
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 29 March 2022
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.836886
This article is part of the Research Topic Diagnosis and Treatment of Sarcoidosis View all 12 articles
 Renaud Prevel1,2
Renaud Prevel1,2 Vivien Guillotin1
Vivien Guillotin1 Sébastien Imbert2,3
Sébastien Imbert2,3 Patrick Blanco4,5Laurence Delhaes2,3
Patrick Blanco4,5Laurence Delhaes2,3 Pierre Duffau1,5*
Pierre Duffau1,5*Introduction: Cryptococcus spp. infection of the central nervous system (CINS) is a devastating opportunistic infection that was historically described in patients with acquired immunodeficiency syndrome (AIDS). Cryptococcus spp. infections are also associated with sarcoidosis; the impairment of cell-mediated immunity and long-term corticosteroid therapy being evoked to explain this association. Nevertheless, this assertion is debated and the underlying pathophysiological mechanisms are still unknown. The aims of this study were (i) to describe the clinical and biological presentation, treatments, and outcomes of CINS patients with and without sarcoidosis and (ii) to review the pathophysiological evidence underlying this clinical association.
Patients and Methods: Every patient with positive cerebrospinal fluid (CSF) cryptococcal antigen testing, India ink preparation, and/or culture from January 2015 to December 2020 at a tertiary university hospital were included, and patients with sarcoidosis were compared with non-sarcoidosis patients. Quantitative variables are presented as mean ± SD and are compared using the Mann-Whitney Wilcoxon rank-sum test. Categorical variables are expressed as the number of patients (percentage) and compared using the χ2 or Fisher's tests.
Results: During the study period, 16 patients experienced CINS, of whom 5 (31%) were associated with sarcoidosis. CINS symptoms, biological, and CSF features were similar between CINS patients with and without sarcoidosis except regarding CD4 cells percentages and CD4/CD8 ratio that was higher in those with sarcoidosis (47 ± 12 vs. 22 ± 18, p = 0.02 and 2.24 ± 1.42 vs. 0.83 ± 1.10, p = 0.03, respectively). CINS patients with sarcoidosis had less often positive blood antigen testing than those without sarcoidosis (2/5 vs. 11/11, p = 0.02). CINS patients with and without sarcoidosis were treated with similar drugs, but patients with sarcoidosis had a shorter length of treatment. CD4 cell levels do not seem to explain the association between sarcoidosis and cryptococcosis.
Conclusion: Sarcoidosis was the most frequently associated condition with CINS in this study. CINS patients associated with sarcoidosis had overall similar clinical and biological presentation than CINS patients associated with other conditions but exhibited a lower rate of positive blood cryptococcal antigen testing and higher CD4/CD8 T cells ratio. Pathophysiological mechanisms underlying this association remain poorly understood but B-1 cell deficiency or lack of IgM could be a part of the explanation. Another plausible mechanism is the presence of anti-granulocyte-macrophage colony-stimulating factor (GM-CSF) antibodies in a subset of patients with sarcoidosis, which could impair macrophage phagocytic function. Further studies are strongly needed to better understand those mechanisms and to identify at-risk patients.
Sarcoidosis is a systemic disease characterized by the formation of non-caseating epithelioid granulomas in several organs, mainly the lungs and the lymphatic system (1). It affects between 4.7 and 64 per 100,000 people and its prevalence varies from 1.0 to 64 per 100,000 per year (2). It can occur at any age of life, but with a particular proclivity for young adults. Spontaneous resolution occurs in about 60% of patients. Nevertheless, chronic and progressive forms are not rare and about 20% of patients have permanent clinical symptoms due to fibrotic lesions in the involved organs (2). Mortality is thought to be up to 5–10% (1), mainly associated with severe pulmonary fibrosis or, less usually, with cardiac or central nervous system involvement. Even if its exact origin remains unknown, the persistence of an unidentified antigen in individuals with genetic predisposition is supposed to trigger a pro-inflammatory Th1 response, leading to the formation of these granulomas. Sarcoidosis is characterized by a paradoxical immune status, i.e., an exaggerated immune response within granulomas, in contrast to various immune defects as stated by anergy to tuberculin test and the occurrence of opportunistic infections (3, 4), with corticosteroid therapy being a constant risk factor (4).
The first suspected opportunistic infections were mycobacterial ones but, except in patients receiving anti-TNFα treatments, sarcoidosis does not seem to be at particular risk for tuberculosis nor for any other mycobacterial infections. In fact, tuberculosis is less frequent, more typical, and not associated with immune reconstitution inflammatory syndrome in sarcoidosis patients compared with patients with acquired immunodeficiency syndrome (AIDS) (5). Mycobacterium avium complex infections were organ-specific in sarcoidosis patients and not disseminated as in patients with AIDS with no correlation with CD4 count (6). On the contrary, opportunistic infections such as progressive multifocal leukoencephalopathy (PML) and aspergillosis have been described in patients with sarcoidosis (4). Sarcoidosis is an underlying disease in 8–9% of PML cases with most patients who had not received any immunosuppressive drug (7, 8). Moreover, sarcoidosis represents a risk factor in 7–17% of chronic pulmonary aspergillosis (9, 10), and chronic pulmonary aspergillosis complicates around 2% of sarcoidosis (11, 12) with long-term corticosteroid therapy being a major risk factor for invasive aspergillosis, increasing in parallel with treatment dose and duration. Nocardiosis, histoplasmosis, and pneumocystosis are also reported in patients with sarcoidosis, but less frequently when compared with patients with rheumatological disorders who have more profound immunosuppression, especially after corticosteroid exposure (4).
Cryptococcus spp. infection of the central nervous system (CINS) is a devastating opportunistic infection that was first described in patients affected by AIDS historically representing about 70% of cryptococcal infections (13, 14). Cryptococcus spp. is responsible for one million infections per year among human immunodeficiency virus (HIV)-infected patients in the world; of these, approximately 625,000 die (15). Cryptococcus neoformans and Cryptococcus gattii are the most common and major pathogenic species complex in the genus Cryptococcus (16). C. gattii shares major virulence determinants with C. neoformans and was previously thought to be a subtype of C. neoformans, but genomic and transcriptomic studies revealed distinctions leading to recognize C. gattii as a unique species (17). Both species usually cause pulmonary or central nervous system (CNS) infections, but they differ in epidemiology, clinical features, and pathophysiology (18). C. gattii has traditionally been considered as a “tropical or subtropical fungus” despite the fact that, even before the North American outbreak, a large proportion of disease in Australia occurred in its southern temperate region. It has now been isolated from human and animal samples worldwide (17). Shifts in the appreciation of the clinical epidemiology of C. gattii in the past two decades include the recognition that it affects hosts known to be immunocompromised (including those with HIV/AIDS) as well as hosts presumed to be immunocompetent (17). The patients affected by other immunocompromising conditions such as sarcoidosis or others (lymphoproliferative disorders, malignancy diseases, organ transplant, and/or immunosuppressive therapy) are so predisposed to CINS, possibly caused by both C. neoformans and C. gattii (19–21) and cryptococcal infections affect 0.8 per 100,000 HIV-negative inhabitants (22). Their proportion is increasing with the advances in the care of HIV-infected patients (23, 24) and the increasing number of patients receiving immunosuppressive drugs. T cell-mediated immunity is the major pathway of defense against Cryptococcus spp. with a key role for Th1-Th2 imbalance resulting in impaired TNFα, IL-12, and IFN-γ production (25), and patients with AIDS are known to have impaired T cell-mediated immunity. The use of corticosteroids is a well-recognized risk factor for cryptococcosis (20, 22, 26), as for other opportunistic infections, with an estimated risk of fungal infections 1.5 times greater (95% CI: 1.3–1.9) in patients taking corticosteroids compared with naïve controls (11). The risk is especially increased for dosages exceeding 20 mg/day (27). In fact, corticosteroids cause dysregulation of Th1/Th2 T helper cells to balance favoring Th2 cytokines response and decrease cooperation with B cells (28). They are also responsible for a reduction in monocyte-macrophage functions by reducing chemotaxis, phagocytosis, and production of IL-1, IL-6, and TNF-α (29). The impairment of cell-mediated immunity (low CD4 cell count and lower CD4/CD8 ratio) has also been suggested as a risk factor for opportunistic infections in patients with sarcoidosis (11, 30, 31). Inconsistent with this hypothesis, numerous patients with sarcoidosis suffering from CINS reported in the literature were not receiving long-term corticosteroids therapy (11, 32, 33). A case-control study comparing sarcoidosis patients with and without CINS further confirmed corticosteroids therapy as a risk factor for CINS (34) but no association between the risk of opportunistic infection and severe CD4 lymphocytopenia was found.
