
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 01 August 2022
Sec. Nuclear Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.950717
This article is part of the Research Topic Sentinel Lymph Node Mapping: Current Applications and Future Perspectives View all 8 articles
 Saeideh Ataei Nakhaei1Sayyed Mostafa Mostafavi2Marjaneh Farazestanian3
Saeideh Ataei Nakhaei1Sayyed Mostafa Mostafavi2Marjaneh Farazestanian3 Malihe Hassanzadeh3
Malihe Hassanzadeh3 Ramin Sadeghi1*
Ramin Sadeghi1*Purpose of the report: Since the presence of lymph node metastases upstages the disease and to reduce the morbidity of total lymphadenectomy, sentinel lymph node (SLN) mapping in ovarian mass has been the focus of extensive research. This study aims to review all the literature associated with ovarian SLN mapping and assess the feasibility of ovarian SLN mapping.
Materials and methods: PubMed and Scopus were searched using the following keywords: (Sentinel lymph node) AND (Ovary OR Ovarian) AND (Tumor OR Neoplasm OR Cancer). All studies with information regarding sentinel node biopsy in ovaries were included. Different information including mapping material, injection sites, etc., was extracted from each study. In total, two indices were calculated for included studies: detection rate and false-negative rate. Meta-analysis was conducted using Meta-MUMS software. Pooled detection rate, sensitivity, heterogeneity, and publication bias were evaluated. Quality of the studies was evaluated using the Oxford center for evidence-based medicine checklist.
Results: Overall, the systematic review included 14 studies. Ovarian SLN detection rate can vary depending on the type of tracer, site of injection, etc., which signifies an overall pooled detection rate of 86% [95% CI: 75–93]. The forest plot of detection rate pooling is provided (Cochrane Q-value = 31.57, p = 0.003; I2 = 58.8%). Trim and fill method resulted in trimming of 7 studies, which decreased the pooled detection rate to 79.1% [95% CI: 67.1–87.5]. Overall, pooled sensitivity was 91% [59–100] (Cochrane Q-value = 3.93; p = 0.41; I2 = 0%). The proportion of lymph node positive patients was 0–25% in these studies with overall 14.28%.
Conclusion: Sentinel lymph node mapping in ovarian tumors is feasible and seems to have high sensitivity for detection of lymph node involvement in ovarian malignant tumors. Mapping material, injection site, and previous ovarian surgery were associated with successful mapping. Larger studies are needed to better evaluate the sensitivity of this procedure in ovarian malignancies.
Ovarian cancer is one of the leading causes of gynecological cancer-related mortalities. This is primarily due to the fact that 75% of cases are diagnosed in advanced stages of the disease. However, up to one-third of patients with ovarian cancer are diagnosed in early stages of the disease (1). Because of missing involved lymph nodes during lymph node sampling, bilateral pelvic and para-aortic lymphadenectomy is the N-staging recommendation by FIGO in early stage ovarian cancer (2). However, only 14% (3) of these patients have nodal metastasis and would not benefit should routine lymph node dissection be performed. Additionally, systematic lymphadenectomy has a high risk of complications such as longer operative time, longer hospital stay, larger amount of blood loss, and an increased risk of developing lymphoceles or chronic lower limb lymphedema (4–6). Because the occurrence of lymph node metastases increases the severity of the disease (7) and in an attempt to diminish procedure-related morbidity of routine systematic lymphadenectomy, sentinel lymph node (SLN) mapping in ovarian mass has been the focus of extensive research over the past decade. The aim of this study was to systematically review the available series on sentinel lymph node mapping in ovarian mass. This includes a discussion of the feasibility of ovarian SLN mapping and a characterization of these studies.
We searched PubMed and Scopus for relevant articles with following keywords on 6 October 2021:
(Sentinel lymph node) AND (Ovary OR Ovarian) AND (Tumor OR Neoplasm OR Cancer).
A number of two reviewers (SA and RS) jointly examined the retrieved articles by going through the title and abstract sections. All studies with information regarding sentinel node biopsy in ovaries (ovarian tumors or normal ovaries) were included into the systematic review. The reference lists as well as citing articles of included studies were searched for possible missing relevant studies. Citing articles were evaluated using Google Scholar. Case reports (less than 5 patients), review articles, and commentaries were excluded. No language restriction was imposed on our search.
Information on mapping material, injection sites, time from injection to sentinel node mapping, number and location of sentinel nodes, lymphoscintigraphy findings, pathological involvement of the sentinel nodes, and other harvested nodes was extracted from each included study by the same two reviewers. This was done by going through the Methods and Results sections of the studies. A number of two indices were calculated for included studies: Detection rate: number of patients with at least one detected sentinel node/all patients. We also performed a sensitivity analysis for studies which only included ovarian tumors.
False-negative rate: number of patients with pathologically involved non-sentinel node despite non-involved sentinel node/all patients with at least one detected sentinel node.
Meta-analysis was done using Meta-MUMS software (8). Random effects model was used for pooling data across included studies. Forest plots were used for visual presentation of the results. Heterogeneity was evaluated using Cochrane Q-value (p < 0.05 was considered statistically significant) and I2index. Subgroup analysis was used to explore the heterogeneity across studies. Funnel plots and Egger’s regression intercept were used to evaluate possible publication bias.
Quality of the included studies was evaluated by Oxford center for evidence-based medicine checklist for diagnostic studies1. This review was prepared according to PRISMA checklist2.
We identified a total of 14 sentinel lymph node ovarian-related studies (Figure 1). Overall, a total of 234 patients were included in the studies who underwent sentinel lymph node ovarian mapping (Table 1). A total of 162 (69%) patients underwent laparotomy whereas the remaining 31% of patients underwent minimal invasive surgery (laparoscopy). The majority of the patients (81%) had suspicious ovarian mass (121 patients) or early ovarian cancer (69 patients). Other cases of note were other gynecological cancer (29 endometrial cancer, 3 cervical cancer, and 1 fallopian tube tumor) identified for surgery. Ovarian sentinel lymph nodes detection rate can vary depending on the type of tracer, site of injection, etc. Sentinel lymph nodes were found in 199 of 234 patients, which signifies an overall pooled detection rate of 86% [95% CI: 75–93]. Figure 2 shows the forest plot of detection rate pooling (Cochrane Q-value = 31.57, p = 0.003; I2 = 58.8%). Figure 3 shows the funnel plot of the overall detection rate pooling. Trim and fill method after trimming 7 studies decreased the pooled detection rate to 79.1% [95% CI: 67.1–87.5]. Table 2 shows the subgroup analyses of the detection rate pooling according to different variables.
