 Céline Jamart1Hervé Levesque1Sara Thietart2Olivier Fain2Sébastien Rivière2Ygal Benhamou1†
Céline Jamart1Hervé Levesque1Sara Thietart2Olivier Fain2Sébastien Rivière2Ygal Benhamou1† Arsène Mekinian2,3*†
Arsène Mekinian2,3*†- 1Service de Médecine Interne, Hôpital Rouen, Université de Rouen, Rouen, France
- 2Sorbonne Université, APHP, Service de Médecine Interne-DMU i3, Hôpital Saint-Antoine, Paris, France
- 3INSERM U938, Centre de Recherche Saint-Antoine, Paris, France
Objective: Ischemic digital ulcers (DUs) are frequent and severe complications of systemic sclerosis (SSc). Treatment options for SSc-related digital vasculopathy are based on aggressive vasodilation, with the objective to improve blood flow in ischemic areas. Intravenous prostanoids are recommended to treat active DUs. However, the level of evidence for the duration of 5 days is low. Therefore, the aim of this study was to determine whether prolonging the infusion beyond 5 days increases the rate of healing of active DUs in SSc.
Methods: This is an observational longitudinal retrospective bicenter study from 2000 to 2017. The objective was to compare the healing rate and time (defined by a healing of at least 50% of DUs) between two durations of iloprost administration: 5 days or less, or more than 5 days.
Results: Forty-one patients, with a mean age of 47 ± 15 years at diagnosis and 32 (78%) females have been included. Systemic sclerosis was diffuse in 10 (24%) cases and 13 (32%) had an interstitial lung disease. A total of 243 iloprost infusions for DUs were performed: 140 infusions for 5 days or less, and 103 infusions for more than 5 days (prolonged duration). Patients with active DUs which received >5 days of iloprost had higher modified Rodnan skin scale at the time of iloprost infusion (median 33 vs. 15; p < 0.05), more interstitial lung disease (44 vs. 27%; p < 0.05), more anti-topoisomerase I antibody positivity (59 vs. 44%; p < 0.05), and received more previous cyclophosphamide therapy (48 vs. 19%; p < 0.05). While the number of active DUs before iloprost infusion was not significantly different among those who received ≤5 days and >5 days of iloprost, the time to healing after iloprost infusion significantly decreased in SSc patients who received >5 days iloprost infusion: 48 [7–392] vs. 91 [9–365] days (p < 0.05). The proportion of SSc patients with healed DUs tended to increase in patients with >5 days iloprost infusion (log rank = 0.06). The number of patients with complete DU healing at day 90 was significantly increased in SSc who received >5 days of iloprost: 53 (51%) vs. 52 (37%) (p < 0.05). In addition, the time to healing was not significantly associated with the use of calcium channel blockers, endothelin receptor antagonists or a combination of PDE-5 inhibitors.
Conclusion: Prolonging duration of iloprost >5 days could improve the healing rate and the time to healing of SSc-related DUs. Prospective randomized studies are needed to confirm these data and define the optimal duration of iloprost therapy.
HIGHLIGHTS
- Iloprost infusion during more than 5 days improves the healing rate and the time to healing, as well as the proportion of healed DUs at 3 months in SSc-related DUs.
- The value of endothelin receptor antagonists or a combination of PDE-5 inhibitors and of hemodilution during the iloprost infusion remains to be determined.
- Pursuing calcium channel blockers during the iloprost infusion is associated with increased infusion-related side effects.
Introduction
Systemic sclerosis (SSc) is a severe connective tissue disease in which vasculopathy, autoimmunity and fibrosis are the key events. Despite the progress that has been made in early diagnosis and management of organ-based complications, many challenges still remain in the management of SSc. Therefore, DUs are still common in the course of SSc (from 24 to 58%), and are a major source of disability (1, 2). The presence of DUs has been identified as an independent risk factor of mortality (3). Management of DUs includes a local treatment, such as non-invasive debridement and occlusive dressings, and a systemic administration of calcium-channel inhibitors. A combination of iloprost infusions and phosphodiesterase 5 inhibitors are used in severe cases.
Several clinical trials evaluated the efficacy of iloprost for SSc-related DUs (4–8). In two multicenter double-blinded randomized trials, infusion of iloprost (0.5–2.0 ng/kg/min over 6 h, during 5 consecutive days) was associated with significantly greater proportion of DU healings in comparison to placebo (7, 8). In a meta-analysis of therapies for DU prevention and healing, oral prostanoids (iloprost, beraprost, cisaprost, and treprostinil) were not associated with less occurrence of new DUs, when compared with placebo (9).
Unlike thromboangiitis obliterans, where the duration of iloprost infusion is well-established, the optimal schedule of iloprost infusion in SSc has not yet been defined. Therefore, the benefit of prolonged iloprost therapy is uncertain for SSc patients (10). In addition, the value of additional drugs, such as endothelin receptor antagonists (ERAs, i.e., bosentan) and phosphodiesterase 5 inhibitors (PDE-5, i.e., sildenafil) concomitant to iloprost infusion remains to be determined.
In this retrospective study, we therefore aimed (1) to compare the time to healing between two regimens of ilosprost administration: duration greater than 5 days, or 5 days or less; (2) to assess the factors associated with the time to healing, particularly the benefit of concomitant use of endothelin receptor antagonists with phosphodiesterase 5 inhibitors.
Patients and Methods
Study Design
The study was a bicenter retrospective observational study carried out in two tertiary medical centers labeled as reference centers for SSc. All patients with SSc who received at least 3 consecutive days of iloprost infusion for DUs between January 2000 and January 2017 were included. Patients were also subjected to local therapy as debridement and topical medications.
Patients
The inclusion criteria were as follows: (1) age ≥ 18 years; (2) limited or diffuse SSc (ACR/EULAR criteria) (11); (3) at least one active digital ischemic ulcer, defined as a lesion with visually discernable depth and a loss of continuity of epithelial coverage, which could be denuded or covered by a scab or necrotic tissue, localized at distal to the proximal interphalangeal joints and without bone infection or calcinosis (12); (4) at least 3 consecutive days of iloprost infusion (Figure 1).
