 Nadia Cubas-Vega1,2
Nadia Cubas-Vega1,2 Paola López Del-Tejo1,2
Paola López Del-Tejo1,2 Djane C. Baia-da-Silva1,2,3
Djane C. Baia-da-Silva1,2,3 Vanderson Souza Sampaio1,2,4,5
Vanderson Souza Sampaio1,2,4,5 Bruno Araújo Jardim2
Bruno Araújo Jardim2 Monique Freire Santana1,2
Monique Freire Santana1,2 Luiz Carlos Lima Ferreira1,2,6,7Izabella Picinin Safe1,2,7
Luiz Carlos Lima Ferreira1,2,6,7Izabella Picinin Safe1,2,7 Márcia A. Araújo Alexandre7
Márcia A. Araújo Alexandre7 Marcus Vinícius Guimarães Lacerda1,2,3,7
Marcus Vinícius Guimarães Lacerda1,2,3,7 Wuelton Marcelo Monteiro1,2
Wuelton Marcelo Monteiro1,2 Fernando Val1,2,5,7*
Fernando Val1,2,5,7*- 1Programa de Pós-Graduação em Medicina Tropical, Universidade do Estado do Amazonas, Manaus, Brazil
- 2Instituto de Pesquisa Clínica Carlos Borborema, Fundação de Medicina Tropical Dr. Heitor Vieira Dourado, Manaus, Brazil
- 3Instituto Leônidas and Maria Deane, Fiocruz-Amazonas, Manaus, Brazil
- 4Gerência de Endemias, Fundação de Vigilância em Saúde do Amazonas, Manaus, Brazil
- 5Programa de Pós-Graduação em Ciências da Saúde, Universidade Federal do Amazonas, Manaus, Brazil
- 6Departameto de Patologia e Medicina Legal, Universidade Federal do Amazonas, Manaus, Brazil
- 7Departamento Clínico, Fundação de Medicina Tropical Dr. Heitor Vieira Dourado, Manaus, Brazil
Background: Evidence on the optimal time to initiate antiretroviral therapy (ART) in the presence of toxoplasmic encephalitis (TE) is scarce. We compared the impact of early vs. delayed ART initiation on mortality and neurologic complications at discharge in a Brazilian population co-infected with HIV and TE.
Methods: We retrospectively evaluated data from 9 years of hospitalizations at a referral center in Manaus, Amazonas. All ART-naïve hospitalized patients were divided into early initiation treatment (EIT) (0-4 weeks) and delayed initiation treatment (DIT) (>4 weeks). The groups were compared using chi-square test and mortality at 16 weeks.
Results: Four hundred sixty nine patients were included, of whom 357 (76.1%) belonged to the EIT group. The median CD4+ lymphocyte count and CD4+/CD8+ ratio were 53 cells/mm3 and 0.09, respectively. Mortality rate and presence of sequelae were 4.9% (n = 23) and 41.6% (n = 195), respectively. Mortality was similar between groups (p = 0.18), although the EIT group had the highest prevalence of sequelae at discharge (p = 0.04). The hazard ratio for death at 16 weeks with DIT was 2.3 (p = 0.18). The necessity for intensive care unit admission, mechanical ventilation, and cardiopulmonary resuscitation were similar between groups.
Conclusion: In patients with AIDS and TE, early ART initiation might have a detrimental influence on the occurrence of sequelae.
Introduction
Toxoplasmic encephalitis (TE), caused by the intracellular protozoan parasite Toxoplasma gondii, is the most common central nervous system (CNS) opportunistic infection (OI) of people living with the human immunodeficiency virus (PLHIV) (1–3). If left untreated, it is a life-threatening condition that may cause different cognitive, psychological, and physical sequelae (4, 5). In Brazil, where clinical management of HIV/AIDS is provided free of charge (6), and despite the fact that the advent of highly active antiretroviral therapy (ART) has significantly decreased the morbidity and mortality of HIV/AIDS (7–9) in the past years, the prevalence of TE is a major cause of hospitalization in PLHIV and still represents a challenge for the healthcare system (10, 11). The treatment of patients with HIV and acute neurological infections (ANI) is challenging and the optimal timing to initiate ART remains a topic of major discussion (12–14).
The Brazilian Ministry of Health recommends the early initiation of ART in all PLHIV, regardless of symptoms and CD4+ T cell count, except for those with active meningeal tuberculosis and cryptococcal meningoencephalitis. In these patients, ART should be postponed 4 and 6 weeks after the initiation of tuberculous and fungal treatment, respectively (6). Similar approaches to the initiation of ART in PLHIV can be found in recommendations provided by international panels of experts (15, 16). Studies and data on when to start ART for PLHIV with TE and its impact are scarce. In this study, we aimed to compare major clinical outcomes of early vs. delayed ART initiation time in ART-naïve patients with HIV-associated TE who were admitted to an infectious disease referral center in the Amazonas state, Western Brazilian Amazon.
Materials and Methods
Study Design and Participants
This study collected retrospective data from HIV-infected patients with a clinical/radiological diagnosis of TE admitted to the Fundação de Medicina Tropical Dr Heitor Vieira Dourado (FMT-HVD) between January 2010 and December 2018. FMT-HVD is a tertiary-care referral hospital for infectious diseases located in Manaus, Western Brazilian Amazon, which receives patients seeking medical care as well as those referred from public and private health care units in surrounding localities. FMT-HVD is part of the Brazilian public health network and adopts all Brazilian guidelines for the management of sexually transmitted infections (17) and HIV infection (6). Clinical assistance, diagnostic tests, treatment, and follow-up are free of charge to all Brazilians and foreigners.
