 Zexuan Yu
Zexuan Yu Wen Qin3*
Wen Qin3* Jiajia Li
Jiajia Li
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 09 January 2023
Sec. Family Medicine and Primary Care
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.842817
This article is part of the Research Topic Population Medicine and Health Economics View all 16 articles
Background: Risky health behaviors in childhood, including smoking, alcohol consumption, and having a poor diet, are the major sources of non-communicable diseases in adulthood. This study aimed to examine how parents affect children's risky health behaviors and whether intergenerational transmission differs based on socioeconomic status (SES).
Methods: Data were extracted from the 1991–2015 China Health and Nutrition Survey (CHNS). Smoking (n = 5,946), alcohol consumption (n = 7,821), and sugar-sweetened beverages (SSBs) consumption (n = 3,537) were used as proxies for risky health behaviors in children. A binary choice model for panel data with a random-effect specification was employed to examine whether risky health behaviors can be transmitted from parents to their children. Subsequently, we conducted a seemingly unrelated estimation test (SUEST) to explore the differences in parental transmission between the different SES groups.
Results: We found strong intergenerational persistence of smoking, alcohol drinking, and SSBs drinking behaviors, except for the mothers' smoking behavior. Mothers had a greater influence on children's alcohol drinking and SSBs drinking behaviors than fathers both in urban and rural areas and in different SES groups. The intergenerational transmission of SSBs drinking behavior exhibited a decreasing trend with increasing SES for both urban and rural families. In urban areas, mothers' alcohol drinking behavior has a decreasing trend with increasing education level, occupation, and income; however, in rural areas, the influence of mothers' alcohol drinking behavior occurred in the same direction with increasing education level and occupation type. In rural areas, the influence of fathers' drinking and smoking behaviors on children appears to mostly increase with increasing SES. Meanwhile, the influence of such behaviors among urban fathers would decrease with increasing SES.
Conclusion: Parents' behaviors and SES can influence the initiation of risky health behaviors in their offspring. Thus, to promote healthy behaviors, policymakers can introduce health education programs for parents, particularly for those living in rural areas and with a low SES.
Risky health behaviors, such as smoking, drinking alcohol, and having a poor diet, are major potential causes of death (1–6) and are often initiated in childhood and tend to persist into adulthood (5, 7–11). Thus, it is of great significance to prevent them earlier in life as the disease progresses (5, 12). However, the prevalence of smoking, alcohol drinking, and having unhealthy diets, such as sugar-sweetened beverages (SSBs), is substantial among children and adolescents. In 2018, ~43 million children aged 13–15 years used tobacco (13), and ~155 million adolescents were current drinkers globally (14). Investigations from the United States and China have found that over 60% of children and adolescents consume SSBs daily (15–18). Although the dangers of tobacco and alcohol are well-known (1, 10, 11, 13, 14), SSBs are dangerous because they often contain caffeine and sugar, which can be addictive. Caffeine addiction is a well-known problem (19, 20), but it has received more attention in recent years. Some animal-based studies have not only revealed similarities between added sugars and substance abuse in binge eating, craving, tolerance, and withdrawal (21) but also some have confirmed similar addictive characteristics in adolescents (22). In addition, some human neuroimaging studies have shown that high sugar intake activates neural circuits and reward systems like those of substance abuse (23, 24). Long-term sugar consumption can lead to obesity and diabetes, among other serious consequences (15–17).
Family is a key environment that influences children's behavior. As children's first teachers and socializing agents, parents' negative health behaviors can act as a bad model for their children (25–28). In addition, parental socioeconomic status (SES) variables, including educational attainment, income, and occupational status, together with parenting styles, constitute the home environment in which children's behaviors are embedded (25, 29–39).
There have already been many studies on the relationship between SES and children's risky health behaviors; however, whether SES differences affect the intergenerational transmission of unhealthy behaviors has not been sufficiently clarified. Previous studies have focused on parents' own behavior and the relationship between SES and parenting styles, which provide a reference for our own research proposition (26, 27, 29–31, 40–44). According to Cockerham's Health Lifestyle Theory (45), high-SES parents not only avoid the transmission of their own negative health behaviors but also their gentle parenting style helps to develop self-control in their children (45). In contrast, low-SES families tend to adopt strict, punitive, and authoritarian parenting styles, leading to children's poor self-control and making them more likely to emulate their parents' risky health behavior (28–31, 33, 34, 39, 46–52). In other words, the intergenerational transmission of risky health behaviors is likely to be in reverse to the SES gradient. However, other research studies showed that with increasing SES, the intergenerational transmission of risky parental health behaviors becomes increasingly apparent (35, 37, 53–55). Yu and Abler (54) proposed that higher education in rural China is often associated with more social activities, and with cigarettes and wine being more accessible. Wu (56) confirmed Yu's conclusion regarding the association between education and alcohol drinking. Furthermore, a Belgian study found that higher-educated mothers tended to have higher workloads and thus spent less time with their children, making them more vulnerable to risky health behaviors (53). Therefore, the contribution of this study is not only to measure the intergenerational transmission effect of these risky health behaviors with panel data including nine waves spanning 15 years but also to further measure whether there are SES differences in the intergenerational transmission effect based on Cockerham's health lifestyle theory with seemingly unrelated estimation test (SUEST). Urban and rural differences are also considered.
In the hope of adding up-to-date evidence to previous cross-sectional studies and using the longitudinal database from the China Health and Nutrition Survey (CHNS), this study aimed to examine how parents affect children's risky health behaviors. China, a developing country with rapid economic growth, is quite different from developed countries that have been studied earlier in this field (28, 31, 33, 39). Thus, the characteristics of this research proposal may be different, and the research conclusions can provide a reference for other developing countries. As a developing country, and unlike developed countries like the United States, China's laws do not make it clear that children's smoking and drinking behaviors are illegal. Without such legal restrictions, children's behaviors depend more on family constraints, and hence identifying the effects of intergenerational transmission of these risky health behaviors is more critical (25, 57–61). Moreover, considering that adults often have difficulty making behavioral changes to addictive behaviors, it may be more effective to prevent and reduce risky health behaviors in children from the perspective of reducing intergenerational transmission. Therefore, we further explored whether intergenerational transmission differed by parental SES.
The primary database used in this study was the CHNS. The CHNS is an ongoing nationwide cohort project in China with 10 available waves from 1989 to 2015. These areas are representative and diverse in terms of a wide range of socioeconomic factors (including income, education, and employment) and other related demographic, health, and nutritional factors. As only individuals aged between 20 and 45 years were surveyed in 1989, we excluded the baseline data, and only used data from 1991 to 2015 in the analysis, singling out smoking, alcohol drinking, and SSB drinking as proxies for risky health behaviors in children aged <18 years. We excluded samples with outliers and missing data, leaving 5,946 observations in the smoking group, 7,821 observations in the alcohol drinking group, and 3,537 observations in the SSBs drinking group. After matching the parent's ID with the child's ID, we obtained 24,573 observations in total: 4,609 observations in 1991, 4,140 in 1993, 3,577 in 1997, 3,312 in 2000, 1,972 in 2004, 1,583 in 2006, 1,424 in 2009, 1,782 in 2011, and 2,174 in 2015. Due to the existence of missing values in the dependent and control variables, we had to drop records containing missing values. Finally, we obtained 5,946 observations in the sample of children's smoking behavior, 7,821 observations in the sample of children's alcohol drinking behavior, and 3,537 observations in the sample of children's SSBs drinking behavior.
The main dependent variables in this study were children's smoking, alcohol drinking, and SSB drinking behaviors. Smoking was assessed using the question, “Have you ever smoked?,” and was coded as 1 if the respondent answered “Yes.” Alcohol consumption was assessed based on the question, “Did you drink beer or any other alcoholic beverage?” and was coded as 1 if the respondent answered “Yes.” SSBs consumption was assessed based on the question, “Did you drink soft drinks or sugared fruit?” and coded as 1 if the respondent answered “Yes.” All risky health behaviors were answered by the respondents. We then linked answers from the parent questionnaires to those of their children.
