 Dan Lu
Dan Lu Jing-Hua Wang2
Jing-Hua Wang2 Chao Lu
Chao Lu Feng Ji
Feng Ji- 1Department of Endoscopy Center, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, China
- 2Department of Gastroenterology, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, China
- 3Department of Anesthesiology, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, China
- 4Meridian Medical Group, Indiana University Health Methodist Hospital, Indianapolis, IN, United States
Aim: The research aimed to study the effect of using WeChat (a mobile social media application) on pregastroscopy anxiety and the cooperation of patients with different coping styles.
Methods: In order to decrease patients' pregastroscopy anxiety and improve the tolerance of unsedated gastroscopy, WeChat, a widely used mobile social media application, was applied to provide information prior to their endoscopic procedure. Two hundred and thirty patients who underwent initial unsedated gastroscopy in a large teaching hospital in China were classified into two groups based on their coping style: information seekers or information avoiders, using the Information Subscale of the Krantz Health Opinion Survey (KHOS-I). Each of the two groups was prospectively randomly assigned to either receiving the brochure information or conjunctive interactive WeChat-delivered information of gastroscopy. To measure the level of state anxiety, the State Anxiety Scale of Spielberg's State-Trait Anxiety Inventory questionnaire was used. State anxiety, blood pressure and heart rate were measured at enrollment, upon arrival, and before gastroscopy.
Results: Information seekers and avoiders who received information from the brochure and the WeChat platform experienced significantly less state anxiety upon arrival and before gastroscopy. Furthermore, information seekers who received information from the conjunctive WeChat platform had lower frequency of retching, lower scores of nausea and bloating, and better tolerance. Information avoiders who received information from the conjunctive WeChat platform had lower frequency of retching, lower scores of discomfort while swallowing the scope and nausea, and better tolerance. However, we found the percentage of information seekers who preferred no WeChat-delivered pregastroscopy information is greater than WeChat-delivered information at the initial questionnaire. No significant difference was found in blood pressure or heart rate upon arrival and before gastroscopy.
Conclusions: Although people preferred no WeChat-delivered pregastroscopy information, the provision of gastroscopy information through a mobile social media application, such as WeChat, could significantly reduce patients' pregastroscopy anxiety, lower the frequency of retching, reduce the scores of nausea and bloating, and improve tolerance for information seekers. In addition, it could lower the frequency of retching, reduce the scores of discomfort while swallowing the scope and its concurrent nausea, and improve tolerance for information avoiders.
Introduction
Gastric cancer has become the second leading cause of death worldwide. Furthermore, incidence rates are highest in Eastern and Central Asia and confer a higher mortality rate there than in other nations (1). One well-documented method for gastric cancer prevention is via endoscopic screening in the asymptomatic population (2). Despite this globally well-known procedure, patients quite often perceive this procedure as uncomfortable and/or possibly embarrassing and may have concerns with potential exam results. These feelings about a commonplace procedure are generated from limited information, distress caused by perceived fear of discomfort, and an unfamiliarity with the process (3). Such preoccupations produce burdensome anxiety (4). As the need for these procedures increases, the process is dictated by direct referral and so the chance to meet the endoscopist in advance of the procedure is often bypassed, and also the ability of physicians to detect and gauge patient anxiety has proven less than adequate (5, 6).
Furthermore, procedural anxiety could affect patients' satisfaction and impede patient compliance with this routine procedure, and make it more difficult for them to tolerate gastroscopy (7, 8). There are instances whereby the stomach cannot be thoroughly examined which can be attributed to poor patient cooperation. In addition, the lack of patient cooperation amplifies the possibility of endoscopic complications and the miss rate of significant gastric lesions (9).
Recently, alternative methods, including tools like booklets, cartoons, and short message services (SMS) (10–12), have been used to relieve patients' stress and improve patient cooperation (13). Even more recently, smart phone-based strategies have been developed to help patients get prepared (14–21).
One critical method to consider when dealing with patients is their coping styles. In treatment, there may be information seekers, those who like to gather as much information as possible about the illness and/or procedure to make it more predictable and controllable, or they may be information avoiders, those who like to avoid the stressful situation and distract themselves from any threat-relevant information, siding toward unpredictability. Taking patients' coping styles into consideration could reduce procedural anxiety more effectively (22, 23). This is even as important as the content of the illness itself.
Liu, et al. reported that the provision of sensory information could reduce patients' pregastroscopy anxiety significantly, regardless of patients' information coping style (24). Morgan, et al. found information congruent with coping style reduced anxiety and observed behavioral indices of colonoscopy pain (25). In a study by Yang, et al., it was demonstrated that pregastroscopy anxiety was an independent predictor of severe discomfort and poor tolerance in patients undergoing unsedated gastroscopy (26). Kang, et al. claimed instruction via a mobile social media application, in conjunction with standard instruction, improves the adequacy of bowel preparation for colonoscopy (16). However, to date, few studies have been conducted to identify the effect of interactive information delivery via mobile social media application on the pregastroscopy anxiety of different coping styles, patient cooperation and tolerance during gastroscopy.
WeChat is the most widely used multipurpose social media platform in China, which is integrated with messaging, voice and video calls, and other services. The number of daily active WeChat users is estimated to be around 1 billion and the popularity of WeChat stems from its instant messaging and interaction function (27). WeChat could also provide a platform for medical professionals to more effectively clarify and reassure gastroscopy information. Through WeChat, patients can raise their concerns in complete privacy.
In the study we performed a prospective, randomized, controlled trial to compare the effect of pregastroscopy anxiety, and patient cooperation of different coping styles receiving gastroscopy informational brochure with interactive WeChat-delivered information vs. the informational brochure only. We tested the hypothesis that information delivered by the WeChat reduces pregastroscopy anxiety, improves patient cooperation, and tolerance for information seekers. And we also tested the hypothesis that the percentage of information seekers who preferred WeChat-delivered pregastroscopy information is greater than no WeChat-delivered information.
