 Shaozhong Yang
Shaozhong Yang Chuanyu Fang†
Chuanyu Fang† Yu Liu
Yu Liu Shanshan Huang
Shanshan Huang Rui Wang
Rui Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 14 April 2022
Sec. Intensive Care Medicine and Anesthesiology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.844710
Background: Surgical masks (SMs) protect medical staff and reduce surgical site infections. Extended SM use may reduce oxygen concentrations in circulation, causing hypoxia, headache, and fatigue. However, no research has examined the effects of wearing SMs on oxygenation and physical discomfort of anesthesiologists.
Methods: An electronic questionnaire was established and administered through WeChat, and a cross-sectional survey was conducted to determine SM use duration and related discomfort of operating room medical staff. Then, operating room anesthesiologists were enrolled in a single-arm study. Peripheral blood oxygen saturation (SpO2), heart rate, and respiratory rate were determined at different times before and after SM use. Shortness of breath, dizziness, and headache were subjectively assessed based on the visual analog scale (VAS) scores.
Results: In total, 485 operating room medical staff completed the electronic questionnaire; 70.5% of them did not change SMs until after work, and 63.9% wore SMs continuously for more than 4 h. The proportion of anesthesiologists was the highest. After wearing masks for 4 h, the shortness of breath, fatigue, and dizziness/headache rates were 42.1, 34.6, and 30.9%, respectively. Compared with other medical staff, the proportion of subjective discomfort of anesthesiologists increased significantly with prolonged SM use from 1 to 4 h. Thirty-five anesthesiologists completed the study. There was no difference in anesthesiologist SpO2, heart rate, or respiratory rate within 2 h of wearing SMs. After more than 2 h, the variation appears to be statistically rather than clinically significant—SpO2 decreased (98.0 [1.0] vs. 97.0 [1.0], p < 0.05), respiratory rate increased (16.0 [3.0] vs. 17.0 [2.0], p < 0.01), and heart rate remained unchanged. As mask use duration increased, the VAS scores of shortness of breath, dizziness, and headache gradually increased.
Conclusion: In healthy anesthesiologists, wearing SMs for more than 2 h can significantly decrease SpO2 and increase respiratory rates without affecting heart rates.
Since December 2019, coronavirus disease 2019 (COVID-19) has spread globally and attracted worldwide attention (1). On 11 March 2020, the World Health Organization (WHO) declared COVID-19 a pandemic (2). It is essential to protect healthcare workers in the context of the COVID-19 pandemic. Medical institutions require medical staff to wear personal protective equipment during diagnosis and treatment (3). However, frequent use of personal protective equipment, especially protective masks, can lead to various health-related problems, including headache, hypoxia, and skin damage (4, 5).
In daily work, anesthesiologists face long exposures to infected bodily fluids and blood, toxic surgical smoke, bacteria, and viruses in patients' respiratory tract and the possibility of needle stab injuries, resulting in anxiety and fear (6–8). As part of the main staff in the operating room, anesthesiologists must follow the recognized infection control measures for the operating room, including the use of surgical masks (SMs). Although there is still substantial controversy (9, 10), it is generally believed that wearing SMs can protect patients from bacteria in the mouth and nose of operating room staff and protect medical staff from contaminated blood, bodily fluids, and most of the operation smoke (11).
At present, there is a serious shortage of anesthesiologists in China. The number of sudden deaths of anesthesiologists in China has increased sharply in recent years, and most of them die due to heavy workloads (12). From 11 November 2008 to 27 January 2018, 104 deaths due to overwork were reported among Chinese doctors, and anesthesiologists accounted for 20.19% of these cases (13). Increasing work pressure often leads to excessive fatigue and physical discomfort in anesthesiologists and threatens the safety of patients (14, 15). Chinese anesthesiologists need to wear SMs to work for long periods of time every day, which may increase physical and mental fatigue. Research shows that wearing masks can significantly increase the temperature and humidity of the face, resulting in a decline in the mental and physical performance of medical staff (16, 17). Recent studies have confirmed that SMs can reduce blood oxygen saturation and increase the pulse rate in surgeons after surgery (18). Although wearing SMs during vigorous exercise had no significant adverse effects on the oxygenation and exercise performance of young healthy participants (19), there is no relevant study on the effects of SM use on anesthesiologists' oxygenation and physical discomfort.
It is unclear whether wearing SMs for a long time causes changes in anesthesiologists' oxygenation, heart rate, and respiratory rate and aggravates physical and mental fatigue and whether wearing SMs for a long time is related to the high rate of sudden death among Chinese anesthesiologists. The primary purpose of this study was to investigate the effects of wearing disposable lace-up SMs for long periods of time on peripheral blood oxygen saturation (SpO2), heart rate, respiratory rate, and subjective discomfort of anesthesiologists.
This study was carried out in accordance with the Declaration of Helsinki (2013 Edition) and approved by Qilu Hospital of Shandong University Medical Ethics Committee (No. KYLL-202107-115). The requirement to obtain written informed consent was waived.
First, an electronic questionnaire was designed on the Wenjuan platform (https://www.wenjuan.com) and distributed via WeChat in 8 general hospitals in Shandong Province. The duration of mask use and the related discomfort of medical staff in the operating room were determined by a cross-sectional survey. The survey included demographic data (gender, occupation), the reasons for wearing SMs in the operating room, the duration of continuous mask use, the number of mask changes per day, and personal discomfort related to continuous mask use for 1, 2, 3, and ≥4 h. After the questionnaire was released, participants were asked to familiarize themselves with the questions and reply to the questionnaire after 1 week of work. Only one submission per person was allowed to prevent duplication.
