 Guillermo Droppelmann1,2,3*
Guillermo Droppelmann1,2,3* Manuel Tello4
Manuel Tello4 Nicolás García5Cristóbal Greene6
Nicolás García5Cristóbal Greene6 Carlos Jorquera7
Carlos Jorquera7 Felipe Feijoo4
Felipe Feijoo4- 1Research Center on Medicine, Exercise, Sport and Health, MEDS Clinic, Santiago, RM, Chile
- 2Health Sciences Ph.D. Program, Universidad Católica de Murcia UCAM, Murcia, Spain
- 3Principles and Practice of Clinical Research (PPCR), Harvard T.H. Chan School of Public Health, Boston, MA, United States
- 4School of Industrial Engineering, Pontificia Universidad Católica de Valparaíso, Valparaíso, Chile
- 5MSK Diagnostic and Interventional Radiology Department, MEDS Clinic, Santiago, RM, Chile
- 6Hand and Elbow Unit, Department of Orthopaedic Surgery, MEDS Clinic, Santiago, RM, Chile
- 7Facultad de Ciencias, Escuela de Nutrición y Dietética, Universidad Mayor, Santiago, RM, Chile
Background: Ultrasound (US) is a valuable technique to detect degenerative findings and intrasubstance tears in lateral elbow tendinopathy (LET). Machine learning methods allow supporting this radiological diagnosis.
Aim: To assess multilabel classification models using machine learning models to detect degenerative findings and intrasubstance tears in US images with LET diagnosis.
Materials and methods: A retrospective study was performed. US images and medical records from patients with LET diagnosis from January 1st, 2017, to December 30th, 2018, were selected. Datasets were built for training and testing models. For image analysis, features extraction, texture characteristics, intensity distribution, pixel-pixel co-occurrence patterns, and scales granularity were implemented. Six different supervised learning models were implemented for binary and multilabel classification. All models were trained to classify four tendon findings (hypoechogenicity, neovascularity, enthesopathy, and intrasubstance tear). Accuracy indicators and their confidence intervals (CI) were obtained for all models following a K-fold-repeated-cross-validation method. To measure multilabel prediction, multilabel accuracy, sensitivity, specificity, and receiver operating characteristic (ROC) with 95% CI were used.
Results: A total of 30,007 US images (4,324 exams, 2,917 patients) were included in the analysis. The RF model presented the highest mean values in the area under the curve (AUC), sensitivity, and also specificity by each degenerative finding in the binary classification. The AUC and sensitivity showed the best performance in intrasubstance tear with 0.991 [95% CI, 099, 0.99], and 0.775 [95% CI, 0.77, 0.77], respectively. Instead, specificity showed upper values in hypoechogenicity with 0.821 [95% CI, 0.82, −0.82]. In the multilabel classifier, RF also presented the highest performance. The accuracy was 0.772 [95% CI, 0.771, 0.773], a great macro of 0.948 [95% CI, 0.94, 0.94], and a micro of 0.962 [95% CI, 0.96, 0.96] AUC scores were detected. Diagnostic accuracy, sensitivity, and specificity with 95% CI were calculated.
Conclusion: Machine learning algorithms based on US images with LET presented high diagnosis accuracy. Mainly the random forest model shows the best performance in binary and multilabel classifiers, particularly for intrasubstance tears.
Introduction
Lateral elbow tendinopathy (LET) (1), also known as tennis elbow (2), is one of the most frequent musculoskeletal disorders (3). The common extensor tendon, specifically the extensor carpi radialis brevis, is directly involved in the development of this condition (4). LET is a potentially debilitating condition causing significant pain and disability for periods of 12 months or more (5), and in some cases, also generates disruptive sleep (6). This condition is estimated to affect 3.3–3.5 per 1,000 by year (7), affecting individuals during their most productive period (8) and increasing in tennis players with a prevalence of over 40–50% (9). Effective treatment for this tendinopathy is uncertain, with controversial scientific evidence that provides more than 40 modalities (10) in 200 clinical trials and several systematic reviews (11).
Although LET remains primarily a clinical diagnosis (12), the ultrasound (US) findings in common extensor tendon have been well documented in asymptomatic persons (13–17) and LET individuals with tendon structural changes (18–22). However, the degree of these tendon structural changes is highly diverse, with different levels of accuracy (19, 23), making the interpretation of the US imaging a real radiological challenge. For example, a met analysis reported that the US sensitivity and specificity in the detection of common extensor tendon ranged between 64 and 100% and 36 and 100%, respectively (24). Furthermore, this high variability can increase even more if different types of degenerative findings are considered, such as hypoechogenicity, bone changes, neovascularity, calcifications, cortical irregularities (25), and tear (thickness) (26), increasing the lack of precision in the diagnosis by US images. To date, there is still no consensus about what parameters should be considered for the evaluation of changes in the tendon matrix (27).
Recently, artificial intelligence has shown the potential to revolutionize the accuracy of diagnosis by developing a series of classification models (28) and by reducing medical diagnosis variability (29–31). The algorithms based on machine learning and convolutional neural network have been successfully used in pattern recognition in different clinical contexts and specialties, such as neurology (32–34), pulmonary (35–37), cardiovascular (38–42), and oncology (43–51), improving diagnosis accuracy, weighted errors, false-positive rate, sensitivity, specificity, and the area under the receiver operating characteristic curve (AUC) (52). In radiology, machine learning and convolutional neural network algorithms have been used to detect and classify injury patterns in fractures, cartilage defects, meniscal and anterior cruciate ligament tears, and spinal metastases (53, 54) with excellent performance indices.
Most of the studies mentioned above have used computed tomography scan, magnetic resonance imaging, and X-rays as an image-generating source. For example, fracture detection using a computed tomography scan has been used by Tomita et al. (55) with deep neural networks for automatic detection of osteoporotic vertebral fractures, obtaining an accuracy of 89.2%. Another author (56) that also studied automated detection of posterior-element fractures with deep convolutional networks obtained an AUC of 85.7%. There is also some experience using automatic classification and detection of calcaneus fracture with an accuracy of 98% (57). Couteaux et al. (58), Bien et al. (59), and Roblot et al. (60) developed algorithms to automatically detect knee meniscal tears using convolutional neural networks and deep learning assisted with magnetic resonance imaging, obtaining AUC scores of 90.6, 84.7, and 92%, respectively. A similar performance was obtained by authors in (61), where cartilage lesion detection algorithms were developed, reaching accuracy levels of 91%. In radiography, different applications are considered, such as deep learning classification algorithms for the detection of ossification areas of the hand to estimate skeletal maturity (62), obtaining accuracy results similar to an expert radiologist (63). Another publication evaluated knee osteoarthritis in 3,000 subjects (5,960 knees) from the Osteoarthritis Initiative dataset using deep learning techniques. They achieved an AUC of 93%, although the diagnosis is highly dependent on the practitioner’s subjectivity, just like US methods (64). As noted earlier, however, US imaging has not been frequently used as an image-generating source.
Machine learning for the medical US continues to be an opportunity (65), especially in musculoskeletal disorders since the US is highly operator-dependent (66) and the applications are dictated by adequate front-end beamforming, compression, signal extraction, and velocity (67), requiring significant training to acquire a level of competence in clinical diagnosis (68) because the images contain multiplicative noise (69). Baka et al. (70) proposed a model to learn the appearance of the bone interface using US images and random forest methods, obtaining a precision of 86%. Another group proposed an algorithm to segment vertebral US images into three regions with a classification rate of 84.7% (71). In tendon, literature is uncommon yet. In 2017, the University of Salford from the United Kingdom reported in an international conference an automatic method to detect and classify Achilles tendon injuries using decision trees, non-linear support vector machines, and ensemble classifiers (69). Kapinski in 2018 (72) reported a novel method for continuous evaluation of reconstructed Achilles tendon healing based on the responses of intermediate convolutional neural network layers. Note that the task of detecting and classifying different conditions as described above can be considered simple since they are based on binary results (an anomaly can only be present or not) (54). This study differs from others that use deep learning or convolutional neural networks because it uses a multilabel, fast, and simplified classifier to find different degenerative patterns simultaneously, such as hypoechogenicity, neovascularity, bony irregularities, and fibrillar disruptions. Currently, no scientific publications have identified ultrasonographic findings using artificial intelligence algorithms.
This article aims to assess multilabel classification models using machine learning algorithms to detect degenerative findings and intrasubstance tear in US images with LET diagnosis.
