 Joe M. O’Sullivan1*
Joe M. O’Sullivan1* Rana R. McKay2Kambiz Rahbar3Karim Fizazi4
Rana R. McKay2Kambiz Rahbar3Karim Fizazi4 Daniel J. George5Bertrand Tombal6Anja Schmall7Per Sandström8Frank Verholen7
Daniel J. George5Bertrand Tombal6Anja Schmall7Per Sandström8Frank Verholen7 Neal Shore9
Neal Shore9- 1Patrick G. Johnston Centre for Cancer Research, Queen’s University Belfast and Northern Ireland Cancer Centre, Belfast, United Kingdom
- 2Division of Hematology-Oncology, Department of Medicine, University of California, San Diego, La Jolla, CA, United States
- 3Department of Nuclear Medicine, University of Münster Medical Center, Münster, Germany
- 4Institut Gustave Roussy, University of Paris-Saclay, Villejuif, France
- 5Duke University School of Medicine, Durham, NC, United States
- 6Division of Urology, Institut de Recherche Clinique (IREC), Cliniques Universitaires Saint Luc, Brussels, Belgium
- 7Bayer Consumer Care, Basel, Switzerland
- 8Bayer HealthCare Pharmaceuticals, Whippany, NJ, United States
- 9Carolina Urologic Research Center, Myrtle Beach, SC, United States
Radium-223 dichloride (223Ra) is an α-emitter approved for the treatment of metastatic castration-resistant prostate cancer (mCRPC) with bone metastases, but without visceral involvement. Despite being a life-prolonging therapy (LPT), 223Ra remains underutilized. A large body of real-world evidence (RWE) for 223Ra has been published in the decade since the pivotal phase 3 ALSYMPCA study, a period during which the treatment landscape has continued to evolve. How to optimize 223Ra use, including how to integrate it into the mCRPC management pathway amongst other current LPTs (i.e., with respect to timing and concurrent, layered, or sequential use), is therefore of considerable interest. RWE studies lack the conventional restraints of clinical trials and can therefore help to build an understanding of how treatments may be best used in routine practice. Here we review RWE studies investigating the efficacy and safety of 223Ra in mCRPC [including in sequence with the recently approved 177-Lutetium conjugated to the ligand prostate-specific membrane antigen (177Lu-PSMA)], as well as response marker development, imaging techniques, and current clinical practice recommendations.
1 Introduction
The radionuclide radium-223 dichloride (223Ra) is a life-prolonging therapy (LPT) in oncology (1), paving the way as the first approved α-emitter. 223Ra is approved for the treatment of metastatic castration-resistant prostate cancer (mCRPC) with bone metastases, but without visceral involvement (2, 3), with metastatic prostate cancer being primarily a bone-related disease (4), unlike other cancers. This approval was based on improvements in overall survival (OS) vs. placebo [14.9 vs. 11.3 months; hazard ratio (HR) 0.70; 95% confidence interval (CI) 0.58–0.83, P < 0.001] in patients with mCRPC (including those with low-volume lymph node metastases), with or without prior chemotherapy, in the pivotal phase 3 ALSYMPCA study (5).
In addition to investigating efficacy and safety in a real-world setting, the challenges of 223Ra being the first approved α-emitter (e.g., accessibility and understanding of mechanism of action and appropriate usage) also needed to be overcome, with implementation (logistics) and physician and patient education being key to its uptake in clinical practice. However, 223Ra remains underutilized for various reasons, including lack of prostate-specific antigen (PSA) response, intravenous administration issues and the continued use of back-to-back androgen receptor pathway inhibitor (ARPI) regimens [despite a lack of ARPI re-challenge efficacy and current guidelines (6–9) recommending multiple lines of ARPIs are avoided] (10, 11).
Since ALSYMPCA completion, the treatment landscape has evolved. Several currently approved LPTs, specifically the ARPIs abiraterone (12, 13) enzalutamide (14, 15), apalutamide (16), and darolutamide (17), the poly (adenosine diphosphate-ribose) polymerase inhibitor olaparib (18, 19), the immunotherapy sipuleucel-T (20), and 177-Lutetium conjugated to the ligand prostate-specific membrane antigen (177Lu-PSMA-617) (21), were unavailable outside of randomized clinical trials (RCTs) during ALSYMPCA. Furthermore, although docetaxel and cabazitaxel were approved in mCRPC at the time of ALSYMPCA, their position in the treatment pathway has since changed. Consequently, ensuring the appropriate choice of patients and treatment sequence for 223Ra is key to maximizing therapeutic benefit. There is thus a need for RCTs of 223Ra regimens in the current mCRPC landscape, some of which are currently underway [RADIANT (phase 4, 223Ra vs. ARPI), PEACE III (phase 3, 223Ra plus enzalutamide vs. enzalutamide alone) and DORA (phase 3, 223Ra plus docetaxel vs. docetaxel alone)] (22–24), and for real-world evidence (RWE).
Unlike RCTs, RWE gathers data from non-interventional studies, clinical registries and other sources reflecting routine clinical practice, thus helping to refine a treatment’s therapeutic index without conventional RCT constraints (25). RWE studies can complement RCTs, especially for patients ineligible for RCT inclusion and where Level 1 evidence is lacking. Despite recommended treatment algorithms, variability exists in individual treatment pathways, particularly with some mCRPC therapeutic options moving to earlier disease stages and issues around undertreatment (26, 27). Here we review RWE studies (retrospective unless otherwise specified) investigating 223Ra in mCRPC, with discussion focusing on studies with N > 100, except where data are limited.
2 Efficacy
Real-world OS in patients treated with 223Ra was 8.2–29 months (Supplementary Table 1), a range that encompasses the median OS of 14.9 months reported in ALSYMPCA. However, survival outcomes are influenced by patient selection as well as therapy choice, and the studies included in this review vary by patient characteristics, study designs, and prior therapies.
2.1 Treatment completion
OS benefits were more notable (P < 0.01 where reported) in patients who completed 5–6 vs. fewer cycles of 223Ra (28–34) (Figure 1A). Factors associated with completion of 5–6 cycles in some studies included certain patient/disease characteristics (29, 33, 35, 36) [e.g., lower PSA or alkaline phosphatase (ALP) (35) and absolute neutrophil count at least lower limit of normal (36)] and earlier 223Ra use (29) (Figure 1B). Indeed, there was a higher likelihood of completing all 6 cycles of 223Ra when it was given prior- vs. post-chemotherapy (P < 0.001) (32). However, 223Ra position in the treatment sequence (i.e., line 1 vs. 2 or ≥ 3) had no impact on treatment completion in another study (35). Moreover, there was also a greater likelihood of the mean number of 223Ra cycles being higher when 223Ra was used as combination therapy rather than monotherapy (P = 0.003) (32).