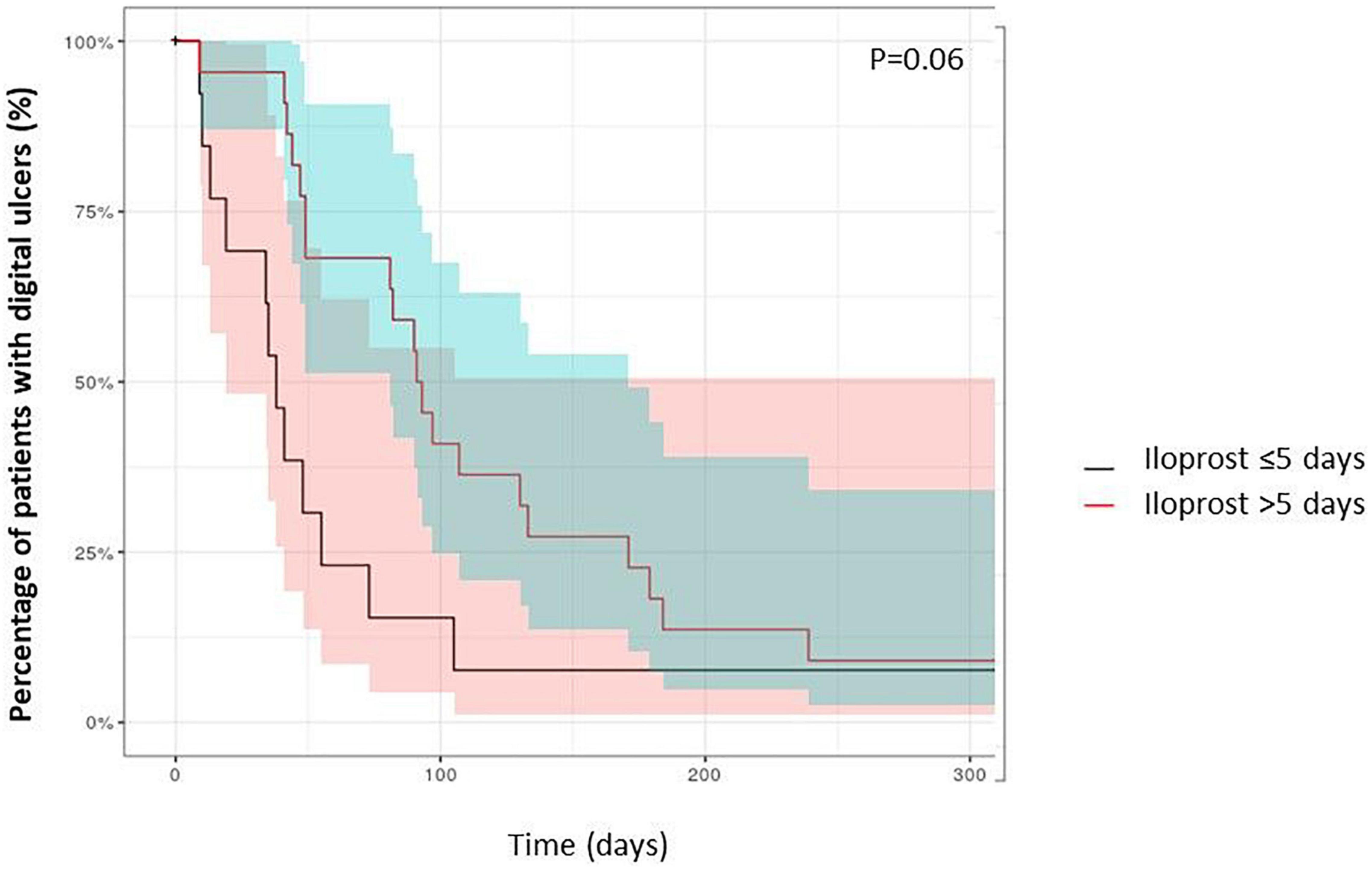
Figure 1. Time to healing of digital ulcers of SSc patients (Kaplan Meyer curves).
Data Collection
Data were collected retrospectively from patients’ charts at the time of iloprost infusion, and at each visit and/or hospitalization after the infusion during the next 90 days and until the last available visit. Baseline data, including patients’ demographics, history and presentation of SSc, organ involvement, autoantibodies, factors associated with digital ischemia (hypertension, smoking, body mass index, diabetes mellitus, cholesterol levels), and treatments were analyzed. Features of iloprost regimen were analyzed as follows: infusion rate, peripheral or central intravenous line, duration and tolerance. Each iloprost cession was considered and all iloprost cessions were pooled to analyze a cumulative prevalence of ulcers healing and time to healing. Healing was defined as complete re-epithelialisation and was considered only when it was notified in the medical files.
Ethical Considerations
This study was conducted in compliance with the Good Clinical Practices protocol and Declaration of Helsinki principles. The study being retrospective and observational, French law did not require formal approval from an ethics committee.
Statistical Analyses
Descriptive statistics [mean, median, range, standard deviation (SD)] are reported for quantitative variables. Numbers and percentages were calculated for categorical variables. To identify potential confounding factors influencing DU healing, we used Fisher’s exact test or Mann Whitney test, and univariate regression analyses were performed. We analyzed a pooled analysis of all active ulcers among 41 patients which received at least one iloprost infusion (a total of n = 243 infusions), and compared patients which received ≤5 days and >5 days of iloprost infusions and determined the time to healing. The Gray cumulative model was used to consider the comparison between all pooled patients iloprost lines of therapy depending on the number of days of iloprost infusion. A p value less than 0.05 was considered as significant.
Results
Patients’ Characteristics
Forty-one patients (32 females, mean age 47 ± 15 years) had been included. Disease duration from the first non-Raynaud symptom was 6 ± 5.2 years. SSc was diffuse in 10 (24%) cases and 13 (32%) have an interstitial lung disease (Table 1). Prevalence of anti-topoisomerase I, anti-centromeres and anti RNA polymerase III antibodies was 16 (40%), 12 (30%), and 3 (7.5%), respectively.
