Corrigendum: Impact of COVID-19 in-hospital mortality in chagas disease patients
 Gilberto Marcelo Sperandio da Silva1*
Gilberto Marcelo Sperandio da Silva1* Mauro Felippe Felix Mediano1Michele Ferreira Murgel1Patricia Mello Andrade1Marcelo Teixeira de Holanda1Andréa Rodrigues da Costa1Henrique Horta Veloso1Fernanda Martins Carneiro1Cláudia Maria Valete Rosalino1Andréa Silvestre de Sousa1Fernanda de Souza Nogueira Sardinha Mendes1Roberta Olmo Pinheiro2Valdiléa Gonçalves Veloso1Roberto Magalhães Saraiva1,3Alejandro Marcel Hasslocher-Moreno1,3
Mauro Felippe Felix Mediano1Michele Ferreira Murgel1Patricia Mello Andrade1Marcelo Teixeira de Holanda1Andréa Rodrigues da Costa1Henrique Horta Veloso1Fernanda Martins Carneiro1Cláudia Maria Valete Rosalino1Andréa Silvestre de Sousa1Fernanda de Souza Nogueira Sardinha Mendes1Roberta Olmo Pinheiro2Valdiléa Gonçalves Veloso1Roberto Magalhães Saraiva1,3Alejandro Marcel Hasslocher-Moreno1,3- 1Evandro Chagas National Institute of Infectious Diseases, Fiocruz, Rio de Janeiro, Brazil
- 2Leprosy Laboratory, Oswaldo Cruz Institute, Fiocruz, Rio de Janeiro, Brazil
- 3Ibero-American Network for Chagas Disease, Barcelona, Spain
The COVID-19 virus infection caused by the new SARS-CoV-2 was first identified in Rio de Janeiro (RJ), Brazil, in March 2020. Until the end of 2021, 504,399 COVID-19 cases were confirmed in RJ, and the total death toll reached 68,347. The Evandro Chagas National Institute of Infectious Diseases from Oswaldo Cruz Foundation (INI-Fiocruz) is a referral center for treatment and research of several infectious diseases, including COVID-19 and Chagas disease (CD). The present study aimed to evaluate the impact of COVID-19 on in-hospital mortality of patients with CD during the COVID-19 pandemic period. This observational, retrospective, longitudinal study evaluated all patients with CD hospitalized at INI-Fiocruz from May 1, 2020, to November 30, 2021. One hundred ten hospitalizations from 81 patients with CD (58% women; 68 ± 11 years) were evaluated. Death was the study's main outcome, which occurred in 20 cases. The mixed-effects logistic regression was performed with the following variables to test whether patients admitted to the hospital with a COVID-19 diagnosis would be more likely to die than those admitted with other diagnoses: admission diagnosis, sex, age, COVID-19 vaccination status, CD clinical classification, and the number of comorbidities. Results from multiple logistic regression analysis showed a higher risk of in-hospital mortality in patients diagnosed with COVID-19 (OR 6.37; 95% CI 1.78–22.86) compared to other causes of admissions. In conclusion, COVID-19 infection had a significant impact on the mortality risk of INI-Fiocruz CD patients, accounting for one-third of deaths overall. COVID-19 presented the highest percentage of death significantly higher than those admitted due to other causes during the COVID-19 pandemic.
Introduction
Chagas disease (CD) is a neglected tropical disease affecting the cardiovascular, digestive and central nervous systems (1). Chagas disease affects about 6–7 million people worldwide, and in Brazil, more than 1 million people are infected with Trypanosoma cruzi (T. cruzi) (2, 3). On 31 December 2019, the WHO was informed of many acute respiratory syndrome cases from unknown etiology detected in Wuhan City, Hubei Province of China. Few months later, WHO declared the COVID-19 pandemic caused by a new coronavirus (SARS-COV2) (4). By the end of 2021, the reported cases of COVID-19 in Brazil were 22,287,521, and the total death toll was 619,056 (5). In the same period, the state of Rio de Janeiro registered 504,399 cases and 68,347 deaths due to COVID-19 (6). Considering that Evandro Chagas National Institute of Infectious Diseases of Oswaldo Cruz Foundation (INI-Fiocruz) is a referral infectious disease center institution in Brazil, the Brazilian Ministry of Health supported the construction of a large hospital unit to face the COVID-19 pandemic, with a capacity for up to 200 beds for the intensive and semi-intensive treatment of patients infected by Sars-CoV-2 (7).
