 Ozlem Sandal1
Ozlem Sandal1 Gokhan Ceylan1,2*
Gokhan Ceylan1,2* Sevgi Topal3Pinar Hepduman1Mustafa Colak4Dominik Novotni2
Sevgi Topal3Pinar Hepduman1Mustafa Colak4Dominik Novotni2 Ekin Soydan1Utku Karaarslan1Gulhan Atakul1
Ekin Soydan1Utku Karaarslan1Gulhan Atakul1 Marcus J. Schultz2,5,6,7
Marcus J. Schultz2,5,6,7 Hasan Ağın1
Hasan Ağın1- 1Department of Pediatric Intensive Care Unit, Dr. Behcet Uz Children’s Disease and Surgery Training and Research Hospital, Health Sciences University, İzmir, Turkey
- 2Department of Medical Research, Hamilton Medical AG, Bonaduz, Switzerland
- 3Department of Pediatric Intensive Care Unit, Erzurum Territorial Training and Research Hospital, Health Sciences University, Erzurum, Turkey
- 4Department of Pediatric Intensive Care Unit, Cam Sakura Training and Research Hospital, Health Sciences University, Istanbul, Turkey
- 5Department of Intensive Care, Amsterdam UMC, Academic Medical Center, Amsterdam, Netherlands
- 6Tropical Medicine Research Unit, Mahidol University, Bangkok, Thailand
- 7Nuffield Department of Medicine, University of Oxford, Oxford, United Kingdom
Background: We assessed the effect of a closed–loop oxygen control system in pediatric patients receiving high–flow nasal oxygen therapy (HFNO).
Methods: A multicentre, single–blinded, randomized, and cross–over study. Patients aged between 1 month and 18 years of age receiving HFNO for acute hypoxemic respiratory failure (AHRF) were randomly assigned to start with a 2–h period of closed–loop oxygen control or a 2–h period of manual oxygen titrations, after which the patient switched to the alternative therapy. The endpoints were the percentage of time spent in predefined SpO2 ranges (primary), FiO2, SpO2/FiO2, and the number of manual adjustments.
Findings: We included 23 patients, aged a median of 18 (3–26) months. Patients spent more time in a predefined optimal SpO2 range when the closed–loop oxygen controller was activated compared to manual oxygen titrations [91⋅3% (IQR 78⋅4–95⋅1%) vs. 63⋅0% (IQR 44⋅4–70⋅7%)], mean difference [28⋅2% (95%–CI 20⋅6–37⋅8%); P < 0.001]. Median FiO2 was lower [33⋅3% (IQR 26⋅6–44⋅6%) vs. 42⋅6% (IQR 33⋅6–49⋅9%); P = 0.07], but median SpO2/FiO2 was higher [289 (IQR 207–348) vs. 194 (IQR 98–317); P = 0.023] with closed–loop oxygen control. The median number of manual adjustments was lower with closed–loop oxygen control [0⋅0 (IQR 0⋅0–0⋅0) vs. 0⋅5 (IQR 0⋅0–1⋅0); P < 0.001].
Conclusion: Closed-loop oxygen control improves oxygenation therapy in pediatric patients receiving HFNO for AHRF and potentially leads to more efficient oxygen use. It reduces the number of manual adjustments, which may translate into decreased workloads of healthcare providers.
Clinical trial registration: [www.ClinicalTrials.gov], identifier [NCT 05032365].
Introduction
Application of high–flow nasal oxygen (HFNO) has become a first–line therapy for acute hypoxemic respiratory failure (AHRF) in intensive care units (ICUs), emergency departments, and now also in pediatric patients (1–3). A recent worldwide survey demonstrated a large variability in HFNO settings, including the fraction of inspired oxygen (FiO2) (3).
Pediatric intensivists tend to avoid both hypoxemia and hyperoxemia (4–7) as previous studies suggest a relation between excessive or inadequate use of oxygen and mortality in pediatric ICU patients receiving oxygen therapy (8–12). While ideally partial pressure of arterial oxygen (PaO2) and arterial oxygen saturation (SaO2) are used to titrate oxygen, these values are often difficult to monitor in pediatric patients. Pulse oximetry (SpO2) may serve as an attractive alternative as it offers the advantage of continuous monitoring. A search in MEDLINE, Embase, CINAHL, and Web of Science on May 16, 2022, with the terms (“closed-loop” OR “automatic”) AND (“oxygen” OR “oxygen therapy”) with no date or language restrictions, identified 33 clinical investigations of which 27 were randomized clinical studies. All studies concluded that SpO2 can be used by closed-loop oxygen systems to automatically adjust the FiO2. None of these studies, however, assessed the effects of closed-loop oxygen control during HFNO in pediatric patients (13–44).
