 Nancy Vicente-Alcalde
Nancy Vicente-Alcalde Esther Ruescas-Escolano2
Esther Ruescas-Escolano2 Carlos Franco-Paredes
Carlos Franco-Paredes José Tuells
José Tuells- 1Penitentiary Center Alicante II, General Secretariat of Penitentiary Institutions, Villena, Spain
- 2Servicio de Urgencias, Hospital Universitario del Vinalopó-Elche, Elche, Spain
- 3Division of Infectious Diseases, Department of Medicine, University of Colorado School of Medicine, Aurora, CO, United States
- 4Hospital Infantil de Mexico, Federico Gomez, Mexico City, Mexico
- 5Department of Community Nursing, Preventive Medicine and Public Health and History of Science, University of Alicante, Alicante, Spain
The rapid spread of highly transmissible respiratory infections in carceral settings occurs due to their conglomerate nature. The COVID-19 pandemic has resulted in large outbreaks in jails and prisons in many settings. Herein, we describe an outbreak of SARS-CoV2 infection in a prison in Alicante, Spain. Prior to January 2021, testing for coronavirus infection was not widely available in jails and prisons nationwide. Offering of testing services in Spanish carceral facilities, coincided with the deployment of COVID-19 vaccination in the larger community. However, COVID-19 vaccine role out of incarcerated individuals occurred later during the deployment plan. With the identification of the initial cases of this outbreak, two units of the facility were assigned for population management: one for inmates with confirmed infection by positive PCR detection of SARS-COV-2 infection in nasopharyngeal swabs. Inmates with confirmed exposure and thus considered close contacts were place in a second isolation unit. Functional quarantine was employed in some instances. A reactive testing strategy was instituted at baseline, and at 7 and 14 days of nasopharyngeal specimens by PCR. A total of 1,097 nasopharyngeal specimens were obtained for PCR testing during the outbreak, which lasted a total of 80 days between the index case the end of medical isolation of the last case. A total of 103 COVID-19 cases were identified during the outbreak. Of these, three inmates developed severe manifestations requiring hospitalization, and one died. Were identified, among which there were three hospitalized and one deceased. Among cases and confirmed contacts, we conducted close clinical monitoring, symptom screening, and daily temperature checks. The implementation of these interventions along with early medical isolation of cases, quarantining of contacts, and interval testing to detect presymptomatic or asymptomatic cases were instrumental in containing this outbreak.
Introduction
Since the onset of the COVID-19 pandemic, some of the largest clusters of SARS-CoV-2 infection have occurred in carceral settings in many regions of the globe During a pandemic, these facilities become epicenters of transmission due to their intrinsic architectural design placing and becoming tinderboxes of transmission since people are densely concentrated in populated cell blocks and dormitories. Most facilities are characterized by having substandard hygienic standards and poor air circulation resulting in a closed environment that creates the worst type of setting for curbing the spread of a highly contagious infection such as SARS-CoV-2. Additionally, jails and prisons frequently hold people with substantial vulnerability to have the worst clinical outcomes such as chronic medical conditions that place them at a higher risk of becoming ill and dying if becoming infected with respiratory pathogens. Numerous public health authorities have acknowledged that outbreaks of transmissible respiratory diseases are more common in correctional settings than in communities at large.
In response to the threat of the introduction of SARS-CoV-2 in correctional facilities and other conglomerate settings in the European region, the regional office of the World Health Organization (WHO/Europe) recommended Nation States to develop preparedness and response plans to prevent or mitigate COVID-19 outbreaks. Therefore, comprehensive public health approaches involving multiple stakeholders (i.e., government, public health organizations, and society) were developed in Spain to prevent the introduction of SARS-CoV-2 in prisons, limit the spread within them, and reduce the possibility of amplifying networks of transmission to the surrounding communities (1). Lessons learned from previous pandemics have demonstrated the crucial role of reinforcing adequate hygiene practices among incarcerated persons, correctional officers, staff, and visitors (2). Furthermore, social distancing strategies such as depopulation of jails and prisons, interruption of visitations, limitation of group activities and unit lockdowns have been used to reduce transmission once an outbreak is identified.