Materials and methods
Study design
This study was designed as a retrospective and multicentric study. It was written following the Strengthening the Reporting of Observation studies in Epidemiology (STROBE) guideline (73). All patients records with an elbow US exam at MEDS Clinic in Santiago, Región Metropolitana, Chile. This study started on March 1st, 2019.
Subjects
Only images of the common extensor tendon were considered. We selected US images and medical records from patients with a LET diagnosis from January 1st, 2017, to December 30th, 2018. The inclusion criteria were: (1) clinical diagnosis of LET established by orthopedists, sports medicine physicians, or any musculoskeletal specialists, (2) US exam made in the medical center of interest, (3) US exam reported by any musculoskeletal radiologist with more than 10 years of experience, and (4) no race or age restriction. Consecutively, exclusion criteria were: (1) US-guided procedures, such as corticoid, stem cell, and platelet-rich plasma injections, (2) previous LET surgery, and (3) duplicate or not distinguishable images, were removed from the dataset. Figure 1 provides the flowchart to select the subjects.
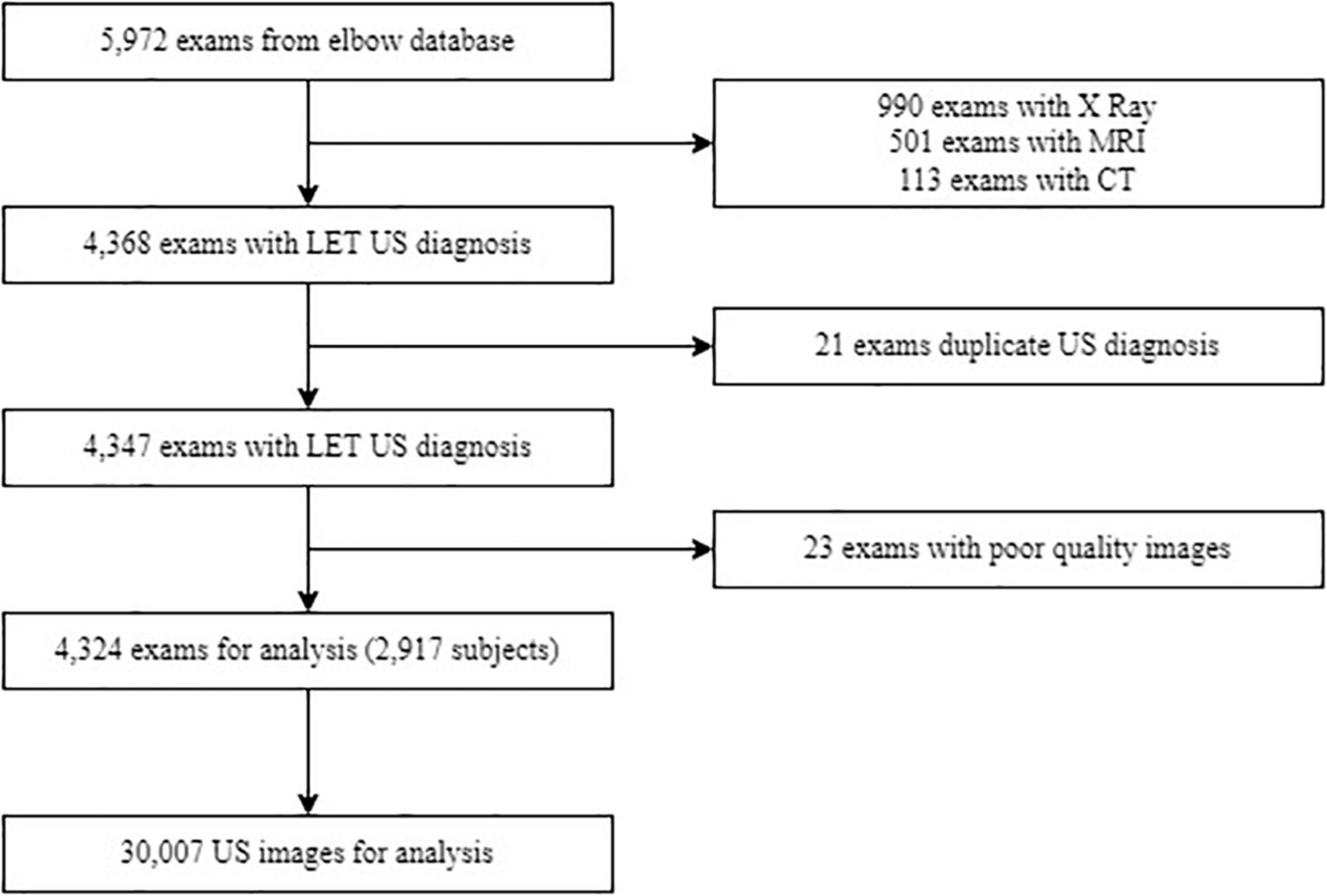
Figure 1. Flowchart of data selection and subjects used in the study. Abbreviations: MRI, magnetic resonance imaging; CT, computed tomography scan; LET, lateral elbow tendinopathy; US, ultrasound.
Ultrasound assessment of common extensor tendon
All common extensor tendons were assessed using an Aplio 500 US system (Toshiba America Medical Systems, Inc, Tustin, CA, USA) equipped with a multifrequency linear transducer was used. A frequency of 18 MHz was chosen. The images were stored as Digital Imaging and Communications in Medicine (DICOM) files and reviewed on a picture archiving and communication system (PACS).
All patients with LET diagnosis were examined in a seated position with flexion elbow in 90 grades with the wrist pronated, and the arm was resting on a table (14).
Greyscale and color Doppler US imaging are standard methods used for assessing tendon structural changes (74). Following the literature recommendations, four common prevalent degenerative findings were selected from US exams, such as hypoechogenicity, neovascularity, enthesopathy, and intrasubstance tear (75). A focal hypoechoic region was defined as being rounded and not associated with tendon disruption. Neovascularity was assessed as the presence of blood flow on color Doppler. Enthesopathy was evaluated as bony abnormalities at the tendon insertion. A linear intrasubstance tear was defined as a linear hypoechoic focus associated with discontinuity of tendon fibers (76–80). Every finding was evaluated with a binary score as present or absent. We recorded when an exam presents more than one degenerative finding. Figure 2A shows the evaluation position, and Figure 2B represents US finding, in this case, an intrasubstance tear.
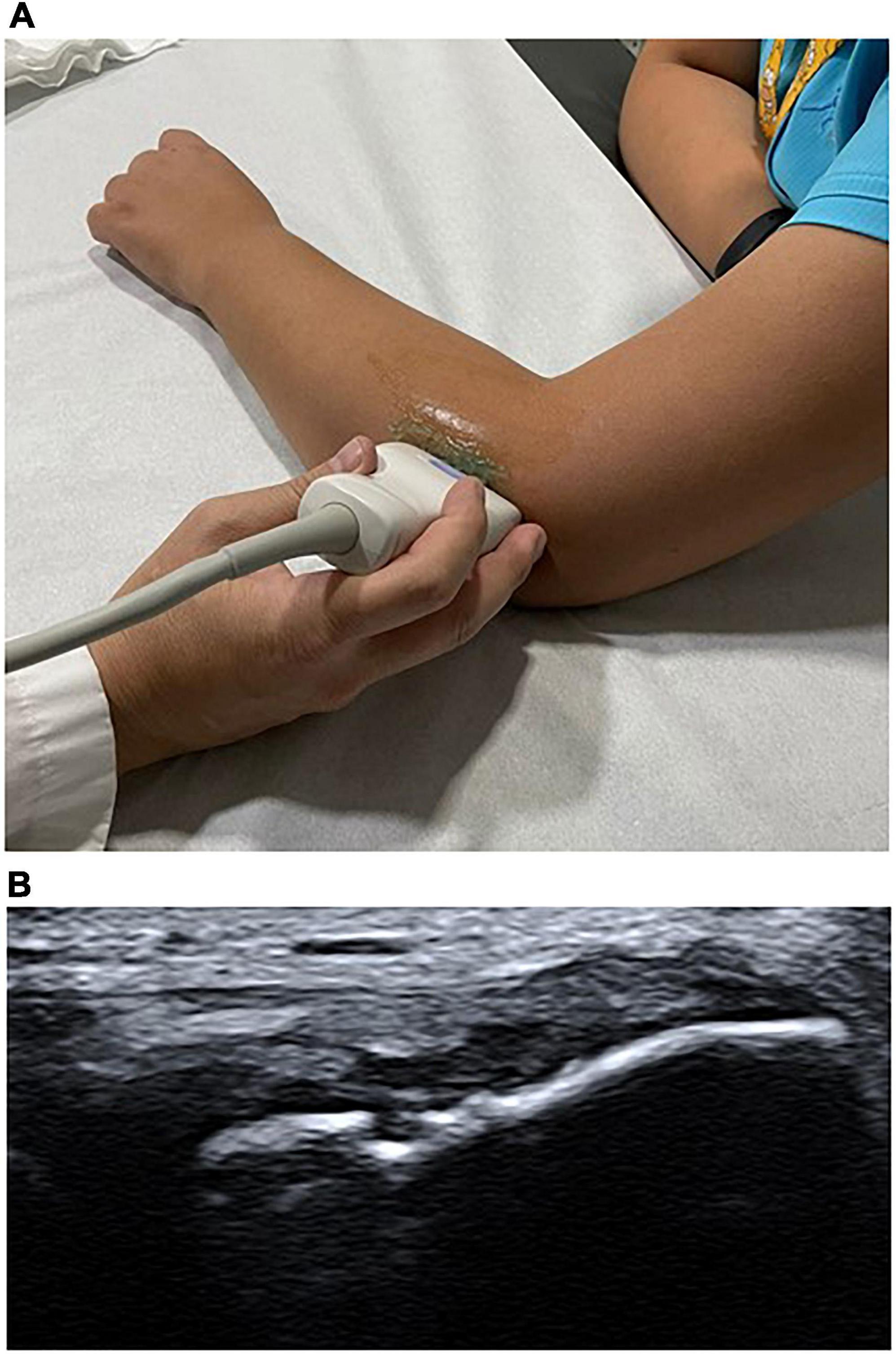
Figure 2. Patient evaluation position and an ultrasound (US) finding, respectively. (A) Probe positioning in the elbow in the US exploration of the extensor tendon complex. (B) US imaging shows intrasubstance tear in extensor tendon complex.