The literature regarding T. cruzi/SARS-CoV-2 coinfection is still scarce, especially considering patients with Chagas heart disease (CHD) (8). In addition, CHD involves a complex interaction between different processes related to tissue damage due to parasite persistence, inflammation, specific immune response, among other physiological abnormalities (9). Another important aspect to be considered in the case of T. cruzi/SARS-CoV-2 coinfection is that the CD population is aging, with individuals with CD also presenting a high prevalence of comorbidities (10, 11). Patients with CHD, especially those with comorbidities, may develop severe forms of COVID-19 (12).
A recent study on mortality in CD and COVID-19 coinfection showed that the presence of comorbidities and their number increased the risk of COVID-19 death (13). In addition, this study identified deaths of patients with CD followed at INI-Fiocruz, through an active search in the Extrajudicial Portal for consultations on births and deaths of the Judiciary of the state of Rio de Janeiro, who died during the pandemic period. It was observed that 31.43% of deaths had COVID-19 as the main cause. Molina et al. in a study that compared hospitalization outcomes in patients with CD and without CD, both with COVID-19 in 11 Brazilian hospitals, observed a similar mortality rate (32.3%) (14). Another study that evaluated the profile of deaths in Brazilian hospitals showed that COVID-19 was the main cause of death in 2020, surpassing deaths from cardiovascular diseases (15).
The preliminary evidence raised by these previous studies addressed CD patients with COVID-19, but did not compare hospitalized CD patients with and without COVID-19. Therefore, the present study aimed to assess the impact of COVID-19 on hospital mortality of patients with CD during the COVID-19 pandemic period.
Materials and Methods
Patients and Procedures
The present work is a single-center retrospective cohort study based on data collected from medical records of patients admitted at INI-Fiocruz hospital, located in Rio de Janeiro, Brazil, between May 1, 2020, and November 30, 2021.
All adult patients with CD diagnosis, confirmed by two different serological tests (ELISA, indirect immunofluorescence assay, or chemiluminescence test), and who had been admitted to INI-Fiocruz hospital center were included in this study.
The Brazilian consensus on Chagas disease (3) was used to assess the degree of cardiac involvement of the disease, based on electrocardiogram (EKG), echocardiogram (ECHO) and presence of heart failure (HF). Patients were classified into the following stages: indeterminate (normal EKG and ECHO, without HF); A (altered EKG, normal ECHO and no HF); B1 (altered EKG, altered ECHO with ventricular ejection fraction ≥45%, without HF); B2 (altered EKG, altered ECHO with ventricular ejection fraction <45%, without HF), C (altered EKG and ECHO with compensated HF); and D (altered EKG and ECHO with decompensated and treatment-refractory HF). Patients with symptoms such as fever, cough, sore throat, runny nose, and dyspnea were considered suspects of COVID-19. COVID-19 diagnosis was confirmed by SARS-CoV-2 positivity in real-time reverse-transcription PCR (RT-PCR) (Biomanguinhos kit [E+P1], Fiocruz, Brazil) of nasopharyngeal secretion and/or bronchoalveolar fluid. Patients with negative RT-PCR, but who had an epidemiological history and/or symptoms and clinical signs compatible with COVID-19, computed tomography (CT) chest with changes characteristic of COVID-19 pneumonia, including the presence of ground-glass opacities, was considered for the diagnosis.
