 Jin-Tong Shi
Jin-Tong Shi Yuexin Zhang
Yuexin Zhang Yuehan She
Yuehan She Hemant Goyal
Hemant Goyal Zhi-Qi Wu
Zhi-Qi Wu Hua-Guo Xu
Hua-Guo Xu- 1Department of Laboratory Medicine, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
- 2Branch of National Clinical Research Center for Laboratory Medicine, Nanjing, China
- 3Department of Medicine, The Wright Center for Graduate Medical Education, Scranton, PA, United States
Background: This study aims to consolidate evidence from published systematic reviews and meta-analyses evaluating the diagnostic performances of non-invasive tests for inflammatory bowel disease (IBD) in various clinical conditions and age groups.
Methods: Two independent reviewers systematically identified and appraised systematic reviews and meta-analyses assessing the diagnostic utility of non-invasive tests for IBD. Each association was categorized as adults, children, and mixed population, based on the age ranges of patients included in the primary studies. We classified clinical scenarios into diagnosis, activity assessment, and predicting recurrence.
Results: In total, 106 assessments from 43 reviews were included, with 17 non-invasive tests. Fecal calprotectin (FC) and fecal lactoferrin (FL) were the most sensitive for distinguishing IBD from non-IBD. However, anti-neutrophil cytoplasmic antibodies (ANCA) and FL were the most specific for it. FC and FL were the most sensitive and specific tests, respectively, to distinguish IBD from irritable bowel syndrome (IBS). Anti-Saccharomyces cerevisiae antibodies (ASCA), IgA, were the best test to distinguish Crohn’s disease (CD) from ulcerative colitis (UC). Interferon-γ release assay was the best test to distinguish CD from intestinal tuberculosis (ITB). Ultrasound (US) and magnetic resonance enterography (MRE) were both sensitive and specific for disease activity, along with the high sensitivity of FC. Small intestine contrast ultrasonography (SICUS) had the highest sensitivity, and FC had the highest specificity for operative CD recurrence.
Conclusion: In this umbrella review, we summarized the diagnostic performance of non-invasive tests for IBD in various clinical conditions and age groups. Clinicians can use the suggested non-invasive test depending on the appropriate clinical situation in IBD patients.
Introduction
Inflammatory bowel diseases (IBD) [Crohn’s disease (CD) and ulcerative colitis (UC)] are idiopathic disorders causing inflammation of the gastrointestinal tract. IBD is emerging as a globally important disease with increasing incidence. Although incidence has started to relatively stabilize in western countries, the disease burden remains high as prevalence surpasses 0.3% (1).
Gastrointestinal endoscopy has remained a reference standard but invasive test for the diagnosis, management, prognostics, and surveillance of IBD. However, endoscopy can be associated with considerable cost, risk, and burden to patients and healthcare systems, and it is the lowest acceptable tool for patients (2).
Accurate non-invasive tests such as biomarkers and radiological examinations would be ideal (3, 4). Several promising non-invasive tests that could fulfill this role, including fecal calprotectin (FC) (5) and ultrasound (US) (6), have been studied. Despite many studies assessing the diagnostic performance of non-invasive tests for IBD, to the best of our knowledge, there has been no systematic effort to summarize and critically appraise this body of evidence. Therefore, we performed an umbrella review of meta-analyses, based on different clinical conditions (including diagnosis, activity assessment, and recurrence) and age groups (children, adults, and mixed population), to provide a comprehensive synopsis of the diagnostic performance and validity of reported non-invasive tests for IBD.
Methods
Search Strategy
Two reviewers (J-TS and Z-QW) independently searched PubMed, Embase, Web of Science, and Cochrane Library databases from inception to 16 April 2020. The search was limited to systematic reviews and meta-analyses without language restrictions. Supplementary Appendix 1 provides a detailed search strategy.
Study Selection and Data Extraction
Systematic reviews or meta-analyses meeting the following criteria were included: it described the conduct of the systematic review in adequate detail, and an attempt was made to identify all of the relevant primary studies in at least one database with provided search strategy and quality appraisal of the primary studies (7). Guidelines, narrative reviews, literature reviews, genetic studies, protocol, conference abstracts, and reviews assessing scoring indices were excluded.
Two reviewers (J-TS and Z-QW) independently carried out the study selection and data extraction from the eligible articles. Extracted data included author, year of publication, number of participants, number and type of studies included, appraisal instrument used, reference standard, outcomes assessed, heterogeneity, and study findings.
Quality Assessment
The methodological quality of included reviews was assessed independently by J-TS and Z-QW using the online AMSTAR 2 (A Measurement Tool to Assess Systematic Reviews) checklist (8). AMSTAR 2 is a validated and reliable quality measurement tool for systematic reviews, with 16 domains. Seven of these domains are considered critical. Shortcomings in any of the critical domains could affect the overall validity of a review. It results in an assessment of the methodologic quality as 1 of 2 grades: high, moderate, low, or critically low (9).
Identification of Age Groups
Based on the age ranges of primary studies included, associations can be categorized as adults, children, and mixed population. We defined children as under the age of 18 years (10). If a systematic review purporting to assess the accuracy in adults included people younger than 18 years, it would be classified as a mixed population. Supplementary Appendix 2 presents the process of identifying age groups.
Overlapping and Outdated Associations
Associations in two or more reviews overlapped if they evaluated the same test in the same clinical condition and same age group. Incorporating results of overlapping reviews could lead to double inclusion resulting in biased findings and estimates (11, 12). In addition, up to 50% of published systematic reviews were considered out of date after 5.5 years. Therefore, we categorized overlapping systematic reviews as outdated (published before October 2015) and contemporary (published after October 2015).
For contemporary reviews found to have overlapping assessments, we generated a graphical cross-tabulation (citation matrix) of the overlapping reviews (in columns) and the included primary studies (in rows) (13). Corrected covered area (CCA) was a validated method to quantify the degree of overlap between two or more reviews. We used a citation matrix to calculate CCA. According to CCA, the overlap can be categorized as very high (CCA > 15%), high (CCA 11–15%), moderate (CCA 6–10%), or slight (CCA 0–5%) (14).
In all the systematic reviews that met the inclusion criteria, all non-overlapping reviews were included. A rigorous management tool was used for the overlapping reviews. Supplementary Appendix 3 shows the citation matrices for all overlapping studies. Supplementary Appendix 4 presents the management of overlapping reviews.
Data Synthesis
Systematic reviews that met the inclusion criteria formed the unit of analysis. Only data available from systematic reviews were presented. Results from systematic reviews were synthesized with a narrative synthesis, with a tabular presentation of findings and forest plots for studies that performed a meta-analysis. Summary tables describing review characteristics and findings were also presented.
Update of Eligible Reviews
We used the framework recommended by Garner et al. (15) to determine whether an update was necessary. An existing review qualified for an update if all of the following were met:
• The review achieved at least a moderate rating with the AMSTAR 2 quality assessment tool (9).
• A focused or abbreviated search of primary studies using the key search terms from the search strategy of an existing review to identify newly published studies that met the inclusion criteria of the review.
• The findings from newly published studies would change the conclusion or credibility of the review.
Supplementary Appendix 5 describes the search strategy used to identify newly published studies. YXZ and YHS initially screened the eligible newly published studies. Full-text screening and data extracting were accomplished by JTS and ZQW.
With findings from newly published studies, we relied on statistical methods using the bivariate model (16) to pool the data from newly published studies with the data from the original meta-analysis (17) (for meta-analyses) and discussion with senior authors (for reviews without meta-analyses) to determine whether a full update of the existing review was needed (18).
If an update was considered necessary, the original methods used in the conduct of the existing review were replicated. Supplementary Appendix 6 summarizes the evaluation process for considering reviews for updates adapted from Ahmadzai et al. (19).
Results
Literature Search
The search retrieved 1,897 articles. After removing duplicates and screening titles and abstracts, 113 articles qualified for full-text screening. Seven outdated reviews were further excluded. Finally, 46 reviews were included. Supplementary Appendix 7 summarizes the study selection process with accurate numbers of studies. Supplementary Appendix 8 provides the list of excluded studies with reasons for exclusion.
Methodological Quality
Twenty-two reviews (5, 6, 10, 20–38) were rated as moderate in quality, and twenty-three reviews (39–60) were rated as low, while one review (61) was rated as critically low in quality (Supplementary Appendix 9). In the seven critical domains, most low-quality reviews had not stated that the methods were established before conducting the study.