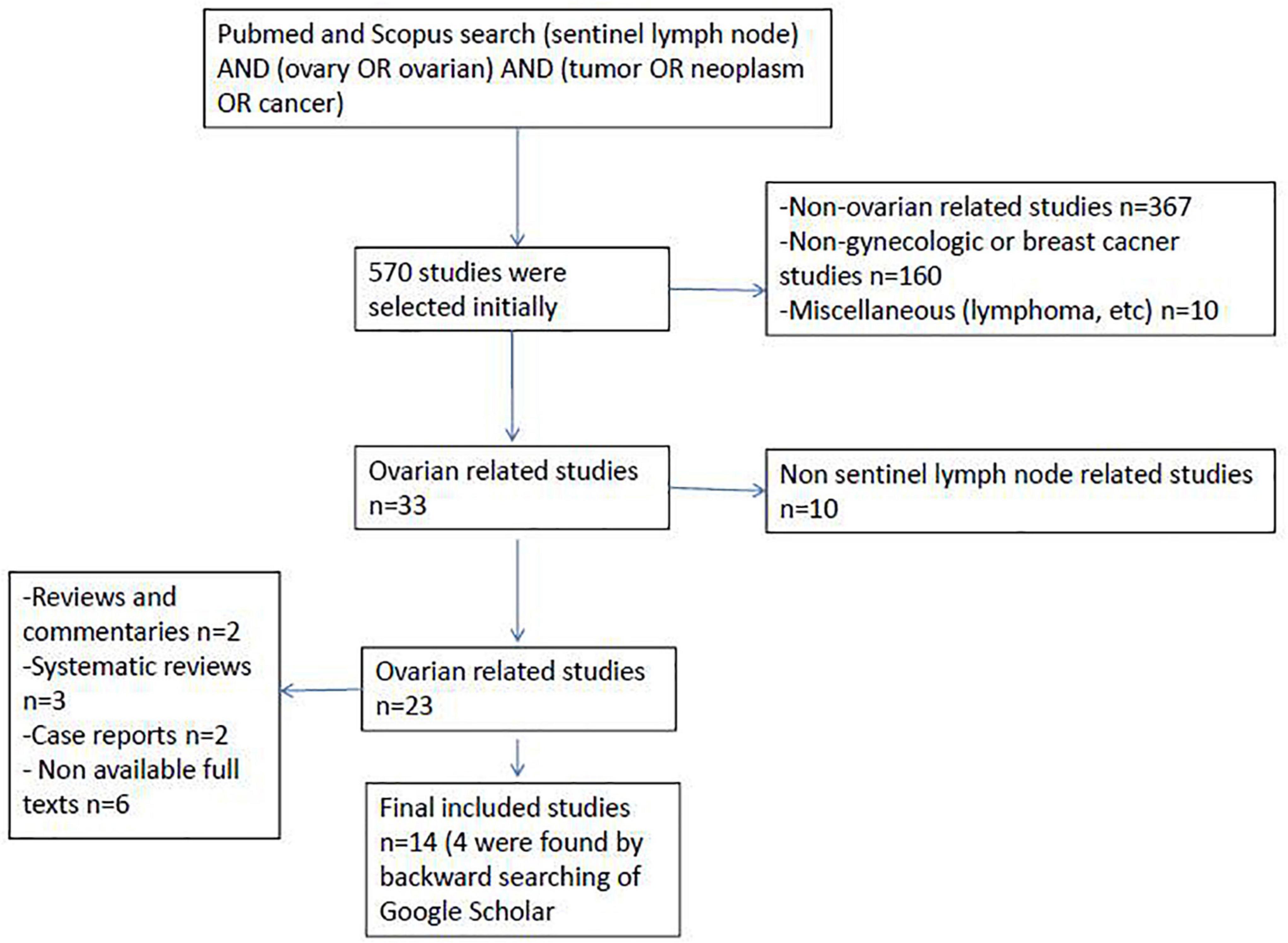
Figure 1. Flow chart of the study selection.
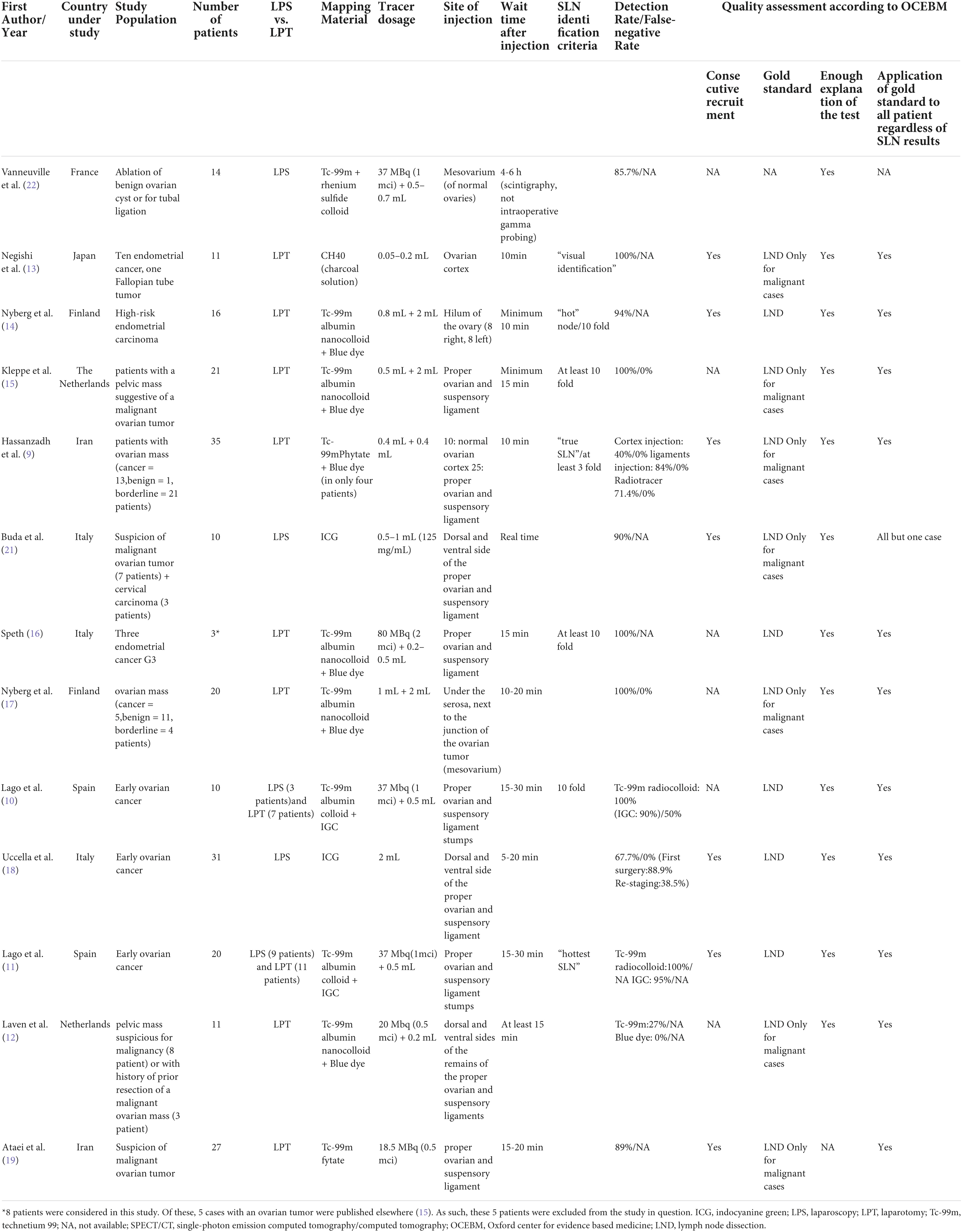
Table 1. Characteristics of the studies (N = 14).