The independent variables were the risky parental health behaviors of these children, which were also assessed based on the three questions above. To analyze how risky health behaviors are transmitted from parents to their children, we also included parental SES variables, including educational attainment (completed years of formal education in regular schools), household per capita income (RMB in 2015), and career type (manual labor/non-manual labor). Demographic variables, such as age (years) and sex (male/female), were also included. In addition, we controlled the area (categorized as Western: Guangxi, Guizhou, and Chongqing; Northeastern: Liaoning and Heilongjiang; Central: Henan, Hubei, and Hunan; Eastern: Jiangsu, Shandong, Beijing, and Shanghai) and wave (1991, 1993, 1997, 2000, 2004, 2006, 2009, 2011, and 2015) effects. The variable of education was transformed into a dichotomous variable, with >6 years of education being classified as a high level of education, and ≤ 6 years of education being classified as a low level of education.
Data analyses were conducted using STATA/SE 14.0. Descriptive statistics for both parental and children's risky health behaviors, including smoking, alcohol use, and drinking SSBs, were reported as proportions, with corresponding chi-square tests to examine whether these behaviors were statistically significant for transmission from parents to their children. Parental SES and demographic variables were also estimated as proportions for categorical variables and means for continuous variables; chi-square tests for dichotomous variables and t-tests for continuous variables were conducted, and p-values were reported.
To investigate whether parental risky health behaviors could be transmitted and how these behaviors were transmitted, we adopted a binary choice model for panel data with random-effect specification after conducting the Hausman test (psmoking= 1.000, palcohol= 0.9043, pSSBs= 0.7745). Odds ratios (ORs) with their p-values are reported. The model is specified as follows:
where Pi,t represents the probability of children's smoking, alcohol drinking, and SSBs drinking behaviors; FatherBehaviori,t/MotherBehaviori indicates whether the child i's father/mother had this kind of risky health behavior, including smoking, alcohol drinking, and SSBs drinking; FatherSESij,t/MotherSESij,t represents the child i's father/mother's SES; Wavei,t indicates the time dummies to explore the dynamic evolution from 1993 to 2015; Areai,t indicates the region dummies to explore the region's effects on children's risky health behaviors; Genderi,t and Agei,t represent the child i's gender and age individually. ui,t represent the individual effects on the child. We used the model above to analyze the total sample, the urban sample, and the rural sample.
To understand the influence of different SES variables on the intergenerational transmission of risky health behaviors, we grouped urban and rural parents according to their education level, income, and occupation type, used model (1) for regression in different subgroups, and drew a bar chart with confidence intervals. Regarding parental education level, we divided parents into low-level ( ≤ 6 years) and high-level (>6 years) education subgroups. Regarding income, those with an income equal to or lower than the average were included in the low-income subgroup, whereas those with an income higher than the average were included in the high-income subgroup. Finally, we divided occupations into manual labor and non-manual labor subgroups and then conducted a subgroup analysis. To test the differences in the coefficients FatherBehaviori,t and MotherBehaviori among different subgroups, a SUEST was used.
The variables used in this study are displayed in Table 1 and include the entire sample, as well as the risky health behavior and non-risky health behavior samples.
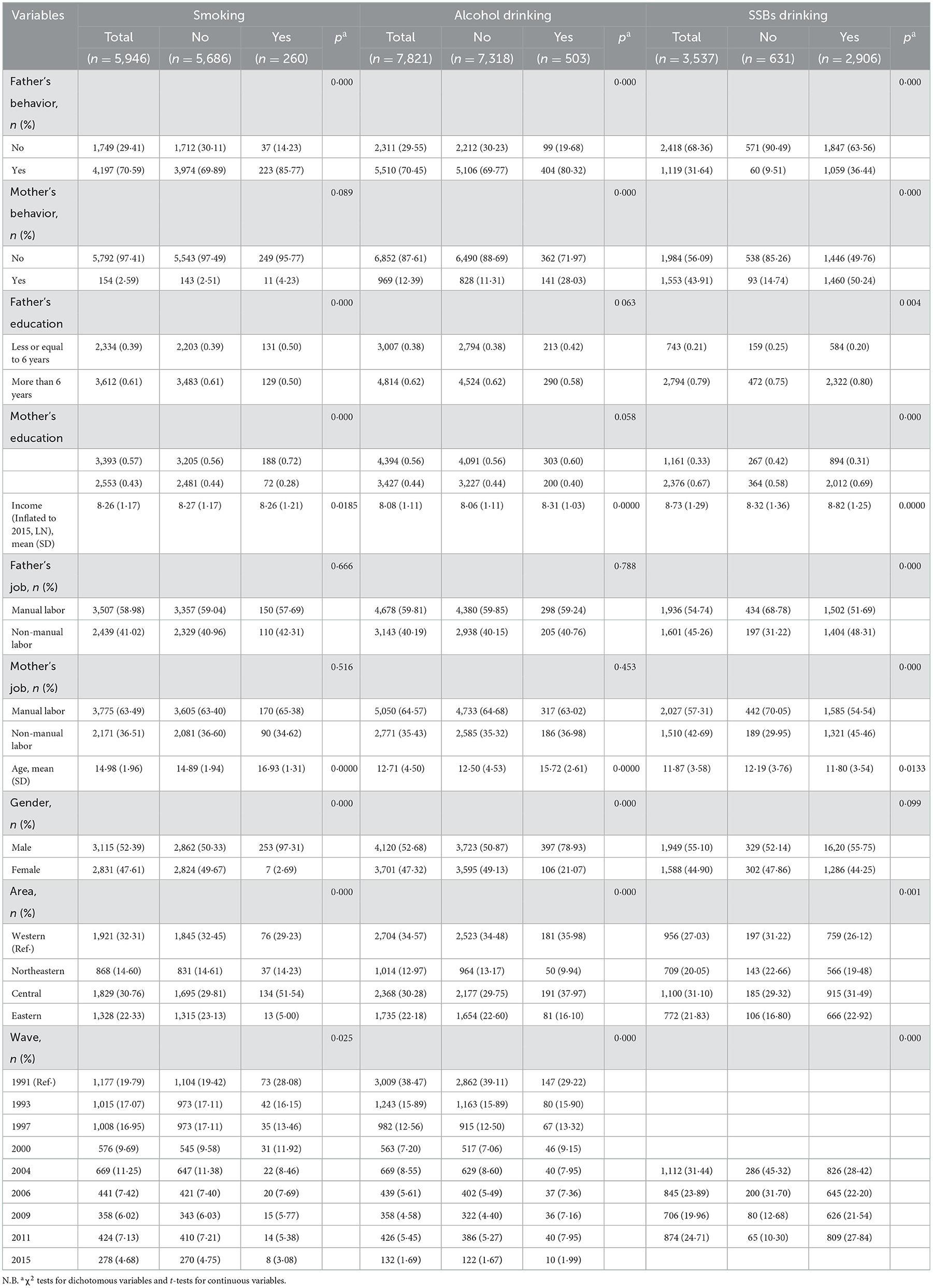
Table 1. Descriptive statistics.
The prevalence of smoking, alcohol consumption, and SSBs consumption in children was 4.37, 6.43, and 82.16%, respectively. Boys had significantly higher proportions of these three risky health behaviors than girls. Children who smoked and drank alcohol were significantly older than those who did not smoke and drink alcohol, while those drinking SSBs were significantly younger than those who did not drink SSBs.