To the best of our knowledge, no case-control study compared CINS patients with and without sarcoidosis to further address the underlying mechanisms. The aims of this study were to describe the clinical and biological presentation, treatments, and outcomes of CINS patients with and without sarcoidosis and to review the pathophysiological evidence underlying this clinical association.
This study was conducted at Bordeaux University Hospital including every patient with positive cerebrospinal fluid (CSF) cryptococcal antigen testing, India ink preparation, and/or culture from January 2015 to December 2020.
Cerebrospinal fluid cryptococcal antigen testing was performed using CryptoPS test (BIOSYNEX®) and blood cryptococcal antigen testing using CALAS® (Meridian Bioscience). CSF samples were processed with India ink preparation and incubated on Sabouraud Agar + Chloramphenicol + Gentamicin media (Bio-Rad). Blood samples were incubated on BACT/ALERT® FA (bioMérieux) culture bottles. Identification of growing isolates was performed using MALDI-TOF mass spectrometry (Microflex®, Bruker Daltonics).
Diagnosis of sarcoidosis was retrospectively confirmed according to the current recommendations (35): (i) clinical and paraclinical features consistent with sarcoidosis, (ii) an histopathological analysis revealing non-caseating granuloma except for patients presenting Löfgren's syndrome, and (iii) exclusion of other possible etiologies, including other granulomatous disorders. Data were retrospectively collected from the electronic medical records, and the electronic worksheet was completed by two medical intensive care residents.
No statistical sample size calculation was performed a priori, and the sample size was equal to the number of patients with positive CSF cryptococcal antigen testing and/or culture during the study period. Quantitative variables are presented as mean ± SD and compared using the Mann-Whitney Wilcoxon rank-sum test. Categorical variables are expressed as the number of patients (percentage) and compared using the χ2 or Fisher's tests. All statistical tests were 2-tailed, and statistical significance was defined as p < 0.05. Statistical analyses were assessed using the R version 3.6.0 statistical software (R Foundation for Statistical Computing Vienna, Austria).
According to the French law and the French Data Protection Authority, the handling of these data for research purposes was declared to the Data Protection Officer of the Bordeaux University Hospital. Patients (or their relatives, if any) were notified about the anonymized use of their healthcare data via the department's booklet.
During the study period, 16 patients presented CINS, of whom five were associated with sarcoidosis, four with an onco-hematological disease including two patients treated with ibrutinib, three patients with AIDS, two with kidney transplantation, one with autoimmune hepatitis, and one with epilepsy associated to Arnold-Chiari malformation (Table 1).
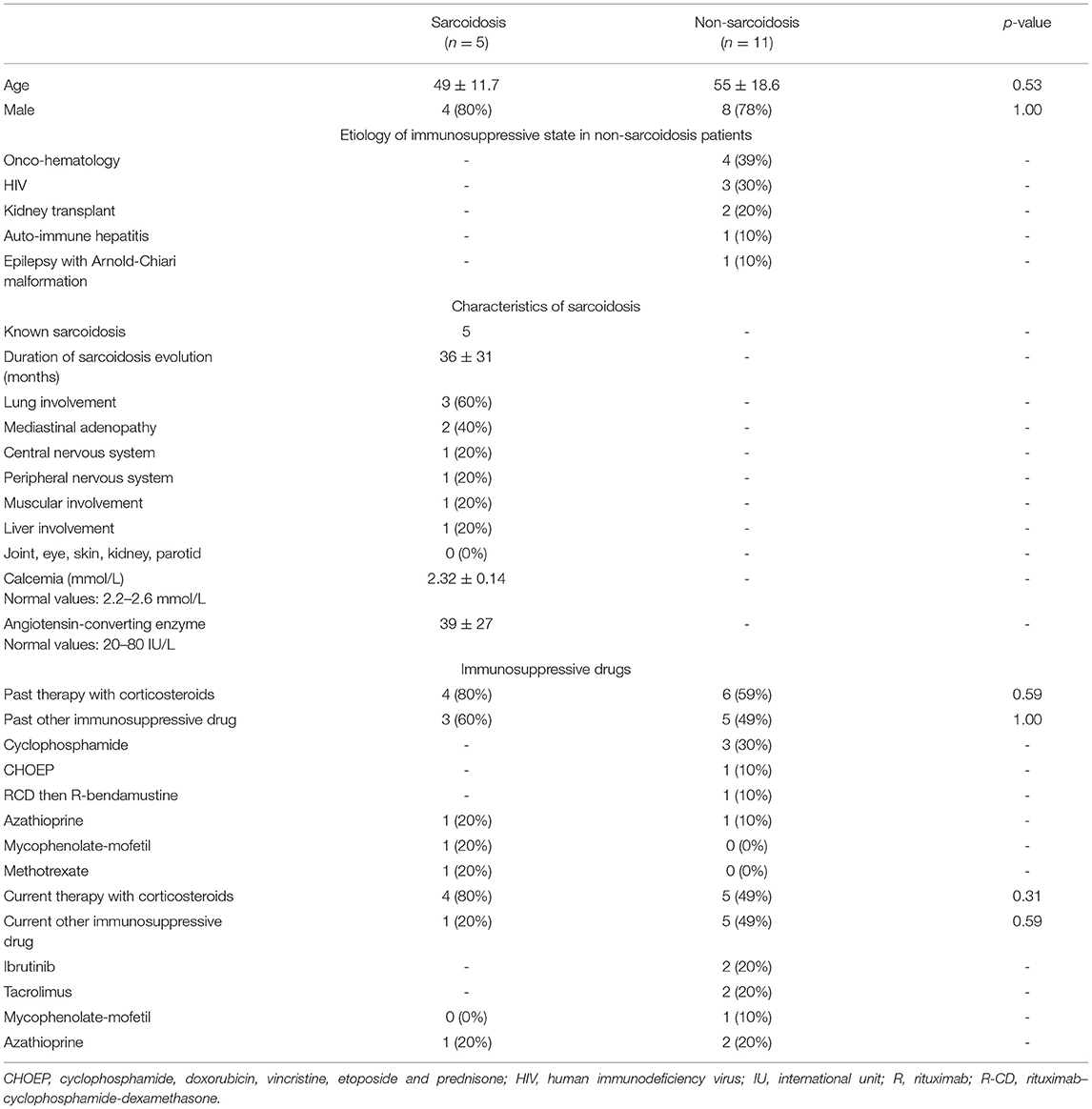
Table 1. Characteristics of patients diagnosed with Cryptococcus sp. infection of the central nervous system.
The median duration of sarcoidosis at cryptococcosis diagnosis was 36 ± 31 months. Patients with sarcoidosis were mostly men (4/5) with a median age of 49 ± 11.7 years, of whom three had lung involvement, two with mediastinal adenopathy, one with central and peripheral nervous system involvement, and one with muscular involvement. One of them only had liver involvement. Of these five patients, four were receiving corticosteroids therapy at the time of cryptococcosis diagnosis and three of them had previously received another immunosuppressive drug (one with azathioprine, one with mycophenolate-mofetil, and one with methotrexate) (Table 1). In patients receiving immunosuppressive drugs, only azathioprine was still ongoing at the time of cryptococcosis onset. No other previous opportunistic infection was reported among those patients with sarcoidosis.
In non-sarcoidosis patients, 6/11 previously received corticosteroid therapy, still ongoing for five of them, and 5/11 previously received other immunosuppressive drugs: 3 cyclophosphamide, 1 CHOEP, 1 R-CD then R-bendamustine, and 1 azathioprine. At the time of diagnosis, five of them were receiving immunosuppressive drugs: 2 ibrutinib, 2 tacrolimus, 2 azathioprine, and 1 mycophenolate-mofetil.
All of the five patients with sarcoidosis reported fever and headaches as symptoms of CINS. Two of them exhibited neck stiffness, two seizures, one behavior abnormalities, and one focal neurological deficit, being similar for all those features to non-sarcoidosis patients (Table 2). CSF cell count, protein, lactate, and glucose levels as a proportion of positive CSF antigen testing or culture were comparable between CINS patients with and without sarcoidosis. Each included patient had blood antigen testing that was less often positive (2/5 vs. 11/11, p = 0.02) in patients with sarcoidosis than in those without sarcoidosis (Table 2). Each cultivated strain but one was from C. neoformans species. Microbiological results on a patient basis are provided (Table 3).