Overlapping and Non-overlapping Assessment
Seventeen reviews reported overlapping assessment (5, 6, 29, 32, 36, 37, 46, 49–52, 54, 58, 59, 61–63). Supplementary Appendix 10 describes the general characteristics of overlapping reviews, including the decision to retain or exclude an assessment. Supplementary Appendix 3 provides the citation matrices for overlapping reviews to assess the degree of overlap. Supplementary Appendix 11 lists forty-six reviews with non-overlapping assessments that were included and one contemporary review that was excluded because of overlap.
Study Characteristics of Reviews With Non-overlapping Assessments
Non-invasive tests for IBD assessed in the included reviews were FC, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), platelet count (PLT), hemoglobin (Hb), albumin (Alb), ASCA, anti-neutrophil cytoplasmic antibodies (ANCA), fecal lactoferrin (FL), US, computed tomography (CT), magnetic resonance imaging enterography (MRE), scintigraphy, autoantibodies-to-glycoprotein-2 (AntiGP2), interferon-γ release assays (IGRA), fecal immunochemical (FIT), microRNA, and S100A12. Of the 46 reviews included, 43 conducted meta-analyses. Supplementary Table 1 summarizes the general characteristics of the reviews and meta-analyses included in the umbrella review.
Summary Findings
Table 1 shows the diagnostic utility of non-invasive tests for IBD in different clinical scenarios and age groups. Tables 2, 3 show the diagnostic utility of non-invasive tests for CD and UC, respectively. The clinical scenarios include diagnosis (IBD vs. non-IBD), diagnosis (IBD vs. IBS), diagnosis (IBD vs. FGID, functional gastrointestinal disorders), diagnosis (CD vs. ITB, intestinal tuberculosis), diagnosis (CD vs. UC), activity assessment, and recurrence. Figure 1 presents the forest plots of sensitivity (Se) and specificity (Sp) of non-invasive tests for IBD. Figures 2, 3 present the forest plots for CD and UC, respectively. Supplementary Tables 2, 3 show the findings of meta-analyses and narrative synthesis from systematic reviews.
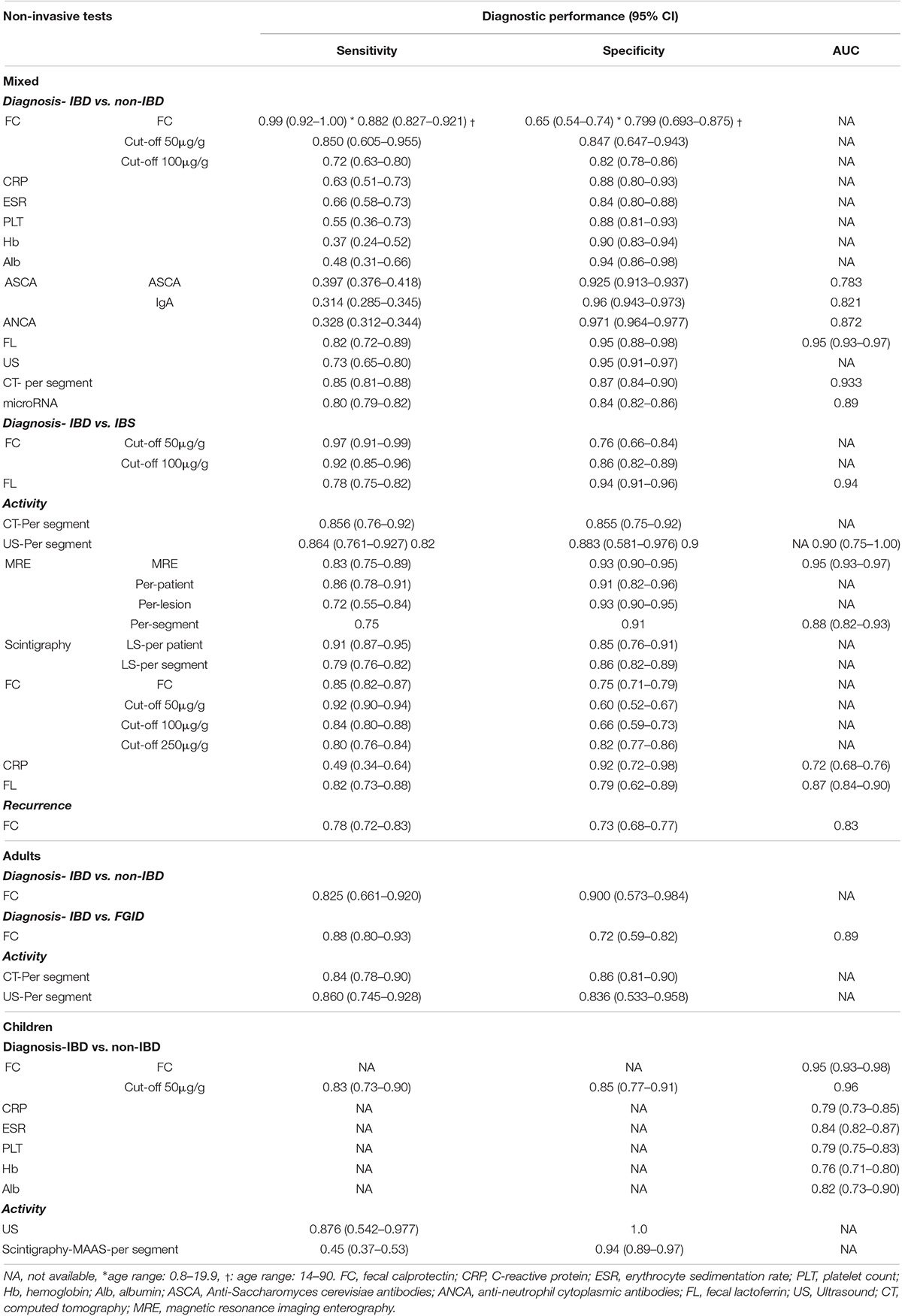
Table 1. Summary findings for each non-invasive tests and diagnostic performance (IBD).
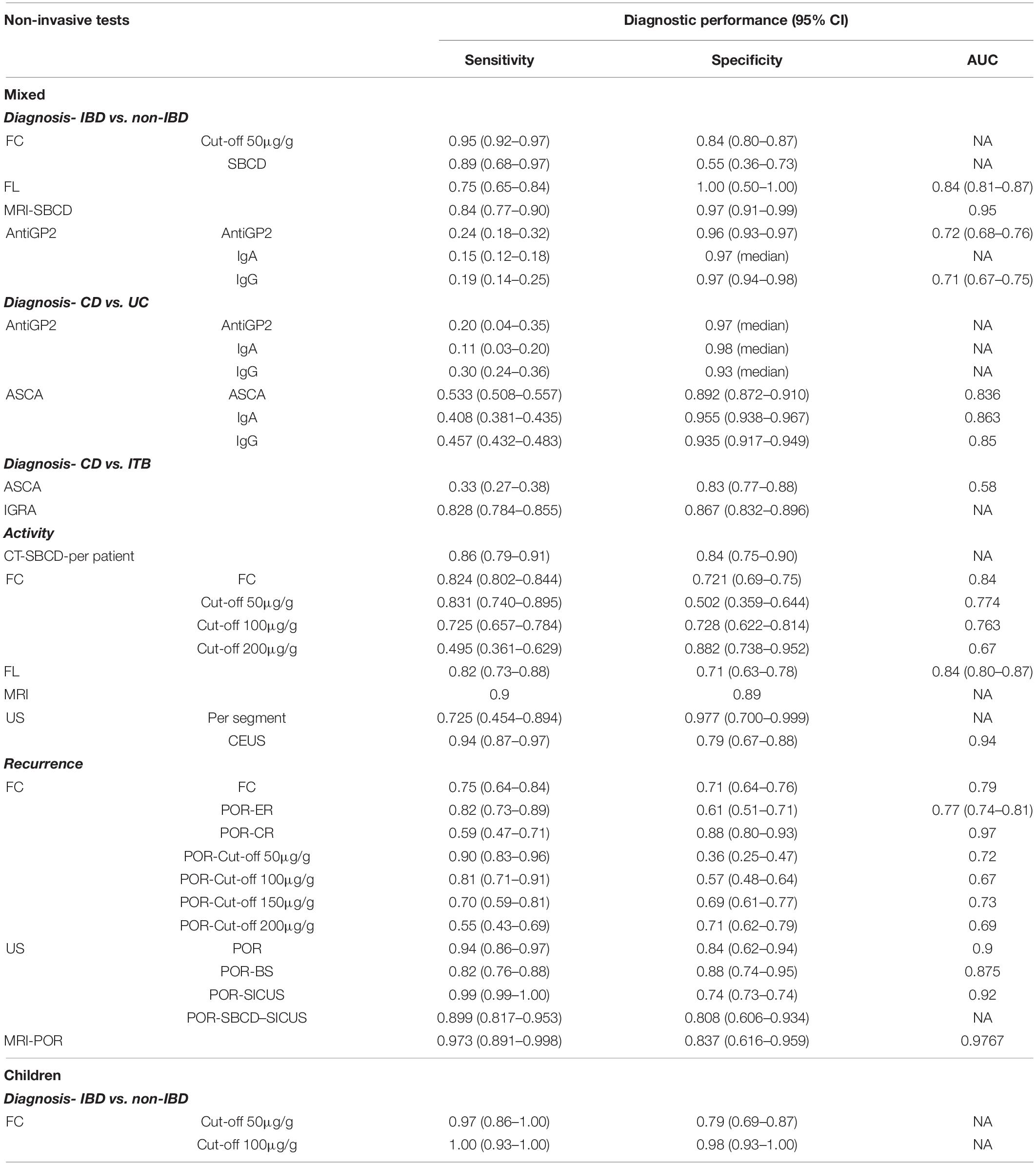
Table 2. Summary findings for each non-invasive tests and diagnostic performance (CD).