Both fathers and mothers of smoking children had higher smoking rates, while the difference in mothers' smoking rates between smoking and non-smoking children was not significant. Both fathers and mothers of children who drank alcohol had a significantly higher rate of alcohol consumption than those who did not drink alcohol. Similarly, among children who drank SSBs, both fathers and mothers had a significantly higher ratio of drinking SSBs than the fathers and mothers of children who did not drink SSBs.
The results of the logistic regression for intergenerational transmission of risky parental health behaviors in Chinese children are presented in Table 2. In the total sample, after controlling for confounding variables, children who had a smoking father were ~240.9% more likely to smoke (p < 0.01) than children who had a non-smoking father. While the intergenerational transmission of fathers' smoking behavior was observed among rural children, the intergenerational transmission effect was even more pronounced among urban children; smoking fathers increased the probability of children smoking by 2,506% (p = 0.034). Considering the unreliability of the small sample size on mothers' smoking, maternal smoking transmission is not reported here.
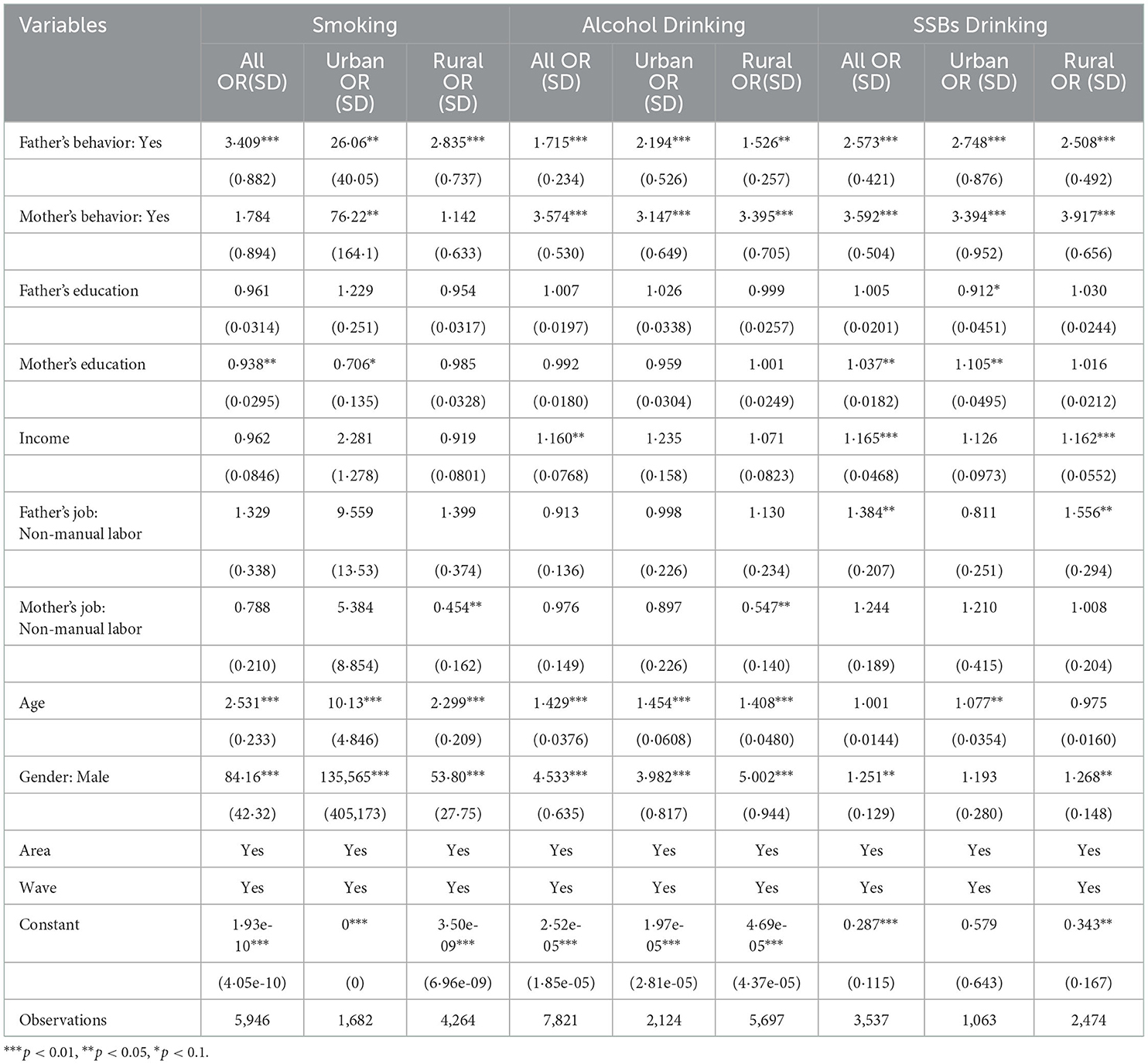
Table 2. Results of random-effect logistic regression.
Similarly, to smoking fathers, fathers who drank alcohol increased the possibility of alcohol drinking in their children by 71.5% (p < 0.01) in the total sample, 119.4% (p = 0.01) in the urban sample, and 52.6% (p = 0.012) in the rural sample. Mother's alcohol consumption increased the possibility of alcohol consumption by 257.4% (p < 0.01) in the total sample, 214.7% (p < 0.01) in the urban sample, and 239.5% (p < 0.01) in the rural sample.
Likewise, in the total sample, children whose fathers drank SSBs were ~161.2% more likely to drink SSBs (p < 0.01) than children whose fathers did not drink SSBs. Indeed, SSBs drinking could increase the likelihood of children consuming SSBs by 259.2% (p < 0.01). A similar intergenerational transmission of this behavior was observed in both urban and rural children. Gender plays an important role in the intergenerational transmission of risky health behaviors. Boys were ~8,316, 353.3, and 25.1% more likely to smoke, drink alcohol, and drink SSBs, respectively, than girls. Furthermore, age also plays an important role in the intergenerational transmission of smoking and alcohol consumption. Similar effects were observed in both urban and rural children.
Various parental SES variables were also shown to significantly affect children's behavior. A higher parental per capita income was shown to make both urban and rural children more likely to drink alcohol and SSBs. However, the effects of educational attainment and occupational status were not consistent or even opposite between urban and rural areas and between parents.
To further clarify the intergenerational transmission of urban and rural parental risky health behaviors between SES groups, the results of the subgroup analysis and SUEST are shown in Table 3, Figures 1, 2. Considering the unreliability of the subgroup analysis due to the small sample size of mothers' smoking, maternal smoking transmission between different SES groups is not reported here.
