 Ruperto González-Pérez
Ruperto González-Pérez Paloma Poza-Guedes
Paloma Poza-Guedes Elena Mederos-Luis1
Elena Mederos-Luis1- 1Allergy Department, Hospital Universitario de Canarias, Santa Cruz de Tenerife, Spain
- 2Severe Asthma Unit, Hospital Universitario de Canarias, Santa Cruz de Tenerife, Spain
Background: Atopic dermatitis (AD) is regarded as a chronic systemic disease which is characterized by a robust overexpression of type 2 related cytokines, with increased total IgE levels and a concomitant sensitization to common allergens. Dupilumab, a fully human monoclonal antibody (mAb) to IL-4Rα that inhibits both IL-4 and IL-13 signaling, has previously shown a marked and rapid improvement when treating the moderate-to-severe forms of AD. We sought to evaluate the real-world evidence (RWE) of dupilumab in the modulation of total and specific IgE (sIgE) serum levels to a panel of molecular house dust mites (HDM) and storage mites (SM) allergens in patients with severe AD.
Methods: Demographic and clinical data for severe AD adult patients receiving dupilumab treatment (300 mg every 2 weeks) were reviewed. Mean (standard deviations SD) values and percent changes from baseline in total and sIgE to the complete HDM and SM extracts, and 14 individual molecular allergens were measured over 52 weeks.
Results: Significant (p < 0.05) changes in mean total IgE levels were observed from baseline to week-52 after treatment with dupilumab. Despite no changes were found in sIgE against the extract of HDM during the 52-week treatment with dupilumab, baseline mean levels from 7 out of 14 individual molecular mite allergens -Der p 1, Der p 2, Der p 5, Der p 7, Der p 21, Der p 23, and Lep d 2- were significantly (p < 0.05) decreased—after 52 weeks of treatment with dupilumab.
Conclusions: Dupilumab therapy for 52 weeks resulted in a profound reduction in blood levels of total IgE and allergen-specific IgE to both HDM and SM at the molecular level in adults with severe AD under RWE conditions. The potential benefits of these concomitant immunomodulatory effects after treatment with dupilumab should be explored to a greater extent.
Introduction
Atopic dermatitis (AD), an inflammatory, chronically relapsing and intensely pruritic skin disease, is nowdays considered a systemic Type 2 inflammation driven disease, enclosing a specific CD4+ T helper type (Th) 2 cell response and the activation of several T-cell lineages, such as Th1, Th17/interleukin (IL)-23, and Th22 (1, 2). Former clinical and experimental studies indicate that house dust mites (HDM) can play a critical role in the pathogenesis of AD in sensitized and genetically predisposed subjects (3, 4). The introduction of Precision Allergy Molecular Diagnosis (PAMD@) has a major effect on analytic specificity and allergy diagnosis, to a comprehensive assessment of the patient's specific IgE (sIgE) binding to a panel of individual allergens (5).
Dupilumab, the first fully human monoclonal IgG4 antibody inhibiting the signaling of IL-4 and IL-13, significantly reduces type 2 biomarkers in circulating serum and lesional skin (6, 7). Nowadays, changes in allergen-specific IgE serum levels have only been described for allergen extracts in subjects with moderate-to-severe AD from clinical trials with dupilumab (8, 9). Herein, we aimed to investigate the real-world evidence (RWE) effects of after 52 weeks of treatment with dupilumab in total and mite-molecular IgE serum levels in a cohort of individuals afflicted with the severe extrinsic AD phenotype subjected to a high local environmental mite exposure (10, 11).
Materials and methods
Subjects
We consecutively recruited patients from May 2020 to November 2021 from the Outpatient Allergy Clinic & Severe Asthma Unit at Hospital Universitario de Canarias (Tenerife, Spain). Eligibility criteria included subjects in treatment with dupilumab 300 mg every 2 weeks (300 mg-q2w) for 52 weeks with a clinician confirmed diagnosis of severe AD with the T2-high endotype (extrinsic subtype) according to current guidelines (12).
Clinical data -including Scoring Atopic Dermatitis (SCORAD), Eczema Area and Severity Index (EASI) score, Investigator's Global Assessment (IGA) and peak pruritus numerical rating scale (PNRS)- were retrieved from the patients' medical records 4 weeks before treatment with dupilumab 300 mg-q2w (Time 0, T0), 26 weeks after starting therapy with dupilumab (Time 1, T1), 32 weeks after dupilumab (Time 2, T2) and finally after completing 52 weeks with dupilumab (Time 3, T3). The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee of CEIC Hospital Universitario de Canarias, Tenerife, Spain with the reference number P.I.-2017/72 on 30 October 2017.