Datasets: Ultrasound image and database
Several recommendations were followed for data (images) pre-processing, object detection, and feature extraction (81–83). Two datasets (A and B) were built for training and testing models. The pre-processing step considers eliminating any elements that generated noise in the images, such as uneven lighting, different sizes, or image portions without information (84). Object detection is a specific injury area of interest for the analysis. However, in this case, we considered the common extensor tendon image. Feature extraction is an important step in the construction of any pattern classification and aims at the extraction of the relevant information that characterizes each class (85). According to the 7th International Conference on System Engineering and Technology 2017, texture analysis and classification in US medical images can use feature extraction and texture characteristics for determining echo pattern characteristics (86). One of the most used are intensities distribution (mean intensity and standard deviation), pixel-pixel co-occurrence patterns, and scales granularity. Then the shape contour was extracted where the texture of the pixels was quantified. The US images were labeled manually with four degenerative findings classification outputs findings (hypoechogenicity, neovascularity, enthesopathy, and intrasubstance tear) (65) and complementary patient data such as sex, age, and side of the injury (right or left). The final process consists of a combination between the patient’s information and image analysis. Dataset A was image prediction and contained data extraction from 95 morphology characteristics, shapes, and texture variables, where one image corresponding to one diagnostic (30.007 rows). Dataset B was the patient prediction and included 380 variables from data extraction, such as median, standard deviation, minimal, and maximal, where one exam corresponds to one diagnostic (4.321 rows). Figure 3 represents the study workflow process.
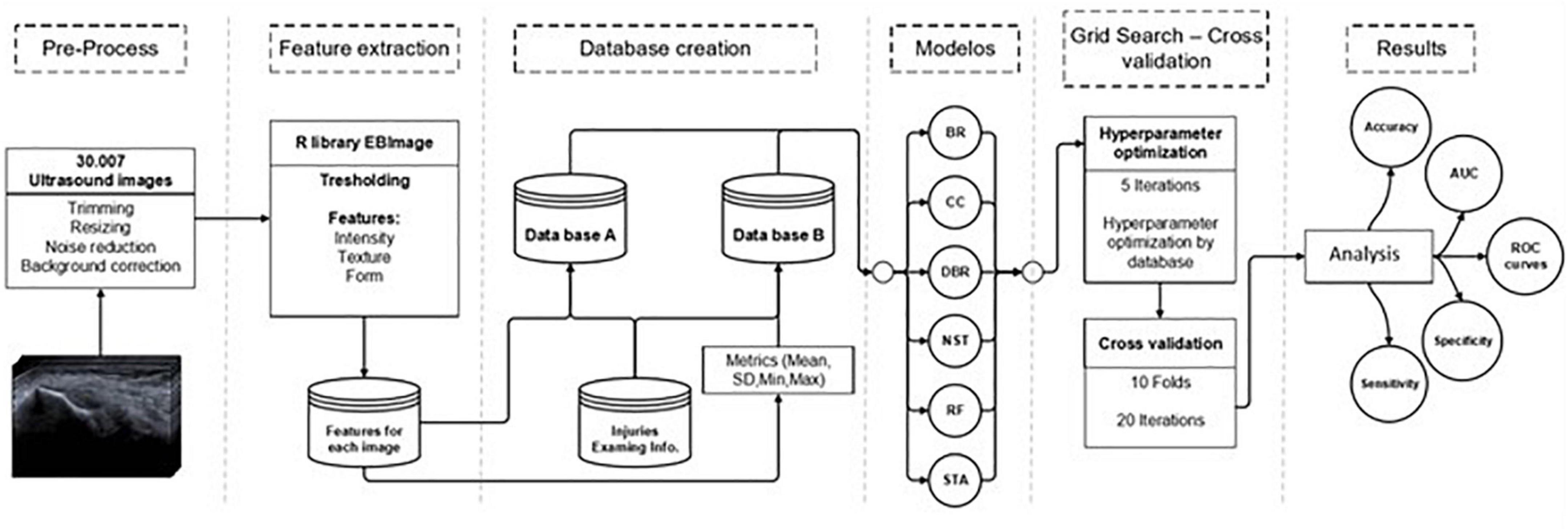
Figure 3. Study workflow. Abbreviations: BR, binary relevance model; CC, classifier chains model; DBR, dependent binary relevance model; NST, nested stacking model; RF, random forest; STA, staking generalization; AUC, area under the curve.
Machine learning and statistical analysis
Supervised learning was used because most machine learning applications for US involve them. Both datasets were implemented into binary and multilabel classification algorithms in six machine learning methods: Binary relevance model, classifier chains model, nested stacking model, dependent binary relevance model, staking generalization, and random forest.
All models were trained to classify four tendon findings (hypoechogenicity, neovascularity, enthesopathy, and intrasubstance tear) in images with LET diagnosis. First, each pattern was recognized individually and then the four finding simultaneously. Different metrics were conducted to assess the classification of machine learning models. A K-fold-repeated-cross-validation (KFRCV) with ten as the number of folds was used. After this process, means and confidence intervals (CI) values were obtained.
Data were analyzed using R version 3.6.2 (R Foundation for Statistical Computing). The following packages were used: “EBImage” for characteristics extraction, “mlr” for each machine learning algorithm, and “randomForest” for the random forest (87–89). Additionally, to measure multilabel prediction (classification) were used multilabel accuracy, sensitivity, specificity, and receiver operating characteristic (ROC) (90). Also, we included a positive predictive value. Differences in US findings between women and men were assessed for significance using the T-test and chi-squared test. The significance level was considered p < (0.05) and 95% CI for all metrics.
Results
Common extensor tendinopathy
A total of 30,007 US images, 6.9 on average in 4,324 exams, and medical records from 2,917 patients with a LET diagnosis were included in the data analysis in this study. Patients’ age was presented with a minimum value of 7 and a maximum of 91 years. Women are older than men in 1 year 47.18 ± 11.00 (p < 0.001) and also, they presented statistical differences in hypoechogenicity finding in comparison with men (p = 0.01). The total of exams presented at least one degenerative finding. US features are summarized in Table 1.
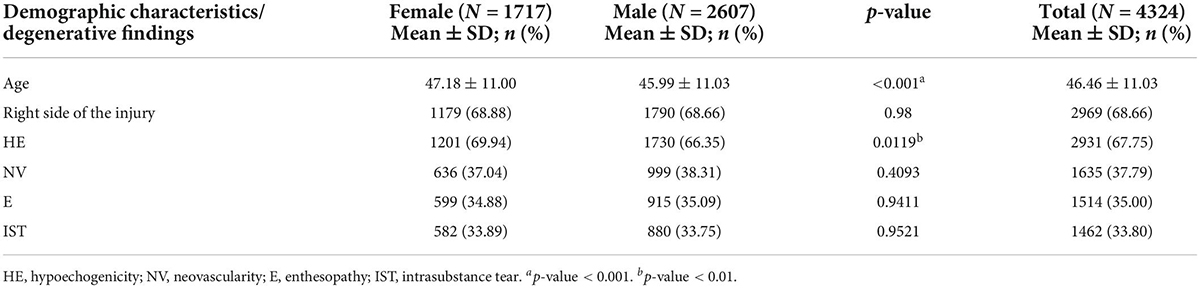
Table 1. Ultrasound findings comparison between sexes.
