 Tobias Hoffmann1*
Tobias Hoffmann1* Peter Oelzner1
Peter Oelzner1 Ulf Teichgräber2
Ulf Teichgräber2 Marcus Franz3Nikolaus Gaßler4Claus Kroegel3†Gunter Wolf1
Marcus Franz3Nikolaus Gaßler4Claus Kroegel3†Gunter Wolf1 Alexander Pfeil1
Alexander Pfeil1- 1Department of Internal Medicine III, Jena University Hospital–Friedrich Schiller University Jena, Jena, Germany
- 2Institute of Diagnostic and Interventional Radiology, Jena University Hospital–Friedrich Schiller University Jena, Jena, Germany
- 3Department of Internal Medicine I, Jena University Hospital–Friedrich Schiller University Jena, Jena, Germany
- 4Department of Pathology, Jena University Hospital–Friedrich Schiller University Jena, Jena, Germany
Lung involvement is the most common and serious organ manifestation in patients with inflammatory rheumatic disease (IRD). The type of pulmonary involvement can differ, but the most frequent is interstitial lung disease (ILD). The clinical manifestations of IRD-ILD and severity can vary from subclinical abnormality to dyspnea, respiratory failure, and death. Consequently, early detection is of significant importance. Pulmonary function test (PFT) including diffusing capacity of the lungs for carbon monoxide (DLCO), and forced vital capacity (FVC) as well as high-resolution computed tomography (HRCT) are the standard tools for screening and monitoring of ILD in IRD-patients. Especially, the diagnostic accuracy of HRCT is considered to be high. Magnetic resonance imaging (MRI) and positron emission tomography/computed tomography (PET/CT) allow both morphological and functional assessment of the lungs. In addition, biomarkers (e.g., KL-6, CCL2, or MUC5B) are being currently evaluated for the detection and prognostic assessment of ILD. Despite the accuracy of HRCT, invasive diagnostic methods such as bronchoalveolar lavage (BAL) and lung biopsy are still important in clinical practice. However, their therapeutic and prognostic relevance remains unclear. The aim of this review is to give an overview of the individual methods and to present their respective advantages and disadvantages in detecting and monitoring ILD in IRD-patients in the clinical routine.
Key messages
• Patients with inflammatory rheumatic diseases (IRD) are at particular risk of developing pulmonary diseases such as interstitial lung disease (ILD) which is associated with a increased morbidity and mortality
• Pulmonary function tests (PFT) with measurements of FVC and DLCO as well as high-resolution computed tomography (HRCT) are the current standards for screening and monitoring ILD in IRD
• Cardiopulmonary stress tests are, additional to PFT, suitable for the assessment of prognosis and evaluating the response to therapy in ILD
• New imaging technologies such as magnetic resonance imaging (MRI) and positron emission tomography (PET) with computed tomography (PET/CT) can evaluate both morphological and functional features
• The value of invasive methods like bronchoalveolar lavage (BAL) and lung biopsy has not yet been adequately investigated
• Numerous biomarkers with good sensitivity and specificity exist for detection and prognostic evaluation but have not yet found their way into clinical routine
Introduction
Inflammatory rheumatic diseases (IRD) belong to the wide spectrum of immune-mediated inflammatory diseases (IMID) comprising inflammatory joint diseases, connective tissue diseases (CTD), myositis as well as vasculitis (1–6).
Many IRD present with complex clinical pictures, involving other tissues: In total, 53% of IRD-patients show an organ involvement at initial diagnosis (7) with a predominant affection of the lungs, followed by the heart and kidneys (8–13). Patients with CTD, myositis/dermatomyositis, and vasculitis are particularly susceptible for solid organ manifestations.
Pulmonary manifestations present special diagnostic and therapeutic challenges and are associated with a significant morbidity and mortality in IRD-patients. The most common clinical pattern of lung illness encountered in IRD is interstitial lung disease (ILD) (8, 9, 11), ranging between 12.5 and 30.8% at the onset of CTD, 66.7–83.3% with vasculitis and 16.7–100.0% with myositis (7). In addition, lung diseases are also found in association with rheumatoid arthritis (RA) with a life-time risk of developing ILD of 7.7% (14, 15).
The clinical manifestations and severity of IRD-ILD can vary from subclinical abnormality to dyspnea, respiratory failure, and death (16–18).
International guidelines for the management and diagnostic of IRD-ILD do not exist. There is only for patients with systemic sclerosis (SSc) an European evidence-based consensus statement available (19). According to the current literature and international guidelines, parallels can only be drawn with idiopathic pulmonary fibrosis (IPF), for which high-resolution computed tomography (HRCT) is the diagnostic gold standard (20–22). Furthermore, in different studies pulmonary function tests (PFT), bronchoalveolar lavage (BAL), and biomarkers [e.g., Krebs von den Lungen 6 (KL-6), chemokine (C-C motif) ligand 2 (CCL2), or mucin 5B (MUC5B)] were also discussed as potential diagnostic tools (23–25).
Patients at early stages of IRD are often asymptomatic with an HRCT-finding of ground-glass opacity (GGO) and reticulation (26, 27). In established ILD and in the presence of pulmonary symptoms, HRCT often reveals a specific pattern like usual interstitial pneumonia (UIP) or non-specific interstitial pneumonia (NSIP) (28, 29). Finally, the autoimmune-mediated lung injury can lead to chronic progressive fibrosing ILD as final manifestation (30, 31).
The frequency and significant increased morbidity and mortality of IRD-ILD as well as the availability of new therapeutic options [e.g., nintedanib and tocilizumab (approved for SSc-ILD by the FDA)] underline the importance of an early diagnosis. However, the optimal use of the different diagnostic tools in the clinical routine is not yet clear defined (32, 33).
Therefore, the present review aims to provide an overview of the various diagnostic tools and their value in detecting ILD and offers an evaluation of these procedures for the long-term follow up. For this an overview is given in Table 1 with advantages and disadvantages of different methods in diagnosing ILD in IRD-patients. Moreover, we supplement a case-report with pulmonary involvement in systemic lupus erythematosus to this review to illustrate and demonstrate the possible and complex pulmonary diagnostic in IRD (see Supplementary material).
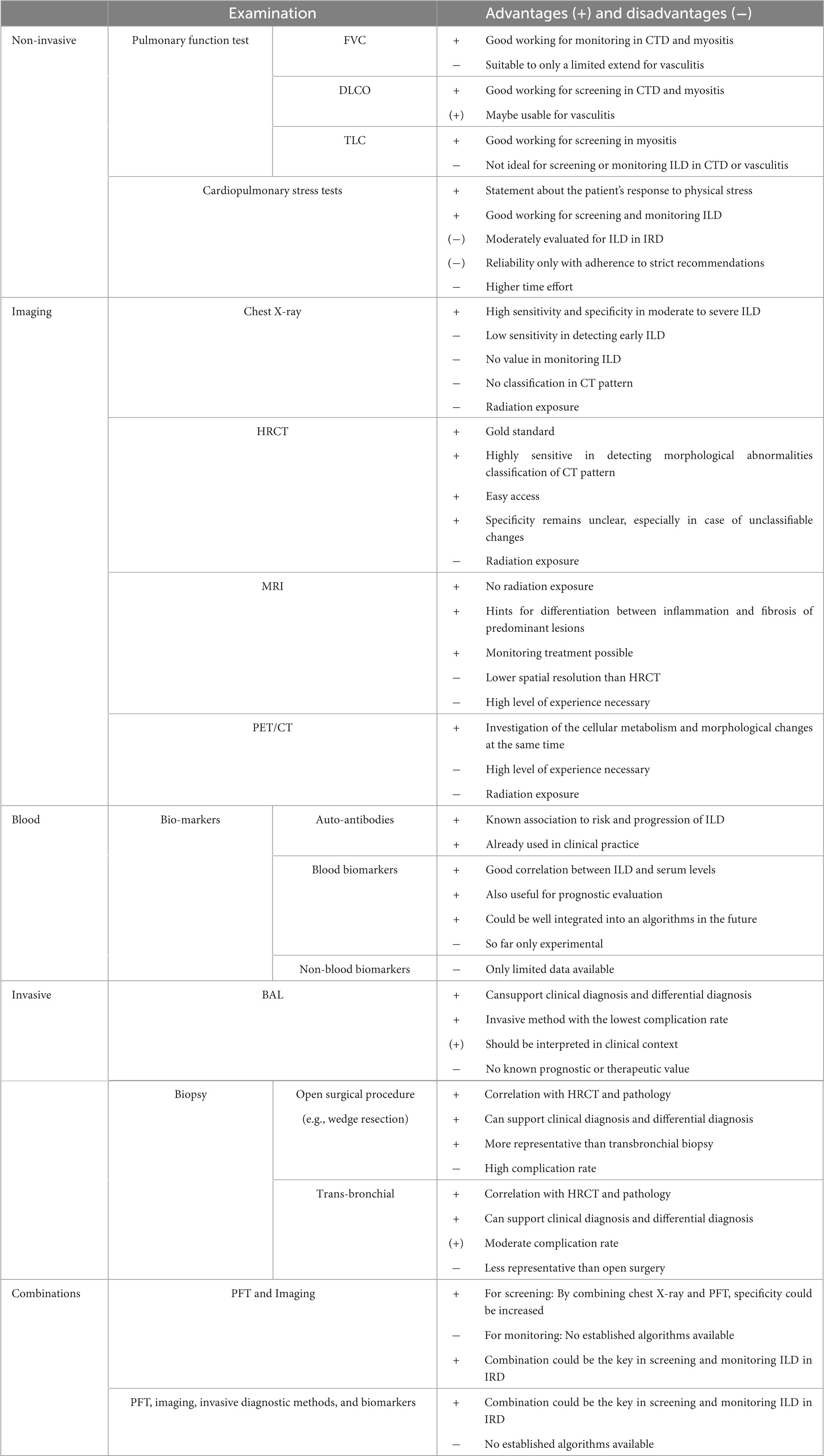
Table 1. Advantages and disadvantages of different methods in diagnosing ILD in IRD-patients.
Clinical signs and symptoms
There are some clinical signs and symptoms that are more likely to be associated with ILD. They may support the suspected diagnosis of ILD and can also justify further investigation. A typical clinical sign for fibrosis of the lung in clinical examination are bibasilar inspiratory crackles (sclerosiphonia), but patients also frequently report dyspnea and cough (21, 34). Distler et al. (35) was able to show that patients with SSc ILD had a mean functional assessment of cancer therapy (FACIT) dyspnea score of 47.01 ± 9.64. Lin et al. (36) describe cough and dyspnea as a risk factor for ILD in Sjögren’s syndrome. Moreover, Hoffmann et al. (27) demonstrated that also at initial diagnosis of IRD-ILD, there is significantly more dyspnea and sclerosiphonia compared with patients without ILD. However, because there are other causes for these signs, they are not necessarily specific for ILD (37).
Digital clubbing is a typical clinical sign of pulmonary fibrosis (PF), but the specificity is low, as many other diseases can also show such abnormalities (38). For ILD in IRD, only a few studies/case reports exist, but no systematic analysis for the presence of digital clubbing. Van Manen et al. (39) describe in a cohort of ILD in IRD 37% of patients with digital clubbing, assessed by a physician. In addition, we know certain pathognomonic findings in IRD increasing the risk of ILD, such as mechanic’s hands (myositis) or Gottron’s papules (dermatomyositis) (40–42). But the risk of ILD, depending on the clinical sign, is very heterogeneous between the IRD. In SSc male sex and ethnicity are considered as independent risk factors for progressive SSc-ILD (19). Moreover, Lin et al. (36) reported Raynaud’s phenomenon as a risk factor for ILD in newly diagnosed Sjögren’s syndrome. Knowing these symptoms and clinical signs, any clinician can take advantage of this knowledge and use it without additional equipment. Furthermore, it should be emphasized that pulmonary asymptomatic patients may already have ILD on HR-CT in the setting of initial diagnosis of IRD (27).