Prisons in Europe are not an exception from the conditions that increase the risk of exposure and transmission of COVID-19. Large numbers of incarcerated individuals are under immunized for diseases for which vaccines are routinely provided by national immunization programs; and most inmate populations also have a high prevalence of chronic medical conditions (2–4). In addition, it should be added that the transfer of prisoners from other facilities, visitations, and the entry or exit of staff working in the prisoners are a potential gateway for new reintroductions of COVID-19 outbreaks. As a result, many prisons in European countries have reported outbreaks during this pandemic (3).
Herein, we were therefore interested in providing an epidemiologic description of an outbreak of COVID-19 that occurred in early 2021 in the Alicante-II Penitentiary Center (CPAII) in Villena, Spain. We also offer a discussion of lessons learned and best practices that assisted public health authorities to control this outbreak. This information may prove useful for public health authorities in responding to future outbreaks of COVID-19 or other highly transmissible infectious pathogens in other carceral facilities in Spain and elsewhere.
Description of the COVID-19 Outbreak
The CPAII prison in Villena Spain houses 982 inmates residing in 15 pods or units. The number of correctional officers and staff that work in the facility covering different shifts is 442. The outbreak was identified in early January 2021, coinciding with a period in which the surrounding communities to the facility with the highest recorded number of COVID-19 cases in the area during this pandemic. The cumulative incidence of test positivity for SARS-CoV-2 by PCR for 14 days prior to the onset of the pandemic was 965 per 100,000 inhabitants in the region. In early January 2021, hospitals in the surrounding communities were overwhelmed and the cumulative number of cases and deaths in prisons nationwide were 1,073 and 5, respectively (5).
The first confirmed case of SARS-CoV-2 infection inside the CPAII facility was identified in an inmate in unit 11 who developed symptoms compatible with COVID-19 after a visitation by a family member from abroad (January 14, 2021). Ensuring adherence to preventive measures including mask wearing and hand hygiene by family members during prison visitations is a major challenge and contact with a visiting relative was likely the mode of transmission to index case. This inmate did not have any significant past medical history. Confirmatory testing of this index case was performed at a referral hospital. Through contact tracing in unit 11 where the index case was detected, we identified an additional 15 asymptomatic infections among inmates. In response to these findings, and to prevent further spread of the outbreak to other units, we submitted by January 18 an official notification of the outbreak to the local health department. This notification led to the quarantining of Unit 11 and the prison went into lockdown.
Despite the implementation of these interventions, we identified a second case of COVID-19 after prison medical services were notified in January 21 by an outside medical institution. This inmate tested positive for SARS-CoV-2 when undergoing a presurgical medical evaluation for an elective surgical procedure. After the prison was notified of this inmate positive testing, we conducted contact investigation in the two units where this individual had resided (units 4 and 7). Testing in these two units identified 64 cases of COVID-19 infection in unit 7; and five cases in unit 4. All infections were identified in asymptomatic individuals except for one individual in unit 4 with gastrointestinal symptoms. These two units were quarantined.
The third and last index case was observed in a prisoner from unit 13 who was evaluated in the prison's infirmary with fever and respiratory symptoms. This individual underwent testing with a rapid antigen test inside the prison. The patient had a past medical history of post-polio syndrome and obesity (body max index >35) and who developed rapidly progressive respiratory failure prompting his transfer to a referral hospital. Despite maximum support in an intensive care unit, he died a few days later. Contact tracing resulting from this case in unit 13 demonstrated an additional 16 cases of COVID-19, all of them asymptomatic. Unit 13 was also quarantined (Figure 1).