Machine learning models for a binary classifier
Table 2 shows the binary classification performance (AUC, sensitivity, and specificity) for both datasets (A and B) in each of the six machine learning algorithms. Main degenerative findings in LET (hypoechogenicity, neovascularity, enthesopathy, and intrasubstance tear) were considered under analysis. Focusing on AUC sensitivity and specificity, most models performed with variability among them. Results were described in most cases with a minimal range of 95% CI, demonstrating a robust performance for all models. Notably, the RF model obtained the best results. For example, Table 2 shows dataset A, where random forest presented the highest mean values in AUC, sensitivity, and also specificity by each degenerative finding. The AUC and sensitivity showed the best performance in IST with 0.991 [95% CI, 0.99, −0.99], and 0.775 [95% CI, 0.77, −0.77], respectively. Instead, specificity showed upper values in hypoechogenicity with 0.821 [95% CI, 0.82, −0.82].
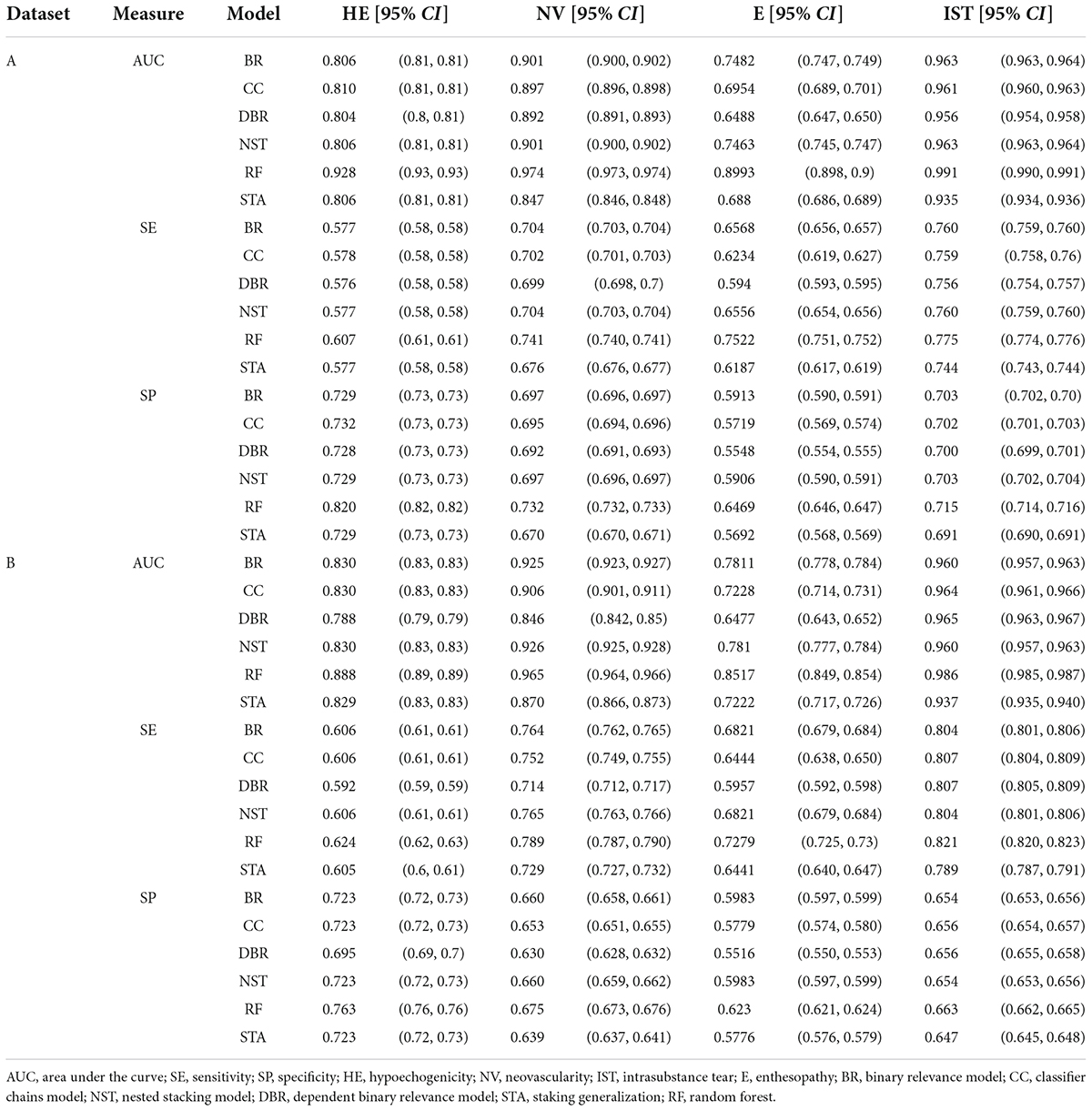
Table 2. The area under the curve (AUC), sensitivity, and specificity [95% CI] values of six machine learning classifiers based on degenerative findings in datasets A and B.
A similar situation occurred for dataset B, which showed slightly lower values for the same findings and models. The RF model also demonstrated the best performance for all measures and degenerative features. Table 2 showed the highest AUC and sensitivity values for ISR 0.937 [95% CI, 0.93–0.94] and 0.82 [95% CI, 0.82, −0.82]. Hypoechogenicity also presented better specificity than other degenerative findings with 0.763 [95% CI, 0.72, −0.72].
Machine learning models for a multilabel classifier
In the previous results section, the machine learning models assessed a binary classification for each degenerative finding. Now, these methods used a multilabel classifier to identify the four types of tendon findings simultaneously in both datasets. In this scenario, the diagnosis presented different accuracy levels in all machine learning models. When the diagnosis was based on the combination of degenerative findings, the random forest algorithm again presented the best performances among the selected models. Table 3 shows that the random forest in dataset A presented the highest multilabel accuracy value of 0.772 [95% CI, 0.771, 0.773]. Similarly, in the condition represented in dataset B, these results show that the model performs well in testing environments without presenting overfitting issues. Multilabel accuracy value was 0.723 [95% CI, 0.721, 0.726]. Additionally, high macro and micro-AUC scores are observed in RF models in both datasets. These results could be explained due to the balance between sensitivity and specificity shown in RF models. Particularly, micro-AUC observed in dataset A of 0.962 [95% CI, 0.962–0.963] and 0.942 [95% CI, 0.941–0.943] in dataset B results are essential because aggregating the contributions of all classes to compute the average metric.
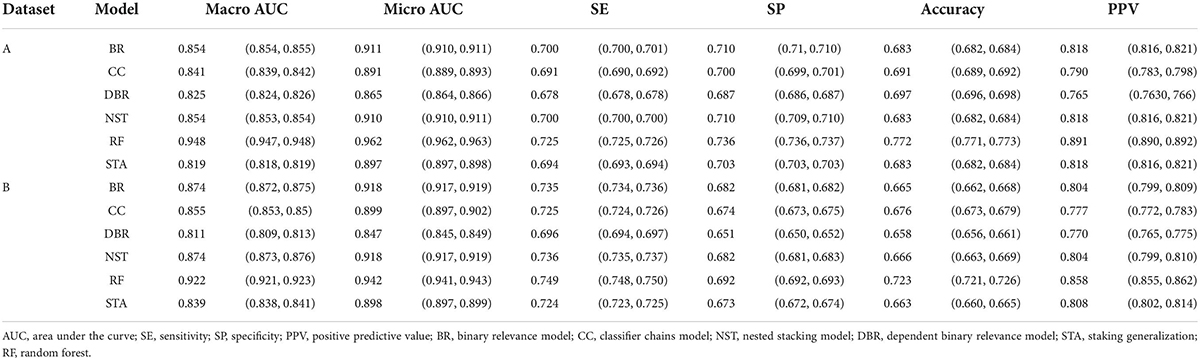
Table 3. Multilabel accuracy values of six machine learning classifiers based on degenerative findings in both datasets.