Pregnant and breast-feeding women and patients receiving allergen immunotherapy (AIT), and/or other biologics apart from dupilumab were excluded from the investigation. Blood specimens were collected for all subjects, identified with a code label, stored at −40°C and immediately thawed in preparation for in vitro analysis to evaluate median values and percent changes from baseline in total and allergen-specific IgE over the 52 weeks follow up.
Skin prick test and mite allergenic extracts
Percutaneous tests were performed according to European standards (13) with standardized allergenic extracts of Dermatophagoides pteronyssinus, Blomia tropicalis, Lepidoglyphus destructor, and Tyrophagus putrescentiae (Diater, Madrid, Spain). Saline (0.9%) and histamine (10 mg/ml) were respectively included as negative and positive controls. Antihistamines were drop back seven days in advance to each SPT, with wheal diameters >3 mm considered positive after a 20 min immediate reading.
Serological workup
Total IgE levels, sIgE to the whole D. pteronyssinus and B. tropicalis extract, and 14 individual molecular allergens -Der p 1, Der p 2, Der p 5, Der p 7, Der p 10, Der p 11, Der p 20, Der p 21, Der p 23, Blo t 5, Blo t 10, Blo t 21, Lep d 2, and Tyr p 2- were measured by a MedTech company (MacroArray Diagnostics, Viena, Austria), according to the manufacturer's instructions. In brief, the Allergy Explorer (ALEX®) test is a multiplex array containing 282 reagents (157 extractive allergens and 125 molecular components). The different allergens and components are coupled onto polystyrene nano-beads, and then the allergen beads are deposited on a nitrocellulose membrane, as previously published (14). Total IgE levels were expressed in international units per unit volume (IU/mL), sIgE levels were expressed in kUA/L. Values ≥0.35 kUA/L were regarded as positive.
Statistical data
Demographic features were summarized by means and standard deviations for continuous variables and percentages for categorical variables. To compare differences analysis of variance, Kruskal–Wallis, Mann–Whitney U and Chi-square tests are required for parametric continuous, non-parametric continuous, and categorical variables respectively. A P-value of <0.05 was considered statistically significant. All statistical data were analyzed using GraphPad Prism version 8.0.0 for Windows, GraphPad Software, La Jolla, California, USA.
Results
Demographic characteristics of patients
We finally selected 12 (out of 22) European-American ethnicity subjects from the outpatient allergy office –10 males and 2 females, median age 27.0 (19–57) years of age- who met the inclusion criteria and a previous clinician-confirmed diagnosis of AD ongoing for more than 15 years. Considering SCORAD >40 and EASI >21 as markers for the severe forms of (15), all selected subjects showed upon inclusion a median SCORAD and EASI of 84.5 (54.0–96.4) and 62.40 (27.0–70.0), respectively. A median Investigator's Global Assessment (IGA) score of 4 (severe on a scale of 0–4) and a median peak pruritus numerical rating scale (NRS) of 8 (severe on a scale of 0–10) was also quantified for all subjects at baseline.
More than 80% (10 out 12 subjects) had a former family history of atopy and regarding comorbidities, 91.66% patients were afflicted with allergic rhinitis and/or asthma, and 25.0% had a clinically confirmed food allergy (milk, seafood and/or tree nuts) associated (Table 1).
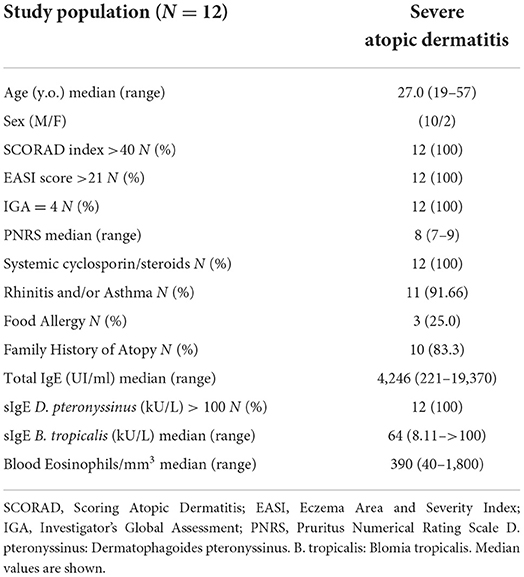
Table 1. Descriptive statistics at baseline.