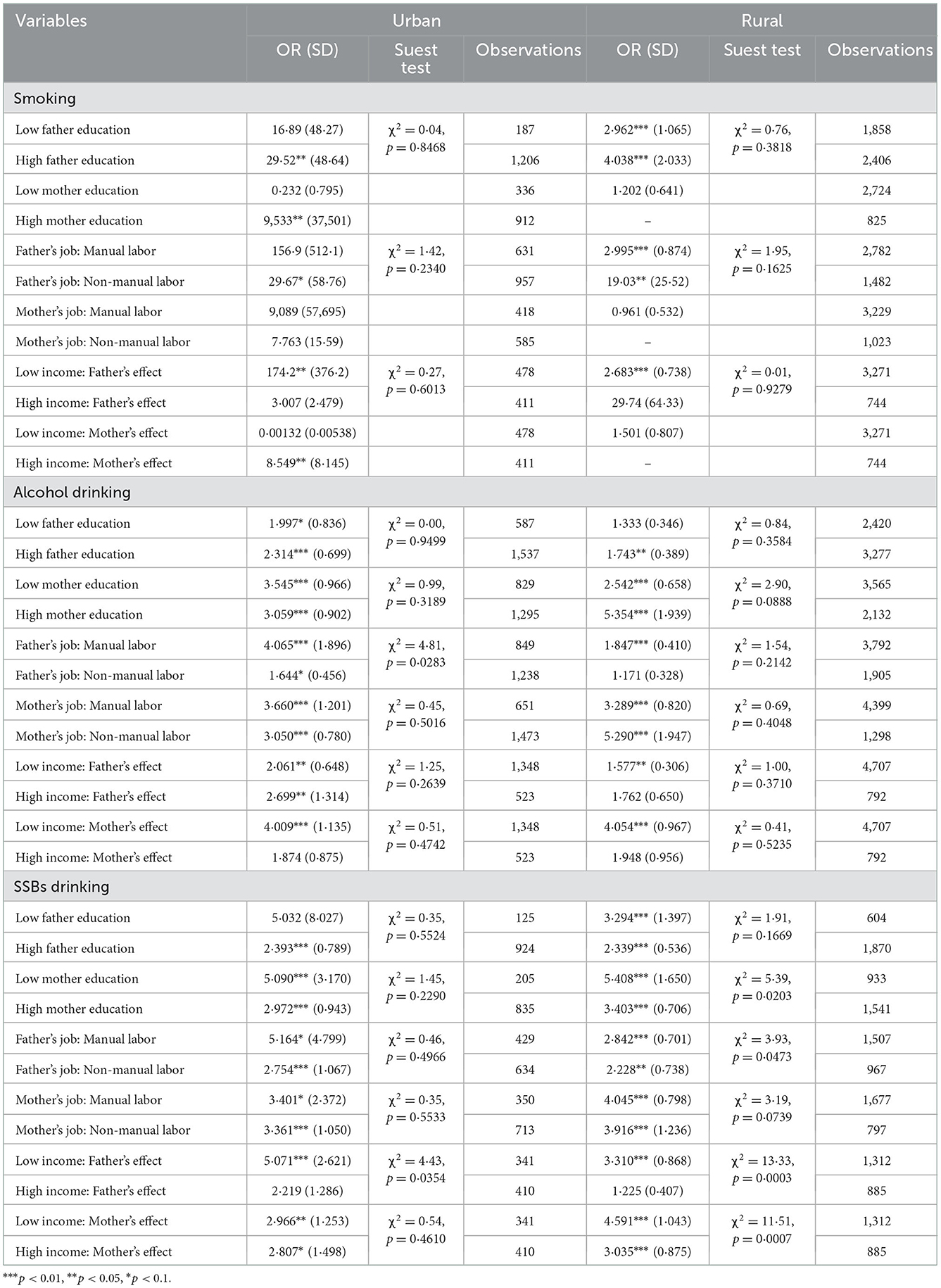
Table 3. Subgroup analysis of intergenerational transmission with different SES.
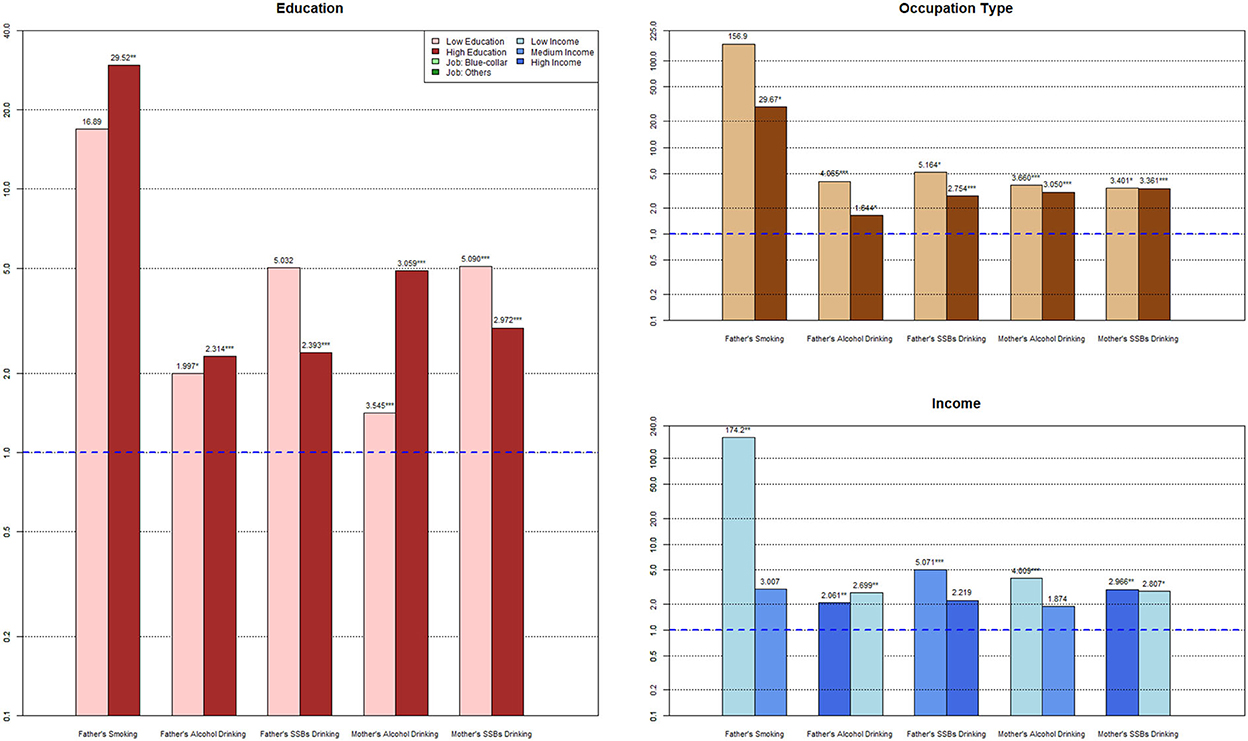
Figure 1. Subgroup analysis for urban families.
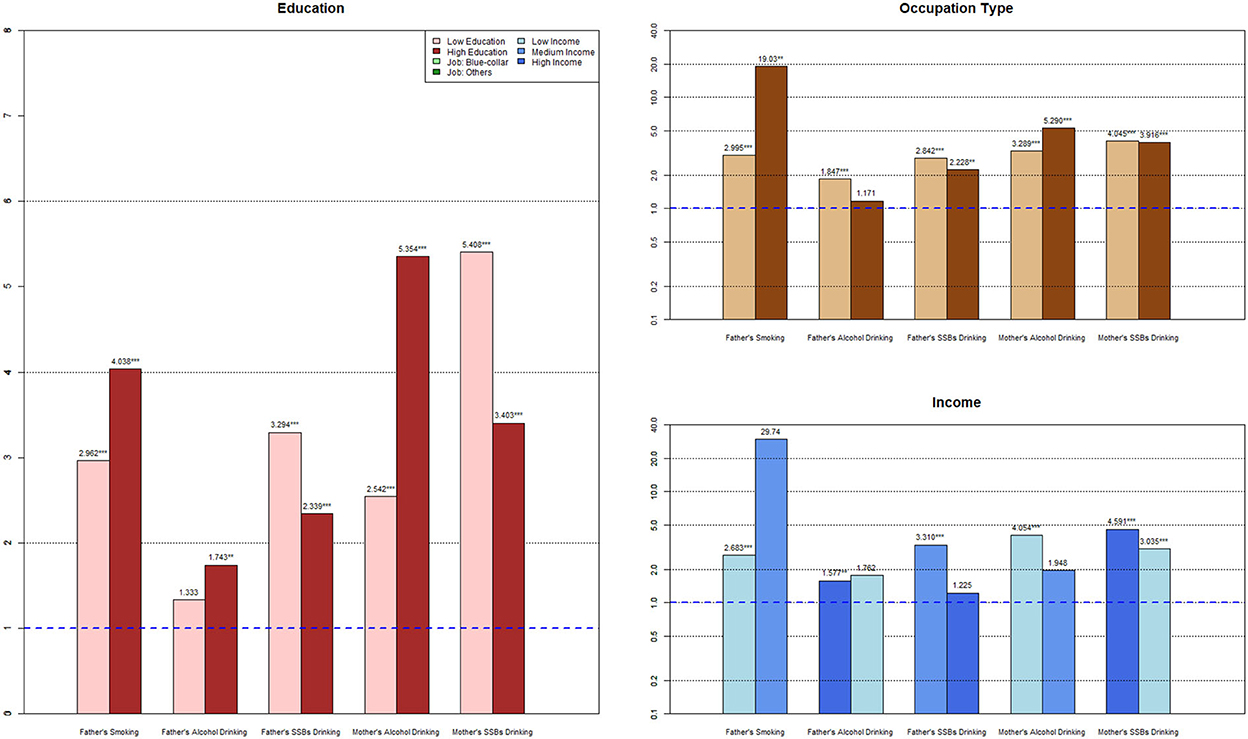
Figure 2. Subgroup analysis for rural families.