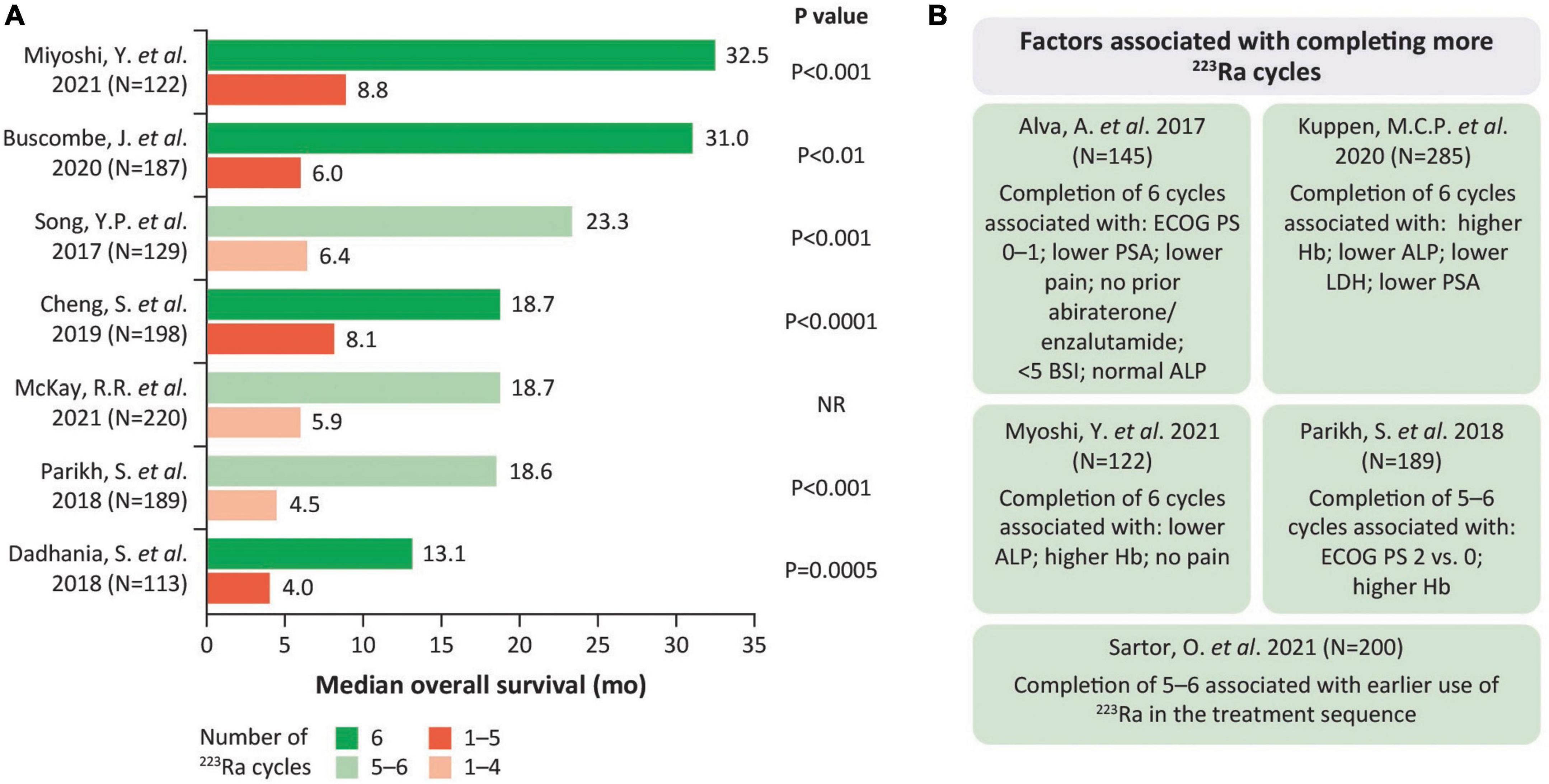
Figure 1. Completing more 223Ra cycles is associated with longer OS. (A) Median OS by 223Ra cycle number. (B) Factors associated with completing more 223Ra cycles. ALP, alkaline phosphatase; BSI, bone scan index; ECOG PS, Eastern Cooperative Oncology Group performance status; Hb, hemoglobin; LDH, lactate dehydrogenase; OS, overall survival; PSA, prostate-specific antigen.
2.2 Treatment sequence
223Ra use earlier in the mCRPC treatment pathway may improve survival outcomes, according to some studies (35, 37). Median survival was greater in patients with one vs. two prior therapies (14.7 vs. 11.2 months; P = 0.03) in one study (37), and another demonstrated worse OS with 223Ra used as line ≥ 3 vs. line 1 (HR 3.267; P < 0.01) (35). However, other studies found OS did not significantly differ by prior line of therapy (0 vs. ≥ 1 or across lines 0, 1, 2, 3, or 4) (38), and was generally similar (14.3–14.7 months) when 223Ra was given immediately after abiraterone as treatment line 2, 3, or ≥ 4 (39).
Similarly, a greater OS benefit was seen with 223Ra used pre- vs. post-chemotherapy in one study (12.3 vs. 8.1 months; P = 0.02), although prior enzalutamide or abiraterone plus prednisolone treatment had no significant OS impact (40). By contrast, another study found no significant OS difference with 223Ra pre- vs. post chemotherapy (including when patients receiving 223Ra in combination with enzalutamide or abiraterone were excluded; the safety of these combinations are discussed in section “3 Safety”) (32). Furthermore, prior cabazitaxel use was not a predictor of OS in a prospective registry analysis (41), and prior docetaxel use had no significant impact on survival in another study (34).
3 Safety
In short- and long-term analyses of ALSYMPCA, 223Ra had limited myelosuppressive effects and was well tolerated, without major safety concerns (5, 42). RWE has similarly indicated that 223Ra is safe and well tolerated in patients with mCRPC (Supplementary Table 2), and importantly demonstrated a lack of rare treatment-emergent adverse events (TEAEs), e.g., second malignancies or cardiovascular events, which RCTs would be underpowered to detect.
When 223Ra monotherapy was compared with standard-of-care, the estimated 36-month fracture risk in the respective groups was 19% vs. 10% (HR 1.61; 95% CI: 0.96–3.02) (43). Regimens combining use of 223Ra and abiraterone (plus prednisolone) or enzalutamide have been reported in real-world studies (44–48). However, based on a significantly increased risk of fractures when 223Ra was used in combination with abiraterone plus prednisolone in the ERA 223 phase 3 RCT (49), this combination is now contraindicated in the EU (2) and is not recommended in the US (3). Of note, in the ERA 223 trial, the incidence of fractures was lower in patients who were taking bone protecting agents (bisphosphonates or denosumab) at baseline (15 and 7% in the 223Ra and placebo groups, respectively) than in patients not taking bone protective agents (37 and 15%, respectively) (49). Furthermore, an increased fracture risk was also reported with 223Ra plus enzalutamide vs. enzalutamide in the phase 3 PEACE III RCT, although fracture risk was largely eliminated in each treatment group with preventative use of bone protecting agents (denosumab and zoledronic acid) (50). Increased fracture risk due to therapy-induced bone loss has been seen for several systemic therapies for prostate cancer, and fracture risk is increased in patients with bone metastases (51). As such, the importance of regularly evaluating bone health and the use of bone protective agents in patients with prostate cancer has been highlighted in the recommendations of a working group of European experts (51).