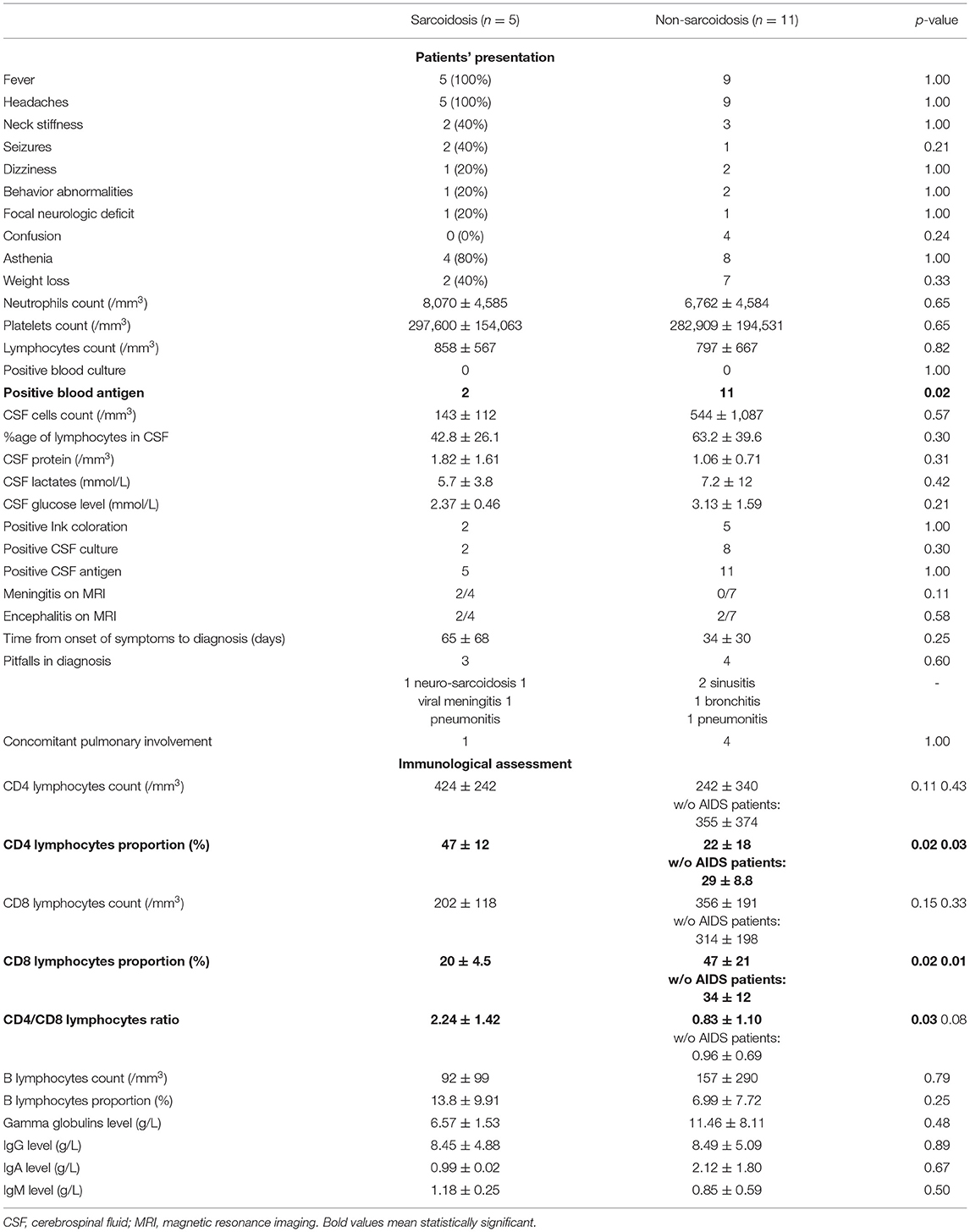
Table 2. Patients' presentation and immunological assessment at diagnosis of Cryptococcus spp. infection of central nervous system.
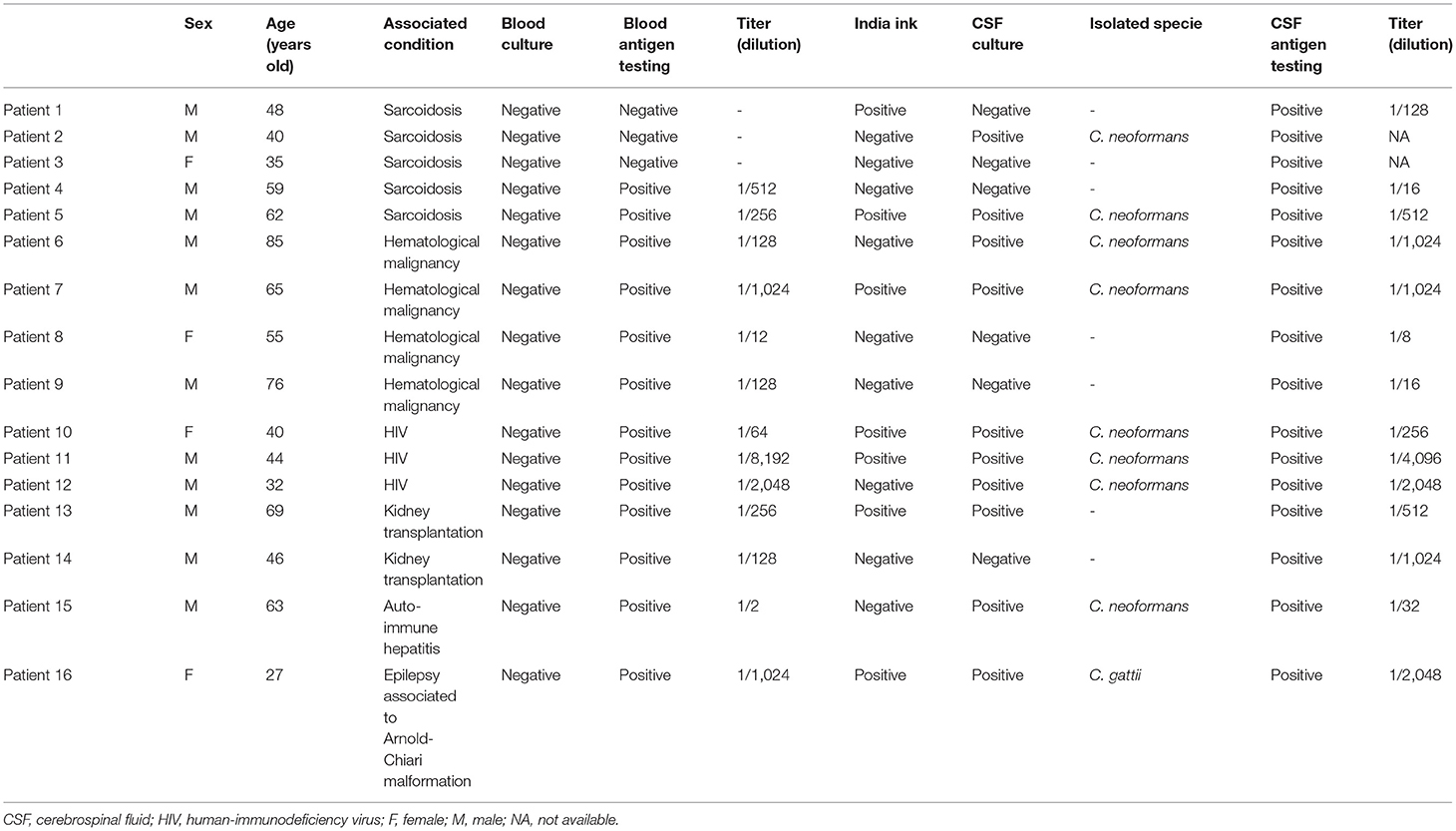
Table 3. Microbiologic results on a patient basis.
The blood B lymphocytes count and proportion and the blood gamma globulin levels were similar between CINS patients with and without sarcoidosis (Table 2).
Regarding cellular immunity, CD4 cells proportion among total lymphocyte blood count and CD4/CD8 ratio were higher in CINS patients with sarcoidosis than in those without sarcoidosis (47 ± 12 vs. 22 ± 18, p = 0.02 and 2.24 ± 1.42 vs. 0.83 ± 1.10, p = 0.03, respectively) (Table 2). The differences in CD4 and CD8 T cells proportion remained statistically significant after excluding patients with AIDS from non-sarcoidosis patients (Table 2).
As stated in current therapeutic guidelines, patients with CINS mostly received a 2-week association of intravenous liposomal B amphotericin (3 mg/kg per day) and flucytosine (25 mg/kg every 6 h) as initial therapy (4/5 in patients with sarcoidosis vs. 8/11 in patients without sarcoidosis, p = 1.00) and then fluconazole per os (400 mg per day for 8 weeks then 200 mg per day) as maintenance therapy (4/5 in patients with sarcoidosis vs. 10/11 in patients without, p = 1.00) (Table 4). Nevertheless, patients with sarcoidosis were treated for a shorter duration (34 ± 29 days vs. 66 ± 13, p = 0.04) than those without sarcoidosis with a similar death rate and long-term sequelae (p = 1.00 for both) (Table 4).