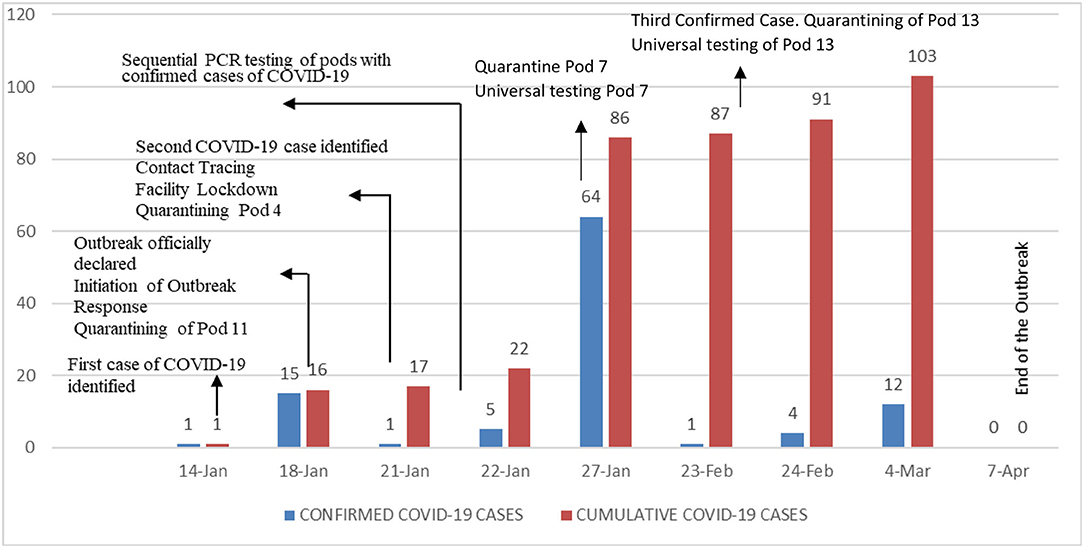
Figure 1. Timing of COVID-19 cases and institution of specific mitigation interventions.
During this outbreak, we identified 103 cases of COVID-19 corresponding to 10.48% of the prison population (982). Of the 103 cases, 7 (6.7%) were foreign born, 46 (44.6%) were smokers, 17 (16.5%) were hypertensive, 7 (6.7%) were diabetic, 4 were HIV positive, 4 had hepatitis C positive, and 5 suffered from chronic lung diseases. Only 3 cases were tested due to initial symptoms consistent with COVID-19, the rest were in asymptomatic individuals. Of the 103 cases, three were transferred to a referral hospital and one died. A total of 1,097 PCR tests were performed during the outbreak. Genomic sequencing demonstrated that the outbreak was due to the alpha variant (B1.1.7) of SARS-CoV-2. On April 7, 2021, public health authorities declared the COVID-19 outbreak over. The maximum number of days of two consecutive incubation periods were used to define the period to consider the end of the outbreak. After this outbreak, this prison has not seen any further reintroductions of SARS-CoV-2 (Table 1).
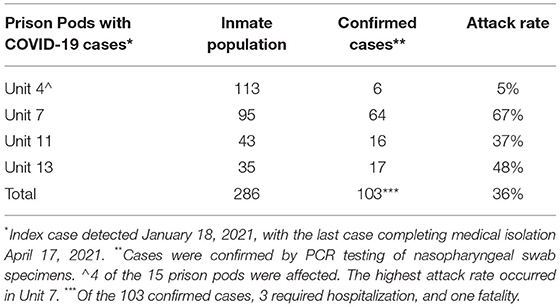
Table 1. Descriptive epidemiology of the COVID-19 outbreak in the CPAII prison in Alicante, Spain (January–April 2021).
Mitigation Strategies Implemented to Control the Outbreak
In addition to prevention measures such as the use of personal protective equipment such as mask wearing, hand hygiene, and physical distancing, we instituted temperature control protocols and daily symptom screens. We also paid attention to improving air circulation of common areas, frequent cleaning of frequently used surfaces, as we all intensified cleaning and disinfection protocols, appropriate waste management and other related facilities management interventions (Table 2).