Materials and Methods
Study Design
This prospective, single-blinded, randomized, controlled study was conducted in the Endoscopy Center in a large teaching hospital in southeast China from 28 June to 8 August 2020. The institutional review board approved the study protocol and informed consent form (Number of Approval: IIT20200203A-R1). This study has been registered at www.Chictr.org.cn (ChiCTR2000034213).
All the patients received pregastroscopy information in the form of an official brochure when scheduling the gastroscopy. The brochure was handed out by two designated nurses who were not involved in gastroscopy and blinded to the randomization. The informational brochure was written in simple words and illustrated by animated pictures.
The patients were classified into two groups based on coping style: information seekers or information avoiders using the Information Subscale of the Krantz Health Opinion Survey (KHOS-I) (24, 28). Each group was randomly assigned by computer-generated random numbers to receive informational brochure only (control group) or both informational brochure and interactive information delivered by the mobile application, WeChat (WeChat group).
Both information seekers and information avoiders allocated to the WeChat portion of the study were invited to get access to the WeChat (Hospital official account: Endoscopy Center) on the day of the gastroscopy scheduling by two trained nurses who were not involved in data collection. In addition to receiving the brochure, they also received the same information delivered by WeChat (Hospital official account: Endoscopy Center). Possible interaction was the only difference between the control and WeChat group of both the information seekers and avoiders. Otherwise, all the information across all four groups was the same.
One nurse practitioner logged in to the WeChat platform using the official account between 4 and 6 p.m. daily to explain the brochure information which some patients could not fully understand by themselves. The nurse practitioner was trained to use therapeutic communication skills to address patients' concerns and give consistent answers to the same question.
All patients and their families were instructed not to disclose that they had access to the WeChat-delivered information, to endoscopists, medical staff, or other patients. State anxiety was assessed by the State Anxiety Scale of Spielberg's State Anxiety Inventory (29). Blood pressure, and pulse were measured at enrollment, upon arrival, and before gastroscopy by a designated nurse that was not involved in the procedure of gastroscopy and blinded to the randomization.
The gastroscopy was performed by 2 professional endoscopists with a minimum experience of 5,000 gastroscopies. The gastroscope (GIF-HQ290; Olympus), Radial Jaw (Boston Scientific), and mouthpiece (MB-142; Olympus) were used for each procedure and a topical anesthetic was applied to anesthetize the throat to suppress the gag reflex. The setup of the endoscopy room is unified.
Patient cooperation, patient discomfort, and tolerance were recorded by trained nurses. Belching, retching, and coughing were the main manifestations of poor cooperation (9). And the visual analog scale (VAS) was used to measure patients' discomfort during the procedure (30–33), including the scope passing through the throat, nausea, abdominal pain, and bloating. Patients were asked to rate the severity of their symptoms from “0–10,” with “0” being “I felt absolutely comfortable during the procedure” and “10” being “I was suffering to death during the procedure.” And patient tolerance was recorded by the answer to the question of the acceptability of unsedated gastroscopy after the procedure (Easy, A little difficult, Very difficult, and Cannot endure). The endoscopists and trained nurses were blinded to the participants.
Study Participants
Participants were from 18–70 years of age and underwent their initial gastroscopies in regular health screening, without any former experience of colonoscopy or bronchoscopy. Patients were considered to meet the inclusion criteria in the study if: They were mentally alert and able to communicate freely, underwent initial, unsedated gastroscopy as outpatients, and had access to WeChat themselves or through close family members. Patients were excluded if they suffered from severe cardiopulmonary disease, underwent emergency gastroscopy, had impaired consciousness or impaired hearing, were mentally distressed or underwent other invasive procedures on the same days, such as colonoscopy contrast enhanced CT, and an ultrasound-guided fine needle aspiration, etc. No sample sizes were performed a priori, as it is difficult to find other studies presenting data which could be used to estimate variance and effect size.
Assessment Methods
Participants' personal characteristics were collected by a questionnaire including their gender, age, education level, employment status, income level, and family gastric and/or esophageal cancer history, their preferences of receiving information via WeChat or the brochure, their knowledge about gastroscopy, and days of waiting for gastroscopy upon enrollment.
The KHOS-I subscale was used to determine patients' coping style by answering “Yes/No” questions relating to their preference for information, their desire to be involved in medical decision-making and their own wish to raise questions about the procedure (34).
Furthermore, subjects completed the Spielberger State Anxiety Inventory, which measures degrees of anxiety (e.g., feelings of tension, apprehension, and nervousness.). It consists of 20 statements and each statement has “1–4” points, with “4” indicating greatest anxiety (35).
All the information distributed via the brochure and through the WeChat (Hospital official account: Endoscopy Center), was collected based on information guides (Endoscopy (Upper GI) from (36)) aga gi patient center and Understanding Upper Endoscopy from ASGE, and from the suggestions of endoscopists, nurses and patients. It consists of five parts, which are detailed in Supplementary Material 1.
Statistical Analysis
The independent samples t-test for age, days of waiting for gastroscopy, and Chi-square test for gender, education level, employment status, income level, and family history of gastric and/or esophageal cancer, preferences of receiving information via WeChat or not, preferences of receiving information via the brochure or not, knowledge about gastroscopy, were used to determine whether there were baseline differences. P < 0.05 was used as the significance level in this study.
An independent sample t-test for state anxiety score, blood pressure, and pulse, frequency of coughing, belching, retching, and scores of discomfort while swallowing the scope, nausea, abdominal pain, and bloating, and Chi-square test for tolerance, was used to find any significant differences between the control group and the WeChat group in information seekers and information avoiders. Multiple regression analysis was used to determine the factors predicting state anxiety. The data were analyzed by using Statistical Package for Social Sciences (SPSS) version 25.