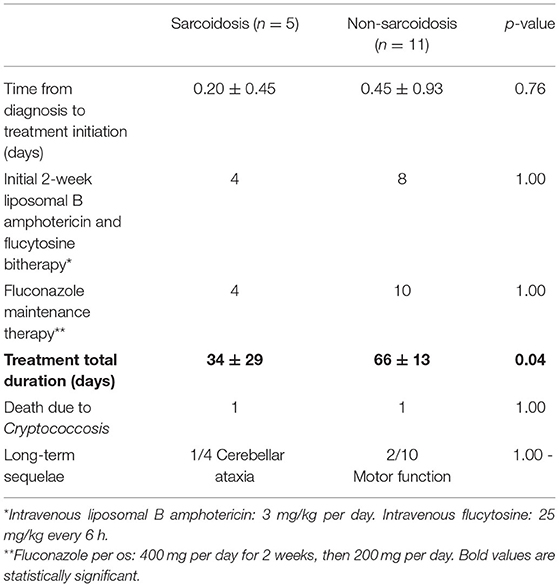
Table 4. Management and outcomes of Cryptococcus spp. infection of the central nervous system.
In this study, sarcoidosis is the most prevalent disease associated with CINS: 5 CINS over a period of 6 years with sarcoidosis accounting for 31% of all CINS and 38% (5/13) of the HIV-negative patients. CINS patients with sarcoidosis have a similar clinical and biological presentation at diagnosis but exhibit a higher CD4/CD8 T cells ratio than those without sarcoidosis. Importantly, CINS patients with sarcoidosis exhibited a lower rate of positive blood antigen testing compared with those without sarcoidosis. In front of CINS suspicion in a patient with sarcoidosis, blood cryptococcal antigen testing should be reiterated if negative when a reasonable clinical probability is assessed. CSF antigen testing should also be performed in case of clinical suspicion even if blood antigen testing is negative. CINS patients with sarcoidosis had a shorter duration of treatment than those without sarcoidosis. Every patient was treated based on specialized team stewardship. Shorter duration could be explained by the absence of severe quantitative CD4 count defect, the rarer use of immunosuppressive drugs, and the lower proportion of blood positive antigen testing in patients with sarcoidosis than in other patients. Recommendations regarding the duration of treatment for CINS have been established in AIDS and solid-organ transplant patients, and to the best of our knowledge, no consensus exists in patients with sarcoidosis.
Contrary to our findings, only very few cases were identified in the main case-control study (cryptOsarc study) comparing sarcoidosis patients with and without cryptococcosis (34). This study included 18 sarcoidosis patients with cryptococcosis, of whom 13 had CINS, over a period of 25 years. These patients were compared with 36 sarcoidosis patients without cryptococcosis. Sarcoidosis accounted for 0.6% of all cryptococcosis patients and 2.9% of the HIV-negative cryptococcosis patients. This discrepancy could be explained by the major therapeutic advances in the care of HIV-infected patients and by increasing the awareness of practitioners regarding the risk of cryptococcosis in other immunosuppressive conditions leading to more frequent testing. Among these 18 sarcoidosis patients with cryptococcosis included in the cryptOsarc study, 4 (23%) had sarcoidosis diagnosed at the time of infection and the 14 others had a median duration of 1,005 days (0–5,876) from the onset of the sarcoidosis. Notably, 12 out of the 18 patients (67%) had previously been treated with corticosteroids with a median therapy duration of 137 days (0–5,695), and a median dose of 18 mg/day (0–55) and two of them were receiving immunosuppressive drugs (cyclophosphamide for one and methotrexate plus infliximab for the other). The median level of CD4 lymphocytes at the time of cryptococcosis diagnosis was 145/mm3 (55–1,300). Compared with those free from cryptococcosis, patients with sarcoidosis and cryptococcosis were mostly men (72 vs. 47%, p = 0.145), they were younger (median age 28 vs. 42, p = 0.0004) and extra-pulmonary involvement was more frequent (83 vs. 56%, p = 0.069), including cardiac involvement, neurosarcoidosis or naso-sinusal, and/or parotid involvement. Factors associated with cryptococcosis in those patients with sarcoidosis were extra-thoracic sarcoidosis (p = 0.055) and possibly the intake of corticosteroid therapy or not (p = 0.123). Nevertheless, in this cryptOsarc study, only two-thirds of these patients received corticosteroids therapy and none of them experienced other opportunistic infections suggesting a specific susceptibility. In fact, patients with sarcoidosis are known to exhibit a decreased T cell response to cryptococcal antigen in vitro (36). As the pathophysiology of sarcoidosis still remains poorly understood, an unexplained primary immunodeficiency could favor both the occurrence of sarcoidosis and cryptococcosis (36).
Cryptococcosis is known to develop in patients with AIDS and idiopathic CD4 lymphopenia underlining the importance of CD4 T cells in the defense against Cryptococcus spp. (37). Systemic CD4 cells anergy is a feature of sarcoidosis as lymphopenia is correlated with disease severity during sarcoidosis (38) due to the accumulation of CD4 T lymphocytes in active granulomas participating in the “immune paradox” described in sarcoidosis: despite an extensive local inflammation, systemic anergy may develop (39). Nevertheless, in the cryptOsarc study, CD4 lymphocytopenia was not an independent risk factor for cryptococcosis (34) consistent with our findings that in CINS patients with sarcoidosis had a higher CD4 T cell proportion and CD4/CD8 T cells ratio than non-sarcoidosis patients. The authors of the cryptOsarc study even considered that “the CD4 levels in this study did not explain cryptococcosis in sarcoidosis”. If quantitative alteration of CD4 T cells function is not responsible per se for this association with cryptococcosis, alteration of qualitative CD4 T cell function could be involved in the pathophysiology (Figure 1), but T cell dysfunction in sarcoidosis is poorly understood so far. Data on peripheral CD25high regulatory T cells (Treg) are contradictory; some authors reported a peripheral expansion that contributed to anergy, whereas others have reported a decrease in Treg cells with an imbalance in favor of Th17 cells (3).
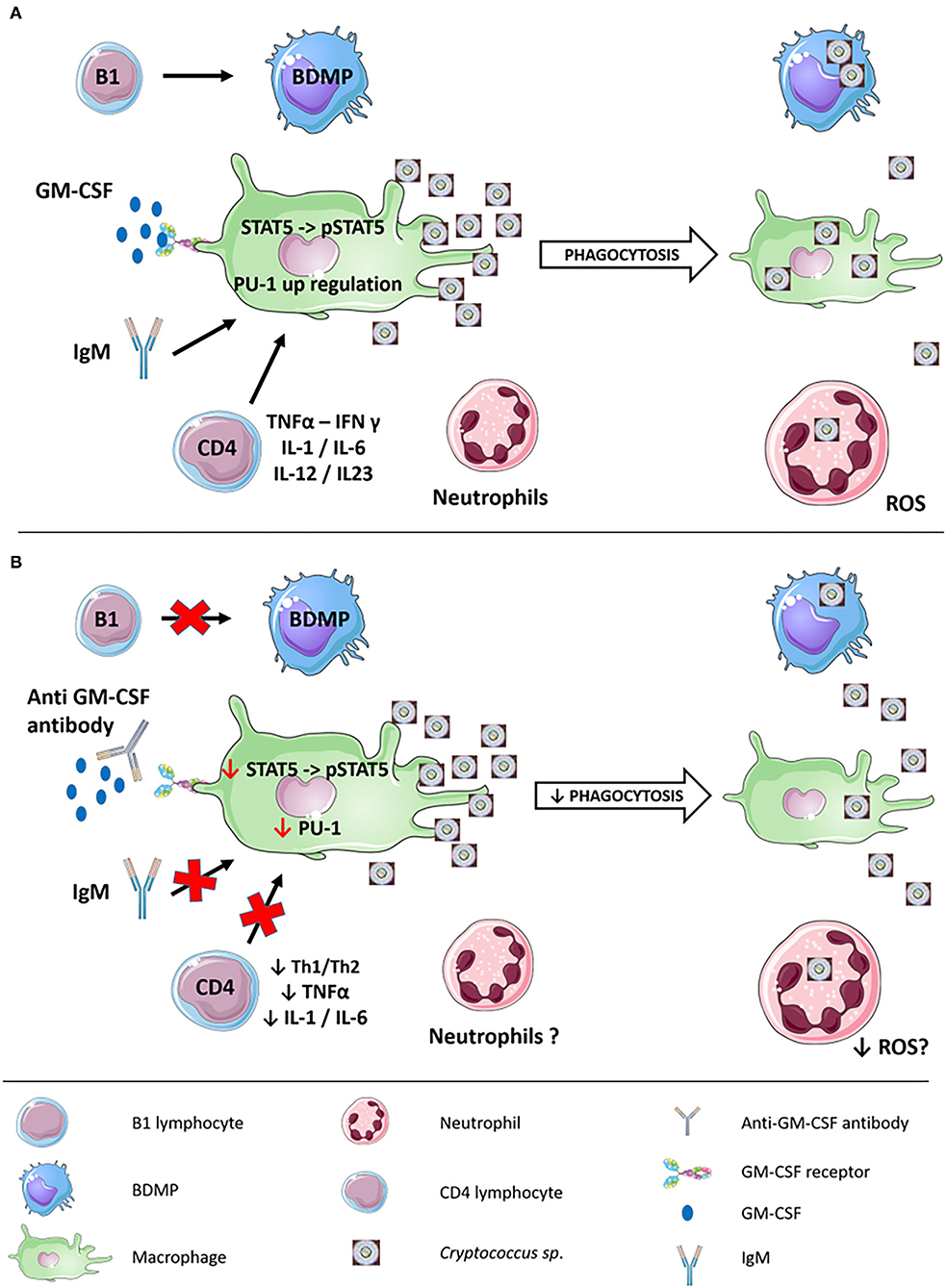
Figure 1. Immune response to cryptococcal infection and potential pathophysiological mechanisms responsible for the association between sarcoidosis and cryptococcosis. (A) Immune response to cryptococcal infection involving both innate and adaptative immunity. B1 cells can differentiate into BDMP with phagocytic activity against Cryptococcus spp. GM-CSF, IgM, and CD4 activate macrophage phagocytic activity, partly via the phosphorylation of STAT-5 upregulating the transcription factor PU-1. Neutrophils exert a fungicidal activity through the production of ROS. (B) Potential pathophysiological mechanisms responsible for the association between sarcoidosis and cryptococcosis. B1 cells could have impaired differentiation leading to defective BDMP phagocytic activity. Lack of IgM and CD-4 qualitative defects could lead to a defect in macrophage phagocytic activity. The presence of anti-GM-CSF antibodies could also prevent STAT-5 phosphorylation downregulating the transcription factor PU-1. Whether ROS species neutrophils production is impaired in sarcoidosis remains unknown. B-1, B-1 lymphocytes; BDMP, B-1-derived mononuclear phagocytes; CD4, CD4 lymphocytes; GM-CSF, granulocyte-macrophage colony-stimulating factor; ROS, reactive oxygen species.