Diagnosis performance
Figure 4 represents dataset A, and the results show the relation between sensitivity vs. 1-specificity across each degenerative finding using the random forest model. In this figure, the plot shows the higher discriminant capacity of diagnosis detection. Most of the lines are located progressively closer to the upper left-hand corner in ROC space. The intrasubstance tear shows the most significant discriminate capacity in comparison with the other tendon injuries. However, the enthesopathy finding presented the lowest discriminate capacity in this model.
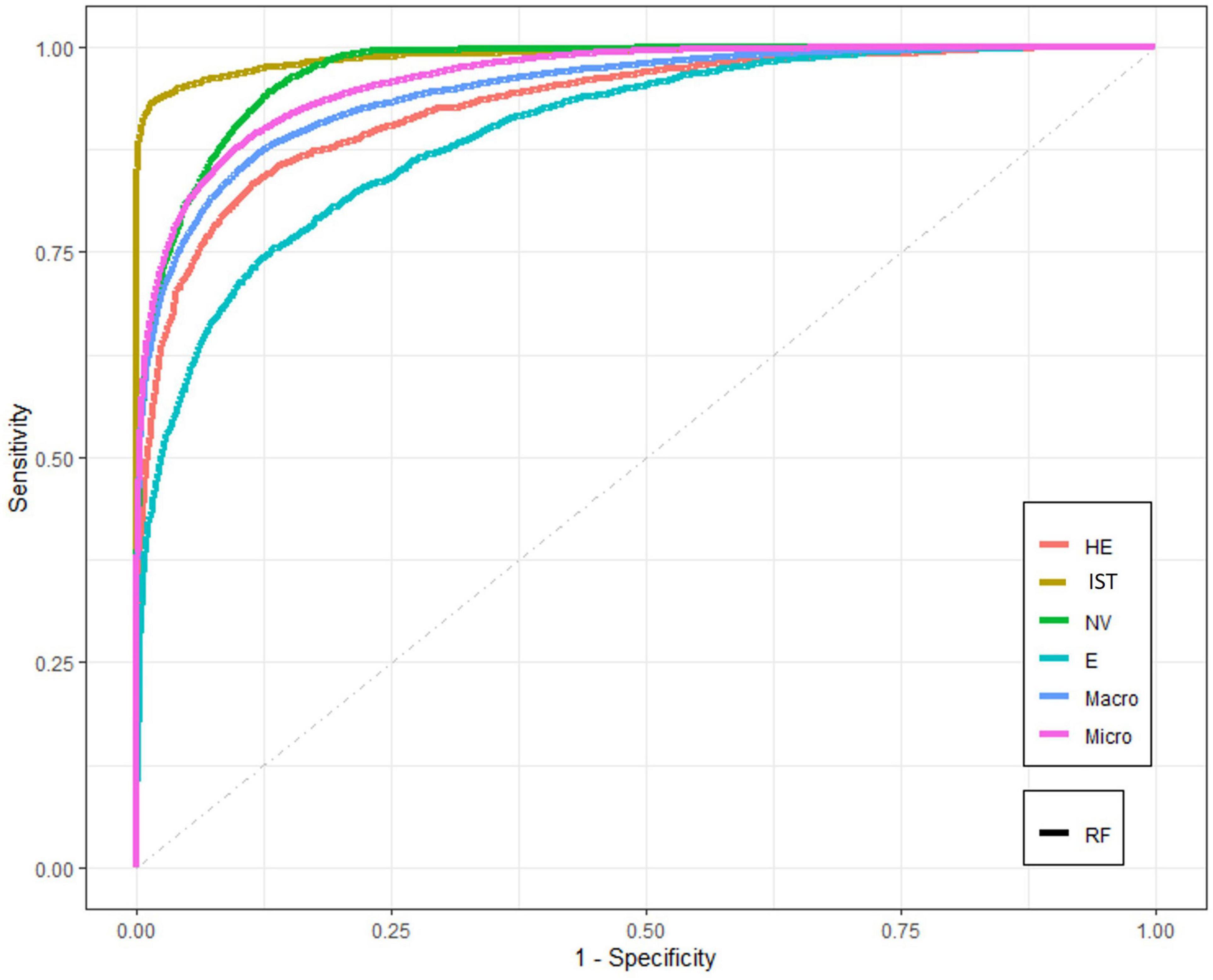
Figure 4. The receiver operating characteristic (ROC) curves for RF model for dataset A. Abbreviations: RF, random forest; HE, hypoechogenicity; NV, neovascularity; IST, intrasubstance tear; E, enthesopathy; Macro, macro-AUC; Micro, micro-AUC.
Discussion
This study is one of the first to present multilabel classification models using machine learning algorithms to detect degenerative findings and intrasubstance tear in US images with LET diagnosis. This retrospective analysis explicitly considered one of the most extensive series of extensor carpi radialis brevis US images, and our machine learning-based tool for diagnosis of LET was trained using the largest dataset so far. The most notable outcomes in this study were obtained by incorporating several machine learning models based on diagnosis know condition. Excellent results and highest values for all degenerative findings were detected in the binary classification performance. Moreover, when the US diagnosis was based on the combination of degenerative findings using a multilabel classifier, the accuracy values presented strong performance too. Our results showed that the random forest algorithm presented the best diagnosis performance, in both binary and multilabel models. These results demonstrate that the implementation of tools derived from artificial intelligence can be used to support the imaging for tendinopathies. Collaborative work between the radiologist and the algorithm could improve the precision of the results, especially if the institution does not have a radiologist specializing in the musculoskeletal area.
Traditionally, US has been demonstrated as a cost-effective tool for detecting abnormalities patterns in tendon structures. Additionally, there is evidence to support the use of US in the detection of LET. A meta-analysis published in 2014 determined that diagnostic test accuracy appears to be highly dependent on numerous variables, such as operator experience, equipment, and stage of pathology. However, US has variable sensitivity and specificity (sensitivity: 64–100%; specificity: 36–100%), decreasing the clinical diagnosis precision (24). Another article published in the same year reported specifically the sensitivity and specificity for each abnormal US finding using traditional detection method. The hypoechogenicity presented the best combination of diagnostic sensitivity and specificity. It is moderately sensitive sensitivity: 0.64 [95% CI, 0.56, 0.72] and highly specific specificity 0.82 [95% CI, 0.72, 0.90]. Additionally, neovascularity specificity 1.00 [95% CI, 0.97, 1.00)], calcifications specificity 0.97 [95% CI, 0.94, 0.99], and cortical irregularities specificity 0.96 [95% CI, 0.88, 0.99] have strong specificity for chronic lateral epicondylalgia (25). Our results, particularly for intrasubstance tear detection using the binary algorithm classification in both datasets, demonstrated a superior performance to the traditional US diagnosis methods. In the case of multilabel accuracy, the performance for both indicators was lowest results of specificity and sensitivity than the binary method. This situation could be explained because it is difficult to find a function that minimized the error for more classes. In other words, it increases the variability of the response variable.
For example, in the binary classification, the enthesopathy presented the lowest performance of the six machine learning classifiers. Notably, in the dependent binary relevance model from dataset B, our analysis showed that AUC was 0.647 [95% CI, 0.64, 0.65]. This result is quite similar to other reports with a sensitivity of 0.65 and specificity of 0.86 for this finding (77). However, our best result in the binary classification was detecting intrasubstance tear injuries using random forest algorithms. The performance showed an AUC of almost 1.0 (0.99) [95% CI, 0.99, 0.99] in contrast with the traditional US methods diagnosis for detecting common extensor tendon tear in the lateral with lower performances in sensitivity, specificity, and accuracy with 64.52, 85.19, and 72.73%, respectively (26).
However, one of our research strengths is the execution of machine learning models using multilabel detection for tendon injury findings. To date, few experiences had been published in the musculoskeletal area using artificial intelligence for tendon pattern detection. Some previous experiences have used Automatic ROI Detection and Classification of the Achilles Tendon ultrasound Images (69), and deep learning models for automatic tracking of the muscle-tendon junction or even measuring muscle atrophy (91). Other disciplines have also used other classification techniques such as neural networks or deep learning convolutional neural networks for image detection, demonstrating excellent results. However, CNN and DL have some drawbacks that should be analyzed when developing predictive models. First, it has been shown that DL requires large datasets to obtain better performance. To handle this, transfer learning is commonly used. However, DL architectures should also be re-trained and model parameters should be optimized, looking out for possible overfitting patterns. Second, DL architectures rely on the high computational performance, and it takes longer to prove results. In this sense, they are more complex to implement, especially in a clinical environment with a high demand for care, so improving diagnostic speed without compromising diagnostic accuracy is crucial for patients and the health system. Therefore, machine learning algorithms are advantageous when speed is of interest. In this case, the execution times of the proposed method were very low, allowing it to be easily implemented in a hospital scenario and re-trained with new data that is daily generated. Finally, the multilabel classification model differs from other algorithms most commonly used in image diagnosis due to the simplicity of its implementation.