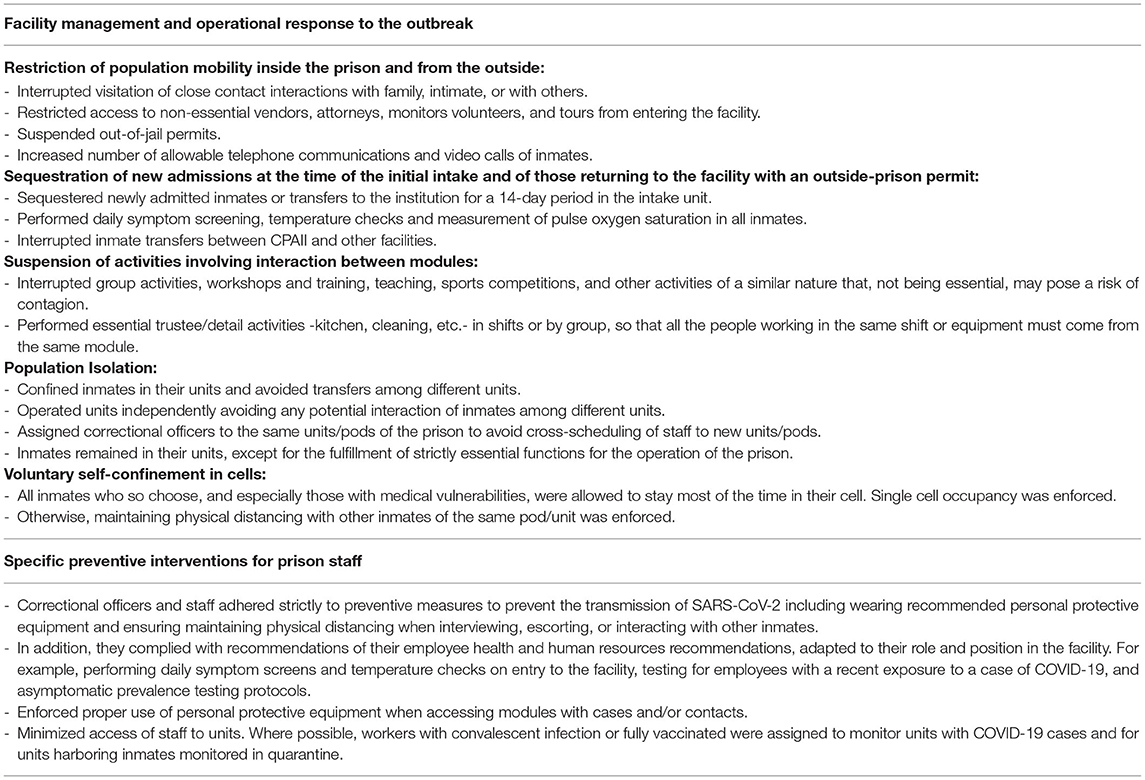
Table 2. Summary of interventions implemented during the COVID-19 outbreak in the CPAII Prison in Alicante, Spain (January-April 2021).
We developed internal protocols for the management of suspected cases, confirmed cases, and close contacts (Table 3). In parallel, measures were adopted to ensure adequate clinical management of confirmed cases according to mild, moderate or severe symptoms (Table 4), establishing when and how they should be referred to the reference hospital for specialized health care.
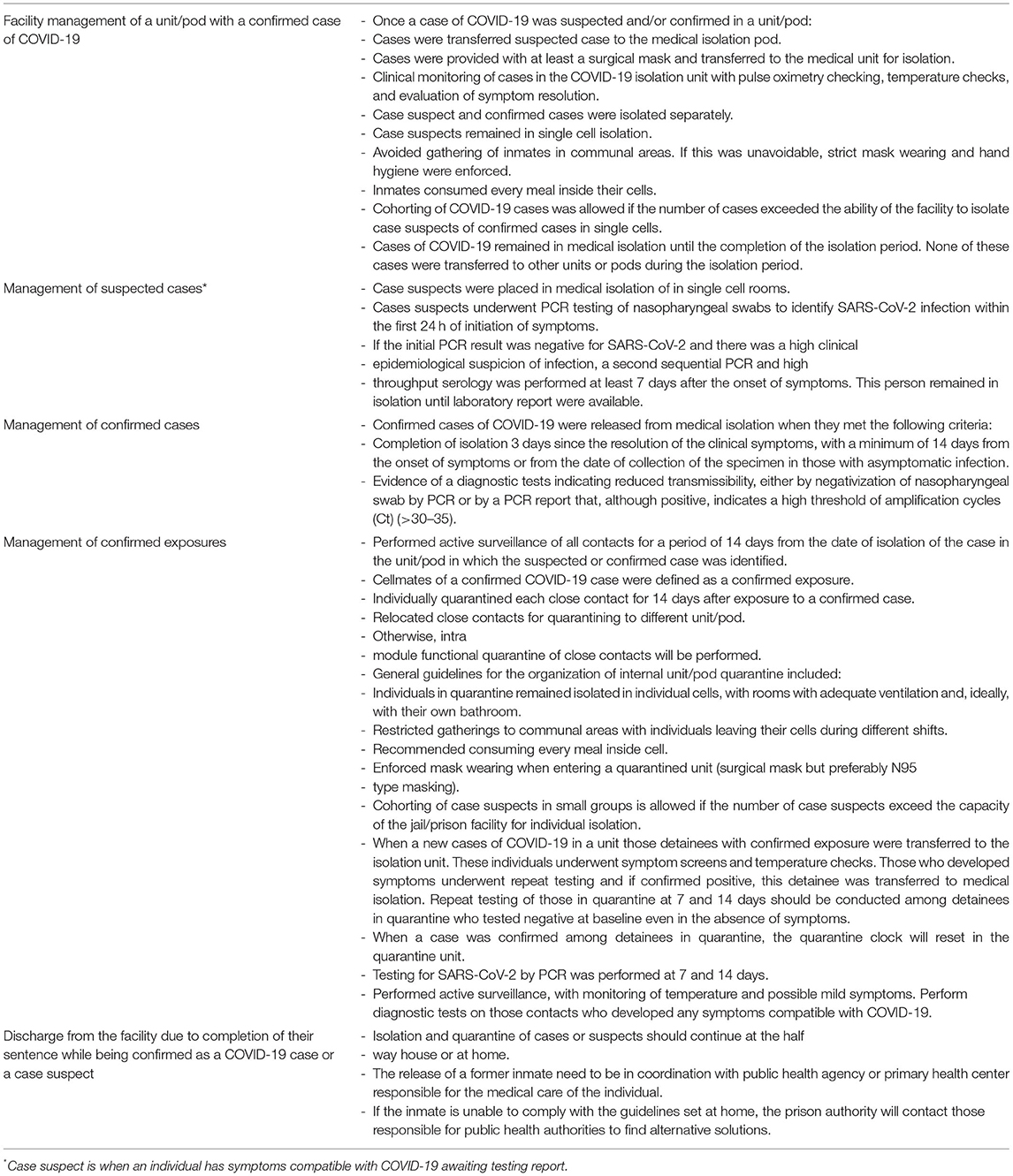
Table 3. Interventions implemented for the management of confirmed cases and close contacts during the COVID-19 outbreak in the CPAII Prison in Alicante, Spain (January-April 2021).
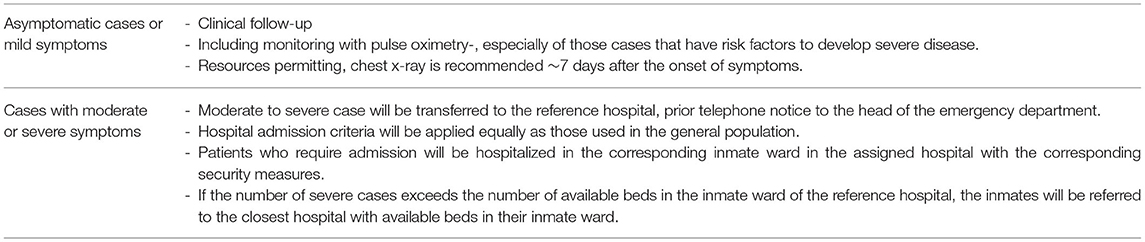
Table 4. Guidelines used for the clinical management of confirmed cases of COVID-19 according to clinical severity during the COVID-19 outbreak in the CPAII Prison in Alicante, Spain (January-April 2021).
Discussion
Detention and incarceration of any kind requires large groups of people to be confined together in a tight space. The COVID-19 pandemic has demonstrated the substantial impact of a rapidly spreading infectious pathogen leading to many cases, hospitalizations, and deaths in carceral settings. Prison settings are ideal for the development of COVID-19 outbreaks due to overcrowding and the high proportion of inmates with comorbidities (6–8). Since the beginning of the pandemic, outbreaks of this disease have been described in prisons around the world (9–12).