Besides this potential qualitative CD4 T cell deficiency, an altered CD4 T cells-macrophage crosstalk could also be involved via decreased macrophage ability to contain Cryptococcus spp. (40). This hypothesis is reinforced as patients with X-linked CD40L deficiency or interleukin 12 receptor mutations exhibit higher susceptibility for cryptococcal infections (37). CD40L−/− mice exhibited exacerbation of infection with a high fungal burden due to diminished interferon-γ production by CD4 and CD8 cells and decreased CD28 expression by CD4 cells (41). Moreover, nitrite production and antimicrobial activity by macrophages were impaired as was IL-12 production by splenic macrophages. Patients with auto-antibodies to interferon-γ and granulocyte-macrophage colony-stimulating factor (GM-CSF) also exhibit higher susceptibility to cryptococcal infections (37) as discussed below. The fact that interferon-γ and GM-CSF are known to be produced by CD4+ helper T cells to activate macrophages reinforce the plausibility of an altered CD4 T cells-macrophage crosstalk as a potential mechanism of increased susceptibility to cryptococcosis in sarcoidosis patients (42) (Figure 1).
Interest in the role of humoral immunity against Cryptococcus spp. was regained after the recent report of an association between invasive fungal infections, including cryptococcosis (43–45), and ibrutinib, an irreversible inhibitor of Bruton's tyrosine kinase (BTK). This clinical finding is strengthened by the fact that X-linked immunodeficient mice, which possess a mutation leading to a defective BTK, lack B-1 cells and natural IgM. These mice exhibit very high fungal burden after challenge with C. neoformans and fungal dissemination to the brain (46) consistent with previous findings in C57BL/6 mice depletion of B-1 cells (47) or sIgM−/− (48). Conclusions from these studies were flawed by the presence of T cells in those models and by associated defects in cellular immunity (XID mice) and in B cell development (sIgM−/− mice). To overcome these limitations, Rag1-deficient mice, which lack both T and B cells, were used, and B cells purified from wild-type animals were transferred (49) restoring B-1a and B-1b cells but not T cells or B-2 cells (50). This transfer led to a marked reduction in the cryptococcal burden in the brain but not in the lungs of the mice. Interestingly, transfer of IgG-depleted, IgM-containing serum in Rag1-deficient mice increased in alveolar macrophage recruitment and phagocytic index suggesting that the host benefit could be mediated by IgM-induced macrophage activation rather than a direct interaction (48). Another hypothesis is that B-1 cells could migrate to the lungs and differentiate into macrophage-like cells called B-1-derived mononuclear phagocytes (BDMP) (Figure 1) even if mechanisms by which B-1 B cells traffic to C. neoformans-infected lungs remains unknown (47). Those BDMP cells have been demonstrated to phagocyte C. neoformans via a complement receptor 3-mediated pathway with a higher fungicidal activity than a macrophage (51).
Even if sarcoidosis and granuloma formation in sarcoidosis are normally considered T cell-mediated peripheral B cells seem to be anergic in patients with sarcoidosis (52). This observed anergy could be due to the decreased levels of NF-κB/p65 (53) or to the lack of co-stimulation from CD4+ helper T cells (54). Nevertheless, whether sarcoidosis is associated with an impaired IgM production or with deficient B-1 cells is still not known.
The real impact of B cells on susceptibility for cryptococcosis has also been questioned as invasive fungal infections are very rare in patients with X-linked agammaglobulinemia with BTK deficiency, probably because of residual BTK activity in myeloid cells (37). In fact, BTK is expressed in all bone marrow cell lineages except T cells and plasma cells (55). The increased susceptibility of X-linked immunodeficient mice seems to be mostly due to the inability of macrophages to phagocyte Cryptococcus spp. rather than impairment of humoral immunity (46).
Besides adaptive immunity deficiency previously discussed, innate immunity deficiency seems to be a key player in the susceptibility to Cryptococcus spp. infection. This deficiency of innate immunity could be indirectly due to the impaired crosstalk with adaptive immunity, i.e., impaired activation of macrophages by deficient CD4 T cells or by lack of IgM as previously discussed, but it can also be directly due to the intrinsic deficiency of innate immunity (Figure 1).
For instance, anti-GM-CSF antibodies have been isolated from the serum of apparently immunocompetent patients with cryptococcosis with or without pulmonary alveolar proteinosis (56–59). The addition of sera from the patients containing anti-GM-CSF antibodies impaired myeloid cells activation from controls in the presence of C. gatii (56). These antibodies are exclusively IgG and mostly IgG1 and are biologically active by inhibition of GM-CSF-induced macrophage inflammatory protein-1α expression (MIP-1 α) and signal transducer and activator of transcription-5 (STAT-5) phosphorylation in control peripheral blood mononuclear cells (58–60). This inhibition reduces myeloid cells proliferation and differentiation but also their phagocytic and bactericidal capacities via the inhibition of PU.1 transcription factor (59, 61) (Figure 1). Anti-GM-CSF antibodies are also involved in pulmonary alveolar proteinosis (PAP), but most of the cryptococcosis patients presenting with anti-GM-CSF antibodies did not suffer from PAP (62). This might be explained by the extreme heterogeneity of those antibodies regarding their avidity and the targeted GM-CSF epitopes (63). Moreover, multiple clones of anti-GM-CSF antibodies could be present in the same patient.
Anti-GM-CSF antibodies could be part of an explanation for this association between cryptococcosis and sarcoidosis as a potential association has been described between PAP and sarcoidosis (64, 65). A recent study found in 5/92 (5.4%) patients with sarcoidosis to have detectable anti-GM-CSF antibodies, two of them with clinical PAP (62). Those patients exhibited significantly higher serum levels of Krebs von den Lungen-6, surfactant protein-D, lactate dehydrogenase and required more often systemic corticosteroid therapy. It would thus be interesting to assess if anti-GM-CSF antibodies are more prevalent in patients with sarcoidosis and suspicion of cryptococcal infection. If so, the presence of those antibodies could help to identify at-risk patients. Nevertheless, whether uptake by macrophages is a conclusive readout for protecting against cryptococcal invasion is still unclear. In fact, recruited M1 polarized monocyte-derived macrophages are thought to have fungicidal activity contrary to alveolar macrophages (66). Alveolar macrophages could even be involved in the cryptococcal dissemination outside the lungs (67, 68).
