 Nansi López-Valverde1,2
Nansi López-Valverde1,2 Bruno Macedo de Sousa3
Bruno Macedo de Sousa3 Antonio López-Valverde1,2
Antonio López-Valverde1,2 Ana Suárez4*
Ana Suárez4* Cinthia Rodríguez5Juan Manuel Aragoneses6
Cinthia Rodríguez5Juan Manuel Aragoneses6- 1Department of Surgery, University of Salamanca, Salamanca, Spain
- 2Instituto de Investigación Biomédica de Salamanca (IBSAL), Salamanca, Spain
- 3Institute for Occlusion and Orofacial Pain Faculty of Medicine, University of Coimbra, Coimbra, Portugal
- 4Department of Preclinical Dentistry, School of Biomedical Sciences, Universidad Europea de Madrid, Madrid, Spain
- 5Department of Dentistry, Universidad Federico Henríquez y Carvajal, Santo Domingo, Dominican
- 6Faculty of Dentistry, Universidad Alfonso X El Sabio, Madrid, Spain
Some research has suggested that dental plaque and saliva could be reservoirs of Helicobacter pylori (H. pylori) and be capable of infecting or re-infecting the gastric mucosa after eradication, with certain studies showing a significant association between PD and gastric infection by this bacterium. An electronic search was performed in PubMed, EMBASE, and Web of Science databases with the terms “Helicobacter pylori AND periodontal diseases”; “Helicobacter pylori AND gingivitis”; “Helicobacter pylori AND chronic periodontitis”; “Helicobacter pylori AND periodontitis”; “Helicobacter pylori AND dental plaque”, to identify articles up to September 2021. The Newcastle-Ottawa scale was used to assess study quality. A meta-analysis was performed using RevMan 2020 (Cochane Collaboration) software. A total of 1,315 studies were identified and 12 were included, analyzing 226,086 patients with mean age between 10.5 and 63.4 years. The prevalence of H. pylori in the oral cavity ranged from 5.4 to 83.3%. A random-effects model was used to analyze the presence of H. pylori and subgroups were made according to the method of evaluation (PCR or RUT). Statistical significance was found in the overall analysis (p = 0.01). There is no clear evidence that H. pylori present in oral bacterial plaque causes gastric infection and vice versa.
Systematic Review Registration: www.INPLASY.COM, identifier: INPLASY2021100097.
Introduction
Helicobacter pylori (H. pylori) is a gram-negative bacterium capable of producing one of the most common gastric bacterial infections in humans, affecting about half of the world's population and is the main cause of chronic gastritis, gastroduodenal ulcer, and adenocarcinoma of the stomach (1, 2). Despite treatment by systemic antibiotic therapy, certain patients have persistence of infection after treatment (3). Therefore, some researchers have suggested that both dental plaque and saliva could act as a reservoir and have implications for reinfection once the bacterium is eradicated from the gastric tract; some studies have even considered that the mouth could be a source of constant reinfection and that eradication of the bacterium from the oral cavity would be more difficult than from the gastrointestinal area (4, 5).
Similarly, periodontal diseases (PDs), are multifactorial infectious diseases, associated with a microbiota composed predominantly of gram-negative species, which show a close relationship with many systemic diseases and affect a high percentage of the elderly human population, presenting irreversible destruction of the supporting structures of the teeth (6, 7). The association between PDs and certain systemic diseases is explained by inflammation or immune response to periodontal pathogens (8). In recent years, using techniques such as polymerase chain reaction (PCR), DNA sequencing and hybridization, about 1,000 bacterial species have been found in the oral cavity (9, 10).
In 1996, 11 pathogens associated with periodontitis (P) were identified, of which three were strongly associated and eight were moderately associated (11). The initiation and spread of PDs is due to a dysbiosis of the oral commensal microbiota (dental plaque). However, periodontitis is considered a complex disease, with etiological factors acting at numerous levels: microbial, host, environmental and genetic, which may predispose or protect against the disease (12–14).
The association between PDs and gastro-duodenal ulcer has only been investigated in a limited number of studies, which have shown a significant association between both pathologies, even suggesting that patients with PDs, who harbor H. pylori in the oral cavity, would be subsidiary to suffer from gastric pathologies (15–18).
Therefore, the aim of this systematic review and meta-analysis was to identify and analyze clinical studies to determine the direct correlation between PDs and H. pylori gastric infection.
Materials and Methods
This systematic review and meta-analysis were reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (19). INSPLAY registration number: INPLASY2021100097. The PRISMA 2009 Checklist is reported in Supplementary Material (Supplementary Table 1).
The research question was elaborated using the PICOS strategy: Is there a correlation between PDs and H. pylori gastric infection? The population (P) was defined as subjects with PD; the intervention (I) was defined as the diagnosis of PD; the comparison group (C) corresponded to subjects without PD; the outcome (O) was defined as H. pylori gastric infection; and the study design (S) was defined to include non-interventional, cross-sectional, or case-control cohort studies. This review had no year restrictions.
Data Sources and Search Strategy
The PubMed, EMBASE and Web of Science (WOS) databases were searched to identify articles that were eligible until September 2021. The search terms used were: [MeSH terms] “Helicobacter pylori AND periodontal diseases,” [MeSH terms] “Helicobacter pylori AND gingivitis,” [MeSH terms] “Helicobacter pylori AND chronic periodontitis,” [MeSH terms] “Helicobacter pylori AND periodontitis” and [MeSH terms] “Helicobacter pylori AND dental plaque.” The Boolean operator “AND” was used to combine the searches. In addition, other articles were retrieved by hand searching recent reviews.
Data Extraction and Quality Assessment
Two authors independently read the titles and abstracts of the articles. The bibliographic references of each study were also reviewed as possible sources to identify additional studies. When there was any discrepancy between the two authors, a third author was consulted to establish a consensus.