All patients are registered in the hospital's electronic medical record (EMR), the IDoctor platform, from which data were collected after a thorough screening process. Data on demographics, clinical, radiological and/or laboratory diagnosis of TE, length of hospitalization and any supportive procedures [intensive care unit (ICU), mechanical ventilation (MV), cardiopulmonary resuscitation (CPR)] and outcome (alive or dead) were retrieved from individual EMRs and sent anonymously to the databank. Selection of eligible participants for analysis is shown in Figure 1.
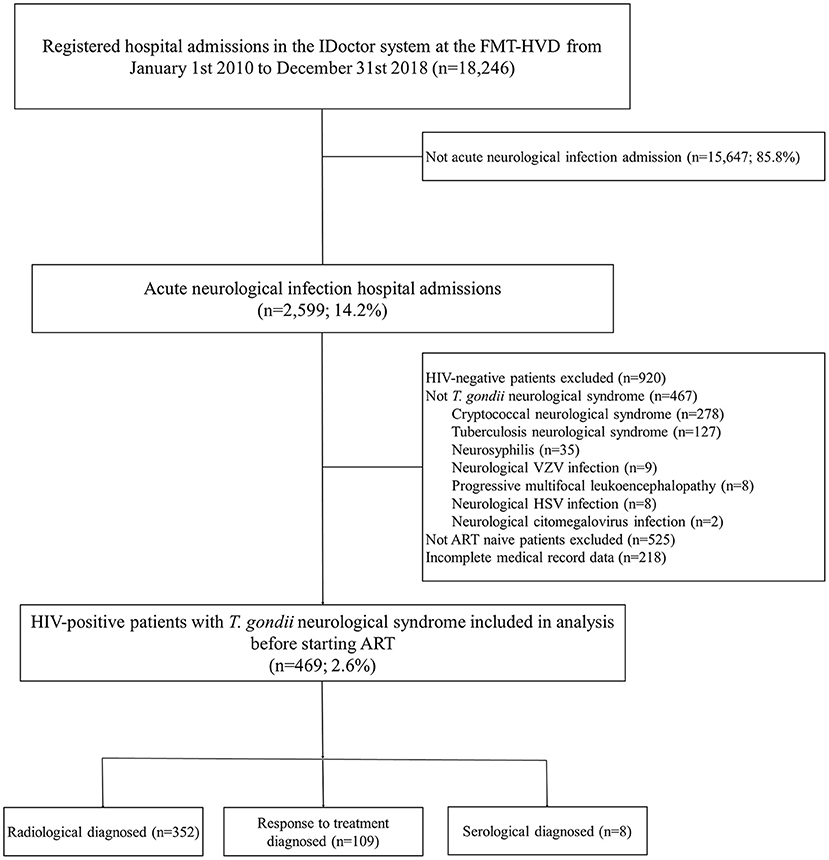
Figure 1. Study flowchart of inclusion of ART-naïve hospitalized patients co-infected with HIV and T. gondii encephalitis.
HIV infection was determined by two different consecutive positive 3rd generation rapid tests (RTs, Abon Alere [Abbott, Chicago, United States] and Bio-Manguinhos [Fiocruz, Rio de Janeiro, Brazil]), and confirmed by an immunoassay test, as defined by the Brazilian Ministry of Health (18). TE was defined by a clinically compatible presentation, most frequently described as headache, focal neurological deficit, fever, mental confusion and seizures (11, 19), either alone (after exclusion of other causes) nor in addition to computerized tomography (CT) or magnetic resonance imaging (MRI) compatible findings (enhancing brain lesions with perilesional edema, with or without expansive effect), serology for Anti-T. gondii IgG and/or IgM antibodies, and a satisfactory response after specific treatment (pyrimethamine, sulfadiazine, and folinic acid, or any other recommended by national guidelines) (6).
Only new episodes of TE were registered. If a patient had other hospitalizations registered in the database due to the same cause, they were considered a duplicate, and excluded. The first laboratory data (hematology and biochemistry) after admission and either the first CD4+, CD8+, and viral loads counts after admission (newly diagnosed HIV infection) or the most recent pre-admission CD4+, CD8+, and viral loads counts (people already living with HIV at the time of TE diagnosis) were recorded. Data collection was carried out by two independent researchers. Any disagreements were resolved by consensus.
Outcome Assessments
The included patients were divided into groups according to the ART initiation time as described elsewhere (14). Briefly, early initiation treatment (EIT) and delayed initiation treatment (DIT) referred to ART starting within the first 4 weeks (28 days) or after 4 weeks (>28 days) of TE diagnosis, respectively. Only ART-naïve patients who had available information regarding ART initiation time on the EMRs were included in this study (Figure 1). Early or delayed initiation of treatment followed the physician's discretion. Deciding which antiretroviral regimen to use was guided by the local protocols in use at the time (6, 20, 21).
The primary study outcome was in-hospital death. Secondary outcomes were the presence of sequelae at hospital discharge, need for ICU, MV, CPR, and number of hospitalization days. Neurological sequelae recorded in the study were defined as the presence until medical discharge, of one or more of the baseline signs or symptoms or the development of a new one; and for their evaluation the last medical statement prior to discharge was reviewed. Patients were followed up until hospital discharge or time of in-hospital death.