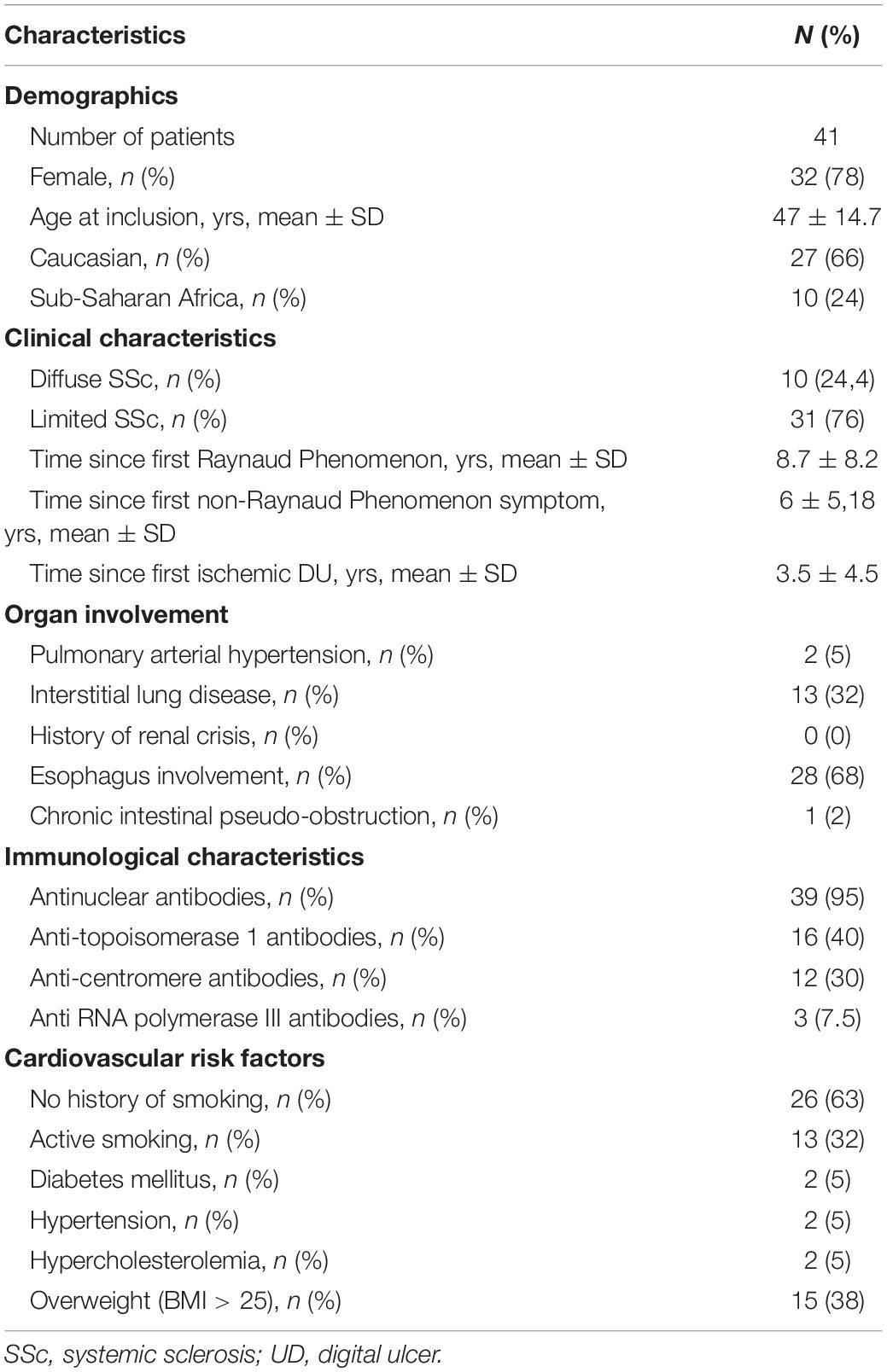
Table 1. Characteristics of 41 patients with SSc.
Iloprost Infusions for Digital Ulcers
Overall, 41 patients received 243 iloprost infusions for DUs. The median infusion duration was at 7.3 days (3–28), with a median infusion rate of 1.7 ng/kg/min. The characteristics between patients who received ≤5 days of iloprost (n = 140 infusions) to those who received >5 days iloprost therapy (n = 103 infusions) are detailed in Table 2, and all patients received consecutive iloprost infusions. The median number of iloprost cessions was 3 (1–12) with median interval between iloprost cessions at 6 weeks (4–42). The number of active DU before overall iloprost infusions was at 3 (1–12). Patients received immunosuppressive therapies at the time of iloprost infusion in 123 cases, with cyclophosphamide (n = 101), mycophenolate mofetil (n = 8), methotrexate (n = 47), and rituximab (n = 14). Patients with active DUs which received iloprost during >5 days had a higher modified Rodnan skin scale at the time of iloprost infusion (median 33 vs. 15; p < 0.05), more frequent interstitial lung diseases (44 vs. 27%; p < 0.05), anti-topoisomerase I antibodies positivity (59 vs. 44%; p < 0.05), and previous cyclophosphamide therapy (48 vs. 19%; p < 0.05) (Table 2). Healing time after iloprost infusion was significantly lower in SSc patients who received >5 days of iloprost [48 (7–392) days] in comparison with patients with ≤5 days of iloprost infusion [91 (9–365) days; p < 0.05] (Figure 2). The number of active DUs was similar between the two groups: 3 (1–12) vs. 3 (1–10) (p = 0.2). There was a tendency toward a higher proportion of patients with healed DUs among patients with a longer iloprost regimen (log rank = 0.06) (Figure 3). The number of patients with complete DU healing at day 90 was significantly higher among patients who received >5 days of iloprost: 51 vs. 37% (p < 0.05).
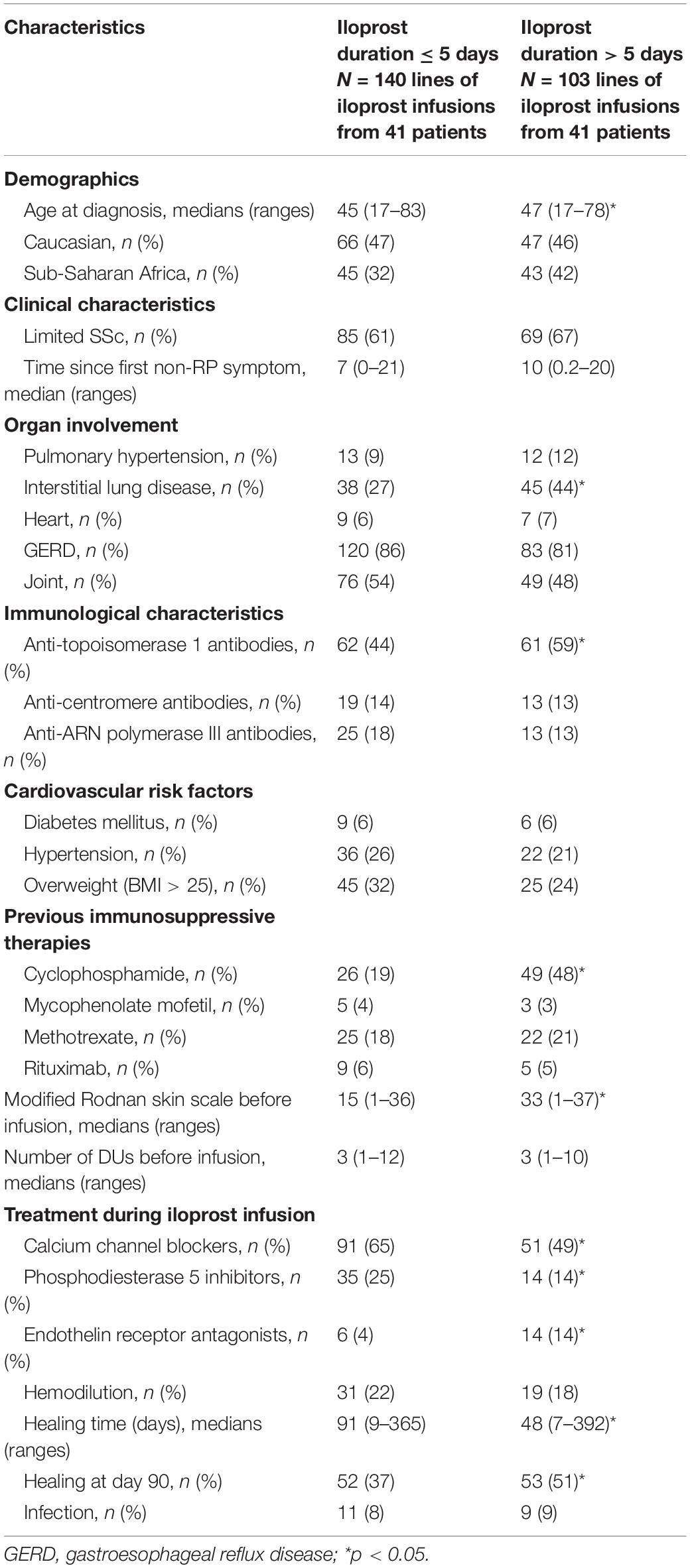
Table 2. Systemic sclerosis features and DUs outcome in patients treated with ≤5 days and >5 days of iloprost infusions: data expressed as number of all lines of iloprost infusions from 41 SSc patients.