3.1 Treatment sequence
RWE suggests that 223Ra is generally well tolerated, irrespective of prior chemotherapy status, although prior chemotherapy may be associated with an increased likelihood of hematological events (52, 53), possibly due to patients having more advanced disease (e.g., bone marrow involvement) and/or prior chemotherapy toxicities.
For example, in the first interim analysis of the REASSURE study, prior chemotherapy status generally did not affect the overall safety profile of 223Ra, with the incidence of drug-related TEAEs being 41 and 36% with or without prior chemotherapy (53). However, drug-related hematologic TEAEs were more than twice as frequent in patients with than without prior chemotherapy (21% vs. 9%) (53). Moreover, in a prospective Japanese study, although there was no marked difference between patients with or without prior chemotherapy with regard to the incidence of drug-related TEAEs (29% vs. 25%), including hematological TEAEs (18% vs. 17%), with 223Ra, the incidence of both events was notably numerically greater in patients who had received two lines of prior chemotherapy (36 and 24%) (52).
Furthermore, the CAPRI registry found a significant (P ≤ 0.015) increase in the incidence of grade ≥ 2 anemia, grade ≥ 2 thrombocytopenia and blood transfusions with later-line use of 223Ra (line ≥ 3 vs. 2 vs. 1), although symptomatic skeletal event (SSE) incidence was not impacted (35). Factors associated with grade ≥ 2 hematological abnormalities include low hemoglobin (Hb) and low platelet count at baseline (52). Of note, 223Ra requires patient hematological evaluation before every dose and caution (2)/close monitoring (3) is advised for patients with evidence of compromised bone marrow reserve.
In an assessment of fracture risk by line of therapy, the estimated adjusted 36-month fracture risk with 223Ra vs. standard-of-care was 18% vs. 12% (HR 1.14; 95% CI, 0.50–2.15) when first line and 16% vs. 9% (HR 1.86; 95% CI: 0.62–10.93) when second line. Later treatment lines had too few fractures for analysis (43).
4 223Ra therapy/177Lu-PSMA treatment sequence and interval duration
177Lu-PSMA targets prostate cancer via a different mechanism to 223Ra. 177Lu-PSMA delivers β-particle radiation to PSMA-expressing tumor cells. In the VISION RCT, 177Lu-PSMA-617 plus standard-of-care prolonged OS vs. standard-of-care alone (15.3 vs. 11.3 months; HR for death 0.62; P < 0.001) (21). Among the 17.4% of patients who had previously received 223Ra, 177Lu-PSMA-617 efficacy was not adversely affected (54), although safety has not been reported for these patients.
Although limited by small patient numbers, real-world studies have demonstrated the clinical feasibility of giving 177Lu-PSMA after 223Ra and indicate this treatment sequence has an acceptable safety profile (55–58). In a post hoc analysis of REASSURE, median OS from start of 177Lu-PSMA was 13.2 months in patients who had previously received 223Ra (56). Moreover, in a large retrospective study, median OS was not significantly different in patients who did vs. did not receive prior 223Ra (10.8 vs. 11.3 months) (55). Furthermore, interim analyses of the RALU study, which investigated 177Lu-PSMA use in patients previously treated with 223Ra, found this approach to be clinically feasible (median OS 12.6 months; 95% CI: 8.8–16.1) and well tolerated (58).
Another consideration around treatment sequencing with radionuclide therapies is the treatment interval. Early initiation of 177Lu-PSMA within 8 weeks of 223Ra treatment (during which disease progression had occurred) was effective and did not reveal major safety concerns (57).
Thus, sequential treatment with 223Ra and 177Lu-PSMA is feasible and can be factored into considerations around optimal sequencing of the LPTs available for patients with mCRPC. However, further studies are warranted.
5 Development of response markers
Surrogate markers predicting treatment outcomes with 223Ra are needed to monitor and achieve optimal treatment duration and to identify patient subpopulations who may benefit most from 223Ra. Multiple RWE studies have investigated potential markers of survival (Supplementary Table 3), with this section focusing on multivariate analyses.
5.1 Laboratory parameters
Multivariate analyses have found various factors to be associated with survival outcomes. Baseline Hb was found to be prognostic of OS (59) and elevated baseline Hb (≥ 120 g/L) was associated with increased OS (60), whereas low baseline albumin (< 35 g/L) (61) and elevated PSA (> 80 μg/L) (61) were associated with poor OS. Similarly, other factors prognostic of OS include baseline neutrophil-to-lymphocyte ratio (28), baseline lactose dehydrogenase (62) [with elevated lactose dehydrogenase associated with shorter OS (41)] and higher baseline ALP (28) [with ALP > 150 U/L associated with poor OS (61)]. Elevated baseline ALP without a subsequent ALP decline of ≥ 10% following the first 223Ra dose was also prognostic of shorter OS (62).
5.2 Clinical parameters
A number of clinical parameters have been associated with patient survival. In terms of patient demographics, age was found to be a predictor of OS (28), with an age of > 75 years being associated with reduced OS (63). Moreover, in an analysis of US electronic heath records of mainly Caucasian patients (73.5%), other race (Asian, Hispanic, Latino, or other) was associated with improved survival (63). With regard to disease characteristics, visceral metastases (63) and prior SSEs (63) reduced OS, whereas bone-only metastases were associated with longer OS (41). Eastern Cooperative Oncology Group performance status (ECOG PS) was also prognostic of OS (59, 62), with ECOG PS 2–3 (61) and ECOG PS 2–4 (63) associated with worse OS and ECOG PS 0–1 associated with increased OS (60). Another clinical parameter prognostic of OS was number of prior systemic therapies (62). Prior chemotherapy use reduced OS (63), whereas no prior use of docetaxel increased OS (60). As discussed in section “2.1 Treatment completion,” the number of completed cycles of 223Ra (5–6 vs. 1–4) was also a predictor of OS (28).
5.3 Composite markers
Several studies have reported composite prognostic scoring methods aimed at identifying patients that may benefit most from 223Ra therapy (59–61, 64). A composite score derived from combining baseline Hb ≥ 120 g/L, total ALP ≤ 110 U/L and ECOG PS 0–1 identified patients with a low-, intermediate- or high-risk of death (composite score 2, 3–4 and 5–6, respectively; median OS 23, 8, and 5 months) (60). A similar 3-variable prognostic score combining baseline ECOG PS, Hb < 12 g/dL and PSA ≥ 20 ng/mL was predictive of OS in an initial cohort (64), with subsequent validation in a larger cohort (59). In the larger cohort, patients in the low (score 0), moderate (score 1–2), or high (score 3–4)-risk groups had a median OS of 33, 16, and 8 months, respectively (59). Likewise, a scoring system that combined albumin < 35 g/L, ALP > 150 U/L, PSA > 80 μg/L, and ECOG PS 2–3 identified three patient groups with different OS outcomes, namely good (score 0–1; median OS 19.4 months), intermediate (score 2; median OS 10.0 months) and poor (score 3–4; median OS 3.1 months) (61).