The Newcastle-Ottawa Scale (NOS) (20) was applied to assess the quality of all studies. The NOS checklist contains three quality parameters: (i) selected population, (ii) comparability of groups, and (iii) assessment of exposure or outcome of interest for case-control or cohort studies. Each study was assigned a score from 0 to 9. Studies with a score ≥7 were considered high quality articles. Discrepancies in quality assessment were discussed and resolved by two authors (NL-V and AL-V). Any discrepancies were resolved by discussion with a third investigator. Studies with scores of nine to seven stars were considered to be of high quality, four to six stars of moderate quality, and one to three stars of poor quality and at high risk of bias.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows:
(a) Clinical studies that provided data on H. pylori infection in both the stomach and oral cavity, confirmed by polymerase chain reaction (PCR) or rapid urease test (RUT).
(b) Clinical studies that associated PDs with H. pylori. The diagnosis of PD was confirmed according to the diagnostic criteria in periodontology.
(c) Types of studies: cross-sectional studies, cohort studies, and case-control studies.
(d) Studies published in English.
Exclusion criteria were as follows:
(a) Studies that did not provide association data (H. pylori/PDs gastric infection).
(b) Studies that correlated H. pylori with oral pathologies other than PDs.
(c) Informative studies, clinical cases or studies published in languages other than English.
Statistical Analysis and Data Synthesis
The meta-analysis was performed with RevMan software (Review Manager (RevMan) [Software]. Version 5.4.1, The Cochrane Collaboration, 2020).
A meta-analysis based on Odds Ratio (OR) with 95% confidence intervals (CI) was performed for adverse event outcomes. Mean difference (MD) and standard deviation (SD) were used to estimate effect size. The random-effects model was selected because of the expected methodological heterogeneity in the included studies; furthermore, heterogeneity was interpreted as significant when the I2 value was >50% (21). The threshold for statistical significance was defined as p < 0.05. A funnel plot was used to assess publication bias.
Two subgroups were performed: one for studies using PCR as a diagnostic test for H. pylori and one for studies using RUT.
Results
Characteristics of Eligible Studies
A total of 1,315 articles were identified up to September 2021. Of the 1,315 studies searched, 1,256 (95.5%) papers were excluded by reviewing the abstract and title. After exclusion, a total of 12 eligible articles were included for analysis (22–33). Figure 1 (Flowchart) shows the article selection procedure. Eight of the selected studies were case-control (22–25, 27, 29, 30, 32) and four were cross-sectional studies (26, 28, 31, 33). Seven were conducted in the university setting (22, 23, 25, 28, 30, 31, 33) and six in hospital settings (24, 26, 27, 29, 32). The sample size ranged from 56 to 173,209 subjects; a total of 226,086 subjects were studied, with a mean age between 10.5 and 63.4 years. The prevalence of H. pylori in the oral cavity ranged from 5.4 to 83.3%. The characteristics of the included studies are shown in Tables 1, 2.
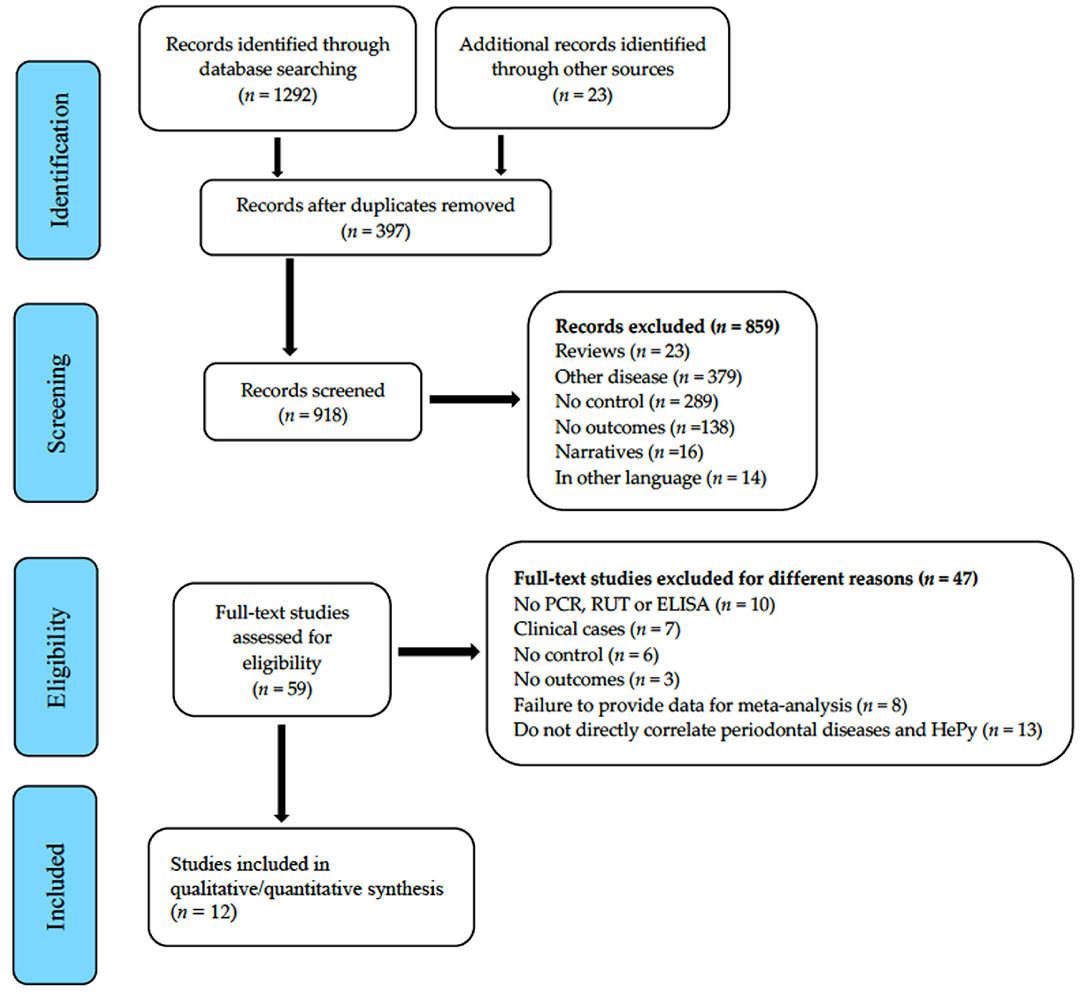
Figure 1. Flowchart.