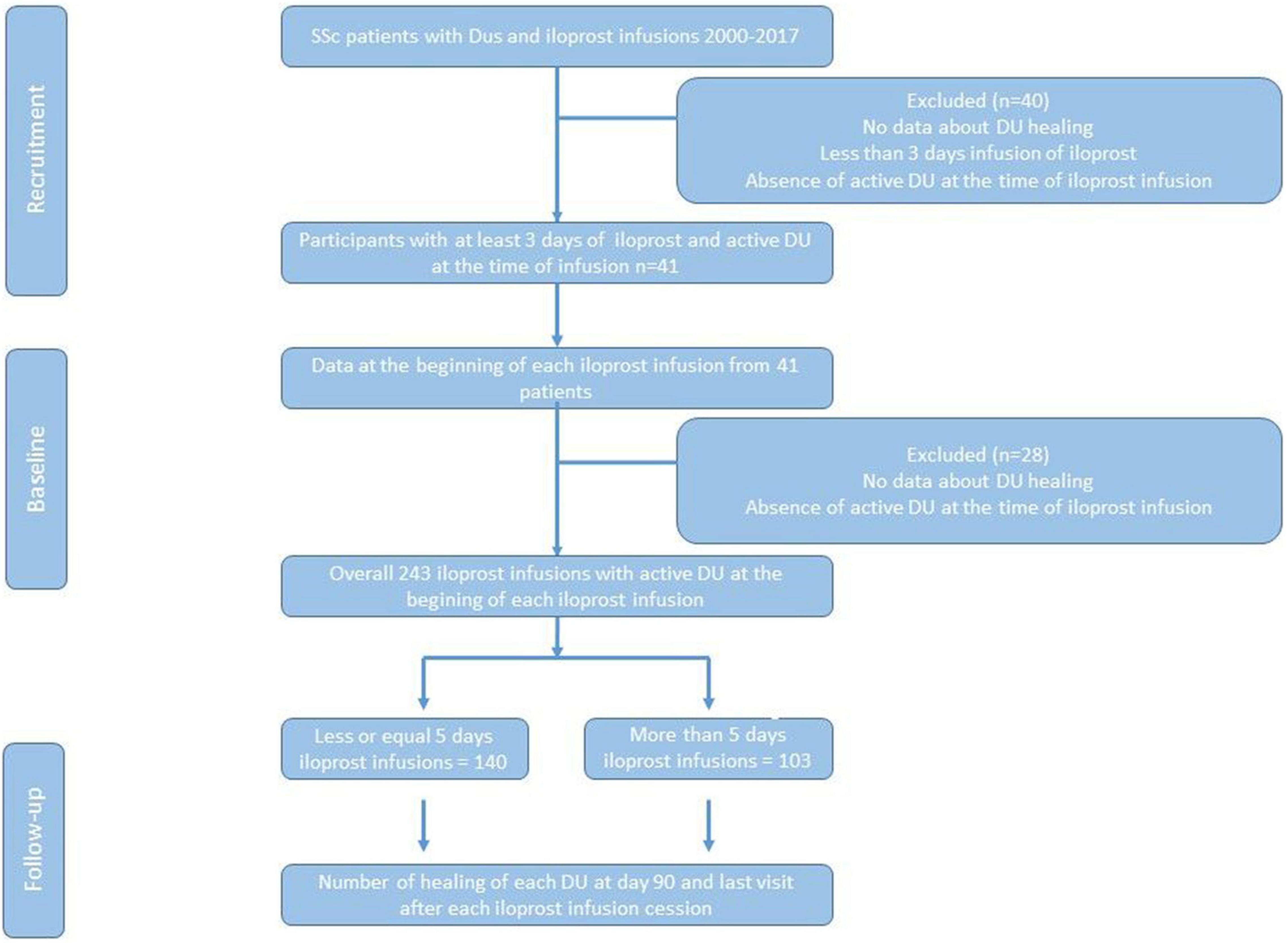
Figure 2. Study flow chart.