6 Imaging
An expert consensus developed at the European Association of Nuclear Medicine Focus 1 meeting concluded that, for patients with mCRPC who are candidates for 223Ra, bone scintigraphy is the recommended pre-treatment imaging method. Consensus was not reached as to which imaging method should be used for monitoring treatment response, although bone scintigraphy was favored by most (14/21) panelists (65).
Automated bone scan index (BSI) is useful for assessing skeletal metastases. Baseline BSI was associated with OS in patients who received 223Ra in two studies (66, 67), with median OS being 8.2 and 15.0 months in patients with BSIs of > 5 or ≤ 5, respectively (HR 2.65; 95% CI: 1.5–4.7; P = 0.001) (67). However, only one of the two studies found a significant association between on-treatment BSI and OS (66). A potential limitation of this approach is the potential uptake of bone scintigraphy agents into healing bone which could confound results (66).
Radionuclide cancer therapies offer considerable potential for personalized treatment as their physical properties enable in vivo imaging of their uptake and retention (68). 223Ra administration is via body weight-adjusted standard dosing regimens, although patient-specific dosimetry and treatment optimization may be possible via quantitative imaging with 223Ra (68). Although 223Ra imaging showed intra- and inter-patient variability for 223Ra dose absorption in metastases, there was a relationship between lesion-absorbed dose and treatment response (69). 18F-fluoride, like 223Ra, localizes primarily to areas of osteoblastic activity in bone and has potential as a surrogate measure of the absorbed 223Ra dose (69). 18F-fluoride uptake into bone metastases correlated significantly with that of 223Ra, as well as the absorbed 223Ra dose and resultant response (69).
Notably, PSMA-positron emission tomography (PET) has been shown to be more sensitive than bone scintigraphy in detecting bone metastases in patients with prostate cancer (70). High PSMA expression on planar/single-photon emission computed tomography (SPECT) or PET/CT scans following standard therapies for mCRPC, including 223Ra, was associated with worse OS than low PSMA expression (71).
7 Clinical practice recommendations
223Ra is recommended for mCRPC in all major treatment guidelines (6–9) and has the highest possible clinical benefit score for non-curative therapies in mCRPC in the ESMO-Magnitude of Clinical Benefit Scale (indicating a substantial magnitude of clinical benefit) (72). Expert recommendations from 11 nuclear medicine centers across six European countries provide additional insights on how to optimize 223Ra use (73). These include guidance for center organization/preparation, 223Ra ordering, preparation and disposal, 223Ra treatment delivery/administration, and patient referral/experience, and highlight the importance of starting 223Ra treatment as soon as possible in eligible patients (including those with early symptoms of bone metastases) (73).
However, for 223Ra to meet the inherent complex needs of patients, communication and coordination within multidisciplinary teams (i.e., nuclear medicine, oncology, and urology services) and centers is advised (73). Communication between the nuclear medicine physician and other specialties is important to maintain awareness for whom and when 223Ra may be appropriate, and to inform of developments in prostate cancer management (including nuclear medicine options) (73). With regard to such developments, when the Advanced Prostate Cancer Consensus Conference discussed questions relating to 223Ra and other therapies in 2021, consensus was reached that using 223Ra after 177Lu-PSMA is safe (76% consensus), based on outcomes from VISION, in which approximately 2.5% of patients received 223Ra following 177Lu-PSMA therapy (74). RWE supporting use of 223Ra followed by 177Lu-PSMA are discussed in section “4 223Ra therapy/177Lu-PSMA treatment sequence and interval duration.”
8 Discussion
For patients with mCRPC, it is important to offer as many approved LPTs as possible. Real-world studies can help healthcare professionals understand how best to utilize currently available treatment options, such as 223Ra, and are used by regulatory bodies in decision making (75–78). Although there are well recognized limitations to these studies, including confounding factors, various types of bias (pertaining to selection, patient/caregiver recall, event detection, and data misclassification) and missing data (limiting statistical power), they can complement/supplement clinical trial data and help to determine whether RCT evidence is generalizable to patient populations in clinical practice (79, 80).
The large body of RWE that has emerged for 223Ra in recent years indicates that 223Ra is an effective and safe LPT option in mCRPC, supporting RCT findings. Completing 5–6 223Ra cycles was associated with better survival outcomes across real-world studies, highlighting the value of being able to identify patients most capable of completing therapy. RWE indicates several potential markers that may help to do this, although these are not yet validated in prospective studies. A potential challenge in optimizing 223Ra use in clinical practice is how to best integrate it into the mCRPC treatment pathway. However, as current RWE has been variable in this regard, there is a need to further evaluate 223Ra in the context of other treatments with respect to timing and concurrent, layered, or sequential use, and the effectiveness and safety of such treatment approaches. To this end, several clinical trials (e.g., PEACE-III; AlphaBet; COMRADE; Rad2Nivo; RADIANT; DORA) (22–24, 81–83) and RWE studies (e.g., REASSURE; RaLu) (58, 84) continue to explore 223Ra use in mCRPC.
Author contributions
JO’S, RM, KR, KF, DG, BT, AS, PS, FV, and NS contributed to the conception and design, drafting and revising of the work, and approval of the final version. All authors agreed to be accountable for all aspects of the respective work.
Acknowledgments
Dr. C. Guise, Cancer Communications and Consultancy Ltd., Cheshire, United Kingdom, provided medical writing assistance (funded by Bayer). Dr. Lila Adnane (Bayer) provided editorial assistance.