Concerning the need of systemic medication for AD at baseline, patients were in treatment with either cyclosporin (75% of subjects with a median dose of 75 mg/day), steroids (16.6% with a median dose of prednisone 15 mg/day) or azathioprine (50 mg/day in 1 individual).
Quantification of basal total IgE, SPT, and SIgE to the extract of D. pteronyssinus and Blomia tropicalis and mite molecular profile
All patients confirming their eligibility for the study showed a marked Th2-high endotype -featuring elevated peripheral eosinophil count, total IgE and aeroallergen-specific IgE levels. Basal total IgE (before treatment with dupilumab) ranged from 221.0 to 19.370.0 IU/mL, with a median value of 3765.0 IU/mL. Basal median blood eosinophils showed a value of 390 (40–1,800) eosinophils/μL. All enrolled individuals had a positive SPT and serum sIgE (≥0.35 kU/l) against both D. pteronyssinus and B. tropicalis (crude extract), with median values of >100 and 64 (8.11 to>100) kU/L, respectively (Table 1).
Globally, all patients were simultaneously sensitized to 3 or more of the 14 mite allergens included in the customized molecular panel. Regarding the frequency of sIgE-binding to individual molecular allergens, Der p 2, Der p 21, and Der p 23 led the sIgE immunoresponse in all individuals (100%), followed by Der p 1 and Der p 5 (83.33%) subjects, while 75.0% individuals were sensitized to Der p 7. Minor allergens as Der p 10 were only present in 8.33%, while Der p 11 and Der p 20 were found in 16.66% of the investigated serum samples. Considering storage mites, Lep d 2 (58.8%) and Blo t 5 (50.0%) were the most frequently identified allergens in the current cohort.
In relation to the aggregation of allergens, despite the repertoire of IgE-recognized molecules was highly polyclonal, a preponderant specific pattern could not be found (Table 2). The quantitative basal mean values of sIgE (kU/L) were the highest for Der p 2 (52.64 ± 5.28), followed by Der p 23 (45.0 ± 12.06), Der p 21 (43.71 ± 22.79), Der p 5 (42.25 ± 16.64), Der p 1 (24.6 ± 17.87), Blo t5 22. 32 ± 13.62 Der p 7 (20.05 ± 20.44), and Lep d 2 (13.95 ± 11.56).

Table 2. Specific IgE profiles to 14 allergen molecules from Dermatophagoides pteronyssinus, Blomia tropicalis, Lepidoglyphus destructor, and Tyrophagus putrescentiae in subjects afflicted with severe atopic dermatitis tested with microarray.
Evolution of clinical severity and pruritus after therapy with dupilumab 300 mg-Q2w for 52 weeks
A significant improvement in both SCORAD index and EASI score was reported at weeks 26 and 52 in all subjects compared to their baseline scores (Table 3). In addition, at weeks 26 and 52, 83.33% patients receiving dupilumab had an IGA score of 0 or 1 and an improvement of 2 points or more on the IGA from the baseline score. Also, at weeks 26 and 52, a reduction of at least 5 points in the peak score on the PNRS was found in all patients after treatment with dupilumab in contrast to their baseline scores (P < 0.05 for all comparisons). Concomitant systemic medication was discontinued (ciclosporin, steroids and/or azathioprine) in all subjects at week 52 after treatment with dupilumab.
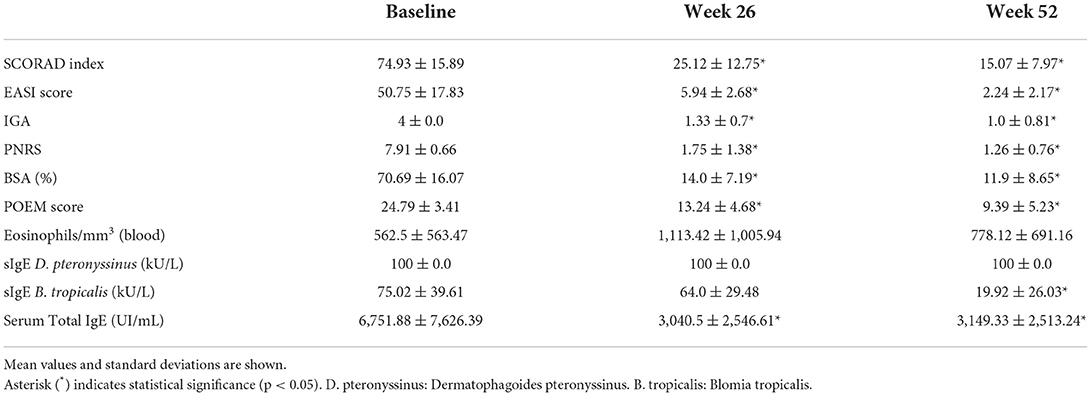
Table 3. Scoring features and routine laboratory testing in patients (n = 12) with severe atopic dermatitis at baseline and follow-up after 26 and 52 weeks of treatment with dupilumab 300 mg every 2 weeks for 52 weeks.