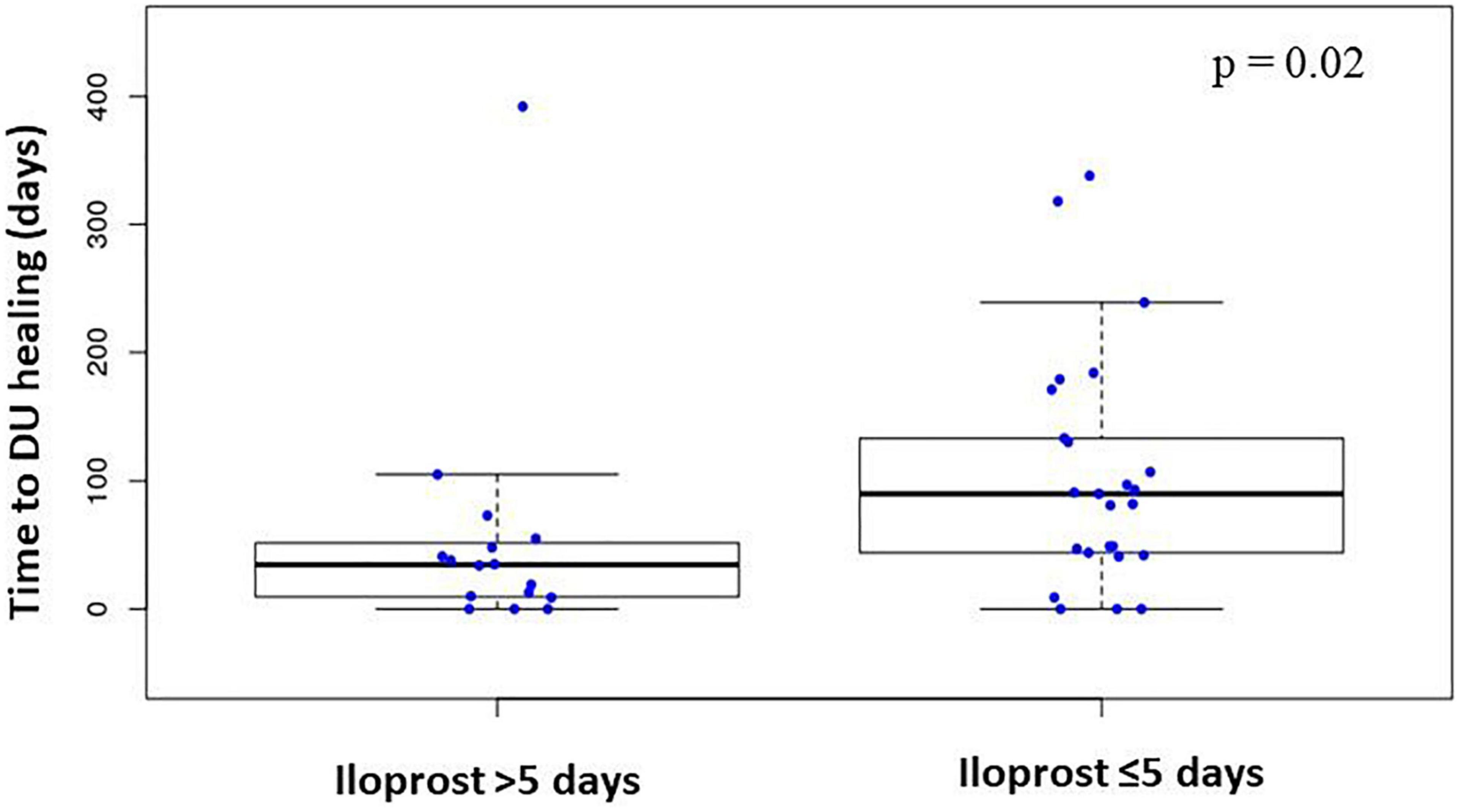
Figure 3. Time to digital ulcers healing in SSc patients with iloprost infusion less or more than 5 days.
Use of calcium channel blockers and PDE-5 inhibitors was less frequent among patients who received >5 days of iloprost, in comparison with patients with the shorter regimen, whereas the concomitant use of endothelin receptor antagonists was more common in these patients (Table 2). Healing time was not significantly modified by the use of calcium channel blockers, endothelin receptor antagonists or of a combination of PDE-5 inhibitors. In addition, the number of DUs and the type of immunosuppressive therapies did not influence healing (data not shown).
The number of DU complications (osteitis and/or gangrene and/or amputation) was not significantly different between groups (p = 0.42).
Safety
At least one adverse event was noted in 51% cases (mostly headaches and nausea), and 20% presented severe side effects (hypotension, incoercible vomiting). Interestingly, adverse events were more common in patients who received concomitant calcium channel blockers (63 vs. 56%; p = 0.045).
Discussion
The determination of the optimal duration of iloprost infusions remains a challenge. We report in this retrospective study that extending iloprost treatment for more than 5 days could be an attractive option for active DUs, especially in patients with severe diffuse SSc. Indeed, prolonged infusions of iloprost shortened the healing time by half, in comparison with patients with shorter treatment duration. The value of endothelin receptor antagonists or the combination of PDE-5 inhibitors remains to be determined, while continuation of calcium-channel blockers was associated with higher proportion of adverse side effects.
Although there is some evidence from clinical trials to use iloprost for SSc-related DUs, administration of iloprost in clinical practice follows various non-validated regimens, often based on the physician’s experience (Tables 3, 4; 2–8, 10–28). In addition, some reports have pointed out that long-term recurrent administration of iloprost was associated with no recurrence of DU (20). Unlike thromboangeitis obliterans or peripheral artery disease, the optimal duration and the frequency of iloprost infusions in SSc patients are uncertain. Therefore, guidelines do not provide any recommendations on iloprost dosage and regimen. Herein, using a clinical endpoint (the healing of DUs), the use of a prolonged regimen of iloprost was associated with a shorter healing time and a trend toward higher proportions of patients with healed DUs.
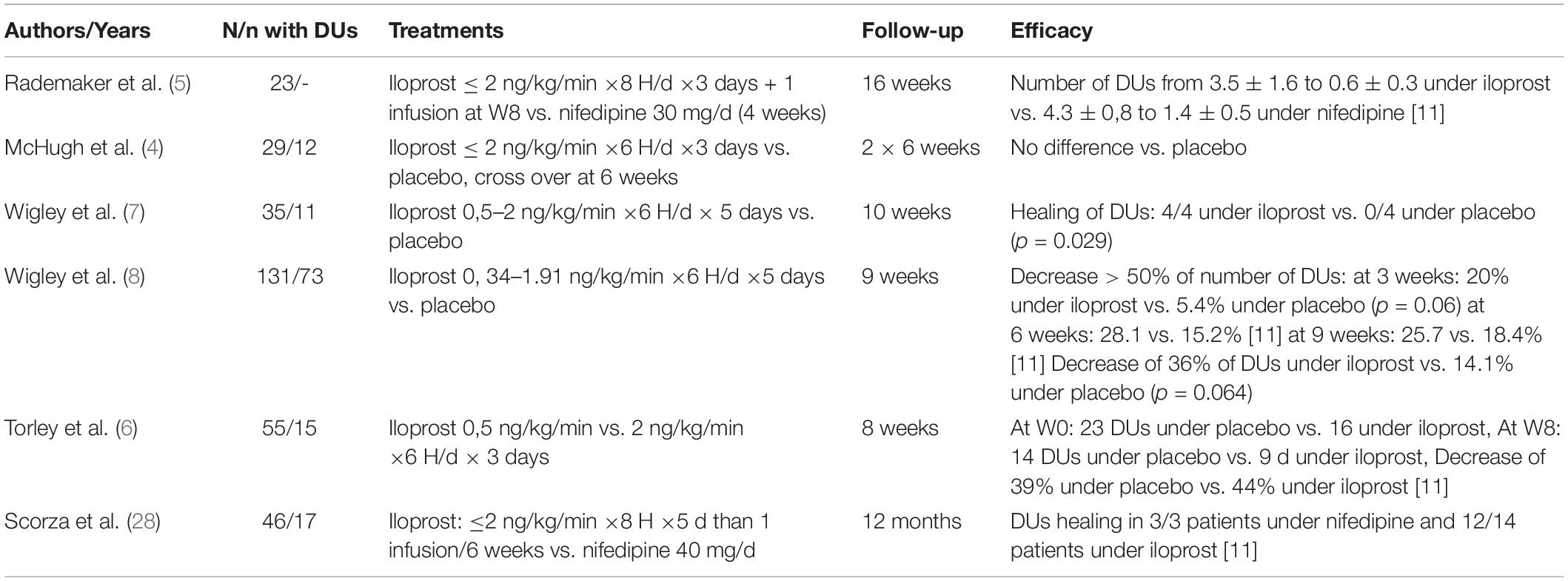
Table 3. Literature review of randomized trials using iloprost for DUs in systemic sclerosis.