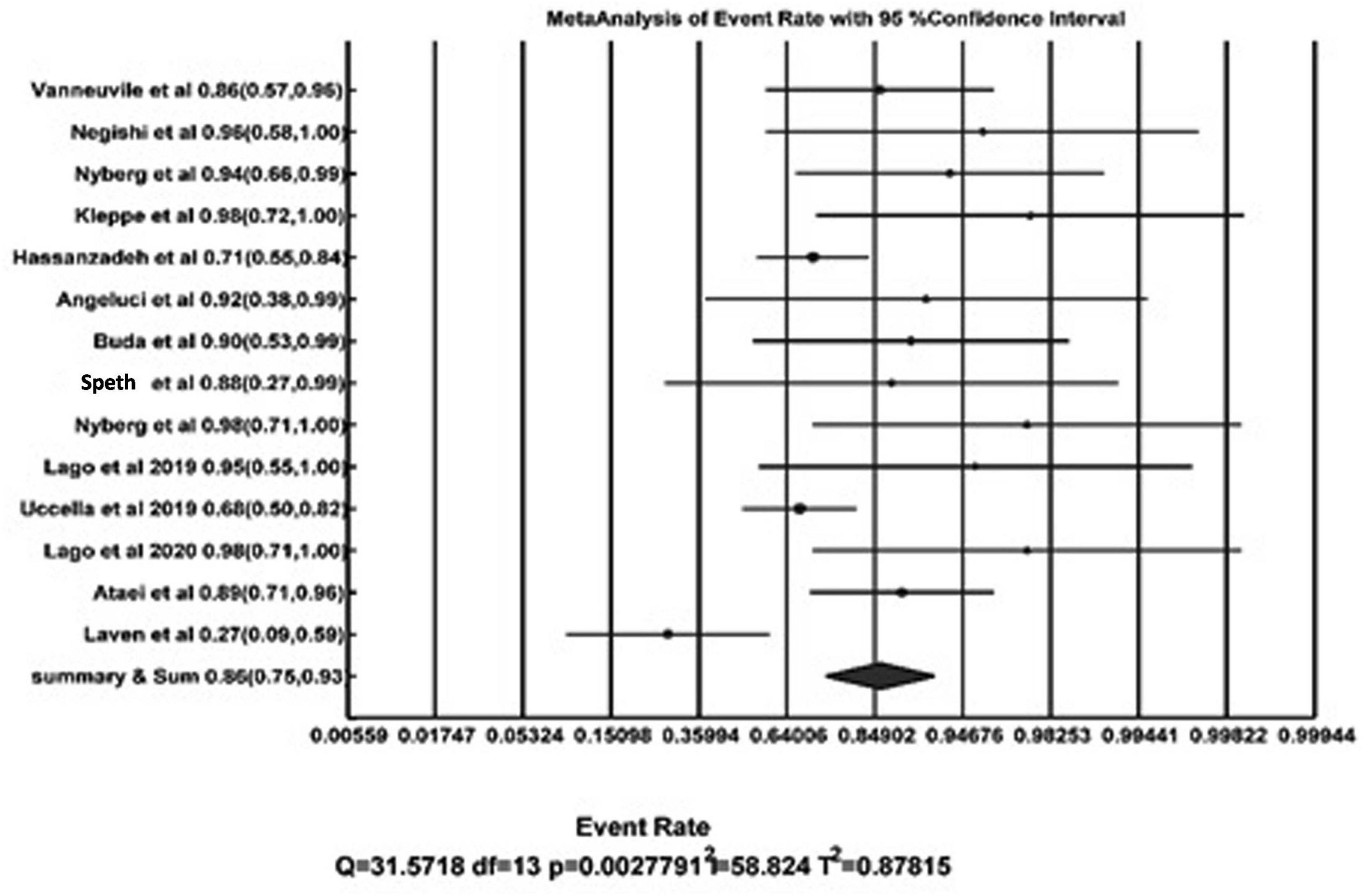
Figure 2. Forest plot of detection rate pooling.

Figure 3. Funnel plot of detection rate pooling using trim and fill method.
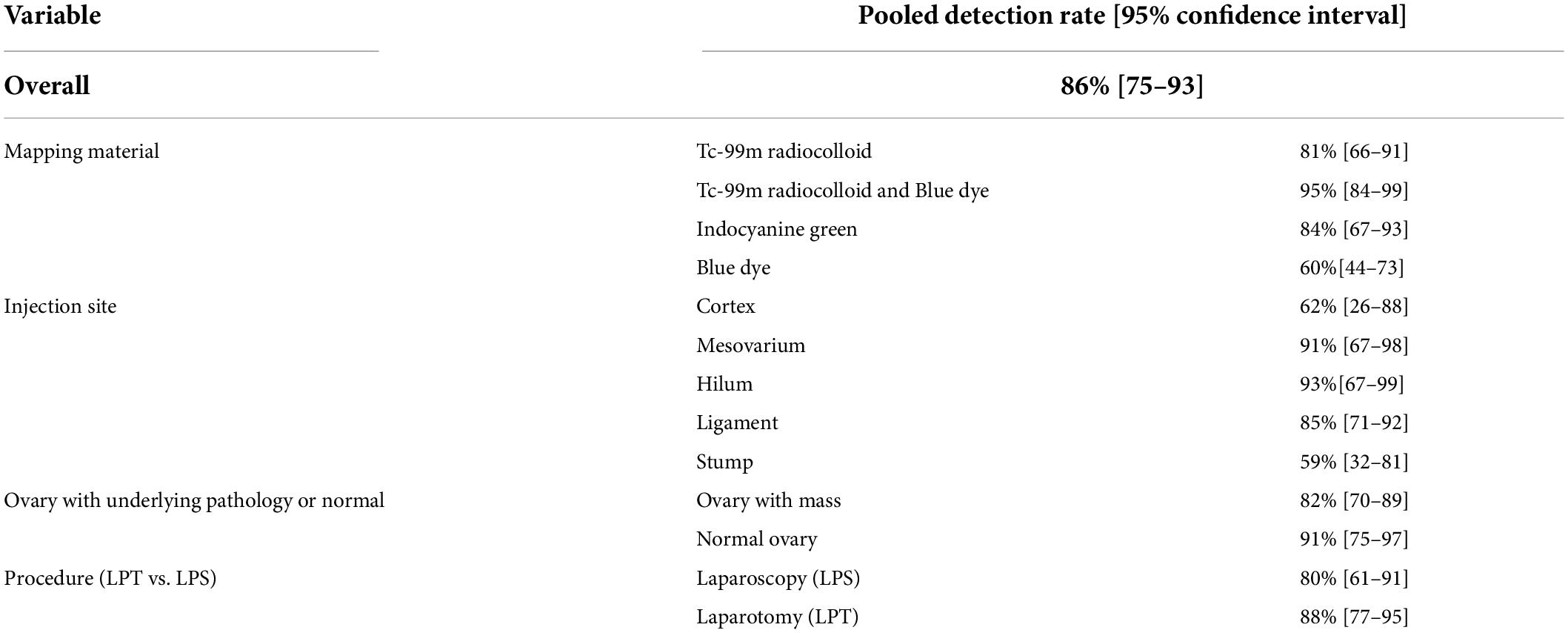
Table 2. Pooled detection rate based on different variables.