Then, according to the survey results, anesthesiologists working in the operating room of Qilu Hospital of Shandong University were selected as subjects. They were required to wear disposable lace-up SMs (the Chinese standard number is YY0469-2011) correctly and not remove them or expose their mouth and nose during the study. All subjects were informed that they could withdraw from the study at any time without any impact. The primary exclusion criteria were acute or chronic respiratory diseases or previous heart diseases, body mass index (BMI) ≥30 kg/m2, the presence of inflammation on the facial skin, lax skin, allergic rhinitis, and nasal septum deviations.
The enrolled anesthesiologists fully understood the study procedures, underwent testing in a familiar constant temperature operating room, and breathed indoor air. The subject ensured that the SM was correctly and continuously worn throughout the process. After resting for at least 10 min, the SpO2 and pulse rate of the subject's right index finger were measured using a portable SpO2 patient monitoring system (Covidien LLC, Manstield, OH, USA) in a sitting position. To eliminate the difference in oxygen content in the operating room, an oxygen detector (Smart Sensor, Dongguan, China) was used to detect the surrounding oxygen content. Another researcher also directly observed 30 s of chest movement and measured the respiratory rate. As a distraction strategy, the investigators pretended to measure the radial pulse so that participants did not realize that their respiratory rate was being measured.
Participants underwent pulse oximetry evaluation. According to the questionnaire survey results, it was determined that data would be collected at 6 time points: 10 min before wearing an SM (T1), immediately after wearing a mask (T2), and after 1 h (T3), 2 h (T4), 3 h (T5), and 4 h (T6) of continuously wearing an SM. The visual analog scale (VAS) was used to record subjects' perception of the sensation of shortness of breath, dizziness, and headache at the same time points. All sensations were scored by means of a 10-point VAS from 0 (no discomfort) to 10 (worst discomfort imaginable). To minimize variability, data were collected twice at each point in time.
The study sample size was calculated with PASS 11 (NCSS, LLC Kaysville, UT, USA). Before the release of the electronic questionnaire, we conducted a small-scale preliminary survey. The incidence of wearing SMs continuously for morethan 4 h was 55%. We assumed that the incidence was 50%, with α of 5%, absolute deviation of 5%, and the sample size of 402. Previous studies have shown that masks can reduce the blood oxygen saturation of medical staff by 1–3.5% (20, 21). We determined whether wearing an SM was associated with an SpO2 decrease of 2% or more. For a 2% decrease in SpO2, a standard deviation of 3%, α of 5%, and power of 90%, a sample size of at least 24 participants was required. Considering the 10% shedding rate, at least 27 participants were required. According to the inclusion and exclusion criteria, we included 39 anesthesiologists. One participant whose resting oxygen saturation reading was lower than 96% and 3 participants who did not complete the test due to removing their masks were excluded, and a total of 35 subjects were included.
The result of electronic questionnaire was charted by Microsoft Excel software. The SpO2, heart rate, respiratory rate data, and subjective sensation scores of anesthesiologists wearing SMs at different durations were analyzed. SPSS 24.0 (IBM, Armonk, NY: IBM Corp.) Graphpad prism 8.2.1 (GraphPad Sofware Inc., California, US) were used for the statistical evaluation and preparation of graphs.
The Shapiro–Wilk test was used to determine whether the measurement data conform to the normal distribution. The data with normal distribution were expressed as mean (standard deviation, SD), and the non-normal distribution data were expressed as median (interquartile range, IQR). Univariate ANOVA was used for comparisons between groups. The non-normal distribution data were analyzed by the Kruskal–Wallis test. A p value of < 0.05 was considered statistically significant.
A total of 485 operating room medical staff completed the electronic questionnaire survey, of which anesthesiologists accounted for 24.9% (n = 121/485) (Figure 1A). Due to professional reasons and gender factors, the gender difference of anesthesiologists was smaller, and men account for 40.0% (n = 48/121) (Figure 1B). As shown in Figure 1B, compared with anesthesiologists (48 men [40.0%]), there were greater gender differences among operating room nurses (42 men [19.7%]), nurse anesthetists (12 men [10.7%]), and surgeons (25 men [86.2%]), and surgeons had lower participation in the questionnaire.
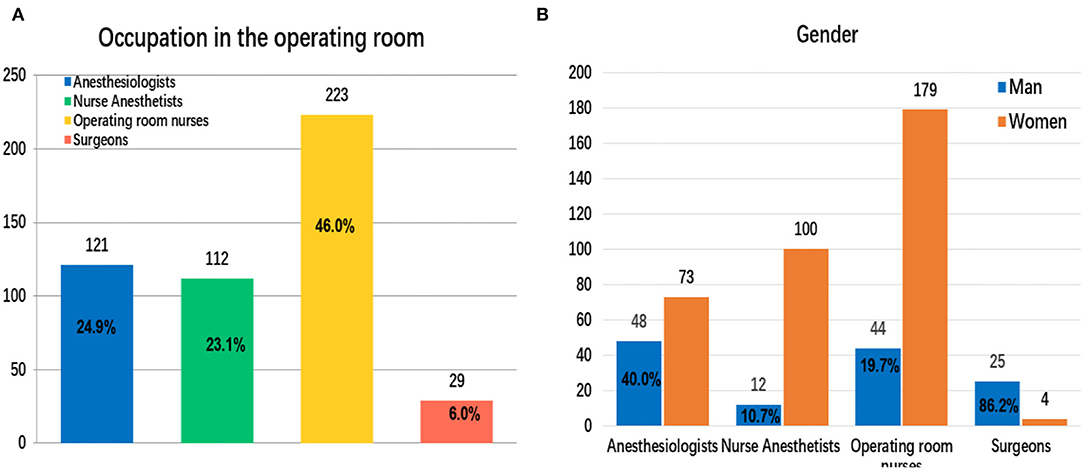
Figure 1. Occupation and gender of operating room medical staff who participated in the electronic questionnaire (A,B).