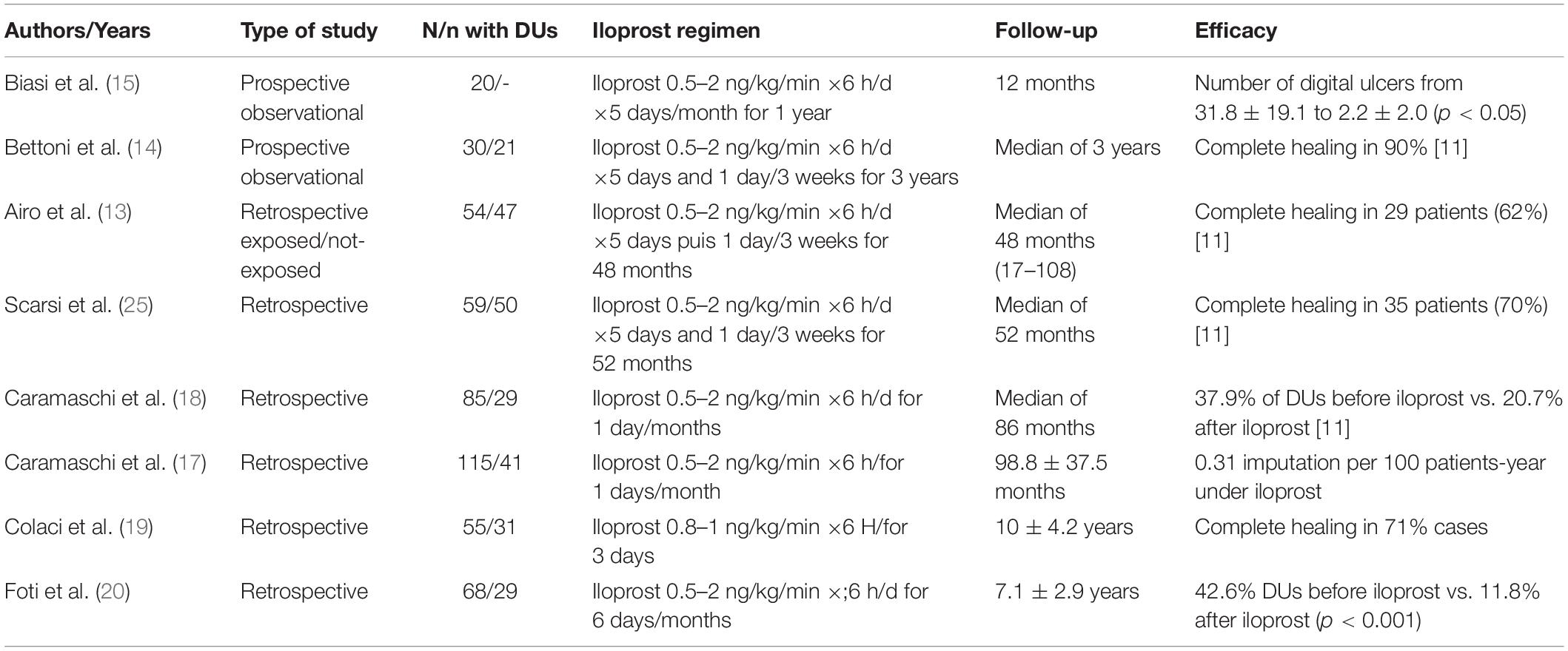
Table 4. Literature review of observational non-randomized trials using iloprost for DUs in systemic sclerosis.
Systemic sclerosis microvascular structural damage and dysfunction represent the initial morphological and functional markers of the disease. Some authors have reported that patients receiving iloprost had an improvement on Doppler and videocapillaroscopy characteristics, when compared with patients without iloprost (29). Unfortunately, these vascular effects were no longer seen at the next infusion (26). Several cappilarscopic and ultrasonographic tools could help to the clinical evaluation of DU healing, and Ultrasound classification of finger pulp blood flow was correlated with the risk of DU (30, 31). We were unable to obtain the results of the vascular examinations, which could have strengthened our data on the benefit of prolonged use of iloprost. However, the beneficial effects of prolonged infusion of iloprost is supported by the mechanisms of the drug. Prostanoids are potent vasodilators, and inhibit platelet aggregation and vascular smooth muscle cell proliferation. In SSc, DUs involve both microvessels and digital arteries (20). Moreover, an increased prevalence of macrovascular diseases proximal to the digital artery has been reported in SSc (27), in particular affecting the ulnar artery. After iloprost, a significant improvement in endothelial-dependent vasodilation was seen only in SSc patients with an “active” Nailfold videocapillaroscopy pattern. The iloprost effects vanished within 7 days after the last infusion (32). Therefore, our results are consistent with those of thromboangeitis obliterans, where a prolonged duration of infusion is required (10, 29). Patients under iloprost have Doppler and videocapillaroscpy improvement in comparison with those without iloprost, but these vascular effects were no longer observed at the following infusion (26).
The other major result is the benefit of concomitant vasoactive drugs. Two extensive, multicenter placebo-controlled studies have proved bosentan to be an effective treatment option in preventing new DUs and in the treatment of current DUs in relatively small series (22, 23). However, the beneficial effect of combining bosentan with iloprost has not yet been reported. Here, we found no improvement with this dual therapy, particularly among patients with the longer iloprost regimen, as they received more frequently an endothelin receptor antagonist. This result is consistent with the results of RAPIDS-2 (for the Randomized, double-blind, Placebo-controlled study with bosentan on the healing and prevention of Ischemic Digital ulcers in patients with systemic Sclerosis), where treatment with bosentan reduced the occurrence of new DU in patients with SSc, but had no effect on healing of DU compared to placebo (23). To date, it is unclear why a drug that presumably promotes vasodilation as an antagonist of ET-1 would not also promote ulcer healing. One hypothesis is that the expression of endothelin receptors on keratinocytes suggests that ET-1 could be a modulator of function and, therefore, receptor blockade might impair epithelialization despite beneficial effects on other aspects of healing. Likewise, PDE-5 inhibitors have also been studied for curing DU in SSc. In a French randomized study, even though the healing time was not improved under sildenafil, there was a significant decrease in the number of DUs in favor of sildenafil at the 8th and 12th week (33). To our knowledge, data is scarce on this aspect, and we have not found data suggesting that these various drug combinations could improve healing time in patients with SSc. However, the present study could not allow us to draw a definitive conclusion, due to the small number of patients treated with each drug and combination of drugs.