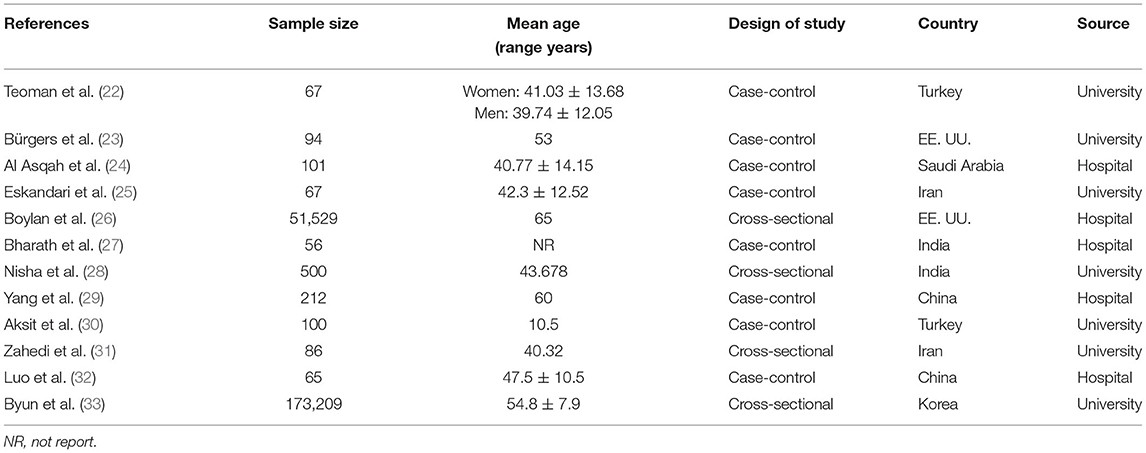
Table 1. Characteristics of studies.
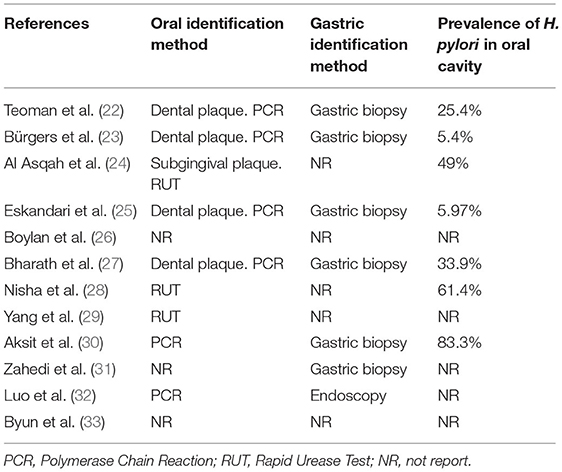
Table 2. Helicobacter pylori identification method and prevalence in oral cavity/plaque.
Quality of the Included Studies
Using the Newcastle-Ottawa scale, each study was assigned a score from 0 to 9. All studies scored ≥7 and were therefore of high quality. The highest score (9) was obtained by six of the twelve included studies (21, 22, 24, 28, 30, 31) and the lowest (7) by Boylan et al. (25) and Byun et al. (32) (Table 3).
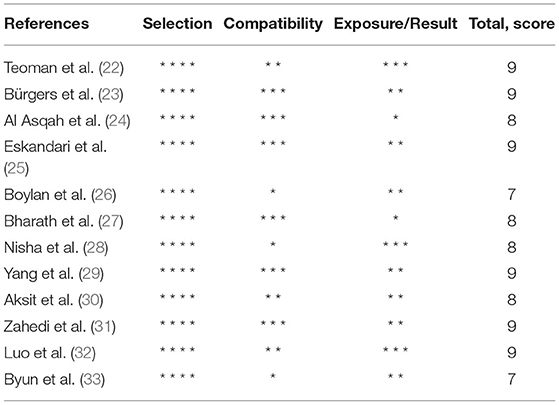
Table 3. Assessment of the quality of included studies using the Newcastle-Ottawa Scale.
Quantitative Synthesis (Meta-Analysis Results)
The same studies included in the qualitative synthesis were used to perform a meta-analysis comparing gastric H. pylori infection with the presence of the bacterium in the oral cavity. A forest plot was used to test the results. A meta-analysis of adverse outcomes could not be performed due to lack of data. Heterogeneity was very high (I2 = 92%), p = 0.01 indicating that patients with H. pylori gastric infection were positively associated with the presence of the bacteria in the oral cavity. The studies by Bharath et al. (27) and Luo et al. (32) had the highest weight (24 and 24.2%, respectively), due to sample size. The studies with the lowest weight were those of Al Asqah et al., Eskandari et al., Boylan et al., and Aksit et al. (24–26, 30) (Figure 2).
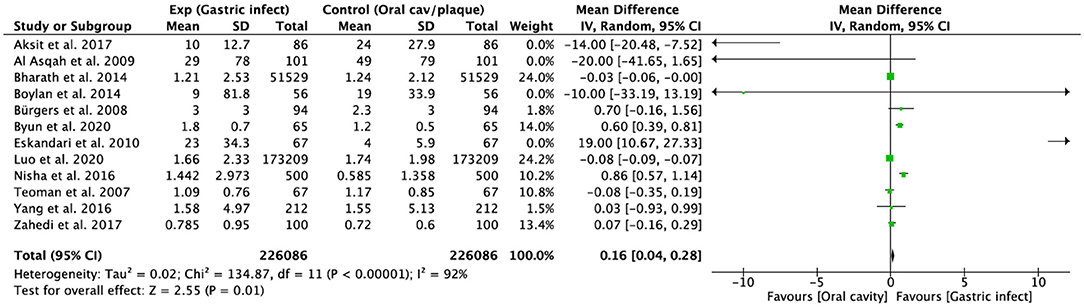
Figure 2. Forest plot of the prevalence of H. pylori gastric infection and oral cavity. SD, Standard Deviation; CI, Confidence Interval.