The outbreak involving this prison in the Valencian Community of Spain affected one tenth of the prison population. Except for three cases who require transferred to a referral hospital, most cases developed mild clinical manifestations and did not require hospitalization. Unfortunately, there was one fatality identified during this outbreak. At the time of the declaration of the outbreak, this facility did not have availability of diagnostic testing for SARS-CoV-2 infection. Most cases had at least one co-morbidity. The outbreak took place at a point where the prison population was not vaccinated. However, despite the limitations experienced at the beginning of the outbreak in terms of testing capabilities, the timely institution of mitigation strategies and population management allowed for controlling this outbreak in only 80 days.
According to the European Centre for Disease Control (ECDC), achieving COVID-19-free prisons requires ensuring strict implementation of public health recommendations. This could be achieved through continuous risk assessment, strict enforcement of infection prevention and control measures, ongoing educational programmes for incarcerated individuals and correctional officers. Collaboration between medical staff with local public health authorities is essential (13). In addition, the ECDC and WHO/Europe advise on special protective interventions for inmates that pose a greater risk for developing severe COVID-19 including older people, history of smoking, obesity, cardiovascular diseases and hypertension, chronic obstructive pulmonary disease, diabetes, chronic kidney disease, HIV infection, and other chronic medical conditions (14–19).
COVID-19 outbreaks in carceral settings are a public health priority, as they rapidly overload prison and community health services, spreading to surrounding communities and playing an important role in amplifying the pandemic. The limitations of health care in prisons and possible delays in transfers to hospitals increase the risk of negative medical outcomes (13). At present, the ratio of reference hospital security rooms occupied by inmates is very low. Medical protocols to provide care for incarcerated individuals are the same as for the general population.
In prisons, when there is an ongoing outbreak, maintaining social distancing, even as necessary, can be physically impossible when cells are shared and dining rooms and spaces for daily sociocultural activities are common (12, 20–22). Actions to reduce the prison population are crucial, such as delaying minor trials, advancing releases in prisoners with misdemeanors and, above all, providing for people at high risk of serious illness with alternative forms of custody such as community-based parole, if the jails and prisons do not guarantee inmate protection during this pandemic (20, 23, 24).
We instituted mitigation interventions promptly after the identification of the index case. Early and effective action during public health emergencies is vital to interrupt the spread of the outbreak, but the institution of these interventions in a timely fashion remains a major challenge due to the bureaucratic rigidity related to maintaining security in these facilities. Delayed in diagnosis and prompt medical management of severe cases have important negative consequences (7). There are different strategies for viral testing during an outbreak including universal testing, reactive testing, and prevalence testing (11). Similar to other conglomerate centers, testing of contacts even if asymptomatic is crucial to halt the spread of COVID-19 outbreaks (22, 25).
Facing an outbreak in a pandemic situation increases the needs of health care and public health actions in all environments, including jails, prisons and detention centers. The overload that is generated together with the limitation of the health infrastructures that prisons have, can mean insufficient provision of medical care to prisoners.
In many countries, responsibility for the provision of health care in prisons lies with the Ministry of Justice or the Ministry of the Interior and the Ministry of Health, which is why coordination and collaboration between the health and justice sectors is necessary to protect the health of people in prisons and thus reduce the disparities and health inequities experienced by prisoners in facing future outbreaks of COVID-19 in a carceral setting (26).
Protecting incarcerated individuals in jails and prisons during this pandemic is a public health priority. The risk for widespread contagion is exacerbated by the fact that staff, contractors, and vendors all pass between communities and correctional facilities, and each group can bring infectious diseases into and back out of those facilities. Additionally, correctional facility populations are constantly turning over, with many people flowing into and out of prisons every week. One study using data from the Cook County Jail in the United States found that jail cycling is a significant predictor of coronavirus infection, accounting for 55% of the variance in case rates across zip codes in Chicago and 37% in Illinois generally, with case rates much higher in zip codes with higher rates of arrest and released inmates (27).