Results
Patient Baseline Characteristics
Two hundred and sixty-two patients were screened in total. Twenty-seven patients (one patient with severe cardiopulmonary disease, 10 patients who underwent emergency gastroscopy, four patients with psychiatric mental health problems, 10 patients who made the appointment of colonoscopy and two patients who made the appointment of contrast enhanced CT on the same day with gastroscopy), who did not meet the criteria were excluded. Two patients of information seekers from the WeChat group who were hospitalized before gastroscopy were excluded. This study also excluded three cases of treatment failure: Two patients of information avoiders from the WeChat group and one patient of information avoiders from the control group who could not tolerate the procedure and changed to the sedated procedure. A total of 230 participants (76 Seekers and 154 Avoiders) completed all the questionnaires (Response Rate = 97.9%) (Figure 1).
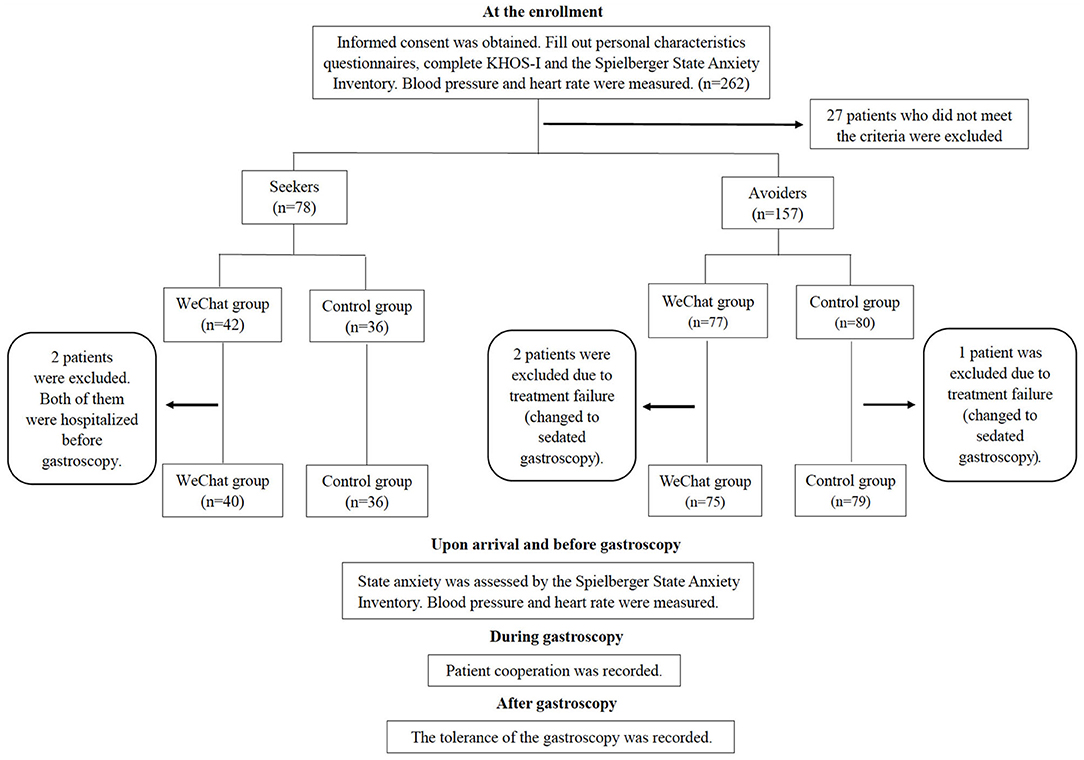
Figure 1. The flowchart of procedure. KHOS-I indicates Krantz Health Opinion Survey.
As shown in Table 1, there were no significant differences among the measured patient baseline parameters. However, Table 1 shows that greater percentage of participants in all groups preferred pregastroscopy information “brochure” over “no brochure information,” and greater percentage of participants preferred “no WeChat pregastroscopy information” over “WeChat pregastroscopy information.”