Pulmonary function test
The presence and progression of ILD are routinely monitored using PFT. Various parameters can be measured through different examinations like spirometry, body plethysmography or diffusing capacity of the lungs for carbon monoxide (DLCO) (43–45). Spirometry is the most common PFT (43–45). The most relevant measurements are the forced vital capacity (FVC), which describes the total air volume that can be exhaled after a full inspiration, and the forced expiratory volume in 1 s (FEV1), which is the expiratory volume in the first second of an FVC maneuver (44). Supplementary information is provided by body plethysmography which allows to determine total lung capacity (TLC), lung residual volume (RV), and airway resistance (46, 47). Additionally, DLCO is used to estimate the lungs’ ability to transfer gas from the inspired air to the bloodstream (48).
In rheumatology, many studies evaluated the relevance of PFT as surrogate markers for ILD in IRD; we summarized the most relevant literature in Table 2. Various parameters can be considered, with the focus on FVC and DLCO in the current literature. Although data are limited, there is evidence, that we have to differentiate between monitoring a known ILD and screening for newly onset ILD in IRD (27). In addition, it is necessary to distinguish between the different IRD-related diseases (27).
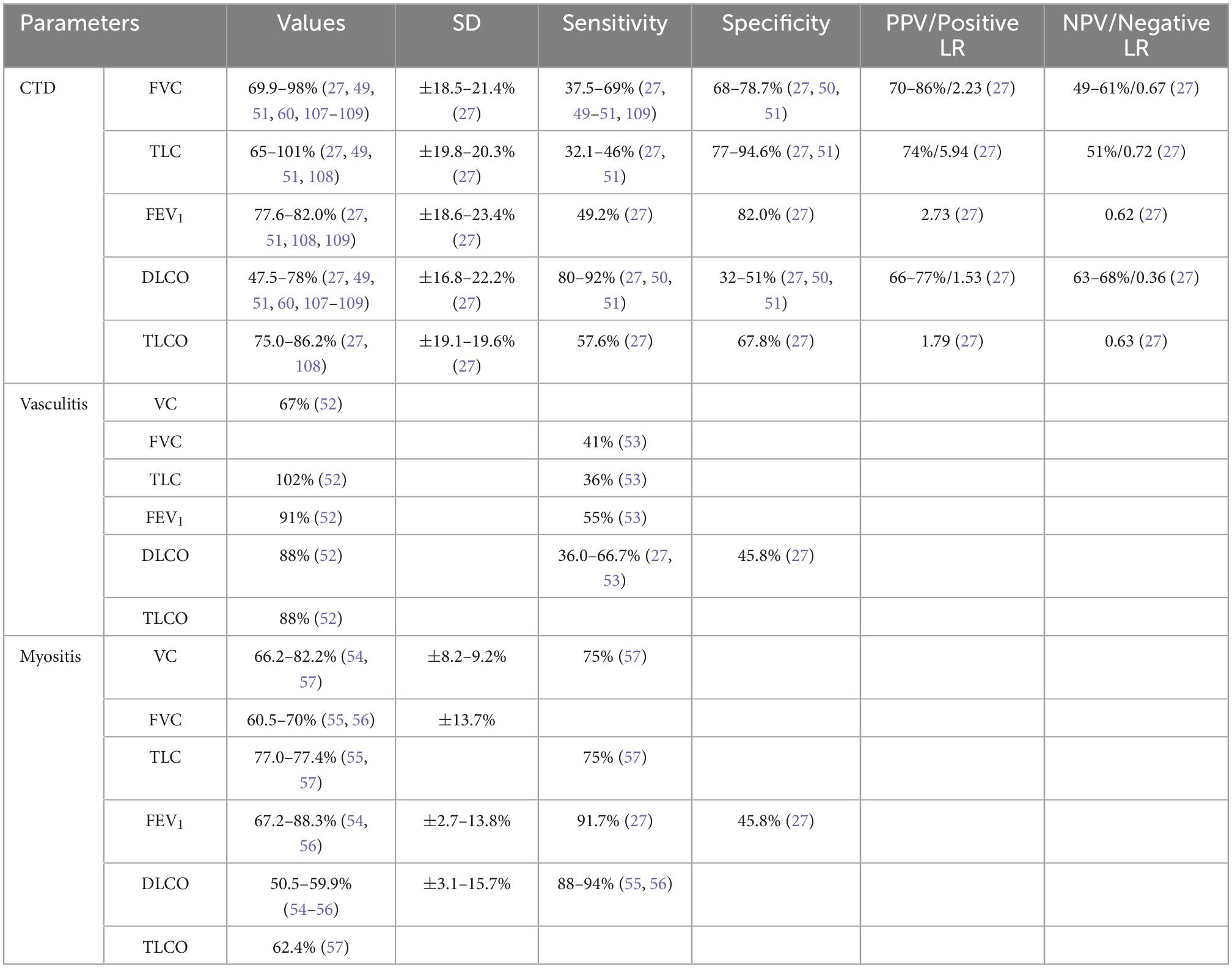
Table 2. Values, sensitivities, specificities, positive (PPV) and negative predictive values (NPV) for different parameters in pulmonary function test (PFT) for screening and monitoring interstitial lung disease (ILD) in patients with inflammatory rheumatic diseases (IRD) (cut-off < 80%).
Pulmonary function test for detecting/Screening for newly onset interstitial lung disease in inflammatory rheumatic disease
Various studies suggest that an impaired DLCO (<80%) may have a predictive value for the development of ILD. Thus, Suliman et al. (49) showed that the DLCO (<80%) was the only frequently pathological parameter in the PFT, compared to FVC or TLC. This in accordance with Showalter et al. (50) demonstrating a sensitivity and specificity of 92.0 and 32.0% for DLCO < 80%, with the highest negative predictive value (NPV) of 63% in patients with SSc. Bernstein et al. (51) reported a sensitivity of 80.0% and specificity of 51.0% with NPV of 68% in detecting ILD by DLCO < 80% in early diffuse SSc. However, TLC shows only sensitivities and specificities intermediate between those of FVC and DLCO (49, 51). Therefore, it can be assumed that TLC is neither suitable for screening nor monitoring of ILD.
In patients with anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV), Newall et al. (52) demonstrated no significant differences in FVC, TLC or FEV1 between patients with or without ILD. Furthermore, the study yielded a reduced DLCO in ANCA vasculitis patients with ILD (52). Rosenberg et al. (53) showed sensitivities of 55% (FEV1) and 41% (FVC). Therefore, PFT based on FVC, TLC, and FEV1 alone do not seem not to be valid surrogate parameters for ILD in AAV-patients.
This also applies for patients with myositis, although the study populations are rather small, which makes it difficult to obtain a conclusion. Ideura et al. (54) reported reduced DLCO- and FVC-values and a normal FEV1 in patients with amyopathic dermatomyositis. The data of a 10-year retrospective analysis published by Chua et al. (55) showed a restrictive ventilatory defect in the majority (79%) of patients with idiopathic inflammatory myositis (IIM) with mean baseline values of FVC and TLC of 70 and 77%, respectively. 94% of patients had a baseline DLCO of <80%. This is in accordance with the results of Won Huh et al. (56), revealing a restrictive defect (92.9%) as the most common PFT abnormality, followed by a low DLCO (88.0%) in patients with polymyositis/dermatomyositis (PM/DM); 80% had a restrictive defect with a reduced DLCO. Fathi et al. (57) observed also restrictive changes on PFT and reduced DLCO in almost all PM/DM-patients with radiological evidence of ILD. Overall, in patients with myositis, restrictive patterns (especially TLC) and a reduced DLCO seem to be important for diagnosing ILD.
Pulmonary function test for monitoring interstitial lung disease in inflammatory rheumatic disease
As shown in a systematic review by Caron et al. (24), FVC (% predicted) is the most commonly used surrogate marker in studies evaluating ILD progression in SSc-patients. FVC is widely used as primary endpoint in studies, but is also a generally recognized sign of disease progression (decline of 10%) (21, 58, 59). One of the main reasons for FVC’s current popularity in SSc is the fact that FVC is believed to be more specific than DLCO for ILD which can be more useful for monitoring ILD (24). Suliman et al. (49) and Showalter et al. (50) demonstrated a sensitivity and specificity of 37.5–69.0% and 73.0–92.0%, respectively, for FVC < 80%. According to the evidence-based European consensus which has been developed by a panel of 27 European pulmonologists, rheumatologists, and internists with expertise in SSc-ILD, FVC, and DLCO are considered to be useful parameters for evaluation disease progression in SSc (19). In addition, multivariate analyses of a prospective cohort study with SSc-patients identified baseline DLCO as one of the predictors of no fibrosis at follow-up and FVC as predictors of >20% fibrosis at follow-up (60). However, there is still a lack of large ILD studies in IRD, especially for myositis and vasculitis.
Cardiopulmonary stress tests
Pulmonary function test is a static examination which does not allow any statement to be made about the patient’s response to physical stress. For many decades, cardiopulmonary stress tests such as the 6-min walk test (6MWT) and cardiopulmonary exercise test (CPET) have been used to evaluate the performance of the patients.
According to American Thoracic Society (ATS) guideline the 6MWT and CPET evaluates the global and integrated responses of all the systems involved during exercise (pulmonary, cardiovasculary, systemic and peripheral circulation, neuromuscular system, muscle metabolism) (61, 62). The 6MWT assesses the submaximal level of functional capability, whereas the CPET evaluates submaximal and peak exercise response (61, 62).
The ATS and European Respiratory Society (ERS) positions paper emphasize the benefits of 6MWT in assessing prognosis, evaluating response and functional exercise capacity in respiratory disease (63). Especially in chronic obstructive pulmonary disease (COPD), a reduced 6MWT was associated with an increased risk of hospitalization and mortality (63). Similar, results were demonstrated for ILD by the ATS/ERS systematic literature review (63). Even CPET is useful in verifying early ILD regarding the detection of minor pulmonary gas exchange abnormalities and therapy monitoring in established ILD (62, 64, 65). Additionally, Keogh et al. (65) could show that CPET can reveal alveolar dysfunction in the presence of normal resting parameter. In summary, 6MWT and CPET represent additional diagnostic (besides PFT and imaging), providing information to improve the care and therapy of patients with ILD.
Imaging
Unlike PFT, imaging techniques allow an overview of the morphologic features of the lungs. Modern techniques such as magnetic resonance imaging (MRI) and positron emission tomography/computed tomography (PET/CT) have broadened the spectrum of “classical methods” such as X-ray or HRCT (66).
Chest X-ray
Chest X-ray is the most simple and cost-effective method for morphological assessment of the lungs. In everyday clinical practice, it continues to be of value for overview imaging of the lungs or to exclude/confirm infections. However, chest radiographs are insensitive to early changes and may appear normal despite respiratory function test abnormalities and are therefore no longer of any value in diagnosing ILD (67) (see Figure 1).

Figure 1. Comparison of chest X-ray with HRCT at initial diagnosis of ILD. (A) Early Sharp syndrome with ground-glass opacities in HRCT and inconspicuous chest X-ray, (B) early systemic sclerosis with ground-glass opacities, reticulations (early NSIP-pattern), and small consolidations in chest X-ray and (C) end-stage Sjögren’s syndrome with distinct consolidations in chest X-ray and beginning UIP-pattern in HRCT.
High-resolution computed tomography
High-resolution computed tomography is the gold standard for the detection, characterization, and monitoring of ILD (19, 67). According to the Fleischner Society, the term interstitial lung abnormalities (ILA) refers to specific CT findings that are potentially compatible with ILD in patients without clinical suspicion of the disease (66). ILA have been described as non-dependent abnormalities affecting more than 5% of any lung zone (upper, middle, and lower lung zones are demarcated by the levels of the inferior aortic arch and right inferior pulmonary vein) (66). ILA include the following radiological signs (66):
• Ground-glass opacity
• Reticular abnormalities
• Lung distortion
• Traction bronchiectasis
• Honeycombing
• Non-emphysematous cysts
These parenchymal findings can be classified according to the definition by the Fleischner Society and the ATS/ERS (see Tables 3, 4) (67–69) in consideration of the differential diagnosis of idiopathic interstitial pneumonia [e.g., hypersensitivity pneumonia (HP)] according to ATS/ERS (details see Table 5) (67–69). If ILA present less than 5% of any lung zone, they are defined as indeterminate ILA. Depending on the cohort, the prevalence of indeterminate ILD ranges from 32 to 59% (70). According to Putman et al. (70), ILA and indeterminate ILA are associated with a greater all-cause mortality. The transition between ILA and ILD is not clearly defined and should be determined by clinical parameters. Especially in IRD, even small ILA is considered as ILD (66). The diagnostic follow up of patients with indeterminate ILA remains completely unclear, because especially in early cases, no extensive pulmonary changes can be expected, but patients could benefit to a greater extent from therapy.