Our study confirms that the isolation of both symptomatic and asymptomatic people, the early study of all contacts, the performance of PCR tests and the establishment of specific preventive measures were decisive in controlling the outbreak. In many settings, insufficient public health attention to carceral settings as hotspots of transmission responsible for large outbreaks inside jails and prison could have prevented many cases of COVID-19 and of COVID-19-related fatalities in correctional facilities. As the influenza pandemics of the 20th and 21st Centuries and the COVID-19 pandemic have shown, carceral settings are important epicenters of transmission of highly transmissible respiratory infections. As such, pandemic preparedness guidelines need to prioritize the role played by these facilities in amplifying cycles of transmission.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The study was approved by the General Secretary of Penitentiary Institutions, Sub-directorate General of Institutional Relations and Territorial Coordination (number 395714). The information was treated confidentially, and in accordance with Organic Law 3/2018, from December 5th, on Protection of Personal Data.
Author Contributions
NV-A, ER-E, CF-P, and JT designed the project, analyzed the data, drafted the manuscript, and gave final approval of the version to be published. NV-A and ER-E collected the data. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization (WHO) Regional Office for Europe. Preparedness, Prevention and Control of COVID-19 in Prisons and Other Places of Detention: Interim Guidance. Copenhagen: WHO-EURO (2020).
2. Stanley LL. Influenza at san quentin prison, California. Public Health Rep. (1919) 43:996–1008. doi: 10.2307/4575142
3. World Health Organization (WHO) Regional Office for Europe. Checklist to Evaluate Preparedness, Prevention and Control of COVID-19 in Prisons and Other Places of Detention. Copenhagen: WHO-EURO (2020).
4. Maruschak LM, Berzofsky M, Unangst J. Medical Problems of State Federal Prisoners Jail Inmates, 2011-12. (2015). Available online at: https://www.bjs.gov/content/pub/pdf/mpsfpji1112.pdf (accessed Jun 11, 2021).
5. Ministry of the Interior. COVID-19 Restrictions in Penitentiary Facilities. Available online at: https://www.institucionpenitenciaria.es/es/gabinete-de-prensa/ (accessed March 26, 2021).
6. Barnert E, Ahalt C, Williams B. Prisons: amplifiers of the COVID-19 pandemic hiding in plain sight. Am J Public Health. (2020) 110:964–6. doi: 10.2105/AJPH.2020.305713
7. Kinner S, Young J, Snow K, Southalan L, Lopez-Acuna D, Ferreira-Borges C, et al. Prisons and custodial settings are part of a comprehensive response to COVID19. Lancet Public Health. (2020) 5:e188–9. doi: 10.1016/S2468-2667(20)30058-X
8. Beaudry G, Zhong S, Whiting D, Javid B, Frater J, Fazel S. Managing outbreaks of highly contagious diseases in prisons: a systematic review. BMJ Glob Health. (2020) 5:e003201. doi: 10.1136/bmjgh-2020-003201
9. Burki T. Prisons are “in no way equipped” to deal with COVID-19. Lancet. (2020) 395:1411–2. doi: 10.1016/S0140-6736(20)30984-3
10. Government of China. China Concludes Investigation on Prison COVID-19 Outbreak. (2020). Available online at: http://www.china.org.cn/china/2020-03/04/content_75774142.htm (accessed June 15, 2021).
11. Wilburn J, Blakey E, Trindall A, Burr H, Tanti V, Doolan S, et al. COVID-19 within a large UK prison with a high number of vulnerable adults, march to june 2020: an outbreak investigation and screening event. Int J Infect Dis. (2021) 104:349–53. doi: 10.1016/j.ijid.2021.01.027
12. Giuliani R, Cairone C, Tavoschi L, Ciaffi L, Sebastiani T, Bartolotti R, et al. COVID-19 outbreak investigation and response in a penitentiary setting: the experience of a prison in Italy, February to April 2020. Euro Surveill. (2021) 26:2001385. doi: 10.2807/1560-7917.ES.2021.26.38.2001385
13. European Centre for Disease Prevention Control (ECDC). COVID-19 Vaccination Prioritisation Strategies in the EU/EEA. Stockholm: ECDC (2020).