The variables considered were age, sex, education level, COVID-19 vaccine, cause of hospital admission (COVID-19 vs. other causes), clinical features (oxygen saturation [SpO2], dyspnea, nausea, vomiting, cough, and fever), the need for respiratory support, RT-PCR results for SARS-COV-2 virus, hospitalization time, CD clinical forms (indeterminate, cardiac or digestive), and presence of comorbidities (systemic arterial hypertension, diabetes mellitus, dyslipidemia, and asthma).
Research Electronic Data Capture (REDCap) and Software R version 4.0.4 were used for data entry and analysis, respectively. Statistical analyzes were performed using the RStudio with the packages epiDisplay: Epidemiological Data Display Package (16). A statistical analysis was performed by descriptive analysis with numerical variables expressed as the mean + SD and the median. Student's t-test or the Mann–Whitney U-test was used to compare means between pairs of groups. Pearson's x2 test or Fisher's exact test for categorical variables was used for simple analysis of each variable for hospital admission (COVID-19 vs. other causes). Multivariate mixed logistic models were performed to test the hypothesis of whether patients admitted to the hospital with a COVID-19 diagnosis would be more likely to die than those admitted with other diagnoses. The mixed-effects logistic regression was performed using the glmer function in the lme4 R package, and estimates of the odds ratios were calculated using the tidy function in the broom mixed package. Models included a random intercept by patient. Multivariate analyses included the cause of hospital admission as the exposure variable (COVID-19 vs. other causes). They were adjusted by potential confounders such as sex, age, COVID-19 vaccination status, CD classification, and the number of comorbidities. Statistical significance was set at p-value < 0.05.
Results
A total of 81 CD patients were included; most of them were women, elderly individuals with <9 years of schooling. Most patients presented the CD cardiac form. There was a high prevalence of comorbidities, mainly systemic arterial hypertension, diabetes mellitus, and dyslipidemia. Only one-fifth of the patients reported no comorbidities (Table 1).
TABLE 1
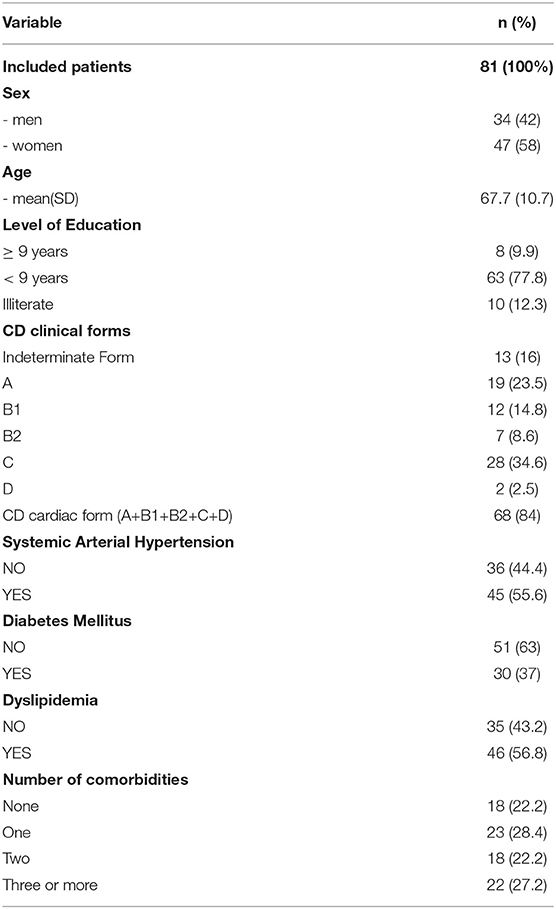
Table 1. Demographics and clinical characteristics of CD patients admitted to the INI-Fiocruz hospital (n = 81).