A total of 63.9% (n = 310/485) of the participants wore SMs continuously for more than 4 h (without removing the masks or exposing their mouths or noses) (Figure 2A). Among the four occupations, the proportion of anesthesiologists wearing SMs continuously for more than 4 h was highest, which was 74.4% (n = 90/121) (Figure 2C). On a given day of work, 70.52% (n = 342/485) did not change their mask until after work (Figure 2B). Among them, the proportion of anesthesiologists was still the highest, accounted for 90.1% (n = 109/121) (Figure 2D).
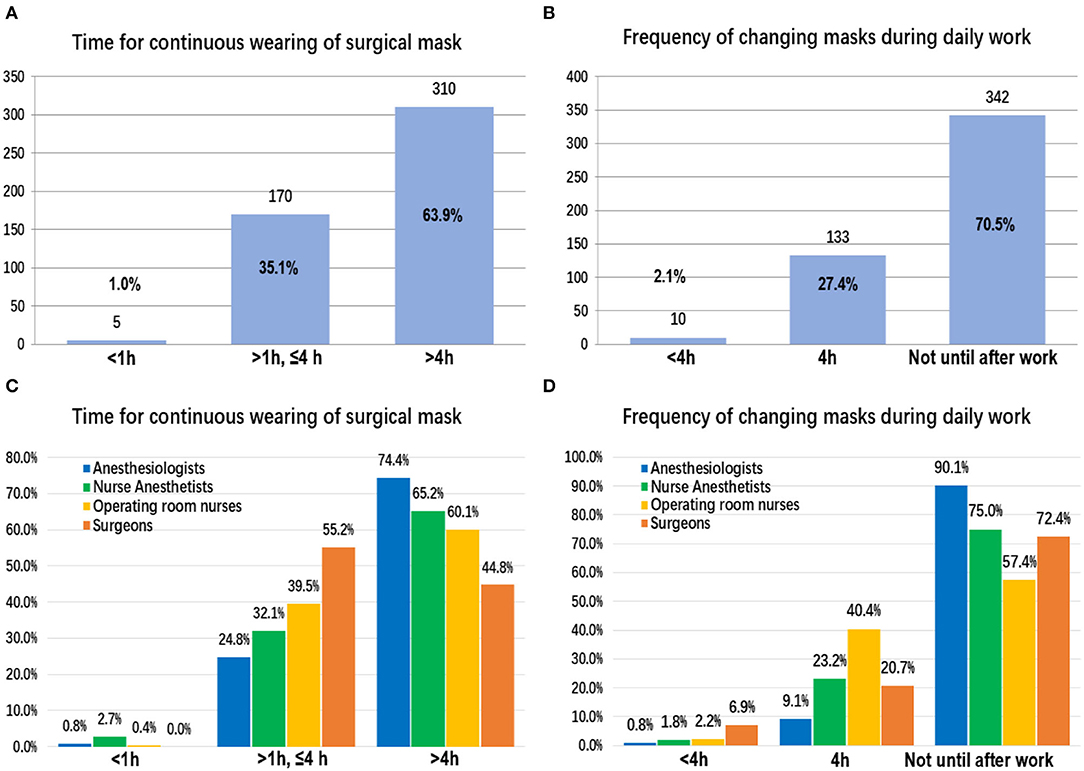
Figure 2. The duration of continuous surgical mask use and the frequency of mask changes on working days: among all participants (A,B) and between different occupations (C,D).
As shown in Figure 3A, 77.73% (n = 377/485) wore SMs continuously for 1 h without any subjective discomfort. As the SM use time increased, this proportion decreased significantly (Figures 3C, 4A,C). While wearing an SM for 4 h, only 30.52% (n = 148/485) had no discomfort (Figure 4C). With prolonged SM use, discomfort, such as shortness of breath, dizziness/headache, fatigue, and inattention, increased significantly. When wearing an SM continuously for 4 h, the proportions of shortness of breath, fatigue, and dizziness/headache reached 42.1% (n = 204/485), 34.6% (n = 168/485), and 30.9% (n = 150/485), respectively (Figure 4C). Compared with operating room nurses, nurse anesthesiologists, and surgeons, the proportions of subjective discomfort of anesthesiologists were almost all the highest in 1–4 h (Figures 3B,D, 4B,D).