Analysis after the exclusion of cases with endometrial carcinoma, cervical carcinoma, and fallopian tube tumors showed pooled DR of 78[95% CI: 60–97].
The most common tracer used in the studies was technetium-99m radiocolloid (Tc-99mradiocolloid). The second most common tracer was a fluorescent tracer named indocyanine green (ICG). Overall, the calculated detection rate, when using Tc-99m radiocolloid only, was 81% [95% CI: 66–91] compared to 84%[95% CI: 67–93] when using indocyanine green (either with Tc-99m radiocolloid or alone), whereas a combination of Tc-99m radiocolloid and Blue dye resulted in a detection rate of 95%[95% CI: 84–99]. However, when Blue dye was considered as the tracer alone, detection rate appeared to be lower compared to other tracers and the detection rate was calculated as 60% [95% CI: 44–73].
Figure 4 shows different tracer injection sites. The most common injection sites in the patients were proper ovarian and suspensory ligaments. These injections were performed on the dorsal and ventral side of the ovarian ligaments, close to the ovary and just underneath the peritoneum. The second most common site was the mesovarium, followed by the hilum of the ovary, and the ovarian cortex. Hassanzadeh et al. (9) selected two sites for injection of Tc-99mPhytate in patients with ovarian mass. Overall, detection rates for the cases where the injection site was just underneath the peritoneum ovarian ligaments, mesovarium, and ovarian hilum were 85 [95% CI: 71–92], 91 [95% CI: 67–98], and 93% [95% CI: 67–99], respectively. These appeared to have higher detection rates as compared to the cases where the injection was into the ovarian cortex (detection rate: 62% [95% CI: 26–88]).
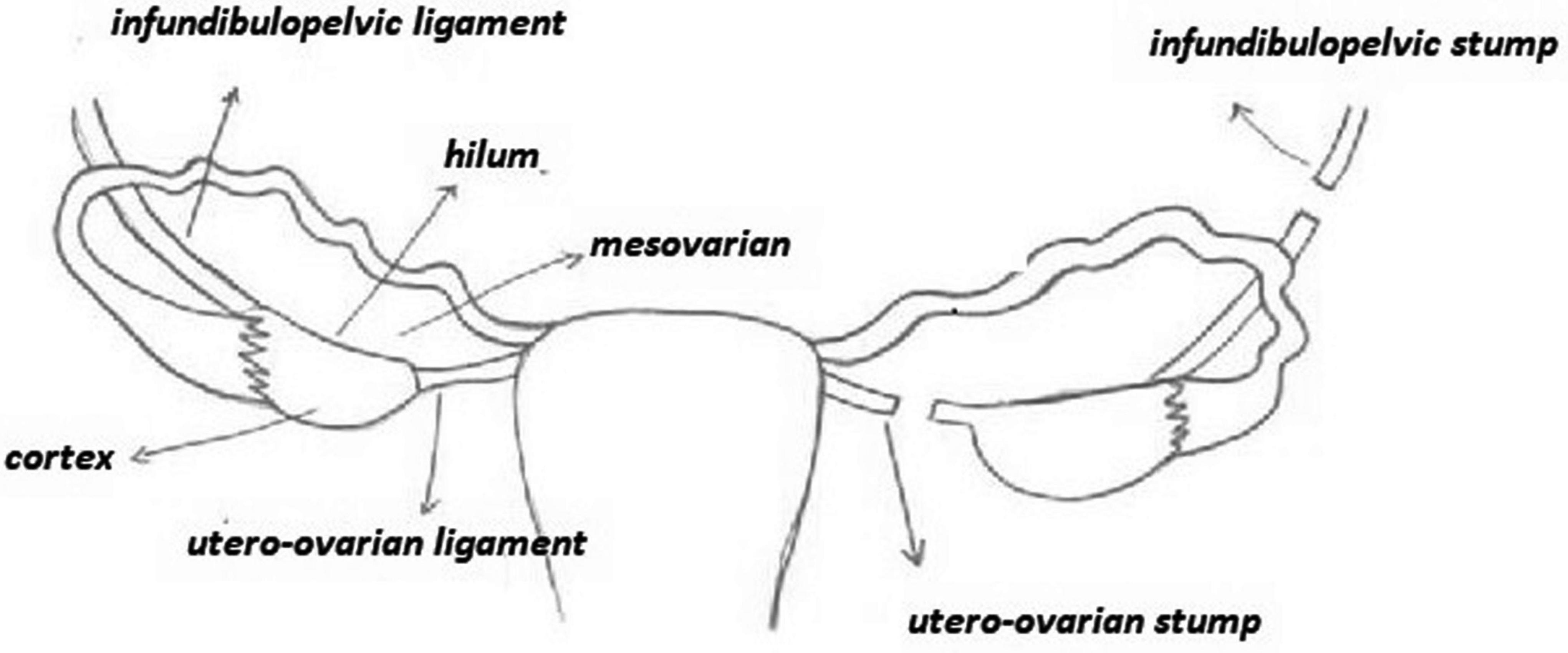
Figure 4. Different sites of tracer injection.
A number of three studies by Lago et al. (10, 11) and Laven et al. (12) considered an overall total of 41 patients with tracer injection after ovarian mass resection during the same or a subsequent surgical procedure. In other words, the patients underwent laparotomy with frozen section for a pelvic mass suspicious for malignancy or a second staging laparotomy after prior resection of a malignant ovarian mass. The injections were performed at the ipsilateral or bilateral infundibulopelvic and utero-ovarian ligament stumps for unilateral or bilateral tumors with no previous hysterectomy, respectively. An injection was performed only at the infundibulopelvic stump if a hysterectomy had been previously performed. SLN detection rates were 100% in the Lago et al.’s studies (10, 11), but the reported detection rate was much lower (27%) by Laven et al. (12). However, overall, pooled detection rate for the cases (with the injection site in the ligament stumps) was 59% [95% CI: 32–81].
There were two groups of patients in the included studies: a group with normal ovary (e.g., cases of endometrial, cervix cancers, or fallopian tube tumor) and another group which included the patients with underlying ovarian pathology (e.g., ovarian mass or early ovarian cancer). We observed that the detection rates were 91 [95% CI: 75–97] and 82% [95% CI: 70–89] in the normal and abnormal ovary groups, respectively.
There were two groups of studies in our systematic review according to the type of surgery (laparotomy vs. laparoscopy). We compared ovarian sentinel lymph node detection rate based on the procedure of surgery, which was calculated as 80[95% CI: 61–91] and 88% [95% CI: 77–95] for laparoscopy and laparotomy, respectively.
The majority of the studies considered 15 min as the median time between tracer injection and sentinel lymph node mapping (visually for Blue dye and by NIR/ICG system and handed gamma probe for ICG and Tc-99m radiocolloid tracer, respectively) (9–19). However, Angelucci et al. (20) considered only 2 min before the start of sentinel lymph node mapping. Also, Buda et al. (21) injected the tracer over the course of laparoscopic surgery and conducted a real-time mapping. However, the last two studies applied ICG as the tracer, which needs less time for lymphatic uptake. In one study (22), there was a reported 4- to 6-h waiting time after injection in lymphoscintigraphy analysis. In the Ataei et al.’s (19) and Speth et al.’s (16) studies, in addition to intraoperative SLN mapping, SPECT/CT lymphoscintigraphy was performed 24 h postsurgery depending on the patients’ conditions.