Statistical Analysis
Socio-demographic and clinical characteristics of patients were summarized as mean and standard deviation (SD) when distributions were confirmed as normal. Otherwise, data were expressed as medians and interquartile ranges (IQR). Categorical variables are reported as frequency and percentage. Comparative statistics between ART initiation groups were performed using Chi-square test for categorical variables and the Wilcoxon test or the Student's t-test for continuous variables. Shapiro-Wilk test was used to verify normality. Mortality at 16 weeks was compared between groups with the use of Peto-Peto-Prentince test and Cox-regression, which was performed to derive the hazard ratio (HR) two-sided 95% confidence intervals (CI) and represented with Kaplan-Meier curves. Each patient's survival time began on the date of hospitalization and ended on the date of death or hospital discharged. All data were analyzed using Stata® version 13 (StataCorp., College Station, Texas, United States). Statistical significance was set as a value of p < 0.05.
Ethical Considerations
The study protocol was approved by the FMT-HVD Ethics Review Board (ERB) (approval number 3.085.269/2018). Due to the retrospective nature of data collection and analysis, the ERB granted a waiver of the requirement to obtain informed consent.
Results
Study Population
A total of 2,599 patients were diagnosed with an acute neurological infection during the study period. Of these, 469 (18.0%) were ART-naïve HIV-TE patients (Figure 1). HIV cases per year are shown in Supplementary Figure 1, along with a timeline describing the changes in ART outlined by the Brazilian Ministry of Health throughout the study period. Table 1 summarizes baseline characteristics and outcomes. Men (n = 339, 72.3%), with a median age of 35 years (IQR: 28-44) and living in an urban area (n = 443, 94.5%) were the most affected. Headache (n = 315, 67.2%), limb paresis (n = 295, 62.9%) and altered consciousness level (n = 230, 49.0%) were the most frequent neurological signs at hospitalization. Clinical presentation at admission and laboratory baseline data are shown in Supplementary Table 1. Fifty-eight (12.4%) individuals were aware of the HIV status, with the time interval between HIV diagnosis and neurological clinical manifestation ranging from 1 month to 11 years. A total of 357 (76.1%) individuals were EIT, with a median time between hospital admission and ART initiation of 10 days (IQR: 5–16 days); 112 (23.9%) were in the DIT group (median ART initiation time 62 days, IQR: 40-221).
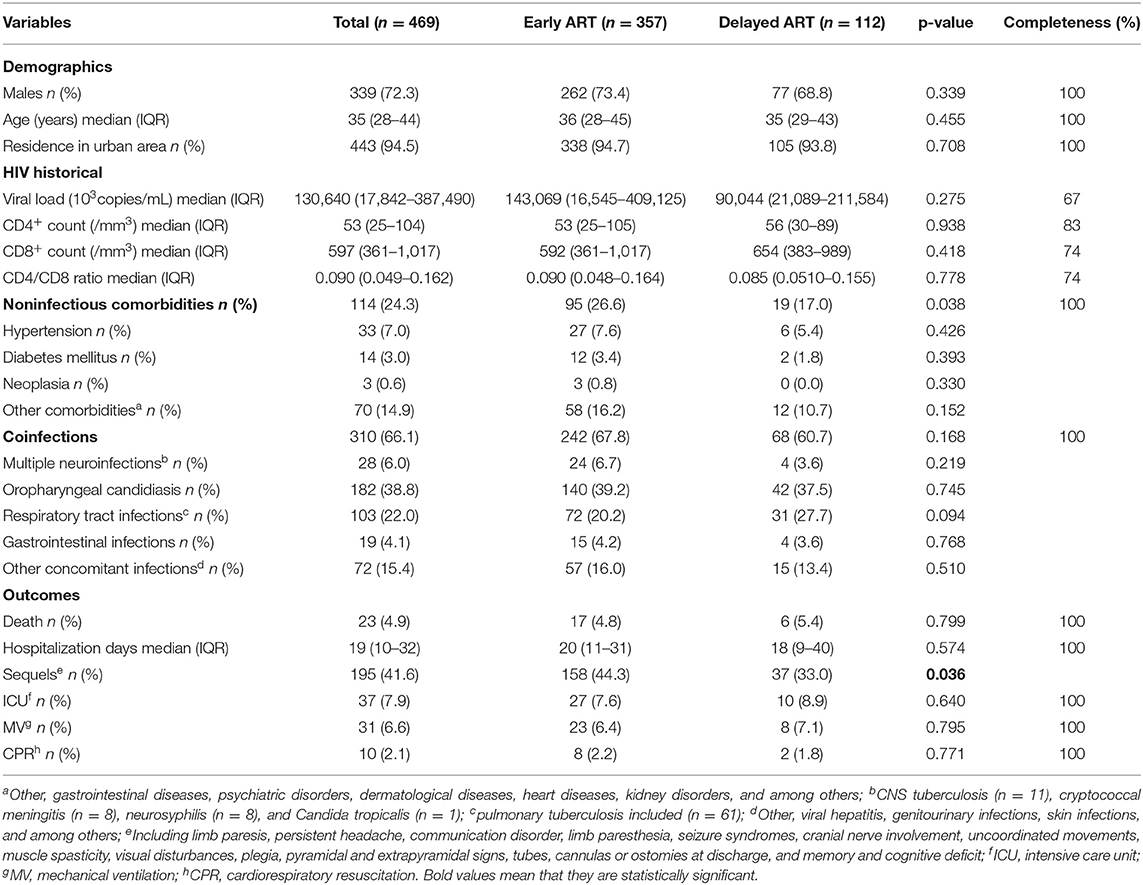
Table 1. Baseline characteristics and outcome according to ART initiation time.