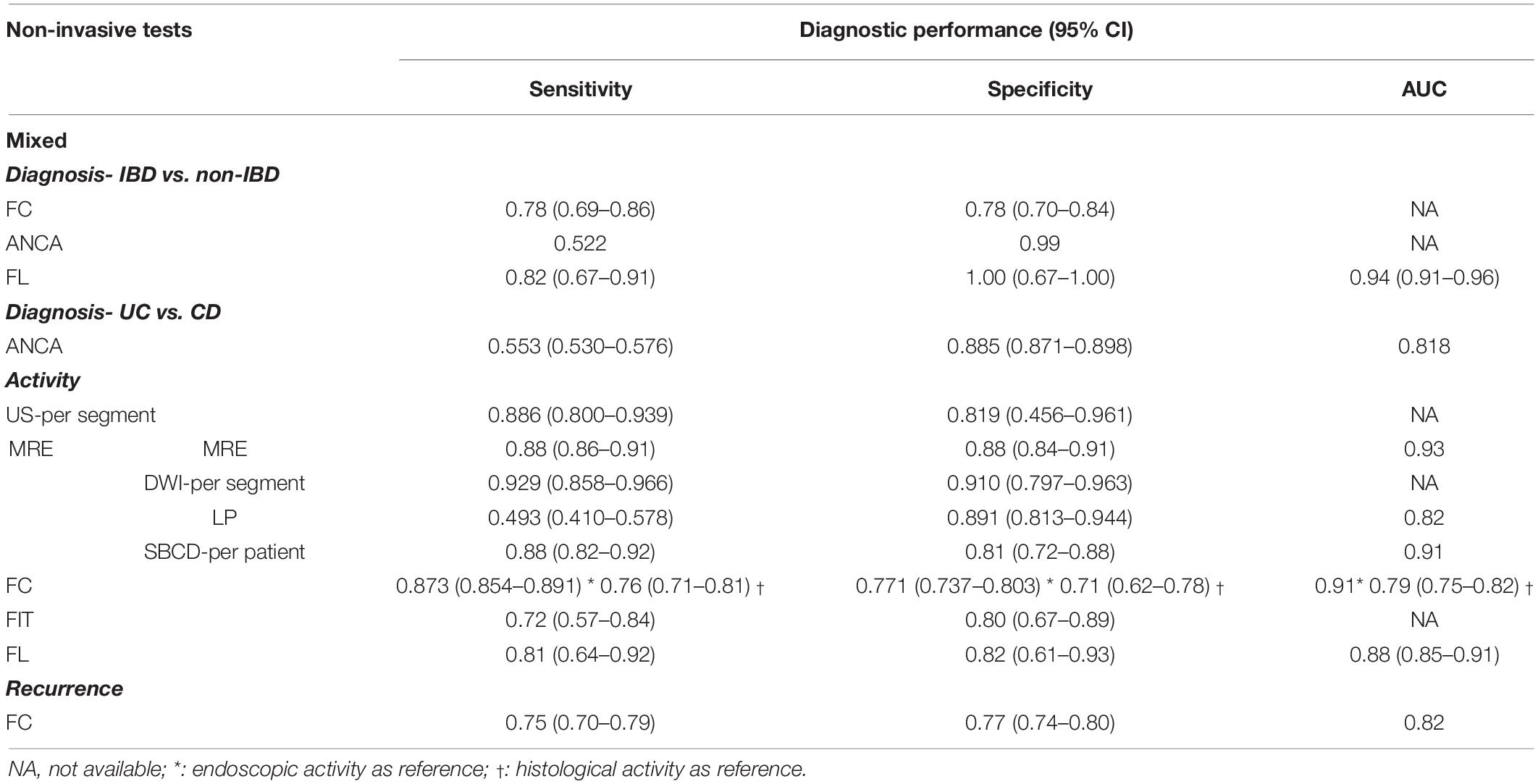
Table 3. Summary findings for each non-invasive tests and diagnostic performance (UC).
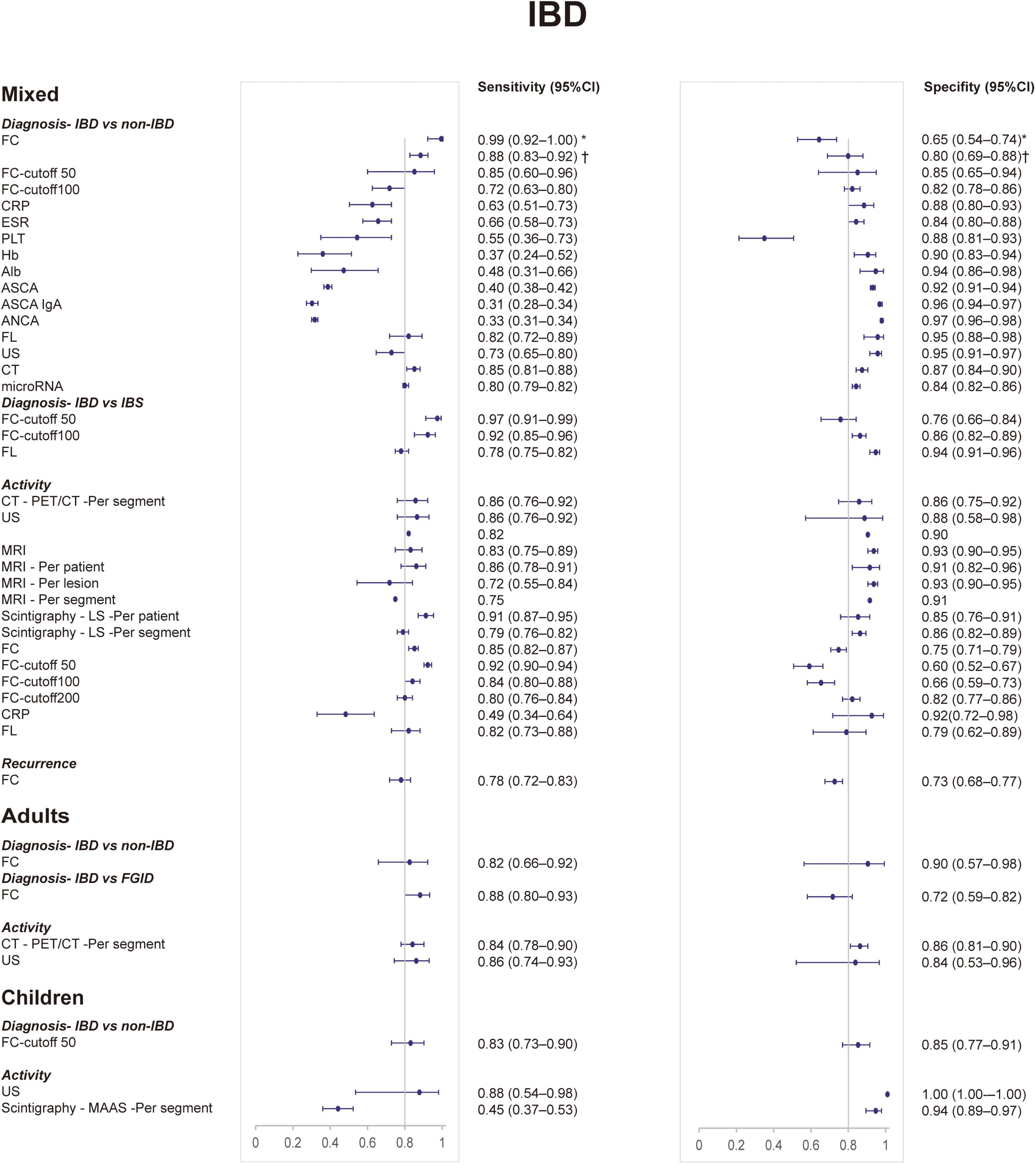
Figure 1. Forest plots of sensitivity and specificity of non-invasive tests for inflammatory bowel disease from meta-analyses. CI, confidence interval. *Age range: 0.8–19.9, †age range: 14–90.