Prolonged duration of iloprost can be a source of morbidity and disability, due to increased frequency and duration of hospitalizations and venous access. In addition, no criteria has yet been determined to stop the treatment. It is questionable to prescribe a drug that can possibly be responsible for side effects, without clear guidelines based on robust studies. Another important problem relates to strategies for preventing the recurrence of DUs, and in particular the preventive use of endothelin receptor antagonists or PDE-5 inhibitors. Only a small proportion of our cohort was treated by endothelin receptor inhibitor, though this drug is known as an effective preventive drug for DU recurrence (22, 23), even though 90% of the infusions were performed for recurrent DUs. However, these data are similar to a recent analysis from the observational real-life DESScipher study, showing that the proportion of patients with a combination therapy is still low with 32.6% patients under 2 drugs and 11.5% under three or more therapies (16).
Several limitations should be addressed, in particular the retrospective nature of the study and the limited number of iloprost infusions. In addition, the classification criteria for defining healing are heterogeneous. Finally, the duration of iloprost infusion has been based on the physician’s experience and may therefore differ between two medical centers. Despite these limitations, a prolonged use of iloprost in patients with severe diffuse SSc with dominant microcirculatory involvement is coherent and seem to improve the healing rates.
To conclude, a prolonged administration of iloprost may improve the healing rate and the time to healing of DUs related to SSc. Prospective randomized studies are guaranteed to confirm these data and define the optimal duration of iloprost.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author Contributions
CJ, HL, OF, SR, YB, and AM: conception and design of the study and analyzing and interpretation of data. CJ and AM: acquisition of data. CJ, HL, ST, OF, SR, YB, and AM: drafting and final approval of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
AM was investigator of CELGENE, ROCHE, CHUGAI founded trials with APHP and Hôpital 15-20 promotion; AM received several fees for congress travels and experts’ use from LFB, SANOFI, SHIRE, and CELGENE.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Steen V, Denton CP, Pope JE, Matucci-Cerinic M. Digital ulcers: overt vascular disease in systemic sclerosis. Rheumatology (Oxford Engl). (2009) 48(Suppl. 3):iii19–24. doi: 10.1093/rheumatology/kep105
2. Sunderkötter C, Herrgott I, Brückner C, Moinzadeh P, Pfeiffer C, Gerss J, et al. Comparison of patients with and without digital ulcers in systemic sclerosis: detection of possible risk factors. Br J Dermatol. (2009) 160:835–43. doi: 10.1111/j.1365-2133.2008.09004.x
3. Elhai M, Meune C, Boubaya M, Avouac J, Hachulla E, Balbir-Gurman A, et al. Mapping and predicting mortality from systemic sclerosis. Ann Rheum Dis. (2017) 76:1897–905. doi: 10.1136/annrheumdis-2017-211448
4. McHugh NJ, Csuka M, Watson H, Belcher G, Amadi A, Ring EF, et al. Infusion of iloprost, a prostacyclin analogue, for treatment of Raynaud’s phenomenon in systemic sclerosis. Ann Rheum Dis. (1988) 47:43–7. doi: 10.1136/ard.47.1.43
5. Rademaker M, Cooke ED, Almond NE, Beacham JA, Smith RE, Mant TG, et al. Comparison of intravenous infusions of iloprost and oral nifedipine in treatment of Raynaud’s phenomenon in patients with systemic sclerosis: a double blind randomised study. BMJ (Clin Res ed). (1989) 298:561–4. doi: 10.1136/bmj.298.6673.561
6. Torley HI, Madhok R, Capell HA, Brouwer RM, Maddison PJ, Black CM, et al. A double blind, randomised, multicentre comparison of two doses of intravenous iloprost in the treatment of Raynaud’s phenomenon secondary to connective tissue diseases. Ann Rheum Dis. (1991) 50:800–4.
7. Wigley FM, Seibold JR, Wise RA, McCloskey DA, Dole WP. Intravenous iloprost treatment of Raynaud’s phenomenon and ischemic ulcers secondary to systemic sclerosis. J Rheum. (1992) 19:1407–14.
8. Wigley FM, Wise RA, Seibold JR, McCloskey DA, Kujala G, Medsger TA Jr., et al. Intravenous iloprost infusion in patients with Raynaud phenomenon secondary to systemic sclerosis. A multicenter, placebo-controlled, double-blind study. Ann Intern Med. (1994) 120:199–206. doi: 10.7326/0003-4819-120-3-199402010-00004
9. Tingey T, Shu J, Smuczek J, Pope J. Meta-analysis of healing and prevention of digital ulcers in systemic sclerosis. Arthritis Care Res. (2013) 65:1460–71. doi: 10.1002/acr.22018
10. Fiessinger JN, Schäfer M. Trial of iloprost versus aspirin treatment for critical limb ischaemia of thromboangiitis obliterans. The TAO Study. Lancet (Lond Engl). (1990) 335:555–7. doi: 10.1016/0140-6736(90)90346-7
11. van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A, et al. 2013 classification criteria for systemic sclerosis: an American college of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. (2013) 65:2737–47.
12. Baron M, Chung L, Gyger G, Hummers L, Khanna D, Mayes MD, et al. Consensus opinion of a North American working group regarding the classification of digital ulcers in systemic sclerosis. Clin Rheum. (2014) 33:207–14. doi: 10.1007/s10067-013-2460-7
13. Airò P, Rossi M, Scarsi M, Danieli E, Grottolo A, Zambruni A. Disease-modifying effects of long-term cyclic iloprost therapy in systemic sclerosis. A retrospective analysis and comparison with a control group. Clin Exp Rheumatol. (2007) 25:722–7.
14. Bettoni L, Geri A, Airò P, Danieli E, Cavazzana I, Antonioli C, et al. Systemic sclerosis therapy with iloprost: a prospective observational study of 30 patients treated for a median of 3 years. Clin Rheumatol. (2002) 21:244–50. doi: 10.1007/pl00011223
15. Biasi D, Carletto A, Caramaschi P, Zeminian S, Pacor ML, Corrocher R, et al. Iloprost as cyclic five-day infusions in the treatment of scleroderma. An open pilot study in 20 patients treated for one year. Revue Rhum (English ed). (1998) 65:745–50.