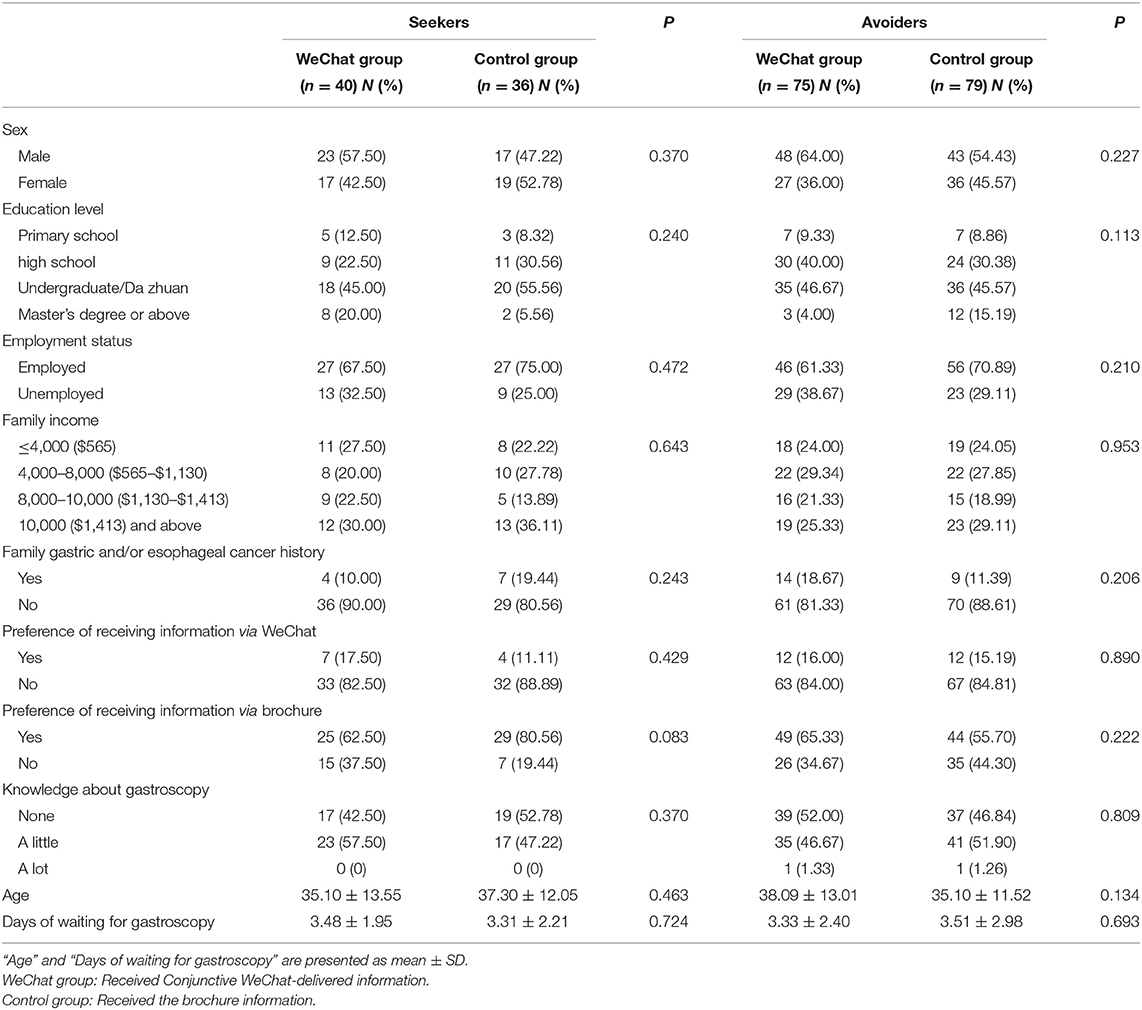
Table 1. Baseline characteristics of patients undergoing gastroscopy included in the study.
As shown in Table 2, no significant difference was found in anxiety level, blood pressure (BP), heart rate (HR), upon enrollment at baseline for information seekers and information avoiders, between patients who received gastroscopy information via the brochure and those who received information via brochure as well as the WeChat platform. There was no significant difference in endoscopist distribution between groups (Supplementary Tables S1, S2).
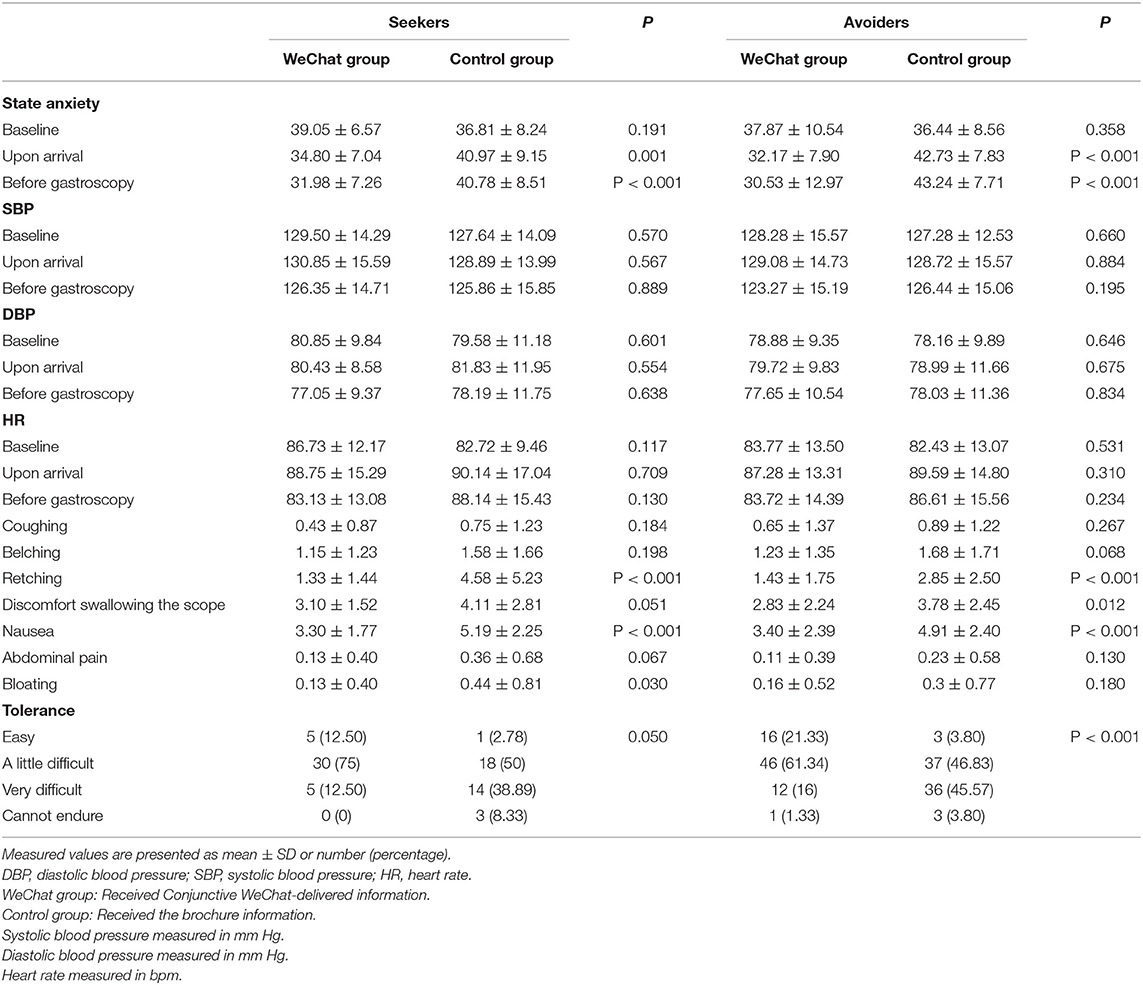
Table 2. Anxiety level at baseline, upon arrival and before gastroscopy, and patient cooperation and tolerance by information seekers and avoiders in each of the two information groups.