Total serum IgE and mite molecular responses after treatment with dupilumab 300 mg every 2 weeks for 52 weeks
Significant (p < 0.05) changes in mean total IgE levels were observed from baseline (6,751.88 ± 7,626.39 IU/mL) to week-26 (3,040.5 ± 2,546.61 IU/mL) and week-52 (3,149.33 ± 2,513.24 IU/mL) after treatment with dupilumab. No changes were found in sIgE against the extract of D. pteronyssinus-as mean values remained >100 kU/L- during the 52-week treatment with dupilumab. Mean sIgE levels against the extract of B. tropicalis were significantly reduced from baseline (75.02 ± 39.61 kU/L) to (19.92 ± 26.03 kU/L) by week 52.
Interestingly, baseline mean levels (kU/L) from 7 out of 14 (50%) individual molecular mite allergens -Der p 1 (24.6 ± 17.87), Der p 2 (52.64 ± 5.28), Der p 5 (42.25 ± 16.64), Der p 7 (20.05 ± 20.44), Der p 21 (43.71 ± 22.79), Der p 23 (45.0 ± 12.06) and Lep d 2 (13.95 ± 11.56)- were significantly (p < 0.05) decreased -Der p 1 (11.82 ± 11.5), Der p 2 (28.63 ± 15.64), Der p 5 (25.74 ± 18.02), Der p 7 (14.78 ± 16.08), Der p 21 (29.31 ± 23.31), Der p 23 (27.0 ± 11.99), and Lep d 2 (3.72 ± 4.35)- after 52 weeks of treatment with dupilumab. In addition, despite no statistical significance was reached, even a decreased in the mean sIgE levels was confirmed for Der p 10, Der p 11 and Der p 20 (regarded as minor allergens from D. pteronyssinus), and also for the major allergens (Blo t 5 and Blo t 21) from B. tropicalis and T. putrescentiae (Tyr p 2), respectively, after 52 weeks of treatment with dupilumab (Figure 1).
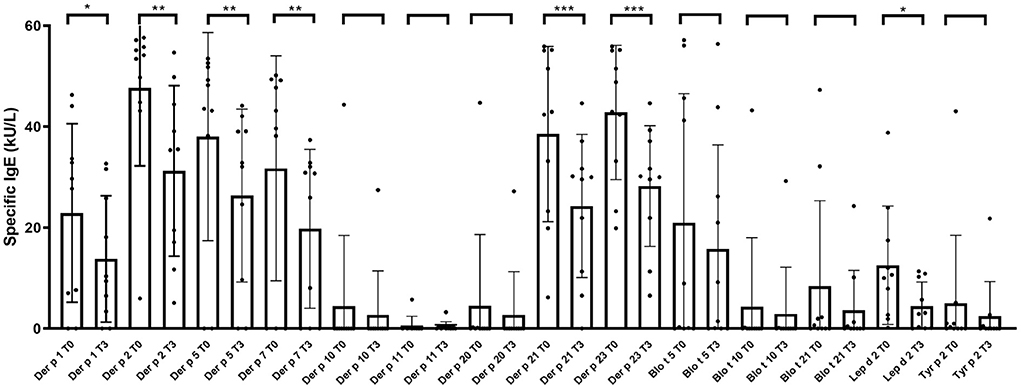
Figure 1. Evolution of serum specific IgE profiles to 14 allergen molecules from Dermatophagoides pteronyssinus, Blomia tropicalis, Lepidoglyphus destructor, and Tyrophagus putrescentiae in subjects afflicted with severe atopic dermatitis tested with microarray, before (T0) and after treatment with dupilumab 300 mg every 2 weeks for 52 weeks (T3). Asterisk indicate statistical significance (*p < 0.05; **P < 0.01; and ***p < 0.005).