The subgroup analysis (studies that used PCR and studies that used RUT), presented greater heterogeneity (I2 = 99%) and no statistical significance was found (p = 0.11 for RUT and p = 0.15 for PCR) (Figure 3).
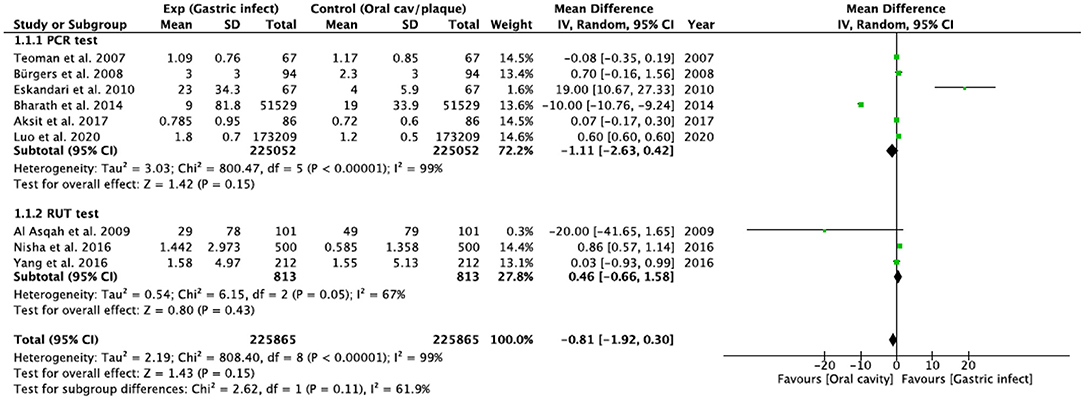
Figure 3. Subgroup analysis.
Publication Bias and Heterogeneity
The included studies showed important graphic signs of publication bias as can be seen in both Funnel Plots (Figures 4, 5).
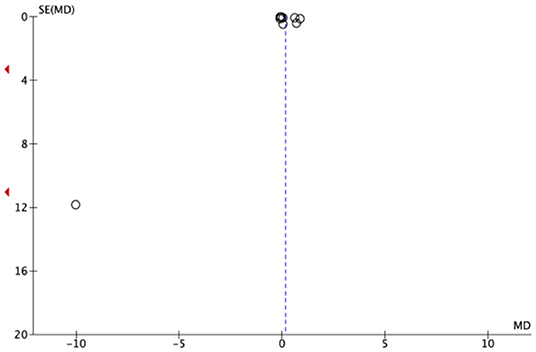
Figure 4. Funnel plot of all included studies.
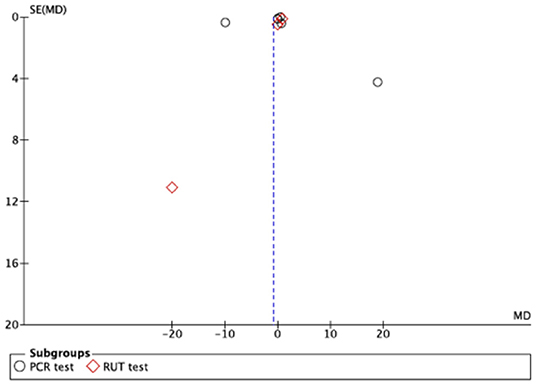
Figure 5. Funnel plot of subgroups.
Discussion
The aim of the present study was to answer the following question: To what extent are periodontal diseases capable of producing gastric infection by H. pylori? To quantify the potential effect of this ability, a meta-analysis of studies that assessed the bacteria in dental plaque was performed.
Helicobacter Pylori is a common bacterium that colonizes the gastric mucosa and is also considered by many researchers to be a risk factor for certain oral diseases, such as PDs, canker sores, squamous cell carcinoma, burning tongue and halitosis (34).
Both the oral cavity and the peridontal pockets have been hypothetically considered as one of the mechanisms of reinfection and recolonization of H. pylori and that, conversely, the chronically infected condition of PD could favor the colonization of periodontal pockets by H. pylori (35, 36). In turn, certain studies have pointed to the oral cavity as the main colonizer of H. pylori and subsequent gastric infection indicating that there is a relationship between the presence of H. pylori in the oral cavity and the severity of periodontal disease (37–39). There are serious discrepancies among researchers on the presence of H. pylori in the oral cavity. Doré-Davin et al. (40) reported figures of 41% for the presence of H. pylori in the oral cavity; other studies have even reported 97% positivity for H. pylori in dental plaque samples (41), on the contrary, some studies even associate H. pylori infection with a lower risk of PD (42) arguing a lower H. pylori infection in patients with severe atrophic gastritis or differences between men and women, as female hormonal fluctuations due to pregnancy or menopause affect periodontopathic bacterial flora, saliva volume and viscosity, and oral mucosal vascularization (43). In addition, during pregnancy, there is a neglect of oral hygiene, associated with frequent vomiting can lead to dental erosions and even periodontitis. All this together with a postmenopausal loss of bone density and dental loss (44, 45). Kadota et al. (46) found higher rates of Porphyromonas gingivalis, Treponema denticola, and Prevotella intermedia in H. pylori-positive subjects than in H. pylori-negative subjects, highlighting the incidence of H. pylori and many periodontopathic bacterial species increases with age and concluding that H. pylori can coexist with specific periodontopathic bacterial species, although the interactions between the two bacteria have not been demonstrated. Umeda et al. (15), in a study of 57 subjects, highlighted the importance of removing H. pylori from the mouth because of the danger of colonization in the stomach and the importance of paying special attention to patients with periodontitis who harbor H. pylori in the oral cavity. In this regard, some authors have suggested that H. pylori recolonized in the gastric mucosa from dental plaque would be resistant to systemic antimicrobial therapy (47). A retrospective case-control study on a large population-based sample (177,240 patients), with a prolonged follow-up period (13 years), concluded a positive association between gastroduodenal ulceration and PD (48).