After receiving the intervention, the state anxiety score upon arrival (P = 0.001) and before gastroscopy (P < 0.001) from the WeChat group of information seekers, and the state anxiety score upon arrival (P < 0.001) and before gastroscopy (P < 0.001) from the WeChat group of information avoiders, all significantly declined.
In our study, we have two information avoiders from the WeChat group and one information avoider from the control group who could not tolerate the procedure and changed to the sedated procedure. The anxiety levels of the two information avoiders from the WeChat group (35 at baseline, 30 upon arrival, and 39 before gastroscopy; 31 at baseline, 28 upon arrival, and 35 before gastroscopy) showed no significant difference from their group anxiety levels. The anxiety level of the information avoider from the control group (34 at baseline, 40 upon arrival, and 42 before gastroscopy) shows no significant difference from their group anxiety levels either.
No significant difference was found in BP and HR upon arrival and before gastroscopy for information seekers or information avoiders, between those who received gastroscopy information via the brochure and those who received information via brochure, as well as the WeChat platform.
Compared to information seekers who received information from the brochure only, those who received information from the WeChat and the brochure, had lower frequency of retching (P < 0.001), lower scores of nausea (P < 0.001), and bloating (P < 0.05), and better tolerance (P < 0.001).
In contrast to information avoiders who received information from brochure only, those who received information from WeChat and the brochure, had lower frequency of retching (P < 0.001), lower scores of Discomfort while swallowing the scope (P < 0.05), and nausea (P < 0.001), and better tolerance (P < 0.001).
Women have been found to have higher anxiety score than men at the baseline when scheduling the procedure (P < 0.05), but no significant differences in anxiety score were found upon arrival and before the gastroscopy between women and men (P > 0.05) (Table 3).
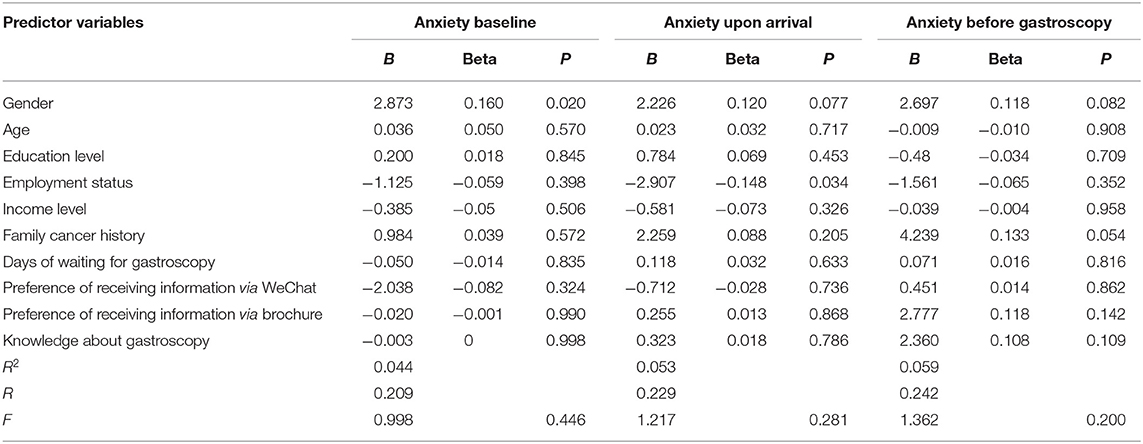
Table 3. Predictors of anxiety level of patients undergoing gastroscopy at three different stages.
Discussion
This study found that the anxiety state score improved for information seekers and information avoiders who received information from the brochure as well as the WeChat platform compared to the informational brochure only. This finding was found both upon arrival and before the gastroscopy procedure.
Information seekers who received information from the brochure and the WeChat platform had less frequency of retching, lower scores of nausea, bloating, and better tolerance than information seekers receiving information only from the brochure.
Information avoiders who received information from the brochure and the WeChat platform had less frequency of retching, lower scores of discomfort while swallowing the scope, and nausea, and better tolerance, compared to information avoiders receiving information from the brochure only.
These results support the conclusion that the delivery of pregastroscopy information though mobile social media app could significantly reduce patients' pregastroscopy anxiety no matter the patients' information coping style. Furthermore, it could improve patient cooperation and tolerance.
According to previous studies, Vukmir, et al. reported that a computer printout, like a brochure, does not help most patient comply with the physician's instructions (37). Abbott reported that poor understanding of the procedure may result in lack of patient cooperation (31).
Online interactive guidance conveys a more personalized set of instructions, making them more relevant to the patient (38). Professional communication provided the patients with reassurance and clarity, and helped remove the uncertainty for those who were concerned about their lack of understanding of the procedure.