Diagnosis and Treatment
A total of 352 (75.0%) patients were diagnosed from radiological findings, 8 (1.7%) had positive IgM (7 with positive IgG), and 109 (23.3%) diagnosed according to clinical signs and symptoms and response to treatment (Figure 1). Of the total patients, 296 (63.1%) had information on serology for T. gondii, out of these, 290 (98.0%) had evidence of previous exposure to the disease with positive IgG quantitatively performed by chemiluminescent immunoassay (DiaSorin S.p.A., Saluggia, Italy).
Three hundred and ten (66.1%) patients presented different coinfections; among those, 28 (9.0%) were diagnosed by the treating physicians with more than one infectious agent responsible for the neurological infection, all of them with two simultaneous etiological agents (Table 1). Pyrimethamine, sulfadiazine, and folinic acid (n = 398, 84.9%) were the most common drugs used for TE treatment. In 151 (32.2%) individuals, corticosteroids were used as adjuvant therapy, without significant difference of distribution between groups (p = 0.80). A combination of nucleoside/nucleotide reverse transcriptase inhibitors (NRTIs) and non-nucleoside reverse transcriptase inhibitors (NNRTIs) were the most frequently used ART in both groups (EIT: n = 229, 64.1% and DIT: n = 76, 67.9%) (Supplementary Table 2), without significant association with the development of sequelae (p = 0.21) or progression to death (0.96). No statistical association was found between death rate and corticosteroid use (p = 0.24).
Study Outcomes
The overall mortality was 4.9% (23/469), with higher mortality in the DIT group (5.4%, 6/112, Table 1), however, without statistical significance (p = 0.80). The overall sequelae rate was 41.6% (n = 195), with a higher prevalence of sequelae in the EIT group (158/357; 44.3%) compared to DIT (37/112, 33.0%), p = 0.04. The most prevalent sequelae at discharge were limb paresis (n = 105, 22.4%), followed by recurrent headaches with 11.1% (n = 52) (Supplementary Table 3). No statistical significance was found in the distribution for the need for ICU, MV, and CPR (Table 1). In general, the median length of survival time from admission was 28 weeks (IQR: 18–34). The HR for death at 16 weeks for the DIT group was 2.3 (95%CI 0.68–8.07; p = 0.17) (Figure 2).
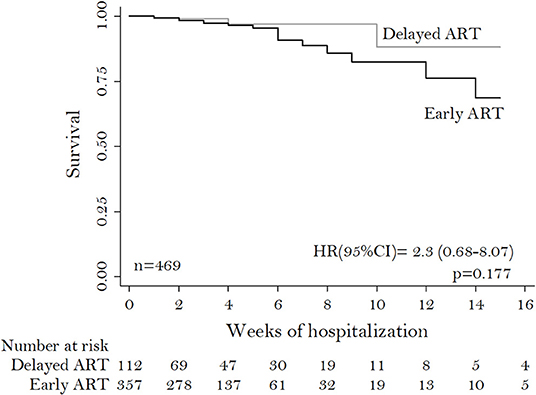
Figure 2. Kaplan-Meier curve of survival of ART-naïve hospitalized patients co-infected with HIV and T. gondii encephalitis.
Discussion
Opportunistic infections (OIs) are the leading cause of mortality in the HIV population (22). Currently, the evidence to guide ART initiation time in PLHIV in low- and middle-income countries co-infected with OIs is limited and based on studies with different socioeconomic and demographic characteristics (23, 24), as also documented in this study. In these countries, scientific research is limited (25, 26) and management of infectious diseases is challenging (27, 28). To our knowledge, not many studies investigate the association between timing of ART initiation and mortality and prevalence of sequelae in hospitalized patients with HIV and TE, regardless of the potential for CNS infections to cause cognitive and/or motor sequelae (5, 29). Our findings indicate that mortality was similar in both groups, but the prevalence of sequelae was lower in those who started ART after 4 weeks, which suggests an association with a better clinical sequelae profile when starting ART in a delayed manner in this population.
The population in our study has three notable characteristics (i) ART-naïve HIV individuals, (ii) the occurrence of TE as an influential factor on the decision to start ART early or administer treatment for the coinfections first, and (iii) a large proportion of patients who at the time of inclusion in the study already had advanced HIV/AIDS disease, with low CD4+ lymphocyte count and CD4+/CD8+ ratio, and a high viral load. The presence of an ANI in ART-naive patients will always bring major therapeutic challenges associated with the possibility of developing immune reconstitution inflammatory syndrome (IRIS) (30, 31) and complex pharmacokinetic interactions and pharmacological co-toxicities (32, 33), which not only occur between ART and coinfections' treatment but also with drugs used chronically to treat other comorbidities (34, 35).
In several decades of the epidemics, Brazilian health authorities have been concerned with the quality of care offered to people with HIV/AIDS (36, 37). Of note, TE remains a persistent problem in the Amazon (38). Furthermore, the morbimortality due to AIDS continues to exceed the national rate (Amazonas: 6.4%, Brazil: 4.1%) (8). Until 2013, the Brazilian Ministry of Health recommended initiation of ART in symptomatic or asymptomatic individuals with CD4+ cells below 350 cells/mm3 (21). At the end of that year, treatment guidelines were updated to recommend ART in all symptomatic PLHIV regardless of the CD4+ count, and asymptomatic individuals with CD4+ <500 cells/mm3 (20). Currently, Brazilian HIV treatment guidelines recommends the start of ART in all PLHIV, despite clinical presentation and CD4+ counts (6). This Brazilian guidelines changes might have influenced the decision of when to start the ART in seven (2012–2018) out of the 9 years of this study period, as well as interfere in which antiretroviral drugs to use, since, as showed in the results, the combination of NRTI plus NNRTI was the most common choice in both groups.