16. Blagojevic J, Abignano G, Avouac J, Cometi L, Frerix M, Bellando-Randone S, et al. Use of vasoactive/vasodilating drugs for systemic sclerosis (SSc)-related digital ulcers (DUs) in expert tertiary centres: results from the analysis of the observational real-life DeSScipher study. Clin Rheumatol. (2020) 39:27–36. doi: 10.1007/s10067-019-04564-8
17. Caramaschi P, Dalla Gassa A, Prati D, Barausse G, Tinazzi I, Ravagnani V, et al. Severe vascular complications in patients affected by systemic sclerosis cyclically treated with iloprost. Rheumatol Int. (2012) 32:1933–8. doi: 10.1007/s00296-011-1878-y
18. Caramaschi P, Martinelli N, Volpe A, Pieropan S, Tinazzi I, Patuzzo G, et al. A score of risk factors associated with ischemic digital ulcers in patients affected by systemic sclerosis treated with iloprost. Clin Rheumatol. (2009) 28:807–13. doi: 10.1007/s10067-009-1155-6
19. Colaci M, Lumetti F, Giuggioli D, Guiducci S, Bellando-Randone S, Fiori G, et al. Long-term treatment of scleroderma-related digital ulcers with iloprost: a cohort study. Clin Exp Rheumatol. (2017) 35(Suppl. 106):179–83.
20. Foti R, Visalli E, Amato G, Benenati A, Converso G, Farina A, et al. Long-term clinical stabilization of scleroderma patients treated with a chronic and intensive IV iloprost regimen. Rheumatol Int. (2017) 37:245–9. doi: 10.1007/s00296-016-3582-4
21. Ingegnoli F, Schioppo T, Allanore Y, Caporali R, Colaci M, Distler O, et al. Practical suggestions on intravenous iloprost in Raynaud’s phenomenon and digital ulcer secondary to systemic sclerosis: systematic literature review and expert consensus. Semin Arthritis Rheum. (2019) 48:686–93. doi: 10.1016/j.semarthrit.2018.03.019
22. Korn JH, Mayes M, Matucci Cerinic M, Rainisio M, Pope J, Hachulla E, et al. Digital ulcers in systemic sclerosis: prevention by treatment with bosentan, an oral endothelin receptor antagonist. Arthritis Rheum. (2004) 50:3985–93. doi: 10.1002/art.20676
23. Matucci-Cerinic M, Denton CP, Furst DE, Mayes MD, Hsu VM, Carpentier P, et al. Bosentan treatment of digital ulcers related to systemic sclerosis: results from the RAPIDS-2 randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. (2011) 70:32–8. doi: 10.1136/ard.2010.130658
24. Negrini S, Magnani O, Matucci-Cerinic M, Carignola R, Data V, Montabone E, et al. Iloprost use and medical management of systemic sclerosis-related vasculopathy in Italian tertiary referral centers: results from the PROSIT study. Clin Exp Med. (2019) 19:357–66. doi: 10.1007/s10238-019-00553-y
25. Scarsi M, Rossi M, Danieli E, Frigè A, Grottolo A, Zambruni A, et al. [Long-term effects of cyclic therapy with iloprost in systemic sclerosis]. Reumatismo. (2008) 60:114–9. doi: 10.4081/reumatismo.2008.114
26. Schioppo T, Orenti A, Boracchi P, De Lucia O, Murgo A, Ingegnoli F. Acute and chronic effects of two different intravenous iloprost regimens in systemic sclerosis: a pragmatic non-randomized trial. Rheumatology (Oxford Engl). (2018) 57:1408–16. doi: 10.1093/rheumatology/key113
27. Schioppo T, Orenti A, Boracchi P, De Lucia O, Murgo A, Ingegnoli F. Evidence of macro- and micro-angiopathy in scleroderma: An integrated approach combining 22-MHz power Doppler ultrasonography and video-capillaroscopy. Microvasc Res. (2019) 122:125–30. doi: 10.1016/j.mvr.2018.07.001
28. Scorza R, Caronni M, Mascagni B, Berruti V, Bazzi S, Micallef E, et al. Effects of long-term cyclic iloprost therapy in systemic sclerosis with Raynaud’s phenomenon. A randomized, controlled study. Clin Exp Rheumatol. (2001) 19:503–8.
29. Trombetta AC, Pizzorni C, Ruaro B, Paolino S, Sulli A, Smith V, et al. Effects of longterm treatment with bosentan and iloprost on nailfold absolute capillary number, fingertip blood perfusion, and clinical status in systemic sclerosis. J Rheumatol. (2016) 43:2033–41. doi: 10.3899/jrheum.160592
30. Lescoat A, Coiffier G, de Carlan M, Droitcourt C, Ballerie A, Cazalets C, et al. Combination of capillaroscopic and ultrasonographic evaluations in systemic sclerosis: results of a cross-sectional study. Arthritis Care Res. (2018) 70:938–43. doi: 10.1002/acr.23413
31. Lescoat A, Robin F, Belhomme N, Ballerie A, de Saint Riquier M, Sebillot M, et al. Ultrasound classification of finger pulp blood flow in patients with systemic sclerosis: a pilot study. Arthritis Care Res. (2021). doi: 10.1002/acr.24779 [Epub ahead of print].
32. Rotondo C, Nivuori M, Chialà A, Praino E, Matucci Cerinic M, Cutolo M, et al. Evidence for increase in finger blood flow, evaluated by laser doppler flowmetry, following iloprost infusion in patients with systemic sclerosis: a week-long observational longitudinal study. Scand J Rheumatol. (2018) 47:311–8. doi: 10.1080/03009742.2017.1397187
Keywords: systemic sclerosis, DUs, iloprost, outcome, digital ulcer
Citation: Jamart C, Levesque H, Thietart S, Fain O, Rivière S, Benhamou Y and Mekinian A (2022) Iloprost Duration for Digital Ulcers in Systemic Sclerosis: French Retrospective Study at Two Centers and Literature Review. Front. Med. 9:878970. doi: 10.3389/fmed.2022.878970
Received: 18 February 2022; Accepted: 21 April 2022;
Published: 06 July 2022.
Edited by:
Peter Korsten, University Medical Center Göttingen, GermanyReviewed by:
Cinzia Rotondo, University of Foggia, ItalyGianluca Bagnato, University of Messina, Italy
Jan-Gerd Rademacher, University Medical Center Göttingen, Germany
Copyright © 2022 Jamart, Levesque, Thietart, Fain, Rivière, Benhamou and Mekinian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Arsène Mekinian, YXJzZW5lLm1la2luaWFuQGFwaHAuZnI=
†These authors have contributed equally to this work