A review by Anand et al. (34) on the prevalence of H. pylori in dental plaque ranged from 0 to 100%, highlighting that the wide variation in the results could be explained by several factors, such as the characteristics of the sample population, the different sampling procedures and the different methodologies used to detect the microorganism in dental plaque; in our meta-analysis, these data ranged from 5.4 to 83.3%, due to the same factors.
On the other hand, due to the biofilm properties of dental plaque, it offers resistance to systemic antimicrobial treatments, thus H. pylori is not susceptible to synthetically administered antimicrobial agents and periodontal therapies that remove microbial deposits from dental plaque, including H. pylori, have been proposed in this regard (49, 50).
The methods for detecting dental plaque are another source of controversy among the authors, giving rise to great heterogeneity of the studies considered. In our meta-analysis we have included studies that identified H. pylori by PCR (21, 22, 24, 26, 29) and RUT methods (23, 27, 28) and others that did not report method of identification (25, 30, 32). Certain authors have criticized the reliability of RUT for detecting H. pylori in dental plaque, because Streptococcus, Haemophilus, and Actinomyces species can be detected as part of the normal oral flora, despite the fact that H. pylori is the only known urease-positive microorganism resident in the stomach (51). A study in 88 patients, published by Chitsazi et al. (52) on the prevalence of H. pylori in dental plaque, using RUT, reported a prevalence of <40%, questioning the validity of urease testing for diagnosing H. pylori in gastric infection; furthermore, the study authors found no association between H. pylori in dental plaque and gastric infection. Other studies, on the contrary, consider the RUT as the test with the best sensitivity (92.16%), although with a lower specificity than the PCR test (53).
On the other hand, reading urease tests before the recommended time can falsify the results (54) and, in addition, in commercial kit designs, the density of bacteria present in the sample affects the diagnostic accuracy, requiring a minimum of 10,000 microorganisms for the RUT result to be reliable; other factors such as the presence of blood in the biopsies or contamination with formalin distort the results, decreasing the sensitivity of the RUT (55–59).
Unlike RUT, the PCR method is used not only for the detection of H. pylori, but also to characterize pathogenic genes and mutations associated with antimicrobial resistance (60). Today, many modifications of PCR technology have been developed to increase the sensibility of detection, even to increase sensitivity to 100% (61). In recent years, a new PCR system has been developed, which uses primer sets specific to 48 H. pylori strains in order to increase the diagnostic accuracy of PCR in the oral cavity; however, despite being a highly sensitive method, certain authors have drawn attention to its poor ability to detect small amounts of bacteria, depending on the specificity and sensitivity of the primer used, for example, primers related to bacterial urease activity often prove to be a confounding factor (62). Amiri et al. (63) described a highly specific and sensitive DNA amplification method for the detection of H. pylori in dental plaque samples, showing that it had a higher detection rate than PCR by 66.67 and 44%, respectively.
For all these reasons, there is great confusion among the scientific community and the evidence supporting the role of the oral cavity as a significant reservoir of H. pylori is inconclusive, and it is necessary to establish the reasons for such discrepancies.
Dowsett and Kowolik in a review article (51) questioned whether the reservoir of H. pylori in the oral cavity would be significant for subsequent gastric infection and that there should be a microenvironment capable of supporting H. pylori growth, such as pH, oxidation/reduction (redox) potential and nutrient availability adequate to maintain H. pylori.
Finallly, another factor to take into account would be the geographic distribution of both pathologies. Gastric infection can be acquired from environmental sources, but in most circumstances, it is probably acquired interpersonally, by the fecal-oral or oral-oral route, depending on the circumstances, although the former is likely to be the more important (64); in contrast, the transmission of periodontal diseases is unclear, with genetically distinct types of Porphyromonas gingivalis considered to be more associated with the disease than others, but further studies are needed to relate this to ethnic differences (65).
Our meta-analysis found a moderate statistical significance (p = 0.01), however, in the subgroup study, no statistical significance was found (p = 0.15). However, the “lack of statistical significance” does not point in a specific direction, since, in certain situations, the relevant effects are not “statistically significant,” since a given association, may not be clinically or epidemiologically relevant. Therefore, we consider, according to the studies consulted and evaluated in this meta-analysis, that there may be situations in which certain periodontal situations can influence H. pylori gastric infection and vice versa.
Nevertheless, this study had several limitations: the small number of studies included in the meta-analysis; the included studies analyzed the presence of H. pylori, both in the bacterial plaque and in the gastric mucosa, in different territories and different assessment methods were used; finally, some studies did not report data.
For all these reasons, we consider that the results obtained should be taken with caution.
Conclusions
The amount of H. pylori bacteria necessary to induce infection in the stomach is still unknown, as well as whether the presence of H. pylori in the mouth is transient and whether there are risk factors that favor its growth in the oral cavity.