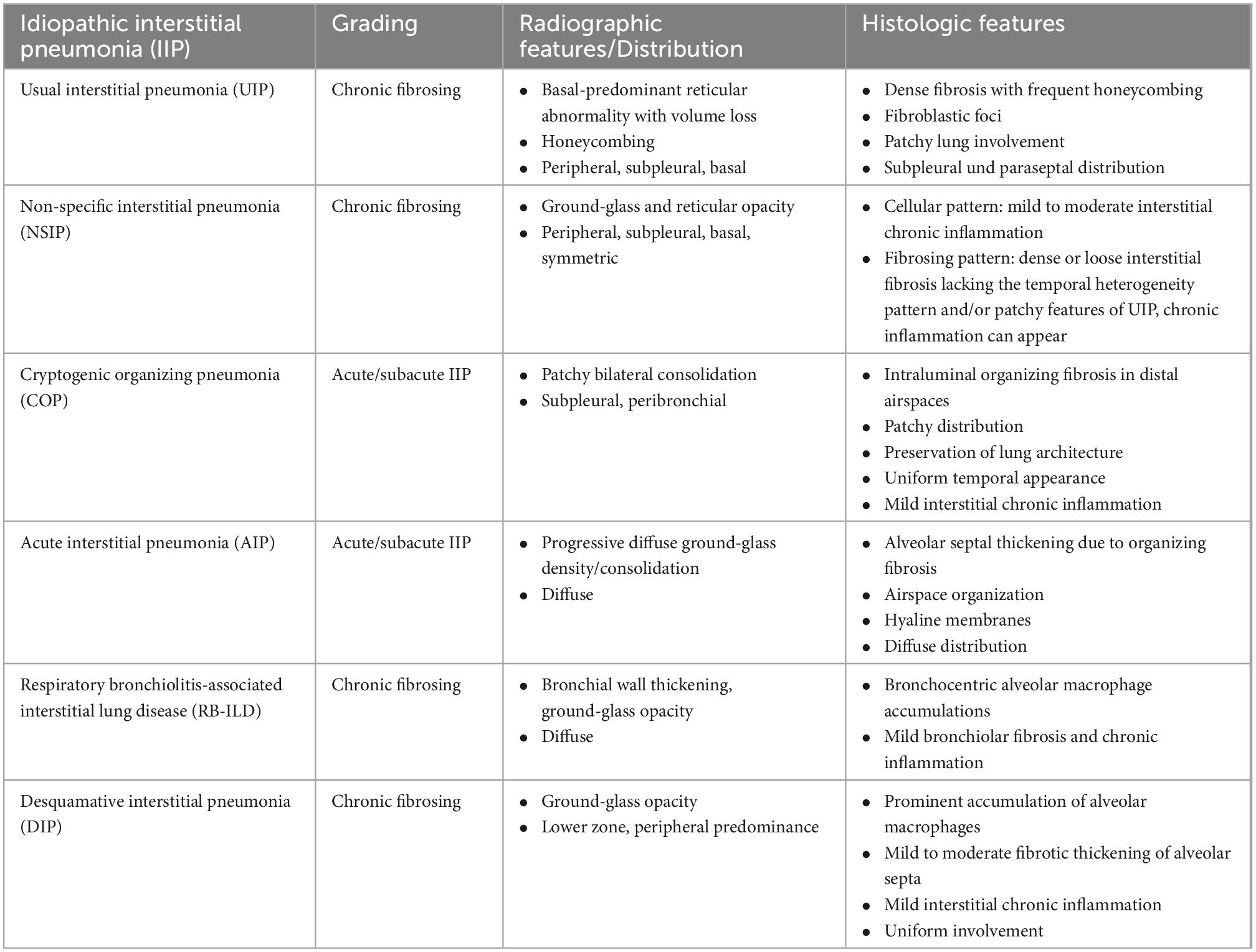
Table 3. Radiographic and histologic features of major idiopathic interstitial pneumonias (IIP) according to the classification of the American Thoracic Society (ATS) and European Respiratory Society (ERS) (68, 69).
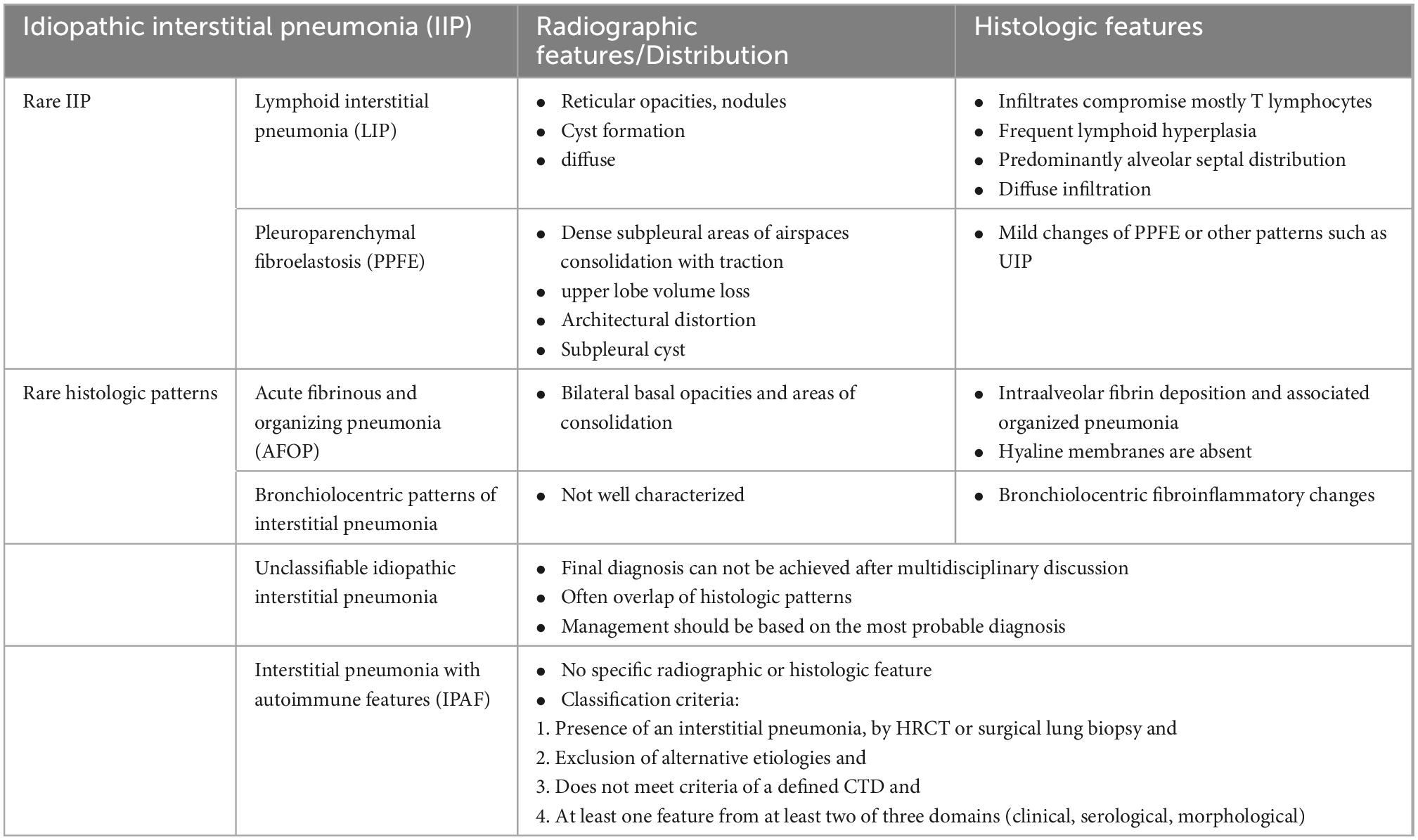
Table 4. Radiographic and histologic features of rare, unclassifiable, and other idiopathic interstitial pneumonias (IIP) according to the classification of the American Thoracic Society (ATS) and European Respiratory Society (ERS) (68, 69, 110).

Table 5. Radiographic and histologic features of important differential diagnosis according to the classification of the American Thoracic Society (ATS) and European Respiratory Society (ERS) (68, 69).
The most common HRCT-patterns in IRD are NSIP and UIP, depending on the underlying immunologically mediated systemic disorder (28) (see Figures 1, 2A–D, F). According to Goldin et al. (26), among other changes pure ground-glass opacities (pGGO) and PF are the most common HRCT scan findings in patients with symptomatic SSc (see Figure 2E). The extent of PF seen on HRCT scans was significantly negatively correlated with FVC (r = −0.22), DLCO (r = −0.44), and TLC (r = −0.36). A positive correlation was revealed between pGGO and the increased number of acute inflammatory cells found in BAL fluid (r = 0.28). In addition, Remy-Jardin observed that areas of ground-glass attenuation are a reliable indicator of inflammation, as shown in histologic evaluations at open lung biopsy (71). Because differentiation from other causes of GGO such as pulmonary edema, alveolar hemorrhage, NSIP, and hypersensitivity pneumonitis can be challenging, consideration of relevant clinical information such as the chronicity of symptoms, the patient’s immune status, and pre-existing medical conditions is essential (72).
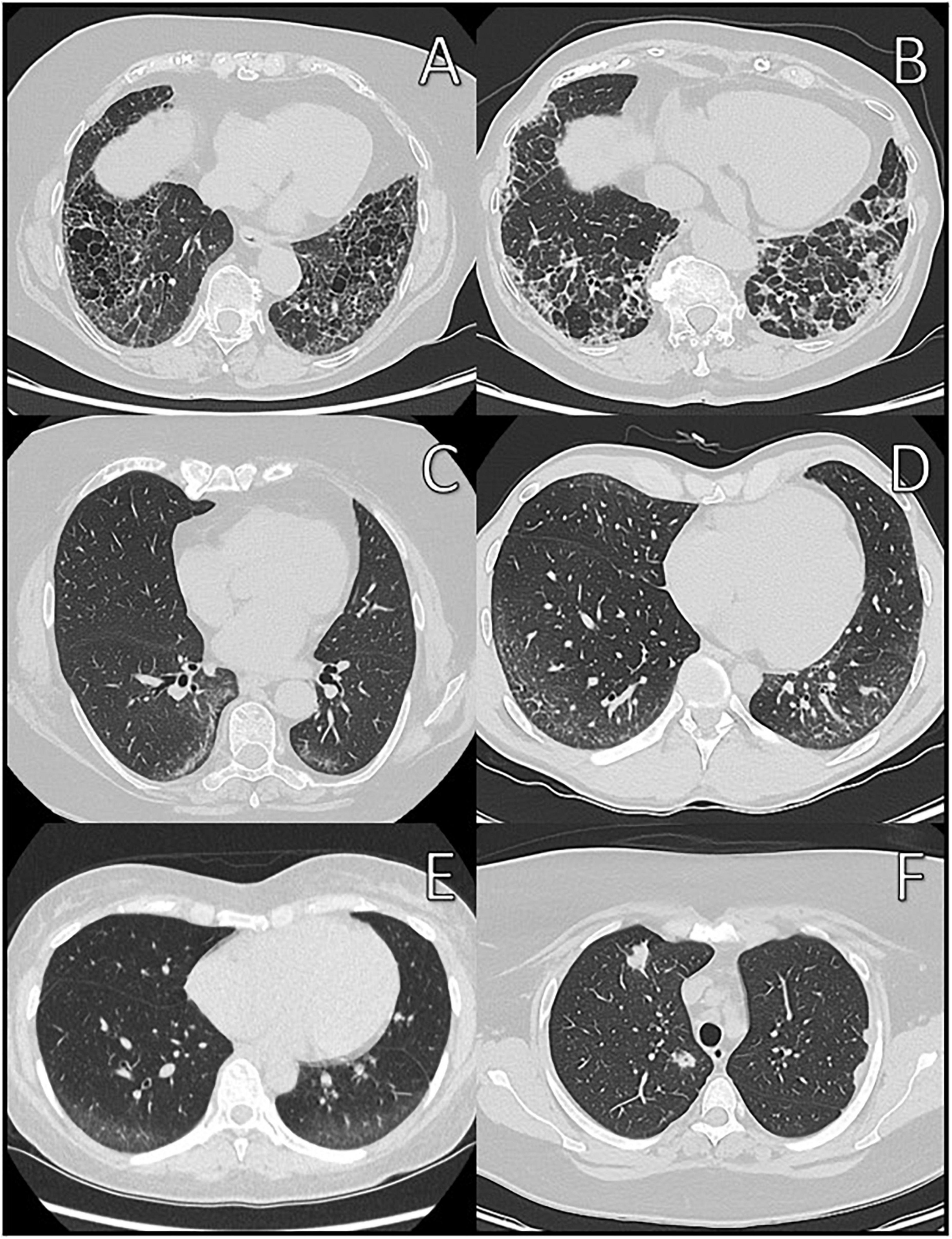
Figure 2. Different CT-patterns in patient with IRD at initial diagnosis. (A) Usual interstitial pneumonia (UIP) in polymyositis; (B) probable UIP in systemic sclerosis; (C,D) non-specific interstitial pneumonia (NSIP) in Sharp syndrome; (E) pure ground-glass opacities in Sharp syndrome; and (F) granuloma/proliferations in granulomatosis with polyangiitis.