Table 3 shows location categorization of the ovarian SLNs. Among patients with identified sentinel lymph nodes (N = 189), 55% (N = 104) were located in the para-aortic region only; 11% (N = 21) in the pelvic region only; and 64% (N = 34) in both the para-aortic and pelvic region. In the study of Lago et al. (10), SLN locations were not categorized clearly. As such, we did not include this study in the calculation of sentinel node locations. A number of six studies (13–15, 17, 18, 21) reported the location of sentinel lymph nodes to be above or beneath the inferior mesenteric artery (IMA) level and categorized percent location of sentinel lymph nodes related to each of right or left side’s ovary (Table 3). Of 130 patients with unilateral ovary injection in whom the side location of the sentinel lymph nodes was recorded (11–15, 17, 18, 21, 22), in 109 (84%) patients, sentinel nodes were identified only ipsilaterally, in 14 patients (11%), sentinel nodes were identified only contralaterally, and in 7 patients (5%), sentinel nodes were detected bilaterally. In the study of Speth (16), intraoperative gamma-probing SLN mapping was compared with detection by postoperative SPECT/CT imaging. In 4 patients, one or more hotspots could still be identified at locations where the SNs were resected (3 aortocaval and 2 pelvic). Furthermore, in 6 patients, hotspots were detected in pelvic regions that were not identified during surgery. Also, Ataei et al. (19) detected three aberrant locations of sentinel lymph node.
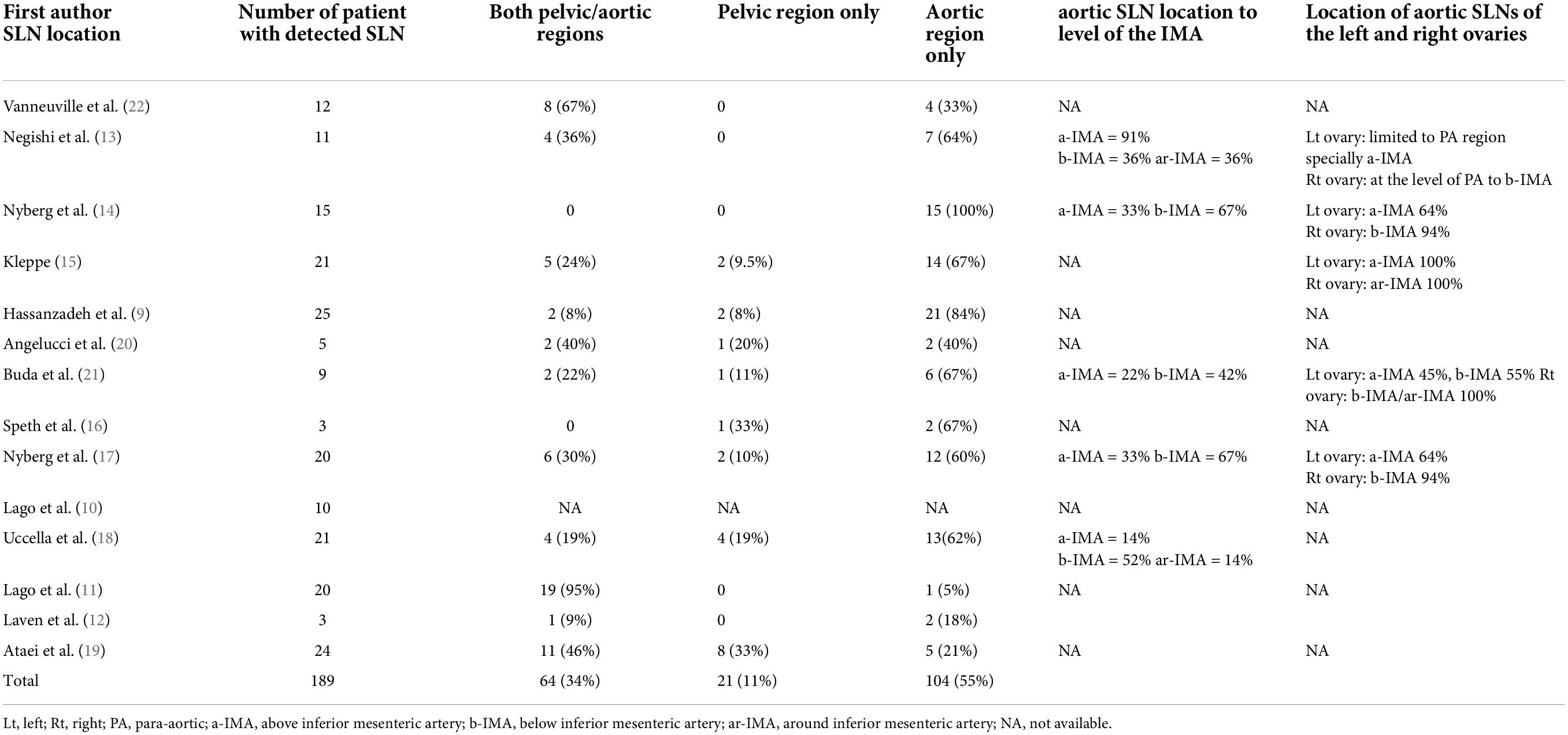
Table 3. Location of the ovarian Sentinal Lymph Nodes.
Only five studies (9, 10, 15, 17, 18) had enough data to calculate the sensitivity of sentinel node mapping in lymphatic staging of ovarian malignancies. The proportion of lymph node-positive patients was 0 to 25% in these studies with overall 14.28%.
Figure 5 shows the forest plot of sensitivity pooling across these studies. Overall, pooled sensitivity was 91% [59–100] (Cochrane Q-value = 3.93; p = 0.41; I2 = 0%).