This study also has some limitations. Firstly, our images come from the same institution, and patients presented similar socioeconomic conditions. Secondly, we included all static US images from common extensor tendon US per patient, not considering real-time and other structures or tissues. Thirdly, we included tendons with a definitive LET diagnosis, and we did not compare inter and intraobserver variability between radiologists. Fourthly, we considered all images without a region of interest, such as most of the publications. Nevertheless, in a short time, it could be a potential advantage. Finally, we did not repeat the US diagnosis to reduce retrospective bias. However, our radiologist presented more than 10 years of experience.
In conclusion, the random forest model presented the highest sensitivity and specificity in binary and multilabel classifiers for degenerative findings in the common extensor tendon. In particular, intrasubstance tear detections obtained the best performance. Machine learning models could be used to support the US diagnosis of LET.
Data availability statement
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
This study has been performed following the latest version of the Declaration of Helsinki and the Chilean scientific legislation. The study was approved by the “Comité de Ética Científico Adulto del Servicio Metropolitano Oriente de la ciudad de Santiago de Chile (SSMO).” The Ethics Committee required no informed consent given the nature of the study. The project was approved on August 7th, 2018. No approval number was recorded.
Author contributions
GD: conceptualization, data curation, formal analysis, investigation, methodology, validation, and writing the original draft. MT: data curation, formal analysis, investigation, and visualization. NG: validation, review, and editing. CG: review and editing. CJ: resources and validation. FF: conceptualization, formal analysis, investigation, supervision, review, and editing. All authors contributed to the article and approved the submitted version.
Funding
The authors received no financial support for the research and authorship. The publication was financially supported by the Universidad Mayor.
Acknowledgments
We are grateful for the kind collaboration and assistance of the Sports Medicine Data Science Center MEDS-PUCV. Special thanks to Sandra Mahecha from MEDS Clinic for her support during this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer AB-C declared a shared affiliation with one of the authors GD to the handling editor at the time of the review.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Stasinopoulos D, Johnson MI. “Lateral elbow tendinopathy” is the most appropriate diagnostic term for the condition commonly referred-to as lateral epicondylitis. Med Hypotheses. (2006) 67:1400–2. doi: 10.1016/j.mehy.2006.05.048
2. Struijs PAA, Buchbinder R, Green SE. Tennis elbow. In: Bhandari M editor. Evidence-Based Orthopedics. Hoboken, NJ: Wiley-Blackwell (2012). p. 787–95. doi: 10.1002/9781444345100.ch92
3. Shiri R, Viikari-Juntura E, Varonen H, Heliövaara M. Prevalence and determinants of lateral and medial epicondylitis: a population study. Am J Epidemiol. (2006) 164:1065–74. doi: 10.1093/aje/kwj325
4. Bunata RE, Brown DS, Capelo R. Anatomic factors related to the cause of tennis elbow. J Bone Joint Surg Am. (2007) 89:1955–63. doi: 10.2106/JBJS.F.00727
5. Coombes BK, Bisset L, Vicenzino B. Cold hyperalgesia associated with poorer prognosis in lateral epicondylalgia: a 1-year prognostic study of physical and PS. Clin J Pain. (2015) 31:30–5. doi: 10.1097/AJP.0000000000000078
6. Obuchowicz R, Bonczar M. Ultrasonographic Differentiation of Lateral Elbow Pain. Ultrasound Int Open. (2016) 2:E38–46. doi: 10.1055/s-0035-1569455
7. Sanders TL, Maradit Kremers H, Bryan AJ, Ransom JE, Smith J, Morrey BF. The epidemiology and health care burden of tennis elbow: a population-based study. Am J Sports Med. (2015) 43:1066–71. doi: 10.1177/0363546514568087
8. Roquelaure Y, Ha C, Leclerc A, Touranchet A, Sauteron M, Melchior M, et al. Epidemiologic surveillance of upper-extremity musculoskeletal disorders in the working population. Arthritis Care Res. (2006) 55:765–78. doi: 10.1002/art.22222
9. Gruchow HW, Pelletier D. An epidemiologic study of tennis elbow. Incidence, recurrence, and effectiveness of prevention strategies. Am J Sports Med. (1979) 7:234–8. doi: 10.1177/036354657900700405
10. Hong Q. Treatment of lateral epicondylitis: where is the evidence? Joint Bone Spine. (2004) 71:369–73. doi: 10.1016/j.jbspin.2003.05.002
11. Bisset LM, Vicenzino B. Physiotherapy management of lateral epicondylalgia. J Physiother. (2015) 61:174–81. doi: 10.1016/j.jphys.2015.07.015
12. Zwerus EL, Somford MP, Maissan F, Heisen J, Eygendaal D, Van Den Bekerom MP. Physical examination of the elbow, what is the evidence? A systematic literature review. Br J Sports Med. (2018) 52:1253–60. doi: 10.1136/bjsports-2016-096712
13. De Maeseneer M, Brigido MK, Antic M, Lenchik L, Milants A, Vereecke E, et al. Ultrasound of the elbow with emphasis on detailed assessment of ligaments, tendons, and nerves. Eur J Radiol. (2015) 84:671–81. doi: 10.1016/j.ejrad.2014.12.007
14. Draghi F, Danesino GM, de Gautard R, Bianchi S. Ultrasound of the elbow: examination techniques and US appearance of the normal and pathologic joint. J Ultrasound. (2007) 10:76–84. doi: 10.1016/j.jus.2007.04.005
15. Radunovic G, Vlad V, Micu MC, Nestorova R, Petranova T, Porta F, et al. Ultrasound assessment of the elbow. Med Ultrasonogr. (2012) 14:141–6.
16. Pierce JL, Nacey NC. Elbow Ultrasound. Curr Radiol Rep. (2016) 4:51. doi: 10.1007/s40134-016-0182-8
17. Barr LL, Babcock DS. Sonography of the normal elbow. Am J Roentgenol. (1991) 157:793–8. doi: 10.2214/ajr.157.4.1892039
18. Poltawski L, Jayaram V, Watson T. Measurement issues in the sonographic assessment of tennis elbow. J Clin Ultrasound. (2010) 38:196–204. doi: 10.1002/jcu.20676
19. Du Toit C, Stieler M, Saunders R, Bisset L, Vicenzino B. Diagnostic accuracy of power Doppler ultrasound in patients with chronic tennis elbow. Br J Sports Med. (2008) 42:872–6. doi: 10.1136/bjsm.2007.043901
20. Maffulli N, Regine R, Carrillo F, Capasso G, Minelli S. Tennis elbow: an ultrasonographic study in tennis players. Br J Sports Med. (1990) 24:151–5. doi: 10.1136/bjsm.24.3.151
21. Clarke AW, Ahmad M, Curtis M, Connell DA. Lateral elbow tendinopathy: correlation of ultrasound findings with pain and functional disability. Am J Sports Med. (2010) 38:1209–14. doi: 10.1177/0363546509359066
22. Longo UG, Franceschetti E, Rizzello G, Petrillo S, Denaro V. Elbow tendinopathy. Muscles Ligaments Tendons J. (2012) 2:115–20.