Therefore, we believe that studies with well-designed and appropriate methodologies are needed to demonstrate a direct correlation between PDs and H. pylori gastric infection.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
NL-V and AL-V: conceptualization and writing—review and editing. JMA and BM: methodology. AL-V, CR, and AS: validation. NL-V: formal analysis. NL-V and BM: data curation. AL-V: supervision. All authors have read and agreed to the published version of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.822194/full#supplementary-material
References
1. Mladenova I. Clinical Relevance of Helicobacter pylori Infection. J Clin Med. (2021) 10:3473. doi: 10.3390/jcm10163473
2. Ribaldone DG, Zurlo C, Fagoonee S, Rosso C, Armandi A, Caviglia GP, et al. A retrospective experience of Helicobacter pylori histology in a large sample of subjects in Northern Italy. Life. (2021) 11:650. doi: 10.3390/life11070650
3. Fagoonee S, Pellicano R. Helicobacter pylori: molecular basis for colonization and survival in gastric environment and resistance to antibiotics. A short review. Infect Dis. (2019) 51:399–408. doi: 10.1080/23744235.2019.1588472
4. Brown LM. Helicobacter pylori: epidemiology and routes of transmission. Epidemiol Rev. (2000) 22:283–97. doi: 10.1093/oxfordjournals.epirev.a018040
5. Zou QH, Li RQ. Helicobacter pylori in the oral cavity and gastric mucosa: a meta-analysis. J Oral Pathol Med. (2011) 40:317–24. doi: 10.1111/j.1600-0714.2011.01006.x
6. Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet. (2005) 366:1809–20. doi: 10.1016/S0140-6736(05)67728-8
7. Hu Z, Zhang Y, Li Z, Yu Y, Kang W, Han Y, et al. Effect of Helicobacter pylori infection on chronic periodontitis by the change of microecology and inflammation. Oncotarget. (2016) 7:66700–12. doi: 10.18632/oncotarget.11449
8. Hajishengallis G. Immunomicrobial pathogenesis of periodontitis: keystones, pathobionts, host response. Trends Immunol. (2014) 35:3–11. doi: 10.1016/j.it.2013.09.001
9. Nabi N, Chaouachi M, Zellama MS, Ben Hafsa A, Mrabet B, Said K, et al. A new QRT-PCR assay designed for the differentiation between elements provided from Agrobacterium sp. in GMOs plant events and natural Agrobacterium sp. bacteria. Food Chem. (2016) 196:58–65. doi: 10.1016/j.foodchem.2015.09.015
10. Dewhirst FE, Chen T, Izard J, Paster BJ, Tanner AC, Yu WH, et al. The human oral microbiome. J Bacteriol. (2010) 192:5002–17. doi: 10.1128/JB.00542-10
11. Consensus Report. Periodontal diseases: pathogenesis and microbial factors. Ann Periodontol. (1996). 1:926–32. doi: 10.1902/annals.1996.1.1.926
12. Kinane DF, Stathopoulou PG, Papapanou PN. Periodontal diseases. Nat Rev Dis Primers. (2017) 3:17038. doi: 10.1038/nrdp.2017.38
13. Meyle J, Chapple I. Molecular aspects of the pathogenesis of periodontitis. Periodontology 2000. (2015) 69:7–17. doi: 10.1111/prd.12104
14. Hajishengallis G. Periodontitis: from microbial immune subversion to systemic inflammation. Nat Rev Immunol. (2015) 15:30–44. doi: 10.1038/nri3785
15. Umeda M, Kobayashi H, Takeuchi Y, Hayashi J, Morotome-Hayashi Y, Yano K, et al. High prevalence of Helicobacter pylori detected by PCR in the oral cavities of periodontitis patients. J Periodontol. (2003) 74:129–34. doi: 10.1902/jop.2003.74.1.129
16. Gülseren D, Karaduman A, Kutsal D, Nohutcu RM. The relationship between recurrent aphthous stomatitis, and periodontal disease and Helicobacter pylori infection. Clin Oral Investig. (2016) 20:2055–60. doi: 10.1007/s00784-015-1704-0
17. Tsimpiris A, Grigoriadis A, Tsolianos I, Moschos I, Goulis DG, Kouklakis G. Periodontitis and Helicobacter pylori infection: eradication and periodontal therapy combination. Eur J Dent. (2022) 16:145–52. doi: 10.1055/s-0041-1731928
18. Song HY, Li Y. Can eradication rate of gastric Helicobacter pylori be improved by killing oral Helicobacter pylori? World J Gastroenterol. (2013) 19:6645–50. doi: 10.3748/wjg.v19.i39.6645
19. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
20. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25:603–5. doi: 10.1007/s10654-010-9491-z
21. Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
22. Teoman I, Ozmeriç N, Ozcan G, Alaaddinoglu E, Dumlu S, Akyön Y, et al. Comparison of different methods to detect Helicobacter pylori in the dental plaque of dyspeptic patients. Clin Oral Investig. (2007) 11:201–5. doi: 10.1007/s00784-007-0104-5
23. Bürgers R, Schneider-Brachert W, Reischl U, Behr A, Hiller KA, Lehn N, et al. Helicobacter pylori in human oral cavity and stomach. Eur J Oral Sci. (2008) 116:297–304. doi: 10.1111/j.1600-0722.2008.00543.x