The higher the father's education level, the more significant the intergenerational transmission of smoking (ORLowEdu = 16.89, ORHighEdu = 29.52) and alcohol drinking (ORLowEdu = 1.997, ORHighEdu = 2.314); however, the OR of SSBs drinking dropped from 5.302 to 2.393, in the low education vs. the high education group, respectively. From low education level to high education level, the OR of the mother's alcohol drinking behavior decreased from 3.545 to 3.509, and the OR of maternal SSBs drinking decreased from 5.090 to 2.972, with insignificant differences in coefficients between the maternal low education and high education groups.
Fathers in the manual labor group had a more significant intergenerational transmission of smoking (ORManuallabor = 156.9, ORNon − manuallabor = 29.67), alcohol drinking (ORManuallabor = 4.065, ORNon − manuallabor = 1.644), and SSBs drinking (ORManuallabor = 5.164, ORNon − manuallabor = 2.754) than fathers in the non-manual labor group. Non-manual labor mothers showed significantly fewer intergenerational transmission effects of alcohol drinking (ORManuallabor = 3.660, ORNon − manuallabor = 3.050) and SSBs drinking (ORManuallabor= 3.401, ORNon − manuallabor = 3.361).
With an increase in income, fathers' intergenerational transmission effect of smoking and SSBs consumption became weaker and insignificant (ORLowInc = 174.2, ORHighInc = 3.007; ORLowInc = 5.071, ORHighInc = 2.219). In contrast, the transmission effect of fathers' wine drinking behavior became stronger (ORLowInc = 2.061, ORHighInc = 2.699) as income increased. Both mother's alcohol drinking behavior (ORLowInc = 4.009, ORHighInc = 1.874) and SSBs drinking behavior (ORLowInc = 2.966, ORHighInc = 2.807) decreased from the low-income to the high-income group.
With the rise in paternal education level, intergenerational transmission of fathers' smoking (ORLowEdu = 2.962, ORHighEdu = 4.038) and alcohol drinking (ORLowEdu = 1.333, ORHighEdu = 1.743) increased, but the OR of fathers' SSBs drinking behavior dropped from 3.294 to 2.339. The OR of highly educated mothers' alcohol drinking behavior increased from 2.542 to 5.354, and that of maternal SSBs drinking reduced from 5.408 to 3.403, with significant coefficient differences (palcoholofSUEST = 0.0888; pssbsofSUEST = 0.0203) than mothers in the low-education group.
Smoking in fathers in non-manual labor jobs had a stronger effect on children's formation of this behavior (ORManuallabor = 2.995, ORNon − manuallabor = 19.03) than in fathers in manual labor jobs. Meanwhile, –labored fathers were less connected with children's alcohol drinking (ORManuallabor = 1.847, ORNon − manuallabor = 1.171) and SSBs drinking (ORManuallabor = 2.842, ORNon − manuallabor = 2.228). Furthermore, mothers in non-manual labor jobs showed significantly lower effects on children's alcohol drinking (ORManuallabor = 3.289, ORNon − manuallabor = 5.290) and SSBs drinking (ORManuallabor = 4.045, ORNon − manuallabor= 3.916) than mothers in manual labor jobs.
With an increase in income, the father's intergenerational transmission effect of smoking became stronger (ORLowInc = 2.683, ORHighInc = 29.74), with a similar effect being observed for fathers' wine drinking behavior (ORLowInc = 1.577, ORHighInc = 1.762). On the contrary, the influence of fathers' SSBs drinking behavior on their children's behavior went through a process of weakening as income increased (ORLowInc = 3.310, ORHighInc = 1.225), and the coefficient difference was significant (p-values ofSUEST = 0.0003). Both mother's alcohol drinking behavior (ORLowInc = 4.054, ORHighInc =1.948) and SSBs drinking behavior (ORLowInc = 4.591, ORHighInc = 3.035) decreased from the low-income to the high-income group (pssbsofSUEST = 0.0007), whereas other subgroups did not.
This study has three central findings: (1) risky health behaviors had significant intergenerational transmission effects; (2) the intergenerational transmission of mothers' alcohol consumption and SSBs drinking behavior was greater than that of fathers; and (3) the influence of SES on intergenerational transmission in urban areas was different from that of rural children. For addictive behaviors, such as alcohol drinking and smoking, intergenerational transmission mostly exhibited a decreasing trend with increasing SES in urban families but increased with increasing SES for rural families. However, the influence of parental SSBs drinking behaviors showed a consistent decreasing trend with increasing SES for both urban and rural families.
This study showed that, consistent with many previous findings (25, 29–39, 46, 48–50, 62), risky parental health behaviors have a significant risk of being transmitted to their children. It is usually easy for children to imitate their parents' behaviors even if they are negative or unhealthy (25–28, 63, 64), and, therefore, parents' words and deeds are very important in preventing risky health behaviors in children.
Importantly, differences between paternal and maternal influences were also observed. Contrary to many previous studies (25, 29, 32, 33, 65, 66), we found that fathers' smoking behavior had a more significant effect on leading children's smoking behavior than mothers. This may be because the sample size of maternal smokers in this study was too small to make good statistical inferences than previous studies. However, when it came to alcohol drinking and SSBs drinking, the impact of both these behaviors on children was significantly higher from mothers than from fathers, which was consistent with some previous research (29, 49, 61). This may be because mothers generally spend more time with their children than fathers. Therefore, children could be more affected by their mother's behavior than their father's (29, 49, 61).
The role of parental SES in the intergenerational transmission of risky health behaviors in urban and rural children was not exactly the same. In general, there was a significant decrease in the intergenerational transmission of SSBs drinking behavior with increasing SES: the risky health behavior transmission effect of high-SES parents was weaker than that of low-SES parents, and SUEST showed that only the education level of fathers in rural areas had no significant differences between groups, while only fathers' income level had significant differences between groups in urban areas. We also noted that the intergenerational transmission effect of urban mothers' drinking behavior tended to decrease when all three SES variables increased, but rural mothers' alcohol drinking behavior had a similar changing trend with the rise in education level and occupational class. However, SUEST showed that only the education levels of mothers in rural areas differed significantly between the subgroups. A similar situation occurred among fathers: rural fathers' risky health behaviors mainly appeared to show a similar changing trend with SES, while urban fathers' smoking had a reverse changing trend with the rise in occupational type and income. However, SUEST showed that there were significant inter-subgroup differences in the occupation types of fathers in urban areas, but there were no significant differences between the other subgroups.