Conflict of interest
JO’S reported consulting or advisory role for Bayer, Janssen, Astellas Pharma, Sanofi, and Novartis. Speakers’ bureau for Bayer, Janssen, and Novartis. His institution received research funding from Bayer. RM reported consulting or advisory role for AstraZeneca, Aveo, Bayer, Calithera, Caris, Dendreon, Exelixis, Janssen, Merck, Myovant, Novartis, Pfizer, Sanofi, Sorrento Therapeutics, Seagen, Tempus, and Telix. KR reported honoraria from Advanced Accelerator Applications, Bayer Healthcare, SIRTEX, Jahnsen Cielag, and Amgen. Consultancy or advisory role for ABX GmbH, ABX-CRO, Bayer Healthcare, and Advanced Accelerator Applications. KF reported participation in advisory boards and talks for Amgen, Astellas, Astrazeneca, Bayer, Clovis, Daiichi Sankyo, Janssen, MSD, Novartis/AAA, Pfizer, and Sanofi. Participation in advisory boards with personal honorarium for CureVac and Orion. Honoraria from his institution (Gustave Roussy). DG reported grants and/or fees from Acerta Pharma, the American Association for Cancer Research, Astellas, AstraZeneca, Axess Oncology, Bayer, BMS, Calithera, Capio Biosciences, EMD Serono, Exelixis, Flatiron, Ipsen, UroGPO, Janssen, Leidos Biomedical Research, Merck Sharp & Dohme, Michael J. Hennessey Associates, Millennium Med. Publishing, Modra Pharmaceuticals, Myovant Sciences, NCI, Nektar Therapeutics, Novartis, Pfizer, Physician Education Resource, Sanofi, UroToday, and Vizuri Health Sciences. BT reported Consulting or Advisory Role for Astellas Pharma, Bayer, Ferring, Janssen, Takeda, Steba Biotech, Sanofi, Myovant Sciences, and Pfizer/Astellas. Speakers’ Bureau for Amgen, Janssen, and Astellas Pharma. Travel, Accommodations, Expenses for Amgen, Astellas Pharma, Bayer, Ferring, Janssen, and Sanofi. Expert Testimony for Tookad. Honoraria for Amgen, Astellas Pharma, Bayer, Ferring, Sanofi, Janssen, Pfizer, and Myovant Sciences. His institution received research funding from Ferring. AS, PS, and FV were employees of Bayer. NS reported consulting fees from AbbVie, Amgen, Astellas, AstraZeneca, Bayer, BMS, Boston Scientific, Clarity, Clovis Oncology, Cold Genesys, Dendreon, Exact Imaging, Exact Sciences, FerGene, Foundation Medicine, Genesis Care, Invitae, Janssen, Lantheus, Lilly, MDxhealth, Merck, Myovant, Myriad, Nymox, Pacific Edge, Pfizer, Phosphorous, Photocure, Propella, PreView, Sanofi Genzyme, Sema4, Speciality Networks, Sesen Bio, Telix, Tempus, Tolmar, Urogen, and Vaxiion. Payment for expert testimony from Ferring.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1070392/full#supplementary-material
References
1. Terrisse S, Karamouza E, Parker C, Sartor A, James N, Pirrie S, et al. Overall survival in men with bone metastases from castration-resistant prostate cancer treated with bone-targeting radioisotopes: a meta-analysis of individual patient data from randomized clinical trials. JAMA Oncol. (2020) 6:206–16. doi: 10.1001/jamaoncol.2019.4097
2. EMC. Xofigo Summary of Product Characteristics. (2022). Available online at: https://www.medicines.org.uk/emc/product/5204/smpc (accessed October 04, 2022).
3. XOFIGO. Xofigo Prescribing Information. (2022). Available online at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/203971lbl.pdf (accessed October 04, 2022).
4. Bubendorf L, Schopfer A, Wagner U, Sauter G, Moch H, Willi N, et al. Metastatic patterns of prostate cancer: an autopsy study of 1,589 patients. Hum Pathol. (2000) 31:578–83. doi: 10.1053/hp.2000.6698
5. Parker C, Nilsson S, Heinrich D, Helle S, O’Sullivan J, Fossa S, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med. (2013) 369:213–23. doi: 10.1056/NEJMoa1213755
6. Basch E, Loblaw D, Oliver T, Carducci M, Chen R, Frame J, et al. Systemic therapy in men with metastatic castration-resistant prostate cancer: American society of clinical oncology and cancer care ontario clinical practice guideline. J Clin Oncol. (2014) 32:3436–48. doi: 10.1200/JCO.2013.54.8404
7. National Comprehensive Cancer Network [NCCN]. NCCN Clinical Practice Guidelines in Oncology: Prostate Cancer Version 2. Plymouth Meeting, PA: National Comprehensive Cancer Network (2017).
8. Mottet N, Bellmunt J, Bolla M, Cornford P, De Santis M, Henry A, et al. Guidelines on Prostate Cancer. (2016). Available online at: http://uroweb.org/guideline/prostate-cancer (accessed October 4, 2022).
9. Parker C, Castro E, Fizazi K, Heidenreich A, Ost P, Procopio G, et al. Prostate cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2020) 31:1119–34. doi: 10.1016/j.annonc.2020.06.011
10. Caffo O, Wissing M, Bianchini D, Bergman A, Thomsen F, Schmid S, et al. Survival outcomes from a cumulative analysis of worldwide observational studies on sequential use of new agents in metastatic castration-resistant prostate cancer. Clin Genitourin Cancer. (2020) 18:69–76e4. doi: 10.1016/j.clgc.2019.09.010
11. Shore N, Laliberte F, Ionescu-Ittu R, Yang L, Mahendran M, Lejeune D, et al. Real-world treatment patterns and overall survival of patients with metastatic castration-resistant prostate cancer in the US prior to PARP inhibitors. Adv Ther. (2021) 38:4520–40. doi: 10.1007/s12325-021-01823-6
12. de Bono J, Logothetis C, Molina A, Fizazi K, North S, Chu L, et al. Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med. (2011) 364:1995–2005. doi: 10.1056/NEJMoa1014618
13. Ryan C, Molina A, Griffin T. Abiraterone in metastatic prostate cancer. N Engl J Med. (2013) 368:1458–9. doi: 10.1056/NEJMc1301594
14. Scher H, Fizazi K, Saad F, Taplin M, Sternberg C, Miller K, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. (2012) 367:1187–97. doi: 10.1056/NEJMoa1207506
15. Beer T, Tombal B. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. (2014) 371:1755–6. doi: 10.1056/NEJMc1410239
16. Chi K, Agarwal N, Bjartell A, Chung B, Pereira de Santana Gomes A, Given R, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. (2019) 381:13–24. doi: 10.1056/NEJMoa1903307
17. Smith M, Hussain M, Saad F, Fizazi K, Sternberg C, Crawford E, et al. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N Engl J Med. (2022) 386:1132–42. doi: 10.1056/NEJMoa2119115
18. de Bono J, Mateo J, Fizazi K, Saad F, Shore N, Sandhu S, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med. (2020) 382:2091–102. doi: 10.1056/NEJMoa1911440
19. Hussain M, Mateo J, Fizazi K, Saad F, Shore N, Sandhu S, et al. Survival with olaparib in metastatic castration-resistant prostate cancer. N Engl J Med. (2020) 383:2345–57. doi: 10.1056/NEJMoa2022485
20. Kantoff P, Higano C, Shore N, Berger E, Small E, Penson D, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. (2010) 363:411–22. doi: 10.1056/NEJMoa1001294
21. Sartor O, de Bono J, Chi K, Fizazi K, Herrmann K, Rahbar K, et al. Lutetium-177-PSMA-617 for metastatic castration-resistant prostate cancer. N Engl J Med. (2021) 385:1091–103. doi: 10.1056/NEJMoa2107322
22. Fizazi K, Alba A, Mustafa Ö, Skoneczna I, Krissel H, Uema D, et al. Radium- 223 (Ra-223) versus novel antihormone therapy (NAH) for progressive metastatic castration-resistant prostate cancer (mCRPC) after 1 line of NAH: RADIANT, an international phase 4, randomized, open-label study. J Clin Oncol. (2021) 39, (Suppl. 15). doi: 10.1200/JCO.2021.39.15_suppl.TPS5093
23. ClinicalTrials.gov. Phase I Radium 223 mCRPC-PEACE III (PEACE III). ClinicalTrials.gov Identifier NCT02194842. (2014). Available online at: https://clinicaltrials.gov/ct2/show/NCT02194842 (accessed October 09, 2022).