24. Al Asqah M, Al Hamoudi N, Anil S, Al Jebreen A, Al-Hamoudi WK. Is the presence of Helicobacter pylori in dental plaque of patients with chronic periodontitis a risk factor for gastric infection? Can J Gastroenterol. (2009) 23:177–9. doi: 10.1155/2009/950527
25. Eskandari A, Mahmoudpour A, Abolfazli N, Lafzi A. Detection of Helicobacter pylori using PCR in dental plaque of patients with and without gastritis. Med Oral Patol Oral Cir Bucal. (2010) 15:e28–31. doi: 10.4317/medoral.15.e28
26. Boylan MR, Khalili H, Huang ES, Michaud DS, Izard J, Joshipura KJ, et al. A prospective study of periodontal disease and risk of gastric and duodenal ulcer in male health professionals. Clin Transl Gastroenterol. (2014) 5:e49. doi: 10.1038/ctg.2013.14
27. Bharath TS, Reddy MS, Dhanapal R, Raj Kumar NG, Neeladri Raju P, Saraswathi T. Molecular detection and corelation of Helicobacter pylori in dental plaque and gastric biopsies of dyspeptic patients. J Oral Maxillofac Pathol. (2014) 18:19–24. doi: 10.4103/0973-029X.131885
28. Nisha KJ, Nandakumar K, Shenoy KT, Janam P. Periodontal disease and Helicobacter pylori infection: a community-based study using serology and rapid urease test. J Investig Clin Dent. (2016) 7:37–45. doi: 10.1111/jicd.12122
29. Yang J, Zhang Q, Chen M, Wu WZ, Wang R, Liu CJ, et al. Association between Helicobacter pylori infection and risk of periodontal diseases in Han Chinese: a case-control study. Med Sci Monit. (2016) 22:121–6. doi: 10.12659/MSM.894583
30. Aksit Bicak D, Akyuz S, Kiratli B, Usta M, Urganci N, Alev B, et al. The investigation of Helicobacter pylori in the dental biofilm and saliva samples of children with dyspeptic complaints. BMC Oral Health. (2017) 17:67. doi: 10.1186/s12903-017-0361-x
31. Zahedi L, Jafari E, Torabi Parizi M, Shafieipour S, Hayat Bakhsh Abbasi M, Darvish Moghadam S, et al. The Association between Oral Hygiene and Gastric Pathology in Patients with Dyspepsia: a Cross-Sectional Study in Southeast Iran. Middle East J Dig Dis. (2017) 9:33–8. doi: 10.15171/mejdd.2016.49
32. Luo W, Li Y, Luo Z, Xu B. Chronic atrophic gastritis aggravate chronic periodontitis with Helicobacter pylori infection and CD4+Th cytokines infiltration. Histol Histopathol. (2020) 35:665–72. doi: 10.14670/HH-18-187
33. Byun SH, Min C, Hong SJ, Choi HG, Koh DH. Analysis of the relation between periodontitis and chronic gastritis/peptic ulcer: a cross-sectional study using KoGES HEXA data. Int J Environ Res Public Health. (2020) 17:4387. doi: 10.3390/ijerph17124387
34. Adler I, Muino A, Aguas S, Harada L, Diaz M, Lence A, et al. Helicobacter pylori and oral pathology: relationship with the gastric infection. World J Gastroenterol. (2014) 20:9922–35. doi: 10.3748/wjg.v20.i29.9922
35. Anand PS, Kamath KP, Anil S. Role of dental plaque, saliva and periodontal disease in Helicobacter pylori infection. World J Gastroenterol. (2014) 20:5639–53. doi: 10.3748/wjg.v20.i19.5639
36. Salehi MR, Shah Aboei M, Naghsh N, Hajisadeghi S, Ajami E. A comparison in prevalence of Helicobacter pylori in the gingival crevicular fluid from subjects with periodontitis and healthy individuals using polymerase chain reaction. J Dent Res Dent Clin Dent Prospects. (2013) 7:238–43. doi: 10.5681/joddd.2013.038
37. Yee JKC. Are the view of Helicobacter pylori colonized in the oral cavity an illusion? Exp Mol Med. (2017) 49:e397. doi: 10.1038/emm.2017.225
38. Lauritano D, Cura F, Candotto V, Gaudio RM, Mucchi D, Carinci F. Periodontal pockets as a reservoir of Helicobacter pylori causing relapse of gastric ulcer: a review of the literature. J Biol Regul Homeost Agent. (2015) 29:123–6.
39. Tongtawee T, Wattanawongdon W, Simawaranon T. Effects of periodontal therapy on eradication and recurrence of Helicobacter pylori infection after successful treatment. J Int Med Res. (2019) 47:875–83. doi: 10.1177/0300060518816158
40. Doré-Davin C, Heitz M, Yang H, Herranz M, Blum AL, Corthesy-Theulaz I. Helicobacter pylori in the oral cavity reflects handling of contaminants but not gastric infection. Digestion. (1999) 60:196–202. doi: 10.1159/000007659
41. Song Q, Lange T, Spahr A, Adler G, Bode G. Characteristic distribution pattern of Helicobacter pylori in dental plaque saliva detected with nested PCR. J Med Microbiol. (2000) 49:349–53. doi: 10.1099/0022-1317-49-4-349
42. Shimoyama T, Higuchi H, Matsuzaka M, Chinda D, Nakaji S, Fukuda S. Helicobacter pylori infection is associated with a decreased risk of tooth loss in healthy Japanese men. Jpn J Infect Dis. (2013) 66:489–92. doi: 10.7883/yoken.66.489
43. Russell SL, Ickovics JR, Yaffee RA. Exploring potential pathways between parity tooth loss among American women. Am J Public Health. (2008) 98:1263–70. doi: 10.2105/AJPH.2007.124735
44. Straka M, Straka-Trapezanlidis M, Deglovic J, Varga I. Periodontitis and osteoporosis. Neuro Endocrinol Lett. (2015) 36:401–6.