A total of 110 hospital admissions were observed in this study. Of the 81 patients, 61 patients were admitted once, 14 patients were admitted twice, three patients were admitted three times, and three patients were admitted four times during the study period. The frequency of sex, mean age, frequency of level of education, CD clinical forms, RT-PCR test, mean O2 saturation, frequency of COVID-19 vaccination, fever, cough, dyspnea, anosmia, CT chest exam, mean of hospitalization time, intensive care unit (ICU) admission, frequency of systemic arterial hypertension, diabetes mellitus, dyslipidemia, asthma, and number of comorbidities are depicted in Table 2. Regarding hospitalizations due to COVID-19, there was a significative higher frequency of positive PCR for COVID-19 (81.2%), fever (58.8%), cough (64.7%), dyspnea (82.4%), anosmia (11.8%), TC chest with presence of ground-glass opacities (82.4%), and admission on ICU (82.4%) than in patients admitted due to other causes (0%, 6.5%, 2.2%, 22.6%, 0%, 9.7% and 26.9%, respectively; all p < 0.05). Regarding the primary outcome of this study, there was a significative higher frequency of death in patients admitted due to COVID-19 (41.2%, p < 0.001) than in others (14%) (Table 2).
TABLE 2
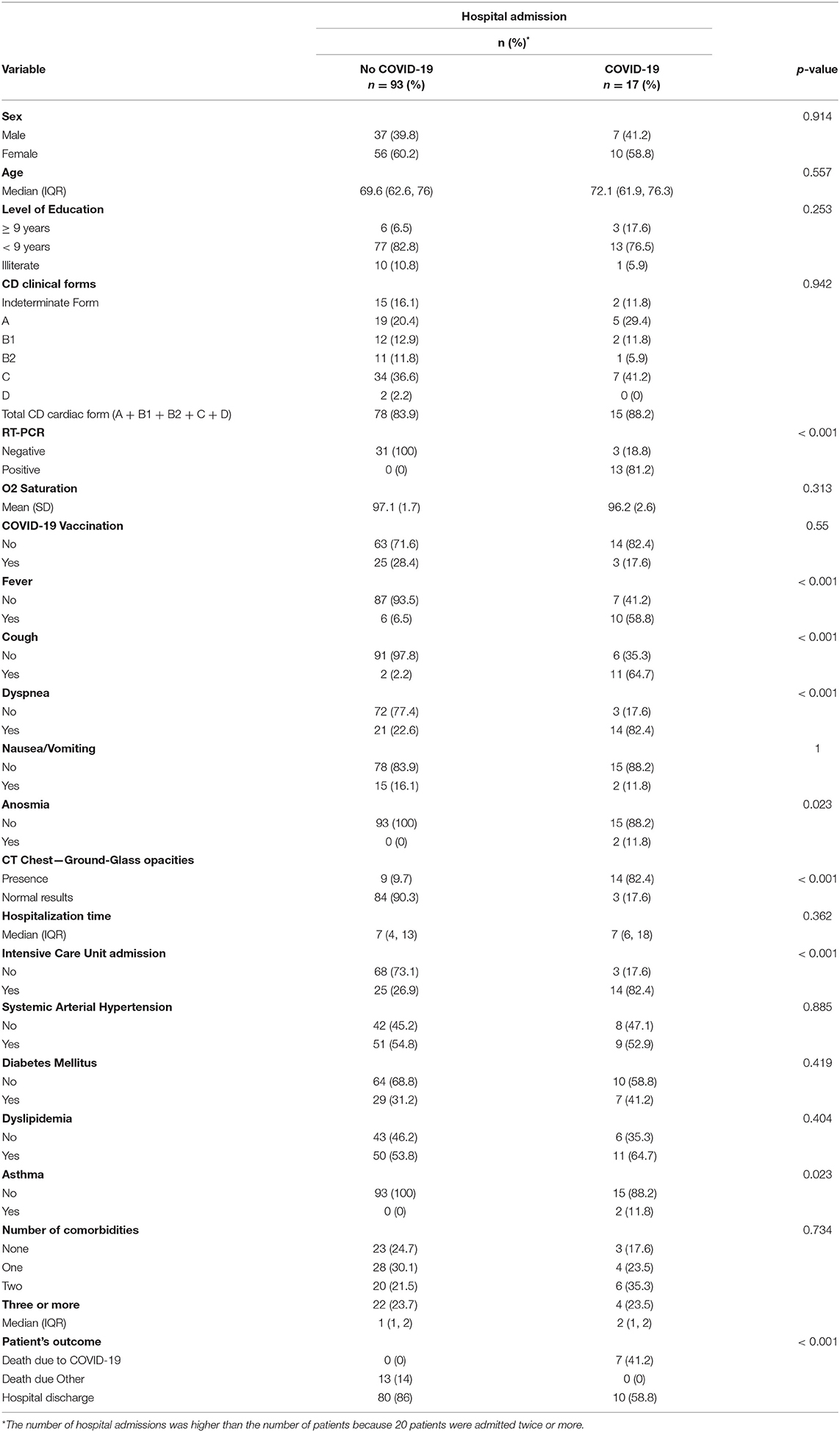
Table 2. Comparison of demographic and clinical characteristics between hospital admissions due to COVID-19 and other causes (n = 110).