24. ClinicalTrials.gov. A Study to Test Radium-223 with Docetaxel in Patients with Prostate Cancer. Clinicaltrials.gov Identifier NCT03574571. (2018). Available online at: https://clinicaltrials.gov/ct2/show/NCT03574571 (accessed October 12, 2022).
25. Sherman R, Anderson S, Dal Pan G, Gray G, Gross T, Hunter N, et al. Real-world evidence - what is it and what can it tell us? N Engl J Med. (2016) 375:2293–7. doi: 10.1056/NEJMsb1609216
26. Justo N, Schweikert B, Simon A, Reginald Waldeck A, Meinhardt M, Samel Y-R, et al. Insights into treatment patterns in the routine care of patients diagnosed with metastatic castration-resistant prostate cancer in Germany after the introduction of new therapies. Clin Oncol Res. (2020) 3:2–8. doi: 10.31487/j.COR.2020.09.04
27. George D, Sartor O, Miller K, Saad F, Tombal B, Kalinovsky J, et al. Treatment patterns and outcomes in patients with metastatic castration-resistant prostate cancer in a real-world clinical practice setting in the United States. Clin Genitourin Cancer. (2020) 18:284–94. doi: 10.1016/j.clgc.2019.12.019
28. Parikh S, Murray L, Kenning L, Bottomley D, Din O, Dixit S, et al. Real-world outcomes and factors predicting survival and completion of radium 223 in metastatic castrate-resistant prostate cancer. Clin Oncol. (2018) 30:548–55. doi: 10.1016/j.clon.2018.06.004
29. Sartor O, Appukkuttan S, Weiss J, Tsao C. Clinical outcomes, management, and treatment patterns in patients with metastatic castration-resistant prostate cancer treated with radium-223 in community compared to academic settings. Prostate. (2021) 81:657–66. doi: 10.1002/pros.24143
30. Cheng S, Arciero V, Goldberg H, Tajzler C, Manganaro A, Kozlowski N, et al. Population-based analysis of the use of radium-223 for bone-metastatic castration-resistant prostate cancer in Ontario, and of factors associated with treatment completion and outcome. Cancer Manag Res. (2019) 11:9307–19. doi: 10.2147/CMAR.S213051
31. Buscombe J, Gillett D, Bird N, Powell A, Heard S, Aloj L. Quantifying the survival benefit of completing all the six cycles of radium-223 therapy in patients with castrate-resistant prostate cancer with predominant bone metastases. World J Nucl Med. (2021) 20:139–44. doi: 10.4103/wjnm.WJNM_74_20
32. McKay R, Silver R, Bhak R, Korves C, Cheng M, Appukkuttan S, et al. Treatment of metastatic castration resistant prostate cancer with radium-223: a retrospective study at a US tertiary oncology center. Prostate Cancer Prostatic Dis. (2021) 24:210–9. doi: 10.1038/s41391-020-00271-7
33. Miyoshi Y, Tsutsumi S, Yasui M, Kawahara T, Uemura K, Hayashi N, et al. A novel prediction model for the completion of six cycles of radium-223 treatment and survival in patients with metastatic castration-resistant prostate cancer. World J Urol. (2021) 39:3323–8. doi: 10.1007/s00345-021-03639-z
34. Dadhania S, Alonzi R, Douglas S, Gogbashian A, Hughes R, Dalili D, et al. Single-centre experience of use of radium 223 with clinical outcomes based on number of cycles and bone marrow toxicity. Anticancer Res. (2018) 38:5423–7. doi: 10.21873/anticanres.12873
35. Kuppen M, Westgeest H, van der Doelen M, van den Eertwegh A, Coenen J, Aben K, et al. Real-world outcomes of radium-223 dichloride for metastatic castration resistant prostate cancer. Future Oncol. (2020) 16:1371–84. doi: 10.2217/fon-2020-0039
36. McKay R, Jacobus S, Fiorillo M, Ledet E, Cotogna P, Steinberger A, et al. Radium-223 use in clinical practice and variables associated with completion of therapy. Clin Genitourin Cancer. (2017) 15:e289–98. doi: 10.1016/j.clgc.2016.08.015
37. Jarvis P, Ho A, Sundram F. Radium-223 therapy for metastatic castration-resistant prostate cancer: survival benefit when used earlier in the treatment pathway. Nucl Med Commun. (2021) 42:332–6. doi: 10.1097/MNM.0000000000001325
38. Maruzzo M, Basso U, Borsatti E, Evangelista L, Alongi F, Caffo O, et al. Results from a large, multicenter, retrospective analysis on radium223 use in metastatic castration-resistant prostate cancer (mCRPC) in the Triveneto Italian Region. Clin Genitourin Cancer. (2019) 17:e187–94. doi: 10.1016/j.clgc.2018.10.013
39. Caffo O, Frantellizzi V, Tucci M, Galli L, Monari F, Baldari S, et al. Fracture risk and survival outcomes in metastatic castration-resistant prostate cancer patients sequentially treated with abiraterone acetate and radium-223. Eur J Nucl Med Mol Imaging. (2020) 47:2633–8. doi: 10.1007/s00259-020-04796-w
40. Jiang X, Atkinson S, Pearson R, Leaning D, Cumming S, Burns A, et al. Optimising radium 223 therapy for metastatic castration-resistant prostate cancer - 5-year real-world outcome: focusing on treatment sequence and quality of life. Clin Oncol. (2020) 32:e177–87. doi: 10.1016/j.clon.2020.05.002
41. Badrising S, Louhanepessy R, van der Noort V, Coenen J, Hamberg P, Beeker A, et al. A prospective observational registry evaluating clinical outcomes of radium-223 treatment in a nonstudy population. Int J Cancer. (2020) 147:1143–51. doi: 10.1002/ijc.32851
42. Parker C, Coleman R, Sartor O, Vogelzang N, Bottomley D, Heinrich D, et al. Three-year safety of radium-223 dichloride in patients with castration-resistant prostate cancer and symptomatic bone metastases from phase 3 randomized alpharadin in symptomatic prostate cancer trial. Eur Urol. (2018) 73:427–35. doi: 10.1016/j.eururo.2017.06.021
43. Stattin P, Westerberg M, Lissbrant I, Eriksson M, Kjellman A, Ullen A, et al. Real world outcomes in patients with metastatic, castration-resistant prostate cancer treated with radium-223 in routine clinical practice in Sweden. Clin Genitourin Cancer. (2022): doi: 10.1016/j.clgc.2022.09.002 [Epub ahead of print].
