
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Med. , 15 August 2022
Sec. Intensive Care Medicine and Anesthesiology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.925751
This article is part of the Research Topic Advances in Extracorporeal Life Support in Critically Ill Patients, Volume II View all 18 articles
 Juan Carlos Ruiz-Rodríguez1,2,3
Juan Carlos Ruiz-Rodríguez1,2,3 Luis Chiscano-Camón1,2,3*
Luis Chiscano-Camón1,2,3* Adolf Ruiz-Sanmartin1,2,3Clara Palmada1,2Ivan Bajaña1,2
Adolf Ruiz-Sanmartin1,2,3Clara Palmada1,2Ivan Bajaña1,2 Gloria Iacoboni3,4Camilo Bonilla1,2Alejandra García-Roche1,2Erika Paola Plata-Menchaca1,2,3
Gloria Iacoboni3,4Camilo Bonilla1,2Alejandra García-Roche1,2Erika Paola Plata-Menchaca1,2,3 Carolina Maldonado1,2
Carolina Maldonado1,2 Marcos Pérez-Carrasco1,2,3
Marcos Pérez-Carrasco1,2,3 Mónica Martinez-Gallo3,5,6,7
Mónica Martinez-Gallo3,5,6,7 Clara Franco-Jarava5,6
Clara Franco-Jarava5,6 Manuel Hernández-González5,6,7
Manuel Hernández-González5,6,7 Ricard Ferrer1,2,3
Ricard Ferrer1,2,3We discuss a single case of Hemophagocytic lymphohistiocytosis (HLH) due to NK-type non-Hodgkin lymphoma and Epstein-Barr virus reactivation with multiorgan dysfunction and distributive shock in which we performed cytokine hemoadsorption with Cytosorb ®. A full microbiological panel was carried out, including screening for imported disease, standard serologies and cultures for bacterial and fungal infection. A liver biopsy and bone marrow aspirate were performed, confirming the diagnosis. The patients fulfilled the HLH-2004 diagnostic criteria, and according to the 2018 Consensus Statements by the HLH Steering Committee of the Histiocyte Society, dexamethasone and etoposide were started. There was an associated hypercytokinemia and, due to refractory distributive shock, rescue therapy with cytokine hemoadsorption was performed during 24 h (within day 2 and 3 from ICU admission). After starting this procedure, rapid hemodynamic control was achieved with a significant reduction in vasopressor support requirements. This case report highlights that cytokine hemoadsorption can be an effective since rapid decrease in IL-10 levels and a significant hemodynamic improvement was achieved.
Hemophagocytic lymphohistiocytosis (HLH) is a severe hyperinflammatory syndrome induced by activated macrophages and cytotoxic T-cells. Secondary (acquired) HLH (1) is the most frequent form in adults, commonly triggered by infections [mainly viruses Epstein-Barr Virus (2) (EBV)], malignancies (mainly malignantlymphoma) (3), macrophage activation syndrome in autoinflammatory or autoinmmune disorders (4) or other causes (for example organ or stem cell transplantation, metabolic, traumatic, immunosupression). Untreated HLH can lead to rapid multiorgan dysfunction and death, so treatment should be started as soon as possible. The pathophysiology of organ dysfunction is led by the cytokine storm, so cytokine hemadsorption could have a potential therapeutic role in this setting.
HLH diagnosis is challenging as its clinical presentation may be indistinguishable from sepsis or autoinflammatory diseases. One of the pillars of treatment includes modulating the cytokine storm (5) responsible for hyperinflammation and multiorgan failure. Treatment should be started as promptly as possible after symptom onset as untreated HLH can lead to multiorgan failure and death. Dexamethasone, etoposide and cyclosporine A are included in the standard HLH treatment protocol (6). In addition, cytokine adsorption can be a potential therapeutical option for the rapid control of cytokine storm. Herein, we report a case of a patient with distributive shock and multiorgan dysfunction due to HLH who underwent cytokine hemoadsorption.