Safety and adverse events
Two subjects (16.66%) had adverse events developing mild conjunctivitis after 16-weeks of treatment with dupilumab. Conjunctivitis was controlled after using moisturizing sodium hyaluronate eye drops. None of the patients had to discontinue therapy with dupilumab during the study period.
Discussion
The identification of in vitro biomarkers -including the reduction of sIgE- and their direct association with disease severity and the potential prediction of severe disease are of great clinical interest in monitoring the effects of targeted therapy for different allergic conditions (16–20).
Previous studies provide evidence that AD and allergic asthma might share related drivers -i.e., IL-4 and IL-13- and that both conditions may benefit from a common therapeutic inhibition of these Th2 cytokines with dupilumab (21).
The contributing role of mites and a high prevailing capacity for sIgE sensitization -based on the frequency of IgE-binding- has been previously described in the pathogenesis and severity of AD in populations from diverse geographical areas and ethnicities (22, 23). In the present investigation, and in addition to the supporting clinical outcomes after therapy with dupilumab, a significant immunomodulation in the sIgE molecular profile to major and mid-tier mite allergens has been found in a RWE subset of patients afflicted with severe AD. The current discernment of B cell activation and differentiation during development and later persistence or resolution of human IgE-mediated allergic diseases is still limited. The lifespan of IgE plasma cells and the conditions in which new IgE plasma cells are generated are essential questions in the recognition of potential pathways for therapeutic intervention in allergic disease (24). In respect to perennial allergens (i.e., mites), persistent IgE could be attributed to long-lived IgE plasma cells or short-lived IgE plasma cells continuously generated from a memory reservoir. As plasmablasts originate from non-IgE memory cells, it has been speculated that dupilumab resulted in a marked reduction of serum allergen-specific IgE -an IL-4 and IL-13-dependent process- as a large portion of circulating IgE in AD patients derives from short-lived IgE plasma cells elicited in recent class-switching events (25).
The disease-modifying effects of AIT are also associated with immune modulation of the innate and adaptive immune responses. In fact, successful AIT has been related to the induction of allergen-specific blocking IgG antibodies, inhibiting allergen-induced mast cell and basophil degranulation and IgE-facilitated allergen presentation to T cells (26–28). In addition to AIT, it has been shown that circulating IgE can be effectively reduced by the binding of omalizumab –a recombinant humanized monoclonal anti-IgE-antibody– to the binding site of the high affinity FcεRI receptor on the IgE antibody priming the downregulation of the FcεRI receptor on basophils and mast cells (29). Interestingly, despite both AIT and omalizumab have confirmed a clinical benefit in a variety of IgE-mediated allergic diseases -i.e., allergic rhinitis and/or asthma and chronic spontaneous urticaria- their role in AD is still controversial (30–32). In the present report, the significant reduction in the molecular sIgE to mite allergens may be only speculated as a part in the mechanistic puzzle to a favored outcome after dupilumab therapy in severe AD individuals. Furthermore, although no changes in the in vitro sIgE to the extract of D. pteronyssinus were identified -as median sIgE values remained >100 kU/L during the 52 weeks of treatment with dupilumab-, PAMD@ unveiled a significant decrease in major and mid-tier molecular allergens from D. pteronyssinus. These observations would suggest that only sIgE antibody responses to the serodominant -but not those molecules with the lowest prevalence- are being continually stimulated by Th2 dependent immune responses. The current research has potential bias as the study was performed in a single center, with a limited number of subjects, and data from T2 could not be retrieved in 5 subjects due to local COVID-19 pandemic restrictions. Also, the identification of minor molecules as Der p 18, Der f 13, Der f 14, Der f 32, and Der f Alt a 10, regarded as mite immunologic markers for AD, was neither assessed in the intended population (33, 34).
Despite previous trials with dupilumab treatment resulted in a prompt decrease of total and allergen serum sIgE in moderate-to-severe AD (35), this is to our knowledge the first RWE report to confirm a significant and sustained reduction in blood levels of mite sIgE at the molecular level after 52 weeks of treatment with dupilumab in a selected cohort of adult patients with severe AD. In line with recent reports, (36–38), our data suggest that a long-term clinical benefit could be sustained even after discontinuing dupilumab therapy in adult patients with AD, similar to the sustained decreases in serum sIgE levels and long-term clinical improvements observed in subjects with allergic rhinitis and/or asthma during and after AIT. Either these results may extend the potential benefit of dupilumab, not only from severe AD to other coexisting atopic conditions but also in the so-called atopic march, it is an issue that certainly deserves further research.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Institutional Ethics Committee of CEIC Hospital Universitario de Canarias, Tenerife, Spain with the reference number P.I.-2017/72 on October 30, 2017. The Ethics Committee waived the requirement of written informed consent for participation.