These conclusions were consistent with some previous studies. Sewitch, et al. reported that a user-centered smart phone application has the benefit of broadening the patient community, educating patients with comprehensive information, and improving patient cooperation (39). Kang, et al. demonstrates that information delivered by the smart phone application WeChat could improve bowel preparation of colonoscopy and patient compliance (16). Vliet, et al. concluded that medical personnel provides invaluable guidance through coaching when preparing patients for gastrointestinal endoscopy (40). Online coaches through a smart phone application, such as WeChat, help fill the gap when patients leave the hospital. Smart phones help patients cope better (14–21). Liu, et al. reported that the state anxiety score significantly declined after the intervention of sensory information for information seekers and information avoiders (24).
However, some studies showed inconsistent outcomes. Morgan, et al. discovered in their anxiety and pain study for patients undergoing initial colonoscopy that patients who received information congruent with coping style experienced less state anxiety, whereas those who received information not congruent with their coping style maintained the same anxiety level (25). There are essential differences between colonoscopy and gastroscopy, even though they are both gastrointestinal endoscopy procedures. Colonoscopy is generally regarded to be a painful procedure (41), and a considerable proportion of patients experience pain (42). However, only a few patients complain of pain and bloating in gastroscopy. The potential for bloating and especially for pain may frighten information avoiders.
In this study, we found that the percentage of people who preferred brochure pregastroscopy information is greater than no brochure information in all groups, and the percentage of people who preferred no WeChat-delivered pregastroscopy information is greater than WeChat-delivered information in all groups, which is inconsistent with our hypothesis that the percentage of information seekers who preferred WeChat-delivered pregastroscopy information is greater than no WeChat-delivered information. The cause could be attributed to unfamiliarity with WeChat as a mode of education. There is no up to date interactive information regarding pregastrscopy patient education delivered via mobile application.
Contrary to our assumptions, information-avoiders also had reduced anxiety level for receiving information through WeChat, which is in contrast to previous studies and original theory (22, 23, 25, 43), in which avoiders were associated with lower demand for information. However, Sewitch, et al. reported that the ability to tailor instructions made the smartphone application preferable to other delivery modes (39). An explanation might be that avoiders did not reject formation input through a non-face to face manner. As such, a social media application that comes from a trusted source, is capable of sending timely and tailored messages, provides reassurance, has clear instructions, and is easy to use (39), may benefit information-avoider patients in the future. Furthermore, we provided information via WeChat with the intent of soothing and calming, believing it constitutes a less threatening means of communication. Without having to look someone in the eye, avoiders may feel more reassured and relaxed using it.
In accordance with previous investigations, women have been found to have higher anxiety score than men when scheduling the procedure. In the investigation of Ersöz, et al., women scored higher STAI state anxiety scores than men in gastroscopy and colonoscopy (44). Luck, et al. claimed higher anxiety levels in female patients before colonoscopy (45). Liu, et al. reported that gender was a predictor of state anxiety prior to gastroscopy (24). Shafer, et al. reported variables associated with higher anxiety about bowel preparation were female gender (46). Muzzarelli, et al. revealed that women had higher percentile of the state anxiety raw score measured prior to a scheduled endoscopy (47).
Therefore, the difference in which men and women handle information is an essential consideration for healthcare providers and should focus on future studies into the use and effectiveness of social media applications in reducing anxiety in medical procedures such as gastroscopy.
The study's major strength is the prospective randomized single-blind design and use of validated scales to assess the effect of interactive instructions via WeChat on patient anxiety toward unsedated gastroscopy. However, our current study has a few limitations. Firstly, the study was performed in a single center and we could focus on a multicenter study in the future to test the outcome. Furthermore, the sedated patients were excluded, which may introduce bias in the state anxiety outcome. Moreover, VAS was applied to measure the patient's discomfort, but one single scale may not be enough. As a result, multi-validated scales should be used to measure patient discomfort in the future. A final limitation is that the study's results may not be widely applicable in countries where unseated gastroscopy is not the norm.
In conclusion, although people prefer to receive information via brochure, the provision of the brochure with WeChat-based disseminated information reduced patients' pregastroscopy anxiety no matter their information coping styles. An acceptable and wide-reaching smartphone application may decrease pregastroscopy anxiety, improve patient cooperation, and tolerance.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics Statement
The studies involving human participants were reviewed and approved by the Clinical Research Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University (Approval Number: IIT20200203A-R1). Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable data included in this article.
Author Contributions
DL, QG, and FJ conceived of the study. DL, J-HW, and CL collected and analyzed data. DL, Z-LL, and AJ drafted and critically revised the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors thank all participants for their valuable contributions that made the study possible and we want to thank the medical staff in the endoscopy center of the participating hospital for their support and understanding. We are also grateful to Björn Berglund for his valuable advice on the project design and manuscript writing. We also thank Halvard Midelfort for his devotion for language editing, and Prof. Krantz, for his permission to use Information Subscale of the Krantz Health Opinion Survey (KHOS-I).