We discuss a single case of HLH due to NK-type non-Hodgkin lymphoma and Epstein-Barr virus reactivation with multiorgan dysfunction and distributive shock in which we performed cytokine hemoadsorption with Cytosorb ® (Cytosorbents Europe, Berlin, Germany) leading to rapid decrease in several cytokines, such as interleukin 10 (IL-10) and interleukin 6 (IL-6), with significant hemodynamic improvement. Plasmatic levels of IL-6 were measured using the automated quantitative immunoassay Cobas® (Roche diagnostics International Ltd, Switzerland), following the manufacturer's instructions. Circulating levels of IL-10 and soluble CD25 (IL-2Ra) were determined using the microfluidics-based quantitative immunoassay, ELLA® (ProteinSimple, United States of America). The severity of the disease was evaluated with sequential organ failure assessment (SOFA) score (7). We analyzed the plasma concentrations of inflammatory biomarkers, including IL-6, interleukin 10 (IL-10), D-dimer, and C-reactive protein upon ICU admission, immediately before hemoadsorption initiation (pre-hemoadsorption), and after the procedure (post-hemoadsorption). Other laboratory parameters were measured to evaluate organ function. The CytoSorb® filter was connected post-hemofilter via a close loop circuit to the Continuous renal replacement therapy (CRRT) pump (Prismaflex, Gambro Lundia AB, Lund, Sweden). CRRT was performed in continuous hemodiafiltration mode (CVVHDF) using a MA 150® hemofilter (Baxter, Illinois, US) at a blood flow rate of 200 ml/min. Anticoagulation was performed with unfractionated heparin.
A 50-year-old African male patient was admitted to the hospital with a 2-month history of mild epistaxis and diffuse abdominal pain. He presented fever and hepatosplenomegaly at physical exam; laboratory values showed cytolysis with undissociated cholestasis, non-oliguric renal failure, pancytopenia with hemolytic anemia, hyperferritinemia, and hypertriglyceridemia. He required a rapid admission to the Intensive Care Unit (ICU) for hemodynamic and respiratory support. A full microbiological panel was carried out, including screening for imported disease, standard serologies and cultures for bacterial and fungal infection; results came back positive for Epstein-Barr virus with a 7.7 Log viremia. The patient fulfilled the HLH-2004 diagnostic criteria, and according to the 2018 Consensus Statements by the HLH Steering Committee of the Histiocyte Society, dexamethasone and etoposide (8) were started, together with empirical antibiotic treatment with meropenem and amikacin. Simultaneously, a liver biopsy and bone marrow aspirate were performed, confirming the diagnosis of NK-type non-Hodgkin's lymphoma with secondary hemophagocytosis.
Although the patient received broad-spectrum antibiotics and the recommended HLH treatment, he rapidly deteriorated in 48 h with a distributive shock and multiorgan dysfunction (renal, neurological, hemodynamic, respiratory, and hepatic) requiring high doses of vasopressor support, continuous veno-venous hemodiafiltration and invasive mechanical ventilation. There was an associated hypercytokinemia and, due to refractory distributive shock, rescue therapy with cytokine hemoadsorption with Cytosorb® was started on the second day after ICU admission. Cytokine adsorption was performed in parallel to the venovenous hemodiafiltration circuit. Interleukin 6, IL-10 and IL-2Ra were monitored in real time. After starting this procedure, rapid hemodynamic control was achieved with a significant reduction in vasopressor support requirements after only a few hours since the start of cytokine hemoadsorption (Table 1). This therapy was started within 24 hours of ICU admission. Vasopressor support was stopped 37 h after the start of this procedure. Despite this, 6 days after completion of cytokine hemoadsorption and 9 days since ICU admission, the patient died due to thrombotic complications related to the underlying lymphoma with thrombosis of the inferior vena cava, hepatic system, right atrium and partial thrombosis of the thoracic aorta.
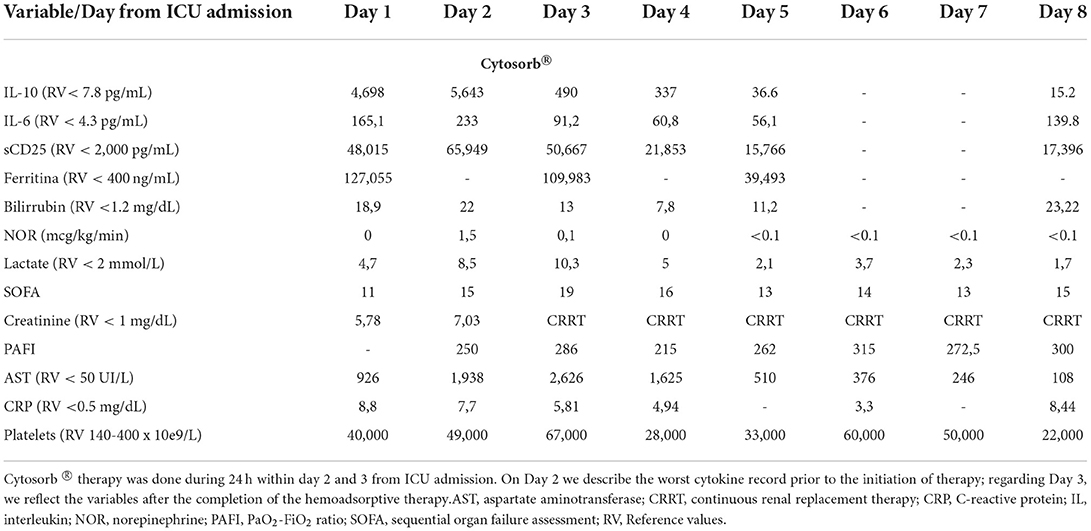
Table 1. Biochemical and clinical parameters.
