psychol Med. (2015) 45:3269–79. doi: 10.1017/S0033291715001270
23. Aguilar-Latorre A, Navarro C, Oliván-Blázquez B, Gervilla E, Magallón Botaya R, Calafat-Villalonga C, et al. Effectiveness and cost-effectiveness of a lifestyle modification programme in the prevention and treatment of subclinical, mild and moderate depression in primary care: a randomised clinical trial protocol. BMJ Open. (2020) 10. doi: 10.1136/bmjopen-2020-038457
24. Kim J, Shin W. How to do random allocation (randomization). Clin Orthop Surg. (2014) 6:103–9. doi: 10.4055/cios.2014.6.1.103
25. Cuijpers P, Quero S, Papola D, Cristea IA, Karyotaki E. Care-as-usual control groups across different settings in randomized trials on psychotherapy for adult depression: a meta-analysis. Psychol Med. (2019) 51:634–44. doi: 10.1017/S0033291719003581
26. Ministry of Health Social Services Equality. (2014). Clinical Practice Guideline on the Management of Major Depression in Adults. SNS Clinical Practice Guidelines. Available online at: http://www.guideline.gov/content.aspx?id=24067&search=depression
27. Calderón-Larrañaga A, Vetrano DL, Onder G, Gimeno-Feliu LA, Coscollar-Santaliestra C, Carfí A, et al. Assessing and measuring chronic multimorbidity in the older population: a proposal for its operationalization. J Gerontol. (2017) 72:1417–23. doi: 10.1093/gerona/glw233
28. Sanz J, García-Vera MP, Espinosa R, Fortún M, Vázquez C, Obreg R, et al. Spanish adaptation of the Beck Depression Inventory-II (BDI-II): 3. Psychometric features in patiens with psychological disorders. Clínica y Salud. (2005) 16:121–42.
29. Kim Y, Park I, Kang M. Convergent validity of the International Physical Activity Questionnaire (IPAQ): meta-analysis. In Public Health Nutrition. (2013). doi: 10.1017/S1368980012002996
30. Roman-Viñas B, Serra-Majem L, Hagströmer M, Ribas-Barba L, Sjöström M, Segura-Cardona R. International physical activity questionnaire: Reliability and validity in a Spanish population. Eur J Sport Sci. (2010) 10:297–304. doi: 10.1080/17461390903426667
31. Martínez-González MÁ, Corella D, Salas-Salvadó J, Ros E, Covas MI, Fiol M, et al. Cohort profile: design and methods of the PREDIMED study. Int J Epidemiol. (2010) 41:377–385. doi: 10.1093/ije/dyq250
32. Schröder H, Fitó M, Estruch R, Martínez-González MA, Corella D, Salas-Salvadó J, et al. A short screener is valid for assessing mediterranean diet adherence among older Spanish men and women. J Nutrit. (2011) 141:1140–5. doi: 10.3945/jn.110.135566
33. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. (1989). doi: 10.1037/t05178-000
34. Royuela-Rico A, Macías-Fernández JA. Propiedades clinimétricas de la versión castellana del Cuestionario de Pittsburgh. Vigilia-Sueño. (1997) 9:81–94.
35. Singer JD, Willett JB. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence. Oxford: Oxford University Press (2003).