Studies testing the efficiency and safety of closed-loop oxygen systems in pediatric patients receiving HFNO for AHRF are currently lacking. Therefore, we performed a randomized crossover study to evaluate the efficiency of a closed-loop oxygen control system integrated into a HFNO device with respect to the quality of oxygen therapy in pediatric patients. We also tested its safety, determined total oxygen use, and compared the number of manual adjustments between closed-loop oxygen control and manual oxygen titration. We hypothesized this closed-loop oxygen system to increase time spent within predefined optimal SpO2 ranges.
Materials and methods
Study design
This is a multicentre, single-blinded, randomized, crossover study of closed-loop oxygen control vs. manual oxygen titrations in pediatric patients in three hospitals in Turkey. Patients were screened for participation in the pediatric ICUs in the Dr. Behcet Uz Children’s Research and Training Hospital in Izmir, the Erzurum Territorial Training and Research Hospital in Erzurum, and the Cam Sakura Research and Training Hospital in Istanbul, from September 2021 to January 2022. The study was approved by the Institutional Review Boards (604/2021/13-01) and conducted in accordance with the Declaration of Helsinki. The study is registered at ClinicalTrials.gov (study identifier NCT 05032365).
Participants
Patients were eligible if: (1) aged between 1 month and 18 years of age and (2) receiving HFNO with FiO2 ≥ 25% to maintain SpO2 within the preferred target ranges. Patients were only included if considered to be in a clinical stable condition, i.e., not expected to need a change in respiratory support, like non-invasive or invasive ventilation in the next 5 h. We excluded patients with congenital or acquired hemoglobinopathies affecting SpO2, patients with cyanotic heart disease, and patients who needed continuous infusion of epinephrine or norepinephrine at rates higher than 0.2 μg/kg per minute. We also excluded patients for which no written informed consent could be obtained, patients that were previously included in this study, and patients that were enrolled in another interventional study.
Randomization and masking
Patients were randomized to start with a 2–h period of closed-loop oxygen control or a 2–h period of manual oxygen titration. Thereafter, patients were switched to the alternate therapy. Randomization was 1:1, with blocks of four, using sealed opaque envelopes. Due to the intervention, healthcare staff could not be blinded. Patients remained blinded for the way oxygen was titrated.
Procedures
Patients were equipped with an appropriately sized and placed nasal cannula and kept in a semi-recumbent position for the duration of the study. A pediatric ventilator equipped with a humidifier device (Hamilton–C1 with H–900 humidifier, Hamilton Medical AG, Bonaduz, Switzerland) was used for HFNO. Patients were sedated as needed, at a sedation level sufficient for each patient. The sedation level was not altered for the duration of the study. Patient care and standard activities, such as suctioning of secretions or feeding, were uninterruptedly performed as usual and at random in either period. At the study sites, during daytime and night-time shifts, the nurse and doctor to patient ratios were approximately 6:1 and 12:1, and 2:1 and 3:1, respectively. This setting not changed during the conduct of the study, i.e., these ratios were not different during the two crossover phases. Also, there was no study personnel present during these two phases.
After randomization, the attending physician decided on the optimal SpO2 range, individualized for each patient according to the current clinical situation and medical history. After the first 2–h period, a washout period was established for 30 min, after which the patient was switched to the second 2–h period with the alternate oxygen titration strategy (Supplementary Figure 1). With closed-loop oxygen control, patients’ SpO2 was kept in a predefined target range via automatic adjustment of the FiO2. In the manual oxygen titration phase of the study, manual adjustments to FiO2 were performed by the bedside doctors or nurses, using the same SpO2 target range. The flow of the HFNC was not altered during the two crossover phases of the trial. The SpO2 target range was defined by setting four cutoffs: an upper and a lower “optimal” cutoff, and an upper and lower “suboptimal” cutoff. The optimal cutoffs were from 94 to 98% or from 92 to 96%. The corresponding suboptimal cutoffs were from 90 to 94% and from 98 to 99%, and from 88 to 92% and 96 to 98% (Supplementary Table 1). The running principles of the closed-loop system are detailed in Supplementary Table 2.
Data collection
Ventilation parameters were captured in a case report form (CRF). HFNO data, including FiO2, airflows, and manual titrations were captured every second using a Memory Box (Hamilton Medical AG) connected to the RS–232 interface port on the ventilator.
Definitions
Every recorded value of SpO2 was classified as either optimal if within the individualized predefined range, suboptimal high or low when outside the optimal SpO2 range, but inside the suboptimal cut-offs, or unacceptable when beyond the suboptimal cut-offs (as shown in Supplementary Table 1).