23. Heales LJ, Broadhurst N, Mellor R, Hodges PW, Vicenzino B. Diagnostic ultrasound imaging for lateral epicondylalgia: a case-control study. Med Sci Sports Exerc. (2014) 46:2070–6. doi: 10.1249/MSS.0000000000000345
24. Latham SK, Smith TO. The diagnostic test accuracy of ultrasound for the detection of lateral epicondylitis: a systematic review and meta-analysis. Orthop Traumatol Surg Res. (2014) 100:281–6. doi: 10.1016/j.otsr.2014.01.006
25. Dones VC, Grimmer K, Thoirs K, Suarez CG, Luker J. The diagnostic validity of musculoskeletal ultrasound in lateral epicondylalgia: a systematic review. BMC Med Imaging. (2014) 4:10. doi: 10.1186/1471-2342-14-10
26. Bachta A, Rowicki K, Kisiel B, Żabicka M, Elert-Kopeæ S, Płomiński J, et al. Ultrasonography versus magnetic resonance imaging in detecting and grading common extensor tendon tear in chronic lateral epicondylitis. PLoS One. (2017) 12:e0181828. doi: 10.1371/journal.pone.0181828
27. Matthews W, Ellis R, Furness J, Hing W. Classification of tendon matrix change using ultrasound imaging: a systematic review and meta-analysis. Ultrasound Med Biol. (2018) 44:2059–80. doi: 10.1016/j.ultrasmedbio.2018.05.022
28. Kermany DS, Goldbaum M, Cai W, Valentim CCS, Liang H, Baxter SL, et al. Identifying medical diagnoses and treatable diseases by image-based deep learning. Cell. (2018) 172:1122–31. doi: 10.1016/j.cell.2018.02.010
29. Hosny A, Parmar C, Quackenbush J, Schwartz LH, Aerts HJWL. Artificial intelligence in radiology. Nat Rev Cancer. (2018) 18:500–10. doi: 10.1038/s41568-018-0016-5
30. Langlotz CP, Allen B, Erickson BJ, Kalpathy-Cramer J, Bigelow K, Cook TS, et al. A roadmap for foundational research on artificial intelligence in medical imaging: from the 2018 NIH/RSNA/ACR/The Academy workshop. Radiology. (2019) 291:781–91. doi: 10.1148/radiol.2019190613
31. Liew C. The future of radiology augmented with artificial intelligence: a strategy for success. Eur J Radiol. (2018) 102:152–6. doi: 10.1016/j.ejrad.2018.03.019
32. Cascianelli S, Scialpi M, Amici S, Forini N, Minestrini M, Fravolini M, et al. Role of Artificial Intelligence Techniques (Automatic Classifiers) in Molecular Imaging Modalities in Neurodegenerative Diseases. Curr Alzheimer Res. (2017) 14:198–207. doi: 10.2174/1567205013666160620122926
33. Liu X, Chen K, Wu T, Weidman D, Lure F, Li J. Use of multimodality imaging and artificial intelligence for diagnosis and prognosis of early stages of Alzheimer’s disease. Transl Res. (2018) 194:56–97. doi: 10.1016/j.trsl.2018.01.001
34. Zhe S, Xu Z, Qi Y, Yu P. Sparse Bayesian multiview learning for simultaneous association discovery and diagnosis of Alzheimer’s disease. In: Proceedings of the National Conference on Artificial Intelligence. Palo Alto, CA: AAAI Press (2015). p. 1966–72. doi: 10.1609/aaai.v29i1.9473
35. Rajpurkar P, Irvin J, Ball RL, Zhu K, Yang B, Mehta H, et al. Deep learning for chest radiograph diagnosis: a retrospective comparison of the CheXNeXt algorithm to practicing radiologists. PLoS Med. (2018) 15:e1002686. doi: 10.1371/journal.pmed.1002686
36. Hwang EJ, Park S, Jin KN, Kim JI, Choi SY, Lee JH, et al. Development and Validation of a Deep Learning-Based Automated Detection Algorithm for Major Thoracic Diseases on Chest Radiographs. JAMA Netw Open. (2019) 2:e191095. doi: 10.1001/jamanetworkopen.2019.1095
37. Nam JG, Park S, Hwang EJ, Lee JH, Jin KN, Lim KY, et al. Development and validation of deep learning-based automatic detection algorithm for malignant pulmonary nodules on chest radiographs. Radiology. (2019) 290:218–28. doi: 10.1148/radiol.2018180237
38. Lee H, Huang C, Yune S, Tajmir SH, Kim M, Do S. Machine friendly machine learning: interpretation of computed tomography without image reconstruction. Sci Rep. (2019) 9:15540. doi: 10.1038/s41598-019-51779-5
39. Itu L, Rapaka S, Passerini T, Georgescu B, Schwemmer C, Schoebinger M, et al. A machine-learning approach for computation of fractional flow reserve from coronary computed tomography. J Appl Physiol. (2016) 121:42–52. doi: 10.1152/japplphysiol.00752.2015
40. Kolossváry M, De Cecco CN, Feuchtner G, Maurovich-Horvat P. Advanced atherosclerosis imaging by CT: radiomics, machine learning and deep learning. J Cardiovasc Comput Tomogr. (2019) 13:274–80. doi: 10.1016/j.jcct.2019.04.007
41. Al’Aref SJ, Anchouche K, Singh G, Slomka PJ, Kolli KK, Kumar A, et al. Clinical applications of machine learning in cardiovascular disease and its relevance to cardiac imaging. Eur Heart J. (2019) 40:1975–86. doi: 10.1093/eurheartj/ehy404
42. Arbabshirani MR, Fornwalt BK, Mongelluzzo GJ, Suever JD, Geise BD, Patel AA, et al. Advanced machine learning in action: identification of intracranial hemorrhage on computed tomography scans of the head with clinical workflow integration. NPJ Digit Med. (2018) 1:9. doi: 10.1038/s41746-017-0015-z
43. Cruz JA, Wishart DS. Applications of machine learning in cancer prediction and prognosis. Cancer Inform. (2006) 2:59–78. doi: 10.1177/117693510600200030
44. Wang Z, Yu G, Kang Y, Zhao Y, Qu Q. Breast tumor detection in digital mammography based on extreme learning machine. Neurocomputing. (2014) 128:175–84. doi: 10.1016/j.neucom.2013.05.053
45. Ramos-Pollán R, Guevara-López MA, Suárez-Ortega C, Díaz-Herrero G, Franco-Valiente JM, Rubio-Del-Solar M, et al. Discovering mammography-based machine learning classifiers for breast cancer diagnosis. J Med Syst. (2012) 36:2259–69. doi: 10.1007/s10916-011-9693-2
46. Xie W, Li Y, Ma Y. Breast mass classification in digital mammography based on extreme learning machine. Neurocomputing. (2016) 173:930–41. doi: 10.1016/j.neucom.2015.08.048
47. Hamidinekoo A, Denton E, Rampun A, Honnor K, Zwiggelaar R. Deep learning in mammography and breast histology, an overview and future trends. Med Image Anal. (2018) 47:45–67. doi: 10.1016/j.media.2018.03.006
48. Fan J, Wu Y, Yuan M, Page D, Liu J, Ong IM, et al. Structure-leveraged methods in breast cancer risk prediction. J Mach Learn Res. (2016) 17:85.