It is difficult to define sensitivity and specificity of HRCT in detecting ILD in IRD-patients. Due to the high resolution, HRCT as a single modality has a very high sensitivity of almost 100% for detecting ILD (27). However, the enhanced image resolution can also result in lower specificity due to unspecific findings. For instance, Hoffmann et al. (27) presented a specificity of 55.3% in detecting ILD in newly diagnosed IRD due to unspecific findings or other diseases. According to the Fleischner Society and Putman et al. (70), the specificity of HRCT may not be 100% and not all changes (ILA and indeterminate ILA) should be considered as being related to ILD. Further invasive diagnostic procedures would be necessary for differentiation.
In conclusion, HRCT is an important diagnostic tool in rheumatology. The evidence-based European consensus statements for identification and management of ILD in SSc recommend that SSc-patients should be screened for ILD using HRCT, particularly if they are showing one or more risk factors (19). In addition, the majority of studies regard HRCT generally as the gold standard for the diagnosis of ILD in IRD (49, 50, 55, 57, 73–75).
Magnetic resonance imaging
Currently, MRI of the lungs is not used in clinical routine for diagnosing ILD, but there were some initial studies showing the potential of MRI in ILD. Although the spatial resolution on MRI is lower than on HRCT, it provides satisfactory results with a sensitivity and specificity of 89 and 91%, respectively, in the detection of ILD in direct comparison, but it can differ based on the technique used (76–78).
In addition, there are studies showing that MRI can differentiate between inflammation- and fibrosis-predominant lesions. Yi et al. (79) correlated biopsies with MRI and demonstrated an early enhancement pattern (82%) on dynamic studies in inflammation-predominant biopsy sites.
Overall, a better assessment and monitoring of ILD in IRD, maybe in combination with HRCT, could be achieved with MRI in the future. Furthermore, there is no risk of exposure to radiation during MRI, which seems to be an advantage for the use of monitoring ILD-IRD and treatment effects.
Positron emission tomography/Computed tomography
The addition of PET to CT offers the ability to non-invasively investigate cellular metabolism in vivo and imaging of fine structural details of lung parenchyma (80).
The results of the first study using of 18F-FDG PET/CT for the investigation of IPF and other diffuse parenchymal lung disease (DPLD) indicate that increased glucose metabolism is associated with both the ground-glass and the reticulation/honeycombing HRCT lung changes (67). In addition, the pulmonary uptake of 18F-FDG on PET significantly correlated with global health scores and pulmonary physiologic measurements.
Initial data also suggested similar characteristics in IRD. Thus, Bellando-Randone et al. (81) demonstrated in patients with SSc that morphologically “positive” GGO segments showed an increased 18F-FDG uptake, suggesting the existence of an increased metabolic activity of GGO. According to the authors, these results might indicate that PET/CT may disclose an underlying inflammatory process, which cannot yet be evidenced by HRCT. In addition, Motegi presented similar results in patients with dermatomyositis (82). So far, there are no longitudinal data existing regarding the use of PET/CT in monitoring the course of ILD-IRD. Therefore, further research projects should be initiated to close this knowledge gap and examine the value of this technique in monitoring IRD-patients with known ILD. However, it has to be considered that PET/CT is mainly available in specialized centers and is characterized by high examination costs.
Invasive diagnostic procedures
Bronchoalveolar lavage
Bronchoalveolar lavage cell patterns and other characteristics can be an useful adjunct in patients with suspected ILD and a lack of confident UIP-pattern on HRCT (83). Although a normal BAL does not exclude ILD, the recognition of a predominantly inflammatory cellular pattern in the BAL can be helpful for the clinician to narrow the differential diagnosis of ILD, and perhaps lessens the need to proceed to more invasive procedures, such as surgical lung biopsy (25, 70–72). In addition, infection and malignancy can be excluded. Furthermore, BAL can be easily and safely performed and the risk of complications is lower than in transbronchial biopsy (84, 85). However, BAL should always be interpreted within the clinical context (medical history, physical examination, and imaging) (83, 86). In patients with suspected ILD, the recommended diagnostic examinations performed on BAL fluid include differential cell count, microbiological studies, and malignant cell cytology laboratory testing (see Table 6) (84, 85). The analysis of the cell patterns in BAL is also called immunological BAL. It has already been shown in the literature that the composition of immunological cells can vary depending on the CT pattern. Ryu et al. (87) reported an elevated lymphocyte count in NSIP compared to UIP in IPF-patients. In addition, differential diagnoses can be evaluated. Domagala described a high total cell count and increased pigmented macrophages in the differential diagnosis of RB-ILD (88). Furthermore, biomarkers measured in BAL could have a value in diagnosing ILD in IRD in the future [e.g., matrix metallopeptidase 9 (MMP-9) or CCL7] (89, 90). However, biomarkers are not yet established in the clinical routine. In Table 6 informative value of different BAL parameters in ILD were summarized.
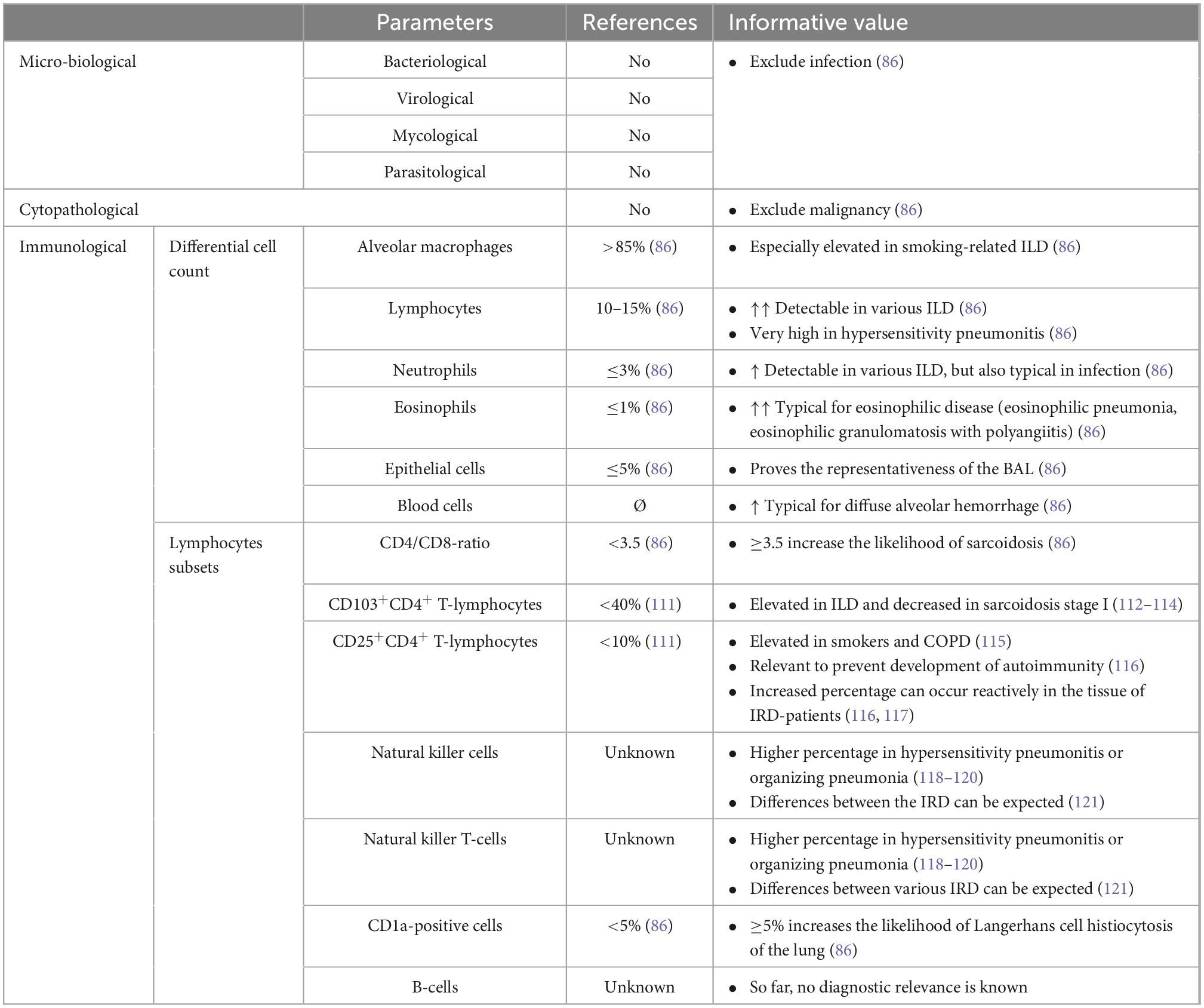
Table 6. Informative value of different parameters in bronchoalveolar lavage (BAL) in ILD.
It should be emphasized that there are no studies or evidence-based recommendations for immunological BAL in diagnosing IRD-ILD available. In addition, protocols for the standardized performance and analysis of a BAL are also lacking which would be essential to compare data. Considering these findings, the diagnostic, prognostic, and therapeutic value of BAL in IRD-ILD remains unclear (91). However, BAL can be a useful tool for the diagnostic evaluation of patients with suspected ILD. In addition, an immunological BAL might be helpful in differentiating between predominantly inflammatory or fibrotic CT patterns in IRD-ILD (23). Further research is necessary to verify these aspects.
In existing ILD in IRD the risk of pulmonary infections (bacteriological, virological, and mycological) is increased with an aggravation due to immunosuppressive therapy (92, 93). Moreover, infection can aggravate clinical symptoms as well as ILD and lead to a delay of the therapy (92, 94). Curtis et al. (94) reported an increased hospitalization rate for RA-ILD patients having a hospitalization for pneumonia in the last 12 months. In this context, BAL can be very helpful for the detection of pulmonary infections and planning an adequate treatment of ILD patients in clinical practice.
Lung biopsy
Currently, biopsies are performed as open surgery or transbronchial biopsy (cryobiopsy or forceps biopsy) (see Figure 3). In IPF, surgical lung biopsy is still an important tool in a subset of patients who cannot be diagnosed based on clinical and imaging features alone (21, 67). According to the White Paper of the Fleischner Society, biopsy should be considered if the clinical context is indeterminate or the HRCT pattern is not definite or probable UIP (21, 67). As highlighted in the update of the ATS/ERS statement on the international classification of idiopathic interstitial pneumonias (IIP), a multidisciplinary approach does not lessen the importance of lung biopsy in the diagnosis of IIPs; rather, it defines the settings where biopsy is more informative than HRCT and those where biopsy is not needed (59).