The multiple logistic regression analysis considering the 110 hospitalizations showed a higher risk of in-hospital mortality in patients diagnosed with COVID-19 after adjustments for potential confounders (Table 3).
TABLE 3
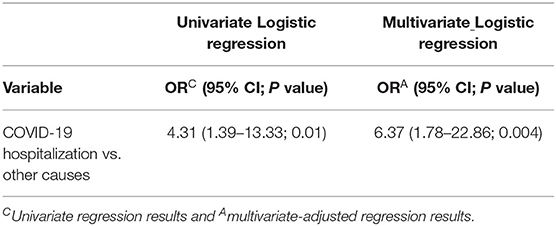
Table 3. Univariate and Multivariate Logistic regression results to assess whether CD patients diagnosed with COVID-19 on hospital admission have a higher chance of in-hospital mortality.
Discussion
Little is known about the impact of COVID-19 on the mortality of hospitalized CD patients during the COVID-19 pandemic. This study analyzed patients with CD who were admitted to a Brazilian hospital center specialized in the treatment of infectious diseases.
The mean age, sex, and comorbidities frequency presented by the patients of the present study were similar to those previously described in ambulatorial patients in our cohort (17). However, the prevalence of CHD patients in this study was higher (84% against 53.6%) than those previously described. This is expected since patients with the cardiac form are more likely to be hospitalized than those who do not have heart disease. In addition, previous studies suggest that systemic arterial hypertension, diabetes mellitus, and prior cardiovascular disease are important risk factors for severity and mortality in COVID-19 infected people (12).
The aging trend of our cohort and a higher prevalence of women had also been previously reported (10). Other study corroborates the previous aging trend and suggests an increase in the average age of the most severe cases (17). Similar to Molina et al. (14), there was a higher frequency of women in the present study and higher mean age among CD patients admitted to the hospital due to COVID-19.
According to Struyf et al. (18), symptoms such as cough, sore throat, fever, myalgia or arthralgia, fatigue, and headache may be present in patients with COVID-19, dyspnea, and anosmia are very specific signs of COVID-19. The present study corroborates that these symptoms are frequent among CD patients with COVID-19.
In our study, the sensitivity of RT-PCR was 81.2%, as described in other studies (19). The three patients diagnosed with COVID-19, and who had negative RT-PCR, had CT chest compatible with COVID-19 pneumonia. Overall, RT-PCR shows low sensitivity in diagnosing patients with COVID-19 infection compared to the CT chest (20).
Molina et al. (14) showed a 32.3 % in-hospital mortality rate in CD patients with COVID-19, similar to the one we described in the present study (33.3%). Moreover, in our study, multivariate analysis indicated that CD patients hospitalized due to COVID-19 had 6 times greater risk of in-hospital mortality than those hospitalized due to other causes. Considering this context, Zimmermann et al. (15) results corroborate our observation, indicating that COVID-19 was the leading cause of death in public hospitals in Brazil in 2020, superior to mortality due to other causes.