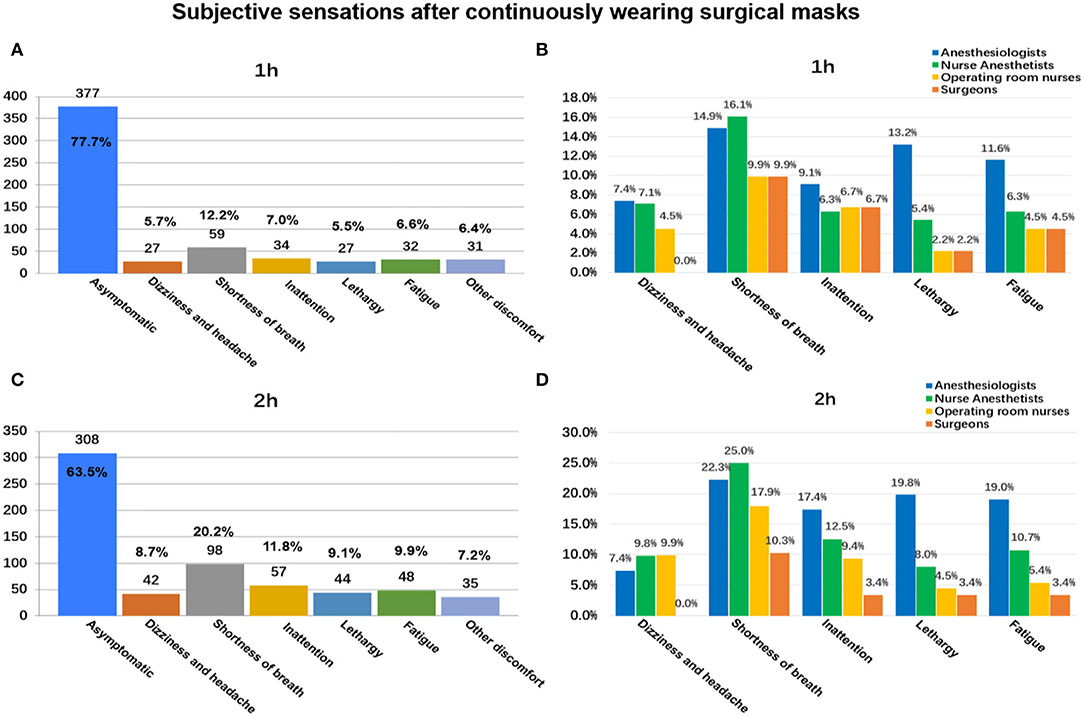
Figure 3. Subjective discomfort associated with continuously wearing surgical masks for 1 and 2 h: among all participants (A,B) and between different occupations (C,D).
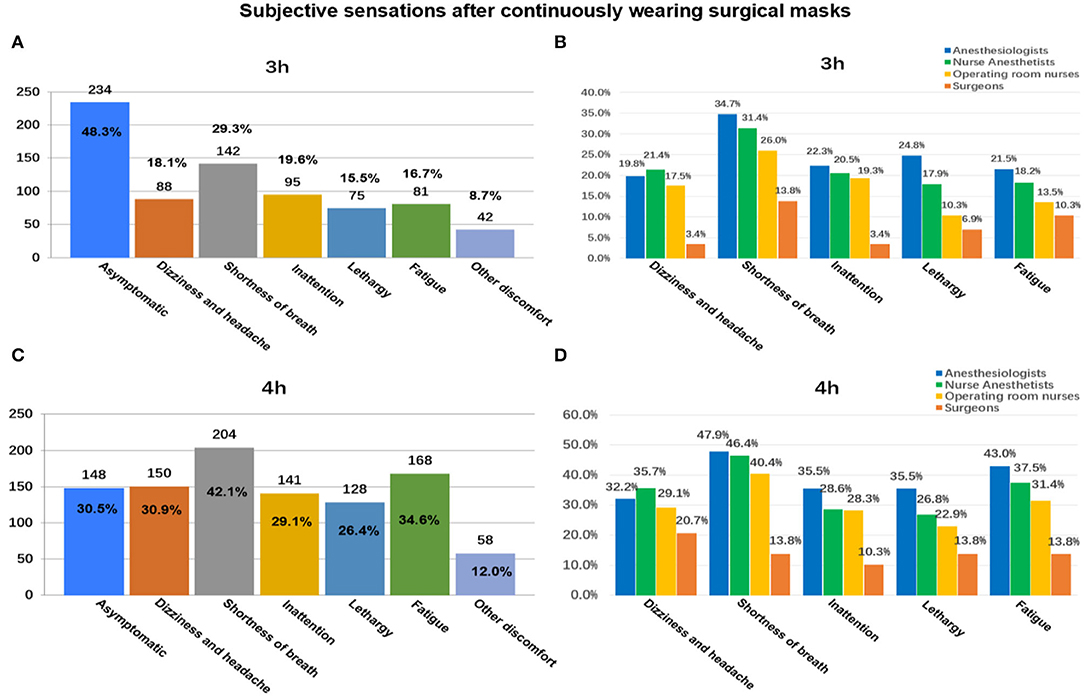
Figure 4. Subjective discomfort associated with continuously wearing surgical masks for 3 and ≥4 h: among all participants (A,B) and between different occupations (C,D).
In further research, 35 anesthesiologists (mean age, 34.5 years [SD, 7.9 years]; 16 men [46.0%]) were enrolled (Table 1). As shown in Figure 5A, there was no significant difference in the average oxygen content of the environment among time points. There was no significant difference in heart rate change at 5 time points after wearing a mask compared with that before use (Figure 5C).
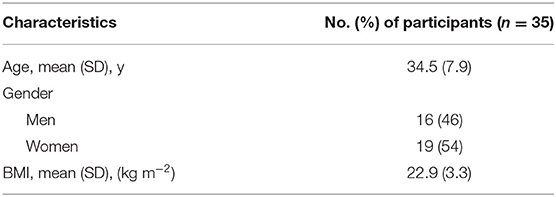
Table 1. Baseline characteristics of participants.