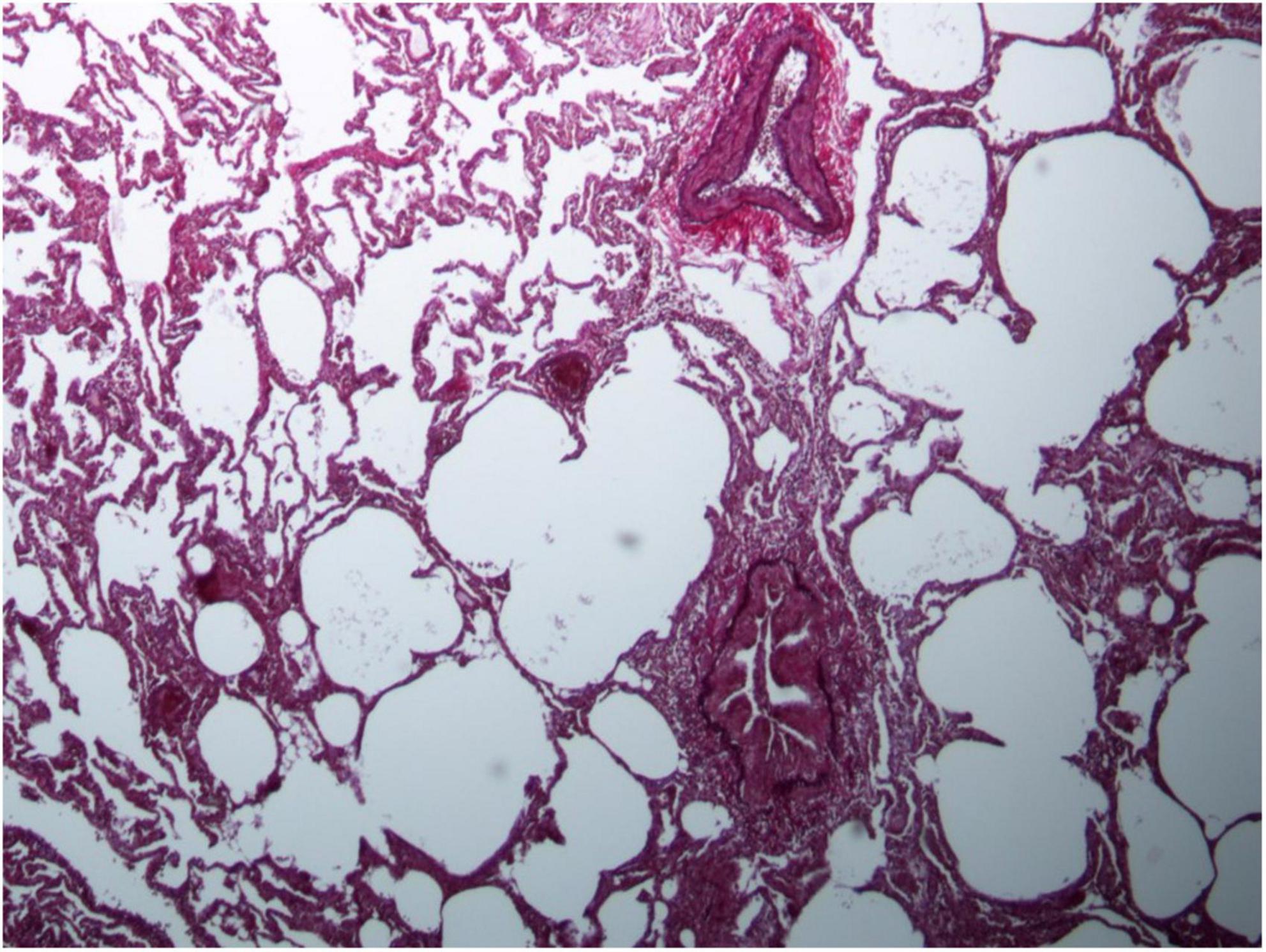
Figure 3. Lung biopsy in patient with MDA5-positive myositis representing with chronic inflammation and subpleural fibrosis.
There are no clear recommendations concerning the diagnostic value of lung biopsy in patients with IRD-ILD. Only a few publications mention the procedure as an additional option to confirm the diagnosis of ILD in IRD (53, 56). This may also be because patients are often considered to be too old or too sick for biopsy (68). Furthermore, major complications are more frequent in transbronchial biopsy (2.7%) than in BAL (0.12%) and in video-assisted thoracoscopic surgery (VATS) (up to 8%) even higher than in transbronchial biopsy (84, 85, 95). Major complications are especially pneumothorax, hemorrhage, respiratory depression, vasovagal episodes, and bronchospasm. In addition, histological knowledge usually does not change the planned therapy (68). In conclusion, lung biopsy can be helpful to exclude other reasons of ILD in IRD-patients and to achieve a higher diagnostic confidence.
Biomarkers
Autoantibodies
Inflammatory rheumatic disease are characterized by immunological laboratory parameters. Numerous autoantibodies are known and are often used to distinguish between the disease entities (e.g., anti-synthetase syndromes). Several serum autoantibodies associated with ILD are described in the literature. In RA, serum rheumatoid factor (RF) and anti-cyclic citrullinated peptide antibodies (anti-CCP) are associated with ILD (51, 96). Regarding patients with SSc, the presence of anti-topoisomerase I (Scl-70) antibodies is associated with progressive ILD and represent an independent risk factor (19). In myositis, myositis-specific and associated antibodies like anti-melanoma differentiation-associated protein 5 (anti-MDA-5) are an independent risk factor for rapid progressive ILD with high mortality, while anti-aminoacyl tRNA synthetase (anti-ARS) antibodies are associated with subacute ILD (97–99).
By using autoantibodies and other laboratory parameters, predictive models for mortality in IRD-patients with ILD were established. Gono et al. (25) reported a prognostic model in patients with myositis, based on serum levels of C-reactive protein (CRP), KL-6, and MDA-5 status. Similar correlations are known for other IRD.
Other blood and non-blood biomarkers
In addition to the traditional autoantibodies, there are other blood and non-blood biomarkers which a potentially associated with IRD-ILD or have a prognostic factor. These biomarkers are the subject of research, but are not yet part of clinical routine.
In RA, different serum biomarkers (e.g., matrix metalloproteinases) and genetic polymorphisms (e.g., MUC5B) are reported with an association to ILD (100, 101). Furthermore, KL-6 is an experimental biomarker for the presence and progression of ILD in SSc (102, 103). There are also non-blood biomarkers, like the measurement of exhaled alveolar nitric oxide (NO), which correlates with the severity of ILD in SSc (104). In addition, there is evidence that intestinal dysbiosis can lead to increased systemic inflammation and increased extraintestinal involvement (105, 106).
Combination of different diagnostic techniques
Combination of clinical examination, pulmonary function test, and imaging
In clinical routine, the diagnosis of IRD-ILD is not made on the basis of a single examination, but is usually based on a combination of different examinations. As described in the literature, the combination of several PFT-parameters did not increase specificity without a significant loss of sensitivity in detecting ILD (49, 50).
Applying a simple clinical decision rule developed by Steele et al. (74) resulted in a sensitivity and specificity of 58.6–88.7% and 60.0%, respectively, in identifying ILD using physical examination or/and chest X-ray. The combination of chest X-ray or PFT (with FVC < 80% and FEV1/FVC > 70%) achieved a sensitivity and specificity of 60.5% and 77.3% with positive likelihood ratio (LR) 2.67 and negative LR of 0.51, respectively (74). Suliman et al. (49) and Bernstein et al. (51) showed sensitivities and specificities of 59.0–74.1% and 45.7–65.8%, respectively, with positive LR of 1.47–1.7 and negative LR of 0.36–0.6, by using a combination of FVC (<80%) and DLCO (<70 or <80%). According to the results gained by Hoffmann et al. (27), combining chest X-ray and PFT (DLCO < 80%) yielded a sensitivity and specificity of 95.2 and 38.7% with a negative LR of 0.12 in newly diagnosed IRD-patients. By combining (1) PFT (DLCO < 80%) and chest X-ray and (2) HRCT, Hoffmann et al. (27) provided a sensitivity and specificity of 95.2 and 77.4% with a negative LR of 0.06 in newly diagnosed IRD-patients.
Combination of clinical examination, pulmonary function test, imaging, invasive techniques, and biomarkers
So far, there is no established algorithm for screening or monitoring of ILD in IRD available. Especially, studies do not exist yet, which examine the value of clinical examination, non-invasive diagnostics (PFT and imaging), invasive techniques (BAL or biopsy), and biomarkers.
Interpretation of these results would also be challenging, because it is difficult to define a gold standard. Perhaps a diagnosis developed within an ILD board on an interdisciplinary basis should become the gold standard. In the future, an algorithm for screening, monitoring, and prognostic assessment could be developed by combining different techniques (non-invasive, imaging, invasive, and biomarkers).
Conclusion
Pulmonary complications in the form of ILD are among the most common and serious complications in IRD patients and may lead to significant morbidity and mortality. Given this background and available modern therapeutic options, early diagnosis of ILD in this patient population is essential.
For some examination techniques such as PFT, 6MWT, and HRCT that are firmly established in clinical practice and widely available, there is clear, broad evidence for their value in screening, monitoring, and prognostic assessment of ILD in IRD. MRI and PET/CT represent additional imaging modalities that may have a greater impact in the future by combining morphological and functional correlations. The results are promising, but further research is needed.
More evidence has also to be demanded on the use of invasive diagnostic methods such as BAL and lung biopsy. Both techniques can support the diagnosis of ILD in IRD, but their additional value [improvement of sensitivity, specificity, NPV, positive predictive value (PPV)] to HRCT remains unclear.
Furthermore, the possibility of a prognostic assessment is still very controversial. There is small evidence for biomarkers in predicting ILD and also on progression of known ILD. In addition, a clear definition of ILD from a rheumatological point of view is missing which would enable clinicians to interpret the available data. This is probably also difficult because there are sliding transitions from no changes to indeterminate ILA to ILA and finally to ILD. Consequently, it is very difficult to define gold standards for diagnosing ILD in IRD-patients.
For many other rheumatological diseases, the principle of “hit hard and early” already applies. Through the improved technology in HRCT, we will increase the proportion of patients with indeterminate ILA. At this point, it is important to differentiate between ILD and non-ILD patients at an early stage. This challenge cannot be addressed by HRCT alone. By combining PFT (in particular DLCO), cardiopulmonary stress tests and HRCT with invasive diagnostics and biomarkers, we might be able to develop an algorithm for screening, but also for monitoring and gaining prognostic information in the future. This would also allow a better management and the implementation of personalized, targeted therapies.
In the future, a combination of various methods (PFT, imaging, invasive diagnostics, and biomarkers) might allow the development of algorithms on the basis of which IRD-patients with ILD can be treated with a personalized, targeted medication.
Author contributions
AP and TH designed the review, collected the data, wrote the manuscript, and revised the manuscript. GW, MF, UT, PO, CK, and NG edited and drafted the manuscript. All authors read and approved the final manuscript.
Acknowledgments
The authors thank Dr. med. Katrina Recker, Hamburg, for the support in editing the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1101448/full#supplementary-material
Abbreviations
6MWT, 6-min walk test; AAV, ANCA-associated vasculitis; ANCA, anti-neutrophil cytoplasmic antibody; anti-ARS, anti-aminoacyl tRNA synthetase antibody; anti-CCP, anti-cyclic citrullinated peptide antibody; anti-MDA-5, anti-melanoma differentiation-associated protein 5 antibody; anti-Scl-70, anti-topoisomerase I antibodies; ATS, American Thoracic Society; BAL, bronchoalveolar lavage; CCL2, chemokine (C-C motif) ligand 2; COPD, chronic obstructive pulmonary disease; CPET, cardiopulmonary exercise test; CRP, C-reactive protein; CTD, connective tissue disease; DLCO, diffusing capacity of the lungs for carbon monoxide; DPLD, diffuse parenchymal lung disease; ERS, European Respiratory Society; FACIT, functional assessment of cancer therapy; FEV1, forced expiratory volume in 1 s; FIP, familiar interstitial pneumonia; FVC, forced vital capacity; GGO, ground-glass opacities; HP, hypersensitivity pneumonia; HRCT, high-resolution computed tomography; IIM, idiopathic inflammatory myositis; IIP, idiopathic interstitial pneumonias; ILA, interstitial lung abnormalities; ILD, interstitial lung disease; IPF, idiopathic pulmonary fibrosis; IRD, inflammatory rheumatic diseases; KL-6, Krebs von den Lungen 6; LR, likelihood ratio; MMP-9, matrix metallopeptidase 9; MRI, magnetic resonance tomography; MUC5B, mucin 5B; NO, nitric oxide; NPV, negative predictive value; NSIP, non-specific interstitial pneumonia; PET/CT, positron emission tomography/computed tomography; PF, pulmonary fibrosis; PFT, pulmonary function tests; PM-DM, polymyositis-dermatomyositis; PPV, positive predictive value; RA, rheumatoid arthritis; RF, rheumatoid factor; SSc, systemic sclerosis; TLC, total lung capacity; TLCO, transfer factor of the lung for carbon monoxide; UIP, usual interstitial pneumonia; VC, vital capacity.