Another major effector of first-line defense against cryptococcal infection is the pool of neutrophils as they have been demonstrated to engulf and kill Cryptococcus spp. more efficiently than monocytes (69) and produce reactive oxygen species (ROS) that kill Cryptococcus spp. (70). However, the role of neutrophils in cryptococcal infections is not straightforward as, in contrast to intravascular infection, they seem to worsen the prognosis in the setting of intratracheal infection (71, 72). Absolute neutrophil count of more than 3,500 cells/mm3 is even associated with increased mortality in HIV-infected patients with cryptococcal meningitis (73). This could be explained by the fact that neutrophils are recruited to the lungs in response to cryptococcal infection by lung parenchymal lymphocytes and that T cells (CD4 cells but also CD8 cells and γδ cells) impairment is associated with a compensatory neutrophil response requiring IL-17A, which worsens lung injury (71, 72, 74). Moreover, the following two distinct neutrophil subsets seem to be generated in response to cryptococcal infection: (i) one with an oxidative stress signature interacting directly with the fungus and generating ROS and (ii) another with enhanced cytokine gene expression which are longer-lived and that indirectly respond to cryptococcal ligands to modulate crosstalk, via the expression of IL-1α, TNFα, and complement C3, with dendritic cells and alveolar macrophages through CCR5 and CCR1, respectively (75). Mechanisms responsible for such a differentiation remain unknown. While in contact, Cryptococcus spp. phagocytosis by neutrophils is dependent on the complement C5a-C5aR axis (76).
Very less is known about neutrophil's involvement in sarcoidosis pathophysiology except for that neutrophil/lymphocyte ratio in the complete blood count can be used as an indicator of inflammation in sarcoidosis (77). Although neutrophil accumulation-inducing chemokines like IL-8 are increased in sarcoidosis, the percentage of neutrophils in the bronchoalveolar lavage remains low and is not correlated to CXCL8 or CXCL5 as in idiopathic pulmonary fibrosis (78–80). Nevertheless, the percentage of neutrophils in bronchoalveolar lavage is associated with progressing sarcoidosis and an increased risk for corticosteroid therapy (81, 82). The role of neutrophils in the association between sarcoidosis and cryptococcosis thus remains to be demonstrated (Figure 1).
Sarcoidosis was the most frequently associated condition with CINS in this study. CINS patients with associated sarcoidosis had overall similar clinical and biological presentation than CINS patients associated with other conditions but exhibited a lower rate of positive blood cryptococcal antigen testing and higher CD4/CD8 T cells ratio. Pathophysiological mechanisms underlying this association remain poorly understood, but B-1 cell deficiency or lack of IgM could be a part of the explanation. Another plausible mechanism is the presence of anti-GM-CSF antibodies in a subset of patients with sarcoidosis that could impair macrophage phagocytic function. Further studies are strongly needed to better understand those mechanisms and to identify at-risk patients.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
RP, LD, PB, and PD contributed to the conception and design of the study. RP, SI, and VG contributed to the data collection. RP and PD wrote the manuscript. Each author drafted or provided critical revision of the article and provided final approval of the version submitted for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Valeyre D, Prasse A, Nunes H, Uzunhan Y, Brillet P-Y, Müller-Quernheim J. Sarcoidosis. Lancet. (2014) 383:1155–67. doi: 10.1016/S0140-6736(13)60680-7
2. Drent M, Crouser ED, Grunewald J. Challenges of sarcoidosis and its management. N Engl J Med. (2021) 385:1018–32. doi: 10.1056/NEJMra2101555
3. Miyara M, Amoura Z, Parizot C, Badoual C, Dorgham K, Trad S, et al. The immune paradox of sarcoidosis and regulatory T cells. J Exp Med. (2006) 203:359–70. doi: 10.1084/jem.20050648
4. Jamilloux Y, Valeyre D, Lortholary O, Bernard C, Kerever S, Lelievre L, et al. The spectrum of opportunistic diseases complicating sarcoidosis. Autoimmun Rev. (2015) 14:64–74. doi: 10.1016/j.autrev.2014.10.006
5. Zumla A, Raviglione M, Hafner R, von Reyn CF. Tuberculosis. N Engl J Med. (2013) 368:745–55. doi: 10.1056/NEJMra1200894
6. Sepkowitz KA. Opportunistic infections in patients with and patients without acquired immunodeficiency syndrome. Clin Infect Dis. (2002) 34:1098–107. doi: 10.1086/339548
7. Rosenbloom MA, Uphoff DF. The association of progressive multifocal leukoencephalopathy and sarcoidosis. Chest. (1983) 83:572–5. doi: 10.1378/chest.83.3.572
8. Brooks BR, Walker DL. Progressive multifocal leukoencephalopathy. Neurol Clin. (1984) 2:299–313. doi: 10.1016/S0733-8619(18)31105-8
9. Denning DW, Pleuvry A, Cole DC. Global burden of chronic pulmonary aspergillosis complicating sarcoidosis. Eur Respir J. (2013) 41:621–6. doi: 10.1183/09031936.00226911
10. Smith NL, Denning DW. Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma. Eur Respir J. (2011) 37:865–72. doi: 10.1183/09031936.00054810
11. Baughman RP, Lower EE. Fungal infections as a complication of therapy for sarcoidosis. QJM. (2005) 98:451–6. doi: 10.1093/qjmed/hci073
12. Pena TA, Soubani AO, Samavati L. Aspergillus lung disease in patients with sarcoidosis: a case series and review of the literature. Lung. (2011) 189:167–72. doi: 10.1007/s00408-011-9280-9
13. Dromer F, Mathoulin-Pélissier S, Fontanet A, Ronin O, Dupont B, Lortholary O, et al. Epidemiology of HIV-associated cryptococcosis in France (1985–2001): comparison of the pre- and post-HAART eras. AIDS. (2004) 18:555–62. doi: 10.1097/00002030-200402200-00024
14. Dromer F, Mathoulin-Pélissier S, Launay O, Lortholary O. French Cryptococcosis Study Group. Determinants of disease presentation and outcome during cryptococcosis: the CryptoA/D study. PLoS Med. (2007) 4:e21. doi: 10.1371/journal.pmed.0040021
15. Oliveira EP, Inácio CP, de Freitas JF, Valeriano CAT, Neves RP, Sobrinho PM, et al. Tuberculosis and neurocryptococcosis by Cryptococcus neoformans molecular type VNI in A non-HIV patient: a comorbidities case report. Med Mycol J. (2022) 32:101213. doi: 10.1016/j.mycmed.2021.101213
16. Morales-López SE, Garcia-Effron G. Infections due to rare Cryptococcus species. A literature review. J Fungi. (2021) 7:279. doi: 10.3390/jof7040279
17. Chen SC-A, Meyer W, Sorrell TC. Cryptococcus gattii infections. Clin Microbiol Rev. (2014) 27:980–1024. doi: 10.1128/CMR.00126-13
18. Xue X, Deng H, Zhao L, Zang X, Asuquo IP, Meng M, et al. Cryptococcosis caused by Cryptococcus gattii: 2 case reports and literature review. Medicine. (2020) 99:e23213. doi: 10.1097/MD.0000000000023213
19. Bicanic T, Harrison TS. Cryptococcal meningitis. Br Med Bull. (2004) 72:99–118. doi: 10.1093/bmb/ldh043
20. Pappas PG, Perfect JR, Cloud GA, Larsen RA, Pankey GA, Lancaster DJ, et al. Cryptococcosis in human immunodeficiency virus-negative patients in the era of effective azole therapy. Clin Infect Dis. (2001) 33:690–9. doi: 10.1086/322597
21. Husain S, Wagener MM, Singh N. Cryptococcus neoformans infection in organ transplant recipients: variables influencing clinical characteristics and outcome. Emerg Infect Dis. (2001) 7:375–81. doi: 10.3201/eid0703.017302
22. Hajjeh RA, Conn LA, Stephens DS, Baughman W, Hamill R, Graviss E, et al. Cryptococcosis: population-based multistate active surveillance and risk factors in human immunodeficiency virus-infected persons. Cryptococcal active surveillance group. J Infect Dis. (1999) 179:449–54. doi: 10.1086/314606
23. Iroezindu MO. Disparities in the magnitude of human immunodeficiency virus-related opportunistic infections between high and low/middle-income countries: is highly active antiretroviral therapy changing the trend? Ann Med Health Sci Res. (2016) 6:4–18. doi: 10.4103/2141-9248.180234
24. UK Collaborative HIV. Cohort (CHIC) Study Steering Committee, Garvey L, Winston A, Walsh J, Post F, Porter K, et al. HIV-associated central nervous system diseases in the recent combination antiretroviral therapy era. Eur J Neurol. (2011) 18:527–34. doi: 10.1111/j.1468-1331.2010.03291.x
25. Lortholary O, Sitbon K, Dromer F. French Cryptococcosis Study Group. Evidence for human immunodeficiency virus and Cryptococcus neoformans interactions in the pro-inflammatory and anti-inflammatory responses in blood during AIDS-associated cryptococcosis. Clin Microbiol Infect (2005) 11:296–300. doi: 10.1111/j.1469-0691.2005.01074.x
26. Dromer F, Mathoulin S, Dupont B, Laporte A. Epidemiology of cryptococcosis in France: a 9-year survey (1985-1993). French cryptococcosis study group. Clin Infect Dis. (1996) 23:82–90. doi: 10.1093/clinids/23.1.82
27. Baddley JW, Perfect JR, Oster RA, Larsen RA, Pankey GA, Henderson H, et al. Pulmonary cryptococcosis in patients without HIV infection: factors associated with disseminated disease. Eur J Clin Microbiol Infect Dis. (2008) 27:937–43. doi: 10.1007/s10096-008-0529-z
28. Kovalovsky D, Refojo D, Holsboer F, Arzt E. Molecular mechanisms and Th1/Th2 pathways in corticosteroid regulation of cytokine production. J Neuroimmunol. (2000) 109:23–9. doi: 10.1016/S0165-5728(00)00298-8
29. Lionakis MS, Kontoyiannis DP. Glucocorticoids and invasive fungal infections. Lancet. (2003) 362:1828–38. doi: 10.1016/S0140-6736(03)14904-5
30. Ross JJ, Katz JD. Cryptococcal meningitis and sarcoidosis. Scand J Infect Dis. (2002) 34:937–9. doi: 10.1080/0036554021000026969
31. Stern BJ. Neurological complications of sarcoidosis. Curr Opin Neurol. (2004) 17:311–6. doi: 10.1097/00019052-200406000-00013
32. Rubinstein I, Baum GL, Rosenthal T. Fungal infections complicating pulmonary sarcoidosis. J Infect Dis. (1985) 152:1360.