Author contributions
RG-P and PP-G: conceptualization, data curation, writing—original draft preparation, and funding acquisition. RG-P, PP-G, and EM-L: methodology. PP-G: software. PP-G and IS-M: validation and formal analysis. IS-M, RG-P, PP-G, and EM-L: investigation and writing—review and editing. IS-M: resources. RG-P, PP-G, and IS-M: project administration. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Fundación Canaria Instituto de Investigación Sanitaria de Canarias (FIISC), Servicio Canario de Salud, grant number OA17/042.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AD, Atopic Dermatitis; HDM, House Dust Mite; PAMD@, Personalized Allergy Molecular Diagnosis; D. pteronyssinus, Dermatophagoides pteronyssinus; B. tropicalis, Blomia tropicalis; SPT, Skin Prick Test; RWE, Real World Evidence.
References
1. Bakker DS, van der Wal MM, Heeb LEM, Giovannone B, Asamoah M, Delemarre EM, et al. Early and long-term effects of dupilumab treatment on circulating T-cell functions in patients with moderate-to-severe atopic dermatitis. J Invest Dermatol. (2021) 141:1943–53.e13. doi: 10.1016/j.jid.2021.01.022
2. Czarnowicki T, He H, Krueger JG, Guttman-Yassky E. Atopic dermatitis endotypes and implications for targeted therapeutics. J Allergy Clin Immunol. (2019) 143:1–11. doi: 10.1016/j.jaci.2018.10.032
3. Tamagawa-Mineoka R, Katoh N. Atopic dermatitis: identification and management of complicating factors. Int J Mol Sci. (2020) 21:2671. doi: 10.3390/ijms21082671
4. González-Pérez R, Poza-Guedes P, Pineda F, Castillo M, Sánchez-Machín I. House dust mite precision allergy molecular diagnosis (PAMD@) in the Th2-prone atopic dermatitis endotype. Life. (2021) 11:1418. doi: 10.3390/life11121418
5. Valenta R, Lidholm J, Niederberger V, Hayek B, Kraft D, Grönlund H. The recombinant allergen-based concept of component-resolved diagnostics and immunotherapy (CRD and CRIT). Clin Exp Allergy. (1999) 29:896–904.
6. Hamilton JD, Suarez-Fariñas M, Dhingra N, Cardinale I, Li X, Kostic A, et al. Dupilumab improves the molecular signature in skin of patients with moderate-to-severe atopic dermatitis. J Allergy Clin Immunol. (2014) 134:1293e300. doi: 10.1016/j.jaci.2014.10.013
7. Sastre J, Dávila I. Dupilumab: a new paradigm for the treatment of allergic diseases. J Investig Allergol Clin Immunol. (2018) 28:139–50. doi: 10.18176/jiaci.0254
8. Guttman-Yassky E, Bissonnette R, Ungar B, Suárez-Fariñas M, Ardeleanu M, Esaki H, et al. Dupilumab progressively improves systemic and cutaneous abnormalities in patients with atopic dermatitis. J Allergy Clin Immunol. (2019) 143:155–72. doi: 10.1016/j.jaci.2018.08.022
9. Simpson E, Cork M, Arkwright P, Deleuran M, Chen Z, Rodriguez Marco A, et al. Dupilumab decreases total and allergen-specific IgE in adolescents with moderate-to-severe atopic dermatitis. Ann Allergy Asthma Immunol. (2021) 127 (Suppl. 5):S54–5. doi: 10.1016/j.anai.2021.08.164
10. Sanchez-Covisa A, Rodriguez-Rodriguez JA, De la Torre F, Garcia-Robaina JC. Mite fauna of house dust of the island of Tenerife. Acarologica. (1999) 1:55–8.