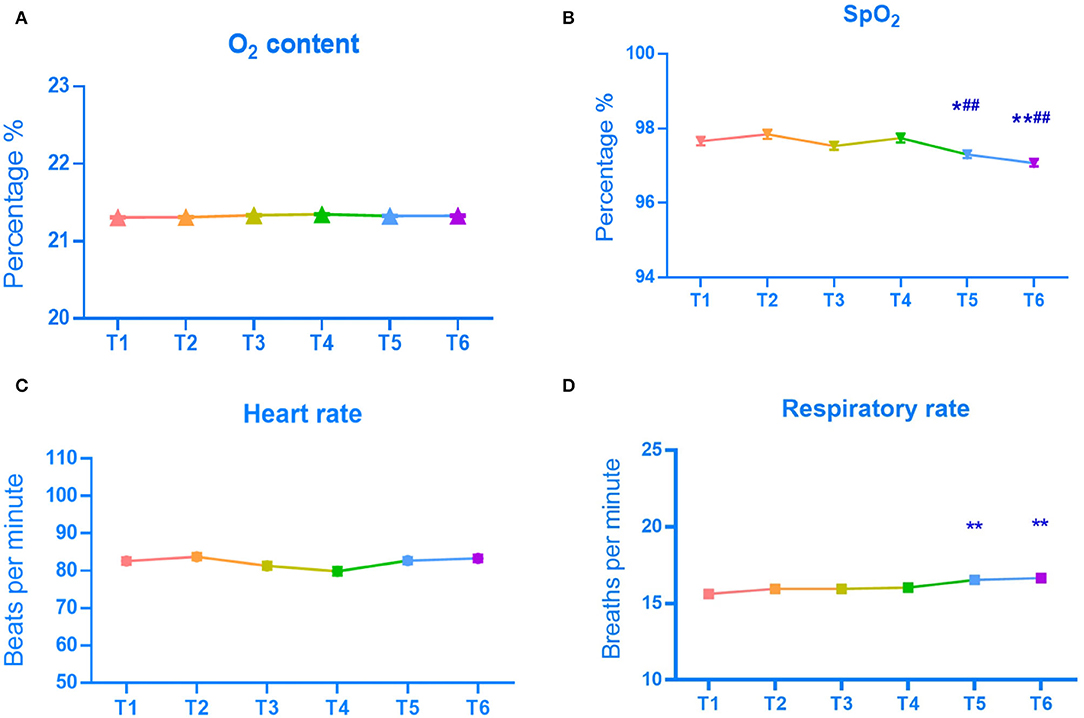
Figure 5. Mean O2 content (A), SpO2 (B), heart rate (C), and respiratory rate (D) by time point. *P < 0.01, **P < 0.01, vs. the value of before SM use (T1). ##P < 0.01, vs. the value of immediately after SM use (T2).
The mean SpO2 from T1 to T6 was 98.0, 98.0, 98.0, 98.0, 97.0, and 97.0%, respectively (Table 2). As shown in Figures 5B,D, SpO2 gradually decreased, and the respiratory rate gradually increased as the duration of SM use increased. Compared with before and immediately after wearing an SM, after wearing an SM for 2 h, there was a statistically significant decrease in SpO2 (p < 0.05) and an increase in respiratory rate (p < 0.01).
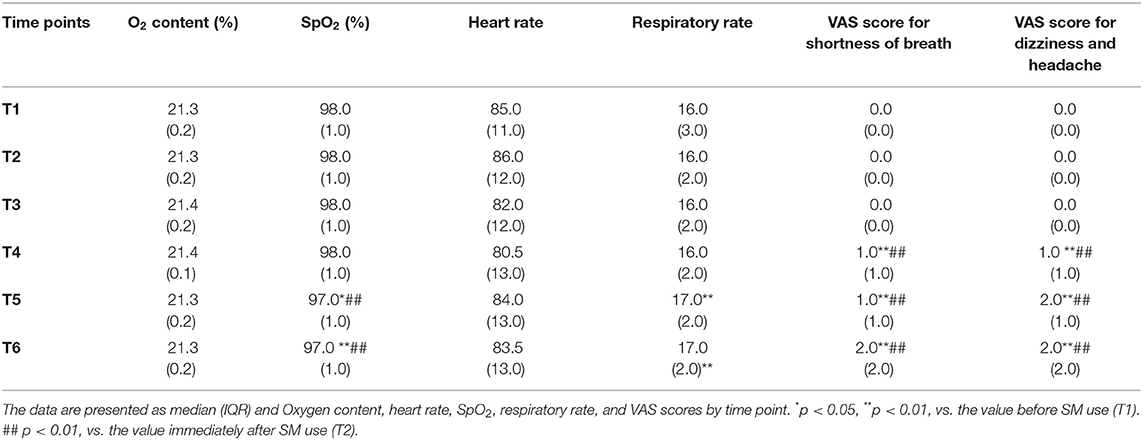
Table 2. Results.
The VAS scores of 35 participants at six time points were compared. The results showed that the VAS scores for shortness of breath, dizziness, and headache increased significantly as the duration of continuous SM use increased (Table 2). Compared with before and immediately after wearing an SM, there was a significant difference in the VAS scores after wearing an SM ≥ 1 h (p < 0.01) (Figures 6A,B).