33. Winterbauer RH, Kraemer KG. The infectious complications of sarcoidosis: a current perspective. Arch Intern Med. (1976) 136:1356–62. doi: 10.1001/archinte.136.12.1356
34. Bernard C, Maucort-Boulch D, Varron L, Charlier C, Sitbon K, Freymond N, et al. Cryptococcosis in sarcoidosis: cryptOsarc, a comparative study of 18 cases. QJM. (2013) 106:523–39. doi: 10.1093/qjmed/hct052
35. Crouser ED, Maier LA, Wilson KC, Bonham CA, Morgenthau AS, Patterson KC, et al. Diagnosis and detection of sarcoidosis. Am J Respir Crit Care Med. (2020) 201:e26–51. doi: 10.1164/rccm.202002-0251ST
36. Belcher RW, Palazij R, Wolinsky E. Immunologic studies in patients with sarcoidosis and cryptococcosis. Arch Dermatol. (1975) 111:711–6. doi: 10.1001/archderm.111.6.711
37. Lionakis MS, Netea MG, Holland SM. Mendelian genetics of human susceptibility to fungal infection. Cold Spring Harb Perspect Med. (2014) 4:a019638. doi: 10.1101/cshperspect.a019638
38. Sweiss NJ, Salloum R, Gandhi S, Ghandi S, Alegre M-L, Sawaqed R, et al. Significant CD4, CD8, and CD19 lymphopenia in peripheral blood of sarcoidosis patients correlates with severe disease manifestations. PLoS ONE. (2010) 5:e9088. doi: 10.1371/journal.pone.0009088
39. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. (2007) 357:2153–65. doi: 10.1056/NEJMra071714
40. Kawakami K, Kohno S, Morikawa N, Kadota J, Saito A, Hara K. Activation of macrophages and expansion of specific T lymphocytes in the lungs of mice intratracheally inoculated with Cryptococcus neoformans. Clin Exp Immunol. (1994) 96:230–7. doi: 10.1111/j.1365-2249.1994.tb06547.x
41. Pietrella D, Lupo P, Perito S, Mosci P, Bistoni F, Vecchiarelli A. Disruption of CD40/CD40L interaction influences the course of Cryptococcus neoformans infection. FEMS Immunol Med Microbiol. (2004) 40:63–70. doi: 10.1016/S0928-8244(03)00297-9
42. Fischer HG, Frosch S, Reske K, Reske-Kunz AB. Granulocyte-macrophage colony-stimulating factor activates macrophages derived from bone marrow cultures to synthesis of MHC class II molecules and to augmented antigen presentation function. J Immunol. (1988) 141:3882–8.
43. Chamilos G, Lionakis MS, Kontoyiannis DP. Call for action: invasive fungal infections associated with ibrutinib and other small molecule kinase inhibitors targeting immune signaling pathways. Clin Infect Dis. (2018) 66:140–8. doi: 10.1093/cid/cix687
44. Stankowicz M, Banaszynski M, Crawford R. Cryptococcal infections in two patients receiving ibrutinib therapy for chronic lymphocytic leukemia. J Oncol Pharm Pract. (2019) 25:710–4. doi: 10.1177/1078155217752078
45. Brochard J, Morio F, Mahe J, Le Pape P, Guimard T, Mahe B, et al. Ibrutinib, a Bruton's tyrosine kinase inhibitor, a new risk factor for cryptococcosis. Med Mal Infect. (2020) 50:742–5. doi: 10.1016/j.medmal.2020.07.005
46. Szymczak WA, Davis MJ, Lundy SK, Dufaud C, Olszewski M, Pirofski L. X-linked immunodeficient mice exhibit enhanced susceptibility to Cryptococcus neoformans infection. MBio. (2013) 4:e00265–13. doi: 10.1128/mBio.00265-13
47. Rohatgi S, Pirofski L. Molecular characterization of the early B cell response to pulmonary Cryptococcus neoformans infection. J Immunol. (2012) 189:5820–30. doi: 10.4049/jimmunol.1201514
48. Subramaniam KS, Datta K, Quintero E, Manix C, Marks MS, Pirofski L-A. The absence of serum IgM enhances the susceptibility of mice to pulmonary challenge with Cryptococcus neoformans. J Immunol. (2010) 184:5755–67. doi: 10.4049/jimmunol.0901638
49. Dufaud C, Rivera J, Rohatgi S, Pirofski L-A. Naïve B cells reduce fungal dissemination in Cryptococcus neoformans infected Rag1-/- mice. Virulence. (2018) 9:173–84. doi: 10.1080/21505594.2017.1370529
50. Weber GF, Chousterman BG, Hilgendorf I, Robbins CS, Theurl I, Gerhardt LMS, et al. Pleural innate response activator B cells protect against pneumonia via a GM-CSF-IgM axis. J Exp Med. (2014) 211:1243–56. doi: 10.1084/jem.20131471
51. Ghosn EEB, Russo M, Almeida SR. Nitric oxide-dependent killing of Cryptococcus neoformans by B-1-derived mononuclear phagocyte. J Leukoc Biol. (2006) 80:36–44. doi: 10.1189/jlb.1005603
52. Zhou E-R, Arce S. Key players and biomarkers of the adaptive immune system in the pathogenesis of sarcoidosis. Int J Mol Sci. (2020) 21:E7398. doi: 10.3390/ijms21197398
53. Lee N-S, Barber L, Akula SM, Sigounas G, Kataria YP, Arce S. Disturbed homeostasis and multiple signaling defects in the peripheral blood B-cell compartment of patients with severe chronic sarcoidosis. Clin Vaccine Immunol. (2011) 18:1306–16. doi: 10.1128/CVI.05118-11
54. Martinez GJ, Hu JK, Pereira RM, Crampton JS, Togher S, Bild N, et al. Cutting edge: NFAT transcription factors promote the generation of follicular helper T cells in response to acute viral infection. J Immunol. (2016) 196:2015–9. doi: 10.4049/jimmunol.1501841
55. Stiff A, Trikha P, Wesolowski R, Kendra K, Hsu V, Uppati S, et al. Myeloid-derived suppressor cells express Bruton's tyrosine kinase and can be depleted in tumor-bearing hosts by ibrutinib treatment. Cancer Res. (2016) 76:2125–36. doi: 10.1158/0008-5472.CAN-15-1490
56. Crum-Cianflone NF, Lam PV, Ross-Walker S, Rosen LB, Holland SM. Autoantibodies to granulocyte-macrophage colony-stimulating factor associated with severe and unusual manifestations of Cryptococcus gattii infections. Open Forum Infect Dis. (2017) 4:ofx211. doi: 10.1093/ofid/ofx211
57. Demir S, Chebib N, Thivolet-Bejui F, Cottin V. Pulmonary alveolar proteinosis following cryptococcal meningitis: a possible cause? BMJ Case Rep. (2018) 2018:bcr-2017-222940. doi: 10.1136/bcr-2017-222940
58. Kuo C-Y, Wang S-Y, Shih H-P, Tu K-H, Huang W-C, Ding J-Y, et al. Disseminated cryptococcosis due to anti-granulocyte-macrophage colony-stimulating factor autoantibodies in the absence of pulmonary alveolar proteinosis. J Clin Immunol. (2017) 37:143–52. doi: 10.1007/s10875-016-0364-4
59. Rosen LB, Freeman AF, Yang LM, Jutivorakool K, Olivier KN, Angkasekwinai N, et al. Anti-GM-CSF autoantibodies in patients with cryptococcal meningitis. J Immunol. (2013) 190:3959–66. doi: 10.4049/jimmunol.1202526