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.855892/full#supplementary-material
References
1. Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. (2015) 136:E359–86. doi: 10.1002/ijc.29210
2. Dan YY, So JB, Yeoh KG. Endoscopic screening for gastric cancer. Clin Gastroenterol Hepatol. (2006) 4:709–16. doi: 10.1016/j.cgh.2006.03.025
3. Clements H, Melby V. An investigation into the information obtained by patients undergoing gastroscopy investigations. J Clin Nurs. (1998) 7:333–42. doi: 10.1046/j.1365-2702.1998.00161.x
4. Jones MP, Ebert CC, Sloan T, Spanier J, Bansal A, Howden CW, et al. Patient anxiety and elective gastrointestinal endoscopy. J Clin Gastroenterol. (2004) 38:35–40. doi: 10.1097/00004836-200401000-00009
5. Maguire GP, Julier DL, Hawton KE, Bancroft JH. Psychiatric morbidity and referral on two general medical wards. Br Med J. (1974) 1:268–70. doi: 10.1136/bmj.1.5902.268
6. Brody DS. Physician recognition of behavioral, psychological, and social aspects of medical care. Arch Intern Med. (1980) 140:1286–9. doi: 10.1001/archinte.1980.00330210034019
7. Nasiri J, Khatib N, Kheiri S, Najafi M. The influence of escort during upper endoscopy and colonoscopy on patient satisfaction and anxiety. J Family Med Prim Care. (2016) 5:134–8. doi: 10.4103/2249-4863.184638
8. Campo R, Brullet E, Montserrat A, Calvet X, Moix J, Rué M, et al. Identification of factors that influence tolerance of upper gastrointestinal endoscopy. Eur J Gastroenterol Hepatol. (1999) 11:201–4. doi: 10.1097/00042737-199902000-00023
9. Lee SP, Sung IK, Kim JH, Lee SY, Park HS, Shim CS. Factors impacting patient cooperation during elective gastroscopy. Korean J Intern Med. (2017) 32:819–26. doi: 10.3904/kjim.2015.393
10. Park J, Kim TO, Lee NY, Kim H, Seo EH, Heo NY, et al. The effectiveness of short message service to assure the preparation-to-colonoscopy interval before bowel preparation for colonoscopy. Gastroenterol Res Pract. (2015) 2015:628049. doi: 10.1155/2015/628049
11. Walter BM, Klare P, Neu B, Schmid RM, von Delius S. Development and testing of an automated 4-day text messaging guidance as an aid for improving colonoscopy preparation. JMIR Mhealth Uhealth. (2016) 4:e75. doi: 10.2196/mhealth.5289
12. Liu Z, Zhang MM, Li YY, Li LX, Li YQ. Enhanced education for bowel preparation before colonoscopy: a state-of-the-art review. J Dig Dis. (2017) 18:84–91. doi: 10.1111/1751-2980.12446
13. Deng X, Wang Y, Zhu T, Zhang W, Yin Y, Ye L. Short message service (SMS) can enhance compliance and reduce cancellations in a sedation gastrointestinal endoscopy center: a prospective randomized controlled trial. J Med Syst. (2015) 39:169. doi: 10.1007/s10916-014-0169-z
14. Lee YJ, Kim ES, Choi JH, Lee KI, Park KS, Cho KB, et al. Impact of reinforced education by telephone and short message service on the quality of bowel preparation: a randomized controlled study. Endoscopy. (2015) 47:1018–27. doi: 10.1055/s-0034-1392406
15. Lorenzo-Zúñiga V, Moreno de Vega V, Marín I, Barberá M, Boix J. Improving the quality of colonoscopy bowel preparation using a smart phone application: a randomized trial. Dig Endosc. (2015) 27:590–5. doi: 10.1111/den.12467
16. Kang X, Zhao L, Leung F, Luo H, Wang L, Wu J, et al. Delivery of instructions via mobile social media app increases quality of bowel preparation. Clin Gastroenterol Hepatol. (2016) 14:429–35.e3. doi: 10.1016/j.cgh.2015.09.038
17. Jung JW, Park J, Jeon GJ, Moon YS, Yang SY, Kim TO, et al. The effectiveness of personalized bowel preparation using a smartphone camera application: a randomized pilot study. Gastroenterol Res Pract. (2017) 2017:4898914. doi: 10.1155/2017/4898914
18. Sharara AI, Chalhoub JM, Beydoun M, Shayto RH, Chehab H, Harb AH, et al. A customized mobile application in colonoscopy preparation: a randomized controlled trial. Clin Transl Gastroenterol. (2017) 8:e211. doi: 10.1038/ctg.2016.65
19. Walter B, Schmid R, von Delius S. A smartphone app for improvement of Colonoscopy Preparation (ColoprAPP): development and feasibility study. JMIR Mhealth Uhealth. (2017) 5:e138. doi: 10.2196/mhealth.7703
20. Cho J, Lee S, Shin JA, Kim JH, Lee HS. The impact of patient education with a smartphone application on the quality of bowel preparation for screening colonoscopy. Clin Endosc. (2017) 50:479–85. doi: 10.5946/ce.2017.025
21. Back SY, Kim HG, Ahn EM, Park S, Jeon SR, Im HH, et al. Impact of patient audiovisual re-education via a smartphone on the quality of bowel preparation before colonoscopy: a single-blinded randomized study. Gastrointest Endosc. (2018) 87:789–99.e4. doi: 10.1016/j.gie.2017.09.007
22. Auerbach SM, Martelli MF, Mercuri LG. Anxiety, information, interpersonal impacts, and adjustment to a stressful health care situation. J Pers Soc Psychol. (1983) 44:1284–96. doi: 10.1037/0022-3514.44.6.1284
23. Miller SM, Mangan CE. Interacting effects of information and coping style in adapting to gynecologic stress: should the doctor tell all? J Pers Soc Psychol. (1983) 45:223–36. doi: 10.1037/0022-3514.45.1.223
24. Liu YY, Liu YQ, Petrini MA. Effect of information of patients' coping style on pregastroscopy anxiety. Gastroenterol Nurs. (2018) 41:47–58. doi: 10.1097/SGA.0000000000000302