Outcomes
The primary objective of the study was to assess the efficiency of the closed-loop oxygen control system. Therefore, the primary endpoint was the percentage of time spent in predefined target ranges for SpO2 in each 2–h period. Secondary endpoints were the percentage of time spent in suboptimal and unacceptable SpO2 ranges, the FiO2 and PaO2/FiO2 ratio, the number of manual oxygen adjustments, and the number of alarms.
Power calculation
The sample size was calculated by means of a pilot study of seven patients (7 × 240 = 1,680 min) in which we determined the difference in the percentage of time spent in optimal target ranges for SpO2 between closed-loop and manual oxygen titrations. Based on the pilot data, G*Power computed that the study should have an additional 21 patients to detect an effect size of Cohen’s d = 0.86 with 95% power (two-tailed α of 0.05) in a Wilcoxon signed-rank test (45). To account for potential dropouts, defined as a patient who required either non-invasive ventilation or intubation for invasive ventilation during the two phases of the study, consent withdrawal by patient or family, poor quality of SpO2 readings for > 1 h during one of the study phases, or technical problem in recording, we decided to have a sample size of 23 patients.
Statistical analysis
Shapiro–Wilk, skewness, and kurtosis normality tests were used to check the distribution of data. Continuous data were expressed in terms of either mean and standard deviation (SD) or median and interquartile range [IQR], according to the distribution.