This reflected that SES had a dual influence on the intergenerational transmission of risky parental health behavior. On the one hand, higher SES means better family capital and better parenting style, which will prevent the formation of children's unhealthy behaviors and reduce the transmission of these behaviors from their parents (26, 27, 30, 41, 42, 49, 67–71). High-SES parents were usually well aware of the dangers of risky health behavior and were therefore inclined to discourage their children from these behaviors, while low-SES parents often did not care whether their children engaged in these behaviors or even engaged in these behaviors in front of their children, setting a bad example for their children and leading them to engage in these behaviors (27, 41, 42, 67, 70–72). Some facts support the standpoint that higher SES can promote people's health and healthy behaviors. In the health model presented by Grossman, more affluent families tend to spend more money on healthcare, such as better-quality medical care and healthy food (40, 68, 71). Well-educated parents are more inclined to adopt healthy behaviors, both for themselves and their children, so the incidence of risky health behaviors among children is lower (68, 69, 71). In addition to the fact that education can lead to a better knowledge of the importance of promoting healthy behaviors, there were also potential indirect effects, such as smoother ways to get a job, better affordability of health-improving goods, less stress, and better work environments due to high-SES parents also being exposed to healthier colleagues (35, 43, 71). However, lower-SES people may care less about their health and that of their family members, be less responsive to health promotion, receive less information about how to get healthy, and have limited access to health promotion services (34, 67, 70). Similar effects of low-SES have been observed in risky health behaviors, such as SSBs consumption, which mainly exists in children and adolescents.
On the contrary, however, higher SES can mean that parents will devote more time to their own careers to cope with higher workloads (53), more often ignoring messages they received, hiring nannies or, in Chinese traditional culture, asking for support from their own retired parents, who are often less educated, leading to the absence of family education. Children with high-SES parents tend to have more disposable pocket money, which makes it easier for them to access substances that pose health risks, such as SSBs and wine (73). All of these factors may increase the risk of unhealthy behaviors in children. If the degree of intergenerational transmission is more severe than that of rural and low SES parents, the effect of parents' actions is greater than the effect of their words, which may promote intergenerational transmission of risky health behaviors in children. This may be because high-SES parents tend to have a higher status in their children's minds, and children are more likely to imitate risky parental health behaviors (25, 74). In our sample, for traditional rational addictive behaviors such as smoking and alcohol drinking, higher parental occupation and education level could enhance intergenerational transmission, which is an example of the effect of their actions being greater than that of their words. This shows the necessity and importance of behavioral changes starting with the parents.
We observed that parents played an important role in the development of risky health behaviors in children. Risky parental health behaviors set a bad example for their children and tempt children to imitate their parents' behaviors. It is worth noting that urban areas, especially urban mothers, mostly reflected the positive effects of SES, whereas fathers, especially those in rural areas, reflected adverse effects. This suggests that we should pay more attention to fathers' behaviors and awareness of health education in rural areas and invest in the rearing of their children. In addition to persuading children to drop these behaviors, more attention should be paid to reducing intergenerational transmission.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Data for this study was from the China Health and Nutrition Survey (CHNS). CHNS was approved by the Institutional Review Committees of the University of North Carolina at Chapel Hill and the National Institute of Nutrition and Food Safety, Chinese Center for Disease Control and Prevention.
ZY and JL conceptualized and designed the study, participated in explaining the data, and writing and revising the manuscript. ZY analyzed the data. WQ helped to revise the manuscript. All authors approved the final version of the paper and have directly accessed and verified the underlying data reported in the manuscript.
This work was supported by the Humanities and Social Science Foundation of the Ministry of Education, China, No. 21YJC630060 and the National Natural Science Foundation of China [Grant Numbers 71673170 and 71303137].
This research uses data from the China Health and Nutrition Survey (CHNS). We are grateful to research grant funding from the National Institute for Health (NIH), the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) for R01 HD30880, the National Institute on Aging (NIA) for R01 AG065357, the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) for R01DK104371 and R01HL108427, the NIH Fogarty grant D43 TW009077 since 1989, and the China-Japan Friendship Hospital, Ministry of Health for support for CHNS 2009, Chinese National Human Genome Center at Shanghai since 2009, and Beijing Municipal Center for Disease Prevention and Control since 2011. We thank the National Institute for Nutrition and Health, China Center for Disease Control and Prevention, Beijing Municipal Center for Disease Control and Prevention, and the Chinese National Human Genome Center in Shanghai.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.842817/full#supplementary-material
CHNS, China Health and Nutrition Survey; SSB, sugar-sweetened beverage; SES, socioeconomic status; SUEST, Seemingly Unrelated Estimation Test; OR, odds ratio.
1. Currie C, Roberts C, Settertobulte W, Morgan A, Smith R, Samdal O, Barnekow Rasmussen V. Young People's Health in Context: Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2001/2002 Survey. Copenhagen: WHO Regional Office for Europe (2004).
2. Escobedo LG, Anda RF, Smith PF, Remington PL, Mast EE. Sociodemographic characteristics of cigarette smoking initiation in the United States: implications for smoking prevention policy. JAMA. (1990) 264:1550–5. doi: 10.1001/jama.264.12.1550
3. Marmot MG, Kogevinas M, Elston MA. Social/economic status and disease. Annu Rev Public Health. (1987) 8:111–35. doi: 10.1146/annurev.pu.08.050187.000551
4. Winkleby MA, Fortmann SP, Barrett DC. Social class disparities in risk factors for disease: eight-year prevalence patterns by level of education. Prevent Med. (1990) 19:1–12. doi: 10.1016/0091-7435(90)90001-Z
5. Kann L, McManus T, Harris WA, Shanklin SL, Flint KH, Queen B, et al. Youth risk behavior surveillance - United States, 2017. MMWR Surveill Summ. (2018) 67:1–114. doi: 10.15585/mmwr.ss6708a1
6. Collaborators GRF. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1223–49. doi: 10.1016/S0140-6736(20)30752-2
7. Catalano RF, Fagan AA, Gavin LE, Greenberg MT, Irwin CE, Ross DA, et al. Worldwide application of prevention science in adolescent health. Lancet. (2012) 379:1653–64. doi: 10.1016/S0140-6736(12)60238-4
8. Chowdhury P, Balluz L, Town M, Chowdhury FM, Bartoli W, Garvin W, et al. Surveillance of certain health behaviors and conditions among states and selected local areas—Behavioral Risk Factor Surveillance System, United States, 2007. Morbidity Mortality Weekly Rep Surveillance Summaries. (2010) 59:1–220. Available online at: http://www.jstor.org/stable/24805766
9. Jefferis BJ, Power C, Graham H, Manor O. Effects of childhood socioeconomic circumstances on persistent smoking. Am J Public Health. (2004) 94:279–85. doi: 10.2105/AJPH.94.2.279
10. Underwood JM, Brener N, Thornton J, Harris WA, Bryan LN, Shanklin SL, et al. Overview and methods for the youth risk behavior surveillance system—United States, 2019. MMWR Supplem. (2020) 69:1. doi: 10.15585/mmwr.su6901a1
11. Kowalski AJ, Addo OY, Kramer MR, Martorell R, Norris SA, Waford RN, et al. Initial engagement and persistence of health risk behaviors through adolescence: longitudinal findings from urban South Africa. BMC Pediatr. (2021) 21:31. doi: 10.1186/s12887-020-02486-y
12. Hanson MD, Chen E. Socioeconomic status and health behaviors in adolescence: a review of the literature. J Behav Med. (2007) 30:263. doi: 10.1007/s10865-007-9098-3
13. World Health Organization. WHO Global Report on Trends in Prevalence of Tobacco Use 2000–2025. Geneva: World Health Organization (2019).
14. World Health Organization. Global Status Report on alcohol and Health 2018. Geneva: World Health Organization (2019).