25. Morgan J, Roufeil L, Kaushik S, Bassett M. Influence of coping style and precolonoscopy information on pain and anxiety of colonoscopy. Gastrointest Endosc. (1998) 48:119–27. doi: 10.1016/S0016-5107(98)70152-X
26. Yang M, Lu LL, Zhao M, Liu J, Li QL, Li Q, et al. Associations of anxiety with discomfort and tolerance in Chinese patients undergoing esophagogastroduodenoscopy. PLoS ONE. (2019) 14:e0212180. doi: 10.1371/journal.pone.0212180
28. Zhang Y. The effects of preference for information on consumers' online health information search behavior. J Med Internet Res. (2013) 15:e234. doi: 10.2196/jmir.2783
29. Gong M, Dong H, Tang Y, Huang W, Lu F. Effects of aromatherapy on anxiety: a meta-analysis of randomized controlled trials. J Affect Disord. (2020) 274:1028–40. doi: 10.1016/j.jad.2020.05.118
30. Parvini P, Saminsky M, Stanner J, Klum M, Nickles K, Eickholz P. Discomfort/pain due to periodontal and peri-implant probing with/without platform switching. Clin Oral Implants Res. (2019) 30:997–1004. doi: 10.1111/clr.13513
31. Wang D, Tang L, Wu H, Gu D. Analysis of the effect of overusing thumbs on smartphone games. J Int Med Res. (2019) 47:6244–53. doi: 10.1177/0300060519881016
32. Attali V, Collet JM, Jacq O, Souchet S, Arnulf I, Rivals I, et al. Mandibular advancement reveals long-term suppression of breathing discomfort in patients with obstructive sleep apnea syndrome. Respir Physiol Neurobiol. (2019) 263:47–54. doi: 10.1016/j.resp.2019.03.005
33. Baser E, Togrul C, Ozgu E, Esercan A, Caglar M, Gungor T. Effect of pre-procedural state-trait anxiety on pain perception and discomfort in women undergoing colposcopy for cervical cytological abnormalities. Asian Pac J Cancer Prev. (2013) 14:4053–6. doi: 10.7314/APJCP.2013.14.7.4053
34. Krantz DS, Baum A, Wideman M. Assessment of Preferences for self-treatment and information in health care. J Pers Soc Psychol. (1980) 39:977–90. doi: 10.1037/0022-3514.39.5.977
35. American Gastroenterological Association. Endoscopy (upper GI) (2021). Available online at: https://patient.gastro.org/upper-gi-endoscopy/ (accessed January 15, 2022).
36. American Society for Gastrointestinal Endoscopy. Understanding Upper Endoscopy. (2020). Available online at: https://www.asge.org/home/for-patients/patient-information/understanding-upper-endoscopy (accessed March 15, 2021).
37. Vukmir RB, Kremen R, Ellis GL, DeHart DA, Plewa MC, Menegazzi J. Compliance with emergency department referral: the effect of computerized discharge instructions. Ann Emerg Med. (1993) 22:819–23. doi: 10.1016/S0196-0644(05)80798-X
38. Delp C, Jones J. Communicating information to patients: the use of cartoon illustrations to improve comprehension of instructions. Acad Emerg Med. (1996) 3:264–70. doi: 10.1111/j.1553-2712.1996.tb03431.x
39. Sewitch MJ, Fallone CA, Ghali P, Lee GE. What patients want in a smartphone app that supports colonoscopy preparation: qualitative study to inform a user-centered smartphone app. JMIR Mhealth Uhealth. (2019) 7:e12242. doi: 10.2196/12242
40. van Vliet MJ, Grypdonck M, van Zuuren FJ, Winnubst J, Kruitwagen C. Preparing patients for gastrointestinal endoscopy: the influence of information in medical situations. Patient Educ Couns. (2004) 52:23–30. doi: 10.1016/S0738-3991(02)00245-8
41. Allen P, Shaw E, Jong A, Behrens H, Skinner I. Severity and duration of pain after colonoscopy and gastroscopy: a cohort study. J Clin Nurs. (2015) 24:1895–903. doi: 10.1111/jocn.12817
42. Holme O, Bretthauer M, de Lange T, Seip B, Huppertz-Hauss G, Høie O, et al. Risk stratification to predict pain during unsedated colonoscopy: results of a multicenter cohort study. Endoscopy. (2013) 45:691–6. doi: 10.1055/s-0033-1344239
43. Kola S, Walsh JC, Hughes BM, Howard S. Matching intra-procedural information with coping style reduces psychophysiological arousal in women undergoing colposcopy. J Behav Med. (2013) 36:401–12. doi: 10.1007/s10865-012-9435-z
44. Ersöz F, Toros AB, Aydogan G, Bektaş H, Ozcan O, Arikan S. Assessment of anxiety levels in patients during elective upper gastrointestinal endoscopy and colonoscopy. Turk J Gastroenterol. (2010) 21:29–33. doi: 10.4318/tjg.2010.0044
45. Luck A, Pearson S, Maddern G, Hewett P. Effects of video information on precolonoscopy anxiety and knowledge: a randomised trial. Lancet. (1999) 354:2032–5. doi: 10.1016/S0140-6736(98)10495-6
46. Shafer LA, Walker JR, Waldman C, Yang C, Michaud V, Bernstein CN, et al. Factors associated with anxiety about colonoscopy: the preparation, the procedure, and the anticipated findings. Dig Dis Sci. (2018) 63:610–8. doi: 10.1007/s10620-018-4912-z
Keywords: gastroscopy, anxiety, social media, mobile application, patient cooperation, tolerance
Citation: Lu D, Wang J-H, Lu C, Liu Z-L, Jain A, Ji F and Gu Q (2022) Alleviating Pregastroscopy Anxiety Using Mobile Social Media Application. Front. Med. 9:855892. doi: 10.3389/fmed.2022.855892
Received: 16 January 2022; Accepted: 12 May 2022;
Published: 22 June 2022.
Edited by:
Tony Tham, Ulster Hospital, United KingdomReviewed by:
George Ou, University of British Columbia, CanadaXiao Jing Wang, Mayo Clinic, United States
Copyright © 2022 Lu, Wang, Lu, Liu, Jain, Ji and Gu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Feng Ji, amlmZW5nQHpqdS5lZHUuY24=; Qing Gu, MTE5MTAxNkB6anUuZWR1LmNu