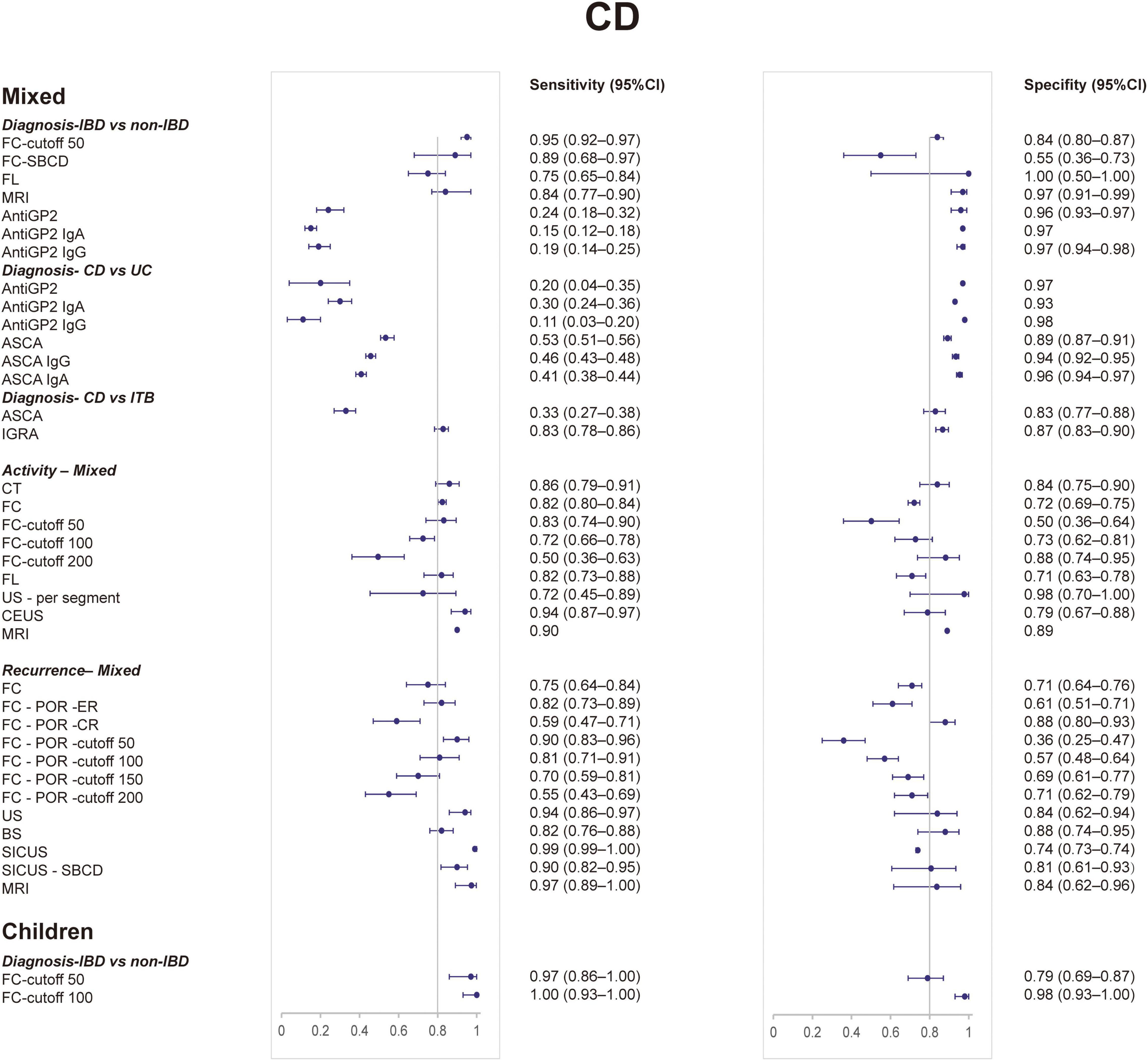
Figure 2. Forest plots of sensitivity and specificity of non-invasive tests for Crohn’s disease from meta-analyses. CI, confidence interval.
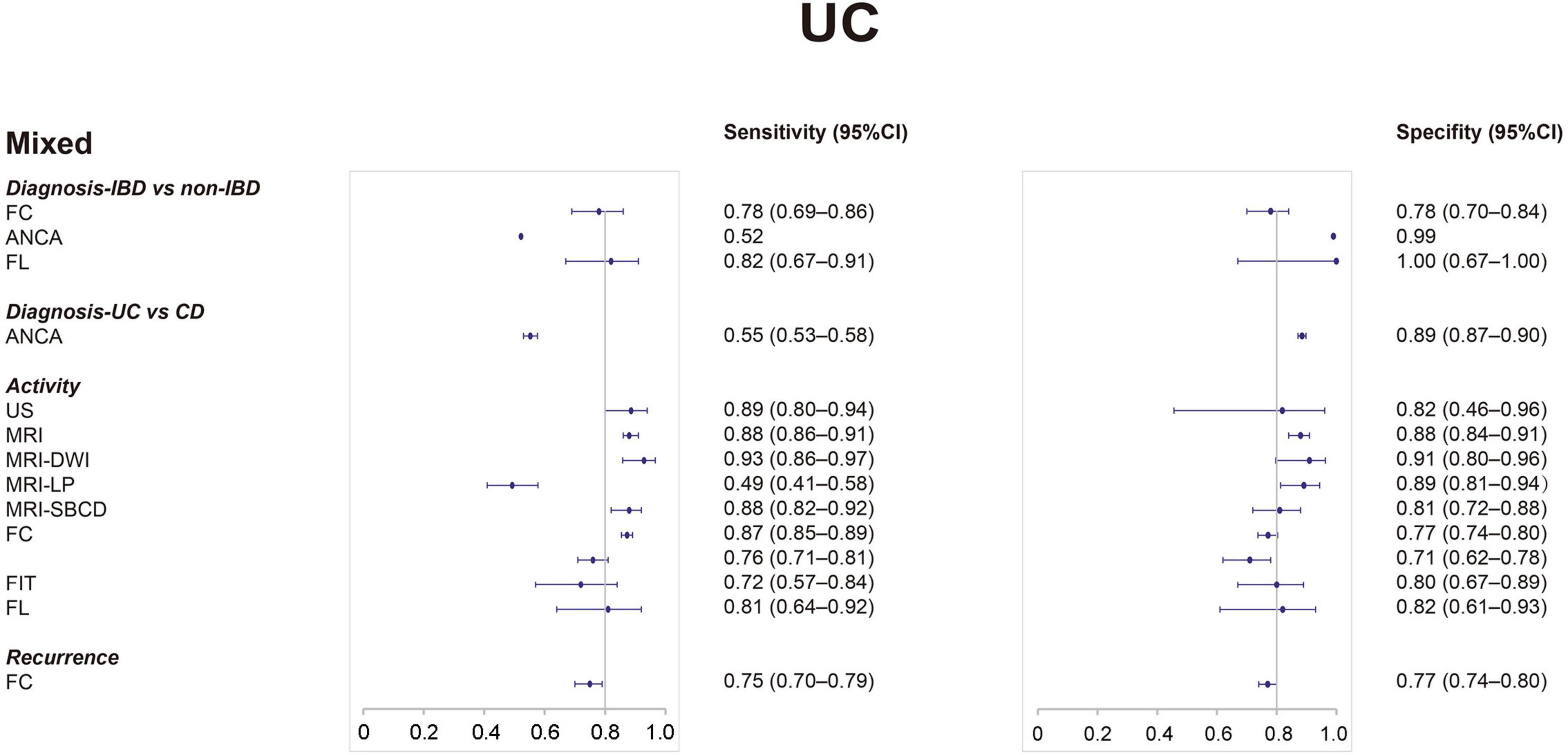
Figure 3. Forest plots of sensitivity and specificity of non-invasive tests for ulcerative colitis from meta-analyses. CI, confidence interval.