Although the initiation of ART is associated with a lower mortality rate, HIV-infected individuals continue to present late for treatment and care, and consequently initiate ART with low CD4+ count and have a significantly higher risk of mortality (39, 40). The mortality rate in our series was 4.9%, which is lower than in a 20-year population based cohort study (31.0%) conducted in Denmark (5), where all TE patients had advanced HIV-disease and approximately 40% knew their serological status. Zolopa et al. (12), in a multicenter randomized trial with PLHIV and OIs, showed a decrease in mortality when ART was initiated within the first 2 weeks after diagnosis, compared to after 4 weeks. However, the study had a higher prevalence of patients with lung infections, not ART-naïve, and the whole population had CD4+ counts lower than 200 cells/mm3 and only 13 patients with HIV/TE were included. Similar findings were reported in a Spanish cohort study (13) involving ART-naïve patients with AIDS-defining diseases (with pulmonary infections being the most frequent), where late initiation of ART was associated with faster progression to death. In our study, the data reflect similar findings, in which patients with neurological infections due to T. gondii, who had ART introduced earlier, showed a trend toward lower mortality rates, although not statistically significant differences were demonstrated.
Sequelae can range from impairment of cranial nerves and headache to motor deficits and cognitive disorders (5, 29), occurring in up to 38% of patients (41). Here, sequelae at discharge were significantly more prevalent in the EIT group, indicating that the early start of ART in this population could be detrimental for this population. This could be due to the nature of the TE itself, because although, to our knowledge, no other study has directly addressed the relationship between the onset of ART and the incidence of sequelae, other studies have shown that patients coinfected with HIV-TE present more severe and persistent cognitive and motor deficits when compared with other ANI (23, 42, 43). It seems that early initiation of ART is always beneficial or does not interfere (44, 45), however the number of subjects in several of these studies is reduced in comparison to the present study. We show an elevated prevalence of sequelae, higher than the reported by Erdem et al. (46) (18.5%) regarding a multicenter study of CNS infections, with neurocryptococcosis and neurotuberculosis becoming the most prevalent diseases among 84 patients with HIV (41.6 and 18.5%, respectively). The same scenario is in agreement with the findings of an 11-year French study by Sonneville et al. (4) with PLHIV with TE admitted to the ICU, showing a lower prevalence of sequelae in their population (37.0%).
Our study has several limitations. Its retrospective nature accounts for incomplete data availability on patients' medical charts, mostly due to the absence of detailed targeted investigation, including proper registration of imaging and laboratory studies. The decision to admit patients and clinical management approaches were made at the physician's discretion, and may have resulted in classification bias for some of the outcomes here reported, which were minimized by the choice of hard clinical outcomes. Finally, our study could not fully characterize IRIS, associated with ART introduction, which has been shown to be associated with neurological sequelae and high mortality rates, especially in patients with cerebral tuberculosis and neurocryptococcosis (47, 48). Notwithstanding this, we do not believe that this is a major limitation, since several studies have reported a low incidence of IRIS in HIV-TE coinfection (49, 50), and the early or late introduction of ART does not seem to influence its onset (51, 52).
Conclusions
This is the largest series of cases presenting data on mortality, prevalence of sequelae and secondary neurologic complications in people with HIV and TE. The analyzed data show that early ART initiation in this population might have a detrimental influence on the occurrence of sequelae in these patients. These findings have not been previously reported, as ART initiation in this population has been based on limited availability of clinical evidence (17), routinely within the first 2 weeks after diagnosis and TE treatment. Neurological infections remain a major challenge in Brazil, especially in increasing HIV prevalence scenarios and decreasing government interest in this population's health status. Further studies under controlled conditions to generate evidence are needed to corroborate these findings. Future research also needs to address the chronic complications of those who manage to survive ANI secondary to HIV/AIDS and OIs and provide insights into cognitive and physical disabilities and rehabilitation (53).
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by FMT-HVD Ethics Review Board. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
NC-V, ML, WM, and FV: study concept and design. NC-V and PL: acquisition of the data. NC-V, VS, DB-d-S, and FV: analysis of the data. NC-V, DB-d-S, ML, and FV: drafting of the manuscript. NC-V, PL, DB-d-S, VS, BJ, MS, LF, IS, MA, ML, WM, and FV: critical revision of the manuscript and approval of final manuscript. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nivel Superior (CAPES) and the Fundação de Amparo à Pesquisa do Estado do Amazonas (FAPEAM) RESOLUÇÃO No. 002/2008, 007/2018 e 005/2019—Pró-Estado and RESOLUÇÃO No. 006/2020. WM and ML are CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico) fellows. The funders had no role in study design, data collection, manuscript preparation, or decision to publish.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We appreciate the assistance of Dr. Judith Recht in reviewing the manuscript.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.759091/full#supplementary-material
Supplementary Figure 1. Distribution per year of ART-naïve hospitalized patients co-infected with HIV and T. gondii encephalitis and ART transition timeline during the study period.