The therapeutic strategy of HLH includes a triple approach: organ support measures, trigger resolution and inflammatory response suppression (1). Although dexamethasone, etoposide and cyclosporine A are considered standard HLH treatment, these patients present a cytokine storm that needs rapid control. The pathophysiologic process of HLH is characterized by an uncontrolled activation and expansion of T lymphocytes and macrophages, responsible for the production of a large amount of proinflammatory cytokines, the latter causing a “cytokine storm” (9). Cytokine control could be carried out with drugs such as Tocilizumab (10) or Anakinra (11) but also with extracorporeal blood purification (2).
Several extracorporeal blood purification techniques have been proposed in critical patients with multiorgan dysfunction (12). Cytosorb®, licensed for extracorporeal cytokine removal in the European Union, is a high-flow, low-resistance cytokine adsorbent, containing specially developed polymer beads with a large surface and adsorption spectrum up to 60kDa. Results with Cytosorb indicate not only a broad-spectrum removal of inflammatory mediators, but also significant survival improvement in high-lethality models (13).
In the sepsis cytokine-storm related pattern, IL-6 is the best studied molecule (14), but in secondary HLH the elevation of interferon gamma and IL-10 is more significant (15). Very high levels of interferon gamma and IL-10 with a mildly elevated IL-6 has a high diagnostic accuracy for secondary HLH and could be a useful approach to differentiate HLH from infection (16, 17). In this case, the indication of cytokine hemoadsorption in HLH would have as its main objective the elimination of IL-10 since the inflammatory response is unbalanced toward anti-inflammation.
Experience in the use of cytokine hemoadsorption as adjuvant treatment for HLH is scarce. Greil et al. (18) described a CTLA4-deficient patient who developed secondary HLH due to EBV-induced Hodgkin lymphoma under treatment with abatacept. Their patient also presented multiorgan dysfunction and Cytosorb® was used for 4 days, achieving a reduction in inflammatory parameters and clinical improvement. This case is similar to ours, including the type of technique, since it is performed in parallel with renal hemodiafiltration. Unlike the study by Greil et al. we monitored in real time the plasma concentrations of IL-6 and IL-10 to adjust the duration of hemoadsorption. Once the cytokine levels were controlled and the patient clinically improved (with reduction in vasopressor support), we discontinued hemoadsorption. This system allows us to shorten the hemoadsorption time, an important step since it can alter the concentrations of certain drugs, such as antibiotics (19, 20). Frimmel et al. (21) reported a case of multiorgan dysfunction due to liver failure in a patient with HLH secondary to reactivation of the Herpes simplex virus type 1. In this case, the indication for hemadsorption was a distributive shock due to liver failure. In this patient, there was a very significant elevation of IL-6 but IL-10 concentrations were not reported.
As this is a case report, causality cannot be confirmed, particularly when considering the other treatment interventions (e.g., dexamethasone, etoposide). However, there was a close temporal relationship between the initiation of hemoadsorption and the reduction in cytokine levels and clinical improvement. IL-10 levels were significantly reduced in 24 h and a rapid improvement in hemodynamic dysfunction was documented 24 h from initiation of therapy, thus controlling the cytokine storm causing distributive shock. The patient's favorable clinical evolution should be attributed to all therapeutic interventions, though the rapid clinical improvement may be related to cytokine elimination by hemoadsorption, as this has not been described as a pharmacological effect of corticosteroids or etoposide. In our institution, we monitor cytokines (IL-6 and IL-10) in real time, which allows us to suspend therapy when a significant clinical and biological improvement (decrease in cytokines) has been achieved.
As we quoted before, haemadsorption therapy has been administered in parallel to conventional treatment of haemophagocytic syndrome. In our case with Etoposide and Dexamethasone. Regarding the administered dose of these immunosuppressive drugs, to date no PK data during Cytosorb is available on this treatment, so we employed conventional dosage (22). Indeed, certain pharmacokinetic consequences of hemoadsorption cannot be ruled out. However, recent studies do not show that plasma concentrations of meropenem (19) are altered, although it could be possible with other antibiotics such as teicoplanin (20). In any case, it is important to monitor antibiotic concentrations, especially when the periods of hemoadsorption are very long.