References
1. Al Maini M, Adelowo F, Al Saleh J, Al Weshahi Y, Burmester GR, Cutolo M, et al. The global challenges and opportunities in the practice of rheumatology: white paper by the world forum on rheumatic and musculoskeletal diseases. Clin Rheumatol. (2015) 34:819–29. doi: 10.1007/s10067-014-2841-6
2. Mandl P, Navarro-Compán V, Terslev L, Aegerter P, van der Heijde D, D’Agostino MA, et al. Eular recommendations for the use of imaging in the diagnosis and management of spondyloarthritis in clinical practice. Ann Rheum Dis. (2015) 74:1327–39. doi: 10.1136/annrheumdis-2014-206971
3. Kowal-Bielecka O, Fransen J, Avouac J, Becker M, Kulak A, Allanore Y, et al. Update of eular recommendations for the treatment of systemic sclerosis. Ann Rheum Dis. (2017) 76:1327–39. doi: 10.1136/annrheumdis-2016-209909
4. Kerschbaumer A, Sepriano A, Smolen JS, van der Heijde D, Dougados M, van Vollenhoven R, et al. Efficacy of pharmacological treatment in rheumatoid arthritis: a systematic literature research informing the 2019 update of the eular recommendations for management of rheumatoid arthritis. Ann Rheum Dis. (2020) 79:744–59. doi: 10.1136/annrheumdis-2019-216656
5. Mukhtyar C, Guillevin L, Cid MC, Dasgupta B, de Groot K, Gross W, et al. Eular recommendations for the management of primary small and medium vessel vasculitis. Ann Rheum Dis. (2009) 68:310–7. doi: 10.1136/ard.2008.088096
6. Mammen AL. Autoimmune myopathies: autoantibodies, phenotypes and pathogenesis. Nat Rev Neurol. (2011) 7:343–54. doi: 10.1038/nrneurol.2011.63
7. Hoffmann T, Oelzner P, Busch M, Franz M, Teichgräber U, Kroegel C, et al. Organ manifestation and systematic organ screening at the onset of inflammatory rheumatic diseases. Diagnostics. (2022) 12:67. doi: 10.3390/diagnostics12010067
8. McNearney TA, Reveille JD, Fischbach M, Friedman AW, Lisse JR, Goel N, et al. Pulmonary involvement in systemic sclerosis: associations with genetic, serologic, sociodemographic, and behavioral factors. Arthritis Rheum. (2007) 57:318–26. doi: 10.1002/art.22532
9. Schnabel A, Reuter M, Biederer J, Richter C, Gross WL. Interstitial lung disease in polymyositis and dermatomyositis: clinical course and response to treatment. Semin Arthritis Rheum. (2003) 32:273–84. doi: 10.1053/sarh.2002.50012
10. Bulkley BH, Ridolfi RL, Salyer WR, Hutchins GM. Myocardial lesions of progressive systemic sclerosis. a cause of cardiac dysfunction. Circulation. (1976) 53:483–90. doi: 10.1161/01.cir.53.3.483
11. Moinzadeh P, Aberer E, Ahmadi-Simab K, Blank N, Distler JH, Fierlbeck G, et al. Disease progression in systemic sclerosis-overlap syndrome is significantly different from limited and diffuse cutaneous systemic sclerosis. Ann Rheum Dis. (2015) 74:730–7. doi: 10.1136/annrheumdis-2013-204487
12. Haupt HM, Moore GW, Hutchins GM. The lung in systemic lupus erythematosus. analysis of the pathologic changes in 120 patients. Am J Med. (1981) 71:791–8. doi: 10.1016/0002-9343(81)90366-1
13. Bastian HM, Roseman JM, McGwin G Jr., Alarcón GS, Friedman AW, Fessler BJ, et al. Systemic lupus erythematosus in three ethnic groups. Xii. Risk factors for lupus nephritis after diagnosis. Lupus. (2002) 11:152–60. doi: 10.1191/0961203302lu158oa
14. Bongartz T, Nannini C, Medina-Velasquez YF, Achenbach SJ, Crowson CS, Ryu JH, et al. Incidence and mortality of interstitial lung disease in rheumatoid arthritis: a population-based study. Arthritis Rheum. (2010) 62:1583–91. doi: 10.1002/art.27405
15. Gabbay E, Tarala R, Will R, Carroll G, Adler B, Cameron D, et al. Interstitial lung disease in recent onset rheumatoid arthritis. Am J Respir Crit Care Med. (1997) 156(2 Pt 1):528–35. doi: 10.1164/ajrccm.156.2.9609016
16. Bouros D, Wells AU, Nicholson AG, Colby TV, Polychronopoulos V, Pantelidis P, et al. Histopathologic subsets of fibrosing alveolitis in patients with systemic sclerosis and their relationship to outcome. Am J Respir Crit Care Med. (2002) 165:1581–6. doi: 10.1164/rccm.2106012
17. Hoffmann T, Oelzner P, Böttcher J, Wolf G, Pfeil A. [analysis of referral diagnoses to the rheumatology department]. Z Rheumatol. (2020) 79:160–7. doi: 10.1007/s00393-019-0672-1
18. Doyle TJ, Hunninghake GM, Rosas IO. Subclinical interstitial lung disease: why you should care. Am J Respir Crit Care Med. (2012) 185:1147–53. doi: 10.1164/rccm.201108-1420PP
19. Hoffmann-Vold A-M, Maher TM, Philpot EE, Ashrafzadeh A, Barake R, Barsotti S, et al. The identification and management of interstitial lung disease in systemic sclerosis: evidence-based european consensus statements. Lancet Rheumatol. (2020) 2:e71–83. doi: 10.1016/S2665-9913(19)30144-4
20. Raghu G, Remy-Jardin M, Myers JL, Richeldi L, Ryerson CJ, Lederer DJ, et al. Diagnosis of idiopathic pulmonary fibrosis. An official Ats/Ers/Jrs/Alat clinical practice guideline. Am J Respir Crit Care Med. (2018) 198:e44–68. doi: 10.1164/rccm.201807-1255ST
21. Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, et al. An official Ats/Ers/Jrs/Alat statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. (2011) 183:788–824. doi: 10.1164/rccm.2009-040GL
22. Raghu G, Remy-Jardin M, Richeldi L, Thomson CC, Inoue Y, Johkoh T, et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: an official Ats/Ers/Jrs/Alat clinical practice guideline. Am J Respir Crit Care Med. (2022) 205:e18–47. doi: 10.1164/rccm.202202-0399ST
23. Tomassetti S, Colby TV, Wells AU, Poletti V, Costabel U, Matucci-Cerinic M. Bronchoalveolar lavage and lung biopsy in connective tissue diseases, to do or not to do? Ther Adv Musculoskelet Dis. (2021) 13:1759720x211059605. doi: 10.1177/1759720x211059605
24. Caron M, Hoa S, Hudson M, Schwartzman K, Steele R. Pulmonary function tests as outcomes for systemic sclerosis interstitial lung disease. Eur Respir Rev. (2018) 27:170102. doi: 10.1183/16000617.0102-2017
25. Gono T, Masui K, Nishina N, Kawaguchi Y, Kawakami A, Ikeda K, et al. Risk prediction modeling based on a combination of initial serum biomarker levels in polymyositis/dermatomyositis-associated interstitial lung disease. Arthritis Rheumatol. (2021) 73:677–86. doi: 10.1002/art.41566
26. Goldin JG, Lynch DA, Strollo DC, Suh RD, Schraufnagel DE, Clements PJ, et al. High-resolution Ct scan findings in patients with symptomatic scleroderma-related interstitial lung disease. Chest. (2008) 134:358–67. doi: 10.1378/chest.07-2444
27. Hoffmann T, Oelzner P, Franz M, Teichgräber U, Renz D, Förster M, et al. Assessing the diagnostic value of a potential screening tool for detecting early interstitial lung disease at the onset of inflammatory rheumatic diseases. Arthritis Res Ther. (2022) 24:107. doi: 10.1186/s13075-022-02786-x
28. Capobianco J, Grimberg A, Thompson BM, Antunes VB, Jasinowodolinski D, Meirelles GS. Thoracic manifestations of collagen vascular diseases. Radiographics. (2012) 32:33–50. doi: 10.1148/rg.321105058
29. Oliveira RP, Ribeiro R, Melo L, Grima B, Oliveira S, Alves JD. Connective tissue disease-associated interstitial lung disease. Pulmonology. (2020) 8:53–82. doi: 10.1016/j.pulmoe.2020.01.004
30. Hoffmann-Vold AM, Allanore Y, Alves M, Brunborg C, Airó P, Ananieva LP, et al. Progressive interstitial lung disease in patients with systemic sclerosis-associated interstitial lung disease in the eustar database. Ann Rheum Dis. (2021) 80:219–27. doi: 10.1136/annrheumdis-2020-217455
31. Ye S, Chen XX, Lu XY, Wu MF, Deng Y, Huang WQ, et al. Adult clinically amyopathic dermatomyositis with rapid progressive interstitial lung disease: a retrospective cohort study. Clin Rheumatol. (2007) 26:1647–54. doi: 10.1007/s10067-007-0562-9
32. Highland KB, Distler O, Kuwana M, Allanore Y, Assassi S, Azuma A, et al. Efficacy and safety of nintedanib in patients with systemic sclerosis-associated interstitial lung disease treated with mycophenolate: a subgroup analysis of the senscis trial. Lancet Respir Med. (2021) 9:96–106. doi: 10.1016/s2213-2600(20)30330-1
33. Khanna D, Lin CJF, Furst DE, Goldin J, Kim G, Kuwana M, et al. Tocilizumab in systemic sclerosis: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. (2020) 8:963–74. doi: 10.1016/s2213-2600(20)30318-0
34. Weinrib L, Sharma OP, Quismorio FP Jr. A long-term study of interstitial lung disease in systemic lupus erythematosus. Semin Arthritis Rheum. (1990) 20:48–56. doi: 10.1016/0049-0172(90)90094-v
35. Distler O, Highland KB, Gahlemann M, Azuma A, Fischer A, Mayes MD, et al. Nintedanib for systemic sclerosis-associated interstitial lung disease. N Engl J Med. (2019) 380:2518–28. doi: 10.1056/NEJMoa1903076
36. Lin W, Xin Z, Zhang J, Liu N, Ren X, Liu M, et al. Interstitial lung disease in primary sjögren’s syndrome. BMC Pulm Med. (2022) 22:73. doi: 10.1186/s12890-022-01868-5
37. Bettencourt PE, Del Bono EA, Spiegelman D, Hertzmark E, Murphy RL Jr. Clinical utility of chest auscultation in common pulmonary diseases. Am J Respir Crit Care Med. (1994) 150(5 Pt 1):1291–7. doi: 10.1164/ajrccm.150.5.7952555
38. Spicknall KE, Zirwas MJ, English JC III. Clubbing: an update on diagnosis, differential diagnosis, pathophysiology, and clinical relevance. J Am Acad Dermatol. (2005) 52:1020–8. doi: 10.1016/j.jaad.2005.01.006
39. van Manen MJG, Vermeer LC, Moor CC, Vrijenhoeff R, Grutters JC, Veltkamp M, et al. Clubbing in patients with fibrotic interstitial lung diseases. Respir Med. (2017) 132:226–31. doi: 10.1016/j.rmed.2017.10.021
40. Li J, Liu Y, Li Y, Li F, Wang K, Pan W, et al. Associations between anti-melanoma differentiation-associated gene 5 antibody and demographics, clinical characteristics and laboratory results of patients with dermatomyositis: a systematic meta-analysis. J Dermatol. (2018) 45:46–52. doi: 10.1111/1346-8138.14092
41. Vojinovic T, Cavazzana I, Ceruti P, Fredi M, Modina D, Berlendis M, et al. Predictive features and clinical presentation of interstitial lung disease in inflammatory myositis. Clin Rev Allergy Immunol. (2021) 60:87–94. doi: 10.1007/s12016-020-08814-5