References
1. Coelho L, Cardoso SW, Amancio RT, Moreira RI, Campos DP, Veloso VG, et al. Trends in AIDS-defining opportunistic illnesses incidence over 25 years in Rio de Janeiro, Brazil. PLoS ONE. (2014) 9. doi: 10.1371/journal.pone.0098666
2. Ramírez-Crescencio MA, Velásquez-Pérez L, Ramírez-Crescencio MA, Velásquez-Pérez L. Epidemiology and trend of neurological diseases associated to HIV/AIDS. Experience of Mexican patients 1995-2009. Clin Neurol Neurosurg. (2013) 115:1322–5. doi: 10.1016/j.clineuro.2012.12.018
3. Siddiqi OK, Ghebremichael M, Dang X, Atadzhanov M, Kaonga P, Khoury MN, et al. Molecular diagnosis of central nervous system opportunistic infections in HIV-infected Zambian adults. Clin Infect Dis. (2014) 58:1771–7. doi: 10.1093/cid/ciu191
4. Sonneville R, Schmidt M, Messika J, Hssain AA, Da Silva D, Klein IF, et al. Neurologic outcomes and adjunctive steroids in HIV patients with severe cerebral toxoplasmosis. Neurology. (2012) 79:1762–6. doi: 10.1212/WNL.0b013e3182704040
5. Martin-Iguacel R, Ahlström MG, Touma M, Engsig FN, Stærke NB, Stærkind M, et al. Incidence, presentation and outcome of toxoplasmosis in HIV infected in the combination antiretroviral therapy era. J Infect. (2017) 75:263–73. doi: 10.1016/j.jinf.2017.05.018
6. Ministerio da Saúde. Departamento de Vigilância, Prevenção e Controle das Infecções Sexualmente Transmisíveis, do HIV/Aids e das Hepatites Virais. Protocolo clínico e diretrizes terapêuticas para manejo da infecção pelo HIV em adultos. Brasilia (2018). p. 412.
7. The Joint United Nations Programme on HIV/AIDS (UNAIDS). UNAIDS Data 2021. Geneva (2021). p. 464.
8. Ministério da Saúde. Secretaria de Vigilância em Saúde. Boletim Epidemiológico HIV/Aids | 2020. Vol. 1. Brasilia (2020). p. 67.
9. Ministerio da Saúde,. Departamento de Vigilância, Prevenção e Controle das Infecções Sexualmente Transmissíveis, do HIV/Aids e das Hepatites Virais. Indicadores e dados básicos da Aids nos municipios Brasileiros. Brasilia (2019). Available online at: http://indicadores.aids.gov.br/
10. Vidal JE, de Oliveira ACP. AIDS-related cerebral toxoplasmosis in São Paulo State, Brazil: Marked improvements in the highly active antiretroviral therapy-era but the challenges continue. Brazilian J Infect Dis. (2013) 17:379–80. doi: 10.1016/j.bjid.2012.10.030
11. de Oliveira GB, da Silva MAL, Wanderley LB, da Cunha Correia C, Ferreira ECB, de Medeiros ZM, et al. Cerebral toxoplasmosis in patients with acquired immune deficiency syndrome in the neurological emergency department of a tertiary hospital. Clin Neurol Neurosurg. (2016) 150:23–6. doi: 10.1016/j.clineuro.2016.08.014
12. Zolopa AR, Andersen J, Komarow L, Sanne I, Sanchez A, Hogg E, et al. Early antiretroviral therapy reduces AIDS progression/death in individuals with acute opportunistic infections: A multicenter randomized strategy trial. PLoS ONE. (2009) 4:e5575. doi: 10.1371/journal.pone.0005575
13. Manzardo C, Esteve A, Ortega N, Podzamczer D, Murillas J, Segura F, et al. Optimal timing for initiation of highly active antiretroviral therapy in treatment-naïve human immunodeficiency virus-1-infected individuals presenting with AIDS-defining diseases: the experience of the PISCIS cohort. Clin Microbiol Infect. (2013) 19:646–53. doi: 10.1111/j.1469-0691.2012.03991.x
14. Crabtree-Ramírez B, Caro-Vega Y, Shepherd BE, Grinsztejn B, Wolff M, Cortes CP, et al. Time to HAART initiation after diagnosis and treatment of opportunistic infections in patients with AIDS in Latin America. PLoS ONE. (2016) 11:1–11. doi: 10.1371/journal.pone.0153921
15. Panel on opportunistic infections in adults and adolescents with HIV. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. Maryland (2021).
16. World Health Organization. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy. (2017). p. 1–56.
17. Ministério da Saúde. Secretaria de Vigilância em Saúde Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. In: Protocolo clínico e diretrizes terapeuticas para atenção às pessoas com infecções sexualmente transmissíveis. Brasilia (2020). p. 248.
18. Ministério da Saúde. Secretaria de Vigilância em Saúde Departamento de Vigilância, Prevenção e Controle das Infecções Sexualmente Transmissíveis, do HIV/Aids e das Hepatites Virais. In: Manual Técnico Para o Diagnóstico Da Infecção Pelo HIV Em Adultos e Crianças 4th ed. Brasilia (2018). p. 146.
19. Vidal JE. HIV-Related cerebral toxoplasmosis revisited: Current concepts and controversies of an old Disease. J Int Assoc Provid AIDS Care. (2019) 18:1–20. doi: 10.1177/2325958219867315
20. Saúde Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de DST A e HV. Protocolo Clínico e Diretrizes Terapêuticas para Manejo da Infecção pelo HIV em Adultos. (2013). p. 186–8.
21. Ministerio da Saúde. Secretaria de Vigilância em Saúde: Recomendações para Terapia Anti–retroviral em Adultos Infectados pelo HIV: 2008. 7a Edição (2008). p. 1–136.