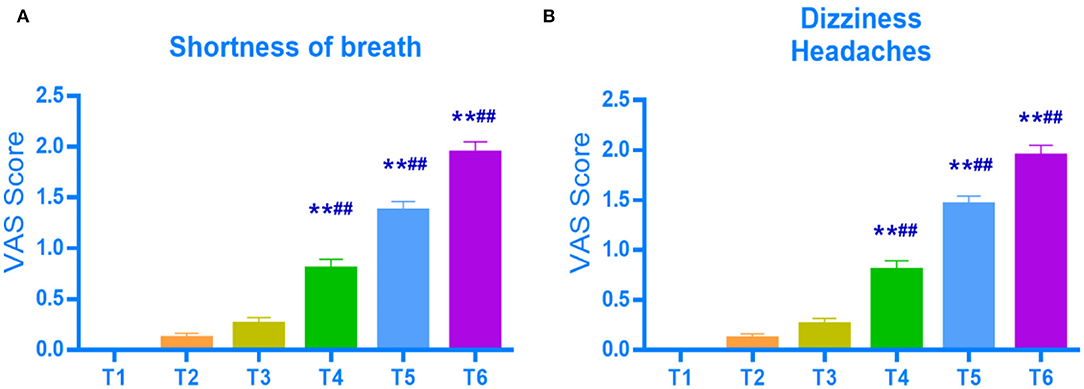
Figure 6. VAS scores for shortness of breath (A), dizziness and headaches (B) by time point. **P < 0.01, vs. the value of before SM use (T1). ##P < 0.01, vs. the value of immediately after SM use (T2).
The results of the electronic questionnaire showed 70.5% of the respondents wore SMs from the beginning of a day's work to the end. Most staff (63.9%) continued to wear masks (without removing the mask or exposing their mouth or nose) for more than 4 h, with the highest proportion of anesthesiologists. Subjective discomfort, such as shortness of breath, dizziness and headache, inattention, lethargy, and fatigue, worsened with the prolonged use of SMs. Compared with operating room nurses, nurse anesthetists, and surgeons, with prolonged SM use, the proportion of subjective discomfort of anesthesiologists increased significantly, and was almost the highest in 1–4 h. Further research results showed that anesthesiologists wearing SMs for more than 2 h exhibited significantly reduced SpO2 levels and significantly increased respiratory rates, but no change was observed in heart rates. Although the data showed statistically significant differences, these changes have clinical significance needs to be further studied. In addition, wearing SMs for more than 2 h caused mild shortness of breath, dizziness, and headaches.
The results of this study are different from those of other studies. Many studies have shown that SMs can reduce oxygen concentrations and increase heart rate. Beder et al. repeatedly measured the SpO2 of 53 surgeons before and after surgery. The results showed that the surgeon's pulse rate increased, and their blood oxygen saturation decreased by more than 1% after 1 h, which was related to SM or operational stress (18). The SpO2 and heart rate of 20 oral surgeons wearing SMs during surgery were measured. It was found that as heart rate increased, SpO2 decreased from 97.5% before the operation to 94.0% after the operation, accompanied by shortness of breath and lightheadedness/headache (20). In a study of college students, it was found that the use of SMs in 150-min college courses could lead to an increase in heart rate and a decrease in blood oxygen saturation but it had no significant effect on students' perception of psychological fatigue or reaction time (21).
In this study, it was observed that the decrease in SpO2 and the increase in the respiratory rate occurred only after anesthesiologists wore SMs for more than 2 h, and it was observed that the degree of shortness of breath, dizziness, and headache increased as the duration of continuous mask use increased. However, no significant change in heart rate was observed, which may be because anesthesiologists who work in operating rooms and wear masks for long periods of time adapt to the psychological and physical effects caused by mask use and are familiar with the operating room environment. In addition, the long-term stress of anesthesiologists can aggravate occupational fatigue and lead to decreased reactivity and attention (22, 23), reducing the stress response of the cardiovascular system.
Wearing SMs in the operating room is not only a traditional practice (7, 24) but also a requirement for the prevention of surgical site infections (SSIs) and the protection of staff, according to the relevant guidelines of the Centers for Disease Control and Prevention (CDC) and the Healthcare Infection Control Practices Advisory Committee (HICPAC) (25). SMs are disposable and provide protection for at least 4 h (9), but this protective effect decreases over time. The general recommended time to wear an SM is 4 h (26). Studies have shown that SMs are a source of bacterial contamination during surgery. After 2 h of continuous SM use, the bacterial count in SMs increased significantly. Therefore, it is recommended that surgeons replace their masks after each operation, especially for operations lasting longer than 2 h (27). However, most operating room staff do not use masks correctly, as required, and do not understand the current guidelines for mask use, which may increase the SSI rate (28).
One study that used thermal infrared imaging was used to evaluate changes in facial skin temperature while wearing masks, and perceptual scores related to humidity, heat, dyspnea, and overall discomfort were recorded (16). It was found that wearing an SM or respirator continuously for 1 h leads to an increase in facial skin temperature under the mask and subjective discomfort, which decreases rapidly after removing the mask for 1 min and returns to the baseline level after 5 min (16). This study showed that heat stimulation on the surface around the mouth, nose, and cheeks plays an important role in regulating heat exchange in the respiratory tract. An earlier study showed that SMs may increase airway resistance and significantly reduce the surgeon's blood oxygen saturation level (29). A recent study also confirmed that airway resistance with SMs is twice as high as that without a mask, which causes an increase in heart rate (30).
The decrease in SpO2 may be due to the increased CO2 content in the inhaled air resulting from exhaled CO2 becoming trapped under the SM. While wearing an SM, repeated inhalation and exhalation of a small amount of CO2 may increase dyspnea (31). Mild CO2 retention and hypoxemia may also lead to cognitive effects and reduce responsiveness (32). A small decrease in oxygen stimulates the sympathetic nervous system, resulting in a faster heart rate (33). The increase in respiratory resistance caused by masks leads to an increase in respiratory muscle work and intrathoracic negative pressure, increases cardiopulmonary oxygen consumption, significantly increases heart rate, and further leads to physical discomfort and increased pressure (34). During the COVID-19 outbreak, medical staff had headaches due to the use of masks. In addition, symptoms, such as shortness of breath, sleep disorders, and fatigue, increased significantly (35, 36).