44. Zhao H, Howard L, De Hoedt A, Terris M, Amling C, Kane C, et al. Safety of concomitant therapy with radium-223 and abiraterone or enzalutamide in a real-world population. Prostate. (2021) 81:390–7. doi: 10.1002/pros.24115
45. Kim S, Szeto A, Morgan K, Brower B, Dunn M, Khandani A, et al. A real-world evaluation of radium-223 in combination with abiraterone or enzalutamide for the treatment of metastatic castration-resistant prostate cancer. PLoS One. (2021) 16:e0253021. doi: 10.1371/journal.pone.0253021
46. Ahmed M, Joshi V, Badawy M, Pagliaro L, Karnes R, Lowe V, et al. Radium-223 in the third-line setting in metastatic castration-resistant prostate cancer: impact of concomitant use of enzalutamide on overall survival (OS) and predictors of improved OS. Clin Genitourin Cancer. (2021) 19:223–9. doi: 10.1016/j.clgc.2020.12.009
47. Trieu J, Chang M, Rojas V, Varada N, Cao Y, Anderson M, et al. Lower fracture rates in patients treated with radium-223, abiraterone or enzalutamide, when given concurrently with bone health agents: a real-world analysis. Clin Genitourin Cancer. (2022) 20:399–403. doi: 10.1016/j.clgc.2022.04.015
48. Shore N, Higano C, George D, Sternberg C, Saad F, Tombal B, et al. Concurrent or layered treatment with radium-223 and enzalutamide or abiraterone/prednisone: real-world clinical outcomes in patients with metastatic castration-resistant prostate cancer. Prostate Cancer Prostatic Dis. (2020) 23:680–8. doi: 10.1038/s41391-020-0236-0
49. Smith M, Parker C, Saad F, Miller K, Tombal B, Ng Q, et al. Addition of radium-223 to abiraterone acetate and prednisone or prednisolone in patients with castration-resistant prostate cancer and bone metastases (ERA 223): a randomised, double-blind, placebo-controlled, Phase 3 trial. Lancet Oncol. (2019) 20:408–19. doi: 10.1016/S1470-2045(18)30860-X
50. Gillessen S, Choudhury A, Rodriguez-Vida A, Nole F, Diaz E, Roumeguere T, et al. Decreased fracture rate by mandating bone protecting agents in the EORTC 1333/PEACEIII trial combining Ra223 with enzalutamide versus enzalutamide alone: an updated safety analysis. J Clin Oncol. (2021) 39, (Suppl. 15):5002. doi: 10.1200/JCO.2021.39.15_suppl.5002
51. O’Sullivan J, Carles J, Cathomas R, Gomez-Iturriaga A, Heinrich D, Kramer G, et al. Radium-223 within the evolving treatment options for metastatic castration-resistant prostate cancer: recommendations from a European Expert Working Group. Eur Urol Oncol. (2020) 3:455–63. doi: 10.1016/j.euo.2019.02.007
52. Uemura H, Masumori N, Takahashi S, Hosono M, Kinuya S, Sunaya T, et al. Real-world safety and effectiveness of radium-223 in Japanese patients with castration-resistant prostate cancer (CRPC) and bone metastasis: exploratory analysis, based on the results of post-marketing surveillance, according to prior chemotherapy status and in patients without concomitant use of second-generation androgen-receptor axis-targeted agents. Int J Clin Oncol. (2021) 26:753–63. doi: 10.1007/s10147-020-01850-3
53. Dizdarevic S, Petersen P, Essler M, Versari A, Bourre J, la Fougere C, et al. Interim analysis of the REASSURE (Radium-223 alpha emitter agent in non-intervention safety study in mCRPC population for long-term evaluation) study: patient characteristics and safety according to prior use of chemotherapy in routine clinical practice. Eur J Nucl Med Mol Imaging. (2019) 46:1102–10. doi: 10.1007/s00259-019-4261-y
54. Vaishampayan N, Morris M, Krause B, Vogelzang N, Kendi A, Nordquist L, et al. [177Lu]Lu-PSMA-617 in PSMA-positive metastatic castration-resistant prostate cancer: prior and concomitant treatment subgroup analyses of the VISION trial. J Clin Oncol. (2022) 40(16_Suppl.):5001.
55. Ahmadzadehfar H, Zimbelmann S, Yordanova A, Fimmers R, Kurpig S, Eppard E, et al. Radioligand therapy of metastatic prostate cancer using 177Lu-PSMA-617 after radiation exposure to 223Ra-dichloride. Oncotarget. (2017) 8:55567–74. doi: 10.18632/oncotarget.15698
56. Sartor O, la Fougère C, Essler M, Ezziddin S, Kramer G, Ellinger J, et al. Lutetium-177–prostate-specific membrane antigen ligand following radium-223 treatment in men with bone-metastatic castration-resistant prostate cancer: real-world clinical experience. J Nucl Med. (2021) 63:410–4. doi: 10.2967/jnumed.121.262240
57. Baumgarten J, Groener D, Nguyen Ngoc C, Mader N, Chaurasia M, Davis K, et al. Safety and efficacy of 177Lutetium-PSMA-617 radioligand therapy shortly after failing 223radium-dichloride. Cancers. (2022) 14:557. doi: 10.3390/cancers14030557
58. Rahbar K, Essler M, Eiber M, la Fougère C, Prasad V, Fendler W, et al. Safety and survival outcomes in patients (Pts) with metastatic castration-resistant prostate cancer (mCRPC) treated with lutetium-177–prostate-specific membrane antigen (177Lu-PSMA) after radium-223 (223Ra): interim analysis of the RALU study. J Clin Oncol. (2022) 40:5040.
59. Frantellizzi V, Monari F, Mascia M, Costa R, Rubini G, Spanu A, et al. Validation of the 3-variable prognostic score (3-PS) in mCRPC patients treated with 223radium-dichloride: a national multicenter study. Ann Nucl Med. (2020) 34:772–80. doi: 10.1007/s12149-020-01501-7
60. Charrois-Durand C, Saad F, Barkati M, Lattouf J, Perrotte P, Karakiewicz P, et al. A single-center, multidisciplinary experience with radium-223 dichloride in men with metastatic castrate-resistant prostate cancer. Can Urol Assoc J. (2022) 16:199–205. doi: 10.5489/cuaj.7591
61. Al-Ezzi E, Alqaisi H, Iafolla M, Wang L, Sridhar S, Sacher A, et al. Clinicopathologic factors that influence prognosis and survival outcomes in men with metastatic castration-resistant prostate cancer treated with radium-223. Cancer Med. (2021) 10:5775–82. doi: 10.1002/cam4.4125
62. van der Doelen M, Stockhaus A, Ma Y, Mehra N, Yachnin J, Gerritsen W, et al. Early alkaline phosphatase dynamics as biomarker of survival in metastatic castration-resistant prostate cancer patients treated with radium-223. Eur J Nucl Med Mol Imaging. (2021) 48:3325–34. doi: 10.1007/s00259-021-05283-6
63. George D, Agarwal N, Sartor O, Sternberg C, Tombal B, Saad F, et al. Real-world patient characteristics associated with survival of 2 years or more after radium-223 treatment for metastatic castration-resistant prostate cancer (Epix Study). Prostate Cancer Prostatic Dis. (2022) 25:306–13.