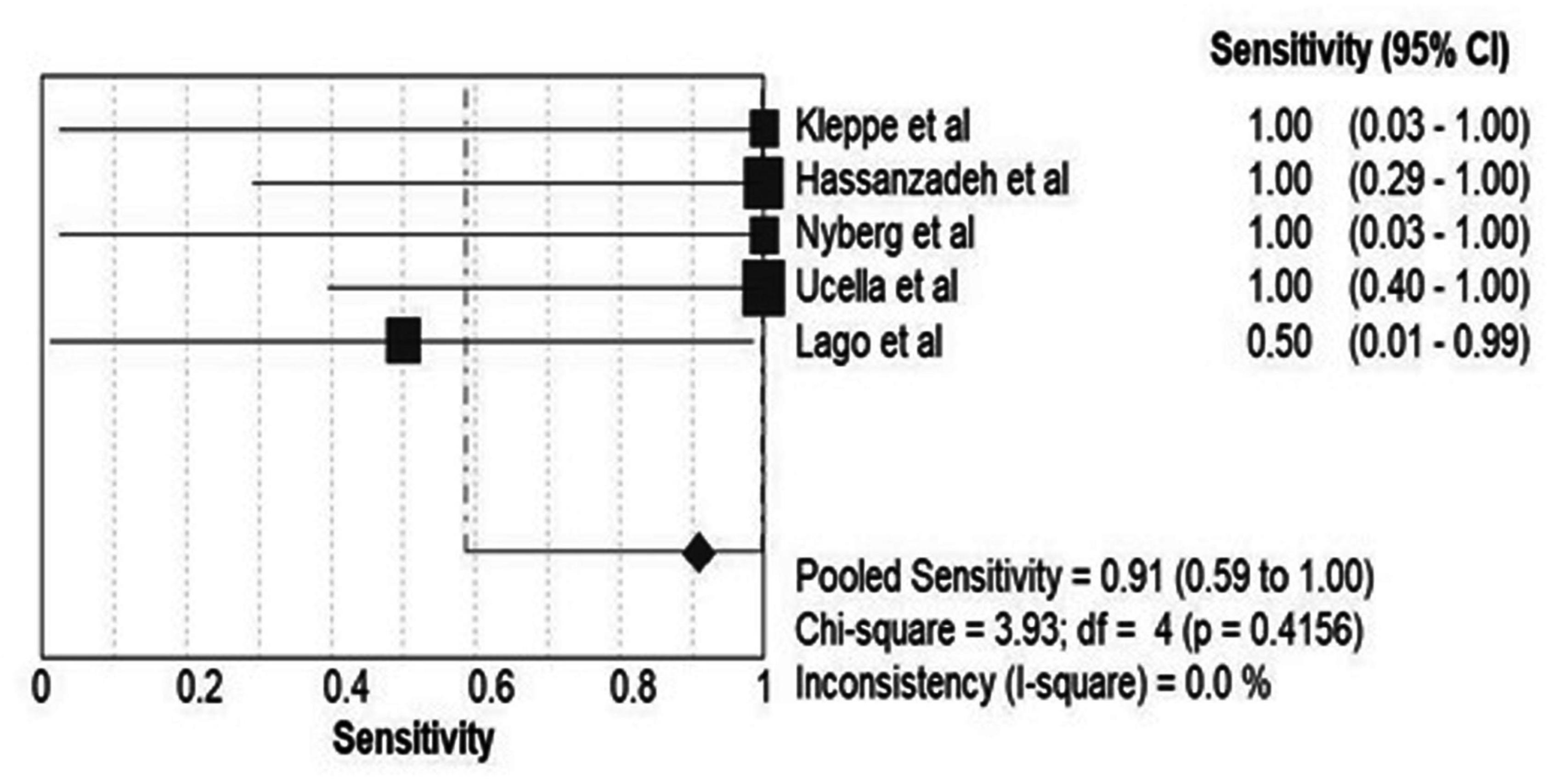
Figure 5. Pooled sensitivity of the included studies for detection of involved nodes.
We conducted a systematic review and meta-analysis of the literature regarding the feasibility of sentinel node mapping and biopsy in ovarian tumors. There have been other reviews on this topic including Uccella et al. (23) and Mach et al. (24). Both studies reported acceptable detection rate and sensitivity for the technique. In addition, both acknowledged that the available evidence is still scarce. We further evaluated the factors that affect the success of sentinel node mapping which we described in the following sections of the discussion.
As mentioned before, the presence of lymph node metastases in early ovarian cancer upstages the disease (7, 10, 18). On the other hand, systemic lymphadenectomy for staging has a high risk of complications (6, 25, 26). Thus, the need for ovarian sentinel lymph node mapping in early ovarian cancer is evidently clear. The present review illustrates that sentinel node mapping of the ovarian masses sounds plausible with an overall detection rate of 86% [95% CI: 75–93] and can vary depending on the type of tracer, site of injection, etc.
As for the type of tracer, detection rate of Blue dye appeared to be lower compared to Tc-99m radiocolloid and indocyanine green. On the other hand, allergic reactions to Blue dye during SLN mapping have been reported in up to 2% of patients (range from urticarial reactions to severe anaphylaxis). In addition, sentinel node mapping using Blue dye seems to be more affected with high BMI as reported by Neyberg et al. (17). In other words, the probability of Blue dye visibility in SLNs with BMI ≥ 27 is lower compared to BMI < 27. One of the advantages of ICG compared to Blue dye is its faster migration to the SLNs as well as better tissue penetration of NIR light compared to normal light. This allows for earlier and deeper detection of the SLNs (27). However, near-infrared fluorescent technology is not available in all centers. Assuming a median net activity of 19 MBq (0.5 mci) per patient, an effective radiation dose equivalent to a chest X-ray (less than 0.1 mSv) is calculated. This implies that the patient is exposed to a small amount of radiation. Alternatively, among three investigated tracers, we observed a maximum SLN detection rate corresponding to the combination of Tc-99m radiocolloid and Blue dye. Therefore, this seems to be the preferred method for ovarian SLN mapping. Interval between tracer injection and lymph node harvesting or mapping can also affect the results of sentinel node mapping. Using Tc-99m radiocolloid, a median 15-min interval seems to have an acceptable SLN detection rate. In contrast, ICG requires a shorter time interval for lymphatic uptake, implying that even a 2-min interval between injections and SLN mapping would yield a high detection rate (20).
It should be mentioned that other radioactive and non-radioactive tracers have also been used for sentinel node mapping in various malignancies. Tc-99m labeled ICG is a very commonly used tracer for sentinel node mapping. In addition to radioactivity guided mapping of the lymph nodes, a visual assistance using near infrared light is used which can help the surgeons in the operative theatre to identify the sentinel nodes more efficiently. However, the need for dimming of the light as well as requiring near infrared cameras can hamper the use of this tracer (28–30). Magnetic materials such as superparamagnetic iron oxide (SPIO) nanoparticles have also been used for sentinel node mapping in different malignancies. The advantage of these tracers is the lack of radiation, and more flexibility regarding the time of injection of the tracer in addition pre-operative imaging is possible (31–34).
The majority of studies have used injection of tracer in the suspensory and the infundibulopelvic ligaments, which showed a pooled detection rate of 85% [95% CI: 71–92]. In the Hassanzadeh et al.’s (9) study, all cases with failed SLN detection were corresponding to the patients with ovarian torsion in addition to their underlying pathology in the ovary. After omitting these four patients, injection of the tracer in the in the suspensory and the infundibulopelvic ligaments showed SLN detection rate of 93%. When observing the correlation between site of injection and detection rate, we recognized that an injection just underneath the peritoneum (ovarian ligaments, mesovarium, and ovarian hilum) resulted in higher detection rate compared to an injection into the ovarian cortex.
Location of sentinel nodes was reported clearly in all but one of the included studies (10). Overall, detection in the aortic region was 55%, whereas the corresponding detection rates for the pelvis and both pelvic/aortic regions were 11 and 34%, respectively. This is in line with the findings of another study which reported that in stage I–II ovarian cancer, lymph node metastases are detected as isolated para-aortic nodes in 50% of patients, in the pelvic region in 20% of patients, and in both the para-aortic and the pelvic region in the remaining 30% (4, 35). This study also concluded that in the majority of cases, aortic region lymphatic drainage of the right ovary is below IMA and that of the left ovary is above IMA. In the patients with unilateral ovary injection in whom the side location of the sentinel lymph nodes was recorded, SLNs were identified in 11 and 5% of cases contralaterally and bilaterally, respectively.