Diagnosis: Inflammatory Bowel Disease vs. Non-inflammatory Bowel Disease
Mixed Population
For IBD, FC was the most sensitive test with a sensitivity of 0.99 (0.92–1.00) (46). ANCA showed the highest specificity 0.971 (0.964–0.977) (20). The sensitivity and specificity of CT, FL, and microRNA were both balanced (41, 44). The other tests performed well in specificity but poorly in sensitivity, including US, ESR, CRP, PLT, Alb, Hb, and ASCA (20, 46).
For UC, FL had both the best sensitivity (0.82; 0.67–0.91) and the best specificity (1.00; 0.67–1.00) (44). The other biomarkers were FC (Se, 0.78; 0.69–0.86/Sp, 0.78; 0.70–0.84) (21), and ANCA (Se, 0.522/Sp, 0.99) (64).
For CD, FC showed the highest sensitivity: 0.95 (0.92–0.97) (21). FL showed the highest specificity: 1.00 (0.50–1.00) (44). Also, the specificity of anti-GP2 was good (49).
Adults
For IBD, only FC was performed with Se of 0.825 (0.661–0.920) and Sp of 0.900 (0.573–0.984) (5). For UC, there was a review showing that the Se and Sp for ANCA IgG were 0.67 (0.54–0.79) and 0.85 (0.70–0.94), respectively (39).
Children
For IBD, FC with a cutoff of 50 μg/g showed the highest AUC of 0.96 (21). The AUCs of other biomarkers [FC, CRP, ESR, PLT, Hb, and Alb (30)] ranged from 0.76 to 0.95. One review presented results of US from three primary studies: sensitivity range from 0.39 to 0.55 and specificity range from 0.90 to 1.00 (35).
For CD, FC with a cutoff of 100 μg/g performed best with a sensitivity of 1.00 (0.93–1.00) and specificity of 0.98 (0.93–1.00) (21). MRE (Se, 0.84; 0.77–0.90/Sp, 0.97; 0.91–0.99) (22) also performed well in SBCD.
Diagnosis: Inflammatory Bowel Disease vs. Irritable Bowel Syndrome
Mixed Population
For IBD, FC with a cutoff of 50 μg/g was the most sensitive test with a sensitivity of 0.97 (0.91–0.99) (52). As for specificity, FL was the best: 0.94 (0.91–0.96) (24). One review presented the diagnostic performance of fecal S100A12 (Se, 0.86; 0.73–0.94/Sp, 0.96; 0.79–0.99) (39) (Supplementary Table 3).
Diagnosis: Inflammatory Bowel Disease vs. Functional Gastrointestinal Disorders
Adults
For IBD, there was only one test: FC (Se, 0.88; 0.80–0.93/Sp, 0.71; 0.59–0.82) (53).
Diagnosis: Crohn’s Disease vs. Ulcerative Colitis
Mixed Population
To differentiate CD from UC, the sensitivity of tests is generally low, including anti-GP2, ASCA (20, 54). ASCA IgA showed the highest specificity of 0.955 (0.938–0.967) (20). To differentiate UC from CD, the only test included in our analysis was ANCA (Se, 0.553; 0.530–0.576/Sp, 0.885; 0.871–0.898) (20).
Diagnosis: Crohn’s Disease vs. Intestinal Tuberculosis
Mixed Population
IGRA (Se, 0.828; 0.784–0.855/Sp, 1.00; 0.867–0.896) (48) had better diagnostic performance than ASCA (Se, 0.828; 0.784–0.855/Sp, 0.867; 0.832–0.896) (25).
Activity
Mixed Population
For IBD, FC with a cutoff of 50 μg/g presented the highest sensitivity of 0.92 (0.90–0.94) (42), and MRE showed the highest specificity of 0.93 (0.90–0.95) (30). Besides, other radiological examinations [US, leukocyte scintigraphy (LS), and CT] all performed well with balanced sensitivity and specificity (6, 30, 43, 56, 59). However, other biomarkers (CRP and FL) were not as good as radiological examinations (27). One review suggested a sensitivity range of 0.64 to 0.93 and a specificity range of 0.71 to 1, showing that the diagnostic accuracy of TAUS (transabdominal US) remains inconclusive (Supplementary Table 3) (35).
For CD, US showed the best specificity of 0.977 (0.700–0.999) (6). Contrast-enhanced ultrasound (CEUS) was the most sensitive test with a sensitivity of 0.94 (0.87–0.97) (45). CT and MRE also performed well; however, the sensitivity of DWI-MRE was poor (23, 28, 34, 47). FC and FL performed slightly worse than CT and MRE (32, 55). For UC, US had both best sensitivity (0.886, 0.800–0.939) and specificity (0.819, 0.456–0.961) (6). Among other tests, the specificity of FIT and FL and the sensitivity of FC and FL were fair (32, 36).
Adults
For IBD, US and CT have similar diagnostic performance. The sensitivity of ultrasound was slightly higher (0.860; 0.745–0.928) (6), while the specificity of CT was slightly higher (0.86; 0.81–0.90) (43). Monoclonal anti-granulocyte antibody scintigraphy (MAAS) was sensitive (Se, 0.94; 0.89–0.97), but its specificity was not good (Sp, 0.45; 0.37–0.53) (43).
Children
For IBD, US had great performance: Se, 0.876 (0.542–0.977); Sp, 1.00 (6). One review reported the diagnostic accuracy of TAUS, but showed that it remained inconclusive (Supplementary Table 3) (35). The other review showed that the sensitivity of positron emission tomography/CT (PET/CT): 0.59 (0.36–0.79) (SBFT, small-bowel follow through, used as the reference standard); 0.86 (0.70–0.95) (colonoscopy used as the reference standard) and the specificity: 1.00 (0.77–1.00) and 0.50 (0.01–0.99), respectively (43).
Recurrence
Mixed Population
For IBD, the only test was FC (Se, 0.78; 0.72–0.83/Sp, 0.73; 0.68–0.77/AUC, 0.83) (40). For UC, the sensitivity and specificity of FC were 0.75 (0.70–0.79) and 0.77 (0.74–0.80), respectively (33). For CD, FC showed the sensitivity of 0.75 (0.64–0.84) and specificity of 0.71 (0.64–0.76) (40).
For postoperative CD, SICUS showed the highest sensitivity of 0.99 (0.99–1.00) (62). FC for clinical recurrence presented the highest specificity of 0.88 (0.80–0.93), while FC for endoscopic recurrence presented with better sensitivity (26). Besides, MRE and other subtypes of US performed well in both sensitivity and specificity (50, 51, 57).
Reviews Eligible for Update
We searched for newly published studies for each moderate quality review (Supplementary Appendix 6). After screening, 8 reviews (20, 22, 26, 28–30, 32, 35) have eligible new published studies. However, after calculation, no reviews need to be updated. The overview of updating was presented in Supplementary Appendix 12.
Discussion
Our detailed umbrella review synthesized existing systematic reviews and meta-analyses into one user-friendly document. A total of 106 associations, including 17 non-invasive tests, have been studied.