Data were analyzed using either a paired samples t-test or Wilcoxon test, depending on which was most appropriate. The Wilcoxon signed-rank test was used for the comparison between the percentage of time spent in the target range of SpO2 with manual FiO2 adjustments and the percentage with closed-loop FiO2 control.
A P-value of less than 0⋅05 was considered statistically significant for all comparisons. Data were calculated with MATLAB (version 2021b) (The MathWorks, Inc., Natick, MA, United States) and statistical testing was carried out with the XLSTAT (version 2016) (Addinsoft, Paris, France). Figures were constructed using JASP (version 2022) (JASP Team, Amsterdam, The Netherlands) and GraphPad PRISM (version 9) (San Diego, CA, USA).
Results
From August 2021 to November 2021, 131 patients were screened; of 80 eligible patients, 57 met one or more exclusion criteria, and 23 patients were included (Figure 1). Baseline characteristics are presented in Table 1. The majority of patients was aged 2 years of age or younger, and in approximately half of the patients, AHRF was due to a respiratory infection. Two-third of patients received HFNO after having received invasive ventilation.
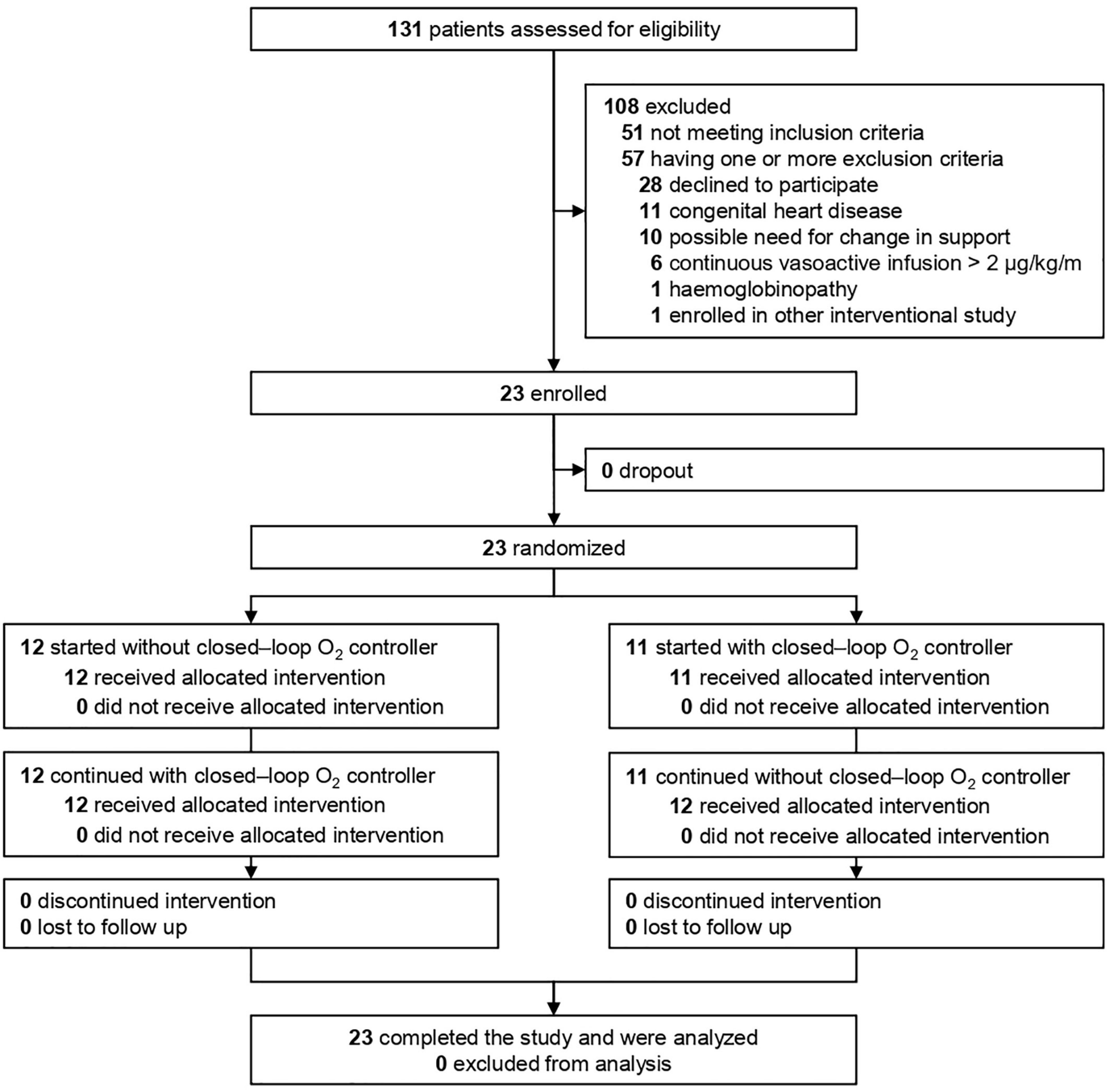
Figure 1. Trial profile.
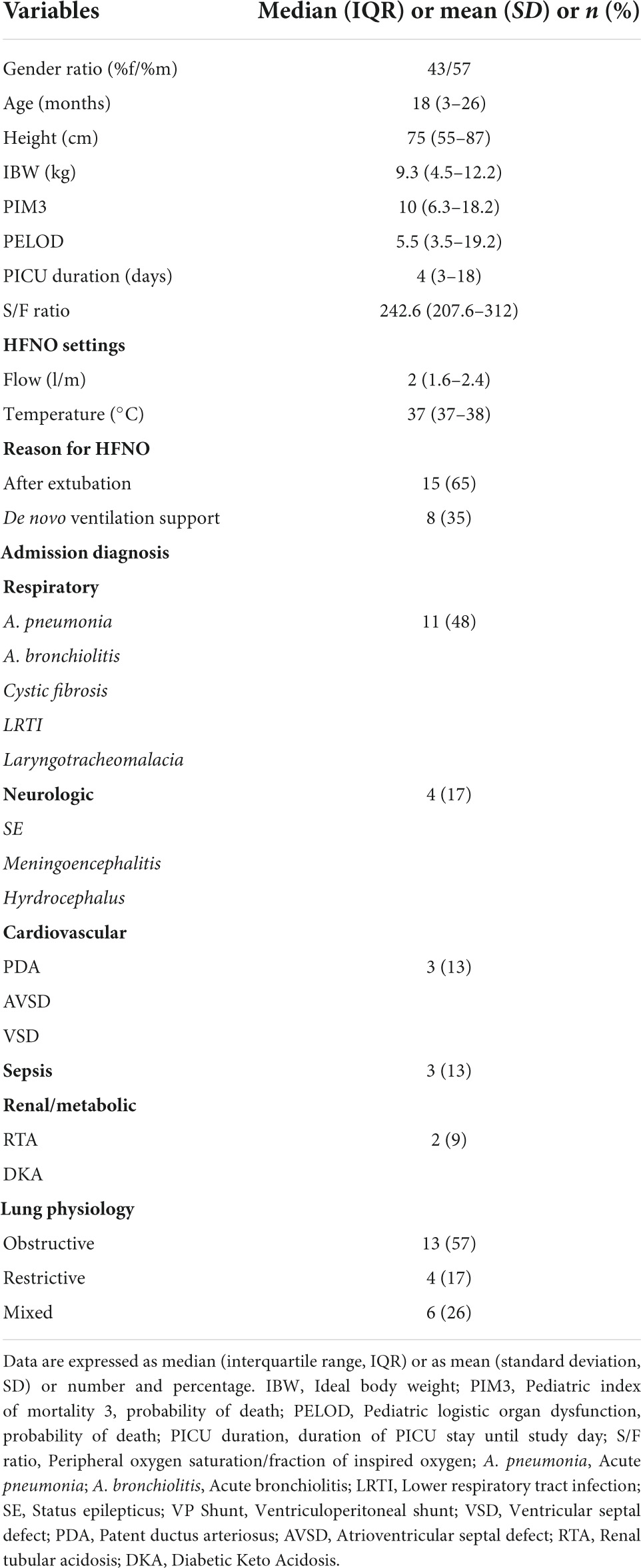
Table 1. Baseline characteristics of the study cohort.