14. United Nations (UN). UNODC, WHO, UNAIDS and OHCHR Joint Statement on COVID-19 in Prisons and Other Closed Settings. Vienna: UNODC, WHO, UNAIDS and OHCHR (2020).
15. Ministry of Health. Action Procedure for Occupational Risk Prevention Services Against Exposure to SARS-CoV-2. Madrid: Ministry of Health (2020).
16. Ministry of the Interior. Rules of Action for Public Prison Employees Who Work in a Penitentiary Center or Social Insertion Center and Who May Have Contact With People Likely to Have or Develop the Coronavirus Disease (SARS-CoV-2). Madrid: Ministry of the Interior, General Secretariat of Penitentiary Institutions (2020).
17. Ministry of the Interior and Ministry of Health. Recommendations in Prisons in Relation to COVID-19. Madrid: Ministry of the Interior, General Secretariat of Penitentiary Institutions and Ministry of Health (2020).
18. Ministry of Health. Report of the Ministry of Health on Ethical Aspects in Pandemic Situations: SARS-CoV-2. Madrid: Ministry of Health (2020).
19. Maner M, LeMasters K, Lao J, Cowell M, Nowotny K, Cloud D, et al. COVID-19 in corrections: quarantine of incarcerated people. PLoS ONE. (2021) 16:e0257842. doi: 10.1371/journal.pone.0257842
20. Amon J,. COVID-19 Detention: Respecting Human Rights. (2020). Available online at: https://www.hhrjournal.org/2020/03/covid-19-and-detention-respecting-human-rights/ (accessed October 29, 2021).
21. Hawks L, Woolhandler S, McCormick D. COVID-19 in prisons and Jails in the United States. JAMA Intern Med. (2020) 180:1041–2. doi: 10.1001/jamainternmed.2020.1856
22. Marco A, Gallego C, Pérez-Cáceres V, Guerrero RA, Sánchez-Roig M, Sala-Farré RM, et al. Public health response to an outbreak of SARS-CoV2 infection in a Barcelona prison. Epidemiol Infect. (2021) 149:e91. doi: 10.1017/S0950268821000789
23. Simpson P, Butler T. COVID-19, prison crowding, and release policies. BMJ. (2020) 369:m155. doi: 10.1136/bmj.m1551
24. Official State Gazette No. 134. Order INT/407/2020, of 12 of May, by Which Adopt Measures to Flexibilize the Restrictions Established in the Field of Penitentiary Institutions Under the Protection of the Royal Decree 463/2020, of 14 of March, by Which Declares the State of Alarm for the Management of the Situation of Sanitary Crisis Caused by the COVID-19. Available online at: https://www.boe.es/eli/es/o/2020/05/12/int407 (accessed October 30, 2021).
25. Gandhi M, Yokoe DS Havlir DV. Asymptomatic transmission, the achilles' heel of current strategies to control covid-19. New Engl J Med. (2020) 382:2158–60. doi: 10.1056/NEJMe2009758
26. Natoli LJ, Vu KL, Sukhija-Cohen AC, Engeran-Cordova W, Maldonado G, Galvin S, et al. Incarceration and COVID-19: recommendations to curb COVID-19 disease transmission in prison facilities and surrounding communities. Int J Environ Res Public Health. (2021) 18:9790. doi: 10.3390/ijerph18189790
Keywords: COVID-19, prisoners, prison health, outbreak investigation, PCR test
Citation: Vicente-Alcalde N, Ruescas-Escolano E, Franco-Paredes C and Tuells J (2022) Control of a COVID-19 Outbreak in a Spanish Prison: Lessons Learned in Outbreak Control. Front. Med. 9:806438. doi: 10.3389/fmed.2022.806438
Received: 31 October 2021; Accepted: 18 February 2022;
Published: 22 March 2022.
Edited by:
Lara Tavoschi, University of Pisa, ItalyReviewed by:
Alina Deshpande, Los Alamos National Laboratory (DOE), United StatesLinda Montanari, European Monitoring Centre for Drugs and Drug Addiction, Portugal
Copyright © 2022 Vicente-Alcalde, Ruescas-Escolano, Franco-Paredes and Tuells. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Tuells, dHVlbGxzQHVhLmVz