60. Saijo T, Chen J, Chen SC-A, Rosen LB, Yi J, Sorrell TC, et al. Anti-granulocyte-macrophage colony-stimulating factor autoantibodies are a risk factor for central nervous system infection by Cryptococcus gattii in otherwise immunocompetent patients. MBio. (2014) 5:e00912–00914. doi: 10.1128/mBio.00912-14
61. Shibata Y, Berclaz PY, Chroneos ZC, Yoshida M, Whitsett JA, Trapnell BC. GM-CSF regulates alveolar macrophage differentiation and innate immunity in the lung through PU1. Immunity. (2001) 15:557–67. doi: 10.1016/S1074-7613(01)00218-7
62. Nishimura M, Yamaguchi E, Takahashi A, Asai N, Katsuda E, Ohta T, et al. Clinical significance of serum anti-GM-CSF autoantibody levels in autoimmune pulmonary alveolar proteinosis. Biomark Med. (2018) 12:151–9. doi: 10.2217/bmm-2017-0362
63. Piccoli L, Campo I, Fregni CS, Rodriguez BMF, Minola A, Sallusto F, et al. Neutralization and clearance of GM-CSF by autoantibodies in pulmonary alveolar proteinosis. Nat Commun. (2015) 6:7375. doi: 10.1038/ncomms8375
64. Ozyilmaz E, Gunasti S, Kuyuku Y, Polat S, Gumurdulu D, Kuleci S, et al. Hermansky pudlak syndrome and pulmonary alveolar proteinosis at the same patient: first case report in the world literature. Sarcoidosis Vasc Diffuse Lung Dis. (2013) 30:217–20.
65. Boerner EB, Costabel U, Wessendorf TE, Theegarten D, Hetzel M, Drent M, et al. Pulmonary alveolar proteinosis: another autoimmune disease associated with sarcoidosis? Sarcoidosis Vasc Diffuse Lung Dis. (2016) 33:90–4.
66. Osterholzer JJ, Chen G-H, Olszewski MA, Zhang Y-M, Curtis JL, Huffnagle GB, et al. Chemokine receptor 2-mediated accumulation of fungicidal exudate macrophages in mice that clear cryptococcal lung infection. Am J Pathol. (2011) 178:198–211. doi: 10.1016/j.ajpath.2010.11.006
67. Feldmesser M, Kress Y, Novikoff P, Casadevall A. Cryptococcus neoformans is a facultative intracellular pathogen in murine pulmonary infection. Infect Immun. (2000) 68:4225–37. doi: 10.1128/IAI.68.7.4225-4237.2000
68. Santiago-Tirado FH, Onken MD, Cooper JA, Klein RS, Doering TL. Trojan horse transit contributes to blood-brain barrier crossing of a eukaryotic pathogen. MBio. (2017) 8:e02183–16. doi: 10.1128/mBio.02183-16
69. Miller MF, Mitchell TG. Killing of Cryptococcus neoformans strains by human neutrophils and monocytes. Infect Immun. (1991) 59:24–8. doi: 10.1128/iai.59.1.24-28.1991
70. Chaturvedi V, Wong B, Newman SL. Oxidative killing of Cryptococcus neoformans by human neutrophils. Evidence that fungal mannitol protects by scavenging reactive oxygen intermediates. J Immunol. (1996) 156:3836–40.
71. Mednick AJ, Feldmesser M, Rivera J, Casadevall A. Neutropenia alters lung cytokine production in mice and reduces their susceptibility to pulmonary cryptococcosis. Eur J Immunol. (2003) 33:1744–53. doi: 10.1002/eji.200323626
72. Wozniak KL, Kolls JK, Wormley FL. Depletion of neutrophils in a protective model of pulmonary cryptococcosis results in increased IL-17A production by γδ T cells. BMC Immunol. (2012) 13:65. doi: 10.1186/1471-2172-13-65
73. Musubire AK, Meya DB, Rhein J, Meintjes G, Bohjanen PR, Nuwagira E, et al. COAT and ASTRO trial teams. Blood neutrophil counts in HIV-infected patients with cryptococcal meningitis: association with mortality. PLoS ONE. (2018) 13:e0209337. doi: 10.1371/journal.pone.0209337
74. Wiesner DL, Smith KD, Kashem SW, Bohjanen PR, Nielsen K. Different lymphocyte populations direct dichotomous eosinophil or neutrophil responses to pulmonary Cryptococcus infection. J Immunol. (2017) 198:1627–37. doi: 10.4049/jimmunol.1600821
75. Deerhake ME, Reyes EY, Xu-Vanpala S, Shinohara ML. Single-cell transcriptional heterogeneity of neutrophils during acute pulmonary Cryptococcus neoformans infection. Front Immunol. (2021) 12:670574. doi: 10.3389/fimmu.2021.670574
76. Sun D, Zhang M, Liu G, Wu H, Zhu X, Zhou H, et al. Real-time imaging of interactions of neutrophils with Cryptococcus neoformans demonstrates a crucial role of complement C5a-C5aR signaling. Infect Immun. (2016) 84:216–29. doi: 10.1128/IAI.01197-15
77. Gungor S, Akturk UA, Yalcinsoy M, Kocak ND, Goksenoglu NC, Altunbey SA, et al. What is the neutrophil/lymphocyte ratio in sarcoidosis? Bratisl Lek Listy. (2016) 117:152–5. doi: 10.4149/BLL_2016_030
78. Sugiyama K, Mukae H, Ishii H, Kakugawa T, Ishimoto H, Nakayama S, et al. Elevated levels of interferon gamma-inducible protein-10 and epithelial neutrophil-activating peptide-78 in patients with pulmonary sarcoidosis. Respirology. (2006) 11:708–14. doi: 10.1111/j.1440-1843.2006.00933.x
79. Cui A, Anhenn O, Theegarten D, Ohshimo S, Bonella F, Sixt SU, et al. Angiogenic and angiostatic chemokines in idiopathic pulmonary fibrosis and granulomatous lung disease. Respiration. (2010) 80:372–8. doi: 10.1159/000245332
80. Vasakova M, Sterclova M, Kolesar L, Slavcev A, Pohunek P, Sulc J, et al. Bronchoalveolar lavage fluid cellular characteristics, functional parameters and cytokine and chemokine levels in interstitial lung diseases. Scand J Immunol. (2009) 69:268–74. doi: 10.1111/j.1365-3083.2008.02222.x
81. Tutor-Ureta P, Citores MJ, Castejón R, Mellor-Pita S, Yebra-Bango M, Romero Y, et al. Prognostic value of neutrophils and NK cells in bronchoalveolar lavage of sarcoidosis. Cytometry B Clin Cytom. (2006) 70:416–22. doi: 10.1002/cyto.b.20120
Keywords: cryptococcal meningitis, sarcoidosis, innate immunity, humoral immune response, anti-GM-CSF autoantibodies
Citation: Prevel R, Guillotin V, Imbert S, Blanco P, Delhaes L and Duffau P (2022) Central Nervous System Cryptococcosis in Patients With Sarcoidosis: Comparison With Non-sarcoidosis Patients and Review of Potential Pathophysiological Mechanisms. Front. Med. 9:836886. doi: 10.3389/fmed.2022.836886
Received: 12 January 2022; Accepted: 02 March 2022;
Published: 29 March 2022.
Edited by:
Aleksandra Barac, University of Belgrade, SerbiaReviewed by:
Hossein Zarrinfar, Mashhad University of Medical Sciences, IranCopyright © 2022 Prevel, Guillotin, Imbert, Blanco, Delhaes and Duffau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pierre Duffau, cGllcnJlLmR1ZmZhdUBjaHUtYm9yZGVhdXguZnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.