36. Mcgough JJ, Faraone SV. Estimating the size of treatment effects: moving beyond p values. Psychiatry. (2009) 6:21–9.
37. McCoy CE. Understanding the intention-to-treat principle in randomized controlled trials. West J Emerg Med. (2017) 18:1075–8. doi: 10.5811/westjem.2017.8.35985
38. Haynes W. Bonferroni Correction. In Dubitzky W, Wolkenhauer O, Cho K-H, Yokota H, editors. Encyclopedia of Systems Biology. New York: Springer. (2013). doi: 10.1007/978-1-4419-9863-7_1213
40. Casañas R, Catalán R, Raya A, Real J. Efectividad de un programa grupal psicoeducativo para la depresión mayor en atención primaria: ensayo clínico controlado aleatorizado. Revista de La Asociación Española de Neuropsiquiatría. (2014) 34:145–6. doi: 10.4321/S0211-57352014000100009
41. Raya-Tena A, Fernández-San-martin MI, Martin-Royo J, Casañas R, Sauch-Valmaña G, Cols-Sagarra C, et al. Effectiveness of a psychoeducational group intervention carried out by nurses for patients with depression and physical comorbidity in primary care: Randomized clinical trial. Int J Environ Res Public Health. (2021) 18:1–17. doi: 10.3390/ijerph18062948
42. Przybylko G, Morton D, Kent L, Morton J, Hinze J, Beamish P, et al. The effectiveness of an online interdisciplinary intervention for mental health promotion: a randomized controlled trial. BMC Psychology. (2021) 9:1–11. doi: 10.1186/s40359-021-00577-8
43. Ka-Yan Ip A, Yan-Yee Ho F, Yeung W-F, Chung K-F, Ng CH, Oliver G, et al. Effects of a group-based lifestyle medicine for depression: A pilot randomized controlled trial. PLoS ONE. (2021) 16:e0258059. doi: 10.1371/journal.pone.0258059
44. Gómez-Gómez I, Bellón J, Resurrección DM, Cuijpers P, Moreno-Peral P, Rigabert A, et al. Effectiveness of universal multiple-risk lifestyle interventions in reducing depressive symptoms: systematic review and meta-analysis. Preventive Med. (2020) 134:106067. doi: 10.1016/j.ypmed.2020.106067
45. Wong VWH, Ho FYY, Shi NK, Sarris J, Chung KF, Yeung WF. Lifestyle medicine for depression: a meta-analysis of randomized controlled trials. J Affect Disord. (2021) 284:203–16. doi: 10.1016/j.jad.2021.02.012
46. Ruiz-Estigarribia L, Martínez-González MÁ, Díaz-Gutiérrez J, Sánchez-Villegas A, Lahortiga-Ramos F, Bes-Rastrollo M. Lifestyles the risk of depression in the “Seguimiento Universidad de Navarra” cohort. European Psychiatry. (2019) 61:33–40. doi: 10.1016/j.eurpsy.2019.06.002
47. Cui N, Cui J, Xu X, Aslam B, Bai L, Li D, et al. Health conditions, lifestyle factors and depression in adults in qingdao, china: a cross-sectional study. Front Psychiat. 12(May). (2021) 1–9. doi: 10.3389/fpsyt.2021.508810
48. Wang X, Arafa A, Liu K, Eshak ES, Hu Y, Dong JY. Combined healthy lifestyle and depressive symptoms: a meta-analysis of observational studies. J Affect Disord. (2021) 289:144–50. doi: 10.1016/j.jad.2021.04.030
49. Kvam S, Lykkedrang C, Hilde I, Hovland A. Exercise as a treatment for depression: A meta-analysis. J Affect Disord. (2016) 202:67–86. doi: 10.1016/j.jad.2016.03.063
50. Stanton R Reaburn Exercise P and and the treatment of depression: A review of the exercise program variables. J Sci Med Sport. (2014) 17:177–82. doi: 10.1016/j.jsams.2013.03.010
51. De Rezende LFM, Rey-López JP, Matsudo VKR, Luiz ODC. Sedentary behavior and health outcomes among older adults: a systematic review. BMC Public Health. (2014) 14:1–9. doi: 10.1186/1471-2458-14-333
52. Achttien R, Van Lieshout J, Wensing M, Van Der Sanden MN, Staal JB. Symptoms of depression are associated with physical inactivity but not modified by gender or the presence of a cardiovascular disease; a cross-sectional study. BMC Cardiovasc Disord. (2019) 19:1–7. doi: 10.1186/s12872-019-1065-8