45. Oziegbe EO, Schepartz LA. Is parity a cause of tooth loss? Perceptions of northern Nigerian Hausa women. PLoS ONE. (2019) 14:e0226158. doi: 10.1371/journal.pone.0226158
46. Kadota T, Hamada M, Nomura R, Ogaya Y, Okawa R, Uzawa N, et al. Distribution of Helicobacter pylori and Periodontopathic bacterial species in the oral cavity. Biomedicines. (2020) 8:161. doi: 10.3390/biomedicines8060161
47. Miyabayashi H, Furihata K, Shimizu T, Ueno I, Akamatsu T. Influence of oral Helicobacter pylori on the success of eradication therapy against gastric Helicobacter pylori. Helicobacter. (2000) 5:30–7. doi: 10.1046/j.1523-5378.2000.00004.x
48. Yu HC, Chen TP, Wei CY, Chang YC. Association between Peptic Ulcer Disease and Periodontitis: a nationwide population-based case-control study in Taiwan. Int J Environ Res Public Health. (2018) 15:912. doi: 10.3390/ijerph15050912
49. Gürbüz AK, Ozel AM, Yazgan Y, Celik M, Yildirim S. Oral colonization of Helicobacter pylori: risk factors and response to eradication therapy. South Med J. (2003) 96:244–7. doi: 10.1097/01.SMJ.0000051069.50950.2B
50. Gebara EC, Faria CM, Pannuti C, Chehter L, Mayer MP, Lima LA. Persistence of Helicobacter pylori in the oral cavity after systemic eradication therapy. J Clin Periodontol. (2006) 33:329–33. doi: 10.1111/j.1600-051X.2006.00915.x
51. Dowsett SA, Kowolik MJ. Oral Helicobacter pylori: can we stomach it? Crit Rev Oral Biol Med. (2003) 14:226–33. doi: 10.1177/154411130301400307
52. Chitsazi MT, Fattahi E, Farahani RM, Fattahi S. Helicobacter pylori in the dental plaque: is it of diagnostic value for gastric infection? Med Oral Patol Oral Cir Bucal. (2006) 11:E325–8.
53. Jalalypour F, Farajnia S, Somi MH, Hojabri Z, Yousefzadeh R, Saeedi N. Comparative evaluation of RUT, PCR and ELISA tests for detection of infection with Cytotoxigenic H. pylori. Adv Pharm Bull. (2016) 6:261–6. doi: 10.15171/apb.2016.036
54. Vaira D, Vakil N, Gatta L, Ricci C, Perna F, Saracino I, et al. Accuracy of a new ultrafast rapid urease test to diagnose Helicobacter pylori infection in 1000 consecutive dyspeptic patients. Aliment Pharmacol Ther. (2010) 31:331–8. doi: 10.1111/j.1365-2036.2009.04196.x
55. Malfertheiner P, Megraud F, O'Morain CA, Atherton J, Axon AT, Bazzoli F, et al. Management of Helicobacter pylori infection–the Maastricht IV/Florence consensus report. Gut. (2012) 61:646–64. doi: 10.1136/gutjnl-2012-302084
56. Siavoshi F, Saniee P, Khalili-Samani S, Hosseini F, Malakutikhah F, Mamivand M, et al. Evaluation of methods for H. pylori detection in PPI consumption using culture, rapid urease test and smear examination. Ann Transl Med. (2015) 3:11. doi: 10.3978/j.issn.2305-5839.2014.11.16
57. Choi YJ, Kim N, Lim J, Jo SY, Shin CM, Lee HS, et al. Accuracy of diagnostic tests for Helicobacter pylori in patients with peptic ulcer bleeding. Helicobacter. (2012) 17:77–85. doi: 10.1111/j.1523-5378.2011.00915.x
58. Ramírez-Lázaro MJ, Lario S, Casalots A, Sanfeliu E, Boix L, García-Iglesias P, et al. Real-time PCR improves Helicobacter pylori detection in patients with peptic ulcer bleeding. PLoS ONE. (2011) 6:e20009. doi: 10.1371/journal.pone.0020009
59. Mishra S, Singh V, Rao GR, Jain AK, Dixit VK, Gulati AK, et al. Detection of Helicobacter pylori in stool specimens: comparative evaluation of nested PCR and antigen detection. J Infect Dev Ctries. (2008) 2:206–10. doi: 10.3855/jidc.264
60. Isaeva G, Isaeva R. Molecular methods for the detection of Helicobacter pylori. Minerva Biotecnologica 2020. (2020) 32:182–7. doi: 10.23736/S1120-4826.20.02665-8
61. Ogaya Y, Nomura R, Watanabe Y, Nakano K. Detection of Helicobacter pylori DNA in inflamed dental pulp specimens from Japanese children and adolescents. J Med Microbiol. (2015) 64:117–23. doi: 10.1099/jmm.0.079491-0
62. Alagl AS, Abdelsalam M, El Tantawi M, Madi M, Aljindan R, Alsayyah A, et al. Association between Helicobacter pylori gastritis and dental diseases: a cross-sectional, hospital-based study in Eastern Saudi Arabia. J Periodontol. (2019) 90:375–80. doi: 10.1002/JPER.18-0289
63. Amiri N, Abiri R, Eyvazi M, Zolfaghari MR, Alvandi A. The frequency of Helicobacter pylori in dental plaque is possibly underestimated. Arch Oral Biol. (2015) 60:782–8. doi: 10.1016/j.archoralbio.2015.02.006
64. Leclerc H. Epidemiological aspects of Helicobacter pylori infection. Bull Acad Natl Med. (2006) 190:949–62. doi: 10.1016/S0001-4079(19)33277-7
Keywords: Helicobacter pylori, dental plaque, periodontal diseases, gastric infection, saliva
Citation: López-Valverde N, Macedo de Sousa B, López-Valverde A, Suárez A, Rodríguez C and Aragoneses JM (2022) Possible Association of Periodontal Diseases With Helicobacter pylori Gastric Infection: A Systematic Review and Meta-Analysis. Front. Med. 9:822194. doi: 10.3389/fmed.2022.822194
Received: 26 November 2021; Accepted: 14 March 2022;
Published: 19 April 2022.
Edited by:
Yi Hu, The First Affiliated Hospital of Nanchang University, ChinaReviewed by:
Rinaldo Pellicano, Molinette Hospital, ItalyShymaa Enany, Suez Canal University, Egypt
Silvia-Giono Cerezo, Instituto Politécnico Nacional (IPN), Mexico
Frederico Lages, Federal University of Minas Gerais, Brazil
Amirhooshang Alvandi, Kermanshah University of Medical Sciences, Iran
Copyright © 2022 López-Valverde, Macedo de Sousa, López-Valverde, Suárez, Rodríguez and Aragoneses. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Suárez, YW5hLnN1YXJlekB1bml2ZXJzaWRhZGV1cm9wZWEuZXM=