Patients spent more time in optimal SpO2 ranges when the oxygen controller was activated compared to manual oxygen titrations [91⋅3% (IQR 78⋅4–95⋅1%) vs. 63⋅0% (IQR 44.4–70.7%), mean difference 28⋅2% (95%–CI 20⋅6–37⋅8)]; P < 0.001] (Table 2 and Figure 2).

Table 2. Primary and secondary outcomes.
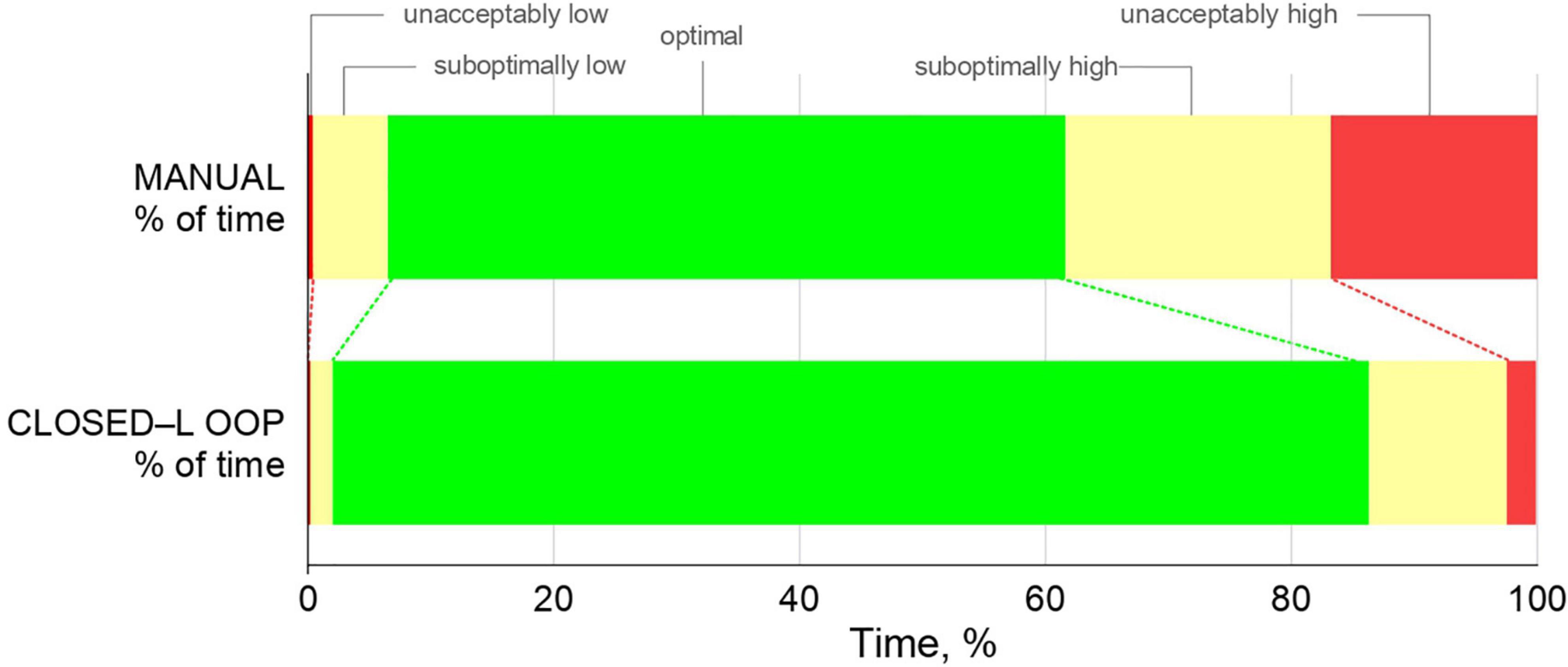
Figure 2. Time spent in optimal, suboptimal, and unacceptable SpO2 ranges.
Patients spent significantly less time in the unacceptably high and unacceptably low SpO2 ranges, and significantly less time in suboptimal low and suboptimal high SpO2 ranges when the oxygen controller was activated (Table 2 and Figure 2).
The median FiO2 was lower with closed-loop oxygen control, although this difference did not reach statistical significance (Table 2). The median SpO2/FiO2 ratio was significantly higher with closed-loop oxygen control (Table 2 and Supplementary Figure 2). There were significantly fewer manual adjustments needed, and the number of alarms was lower with closed-loop oxygen control (Table 2 and Supplementary Figure 2).