The use of haemadsorption therapy is a salvage therapy and, in this case, we indicate its use in a situation of distributive shock refractory to conventional treatment, with evolution to multi-organ dysfunction. To date, there is no threshold plasma cytokine level used for initiation or termination of therapy. In this setting, the cytokine storm in HLH is, as in sepsis, also uncontrolled and, especially in its most severe and life-threatening forms, is responsible for inflammation-driven organ damage. In this setting, blood purification techniques can blunt the inflammatory process with a rapidly considerable, nonselective effect on the cytokine storm, potentially translating into survival benefit for the patient (23).
Cytokine hemoadsorption is a safe procedure without relevant associated adverse effects (24). In our case, we did not observe adverse effects.
In our patient, cytokine hemoadsorption was associated with a rapid decrease in IL-10 levels and a significant hemodynamic improvement. This case report highlights that cytokine hemoadsorption can be an effective and safe rescue therapy in patients with HLH and multiorgan dysfunction, complementary to standard protocol treatments. We suggest real-time monitoring of plasma cytokine concentrations as a tool to monitor the biological effect of cytokine hemadsorption, optimizing the duration of this procedure.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to publish this case was obtained and it was recorded in the medical history. Information revealing the subject's identity was avoided.
All authors carry out assistance and research work associated with the Vall d'Hebron Campus, contributed to the article, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ramos-Casals M, Brito-Zeron P, Lopez-Guillermo A, Khamashta MA, Bosch 28 X. Adult haemophagocytic syndrome. Lancet. (2014) 383:1503–16. doi: 10.1016/S0140-6736(13)61048-X
2. Rouphael NG, Talati NJ, Vaughan C, Cunningham K, Moreira R, Gould C. Infections associated with haemophagocytic syndrome. Lancet Infect Dis. (2007) 7:814–22. doi: 10.1016/S1473-3099(07)70290-6
3. Lehmberg K, Nichols KE, Henter JI, Girschikofsky M, Greenwood T, Jordan M, et al. Consensus recommendations for the diagnosis and management of hemophagocytic lymphohistiocytosis associated with malignancies. Haematologica. (2015) 100:997–1004. doi: 10.3324/haematol.2015.123562
4. Carter SJ, Tattersall RS, Ramanan AV. Macrophage activation syndrome in adults: recent advances in pathophysiology, diagnosis and treatment. Rheumatology. (2019) 58:5–17. doi: 10.1093/rheumatology/key006
5. Brisse E, Wouters CH, Matthys P. Hemophagocytic lymphohistiocytosis (HLH): a heterogeneous spectrum of cytokine-driven immune disorders. Cytokine Growth Factor Rev. (2015) 26:263–80. doi: 10.1016/j.cytogfr.2014.10.001
6. La Rosée P, Horne A, Hines M, von Bahr Greenwood T, Machowicz R, Berliner N, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. (2019) 133:2465–77. doi: 10.1182/blood.2018894618
7. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. on behalf of the working group on sepsis-related problems of the European society of intensive care medicine. Intensive Care Med. (1996) 22:707–10. doi: 10.1007/BF01709751
8. Ehl SA I, von Bahr Greenwood T, Hines M, Horne A.C, Ishii E, Janka G, et al. Recommendations for the use of etoposide-based therapy and bone marrow transplantations for the teratment of HLH: consensus statements by the HLH steering committee of the histiocyte society.xs J Allergy Clin Immunol Pract. (2018) 6:1508–17. doi: 10.1016/j.jaip.2018.05.031
9. Grom AA, Horne A, De Benedetti F. Macrophage activation syndrome in the era of biologic therapy. Nat Rev Rheumatol. (2016) 12:259–68. doi: 10.1038/nrrheum.2015.179
10. Zhou S, Qiao J, Bai J, Wu Y, Fang H. Biological therapy of traditional therapy resistant adult-onset Still's disease: an evidence-based review. Ther Clin Risk Manag. (2018) 14:167–71. doi: 10.2147/TCRM.S155488