Type of surgery was also an important variable in the included studies (LPS vs. LPT). Laparoscopic performance of sentinel lymph node technique in ovarian cancer seems to be feasible (36). We assessed the SLN detection rate in all studies that were based on the surgical procedure (LPT vs. LPS). SLN detection rate in the LPT procedure group was 88%[95% CI: 77–95] compared to 80% [95% CI: 61–91]in the LPS group.
In most of the studies, tracer injection was performed with the adnexa still in situ, with the exception of three studies (10–12). Unlike other studies, these three studies performed injection of the tracer in the infundibulopelvic and utero-ovarian ligament stumps after the removal of the ovarian tumor, during the same or a subsequent surgical procedure. In such cases, the reliability could be lower due to alteration of the lymphatic drainage after ovarian mass resection. Laven et al. (12) reported that “SLN procedure after (previous) resection of the tumor seems inferior to detect sentinel nodes when compared to injection of the tracer in the ovarian ligaments before tumor resection.” However, SLN detection rates were 100% in the Lago et al.’s studies (10, 11). As such, overall, detection rate for these cases (with the injection site in the ligament stumps) was 59% [95% CI: 32–81]. Overall, 41 patients were included in the three aforementioned studies, and further studies are needed to explore the impact of tracer injection after ovarian mass resection in the ovarian SLN mapping.
A few studies (9, 10, 15, 17, 18) had enough data to calculate the sensitivity of sentinel node mapping in lymphatic staging of ovarian malignancies. Overall, pooled sensitivity was 91% [59–100], which seems to be an acceptable sensitivity for ovarian SLN mapping.
Definitive diagnosis of benign or malignant ovarian mass prior to resection is not determined, which is a major limitation in the ovarian SLN mapping. Therefore, patients with malignant ovarian mass who were included in these studies were not enough for lymph node dissection and histopathological examination regarding false-negative rate and sensitivity assessment. As such, further studies are needed to more accurately determine the sensitivity of sentinel node mapping in lymphatic staging of ovarian malignancies.
Sentinel node mapping in ovarian tumors is feasible and seems to have high sensitivity for the detection of lymph node involvement in malignant tumors of ovary. Mapping material, injection site, and previous surgery of the ovaries were associated with successful mapping. Larger studies are still needed to better evaluate the sensitivity of this procedure in ovarian malignancies.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
SA and RS: study design. SA, MF, MH, and RS: data acquisition. SA, SM, and RS: quality control of data and algorithms and manuscript preparation. RS and SA: data analysis and interpretation. RS: statistical analysis. All authors: study the concepts, editing and review the manuscript. All authors have read and agreed to the published version of the manuscript.
The Vice Chancellery of Research of Mashhad University of Medical Sciences financially supported this thesis with the approval number 981455. The funding source did not have any role in the study design; in the collection, analysis, and interpretation of data; in the writing of the manuscript; and in the decision to submit the manuscript for publication.
This study was a result of a thesis which has been conducted as a joint project between the Nuclear Medicine Research Center and the Women’s Health Research Center of Mashhad University of Medical Sciences.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sadeghi R, Tabasi KT, Bazaz SM, Kakhki VR, Massoom AF, Gholami H, et al. Sentinel node mapping in the prostate cancer. Meta-analysis. Nuklearmedizin. (2011) 50:107–15. doi: 10.3413/nukmed-0339-10-07
2. Holschneider CH, Berek JS. Ovarian cancer: epidemiology, biology, and prognostic factors. Semin Surg Oncol. (2000) 19:3–10.
3. Benedet J, Pecorelli S, Ngan H, Hacker NF, Denny L, Jones IIIHW, et al. Staging classifications and clinical practice guidelines for gynaecological cancers. Int J Gyneco Obstet. (2000) 70:207–312.
4. Kleppe M, Wang T, Van Gorp T, Slangen BF, Kruse AJ, Kruitwagen RF. Lymph node metastasis in stages I and II ovarian cancer: a review. Gynecol Oncol. (2011) 123:610–4.
5. Takeshima N, Hirai Y, Umayahara K, Fujiwara K, Takizawa K, Hasumi K. Lymph node metastasis in ovarian cancer: difference between serous and non-serous primary tumors. Gynecol Oncol. (2005) 99:427–31.
6. Maggioni A, Benedetti Panici P, Dell’Anna T, Landoni F, Lissoni A, Pellegrino A, et al. Randomised study of systematic lymphadenectomy in patients with epithelial ovarian cancer macroscopically confined to the pelvis. Br J Cancer. (2006) 95:699–704. doi: 10.1038/sj.bjc.6603323
7. Lago V, Montero B, Lopez S, Padilla-Iserte P, Matute L, Marina T, et al. Ultrastaging protocol in sentinel lymph node for apparent early stage ovarian cancer. Gynecol Oncol. (2021) 161:408–13. doi: 10.1016/j.ygyno.2021.03.001
8. Sokouti M, Sadeghi R, Pashazadeh S, Eslami S, Sokouti M, Ghojazadeh M, et al. Meta-MUMS DTA: implementation, validation, and application of diagnostic test accuracy software for meta-analysis in radiology. Clin Epidemiol Glob Health. (2021) 9:310–25.
9. Hassanzadeh M, Hosseini Farahabadi E, Yousefi Z, Kadkhodayan S, Zarifmahmoudi L, Sadeghi R, et al. Lymphatic mapping and sentinel node biopsy in ovarian tumors: a study using intra-operative Tc-99m-Phytate and lymphoscintigraphy imaging. J Ovarian Res. (2016) 9:55. doi: 10.1186/s13048-016-0265-4
10. Lago V, Bello P, Montero B, Matute L, Padilla-Iserte P, Lopez S, et al. Clinical application of the sentinel lymph node technique in early ovarian cancer: a pilot study. Int J Gynecol Cancer. (2019) 29:377-81.
11. Lago V, Bello P, Montero B, Matute L, Padilla-Iserte P, Lopez S, et al. Sentinel lymph node technique in early-stage ovarian cancer (SENTOV): a phase II clinical trial. Int J Gynecol Cancer. (2020) 30:1390–6. doi: 10.1136/ijgc-2020-001289
12. Laven P, Kruitwagen R, Zusterzeel P, Slangen B, van Gorp T, van der Pol J, et al. Sentinel lymph node identification in early stage ovarian cancer: is it still possible after prior tumor resection? J Ovarian Res. (2020) 14:132. doi: 10.1186/s13048-021-00887-w
13. Negishi H, Takeda M, Fujimoto T, Todo Y, Ebina Y, Watari H, et al. Lymphatic mapping and sentinel node identification as related to the primary sites of lymph node metastasis in early stage ovarian cancer. Gynecol Oncol. (2004) 94:161–6. doi: 10.1016/j.ygyno.2004.04.023
14. Nyberg RH, Korkola P, Mäenpää J. Ovarian sentinel node: is it feasible? Int J Gynecol Cancer. (2011) 21:568–72.
15. Kleppe M, Brans B, Van Gorp T, Slangen BF, Kruse AJ, Pooters IN, et al. The detection of sentinel nodes in ovarian cancer: a feasibility study. J Nucl Med. (2014) 55:1799–804.