Discussion
The findings of this multicentre randomized crossover study in pediatric patients under HFNO for AHRF can be summarized as follows: (1) Compared to manual oxygen titrations, the use of a closed-loop oxygen controller built into an HFNO device increased time spent in optimal SpO2 ranges; (2) decreased time spent in suboptimal and unacceptably high and unacceptably low ranges; (3) decreased time spent in suboptimal and unacceptable SpO2 ranges; (4) reduced oxygen use; and (5) lead to fewer manual adjustments and less alarms.
Our study has several strengths. We used a crossover design, making it possible to compare oxygen therapy under closed-loop oxygen control vs. manual oxygen titrations within each individual patient, increasing the statistical power of our investigation. We performed the study in multiple centers, including university hospitals and teaching hospitals, whereby we increased the external validity of the findings. We followed a strict study protocol and used randomization to prevent potential bias. We had an analysis plan in place before cleaning and closing the database; specifically, we predefined the optimal, suboptimal, and unacceptable SpO2 ranges that were based on consensus before the study. To our best knowledge this is the first study that tested the efficiency of closed-loop oxygen control in pediatric patients receiving HFNO.
The findings of our study are in line with previous studies testing the efficacy of closed-loop oxygen control in preterm infants (13–34) and adults (16, 35–44) receiving HFNO for hypoxemia of various causes. In all those studies, closed-loop oxygen control outperformed healthcare workers performing manual oxygen titrations with respect to the percentage of time spent in target SpO2 ranges and to the time spent in potentially dangerous SpO2 zones (13–44). Our study increases the understanding of the efficacy of closed-loop oxygen control in children with AHRF by providing proof that it also outperforms manual FiO2 titration in patients that are difficult to stabilize. In this respect, the performance is particularly advantageous since it has a strong potential to reduce workloads by the often overtasked ICU healthcare professionals (46, 47).
The findings of our investigation are also in line with studies of closed-loop oxygen controllers in invasively ventilated neonates (17, 48–50) and adult patients (51–56). In those studies, closed-loop oxygen control outperformed manual oxygen titrations with respiratory support in which oxygenation is not only driven by FiO2, but also by the provided tidal volumes and airway pressures. Taken together, closed-loop oxygen control has a wide range of applications in critically ill hypoxemic patients, under various forms of support, from non-intubated patients to intubated patients, from passive to active patients, and in patients that develop hypoxemia after extubation.
It is well known that intensive care doctors and nurses avoid both hypoxemia and hyperoxemia for various valid reasons. This is particularly true for healthcare workers treating critically ill neonates and children (4–7). This approach requires not only well-trained nurses but also large numbers of ICU nurses at the bedside. Indeed, hypoxemia can only be minimized if a nurse is near constantly present to perform manual oxygen titrations (48, 49). This can be very impractical and costly, and can actually not be delivered on a regular basis.
One previous study found that doctors’ responses to oxygen levels beyond the optimal SpO2 zones are “asymmetrical”; they try to prevent both hypoxemia and hyperoxemia, but they seem to put more emphasis on preventing the first than the second (57). Not surprisingly, this results in more time spent in suboptimal or unacceptable higher SpO2 ranges. The advantage of a closed-loop oxygen control system is that deteriorations to both lower and higher SpO2 ranges are prevented equally.
We found that SpO2/FiO2 ratios were higher under closed-loop oxygen control, suggesting that closed-loop oxygen control not only prevents hypoxemic and hyperoxemic deteriorations, but improves oxygenation overall. At the same time, it consumes less oxygen to achieve the same oxygenation levels, which may be critical in low-resource environments or at times of increased demand, such as a rise in oxygen use during a pandemic. This is consistent with several other research demonstrating that patients received less FiO2 under closed-loop control of FiO2 than during manual titration of FiO2 (49, 51, 52, 58).
Interestingly, we noticed much fewer manual adjustments and also much less alarms per hour with closed-loop oxygen control. This may also translate into a reduction in workloads as our data show that manual adjustments are hardly needed with the use of an oxygen controller. Higher workloads for ICU staff are associated with higher mortality rates (59). On top of that, our data also show a strong reduction in the number of alarms, which may increase patient comfort and sleep hygiene, and thereby reduce the risk of delirium (60, 61).