42. Bai Z, Shen G, Dong L. Analysis of risk factors of interstitial lung disease and mortality rates in chinese patients with idiopathic inflammatory myopathy. Int J Rheum Dis. (2021) 24:815–27. doi: 10.1111/1756-185x.14128
43. Graham BL, Steenbruggen I, Miller MR, Barjaktarevic IZ, Cooper BG, Hall GL, et al. Standardization of spirometry 2019 update. an official American thoracic society and European respiratory society technical statement. Am J Respir Crit Care Med. (2019) 200:e70–88. doi: 10.1164/rccm.201908-1590ST
44. Culver BH, Graham BL, Coates AL, Wanger J, Berry CE, Clarke PK, et al. Recommendations for a standardized pulmonary function report. An official American thoracic society technical statement. Am J Respir Crit Care Med. (2017) 196:1463–72. doi: 10.1164/rccm.201710-1981ST
45. Graham BL, Brusasco V, Burgos F, Cooper BG, Jensen R, Kendrick A, et al. 2017 Ers/Ats standards for single-breath carbon monoxide uptake in the lung. Eur Respir J. (2017) 49:1600016. doi: 10.1183/13993003.00016-2016
46. Criée CP, Sorichter S, Smith HJ, Kardos P, Merget R, Heise D, et al. Body plethysmography–its principles and clinical use. Respir Med. (2011) 105:959–71. doi: 10.1016/j.rmed.2011.02.006
47. Coates AL, Peslin R, Rodenstein D, Stocks J. Measurement of lung volumes by plethysmography. Eur Respir J. (1997) 10:1415–27. doi: 10.1183/09031936.97.10061415
48. Forster RE. Exchange of gases between alveolar air and pulmonary capillary blood: pulmonary diffusing capacity. Physiol Rev. (1957) 37:391–452. doi: 10.1152/physrev.1957.37.4.391
49. Suliman YA, Dobrota R, Huscher D, Nguyen-Kim TD, Maurer B, Jordan S, et al. Brief report: pulmonary function tests: high rate of false-negative results in the early detection and screening of scleroderma-related interstitial lung disease. Arthritis Rheumatol. (2015) 67:3256–61. doi: 10.1002/art.39405
50. Showalter K, Hoffmann A, Rouleau G, Aaby D, Lee J, Richardson C, et al. Performance of forced vital capacity and lung diffusion cutpoints for associated radiographic interstitial lung disease in systemic sclerosis. J Rheumatol. (2018) 45:1572–6. doi: 10.3899/jrheum.171362
51. Bernstein EJ, Jaafar S, Assassi S, Domsic RT, Frech TM, Gordon JK, et al. Performance characteristics of pulmonary function tests for the detection of interstitial lung disease in adults with early diffuse cutaneous systemic sclerosis. Arthritis Rheumatol. (2020) 72:1892–6. doi: 10.1002/art.41415
52. Newall C, Schinke S, Savage CO, Hill S, Harper L. Impairment of lung function, health status and functional capacity in patients with anca-associated vasculitis. Rheumatology. (2005) 44:623–8. doi: 10.1093/rheumatology/keh548
53. Rosenberg DM, Weinberger SE, Fulmer JD, Flye MW, Fauci AS, Crystal RG. Functional correlates of lung involvement in wegener’s granulomatosis. use of pulmonary function tests in staging and follow-up. Am J Med. (1980) 69:387–94. doi: 10.1016/0002-9343(80)90009-1
54. Ideura G, Hanaoka M, Koizumi T, Fujimoto K, Shimojima Y, Ishii W, et al. Interstitial lung disease associated with amyopathic dermatomyositis: review of 18 Cases. Respir Med. (2007) 101:1406–11. doi: 10.1016/j.rmed.2007.01.023
55. Chua F, Higton AM, Colebatch AN, O’Reilly K, Grubnic S, Vlahos I, et al. Idiopathic inflammatory myositis-associated interstitial lung disease: ethnicity differences and lung function trends in a British cohort. Rheumatology. (2012) 51:1870–6. doi: 10.1093/rheumatology/kes167
56. Won Huh J, Soon Kim D, Keun Lee C, Yoo B, Bum Seo J, Kitaichi M, et al. Two distinct clinical types of interstitial lung disease associated with polymyositis-dermatomyositis. Respir Med. (2007) 101:1761–9. doi: 10.1016/j.rmed.2007.02.017
57. Fathi M, Dastmalchi M, Rasmussen E, Lundberg IE, Tornling G. Interstitial lung disease, a common manifestation of newly diagnosed polymyositis and dermatomyositis. Ann Rheum Dis. (2004) 63:297–301. doi: 10.1136/ard.2003.006122
58. Noble PW, Albera C, Bradford WZ, Costabel U, Glassberg MK, Kardatzke D, et al. Pirfenidone in patients with idiopathic pulmonary fibrosis (capacity): two randomised trials. Lancet. (2011) 377:1760–9. doi: 10.1016/s0140-6736(11)60405-4
59. Richeldi L, du Bois RM, Raghu G, Azuma A, Brown KK, Costabel U, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. (2014) 370:2071–82. doi: 10.1056/NEJMoa1402584
60. Hoffmann-Vold AM, Aaløkken TM, Lund MB, Garen T, Midtvedt Ø, Brunborg C, et al. Predictive value of serial high-resolution computed tomography analyses and concurrent lung function tests in systemic sclerosis. Arthritis Rheumatol. (2015) 67:2205–12. doi: 10.1002/art.39166
61. Ats Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. Ats statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. (2002) 166:111–7. doi: 10.1164/ajrccm.166.1.at1102
62. American Thoracic Society, American College of Chest Physicians. Ats/Accp statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. (2003) 167:211–77. doi: 10.1164/rccm.167.2.211
63. Holland AE, Spruit MA, Troosters T, Puhan MA, Pepin V, Saey D, et al. An official European respiratory society/American thoracic society technical standard: field walking tests in chronic respiratory disease. Eur Respir J. (2014) 44:1428–46. doi: 10.1183/09031936.00150314
64. Dowman LM, McDonald CF, Hill CJ, Lee AL, Barker K, Boote C, et al. The evidence of benefits of exercise training in interstitial lung disease: a randomised controlled trial. Thorax. (2017) 72:610–9. doi: 10.1136/thoraxjnl-2016-208638
65. Keogh BA, Lakatos E, Price D, Crystal RG. Importance of the lower respiratory tract in oxygen transfer. exercise testing in patients with interstitial and destructive lung disease. Am Rev Respir Dis. (1984) 129(2 Pt 2):S76–80. doi: 10.1164/arrd.1984.129.2P2.S76
66. Hatabu H, Hunninghake GM, Richeldi L, Brown KK, Wells AU, Remy-Jardin M, et al. Interstitial lung abnormalities detected incidentally on ct: a position paper from the fleischner society. Lancet Respir Med. (2020) 8:726–37. doi: 10.1016/s2213-2600(20)30168-5
67. Lynch DA, Sverzellati N, Travis WD, Brown KK, Colby TV, Galvin JR, et al. Diagnostic criteria for idiopathic pulmonary fibrosis: a fleischner society white paper. Lancet Respir Med. (2018) 6:138–53. doi: 10.1016/s2213-2600(17)30433-2
68. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This Joint Statement of the American Thoracic Society (Ats), and the European Respiratory Society (Ers) was adopted by the Ats Board of Directors, June 2001 and by the Ers Executive Committee, June 2001. Am J Respir Crit Care Med. (2002) 165:277–304. doi: 10.1164/ajrccm.165.2.ats01
69. Travis WD, Costabel U, Hansell DM, King TE Jr., Lynch DA, Nicholson AG, et al. An official American thoracic society/European respiratory society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. (2013) 188:733–48. doi: 10.1164/rccm.201308-1483ST
70. Putman RK, Hatabu H, Araki T, Gudmundsson G, Gao W, Nishino M, et al. Association between interstitial lung abnormalities and all-cause mortality. Jama. (2016) 315:672–81. doi: 10.1001/jama.2016.0518
71. Remy-Jardin M, Giraud F, Remy J, Copin MC, Gosselin B, Duhamel A. Importance of ground-glass attenuation in chronic diffuse infiltrative lung disease: pathologic-Ct correlation. Radiology. (1993) 189:693–8. doi: 10.1148/radiology.189.3.8234692
72. El-Sherief AH, Gilman MD, Healey TT, Tambouret RH, Shepard JA, Abbott GF, et al. Clear vision through the haze: a practical approach to ground-glass opacity. Curr Probl Diagn Radiol. (2014) 43:140–58. doi: 10.1067/j.cpradiol.2014.01.004
73. Hax V, Bredemeier M, Didonet Moro AL, Pavan TR, Vieira MV, Pitrez EH, et al. Clinical algorithms for the diagnosis and prognosis of interstitial lung disease in systemic sclerosis. Semin Arthritis Rheum. (2017) 47:228–34. doi: 10.1016/j.semarthrit.2017.03.019
74. Steele R, Hudson M, Lo E, Baron M. Clinical decision rule to predict the presence of interstitial lung disease in systemic sclerosis. Arthritis Care Res. (2012) 64:519–24. doi: 10.1002/acr.21583
75. Hervier B, Devilliers H, Stanciu R, Meyer A, Uzunhan Y, Masseau A, et al. Hierarchical cluster and survival analyses of antisynthetase syndrome: phenotype and outcome are correlated with anti-TRNA synthetase antibody specificity. Autoimmun Rev. (2012) 12:210–7. doi: 10.1016/j.autrev.2012.06.006
76. Lutterbey G, Gieseke J, von Falkenhausen M, Morakkabati N, Schild H. Lung Mri at 3.0 T: a comparison of helical ct and high-field MRI in the detection of diffuse lung disease. Eur Radiol. (2005) 15:324–8. doi: 10.1007/s00330-004-2548-1
77. Rajaram S, Swift AJ, Capener D, Telfer A, Davies C, Hill C, et al. Lung morphology assessment with balanced steady-state free precession Mr imaging compared with Ct. Radiology. (2012) 263:569–77. doi: 10.1148/radiol.12110990
78. Pinal-Fernandez I, Pineda-Sanchez V, Pallisa-Nuñez E, Simeon-Aznar CP, Selva-O’Callaghan A, Fonollosa-Pla V, et al. Fast 1.5 t Chest Mri for the assessment of interstitial lung disease extent secondary to systemic sclerosis. Clin Rheumatol. (2016) 35:2339–45. doi: 10.1007/s10067-016-3267-0
79. Yi CA, Lee KS, Han J, Chung MP, Chung MJ, Shin KM. 3-T Mri for differentiating inflammation- and fibrosis-predominant lesions of usual and nonspecific interstitial pneumonia: comparison study with pathologic correlation. AJR Am J Roentgenol. (2008) 190:878–85. doi: 10.2214/ajr.07.2833
80. Groves AM, Win T, Screaton NJ, Berovic M, Endozo R, Booth H, et al. Idiopathic pulmonary fibrosis and diffuse parenchymal lung disease: implications from initial experience with 18f-Fdg Pet/Ct. J Nucl Med. (2009) 50:538–45. doi: 10.2967/jnumed.108.057901
81. Bellando-Randone S, Tartarelli L, Cavigli E, Tofani L, Bruni C, Lepri G, et al. 18f-fluorodeoxyglucose positron-emission tomography/Ct and lung involvement in systemic sclerosis. Ann Rheum Dis. (2019) 78:577–8. doi: 10.1136/annrheumdis-2018-213376
82. Motegi SI, Fujiwara C, Sekiguchi A, Hara K, Yamaguchi K, Maeno T, et al. Clinical value of (18) F-fluorodeoxyglucose positron emission tomography/computed tomography for interstitial lung disease and myositis in patients with dermatomyositis. J Dermatol. (2019) 46:213–8. doi: 10.1111/1346-8138.14758