In conclusion, COVID-19 infection caused a significant impact on the mortality risk of CD patients. COVID-19 presented the highest percentage of death that was significantly higher than those admitted due to other causes during the COVID-19 pandemic period.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
This study was approved by the INI-Fiocruz Research Ethics Committee (number CAAE: 35748820.1.0000.5262) on September 2, 2020, and was carried out in accordance with the 1964 Declaration of Helsinki and its later amendments. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
AH-M, MMu, MMe, AC, FC, and PA collected, interpreted data, and prepared tables. GS, AH-M, RS, and MMe analyzed the data. MMe, MMu, PA, MH, AC, HV, FC, CV, AS, FM, RP, VV, RS, and AH-M reviewed and edited the manuscript. GS, MH, CV, AS, FM, RP, VV, AC, HV, FC, MMe, RS, and AH-M conceptualized, designed study, supervised the study, and interpreted data. GS wrote the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the Evandro Chagas National Institute of Infectious Diseases, Oswaldo Cruz Foundation (Fiocruz), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES – Telemedicina e Análise de Dados Médicos no 12/2020, processo: 23038.004292/2020-80), Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq - bolsa de produtividade, number: 313327/2018_1).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Saraiva RM, Mediano MFF, Mendes FS, Sperandio da Silva GM, Veloso HH, Sangenis LHC, et al. Chagas heart disease: an overview of diagnosis, manifestations, treatment, and care. World J Cardiol. (2021) 13:654–75. doi: 10.4330/wjc.v13.i12.654
2. World Health Organization. Global Distribution of Cases of Chagas Disease Based on Official Estimates, 2018. World Health Organization (2018). Available online at: https://www.who.int/docs/default-source/ntds/chagas-disease/chagas-2018-cases.pdf?sfvrsn=f4e94b3b_2 (accessed April 13, 2022).
3. Dias JCP, Ramos AN Jr, Gontijo ED, Luquetti A, Shikanai-Yasuda MA, Coura JR, et al. 2nd Brazilian Consensus on Chagas Disease, 2015. Rev Soc Bras Med Trop. (2016) 49:3–60. doi: 10.1590/0037-8682-0505-2016
4. World Health Organization (WHO). Archived: WHO Timeline - COVID-19. (2020). Available online at: https://www.who.int/news/item/27-04-2020-who-timeline—covid-19 (accessed January 29, 2022).
5. Ministerio da Saúde do Brasil. Painel Coronavírus. (2022). Available online at: https://covid.saude.gov.br/ (accessed January 28, 2022).
6. Prefeitura da Cidade do Rio de Janeiro. Painel Rio COVID-19. (2022). Available online at: https://www.data.rio/apps/painel-rio-covid-19/explore (accessed January 28, 2022).
7. Fundação Oswaldo Cruz. Fiocruz constrói Centro Hospitalar para a Pandemia de Covid-19. (2020). Available online at: https://portal.fiocruz.br/noticia/fiocruz-constroi-centro-hospitalar-para-pandemia-de-covid-19-0 (Accessed January 28, 2022).