15. Gui Z-H, Zhu Y-N, Cai L, Sun F-H, Ma Y-H, Jing J, et al. Sugar-sweetened beverage consumption and risks of obesity and hypertension in Chinese children and adolescents: a national cross-sectional analysis. Nutrients. (2017) 9:1302. doi: 10.3390/nu9121302
16. Kit BK, Fakhouri TH, Park S, Nielsen SJ, Ogden CL. Trends in sugar-sweetened beverage consumption among youth and adults in the United States: 1999–2010. Am J Clin Nutr. (2013) 98:180–8. doi: 10.3945/ajcn.112.057943
17. Russo RG, Northridge ME, Wu B, Yi SS. Characterizing sugar-sweetened beverage consumption for us children and adolescents by race/ethnicity. J Racial Ethn Health Disparities. (2020) 7:1100–16. doi: 10.1007/s40615-020-00733-7
18. Gan Q, Xu P, Yang T, Cao W, Xu J, Li L, Pan H, Zhao W, Zhang Q. Sugar-sweetened beverage consumption status and its association with childhood obesity among Chinese children aged 6–17 years. Nutrients. (2021) 13:2211. doi: 10.3390/nu13072211
19. Association AP. Diagnostic and statistical manual for mental disorders. DSM-IIIR 精神障害の分類と診断の手引. (1987) 21:3–24.
20. World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organization (1992).
21. DiNicolantonio JJ, O'Keefe JH, Wilson WL. Sugar addiction: is it real? A narrative review. Br J Sports Med. (2018) 52:910–3. doi: 10.1136/bjsports-2017-097971
22. Falbe J, Thompson HR, Patel A, Madsen KA. Potentially addictive properties of sugar-sweetened beverages among adolescents. Appetite. (2019) 133:130–7. doi: 10.1016/j.appet.2018.10.032
23. Smith DG, Robbins TW. The neurobiological underpinnings of obesity and binge eating: a rationale for adopting the food addiction model. Biol Psychiatry. (2013) 73:804–10. doi: 10.1016/j.biopsych.2012.08.026
24. Jastreboff AM, Sinha R, Arora J, Giannini C, Kubat J, Malik S, et al. Altered brain response to drinking glucose and fructose in obese adolescents. Diabetes. (2016) 65:1929–39. doi: 10.2337/db15-1216
25. Pan J, Han W. Exploring the intergenerational persistence of health behaviour: an empirical study of smoking from China. BMC Public Health. (2017) 17:1–9. doi: 10.1186/s12889-017-4480-8
26. Cox MJ, Janssen T, Lopez-Vergara H, Barnett NP, Jackson KM. Parental drinking as context for parental socialization of adolescent alcohol use. J Adolesc. (2018) 69:22–32. doi: 10.1016/j.adolescence.2018.08.009
27. Bradshaw M, Kent BV, Davidson JC, De Leon S. Parents, peers, and trajectories of cigarette smoking: a group-based approach. Youth Soc. (2021) 53:676–94. doi: 10.1177/0044118X19862450
28. Gottfredson NC, Hussong AM, Ennett ST, Rothenberg WA. The role of parental engagement in the intergenerational transmission of smoking behavior and identity. J Adolesc Health. (2017) 60:599–605. doi: 10.1016/j.jadohealth.2016.11.004
29. Brion M-J, Victora C, Matijasevich A, Horta B, Anselmi L, Steer C, et al. Maternal smoking and child psychological problems: disentangling causal and non-causal effects. Pediatrics. (2010) 126:e57–65. doi: 10.1542/peds.2009-2754
30. Flores G, Lin H. Factors predicting severe childhood obesity in kindergarteners. Int J Obes. (2013) 37:31–9. doi: 10.1038/ijo.2012.168
31. Göhlmann S, Schmidt CM, Tauchmann H. Smoking initiation in Germany: the role of intergenerational transmission. Health Econ. (2010) 19:227–42. doi: 10.1002/hec.1470
32. Melchior M, Chastang J-F, Mackinnon D, Galéra C, Fombonne E. The intergenerational transmission of tobacco smoking—the role of parents' long-term smoking trajectories. Drug Alcohol Depend. (2010) 107:257–60. doi: 10.1016/j.drugalcdep.2009.10.016
33. Rainio SU, Rimpelä AH, Luukkaala TH, Rimpelä MK. Evolution of the association between parental and child smoking in Finland between 1977 and 2005. Prevent Med. (2008) 46:565–71. doi: 10.1016/j.ypmed.2008.01.011
34. Degirmenci N, Fossum IN, Strand TA, Vaktskjold A, Holten-Andersen MN. Consumption of energy drinks among adolescents in Norway: a cross-sectional study. BMC Public Health. (2018) 18:1391. doi: 10.1186/s12889-018-6236-5
35. Jahnel T, Ferguson SG, Shiffman S, Thrul J, Schüz B. Momentary smoking context as a mediator of the relationship between SES and smoking. Addict Behav. (2018) 83:136–41. doi: 10.1016/j.addbeh.2017.12.014
36. Vargas-Martínez AM, Trapero-Bertran M, Mora T, Lima-Serrano M. Social, economic and family factors associated with binge drinking in Spanish adolescents. BMC Public Health. (2020) 20:519. doi: 10.1186/s12889-020-08605-9
37. Usidame B, Hirschtick JL, Mattingly DT, Patel A, Patrick ME, Fleischer NL. Sociodemographic patterns of exclusive and dual combustible tobacco and e-cigarette use among US adolescents-a nationally representative study (2017–2020). Int J Environ Res Public Health. (2022) 19:2965. doi: 10.3390/ijerph19052965
38. Pape H, Norström T, Rossow I. Adolescent drinking-a touch of social class? Addiction. (2017) 112:792–800. doi: 10.1111/add.13721
39. Kitano N, Shiroyama T, Suzuki K, Yamano T, Tomiyama M, Ueno M, et al. Association of household smoking status in childhood with young adults' educational attainment and smoking status: results from a series of population-based cross-sectional surveys in Japan. Prev Med Rep. (2020) 18:101066. doi: 10.1016/j.pmedr.2020.101066
40. Grossman M. Chapter 7—The Human Capital Model* *I am indebted to Robert Kaestner, Sara Markowitz, Tomas Philipson, and Walter Ried for helpful comments. In: Culyer AJ, ed Handbook of Health Economics, Vol 1. Newhouse JP: Elsevier (2000). p. 347–408. doi: 10.1016/S1574-0064(00)80166-3
41. Hiemstra M, de Leeuw RN, Engels RC, Otten R. What parents can do to keep their children from smoking: a systematic review on smoking-specific parenting strategies and smoking onset. Addict Behav. (2017) 70:107–28. doi: 10.1016/j.addbeh.2017.02.003
42. Hiscock R, Bauld L, Amos A, Fidler JA, Munafò M. Socioeconomic status and smoking: a review. Ann N Y Acad Sci. (2012) 1248:107–23. doi: 10.1111/j.1749-6632.2011.06202.x
43. Cutler DM, Lleras-Muney A. Understanding differences in health behaviors by education. J Health Econ. (2010) 29:1–28. doi: 10.1016/j.jhealeco.2009.10.003
44. Kendler KS, Gardner CO, Edwards A, Hickman M, Heron J, Macleod J, et al. Dimensions of parental alcohol use/problems and offspring temperament, externalizing behaviors, and alcohol use/problems. Alcoholism Clin Exp Res. (2013) 37:2118–27. doi: 10.1111/acer.12196
45. Cockerham WC. Health lifestyle theory and the convergence of agency and structure. J Health Soc Behav. (2005) 46:51–67. doi: 10.1177/002214650504600105
46. Almquist YB, Bishop L, Gustafsson N-K, Berg L. Intergenerational transmission of alcohol misuse: mediation and interaction by school performance in a Swedish birth cohort. J Epidemiol Commun Health. (2020) 74:598–604. doi: 10.1136/jech-2019-213523