83. Meyer KC, Raghu G. Bronchoalveolar lavage for the evaluation of interstitial lung disease: is it clinically useful? Eur Respir J. (2011) 38:761–9. doi: 10.1183/09031936.00069509
84. Simpson FG, Arnold AG, Purvis A, Belfield PW, Muers MF, Cooke NJ. Postal survey of bronchoscopic practice by physicians in the United Kingdom. Thorax. (1986) 41:311–7. doi: 10.1136/thx.41.4.311
85. Ahmad M, Livingston DR, Golish JA, Mehta AC, Wiedemann HP. The safety of outpatient transbronchial biopsy. Chest. (1986) 90:403–5. doi: 10.1378/chest.90.3.403
86. Meyer KC, Raghu G, Baughman RP, Brown KK, Costabel U, du Bois RM, et al. An official American thoracic society clinical practice guideline: the clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am J Respir Crit Care Med. (2012) 185:1004–14. doi: 10.1164/rccm.201202-0320ST
87. Ryu YJ, Chung MP, Han J, Kim TS, Lee KS, Chun EM, et al. Bronchoalveolar lavage in fibrotic idiopathic interstitial pneumonias. Respir Med. (2007) 101:655–60. doi: 10.1016/j.rmed.2006.06.003
88. Domagała-Kulawik J. Bal in the diagnosis of smoking-related interstitial lung diseases: review of literature and analysis of our experience. Diagn Cytopathol. (2008) 36:909–15. doi: 10.1002/dc.20944
89. Prasse A, Pechkovsky DV, Toews GB, Schäfer M, Eggeling S, Ludwig C, et al. Ccl18 as an indicator of pulmonary fibrotic activity in idiopathic interstitial pneumonias and systemic sclerosis. Arthritis Rheum. (2007) 56:1685–93. doi: 10.1002/art.22559
90. Andersen GN, Nilsson K, Pourazar J, Hackett TL, Kazzam E, Blomberg A, et al. Bronchoalveolar matrix metalloproteinase 9 relates to restrictive lung function impairment in systemic sclerosis. Respir Med. (2007) 101:2199–206. doi: 10.1016/j.rmed.2007.04.019
91. Costabel U, Guzman J, Bonella F, Oshimo S. Bronchoalveolar lavage in other interstitial lung diseases. Semin Respir Crit Care Med. (2007) 28:514–24. doi: 10.1055/s-2007-991525
92. Zamora-Legoff JA, Krause ML, Crowson CS, Ryu JH, Matteson EL. Risk of serious infection in patients with rheumatoid arthritis-associated interstitial lung disease. Clin Rheumatol. (2016) 35:2585–9. doi: 10.1007/s10067-016-3357-z
93. Barnes H, Holland AE, Westall GP, Goh NS, Glaspole IN. Cyclophosphamide for connective tissue disease-associated interstitial lung disease. Cochrane Database Syst Rev. (2018) 1:Cd010908. doi: 10.1002/14651858.CD010908.pub2
94. Curtis JR, Sarsour K, Napalkov P, Costa LA, Schulman KL. Incidence and complications of interstitial lung disease in users of tocilizumab, rituximab, abatacept and anti-tumor necrosis factor A agents, a retrospective cohort study. Arthritis Res Ther. (2015) 17:319. doi: 10.1186/s13075-015-0835-7
95. Pastre J, Khandhar S, Barnett S, Ksovreli I, Mani H, Brown AW, et al. Surgical lung biopsy for interstitial lung disease. Safety and feasibility at a tertiary referral center. Ann Am Thorac Soc. (2021) 18:460–7. doi: 10.1513/AnnalsATS.202006-759OC
96. Khan T, Jose RJ, Renzoni EA, Mouyis M. A closer look at the role of Anti-Ccp antibodies in the pathogenesis of rheumatoid arthritis-associated interstitial lung disease and bronchiectasis. Rheumatol Ther. (2021) 8:1463–75. doi: 10.1007/s40744-021-00362-4
97. Satoh M, Tanaka S, Ceribelli A, Calise SJ, Chan EK. A comprehensive overview on myositis-specific antibodies: new and old biomarkers in idiopathic inflammatory myopathy. Clin Rev Allergy Immunol. (2017) 52:1–19. doi: 10.1007/s12016-015-8510-y
98. Selva-O’Callaghan A, Labrador-Horrillo M, Muñoz-Gall X, Martínez-Gomez X, Majó-Masferrer J, Solans-Laque R, et al. Polymyositis/dermatomyositis-associated lung disease: analysis of a series of 81 patients. Lupus. (2005) 14:534–42. doi: 10.1191/0961203305lu2158oa
99. Sato S, Hirakata M, Kuwana M, Suwa A, Inada S, Mimori T, et al. Autoantibodies to a 140-Kd polypeptide, Cadm-140, in Japanese patients with clinically amyopathic dermatomyositis. Arthritis Rheum. (2005) 52:1571–6. doi: 10.1002/art.21023
100. Juge PA, Lee JS, Ebstein E, Furukawa H, Dobrinskikh E, Gazal S, et al. Muc5b promoter variant and rheumatoid arthritis with interstitial lung disease. N Engl J Med. (2018) 379:2209–19. doi: 10.1056/NEJMoa1801562
101. Kass DJ, Nouraie M, Glassberg MK, Ramreddy N, Fernandez K, Harlow L, et al. Comparative profiling of serum protein biomarkers in rheumatoid arthritis-associated interstitial lung disease and idiopathic pulmonary fibrosis. Arthritis Rheumatol. (2020) 72:409–19. doi: 10.1002/art.41123
102. Ko UW, Cho EJ, Oh HB, Koo HJ, Do KH, Song JW. Serum krebs von den lungen-6 level predicts disease progression in interstitial lung disease. PLoS One. (2020) 15:e0244114. doi: 10.1371/journal.pone.0244114
103. Benyamine A, Heim X, Resseguier N, Bertin D, Gomez C, Ebbo M, et al. Elevated serum krebs von den lungen-6 in systemic sclerosis: a marker of lung fibrosis and severity of the disease. Rheumatol Int. (2018) 38:813–9. doi: 10.1007/s00296-018-3987-3
104. Hoang-Duc H, Pham-Huy Q, Vu-Minh T, Duong-Quy S. Study of the correlation between Hrct semi-quantitative scoring, concentration of alveolar nitric oxide, and clinical-functional parameters of systemic sclerosis-induced interstitial lung disease. Yale J Biol Med. (2020) 93:657–67.
105. Andréasson K, Alrawi Z, Persson A, Jönsson G, Marsal J. Intestinal dysbiosis is common in systemic sclerosis and associated with gastrointestinal and extraintestinal features of disease. Arthritis Res Ther. (2016) 18:278. doi: 10.1186/s13075-016-1182-z
106. Mandl T, Marsal J, Olsson P, Ohlsson B, Andréasson K. Severe intestinal dysbiosis is prevalent in primary sjögren’s syndrome and is associated with systemic disease activity. Arthritis Res Ther. (2017) 19:237. doi: 10.1186/s13075-017-1446-2
107. Hoffmann-Vold AM, Fretheim H, Halse AK, Seip M, Bitter H, Wallenius M, et al. Tracking impact of interstitial lung disease in systemic sclerosis in a complete Nationwide cohort. Am J Respir Crit Care Med. (2019) 200:1258–66. doi: 10.1164/rccm.201903-0486OC
108. Wells AU, Hansell DM, Rubens MB, King AD, Cramer D, Black CM, et al. Fibrosing alveolitis in systemic sclerosis: indices of lung function in relation to extent of disease on computed tomography. Arthritis Rheum. (1997) 40:1229–36.
109. Goh NS, Desai SR, Veeraraghavan S, Hansell DM, Copley SJ, Maher TM, et al. Interstitial lung disease in systemic sclerosis: a simple staging system. Am J Respir Crit Care Med. (2008) 177:1248–54. doi: 10.1164/rccm.200706-877OC
110. Fischer A, Antoniou KM, Brown KK, Cadranel J, Corte TJ, du Bois RM, et al. An official European respiratory society/american thoracic society research statement: interstitial pneumonia with autoimmune features. Eur Respir J. (2015) 46:976–87. doi: 10.1183/13993003.00150-2015
111. Kroegel C, Bonella F. Klinische Pneumologie : Das Referenzwerk Für Klinik Und Praxis. New York, NY: Thieme (2014).
112. Lohmeyer J, Friedrich J, Grimminger F, Maus U, Tenter R, Morr H, et al. Expression of mucosa-related integrin alphaebeta7 on alveolar t cells in interstitial lung diseases. Clin Exp Immunol. (1999) 116:340–6. doi: 10.1046/j.1365-2249.1999.00894.x
113. Bretagne L, Diatta ID, Faouzi M, Nobile A, Bongiovanni M, Nicod LP, et al. Diagnostic value of the Cd103+Cd4+/Cd4+ ratio to differentiate sarcoidosis from other causes of lymphocytic alveolitis. Respiration. (2016) 91:486–96. doi: 10.1159/000446606
114. Braun RK, Foerster M, Grahmann PR, Haefner D, Workalemahu G, Kroegel C. Phenotypic and molecular characterization of Cd103+ Cd4+ T Cells in bronchoalveolar lavage from patients with interstitial lung diseases. Cytometry B Clin Cytom. (2003) 54:19–27. doi: 10.1002/cyto.b.10021
115. Roos-Engstrand E, Pourazar J, Behndig AF, Bucht A, Blomberg A. Expansion of Cd4+Cd25+ Helper T cells without regulatory function in smoking and copd. Respir Res. (2011) 12:74. doi: 10.1186/1465-9921-12-74
116. Liu H, Leung BP. Cd4+Cd25+ regulatory T cells in health and disease. Clin Exp Pharmacol Physiol. (2006) 33:519–24. doi: 10.1111/j.1440-1681.2006.04401.x
117. van Amelsfort JM, Jacobs KM, Bijlsma JW, Lafeber FP, Taams LS. Cd4(+)Cd25(+) regulatory T cells in rheumatoid arthritis: differences in the presence, phenotype, and function between peripheral blood and synovial fluid. Arthritis Rheum. (2004) 50:2775–85. doi: 10.1002/art.20499
118. Sokhatska O, Padrão E, Sousa-Pinto B, Beltrão M, Mota PC, Melo N, et al. Nk and Nkt cells in the diagnosis of diffuse lung diseases presenting with a lymphocytic alveolitis. BMC Pulm Med. (2019) 19:39. doi: 10.1186/s12890-019-0802-1
119. Papakosta D, Manika K, Gounari E, Kyriazis G, Kontakiotis T, Spyropoulos G, et al. Bronchoalveolar lavage fluid and blood natural killer and natural killer t-like cells in cryptogenic organizing pneumonia. Respirology. (2014) 19:748–54. doi: 10.1111/resp.12305
120. Tøndell A, Rø AD, Børset M, Moen T, Sue-Chu M. Activated Cd8+ T cells and natural killer T cells in bronchoalveolar lavage fluid in hypersensitivity pneumonitis and sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis. (2015) 31:316–24.
Keywords: inflammatory rheumatic disease, interstitial lung disease, pulmonary function tests, high-resolution computed tomography (HRCT), bronchoalveolar lavage (BAL), PET/CT
Citation: Hoffmann T, Oelzner P, Teichgräber U, Franz M, Gaßler N, Kroegel C, Wolf G and Pfeil A (2023) Diagnosing lung involvement in inflammatory rheumatic diseases—Where do we currently stand? Front. Med. 9:1101448. doi: 10.3389/fmed.2022.1101448
Received: 17 November 2022; Accepted: 19 December 2022;
Published: 11 January 2023.
Edited by:
Jiuliang Zhao, Peking Union Medical College Hospital (CAMS), ChinaReviewed by:
Roberto Carbone, University of Genoa, ItalyMariaenrica Tinè, University of Padua, Italy
Copyright © 2023 Hoffmann, Oelzner, Teichgräber, Franz, Gaßler, Kroegel, Wolf and Pfeil. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tobias Hoffmann,  VG9iaWFzLkhvZmZtYW5uQG1lZC51bmktamVuYS5kZQ==
VG9iaWFzLkhvZmZtYW5uQG1lZC51bmktamVuYS5kZQ==
†Deceased