8. Diaz-Hernandez A, Gonzalez-Vazquez MC, Arce-Fonseca M, Rodriguez-Morales O, Cedilllo-Ramirez ML, Carabarin-Lima A. Risk of COVID-19 in Chagas disease patients: what happen with cardiac affectations? Biology. (2021) 10:411. doi: 10.3390/biology10050411
9. Zaidel EJ, Forsyth CJ, Novick G, Marcus R, Ribeiro ALP, Pinazo M-J, et al. COVID-19: implications for people with Chagas disease. Glob Heart. (2020) 15:69. doi: 10.5334/gh.891
10. Vizzoni AG, Varela MC, Sangenis LHC, Hasslocher-Moreno AM, do Brasil PEAA do B, Saraiva RM. Ageing with Chagas disease: an overview of an urban Brazilian cohort in Rio de Janeiro. Parasit Vectors. (2018) 11:2–8. doi: 10.1186/s13071-018-2929-y
11. Xavier IGG, Vieira MC, Rodrigues Junior LF, Sperandio da Silva GM, da Silva PS, de Holanda MT, et al. Prevalence of metabolic syndrome and associated factors among patients with chronic Chagas disease. PLoS ONE. (2021) 16:e0249116. doi: 10.1371/journal.pone.0249116
12. de Almeida-Pititto B, Dualib PM, Zajdenverg L, Dantas JR, de Souza FD, Rodacki M, et al. Severity and mortality of COVID 19 in patients with diabetes, hypertension and cardiovascular disease: a meta-analysis. Diabetol Metab Syndr. (2020) 12:75. doi: 10.1186/s13098-020-00586-4
13. Hasslocher-Moreno AM, Saraiva RM, Sperandio da Silva GM, Xavier SS, Sousa AS, Costa AR da, et al. Chagas disease mortality during the coronavirus disease 2019 pandemic: a Brazilian referral center experience. Rev Soc Bras Med Trop. (2022) 55:e0562. doi: 10.1590/0037-8682-0562-2021
14. Molina I, Marcolino MS, Pires MC, Ramos LEF, Silva RT, Guimarães-Júnior MH, et al. Chagas disease and SARS-CoV-2 coinfection does not lead to worse in-hospital outcomes. Sci Rep. (2021) 11:20289. doi: 10.1038/s41598-021-96825-3
15. Zimmermann IR, Sanchez MN, Alves LC, Frio GS, Cavalcante FV, Cortez-Escalante JJ, et al. COVID-19 as the leading cause of hospital deaths in the Brazilian public health system in 2020. Int J Infect Dis. (2021) 113:162–5. doi: 10.1016/j.ijid.2021.09.077
16. R Core Team. R: A language environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria (2021). Available online at: https://www.R-project.org/
17. Hasslocher-Moreno AM, Saraiva RM, Brasil PEAA do, Sangenis LHC, Xavier SS, Sousa AS de, et al. Temporal changes in the clinical-epidemiological profile of patients with Chagas disease at a referral center in Brazil. Rev Soc Bras Med Trop. (2021) 54:e0040–2021. doi: 10.1590/0037-8682-0040-2021
18. Struyf T, Deeks JJ, Dinnes J, Takwoingi Y, Davenport C, Leeflang MM, et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease. Cochrane Database Syst Rev. (2020) 7:CD013665. doi: 10.1002/14651858.CD013665
19. Long C, Xu H, Shen Q, Zhang X, Fan B, Wang C, et al. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur J Radiol. (2020) 126:108961. doi: 10.1016/j.ejrad.2020.108961
Keywords: Chagas disease, SARS-CoV-2, COVID-19, in-hospital mortality, Trypanosoma cruzi
Citation: Sperandio da Silva GM, Mediano MFF, Murgel MF, Andrade PM, Holanda MTd, da Costa AR, Veloso HH, Carneiro FM, Valete Rosalino CM, de Sousa AS, Mendes FdSNS, Pinheiro RO, Veloso VG, Saraiva RM and Hasslocher-Moreno AM (2022) Impact of COVID-19 In-hospital Mortality in Chagas Disease Patients. Front. Med. 9:880796. doi: 10.3389/fmed.2022.880796
Received: 22 February 2022; Accepted: 31 March 2022;
Published: 09 May 2022.
Edited by:
Reinaldo Bulgarelli Bestetti, University of Ribeirão Preto, BrazilReviewed by:
Rafael B. Polidoro, Indiana University Bloomington, United StatesCelio Geraldo Freire-de-Lima, Federal University of Rio de Janeiro, Brazil
João Marcos Ferreira, Universidade do Estado do Amazonas, Brazil
Copyright © 2022 Sperandio da Silva, Mediano, Murgel, Andrade, de Holanda, da Costa, Veloso, Carneiro, Valete Rosalino, de Sousa, Mendes, Pinheiro, Veloso, Saraiva and Hasslocher-Moreno. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gilberto Marcelo Sperandio da Silva, Z2lsYmVydG9tYXJjZWxvQGdtYWlsLmNvbQ==; Z2lsYmVydG8uc2lsdmFAaW5pLmZpb2NydXouYnI=