Main Findings
Evidence from the umbrella review suggests that FC (0.99) and FL (0.82) were the most sensitive markers for distinguishing IBD from non-IBD. Similarly, ANCA (0.971) and FL (0.95) were the most specific marker for this purpose. To distinguish IBD from IBS, the most sensitive one was FC (cutoff 50 μg/g, 0.97; cutoff 100 μg/g, 0.92) and the most specific marker was FL (0.94). To distinguish CD from UC, all tests had low sensitivity, with ASCA IgA (0.955) having the highest specificity. IGRA (Se, 0.828; Sp, 0.867) was the best test to distinguish CD from ITB. There is only one test to diagnose IBD from FGID and only one test to distinguish UC from CD, FC, and ANCA. As for assessing activity, US (Se, 0.864; Sp, 0.883) and MRE (Se, 0.83; Sp, 0.93) perform well. The sensitivity of FC (0.85) was also good. As for postoperative recurrence of CD, SICUS (0.99) had the highest sensitivity and FC (CR: 0.88) had the highest specificity. We concluded that biomarkers played a good role in diagnosis, while radiological examinations, especially MRE and US, were more prominent in assessing activity and predicting recurrence. Supplementary Table 4 presents the characteristic of diagnostic performance and clinical use of each test.
Strengths and Limitations
Compared with other studies summarizing non-invasive tests for IBD (65, 66), our umbrella review provides the first systematic appraisal of the evidence using robust criteria. We used the AMSTAR 2 tool to assess the quality of reviews and used CCA to evaluate the degree of overlapping and report the highest quality and most current review. Besides, our umbrella review included both blood, stool biomarkers and radiological examinations. Furthermore, we rigorously classified the assessments into age groups based on the exact age range of the primary studies included and into several groups to discuss the diagnostic performance in a different clinical condition more rigorously and reasonably.
Several limitations are present in this review. Lack of data, including missing meta-data, hindered the reporting of some elements of the umbrella review and lack of reviews of children or adults alone. In addition, one review (20) could not undergo the normal updating process because it did not report the included studies of each assessment. Besides, some reviews were rated as low quality for the most common reason: lack of protocol. However, registering protocol has been rare, especially in the IBD field. What’s more, since most articles do not report the value of AUC, we can’t do a good comparison and analysis of AUC.
Implications for Practice and Future Research
This comprehensive umbrella review could help clinicians make better decisions about the appropriate tests prior to endoscopy. In terms of diagnosis, we suggested that in patients with symptoms suggestive of IBD in whom the clinician considers endoscopy, FC could be a sensitive test for safely excluding IBD. For patients with a negative result, we recommend that they continue to be monitored rather than do endoscopic examination immediately, unless it is very urgent. In patients with a positive result, FL is a good choice because of their low false-positive rate and consequent reduction of unnecessary endoscopies if patients are willing to have a stool test; if not, ANCA is an alternative. Clinicians can use our results to select a specific marker based on the practical situation. If both tests are positive, the patient is highly likely to have IBD. Endoscopic examination can be followed to confirm the diagnosis and disease classification. Radiation examinations, especially US and MRE, performed well in the activity assessment and predicting relapse. For patients with CD, we recommend having FC or US tests regularly to monitor the disease activity. Specifically, US or MRE is recommended for patients requiring postoperative recurrence monitoring. For patients with UC, MRE is the best choice to assess activity and predict relapse.
Our results show that there are not many reviews for children, especially in activity assessment and predicting recurrence. However, the use of endoscopy, invasive and requiring general anesthesia, can lead to child disobedience and disapproval of parents. An attitude of “wait and see” may cause unnecessary concerns and loss of wellbeing in children with IBD. Therefore, high-quality prospective studies on non-invasive testing in children should be complemented.
Conclusion
In summary, this umbrella review summarized the diagnostic performance of non-invasive tests for IBD in different clinical conditions and age groups and offered our suggestions on how to use the non-invasive tests appropriately. Researchers and clinicians could choose a suitable test based on our results. Further studies on non-invasive tests in children are needed.
Data Availability Statement
The original contributions presented in this study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
Funding
This study was supported by the Natural Science Foundation of Jiangsu Province of China (BK20181492), the National Key Clinical Department of Laboratory Medicine of China in Nanjing, the Key Laboratory for Laboratory Medicine of Jiangsu Province (ZDXKB2016005), and the Priority Academic Program Development of Jiangsu Higher Education Institutions. The funder of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the manuscript.
Author Disclaimer
The corresponding authors had full access to all the data in the study and has final responsibility for the decision to submit for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.920732/full#supplementary-material
References
1. Ng SC, Shi HY, Hamidi N, Underwood FE, Tang W, Benchimol EI, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. (2017) 390:2769–78. doi: 10.1016/s0140-6736(17)32448-0
2. Buisson A, Gonzalez F, Poullenot F, Nancey S, Sollellis E, Fumery M, et al. Comparative acceptability and perceived clinical utility of monitoring tools: a nationwide survey of patients with inflammatory bowel disease. Inflamm Bowel Dis. (2017) 23:1425–33. doi: 10.1097/MIB.0000000000001140
3. Dulai PS, Peyrin-Biroulet L, Danese S, Sands BE, Dignass A, Turner D, et al. Approaches to integrating biomarkers into clinical trials and care pathways as targets for the treatment of inflammatory bowel diseases. Gastroenterology. (2019) 157:1032–43.e1. doi: 10.1053/j.gastro.2019.06.018
4. Allocca M, Danese S, Laurent V, Peyrin-Biroulet L. Use of cross-sectional imaging for tight monitoring of inflammatory bowel diseases. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. (2020) 18:1309–23.e4. doi: 10.1016/j.cgh.2019.11.052
5. Petryszyn P, Staniak A, Wolosianska A, Ekk-Cierniakowski P. Faecal calprotectin as a diagnostic marker of inflammatory bowel disease in patients with gastrointestinal symptoms: meta-analysis. Eur J Gastroenterol Hepatol. (2019) 31:1306–12. doi: 10.1097/meg.0000000000001509
6. Sagami S, Kobayashi T, Miyatani Y, Okabayashi S, Yamazaki H, Takada T, et al. Accuracy of ultrasound for evaluation of colorectal segments in patients with inflammatory bowel diseases: a systematic review and meta-analysis. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. (2020) 19:908–21.e6. doi: 10.1016/j.cgh.2020.07.067
7. Haddaway NR, Land M, Macura B. “A little learning is a dangerous thing”: a call for better understanding of the term ‘systematic review’. Environ Int. (2017) 99:356–60. doi: 10.1016/j.envint.2016.12.020
8. AMSTAR. Assessing the Methodological Quality of Systematic Reviews. (2017). Available online at: https://amstar.ca/Amstar_Checklist.php (accessed 2021).
9. Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ (Clin Res Ed). (2017) 358:j4008. doi: 10.1136/bmj.j4008
10. Holtman GA, Lisman-van Leeuwen Y, Day AS, Fagerberg UL, Henderson P, Leach ST, et al. Use of laboratory markers in addition to symptoms for diagnosis of inflammatory bowel disease in children a meta-analysis of individual patient data. JAMA Pediatr. (2017) 171:984–91. doi: 10.1001/jamapediatrics.2017.1736
11. Smith V, Devane D, Begley CM, Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol. (2011) 11:15. doi: 10.1186/1471-2288-11-15
12. Senn SJ. Overstating the evidence: double counting in meta-analysis and related problems. BMC Med Res Methodol. (2009) 9:10. doi: 10.1186/1471-2288-9-10
13. Bougioukas KI, Liakos A, Tsapas A, Ntzani E, Haidich AB. Preferred reporting items for overviews of systematic reviews including harms checklist: a pilot tool to be used for balanced reporting of benefits and harms. J Clin Epidemiol. (2018) 93:9–24. doi: 10.1016/j.jclinepi.2017.10.002
14. Pieper D, Antoine SL, Mathes T, Neugebauer EA, Eikermann M. Systematic review finds overlapping reviews were not mentioned in every other overview. J Clin Epidemiol. (2014) 67:368–75. doi: 10.1016/j.jclinepi.2013.11.007
15. Garner P, Hopewell S, Chandler J, MacLehose H, Schünemann HJ, Akl EA, et al. When and how to update systematic reviews: consensus and checklist. BMJ (Clin Res Ed). (2016) 354:i3507. doi: 10.1136/bmj.i3507
16. Vogelgesang F, Schlattmann P, Dewey M. The evaluation of bivariate mixed models in meta-analyses of diagnostic accuracy studies with SAS, Stata and R. Methods Inf Med. (2018) 57:111–9. doi: 10.3414/ME17-01-0021
17. Okoth K, Chandan JS, Marshall T, Thangaratinam S, Thomas GN, Nirantharakumar K, et al. Association between the reproductive health of young women and cardiovascular disease in later life: umbrella review. BMJ (Clin Res Ed). (2020) 371:m3502. doi: 10.1136/bmj.m3502
18. Chung M, Newberry SJ, Ansari MT, Yu WW, Wu H, Lee J, et al. Two methods provide similar signals for the need to update systematic reviews. J Clin Epidemiol. (2012) 65:660–8. doi: 10.1016/j.jclinepi.2011.12.004
19. Ahmadzai N, Newberry SJ, Maglione MA, Tsertsvadze A, Ansari MT, Hempel S, et al. A surveillance system to assess the need for updating systematic reviews. Syst Rev. (2013) 2:104.