This study has some limitations: (1) The questionnaire was released in advance, and responses were required to be submitted 1 week after becoming familiar with the questions, which may introduce recall bias, and the subjects may have provided “ideal” answers. (2) The anesthesiologists involved in the study were younger and more tolerant of hypoxia caused by wearing SMs for a long time, so the time of oxygen saturation reduction and respiratory rate increase was longer. (3) There was no control group because the study was conducted in the emergency situation of the COVID-19 pandemic. According to the requirements of epidemic prevention and control and operating rooms, masks must be worn. (4) The sample size was too small to carry out age- and gender-controlled research.
In conclusion, our study demonstrates that in healthy anesthesiologists, wearing SMs for more than 2 h can lead to statistically significant decreases in SpO2 and increases in respiratory rates, without affecting heart rates, but may not be clinically significant. Shortness of breath, dizziness, and headache gradually worsen as the duration of SM use increases. Therefore, we recommend that anesthesiologists take off their masks and rest for a few minutes every 2 h or after each operation and replace the SM every 4 h according to the guidelines.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Qilu Hospital of Shandong University Medical Ethics Committee. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
XL, CF, SY, and RW contributed to data collection. CF, YL, SY, and SH contributed to statistical analysis. SY, FQ, and YL wrote the manuscript. SY, XL, FQ, and CF contributed to the inception of the study idea. SY, XL, FQ, and RW contributed to study design. SY, FQ, YL, and SH revised the manuscript. All authors approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors thank all involved anesthesiologists for their contribution to this trial.
1. Guan W, Ni Z, Hu Y, Liang W, Ou C, He J, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) 382:1708–20. doi: 10.1056/NEJMoa2002032
2. World Health Organization (WHO). Coronavirus disease (COVID-19). Events as they Happen. (2020). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed March 24, 2020).
3. Zhou P, Huang Z, Xiao Y, Huang X, Fan XG. Protecting Chinese healthcare workers while combating the 2019 novel coronavirus. Infect Control Hosp Epidemiol. (2020) 41:745–6. doi: 10.1017/ice.2020.60
4. Ong JJY, Bharatendu C, Goh Y, Tang JZY, Sooi KWX, Tan YL, et al. Headaches Associated With Personal Protective Equipment - A Cross-Sectional Study Among Frontline Healthcare Workers During COVID-19. Headache. (2020) 60:864–77. doi: 10.1111/head.13811
5. Gheisari M, Araghi F, Moravvej H, Tabary M, Dadkhahfar S. Skin reactions to non-glove personal protective equipment: an emerging issue in the COVID-19 pandemic. J Eur Acad Dermatol Venereol. (2020) 34:e297–8. doi: 10.1111/jdv.16492
6. Steege AL, Boiano JM, Sweeney MH. Secondhand smoke in the operating room? Precautionary practices lacking for surgical smoke. Am J Ind Med. (2016) 59:1020–31. doi: 10.1002/ajim.22614
7. Romney MG. Surgical face masks in the operating theatre: re-examining the evidence. J Hosp Infect. (2001) 47:251–6. doi: 10.1053/jhin.2000.0912
8. Liu Y, Song Y, Hu X, Yan L, Zhu X. Awareness of surgical smoke hazards and enhancement of surgical smoke prevention among the gynecologists. J Cancer. (2019) 10:2788–99. doi: 10.7150/jca.31464
9. Vincent M, Edwards P. Disposable surgical face masks for preventing surgical wound infection in clean surgery. Cochrane Database Syst Rev. (2016) 4:CD002929. doi: 10.1002/14651858.CD002929.pub3
10. Webster J, Croger S, Lister C, Doidge M, Terry MJ, Jones I. Use of face masks by non-scrubbed operating room staff: a randomized controlled trial. ANZ J Surg. (2010) 80:169–73. doi: 10.1111/j.1445-2197.2009.05200.x
11. Leung NHL, Chu DKW, Shiu EYC, Chan KH, McDevitt JJ, Hau BJP, et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat Med. (2020) 26:676–80. Erratum in: Nat Med. 2020. doi: 10.1038/s41591-020-0843-2
12. The Lancet. Physician burnout: a global crisis. Lancet. (2019) 394:93. doi: 10.1016/S0140-6736(19)31573-9
13. Yang S, Fang C, Liu X, Liu Y, Huang S, Qi F. Burnout in healthcare: a sign of death by overwork for doctors in China. BMJ. (2019) 367:l5806. doi: 10.1136/bmj.l5806
14. Moore R, Gupta P, Duval Neto GF. Occupational fatigue: Impact on anesthesiologist's health and the safety of surgical patients. Braz J Anesthesiol. (2013) 63:167–9. doi: 10.1016/S0034-7094(13)70209-5
15. Sinha A, Singh A, Tewari A. The fatigued anesthesiologist: A threat to patient safety? J Anaesthesiol Clin Pharmacol. (2013) 29:151–9. doi: 10.4103/0970-9185.111657
16. Scarano A, Inchingolo F, Lorusso F. Facial Skin Temperature and Discomfort When Wearing Protective Face Masks: Thermal Infrared Imaging Evaluation and Hands Moving the Mask. Int J Environ Res Public Health. (2020) 17:4624. doi: 10.3390/ijerph17134624
17. Kara E, Mete B, Demirhindi H, Mete E, Kanat C. Effect of use of surgical facemasks and FFP2 facepiece respirators with or without exhalation valves on breathing air quality and physiological outcomes in health workers: a quasi-experimental model. Fresenius Environ Bull. (2021) 30:11371–8.