22. Croxford S, Kitching A, Desai S, Kall M, Edelstein M, Skingsley A, et al. Mortality and causes of death in people diagnosed with HIV in the era of highly active antiretroviral therapy compared with the general population: an analysis of a national observational cohort. Lancet Public Heal. (2017) 2:e35–46. doi: 10.1016/S2468-2667(16)30020-2
23. Schäfer G, Hoffmann C, Arasteh K, Schürmann D, Stephan C, Jensen B, et al. Immediate versus deferred antiretroviral therapy in HIV-infected patients presenting with acute AIDS-defining events (toxoplasmosis, Pneumocystis jirovecii-pneumonia): a prospective, randomized, open-label multicenter study (IDEAL-study). AIDS Res Ther. (2019) 16:1–8. doi: 10.1186/s12981-019-0250-2
24. Uthman OA, Okwundu C, Gbenga K, Volmink J, Dowdy D, Zumla A, et al. Optimal timing of antiretroviral therapy initiation for HIV-infected adults with newly diagnosed pulmonary tuberculosis: A systematic review and meta-analysis. Ann Intern Med. (2015) 163:32–9. doi: 10.7326/M14-2979
25. Ciocca DR, Delgado G. The reality of scientific research in Latin America) an insider's perspective. Cell Stress Chaperones. (2017) 22:847–52. doi: 10.1007/s12192-017-0815-8
26. Kalergis AM, Lacerda M, Rabinovich GA, Rosenstein Y. Challenges for scientists in Latin America. Trends Mol Med. (2016) 22:743–5. doi: 10.1016/j.molmed.2016.06.013
27. Bain LE, Tarkang EE, Ebuenyi ID, Kamadjeu R. The HIV/AIDS pandemic will not end by the year 2030 in low and middle income countries. Pan Afr Med J. (2019) 32:4–7. doi: 10.11604/pamj.2019.32.67.17580
28. Hotez PJ, Damania A, Bottazzi ME. Central Latin America: Two decades of challenges in neglected tropical disease control. PLoS Negl Trop Dis. (2020) 14:1–7. doi: 10.1371/journal.pntd.0007962
29. Flegr J. Neurological and Neuropsychiatric consequences of chronic Toxoplasma infection. Curr Clin Microbiol Reports. (2015) 2:163–72. doi: 10.1007/s40588-015-0024-0
30. Bowen LN, Smith B, Reich D, Quezado M, Nath A. HIV-associated opportunistic CNS infections: Pathophysiology, diagnosis and treatment. Nat Rev Neurol. (2016) 12:662–74. doi: 10.1038/nrneurol.2016.149
31. Wilkinson RJ, Rohlwink U, Misra UK, Van Crevel R, Mai NTH, Dooley KE, et al. Tuberculous meningitis. Nat Rev Neurol. (2017) 13:581–98. doi: 10.1038/nrneurol.2017.120
32. Oreagba IA, Usman SO, Oshikoya KA, Akinyede AA, Agbaje EO, Opanuga O, et al. Clinically significant drug-drug interaction in a large antiretroviral treatment centre in Lagos, Nigeria. J Popul Ther Clin Pharmacol. (2019) 26:e1–19. doi: 10.22374/1710-6222.26.1.1
33. Chastain DB, Franco-Paredes C, Stover KR. Addressing antiretroviral therapy-associated drug-drug interactions in patients requiring treatment for opportunistic infections in low-income and resource-limited settings. J Clin Pharmacol. (2017) 57:1387–99. doi: 10.1002/jcph.978
34. Molas E, Luque S, Retamero A, Echeverría-Esnal D, Guelar A, Montero M, et al. Frequency and severity of potential drug interactions in a cohort of HIV-infected patients Identified through a Multidisciplinary team. HIV Clin Trials. (2018) 19:1–7. doi: 10.1080/15284336.2017.1404690
35. Park MS, Yang YM, Kim JS, Choi EJ. Comparative study of antiretroviral drug regimens and drug–drug interactions between younger and older HIV-infected patients at a tertiary care teaching hospital in South Korea. Ther Clin Risk Manag. (2018) 14:2229–41. doi: 10.2147/TCRM.S175704
36. Laurindo-Teodorescu L, Teixeira PR. Histórias da Aids no Brasil, 1983-2003: as respostas governamentais à epidemia de aids 1st ed. Brasilia (2015). p. 464.
37. Ministério da Saúde. Departamento de Vigilância Prevenção e Controle das Infecções Sexualmente Transmissíveis do HIV/Aids e das Hepatites Virais. In: Nota Informativa no 03/18 - COVIG/CGVP/.DIAHV/SVS/MS: switch de esquemas com ITRNN e IP/r por DTG. Brasilia (2018).
38. De Souza SLS, Feitoza PVS, De Araújo JR, De Andrade RV, Ferreira LCDL. Causas de óbito em pacientes com síndrome da imunodeficiência adquirida, necropsiados na Fundação de Medicina Tropical do Amazonas. Rev Soc Bras Med Trop. (2008) 41:247–51. doi: 10.1590/S0037-86822008000300005
39. Ministério da Saúde Secretaria de Vigilância em Saúde. Boletim Epidemiológico HIV/ Aids | 2019. Brasilia (2019). p. 71.