20. Reese GE, Constantinides VA, Simillis C, Darzi AW, Orchard TR, Fazio VW, et al. Diagnostic precision of anti-Saccharomyces cerevisiae antibodies and perinuclear antineutrophil cytoplasmic antibodies in inflammatory bowel disease. Am J Gastroenterol. (2006) 101:2410–22. doi: 10.1111/j.1572-0241.2006.00840.x
21. von Roon AC, Karamountzos L, Purkayastha S, Reese GE, Darzi AW, Teare JP, et al. Diagnostic precision of fecal calprotectin for inflammatory bowel disease and colorectal malignancy. Am J Gastroenterol. (2007) 102:803–13. doi: 10.1111/j.1572-0241.2007.01126.x
22. Giles E, Barclay AR, Chippington S, Wilson DC. Systematic review: MRI enterography for assessment of small bowel involvement in paediatric Crohn’s disease. Alimentary Pharmacol Ther. (2013) 37:1121–31. doi: 10.1111/apt.12323
23. Qiu Y, Mao R, Chen BL, Li XH, He Y, Zeng ZR, et al. Systematic review with meta-analysis: magnetic resonance enterography vs. computed tomography enterography for evaluating disease activity in small bowel Crohn’s disease. Alimentary Pharmacol Ther. (2014) 40:134–46. doi: 10.1111/apt.12815
24. Zhou XL, Xu W, Tang XX, Luo LS, Tu JF, Zhang CJ, et al. Fecal lactoferrin in discriminating inflammatory bowel disease from irritable bowel syndrome: a diagnostic meta-analysis. BMC Gastroenterol. (2014) 14:121. doi: 10.1186/1471-230x-14-121
25. Ng SC, Hirai HW, Tsoi KK, Wong SH, Chan FK, Sung JJ, et al. Systematic review with meta-analysis: accuracy of interferon-gamma releasing assay and anti-Saccharomyces cerevisiae antibody in differentiating intestinal tuberculosis from Crohn’s disease in Asians. J Gastroenterol Hepatol. (2014) 29:1664–70. doi: 10.1111/jgh.12645
26. Qiu Y, Mao R, Chen BL, He Y, Zeng ZR, Xue L, et al. Fecal calprotectin for evaluating postoperative recurrence of Crohn’s disease: a meta-analysis of prospective studies. Inflamm Bowel Dis. (2015) 21:315–22. doi: 10.1097/mib.0000000000000262
27. Mosli MH, Zou G, Garg SK, Feagan SG, MacDonald JK, Chande N, et al. C-Reactive protein, fecal calprotectin, and stool lactoferrin for detection of endoscopic activity in symptomatic inflammatory bowel disease patients: a systematic review and meta-analysis. Am J Gastroenterol. (2015) 110:802–19, quiz 20. doi: 10.1038/ajg.2015.120
28. Ahmed O, Rodrigues DM, Nguyen GC. Magnetic resonance imaging of the small bowel in Crohn’s disease: a systematic review and meta-analysis. Can J Gastroenterol Hepatol. (2016) 2016:7857352. doi: 10.1155/2016/7857352
29. Kopylov U, Yung DE, Engel T, Avni T, Battat R, Ben-Horin S, et al. Fecal calprotectin for the prediction of small-bowel Crohn’s disease by capsule endoscopy: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. (2016) 28:1137–44. doi: 10.1097/meg.0000000000000692
30. Yoon HM, Suh CH, Kim JR, Lee JS, Jung AY, Kim KM, et al. Diagnostic performance of magnetic resonance enterography for detection of active inflammation in children and adolescents with inflammatory bowel disease: a systematic review and diagnostic meta-analysis. JAMA Pediatr. (2017) 171:1208–16. doi: 10.1001/jamapediatrics.2017.3400
31. Tham YS, Yung DE, Fay S, Yamamoto T, Ben-Horin S, Eliakim R, et al. Fecal calprotectin for detection of postoperative endoscopic recurrence in Crohn’s disease: systematic review and meta-analysis. Ther Adv Gastroenterol. (2018) 11:1756284818785571. doi: 10.1177/1756284818785571
32. Rokkas T, Portincasa P, Koutroubakis IE. Fecal calprotectin in assessing inflammatory bowel disease endoscopic activity: a diagnostic accuracy meta-analysis. J Gastrointestinal Liver Dis JGLD. (2018) 27:299–306. doi: 10.15403/jgld.2014.1121.273.pti
33. Li J, Zhao X, Li X, Lu M, Zhang H. Systematic review with meta-analysis: fecal calprotectin as a surrogate marker for predicting relapse in adults with ulcerative colitis. Mediators Inflamm. (2019) 2019:2136501. doi: 10.1155/2019/2136501
34. Bellini D, Rivosecchi F, Panvini N, Rengo M, Caruso D, Carbone I, et al. Layered enhancement at magnetic resonance enterography in inflammatory bowel disease: a meta-analysis. World J Gastroenterol. (2019) 25:4555–66. doi: 10.3748/wjg.v25.i31.4555
35. van Wassenaer EA, de Voogd FAE, van Rijn RR, van der Lee JH, Tabbers MM, Van Etten-Jamaludin FS, et al. Diagnostic accuracy of transabdominal ultrasound in detecting intestinal inflammation in paediatric IBD patients-a systematic review. J Crohn’s Colitis. (2019) 13:1501–9. doi: 10.1093/ecco-jcc/jjz085
36. Lee MW, Pourmorady JS, Laine L. Use of fecal occult blood testing as a diagnostic tool for clinical indications: a systematic review and meta-analysis. Am J Gastroenterol. (2020) 115:662–70. doi: 10.14309/ajg.0000000000000495
37. Jung ES, Lee SP, Kae SH, Kim JH, Kim HS, Jang HJ. Diagnostic accuracy of fecal calprotectin for the detection of small bowel Crohn’s disease through capsule endoscopy: an updated meta-analysis and systematic review. Gut Liver. (2020) 15:732–41. doi: 10.5009/gnl20249
38. Ahmad R, Ajlan AM, Eskander AA, Alhazmi TA, Khashoggi K, Wazzan MA, et al. Magnetic resonance imaging in the management of Crohn’s disease: a systematic review and meta-analysis. Insights Imaging. (2021) 12:118. doi: 10.1186/s13244-021-01064-9
39. Jellema P, van Tulder MW, van der Horst HE, Florie J, Mulder CJ, van der Windt DA. Inflammatory bowel disease: a systematic review on the value of diagnostic testing in primary care. Colorectal Dis Off J Assoc Coloproctol Great Britain Ireland. (2011) 13:239–54. doi: 10.1111/j.1463-1318.2009.02131.x
40. Mao R, Xiao YL, Gao X, Chen BL, He Y, Yang L, et al. Fecal calprotectin in predicting relapse of inflammatory bowel diseases: a meta-analysis of prospective studies. Inflamm Bowel Dis. (2012) 18:1894–9. doi: 10.1002/ibd.22861
41. Treglia G, Quartuccio N, Sadeghi R, Farchione A, Caldarella C, Bertagna F, et al. Diagnostic performance of Fluorine-18-Fluorodeoxyglucose positron emission tomography in patients with chronic inflammatory bowel disease: a systematic review and a meta-analysis. J Crohn’s Colitis. (2013) 7:345–54. doi: 10.1016/j.crohns.2012.08.005
42. Lin JF, Chen JM, Zuo JH, Yu A, Xiao ZJ, Deng FH, et al. Meta-analysis: fecal calprotectin for assessment of inflammatory bowel disease activity. Inflamm Bowel Dis. (2014) 20:1407–15. doi: 10.1097/mib.0000000000000057
43. Zhang J, Li LF, Zhu YJ, Qiu H, Xu Q, Yang J, et al. Diagnostic performance of 18F-FDG-PET versus scintigraphy in patients with inflammatory bowel disease: a meta-analysis of prospective literature. Nuclear Med Commun. (2014) 35:1233–46. doi: 10.1097/mnm.0000000000000202
44. Wang Y, Pei F, Wang X, Sun Z, Hu C, Dou H. Diagnostic accuracy of fecal lactoferrin for inflammatory bowel disease: a meta-analysis. Int J Clin Exp Pathol. (2015) 8:12319–32.