11. Wohlfarth P, Agis H, Gualdoni GA, Weber J, Staudinger T, Schellongowski P, et al. Interleukin 1 receptor antagonist anakinra, intravenous immunoglobulin, and corticosteroids in the management of critically ill adult patients with hemophagocytic lymphohistiocytosis. J Intensive Care Med. (2017) 34:723–31. doi: 10.1177/0885066617711386
12. Harm S, Schildböck C, Hartmann J. Cytokine removal in extracorporeal blood purification: an in vitro study. Blood Purif. (2020) 49:33–43. doi: 10.1159/000502680
13. Peng Z, Bishop J, Wen X, Elder M, Zhou F, Chuasuwan A, et al. Modulation of chemokine gradients by apheresis redirects leukocyte trafficking to different compartments during sepsis, studies in a rat model. Critical Care. (2014) 18:R141 doi: 10.1186/cc13969
14. Scheller J, Chalaris A, Schmidt-Arras D, Rose-John S. The pro- and anti-inflammatory properties of the cytokine interleukin-6. Biochim Biophys Acta. (2011) 1813:878–88. doi: 10.1016/j.bbamcr.2011.01.034
15. Debaugnies F, Mahadeb B, Nagant C, Meuleman N, De Bels D, Wolff F. Biomarkers for early diagnosis io hemophagocytic lymphohistiocytosis in critically ill patients. J Clin Immunol. (2021) 41:658–65. doi: 10.1007/s10875-020-00950-z
16. Xu XJ, Tang YM, Song H, et al. Diagnostic accuracy of a specific cytokine pattern in hemophagocytic lymphohistiocytosis in children. J Pediatr. (2012) 160:984–90 doi: 10.1016/j.jpeds.2011.11.046
17. Han XC, Ye Q, Zhang WY, Tang YM, Xu XJ, Zhang T. Cytokine profiles as novel diagnostic markers of Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis in children. J Crit Care. (2017) 39:72–7. doi: 10.1016/j.jcrc.2017.02.018
18. Greil C, Roether F, La Rosee P, Grimbacher B, Duerschmied D, Warnatz K. Rescue of Cytokine Storm Due to HLH by Hemoadsorption in a CTLA4-Deficient Patient. J Clin Immunol. (2017) 37:273–6. doi: 10.1007/s10875-017-0377-7
19. Singhan W, Vadcharavivad S, Areepium N, Wittayalertpanya S, Chaijamorn W, Srisawat N. The effect of direct hemoperfusion with polymixyin B immobilized cartridge on meropenem in critically ill patients requiring renal support. J Crit Care. (2019) 51:71–6. doi: 10.1016/j.jcrc.2019.02.007
20. Reiter K, Bordoni V, Dall'Olio G, Ricatti M, Soli M, Ruperti S, et al. In vitro removal of therapeutic drugs with a novel adsorbent system. Blood Purif. (2002) (4):380–8. doi: 10.1159/000063108
21. Frimmel S, Schipper J, Henschel J, Yu TT, Mitzner SR, Koball S. First description of single-pass albumin dialysis combined with cytokine adsorption in fulminant liver failure and hemophagocytic syndrome resulting from generalized herpes simplex virus 1 infection. Liver Transpl. (2014) 20:1523–4. doi: 10.1002/lt.24005
22. Scheier J, Nelson PJ, Schneider A, Colombier S, Kindgen-Milles D, Deliargyris EN, et al. Mechanistic considerations and pharmacokinetic implications on concomitant drug administration during cytosorb therapy. Crit Care Explor. (2022) 4:e0688 doi: 10.1097/CCE.0000000000000688
23. Huang P, Huang C, Xu H, Lu J, Tian R, Wang Z, et al. Early use of blood purification in severe epstein-barr virus-associated hemophagocytic syndrome. Pediatrics. (2020) 145:e20193197 doi: 10.1542/peds.2019-3197
Keywords: hemophagocytic lymphohistiocytosis, cytokine storm, multiorgan dysfunction, cytokine hemoadsorption, shock
Citation: Ruiz-Rodríguez JC, Chiscano-Camón L, Ruiz-Sanmartin A, Palmada C, Bajaña I, Iacoboni G, Bonilla C, García-Roche A, Paola Plata-Menchaca E, Maldonado C, Pérez-Carrasco M, Martinez-Gallo M, Franco-Jarava C, Hernández-González M and Ferrer R (2022) Case report: Cytokine hemoadsorption in a case of hemophagocytic lymphohistiocytosis secondary to extranodal NK/T-cell lymphoma. Front. Med. 9:925751. doi: 10.3389/fmed.2022.925751
Received: 21 April 2022; Accepted: 01 August 2022;
Published: 15 August 2022.
Edited by:
Luo Zhe, Fudan University, ChinaReviewed by:
Yini Wang, Capital Medical University, ChinaCopyright © 2022 Ruiz-Rodríguez, Chiscano-Camón, Ruiz-Sanmartin, Palmada, Bajaña, Iacoboni, Bonilla, García-Roche, Paola Plata-Menchaca, Maldonado, Pérez-Carrasco, Martinez-Gallo, Franco-Jarava, Hernández-González and Ferrer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luis Chiscano-Camón, bHVpc2NoaXNjYW5vQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.