Our study has limitations. Due to the nature of the intervention, we were not able to blind the healthcare workers. However, we used predefined SpO2 zones that reflected the zones to which ICU nurses titrate FiO2 in daily practice. The periods of manual oxygen titrations and automated oxygen control were lasting only 2 h, and thus did not cover all daily activities. However, we wanted to have comparable patient conditions in the two crossover phases for as much as possible, and these conditions could change rapidly in pediatric patients. Additionally, we intended the two study phases to take place in a single shift, which limited the amount of time we had for the full investigation in each individual patient. The crossover design prohibits us from examining the effects of closed-loop oxygen control on clinical endpoints like duration of HFNO or escalation of ventilatory support to invasive ventilation. Future studies should focus on these endpoints.
Conclusion
In conclusion, compared to manual oxygen titrations, closed-loop oxygen control improves time spent in favorable SpO2 zones and reduces time spent in potentially dangerous SpO2 zones in pediatric patients under HFNO for AHRF. In addition, closed-loop oxygen control improves overall oxygenation, uses less oxygen, and is associated with fewer manual adjustments and less alarms.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethical Committee of Dr. Behcet Uz Children’s Research and Training Hospital. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
OS, GC, ST, PH, MC, ES, UK, DN, and HA conceived and designed the study. OS, GC, ST, PH, MC, MS, ES, UK, and GA acquired and analyzed the data. GC, MS, GA, and HA interpreted the data. GC and HA did the statistical analysis. OS, GC, DN, MS, and HA drafted the manuscript. OS, GC, ST, PH, MC, ES, UK, and HA had full access to all of the data. All authors critically revised the manuscript for important intellectual content, were responsible for the final decision to submit for publication, and approved the manuscript.
Funding
The participating centers received only material support from the Hamilton Medical AG, Bonaduz, Switzerland. They received HFNO devices and memory boxes for collecting the respiratory support data for the duration of this study.
Acknowledgments
We thank the trial participants, their families, and all investigators involved in this study. We also thank Jan Zimmermann of Hamilton Medical AG for providing data conversion and math-lab code to analyze the study data.
Conflict of interest
Authors GC and DN worked at Hamilton Medical AG in the Department of Medical Research. Author MS partly worked at Hamilton Medical AG in the Department of Medical Research.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1046902/full#supplementary-material
Supplementary Figure 1 | Trial flow diagram.
Supplementary Figure 2 | Effect of closed-loop oxygen control on alarms, manual titrations, and SpO2/FiO2.
References
1. Turnham H, Agbeko RS, Furness J, Pappachan J, Sutcliffe AG, Ramnarayan P. Non-invasive respiratory support for infants with bronchiolitis: a national survey of practice. BMC Pediatr. (2017) 17:20. doi: 10.1186/s12887-017-0785-0
2. Schmid F, Olbertz DM, Ballmann M. The use of high-flow nasal cannula (HFNC) as respiratory support in neonatal and pediatric intensive care units in Germany – A nationwide survey. Respir Med. (2017) 131:210–4. doi: 10.1016/j.rmed.2017.08.027
3. Kawaguchi A, Garros D, Joffe A, DeCaen A, Thomas NJ, Schibler A, et al. Variation in practice related to the use of high flow nasal cannula in critically Ill children. Pediatr Crit Care Med. (2020) 21:e228–35. doi: 10.1097/PCC.0000000000002258
4. Singer M, Young PJ, Laffey JG, Asfar P, Taccone FS, Skrifvars MB, et al. Dangers of hyperoxia. Crit Care. (2021) 25:440. doi: 10.1186/s13054-021-03815-y
5. Palmer E, Post B, Klapaukh R, Marra G, MacCallum NS, Brealey D, et al. The association between supraphysiologic arterial oxygen levels and mortality in critically Ill patients. A multicenter observational cohort study. Am J Respir Crit Care Med. (2019) 200:1373–80. doi: 10.1164/rccm.201904-0849OC
6. de Jonge E, Peelen L, Keijzers PJ, Joore H, de Lange D, van der Voort PH, et al. Association between administered oxygen, arterial partial oxygen pressure and mortality in mechanically ventilated intensive care unit patients. Crit Care. (2008) 12:R156. doi: 10.1186/cc7150
7. Young PJ, Hodgson CL, Rasmussen BS. Oxygen targets. Intensive Care Med. (2022) 48:732–5. doi: 10.1007/s00134-022-06714-0
8. Pelletier JH, Ramgopal S, Au AK, Clark RSB, Horvat CM. Maximum Pao2 in the First 72 hours of intensive care is associated with risk-adjusted mortality in pediatric patients undergoing mechanical ventilation. Crit Care Explor. (2020) 2:e0186. doi: 10.1097/CCE.0000000000000186
9. Peters MJ, Jones GAL, Wiley D, Wulff J, Ramnarayan P, Ray S, et al. Conservative versus liberal oxygenation targets in critically ill children: the randomised multiple-centre pilot Oxy-PICU trial. Intensive Care Med. (2018) 44:1240–8. doi: 10.1007/s00134-018-5232-7
10. Page D, Ablordeppey E, Wessman BT, Mohr NM, Trzeciak S, Kollef MH, et al. Emergency department hyperoxia is associated with increased mortality in mechanically ventilated patients: a cohort study. Crit Care. (2018) 22:9. doi: 10.1186/s13054-017-1926-4
11. Stenson BJ, Tarnow-Mordi WO, Darlow BA, Simes J, Juszczak E, Askie L, et al. Oxygen saturation and outcomes in preterm infants. N Engl J Med. (2013) 368:2094–104.