64. Frantellizzi V, Farcomeni A, Follacchio G, Pacilio M, Pellegrini R, Pani R, et al. A 3-variable prognostic score (3-PS) for overall survival prediction in metastatic castration-resistant prostate cancer treated with 223radium-dichloride. Ann Nucl Med. (2018) 32:142–8. doi: 10.1007/s12149-017-1228-6
65. Fanti S, Minozzi S, Antoch G, Banks I, Briganti A, Carrio I, et al. Consensus on molecular imaging and theranostics in prostate cancer. Lancet Oncol. (2018) 19:e696–708. doi: 10.1016/S1470-2045(18)30604-1
66. Anand A, Tragardh E, Edenbrandt L, Beckman L, Svensson J, Thellenberg C, et al. Assessing radiographic response to 223Ra with an automated bone scan index in metastatic castration-resistant prostate cancer patients. J Nucl Med. (2020) 61:671–5. doi: 10.2967/jnumed.119.231100
67. Fosbol M, Petersen P, Kjaer A, Mortensen J. 223Ra therapy of advanced metastatic castration-resistant prostate cancer: quantitative assessment of skeletal tumor burden for prognostication of clinical outcome and hematologic toxicity. J Nucl Med. (2018) 59:596–602. doi: 10.2967/jnumed.117.195677
68. Flux G. Imaging and dosimetry for radium-223: the potential for personalized treatment. Br J Radiol. (2017) 90:20160748. doi: 10.1259/bjr.20160748
69. Murray I, Chittenden S, Denis-Bacelar A, Hindorf C, Parker C, Chua S, et al. The potential of 223Ra and 18F-fluoride imaging to predict bone lesion response to treatment with 223Ra-dichloride in castration-resistant prostate cancer. Eur J Nucl Med Mol Imaging. (2017) 44:1832–44. doi: 10.1007/s00259-017-3744-y
70. Dondi F, Albano D, Bertagna F, Treglia G. Bone scintigraphy versus PSMA-targeted PET/CT or PET/MRI in prostate cancer: lessons learned from recent systematic reviews and meta-analyses. Cancers. (2022) 14:4470.
71. Vlachostergios P, Niaz M, Sun M, Mosallaie S, Thomas C, Christos P, et al. Prostate-specific membrane antigen uptake and survival in metastatic castration-resistant prostate cancer. Front Oncol. (2021) 11:630589.
72. Cherny N, Dafni U, Bogaerts J, Latino N, Pentheroudakis G, Douillard J, et al. ESMO-magnitude of clinical benefit scale version 1.1. Ann Oncol. (2017) 28:2340–66. doi: 10.1093/annonc/mdx310
73. Du Y, Carrio I, De Vincentis G, Fanti S, Ilhan H, Mommsen C, et al. Practical recommendations for radium-223 treatment of metastatic castration-resistant prostate cancer. Eur J Nucl Med Mol Imaging. (2017) 44:1671–8. doi: 10.1007/s00259-017-3756-7
74. Gillessen S, Armstrong A, Attard G, Beer T, Beltran H, Bjartell A, et al. Management of patients with advanced prostate cancer: report from the advanced prostate cancer consensus conference 2021. Eur Urol. (2022) 82:115–41. doi: 10.1016/j.eururo.2022.04.002
75. Arlett P, Kjaer J, Broich K, Cooke E. Real-world evidence in EU medicines regulation: enabling use and establishing value. Clin Pharmacol Ther. (2022) 111:21–3. doi: 10.1002/cpt.2479
76. Flynn R, Plueschke K, Quinten C, Strassmann V, Duijnhoven R, Gordillo-Maranon M, et al. Marketing authorization applications made to the European Medicines Agency in 2018-2019: what was the contribution of real-world evidence? Clin Pharmacol Ther. (2022) 111:90–7. doi: 10.1002/cpt.2461
77. European Medicines Agency. A Vision for Use of Real-World Evidence in EU Medicines Regulation. (2022). Available online at: https://www.ema.europa.eu/en/news/vision-use-real-world-evidence-eu-medicines-regulation (accessed November 22, 2022).
78. US Food and Drug Administration. Real-World Evidence. (2022). Available online at: https://www.fda.gov/science-research/science-and-research-special-topics/real-world-evidence (accessed November 22, 2022).
79. Azoulay L. Rationale, strengths, and limitations of real-world evidence in oncology: a Canadian review and perspective. Oncologist. (2022) 27:e731–8. doi: 10.1093/oncolo/oyac114
80. Blonde L, Khunti K, Harris S, Meizinger C, Skolnik N. Interpretation and impact of real-world clinical data for the practicing clinician. Adv Ther. (2018) 35:1763–74. doi: 10.1007/s12325-018-0805-y
81. ClinicalTrials.gov. Combination of Radium-223 and Lutetium-177 PSMA-I&T in Men with Metastatic Castration-Resistant Prostate Cancer (AlphaBet). ClinicalTrials.gov Identifier: NCT05383079. (2022). Available online at: https://clinicaltrials.gov/ct2/show/NCT05383079 (accessed October 09, 2022).
82. ClinicalTrials.gov. Testing the Safety of Different Doses of Olaparib given Radium-223 for Men with Advanced Prostate Cancer with Bone Metastasis. ClinicalTrials.gov Identifier: NCT03317392. (2019). Available online at: https://clinicaltrials.gov/ct2/show/NCT03317392 (accessed October 09, 2022).
83. ClinicalTrials.gov. Study of Nivolumab in Combination with Radium-223 in Men with Metastatic Castration Resistant Prostate Cancer (Rad2Nivo). ClinicalTrials.gov Identifier: NCT04109729. (2019). Available online at: https://clinicaltrials.gov/ct2/show/NCT04109729 (accessed October 09, 2022).
84. ClinicalTrials.gov. Observational Study for the Evaluation of Long-Term Safety of Radium-223 used for the Treatment of Metastatic Castration Resistant Prostate Cancer (REASSURE). ClinicalTrials.gov Identifier: NCT02141438. (2014). Available online at: https://clinicaltrials.gov/ct2/show/NCT02141438 (accessed October 09, 2022).
Keywords: targeted alpha therapy, radium-223, Lutetium-177-PSMA, metastatic castration-resistant prostate cancer, real-world practice
Citation: O’Sullivan JM, McKay RR, Rahbar K, Fizazi K, George DJ, Tombal B, Schmall A, Sandström P, Verholen F and Shore N (2022) Real-world effectiveness, long-term safety and treatment pathway integration of radium-223 therapy in patients with metastatic castration-resistant prostate cancer. Front. Med. 9:fmed-09-1070392. doi: 10.3389/fmed.2022.1070392
Received: 14 October 2022; Accepted: 07 December 2022;
Published: 22 December 2022.
Edited by:
Øyvind Bruland, Oslo University Hospital, NorwayReviewed by:
Rob Coleman, The University of Sheffield, United KingdomOliver Sartor, Tulane University, United States
Copyright © 2022 O’Sullivan, McKay, Rahbar, Fizazi, George, Tombal, Schmall, Sandström, Verholen and Shore. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joe M. O’Sullivan, ✉ am9lLm9zdWxsaXZhbkBxdWIuYWMudWs=