16. Speth SC, Kruitwagen RF, Kleppe M, Pooters IN, Van Gorp T, Slangen BF, et al. Comparison of intraoperative gamma-probe imaging and postoperative SPECT/CT in detection of sentinel nodes related to the ovary. J Nucl Med. (2017) 58:243–5. doi: 10.2967/jnumed.116.183426
17. Nyberg RH, Korkola P, Maenpaa JU. Sentinel node and ovarian tumors: a series of 20 patients. Int J Gynecol Cancer. (2017) 27:684–9. doi: 10.1097/IGC.0000000000000948
18. Uccella S, Nero C, Vizza E, Vargiu V, Corrado G, Bizzarri N, et al. Sentinel-node biopsy in early-stage ovarian cancer: preliminary results of a prospective multicentre study (SELLY). Am J Obstet Gynecol. (2019) 221:e1–10. doi: 10.1016/j.ajog.2019.05.005
19. Ataei SMS, Sadri K, Azad A, Jahani N, Esmaeil Poor M, Yousefi Z, et al. Sentinel node mapping in patients with ovarian tumors: a study using intraoperative 99mTc-phytate gamma probing and post-operative SPECT/CT lymphoscintigraphy. Eur J Nucl Med Mol Imaging. (2021) 48:S376–7.
20. Angelucci M, Corrado G, Mancini E, Baiocco E, Chiofalo B, Zampa A, et al. Laparoscopic indocyanine green sentinel lymph node mapping in early ovarian cancer. A pilot study and review of the literature. Ital J Gynaecol Obstet. (2016) 28:23–8.
21. Buda A, Passoni P, Corrado G, Bussi B, Cutillo G, Magni S, et al. Near-infrared fluorescence-guided sentinel node mapping of the ovary with indocyanine green in a minimally invasive setting: a feasible study. J Minim Invasive Gynecol. (2017) 24:165–70. doi: 10.1016/j.jmig.2016.09.006
22. Vanneuville G, Mestas D, Le Bouedec G, Veyre A, Dauplat J, Escande G, et al. The lymphatic drainage of the human ovary in vivo investigated by isotopic lymphography before and after the menopause. Surg Radiol Anat. (1991) 13:221–6. doi: 10.1007/BF01627990
23. Uccella S, Zorzato PC, Lanzo G, Fagotti A, Cianci S, Gallina D, et al. The role of sentinel node in early ovarian cancer: a systematic review. Minerva Med. (2019) 110:358–66. doi: 10.23736/S0026-4806.19.06145-7
24. Mach P, Kimmig R, Buderath P. The role of sentinel-node biopsy in ovarian cancer. Minerva Ginecol. (2020) 72:399–403.
25. Ditto A, Martinelli F, Reato C, Kusamura S, Solima E, Fontanelli R, et al. Systematic para-aortic and pelvic lymphadenectomy in early stage epithelial ovarian cancer: a prospective study. Ann Surg Oncol. (2012) 19:3849–55.
26. van de Poll-Franse LV, Pijnenborg JM, Boll D, Vos MC, van den Berg H, Lybeert ML, et al. Health related quality of life and symptoms after pelvic lymphadenectomy or radiotherapy vs. no adjuvant regional treatment in early-stage endometrial carcinoma: a large population-based study. Gynecol Oncol. (2012) 127:153–60.
27. Schaafsma BE, Verbeek FP, Peters AA, Van der Vorst J, de Kroon CD, van Poelgeest MI, et al. Near-infrared fluorescence sentinel lymph node biopsy in vulvar cancer: a randomised comparison of lymphatic tracers. BJOG. (2013) 120:758–64. doi: 10.1111/1471-0528.12173
28. Rietbergen DDD, van Gennep EJ, KleinJan GH, Donswijk M, Valdes Olmos RA, van Rhijn BW, et al. Evaluation of the hybrid tracer indocyanine green-99mTc-nanocolloid for sentinel node biopsy in bladder cancer-a prospective pilot study. Clin Nucl Med. (2022). doi: 10.1097/RLU.0000000000004301 [Epub ahead of print].
29. Yin R, Ding LY, Wei QZ, Zhou Y, Tang GY, Zhu X. Comparisons of ICG-fluorescence with conventional tracers in sentinel lymph node biopsy for patients with early-stage breast cancer: a meta-analysis. Oncol Lett. (2021) 21:114. doi: 10.3892/ol.2020.12375
30. Manca G, Garau LM, Mazzarri S, Mazzuca L, Muccioli S, Ghilli M, et al. Novel experience in hybrid tracers: clinical evaluation of feasibility and efficacy in using ICG-99mTc nanotop for sentinel node procedure in breast cancer patients. Clin Nucl Med. (2021) 46:e181–7. doi: 10.1097/RLU.0000000000003478
31. Nadeem M, Ansari B, Osborne C. Sentimag(R) technique for sentinel lymph node biopsy in breast cancer patients: evaluation of effectiveness, Feasibility and Challenges. Chirurgia (Bucur). (2022) 117:37–44. doi: 10.21614/chirurgia.2673
32. Winter A, Engels S, Goos P, Suykers MC, Gudenkauf S, Henke RP, et al. Accuracy of magnetometer-guided sentinel lymphadenectomy after intraprostatic injection of superparamagnetic iron oxide nanoparticles in prostate cancer: the SentiMag Pro II study. Cancers. (2019) 12:32. doi: 10.3390/cancers12010032
33. Pouw JJ, Grootendorst MR, Bezooijen R, Klazen CA, De Bruin WI, Klaase JM, et al. Pre-operative sentinel lymph node localization in breast cancer with superparamagnetic iron oxide MRI: the SentiMAG multicentre trial imaging subprotocol. Br J Radiol. (2015) 88:20150634. doi: 10.1259/bjr.20150634
34. Winter A, Chavan A, Wawroschek F. Magnetic resonance imaging of sentinel lymph nodes using intraprostatic injection of superparamagnetic iron oxide nanoparticles in prostate cancer patients: first-in-human results. Eur Urol. (2018) 73:813–4. doi: 10.1016/j.eururo.2018.01.009
35. Benedetti-Panici P, Greggi S, Maneschi F, Scambia G, Amoroso M, Rabitti C, et al. Anatomical and pathological study of retroperitoneal nodes in epithelial ovarian cancer. Gynecol Oncol. (1993) 51:150–4.
Keywords: sentinel node, lymphatic mapping, meta-analysis, systematic review, ovarian cancer, nuclear medicine, lymphoscintigraphy
Citation: Ataei Nakhaei S, Mostafavi SM, Farazestanian M, Hassanzadeh M and Sadeghi R (2022) Feasibility of sentinel lymph node mapping in ovarian tumors: A systematic review and meta-analysis of the literature. Front. Med. 9:950717. doi: 10.3389/fmed.2022.950717
Received: 23 May 2022; Accepted: 07 July 2022;
Published: 01 August 2022.
Edited by:
Nicolas A. Karakatsanis, Cornell University, United StatesReviewed by:
Alexander Winter, University Hospital Oldenburg, GermanyCopyright © 2022 Ataei Nakhaei, Mostafavi, Farazestanian, Hassanzadeh and Sadeghi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ramin Sadeghi, c2FkZWdoaXJAbXVtcy5hYy5pcg==; cmFtaW5zYWRlZ2hpMTM1NUB5YWhvby5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.