11. González-Pérez R, Pineda F, Poza-Guedes P, Castillo M, Matheu V, Sánchez-Machín I. Molecular allergen profiling of dual mite sensitization in severe allergic rhinitis. J Investig Allergol Clin Immunol. (2020) 30:421–29. doi: 10.18176/jiaci.0439
12. Saeki H, Nakahara T, Tanaka A, Kabashima K, Sugaya M, Murota H, et al. Clinical practice guidelines for the management of atopic dermatitis, 2016. J Dermatol. (2016) 43:1117–45. doi: 10.1111/1346-8138.13392
13. Heinzerling L, Mari A, Bergmann K-C, Bresciani M, Burbach G, Darsow U, et al. The skin prick test–European standards. Clin Transl Allergy. (2013) 3:3. doi: 10.1186/2045-7022-3-3
14. Bojcukova J., Vlas T., Forstenlechner P., Panzner P. Comparison of two multiplex arrays in the diagnostics of allergy. Clin Transl Allergy. (2019) 9:31. doi: 10.1186/s13601-019-0270-y
15. Wollenberg A, Christen-Zäch S, Taieb A, Paul C, Thyssen JP, de Bruin-Weller M, et al. European task force on atopic dermatitis/EADV Eczema Task Force. ETFAD/EADV Eczema task force 2020 position paper on diagnosis and treatment of atopic dermatitis in adults and children. J Eur Acad Dermatol Venereol. (2020) 34:2717–44. doi: 10.1111/jdv.16892
16. Thijs JL, Strickland I, Bruijnzeel-Koomen CA, Nierkens S, Giovannone B, Csomor E, et al. Moving toward endotypes in atopic dermatitis: identification of patient clusters based on serum biomarker analysis. J Allergy Clin Immunol. (2017) 140:730–7. doi: 10.1016/j.jaci.2017.03.023
17. Czarnowicki T, Gonzalez J, Shemer A, Malajian D, Xu H, Zheng X, et al. Severe atopic dermatitis is characterized by selective expansion of circulating TH2/TC2 and TH22/ TC22, but not TH17/TC17, cells within the skin-homing T-cell population. J Allergy Clin Immunol. (2015) 136:104–15.e7. doi: 10.1016/j.jaci.2015.01.020
18. Wollmann E, Lupinek C, Kundi M, Selb R, Niederberger V, Valenta R. Reduction in allergen-specific IgE binding as measured by microarray: a possible surrogate marker for effects of specific immunotherapy. J Allergy Clin Immunol. (2015) 136:806–9.e7. doi: 10.1016/j.jaci.2015.02.034
19. Mikus M, Zandian A, Sjöberg R, Hamsten C, Forsström B, Andersson M, et al. Allergome-wide peptide microarrays enable epitope deconvolution in allergen-specific immunotherapy. J Allergy Clin Immunol. (2021) 147:1077–86. doi: 10.1016/j.jaci.2020.08.002
20. Feng M, Su Q, Lai X, Xian M, Shi X, Wurtzen PA, et al. Functional and immunoreactive levels of IgG4 correlate with clinical responses during the maintenance phase of house dust mite immunotherapy. J Immunol. (2018) 200:3897–904. doi: 10.4049/jimmunol.1701690
21. Beck LA, Thaci D, Hamilton JD, Graham NM, Bieber T, Rocklin, et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N Engl J Med. (2014) 371:130–9. doi: 10.1056/NEJMoa1314768
22. Jeong KY, Lee JY, Son M, Yi MH, Yong TS, Shin JU, et al. Profiles of IgE sensitization to Der f 1, Der f 2, Der f 6, Der f 8, Der f 10, and Der f 20 in Korean house dust mite allergy patients. Allergy Asthma Immunol Res. (2015) 7:483–8. doi: 10.4168/aair.2015.7.5.483
23. Mittermann I, Wikberg G, Johansson C, Lupinek C, Lundeberg L, Crameri R, et al. IgE sensitization profiles differ between adult patients with severe and moderate atopic dermatitis. PLoS ONE. (2016) 11:e0156077. doi: 10.1371/journal.pone.0156077
24. Aranda CJ, Curotto de Lafaille MA. The secret life of IgE-producing cells. Immunity. (2019) 50:285–7. doi: 10.1016/j.immuni.2019.01.018
25. Croote D, Darmanis S, Nadeau KC, Quake SR. High-affinity allergen-specific human antibodies cloned from single IgE B cell transcriptomes. Science. (2018) 362:1306–9. doi: 10.1126/science.aau2599
26. Varga EM, Francis JN, Zach MS, Klunker S, Aberer W, Durham SR. Time course of serum inhibitory activity for facilitated allergen-IgE binding during bee venom immunotherapy in children. Clin Exp Allergy. (2009) 39:1353–7. doi: 10.1111/j.1365-2222.2009.03303.x