53. Andrade-Gómez E, García-Esquinas E, Martínez-Gómez D, Rodríguez-Artalejo F. Sedentary behaviors, physical activity, and changes in depression and psychological distress symptoms in older adults. Depress Anxiety. (2018) 35:884–97. doi: 10.1002/da.22804
54. Hartescu I, Morgan K, Stevinson CD. Increased physical activity improves sleep and mood outcomes in inactive people with insomnia: a randomized controlled trial. J Sleep Res. (2015) 24:526–34. doi: 10.1111/jsr.12297
55. Kim Y-J, Lee S-A. The relationship of lifestyle factors with the prevalence of major depressive disorder by ecological factors. Psychiatry Investig. (2021) 18:340–7. doi: 10.30773/pi.2020.0309
56. Becker NB, Jesus SN, João KADR, Viseu JN, Martins S. RIDepression sleep quality in older adults: a meta-analysis. Psychology, Health and Medicine. (2017) 22:889–95. doi: 10.1080/13548506.2016.1274042
57. Wang X, Cheng S, Xu H. Systematic review and meta-analysis of the relationship between sleep disorders and suicidal behaviour in patients with depression. BMC Psychiatry. (2019) 19:1–13. doi: 10.1186/s12888-019-2302-5
58. Hepsomali P, Groeger JA. Diet sleep, and mental health: insights from the uk biobank study. Nutrients. (2021) 13:2573. doi: 10.3390/nu13082573
59. Picard K, Senior PA, Adame Perez S, Jindal K, Richard C, Mager DR. Low Mediterranean Diet scores are associated with reduced kidney function and health related quality of life but not other markers of cardiovascular risk in adults with diabetes and chronic kidney disease. Nutr Metab Cardiovasc Dis. (2021) 31:1445–53. doi: 10.1016/j.numecd.2021.02.002
60. Firth J, Marx W, Dash S, Carney R, Teasdale SB, Solmi M, et al. The effects of dietary improvement on symptoms of depression and anxiety: a meta-analysis of randomized controlled trials. Psychosom Med. (2019) 81:265–80. doi: 10.1097/PSY.0000000000000673
61. Nicolaou M, Colpo M, Vermeulen E, Elstgeest LEM, Cabout M, Gibson-Smith D, et al. Association of a priori dietary patterns with depressive symptoms: A harmonised meta-analysis of observational studies. Psychol Med. (2019) 50:1872–83. doi: 10.1017/S0033291719001958
62. Lassale C, Batty GD, Baghdadli A, Jacka F, Sánchez-Villegas A, Kivimäki M, et al. Healthy dietary indices and risk of depressive outcomes: a systematic review and meta-analysis of observational studies. Mol Psychiatry. (2019) 24:965–86. doi: 10.1038/s41380-018-0237-8
63. Kim J, Park HA. Development of a health information technology acceptance model using consumers' health behavior intention. J Med Internet Res. (2012) 14:1–14. doi: 10.2196/jmir.2143
64. Guimón J. Manual de Terapias de Grupo. Tipos, Modelos y Programas. Madrid: Editorial Biblioteca Nueva (2003).
65. Aguilar-Latorre A, Oliván-Blázquez B, Porroche-Escudero A, Méndez-López F, García-Gallego V, Benedé-Azagra B, et al. The impact of the COVID-19 lockdown on depression sufferers: a qualitative study from the province of Zaragoza, Spain. BMC Public Health. (2022) 22:1–13. doi: 10.1186/s12889-022-13083-2
Keywords: depression, lifestyle modification, primary care, randomized controlled trial (RCT), health promotion
Citation: Aguilar-Latorre A, Pérez Algorta G, Navarro-Guzmán C, Serrano-Ripoll MJ and Oliván-Blázquez B (2022) Effectiveness of a lifestyle modification programme in the treatment of depression symptoms in primary care. Front. Med. 9:954644. doi: 10.3389/fmed.2022.954644
Received: 27 May 2022; Accepted: 07 July 2022;
Published: 26 July 2022.
Edited by:
Hans Olav Thulesius, Linnaeus University, SwedenReviewed by:
Harm Van Marwijk, Brighton and Sussex Medical School, United KingdomLiang-Yu Chen, Taipei Veterans General Hospital, Taiwan
Copyright © 2022 Aguilar-Latorre, Pérez Algorta, Navarro-Guzmán, Serrano-Ripoll and Oliván-Blázquez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María J. Serrano-Ripoll, bWFyaWFqZXN1cy5zZXJyYW5vcmlwb2xsJiN4MDAwNDA7aWJzYWx1dC5lcw==