40. Belaunzarán-Zamudio PF, Caro-Vega YN, Shepherd BE, Rebeiro PF, Crabtree-Ramírez BE, Cortes CP, et al. The population impact of late presentation with advanced HIV disease and delayed antiretroviral therapy in adults receiving HIV care in Latin America. Am J Epidemiol. (2019) 189:564–72. doi: 10.1093/aje/kwz252
41. Simmons RD, Ciancio BC, Kall MM, Rice BD, Delpech VC. Ten-year mortality trends among persons diagnosed with HIV infection in England and Wales in the era of antiretroviral therapy: AIDS remains a silent killer. HIV Med. (2013) 14:596–604. doi: 10.1111/hiv.12045
42. Levine AJ, Hinkin CH, Ando K, Santangelo G, Martinez M, Valdes-Sueiras M, et al. An exploratory study of long-term neurocognitive outcomes following recovery from opportunistic brain infections in HIV+ adults. J Clin Exp Neuropsychol. (2008) 30:836–43. doi: 10.1080/13803390701819036
43. Lau A, Jain MK, Chow JYS, Kitchell E, Lazarte S. Nijhawan A. Toxoplasmosis encephalitis: a cross-sectional analysis at a US safety-net hospital in the late cART era. J Int Assoc Provid AIDS Care. (2021) 20:1–7. doi: 10.1177/23259582211043863
44. Vidal JE, Hernandez A V, Penalva De Oliveira AC, Dauar RF, Barbosa SP, Focaccia R. Cerebral toxoplasmosis in HIV-positive patients in Brazil: Clinical features and predictors of treatment response in the HAART era. AIDS Patient Care STDS. (2005) 19:626–34. doi: 10.1089/apc.2005.19.626
45. Antinori A, Larussa D, Cingolani A, Lorenzini P, Bossolasco S, Finazzi MG, et al. Prevalence, associated factors, and prognostic determinants of AIDS-related toxoplasmic encephalitis in the era of advanced highly active antiretroviral therapy. Clin Infect Dis. (2004) 39:1681–91. doi: 10.1086/424877
46. Erdem H, Inan A, Guven E, Hargreaves S, Larsen L, Shehata G, et al. The burden and epidemiology of community-acquired central nervous system infections: a multinational study. Eur J Clin Microbiol Infect Dis. (2017) 36:1595–611. doi: 10.1007/s10096-017-2973-0
47. Marais S, Meintjes G, Pepper DJ, Dodd LE, Schutz C, Ismail Z, et al. Frequency, severity, and prediction of tuberculous meningitis immune reconstitution inflammatory syndrome. Clin Infect Dis. (2013) 56:450–60. doi: 10.1093/cid/cis899
48. Katchanov J, Blechschmidt C, Nielsen K, Branding G, Arastéh K, Tintelnot K, et al. Cryptococcal meningoencephalitis relapse after an eight-year delay: an interplay of infection and immune reconstitution. Int J STD AIDS. (2015) 26:912–4. doi: 10.1177/0956462414563630
49. Van Bilsen WPH, Van Den Berg CHSB, Rijnders BJA, Brinkman K, Mulder JW, Gelinck LBS, et al. Immune reconstitution inflammatory syndrome associated with toxoplasmic encephalitis in HIV-infected patients. Aids. (2017) 31:1415–24 p. doi: 10.1097/QAD.0000000000001492
50. Martin-Blondel G, Alvarez M, Delobel P, Uro-Coste E, Cuzin L, Cuvinciuc V, et al. Toxoplasmic encephalitis IRIS in HIV-infected patients: A case series and review of the literature. J Neurol Neurosurg Psychiatry. (2011) 82:691–3. doi: 10.1136/jnnp.2009.199919
51. Boulware DR, Meya DB, Muzoora C, Rolfes MA, Huppler Hullsiek K, Musubire A, et al. Timing of antiretroviral therapy after diagnosis of cryptococcal meningitis. N Engl J Med. (2014) 370:2487–98. doi: 10.1056/NEJMoa1312884
52. Grant PM, Komarow L, Andersen J, Sereti I, Pahwa S, Lederman MM, et al. Risk factor analyses for immune reconstitution inflammatory syndrome in a randomized study of early vs. deferred ART during an opportunistic infection. PLoS ONE. (2010) 5:3–9. doi: 10.1371/journal.pone.0011416
53. Zeng YM, Li Y, He XQ, Huang YQ, Liu M, Yuan J, et al. A study for precision diagnosing and treatment strategies in difficult-to-treat AIDS cases and HIV-infected patients with highly fatal or highly disabling opportunistic infections: study protocol for antiretroviral therapy timing in AIDS patients with tox. Medicine (Baltimore). (2020) 99:e21141. doi: 10.1097/MD.0000000000021141
Keywords: Toxoplasma gondii, toxoplasmic encephalitis, HIV/AIDS, therapy, antiretroviral, complications
Citation: Cubas-Vega N, López Del-Tejo P, Baia-da-Silva DC, Sampaio VS, Jardim BA, Santana MF, Lima Ferreira LC, Safe IP, Alexandre MAA, Lacerda MVG, Monteiro WM and Val F (2022) Early Antiretroviral Therapy in AIDS Patients Presenting With Toxoplasma gondii Encephalitis Is Associated With More Sequelae but Not Increased Mortality. Front. Med. 9:759091. doi: 10.3389/fmed.2022.759091
Received: 15 August 2021; Accepted: 25 January 2022;
Published: 25 February 2022.
Edited by:
Hai-Feng Pan, Anhui Medical University, ChinaReviewed by:
Yinguang Fan, Anhui Medical University, ChinaDebanjan Mukhopadhyay, National Institute of Biomedical Genomics (NIBMG), India
Veeranoot Nissapatorn, Walailak University, Thailand
Copyright © 2022 Cubas-Vega, López Del-Tejo, Baia-da-Silva, Sampaio, Jardim, Santana, Lima Ferreira, Safe, Alexandre, Lacerda, Monteiro and Val. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fernando Val, ZmZhdmFsQGdtYWlsLmNvbQ==