49. Arevalo J, González FA, Ramos-Pollán R, Oliveira JL, Guevara Lopez MA. Representation learning for mammography mass lesion classification with convolutional neural networks. Comput Methods Programs Biomed. (2016) 127:248–57. doi: 10.1016/j.cmpb.2015.12.014
50. Al-Hadidi MR, Alarabeyyat A, Alhanahnah M. Breast cancer detection using K-nearest neighbor machine learning algorithm. In: Proceedings 2016 9th International Conference on Developments in eSystems Engineering, DeSE. Liverpool: IEEE (2016). doi: 10.1109/DeSE.2016.8
51. Wang J, Yang X, Cai H, Tan W, Jin C, Li L. Discrimination of breast cancer with microcalcifications on mammography by deep learning. Sci Rep. (2016) 6:27327. doi: 10.1038/srep27327
52. Shen J, Zhang CJP, Jiang B, Chen J, Song J, Liu Z, et al. Artificial intelligence versus clinicians in disease diagnosis: systematic review. J Med Internet Res. (2019) 7:e10010. doi: 10.2196/10010
53. Gyftopoulos S, Lin D, Knoll F, Doshi AM, Rodrigues TC, Recht MP. Artificial intelligence in musculoskeletal imaging: current status and future directions. Am J Roentgenol. (2019) 213:506–13. doi: 10.2214/AJR.19.21117
54. Chea P, Mandell JC. Current applications and future directions of deep learning in musculoskeletal radiology. Skeletal Radiol. (2020) 49:183–97. doi: 10.1007/s00256-019-03284-z
55. Tomita N, Cheung YY, Hassanpour S. Deep neural networks for automatic detection of osteoporotic vertebral fractures on CT scans. Comput Biol Med. (2018) 98:8–15. doi: 10.1016/j.compbiomed.2018.05.011
56. Roth HR, Wang Y, Yao J, Lu L, Burns JE, Summers RM. Deep convolutional networks for automated detection of posterior-element fractures on spine CT. In: Medical Imaging 2016: Computer-Aided Diagnosis. Bellingham, WA: SPIE (2016). doi: 10.1117/12.2217146
57. Pranata YD, Wang KC, Wang JC, Idram I, Lai JY, Liu JW, et al. Deep learning and SURF for automated classification and detection of calcaneus fractures in CT images. Comput Methods Programs Biomed. (2019) 171:27–37. doi: 10.1016/j.cmpb.2019.02.006
58. Couteaux V, Si-Mohamed S, Nempont O, Lefevre T, Popoff A, Pizaine G, et al. Automatic knee meniscus tear detection and orientation classification with Mask-RCNN. Diagn Interv Imaging. (2019) 100:235–42. doi: 10.1016/j.diii.2019.03.002
59. Bien N, Rajpurkar P, Ball RL, Irvin J, Park A, Jones E, et al. Deep-learning-assisted diagnosis for knee magnetic resonance imaging: development and retrospective validation of MRNet. PLoS Med. (2018) 15:e1002699. doi: 10.1371/journal.pmed.1002699
60. Roblot V, Giret Y, Bou Antoun M, Morillot C, Chassin X, Cotten A, et al. Artificial intelligence to diagnose meniscus tears on MRI. Diagn Interv Imaging. (2019) 100:243–9. doi: 10.1016/j.diii.2019.02.007
61. Liu F, Zhou Z, Samsonov A, Blankenbaker D, Larison W, Kanarek A, et al. Deep learning approach for evaluating knee MR images: achieving high diagnostic performance for cartilage lesion detection. Radiology. (2018) 289:160–9. doi: 10.1148/radiol.2018172986
62. Koitka S, Demircioglu A, Kim MS, Friedrich CM, Nensa F. Ossification area localization in pediatric hand radiographs using deep neural networks for object detection. PLoS One. (2018) 13:e0207496. doi: 10.1371/journal.pone.0207496
63. Larson DB, Chen MC, Lungren MP, Halabi SS, Stence NV, Langlotz CP. Performance of a deep-learning neural network model in assessing skeletal maturity on pediatric hand radiographs. Radiology. (2018) 287:313–22. doi: 10.1148/radiol.2017170236
64. Tiulpin A, Thevenot J, Rahtu E, Lehenkari P, Saarakkala S. Automatic knee osteoarthritis diagnosis from plain radiographs: a deep learning-based approach. Sci Rep. (2018) 8:1727. doi: 10.1038/s41598-018-20132-7
65. Brattain LJ, Telfer BA, Dhyani M, Grajo JR, Samir AE. Machine learning for medical ultrasound: status, methods, and future opportunities. Abdom Radiol. (2018) 43:786–99. doi: 10.1007/s00261-018-1517-0
66. Martin K. Special issue on education and training in ultrasound. Ultrasound. (2015) 23:5. doi: 10.1177/1742271X14568074
67. van Sloun RJG, Cohen R, Eldar YC. Deep learning in ultrasound imaging. Proc IEEE. (2019) 108:11–29. doi: 10.1109/JPROC.2019.2932116
68. Ihnatsenka B, Boezaart AP. Ultrasound: basic understanding and learning the language. Int J Shoulder Surg. (2010) 4:55–62. doi: 10.4103/0973-6042.76960
69. Benrabha J, Meziane F. Automatic ROI detection and classification of the achilles tendon ultrasound images. In: Proceedings of the 1st International Conference on Internet of Things and Machine Learning. Liverpool: ACM (2017). p. 1–7. doi: 10.1145/3109761.3158381
70. Baka N, Leenstra S, van Walsum T. Random Forest-Based Bone Segmentation in Ultrasound. Ultrasound Med Biol. (2017) 43:2426–37. doi: 10.1016/j.ultrasmedbio.2017.04.022
71. Berton F, Cheriet F, Miron MC, Laporte C. Segmentation of the spinous process and its acoustic shadow in vertebral ultrasound images. Comput Biol Med. (2016) 72:201–11. doi: 10.1016/j.compbiomed.2016.03.018
72. Kapinski N, Zielinski J, Borucki BA, Trzcinski T, Ciszkowska-Lyson B, Nowinski KS. Estimating achilles tendon healing progress with convolutional neural networks. In: Frangi A, Schnabel J, Davatzikos C, Alberola-López C, Fichtinger G editors. Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics). Cham: Springer (2018). doi: 10.1007/978-3-030-00934-2_105
73. Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Int J Surg. (2014) 12:1500–24. doi: 10.1016/j.ijsu.2014.07.014
74. Palaniswamy V, Ng SK, Manickaraj N, Ryan M, Yelland M, Rabago D, et al. Relationship between ultrasound detected tendon abnormalities, and sensory and clinical characteristics in people with chronic lateral epicondylalgia. PLoS One. (2018) 13:e0205171. doi: 10.1371/journal.pone.0205171
75. Droppelmann G, Feijoo F, Greene C, Tello M, Rosales J, Yáñez R, et al. Ultrasound findings in lateral elbow tendinopathy: a retrospective analysis of radiological tendon features [version 1; peer review: awaiting peer review]. F1000Res. (2022) 11:44. doi: 10.12688/f1000research.73441.1
76. Connell D, Burke F, Coombes P, McNealy S, Freeman D, Pryde D, et al. Sonographic examination of lateral epicondylitis. Am J Roentgenol. (2001) 176:777–82. doi: 10.2214/ajr.176.3.1760777
77. Levin D, Nazarian LN, Miller TT, O’Kane PL, Feld RI, Parker L, et al. Lateral epicondylitis of the elbow: US findings. Radiology. (2005) 237:230–4. doi: 10.1148/radiol.2371040784
79. Coombes BK, Bisset L, Vicenzino B. Management of lateral elbow tendinopathy: one size does not fit all. J Orthop Sports Phys Ther. (2015) 45:938–49. doi: 10.2519/jospt.2015.5841
80. Vaquero-Picado A, Barco R, Antuña SA. Lateral epicondylitis of the elbow. EFORT Open Rev. (2016) 1:391–7. doi: 10.1302/2058-5241.1.000049
81. Sommer C, Gerlich DW. Machine learning in cell biology-teaching computers to recognize phenotypes. J Cell Sci. (2013) 126:5529–39. doi: 10.1242/jcs.123604
82. Sun Y, Li L, Zheng L, Hu J, Li W, Jiang Y, et al. Image classification base on PCA of multi-view deep representation. J Vis Commun Image Represent. (2019) 62:253–8. doi: 10.1016/j.jvcir.2019.05.016
83. Zhang Z, Sejdiæ E. Radiological images and machine learning: trends, perspectives, and prospects. Comput Biol Med. (2019) 108:354–70. doi: 10.1016/j.compbiomed.2019.02.017
84. Buchser W. Assay development guidelines for image-based high content screening, high content analysis and high content imaging. In: Markossian S, Grossman A, Brimacombe K editors. Assay Guidance Manual. Bethesda, MD: Eli Lilly & Company (2014).
85. Kumar G, Bhatia PK. A detailed review of feature extraction in image processing systems. In: 2014 Fourth International Conference on Advanced Computing & Communication Technologies. Rohtak: IEEE (2014). p. 5–12. doi: 10.1109/ACCT.2014.74
86. Nugroho HA, Rahmawaty M, Triyani Y, Ardiyanto I, Choridah L, Indrastuti R. Texture analysis and classification in ultrasound medical images for determining echo pattern characteristics. In: 2017 IEEE International Conference on System Engineering and Technology. Malaysia: IEEE (2017). p. 23–6. doi: 10.1109/ICSEngT.2017.8123414
88. Bosch B. Machine Learning in R. Package ‘mlr’. (2021). Available online at: https://cran.r-project.org/web/packages/mlr/mlr.pdf (accessed September 8, 2021).
89. Breiman L, Cutler A. Breiman and Cutler’s Random Forests for Classification and Regression. Package ‘randomForest’. (2022). Available online at: https://cran.rproject.org/web/packages/randomForest/randomForest.pdf (accessed June 15, 2022).
90. Sorower M. A Literature Survey on Algorithms for Multi-Label Learning. Corvallis: Oregon State University (2010).
Keywords: AUC curve, diagnosis, random forest, tennis elbow, ultrasound
Citation: Droppelmann G, Tello M, García N, Greene C, Jorquera C and Feijoo F (2022) Lateral elbow tendinopathy and artificial intelligence: Binary and multilabel findings detection using machine learning algorithms. Front. Med. 9:945698. doi: 10.3389/fmed.2022.945698
Received: 16 May 2022; Accepted: 29 August 2022;
Published: 23 September 2022.
Edited by:
Jingjing You, The University of Sydney, AustraliaReviewed by:
Kurt Svärdsudd, Uppsala University, SwedenAndrés Bueno-Crespo, Catholic University San Antonio of Murcia, Spain
Copyright © 2022 Droppelmann, Tello, García, Greene, Jorquera and Feijoo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guillermo Droppelmann, Z3VpbGxlcm1vLmRyb3BwZWxtYW5uQG1lZHMuY2w=