27. Till SJ, Francis JN, Nouri-Aria K, Durham SR. Mechanisms of immunotherapy. J. Allergy Clin Immunol. (2004) 113:1025–34. doi: 10.1016/j.jaci.2004.03.024
28. Dreborg S, Lee TH, Kay AB, Durham SR. Immunotherapy is allergen-specific: a double-blind trial of mite or timothy extract in mite and grass dual-allergic patients. Int Arch Allergy Immunol. (2012) 158:63–70. doi: 10.1159/000330649
29. Zielen S, Lieb A, De La Motte S, Wagner F, de Monchy J, Fuhr R, et al. Omalizumab protects against allergen- induced bronchoconstriction in allergic (immunoglobulin E-mediated) asthma. Int Arch Allergy Immunol. (2013) 160:102–10. doi: 10.1159/000339243
30. Nikolov G, Todordova Y, Emilova R, Hristova D, Nikolova M, Petrunov B. Allergen-specific IgE and IgG4 as biomarkers for immunologic changes during subcutaneous allergen immunotherapy. Antibodies. (2021) 10:49. doi: 10.3390/antib10040049
31. Cox L, Calderon MA. Allergen immunotherapy for atopic dermatitis: is there room for debate? J Allergy Clin Immunol Pract. (2016) 4:435–44. doi: 10.1016/j.jaip.2015.12.018
32. Makris MP, Papadavid E, Zuberbier T. The use of biologicals in cutaneous allergies—present and future. Curr Opin Allergy Clin Immunol. (2014) 14:409–16. doi: 10.1097/ACI.0000000000000096
33. Resch Y, Blatt K, Malkus U, Fercher C, Swoboda I, Focke-Tejkl M, et al. Molecular, structural and immunological characterization of Der p 18, a chitinase-like house dust mite allergen. PLoS ONE. (2016) 11:e0160641. doi: 10.1371/journal.pone.0160641
34. Park KH, Lee J-H, Lee SC, Sim DW, Shin JU, Park CO, et al. Sensitization to various minor house dust mite allergens is greater in patients with atopic dermatitis than in those with respiratory allergic disease. Clin Exp Allergy. (2018) 48:1050–8. doi: 10.1111/cea.13164
35. Simpson EL, Paller AS, Siegfried EC, Boguniewicz M, Sher L, Gooderham MJ, et al. Efficacy and safety of dupilumab in adolescents with uncontrolled moderate to severe atopic dermatitis: a phase 3 randomized clinical trial. JAMA Dermatol. (2020) 156:44–56. doi: 10.1001/jamadermatol.2019.3336
36. Lee Y, Kim ME, Nahm DH. Real clinical practice data of monthly dupilumab therapy in adult patients with moderate-to-severe atopic dermatitis: clinical efficacy and predictive markers for a favorable clinical response. Allergy Asthma Immunol Res. (2021) 13:733–45. doi: 10.4168/aair.2021.13.5.733
37. Shamji MH, Durham SR. Mechanisms of allergen immunotherapy for inhaled allergens and predictive biomarkers. J Allergy Clin Immunol. (2017) 140:1485–98. doi: 10.1016/j.jaci.2017.10.010
Keywords: atopic dermatitis, dupilumab, specific IgE, mites, personalized allergy molecular diagnosis
Citation: González-Pérez R, Poza-Guedes P, Mederos-Luis E and Sánchez-Machín I (2022) Dupilumab modulates specific IgE mite responses at the molecular level in severe T2-high atopic dermatitis: A real-world experience. Front. Med. 9:939598. doi: 10.3389/fmed.2022.939598
Received: 09 May 2022; Accepted: 25 July 2022;
Published: 12 August 2022.
Edited by:
Stefania Guida, University of Modena and Reggio Emilia, ItalyReviewed by:
Wayne Robert Thomas, University of Western Australia, AustraliaRyoji Tanei, Tokyo Metropolitan Geriatric Hospital and Institute of Gerontology (TMGH-IG), Japan
Copyright © 2022 González-Pérez, Poza-Guedes, Mederos-Luis and Sánchez-Machín. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ruperto González-Pérez, Z2xlenJ1cGVydG9AZ21haWwuY29t
†ORCID: Ruperto González-Pérezhttps://orcid.org/0000-0002-6664-0276
Paloma Poza-Guedes https://orcid.org/0000-0001-8516-6648
Inmaculada Sánchez-Machín https://orcid.org/0000-0003-0109-8735