47. De Coen V, Vansteelandt S, Maes L, Huybrechts I, De Bourdeaudhuij I, Vereecken C. Parental socioeconomic status and soft drink consumption of the child. The mediating proportion of parenting practices. Appetite. (2012) 59:76–80. doi: 10.1016/j.appet.2012.03.024
48. Mays D, Gilman SE, Rende R, Luta G, Tercyak KP, Niaura RS. Parental smoking exposure and adolescent smoking trajectories. Pediatrics. (2014) 133:983–91. doi: 10.1542/peds.2013-3003
49. Ren Y, Zhang Y, Campos BC, Loy J-P. Unhealthy consumption behaviors and their intergenerational persistence: the role of education. China Econ Rev. (2020) 62:101208. doi: 10.1016/j.chieco.2018.08.004
50. Wickrama KA, Conger RD, Wallace LE, Elder Jr GH. The intergenerational transmission of health-risk behaviors: adolescent lifestyles and gender moderating effects. J Health Social Behav. (1999) 40:258–72. doi: 10.2307/2676351
51. Kerr DCR, Tiberio SS, Capaldi DM, Owen LD. Intergenerational congruence in adolescent onset of alcohol, tobacco, and marijuana use. Psychol Addict Behav. (2020) 34:839–51. doi: 10.1037/adb0000546
52. Bauldry S, Shanahan MJ, Macmillan R, Miech RA, Boardman JD. D OD, Cole V. Parental and adolescent health behaviors and pathways to adulthood. Soc Sci Res. (2016) 58:227–42. doi: 10.1016/j.ssresearch.2016.02.006
53. Van den Branden S, Van den Broucke S, Leroy R, Declerck D, Hoppenbrouwers K. Oral health and oral health-related behaviour in preschool children: evidence for a social gradient. Eur J Pediatr. (2013) 172:231–7. doi: 10.1007/s00431-012-1874-6
54. Yu X, Abler D. Interactions between cigarette and alcohol consumption in rural China. Eur J Health Econ. (2010) 11:151–60. doi: 10.1007/s10198-009-0157-2
55. Pape H, Rossow I, Andreas JB, Norström T. Social class and alcohol use by youth: different drinking behaviors, different associations? J Stud Alcohol Drugs. (2018) 79:132–6. doi: 10.15288/jsad.2018.79.132
56. Wu Y. China's consumer revolution. In: The Oxford Companion to the Economics of China. Oxford Academic Press (2014). p. 85–9. doi: 10.1093/acprof:oso/9780199678204.003.0012
57. Fan Y, Li Y. Children's buying behaviour in China: a study of their information sources. Market Intell Plan. (2010) 28:170–87. doi: 10.1108/02634501011029673
58. Rahman O, Chen X, Au R. Consumer behaviour of pre-teen and teenage youth in China. J Global Fashion Market. (2013) 4:247–65. doi: 10.1080/20932685.2013.817141
59. Zhou N, Cheah CSL Li Y, Liu J, Sun S. The role of maternal and child characteristics in Chinese children's dietary intake across three groups. J Pediatr Psychol. (2017) 43:503–12. doi: 10.1093/jpepsy/jsx131
60. Fu J, Liang F, Wang Y, Qiu N, Ding K, Zeng J, et al. Modeling parental influence on food consumption among Chinese adolescents through self-efficacy: a path analysis. Nutrients. (2021) 13:4454. doi: 10.3390/nu13124454
61. Zhuang X, Liu Y, Gittelsohn J, Lewis E, Song S, Ma Y, et al. Sugar-sweetened beverages consumption and associated factors among northeastern Chinese children. Nutrients. (2021) 13:2233. doi: 10.3390/nu13072233
62. Ikram UZ, Snijder MB, Derks EM, Peters RJG, Kunst AE, Stronks K. Parental smoking and adult offspring's smoking behaviors in ethnic minority groups: an intergenerational analysis in the HELIUS study. Nicotine Tob Res. (2018) 20:766–74. doi: 10.1093/ntr/ntx137
63. Loureiro ML. Sanz-de-Galdeano A, Vuri D. Smoking habits: like father, like son, like mother, like daughter? Oxford Bull Econ Stat. (2010) 72:717–43. doi: 10.1111/j.1468-0084.2010.00603.x
64. O'Loughlin J, Karp I, Koulis T, Paradis G, DiFranza J. Determinants of first puff and daily cigarette smoking in adolescents. Am J Epidemiol. (2009) 170:585–97. doi: 10.1093/aje/kwp179
65. Nakagawa S, Takahashi Y, Nakayama T, Muro S, Mishima M, Sekine A, et al. Gender differences in smoking initiation and cessation associated with the intergenerational transfer of smoking across three generations: the nagahama study. Int J Environ Res Public Health. (2022) 19:1511. doi: 10.3390/ijerph19031511
66. Chadi N, Ahun MN, Laporte C, Boivin M, Tremblay RE, Côté SM, et al. Pre- and postnatal maternal smoking and offspring smoking trajectories: Evidence from a 20-year birth cohort. Prev Med. (2021) 147:106499. doi: 10.1016/j.ypmed.2021.106499
67. Cai L, Cui W, He J, Wu X. The economic burden of smoking and secondhand smoke exposure in rural South-West China. J Asthma. (2014) 51:515–21. doi: 10.3109/02770903.2014.892964
68. Currie J, Goodman J. Parental socioeconomic status, child health, and human capital. Int Encycl Edu. (2010) 2:239–48. doi: 10.1016/B978-0-12-815391-8.00018-5
69. Grossman M. Chapter 10 education and nonmarket outcomes. In: Hanushek E, Welch F, eds Handbook of the Economics of Education. Volume 1. Amsterdam: Elsevier (2006). p. 577–633. doi: 10.1016/S1574-0692(06)01010-5
70. Yang T, Li F, Yang X, Wu Z, Feng X, Wang Y, et al. Smoking patterns and sociodemographic factors associated with tobacco use among Chinese rural male residents: a descriptive analysis. BMC Public Health. (2008) 8:1–7. doi: 10.1186/1471-2458-8-248
71. de Buhr E, Tannen A. Parental health literacy and health knowledge, behaviours and outcomes in children: a cross-sectional survey. BMC Public Health. (2020) 20:1096. doi: 10.1186/s12889-020-08881-5
72. Wardle J, Jarvis M, Steggles N, Sutton S, Williamson S, Farrimond H, et al. Socioeconomic disparities in cancer-risk behaviors in adolescence: baseline results from the Health and Behaviour in Teenagers Study (HABITS). Prevent Med. (2003) 36:721–30. doi: 10.1016/S0091-7435(03)00047-1
73. Ma L, Fang Z, Gao L, Zhao Y, Xue H, Li K, Wang Y. A 3-year longitudinal study of pocket money, eating behavior, weight status: the childhood obesity study in China mega-cities. Int J Environ Res Public Health. (2020) 17:9139. doi: 10.3390/ijerph17239139
Keywords: intergenerational transmission, risky health behaviors, socioeconomic status, socioeconomic differences, CHNS
Citation: Yu Z, Qin W and Li J (2023) Intergenerational transmission of parental risky health behaviors in Chinese children: Are there socioeconomic status differences? Front. Med. 9:842817. doi: 10.3389/fmed.2022.842817
Received: 24 December 2021; Accepted: 05 December 2022;
Published: 09 January 2023.
Edited by:
Chen Wang, China Academy of Chinese Medical Sciences, ChinaReviewed by:
Shuanglong Li, Guangzhou University, ChinaCopyright © 2023 Yu, Qin and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wen Qin,  cWlud2VuQHNkdS5lZHUuY24=; Jiajia Li, bGlqaWFqaWFAc2R1LmVkdS5jbg==
cWlud2VuQHNkdS5lZHUuY24=; Jiajia Li, bGlqaWFqaWFAc2R1LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.