18. Beder A, Büyükkoçak U, Sabuncuoglu H, Keskil ZA, Keskil S. Preliminary report on surgical mask induced deoxygenation during major surgery. Neurocirugia (Astur). (2008) 19:121–6. doi: 10.1016/S1130-1473(08)70235-5
19. Shaw K, Butcher S, Ko J, Zello GA, Chilibeck PD. Wearing of Cloth or Disposable Surgical Face Masks has no Effect on Vigorous Exercise Performance in Healthy Individuals. Int J Environ Res Public Health. (2020) 17:8110. doi: 10.3390/ijerph17218110
20. Scarano A, Inchingolo F, Rapone B, Festa F, Tari SR, Lorusso F. Protective Face Masks: Effect on the Oxygenation and Heart Rate Status of Oral Surgeons during Surgery. Int J Environ Res Public Health. (2021) 18:2363. doi: 10.3390/ijerph18052363
21. Tornero-Aguilera JF, Clemente-Suárez VJ. Cognitive and psychophysiological impact of surgical mask use during university lessons. Physiol Behav. (2021) 234:113342. doi: 10.1016/j.physbeh.2021.113342
22. Stuetzle KV, Pavlin BI, Smith NA, Weston KM. Survey of occupational fatigue in anaesthetists in Australia and New Zealand. Anaesth Intensive Care. (2018) 46:414–23. doi: 10.1177/0310057X1804600411
23. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. (2018) 283:516–29. doi: 10.1111/joim.12752
24. Moszkowicz D, Hobeika C, Collard M, Bruzzi M, Beghdadi N, Catry J, et al. Chirurgie Digestive, Association de Chirurgie Hépato-Bilio-Pancréatique et Transplantation. Operating room hygiene: Clinical practice recommendations. J Visc Surg. (2019) 156:413–22. doi: 10.1016/j.jviscsurg.2019.07.010
25. O'Hara LM, Thom KA, Preas MA. Update to the Centers for Disease Control and Prevention and the Healthcare Infection Control Practices Advisory Committee Guideline for the Prevention of Surgical Site Infection (2017): a summary, review, and strategies for implementation. Am J Infect Control. (2018) 46:602–9. doi: 10.1016/j.ajic.2018.01.018
26. Loveday HP, Wilson JA, Pratt RJ, Golsorkhi M, Tingle A, Bak A, et al. UK Department of Health. epic3: national evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect. (2014) 86 (Suppl 1):S1–70. doi: 10.1016/S0195-6701(13)60012-2
27. Zhiqing L, Yongyun C, Wenxiang C, Mengning Y, Yuanqing M, Zhenan Z, et al. Surgical masks as source of bacterial contamination during operative procedures. J Orthop Translat. (2018) 14:57–62. doi: 10.1016/j.jot.2018.06.002
28. Herron JBT, Kuht JA, Hussain AZ, Gens KK, Gilliam AD. Do theatre staff use face masks in accordance with the manufacturers' guidelines of use? J Infect Prev. (2019) 20:99–106. doi: 10.1177/1757177418815551
29. Yip WL, Leung LP, Lau PF, Tong HK. The effect of wearing a face mask on body temperature. Hong Kong J Emerg Med. (2005) 12:23–7. doi: 10.1177/102490790501200102
30. Lässing J, Falz R, Pökel C, Fikenzer S, Laufs U, Schulze A, et al. Effects of surgical face masks on cardiopulmonary parameters during steady state exercise. Sci Rep. (2020) 10:22363. doi: 10.1038/s41598-020-78643-1
31. Banzett RB, Lansing RW, Brown R, Topulos GP, Yager D, Steele SM, et al. 'Air hunger' from increased PCO2 persists after complete neuromuscular block in humans. Respir Physiol. (1990) 81:1–17. doi: 10.1016/0034-5687(90)90065-7
32. Kent BD, Mitchell PD, McNicholas WT. Hypoxemia in patients with COPD: cause, effects, and disease progression. Int J Chron Obstruct Pulmon Dis. (2011) 6:199–208. doi: 10.2147/COPD.S10611
33. Lamba TS, Sharara RS, Singh AC, Balaan M. Pathophysiology and Classification of Respiratory Failure. Crit Care Nurs Q. (2016) 39:85–93. doi: 10.1097/CNQ.0000000000000102
34. Cheyne WS, Harper MI, Gelinas JC, Sasso JP, Eves ND. Mechanical cardiopulmonary interactions during exercise in health and disease. J Appl Physiol. (2020) 128:1271–9. doi: 10.1152/japplphysiol.00339.2019
35. Köseoglu Toksoy C, Demirbaş H, Bozkurt E, Acar H, Türk Börü Ü. Headache related to mask use of healthcare workers in COVID-19 pandemic. Korean J Pain. (2021) 34:241–5. doi: 10.3344/kjp.2021.34.2.241
Keywords: anesthesiologists, heart rate, peripheral oxygen saturation, respiratory rate, surgical mask
Citation: Yang S, Fang C, Liu X, Liu Y, Huang S, Wang R and Qi F (2022) Surgical Masks Affect the Peripheral Oxygen Saturation and Respiratory Rate of Anesthesiologists. Front. Med. 9:844710. doi: 10.3389/fmed.2022.844710
Received: 28 December 2021; Accepted: 15 March 2022;
Published: 14 April 2022.
Edited by:
Giovanni Damiani, University of Milan, ItalyReviewed by:
Banu Numan Uyal, Cyprus International University, CyprusCopyright © 2022 Yang, Fang, Liu, Liu, Huang, Wang and Qi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Feng Qi, cWlmZW5nNjYzMjFAc2luYS5jb20=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.