45. Serafin Z, Białecki M, Białecka A, Sconfienza LM, Klopocka M. Contrast-enhanced ultrasound for detection of Crohn’s disease activity: systematic review and meta-analysis. J Crohn’s Colitis. (2016) 10:354–62. doi: 10.1093/ecco-jcc/jjv196
46. Holtman GA, Lisman-van Leeuwen Y, Reitsma JB, Berger MY. Noninvasive tests for inflammatory bowel disease: a meta-analysis. Pediatrics. (2016) 137:e20152126., doi: 10.1542/peds.2015-2126
47. Choi SH, Kim KW, Lee JY, Kim KJ, Park SH. Diffusion-weighted magnetic resonance enterography for evaluating bowel inflammation in Crohn’s disease: a systematic review and meta-analysis. Inflamm Bowel Dis. (2016) 22:669–79. doi: 10.1097/mib.0000000000000607
48. Xu H, Li Y, Qian JM. [A Meta-analysis of the accuracy of interferon-γ release assays in differentiating intestinal tuberculosis from Crohn’s disease in Asia]. Zhonghua Nei Ke Za Zhi. (2016) 55:535–40. doi: 10.3760/cma.j.issn.0578-1426.2016.07.010
49. Deng C, Li W, Li J, Zhang S, Li Y. Diagnostic value of the antiglycoprotein-2 antibody for Crohn’s disease: a PRISMA-compliant systematic review and meta-analysis. BMJ Open. (2017) 7:e014843. doi: 10.1136/bmjopen-2016-014843
50. Yung DE, Har-Noy O, Tham YS, Ben-Horin S, Eliakim R, Koulaouzidis A, et al. Capsule endoscopy, magnetic resonance enterography, and small bowel ultrasound for evaluation of postoperative recurrence in Crohn’s disease: systematic review and meta-analysis. Inflamm Bowel Dis. (2017) 24:93–100. doi: 10.1093/ibd/izx027
51. Rispo A, Imperatore N, Testa A, Nardone OM, Luglio G, Caporaso N, et al. Diagnostic accuracy of ultrasonography in the detection of postsurgical recurrence in Crohn’s disease: a systematic review with meta-analysis. Inflamm Bowel Dis. (2018) 24:977–88. doi: 10.1093/ibd/izy012
52. Freeman K, Willis BH, Fraser H, Taylor-Phillips S, Clarke A. Faecal calprotectin to detect inflammatory bowel disease: a systematic review and exploratory meta-analysis of test accuracy. BMJ Open. (2019) 9:e027428. doi: 10.1136/bmjopen-2018-027428
53. An YK, Prince D, Gardiner F, Neeman T, Linedale EC, Andrews JM, et al. Faecal calprotectin testing for identifying patients with organic gastrointestinal disease: systematic review and meta-analysis. Med J Australia. (2019) 211:461–7. doi: 10.5694/mja2.50384
54. Gkiouras K, Grammatikopoulou MG, Theodoridis X, Pagkalidou E, Chatzikyriakou E, Apostolidou AG, et al. Diagnostic and clinical significance of antigen-specific pancreatic antibodies in inflammatory bowel diseases: a meta-analysis. World J Gastroenterol. (2020) 26:246–65. doi: 10.3748/wjg.v26.i2.246
55. Dai C, Jiang M, Sun MJ, Cao Q. Fecal lactoferrin for assessment of inflammatory bowel disease activity: a systematic review and meta-analysis. J Clin Gastroenterol. (2020) 54:545–53. doi: 10.1097/mcg.0000000000001212
56. Treglia G, Sadeghi R, Viccaro A, Muoio B, Giovanella L. Clinical role and accuracy of 18F-FDG PET in evaluating disease activity in patients with chronic inflammatory bowel disease: an updated systematic review and a bivariate meta-analysis. Clin Transl Imaging. (2017) 5:303–13. doi: 10.1007/s40336-017-0234-y
57. Bollegala N, Griller N, Bannerman H, Habal M, Nguyen GC. Ultrasound vs endoscopy, surgery, or pathology for the diagnosis of small bowel Crohn’s disease and its complications. Inflamm Bowel Dis. (2019) 25:1313–38. doi: 10.1093/ibd/izy392
58. Ye X, Wang Y, Wang HHX, Feng R, Ye Z, Han J, et al. Can fecal calprotectin accurately identify histological activity of ulcerative colitis? A meta-analysis. Ther Adv Gastroenterol. (2021) 14:1756284821994741. doi: 10.1177/1756284821994741
59. Alshammari MT, Stevenson R, Abdul-Aema B, Zou G, Jairath V, Radford S, et al. Diagnostic accuracy of non-invasive imaging for detection of colonic inflammation in patients with inflammatory bowel disease: a systematic review and meta-analysis. Diagnostics (Basel). (2021) 11:1926. doi: 10.3390/diagnostics11101926
60. Sun L, Han Y, Wang H, Liu H, Liu S, Yang H, et al. MicroRNAs as potential biomarkers for the diagnosis of inflammatory bowel disease: a systematic review and meta-analysis. J Int Med Res. (2022) 50:3000605221089503. doi: 10.1177/03000605221089503
61. Dai C, Jiang M, Sun MJ, Cao Q. Fecal immunochemical test for predicting mucosal healing in ulcerative colitis patients: a systematic review and meta-analysis. J Gastroenterol Hepatol. (2018) 33:990–7. doi: 10.1111/jgh.14121
62. Zhu C, Ma X, Xue L, Xu J, Li Q, Wang Y, et al. Small intestine contrast ultrasonography for the detection and assessment of Crohn disease: a meta-analysis. Medicine. (2016) 95:e4235. doi: 10.1097/md.0000000000004235
63. Kopylov U, Yung DE, Engel T, Vijayan S, Har-Noy O, Katz L, et al. Diagnostic yield of capsule endoscopy versus magnetic resonance enterography and small bowel contrast ultrasound in the evaluation of small bowel Crohn’s disease: systematic review and meta-analysis. Digest Liver Dis Off J Italian Soc Gastroenterol Italian Assoc Study Liver. (2017) 49:854–63. doi: 10.1016/j.dld.2017.04.013
64. Cui MH, Liu YL, Yu WD, Li XY. [Diagnostic value of antineutrophil cytoplasmic antibodies in patients with ulcerative colitis: a meta-analysis]. Zhonghua Yi Xue Za Zhi. (2008) 88:3116–9.
65. Ince MN, Elliott DE. Effective use of the laboratory in the management of patients with inflammatory bowel diseases. Gastroenterol Clin North Am. (2019) 48:237–58. doi: 10.1016/j.gtc.2019.02.006
Keywords: inflammatory bowel disease, non-invasive tests, diagnostic performance, Crohn’s disease, ulcerative colitis
Citation: Shi J-T, Zhang Y, She Y, Goyal H, Wu Z-Q and Xu H-G (2022) Diagnostic Utility of Non-invasive Tests for Inflammatory Bowel Disease: An Umbrella Review. Front. Med. 9:920732. doi: 10.3389/fmed.2022.920732
Received: 15 April 2022; Accepted: 30 May 2022;
Published: 11 July 2022.
Edited by:
Xiang Xue, University of New Mexico, United StatesReviewed by:
Jin-Xian Huang, The University of Hong Kong-Shenzhen Hospital, ChinaSalem Y. Mohamed, Zagazig University, Egypt
Ben Costello, University of the West of England, Bristol, United Kingdom
Copyright © 2022 Shi, Zhang, She, Goyal, Wu and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhi-Qi Wu, cWllY2hvQDEyNi5jb20=; Hua-Guo Xu, aHVhZ3VveHVAbmptdS5lZHUuY24=
†These authors have contributed equally to this work