12. Lilien TA, Groeneveld NS, van Etten-Jamaludin F, Peters MJ, Buysse CMP, Ralston SL, et al. Association of arterial hyperoxia with outcomes in critically Ill children: a systematic review and meta-analysis. JAMA Network Open. (2022) 5:e2142105. doi: 10.1001/jamanetworkopen.2021.42105
13. Mitra S, Singh B, El-Naggar W, McMillan DD. Automated versus manual control of inspired oxygen to target oxygen saturation in preterm infants: a systematic review and meta-analysis. J Perinatol. (2018) 38:351–60. doi: 10.1038/s41372-017-0037-z
14. Reynolds PR, Miller TL, Volakis LI, Holland N, Dungan GC, Roehr CC, et al. Randomised cross-over study of automated oxygen control for preterm infants receiving nasal high flow. Arch Dis Child Fetal Neonatal Ed. (2019) 104:F366–71. doi: 10.1136/archdischild-2018-315342
15. Waitz M, Schmid MB, Fuchs H, Mendler MR, Dreyhaupt J, Hummler HD. Effects of automated adjustment of the inspired oxygen on fluctuations of arterial and regional cerebral tissue oxygenation in preterm infants with frequent desaturations. J Pediatr. (2015) 166:240–4.e1. doi: 10.1016/j.jpeds.2014.10.007
16. Bourassa S, Bouchard PA, Dauphin M, Lellouche F. Oxygen conservation methods with automated titration. Respir Care. (2020) 65:1433–42. doi: 10.4187/respcare.07240
17. van Kaam AH, Hummler HD, Wilinska M, Swietlinski J, Lal MK, te Pas AB, et al. Automated versus manual oxygen control with different saturation targets and modes of respiratory support in preterm infants. J Pediatr. (2015) 167:545–50.e1-2. doi: 10.1016/j.jpeds.2015.06.012
18. Lal M, Tin W, Sinha S. Automated control of inspired oxygen in ventilated preterm infants: crossover physiological study. Acta Paediatr. (2015) 104:1084–9. doi: 10.1111/apa.13137
19. Dijkman KP, Mohns T, Dieleman JP, van Pul C, Goos TG, Reiss IK, et al. Predictive intelligent control of oxygenation (PRICO) in preterm infants on high flow nasal cannula support: a randomised cross-over study. Arch Dis Child Fetal Neonatal Ed. (2021) 106:621–6. doi: 10.1136/archdischild-2020-320728
20. Dani C, Pratesi S, Luzzati M, Petrolini C, Montano S, Remaschi G, et al. Cerebral and splanchnic oxygenation during automated control of inspired oxygen (FiO2) in preterm infants. Pediatr Pulmonol. (2021) 56:2067–72. doi: 10.1002/ppul.25379
21. Das A, Mhanna M, Teleron-Khorshad A, Houdek J, Kumar N, Gunzler D, et al. A comparison of manual versus automated saturation of peripheral oxygenation in the neonatal intensive care unit. J Matern Fetal Neonatal Med. (2016) 29:1631–5. doi: 10.3109/14767058.2015.1057493
22. Dargaville PA, Sadeghi Fathabadi O, Plottier GK, Lim K, Wheeler KI, Jayakar R, et al. Development and preclinical testing of an adaptive algorithm for automated control of inspired oxygen in the preterm infant. Arch Dis Child Fetal Neonatal Ed. (2017) 102:F31–6. doi: 10.1136/archdischild-2016-310650
23. Zapata J, Gómez JJ, Araque Campo R, Matiz Rubio A, Sola A. A randomised controlled trial of an automated oxygen delivery algorithm for preterm neonates receiving supplemental oxygen without mechanical ventilation. Acta Paediatr. (2014) 103:928–33. doi: 10.1111/apa.12684
24. Van Zanten HA, Kuypers KLAM, Stenson BJ, Bachman TE, Pauws SC, Te Pas AB. The effect of implementing an automated oxygen control on oxygen saturation in preterm infants. Arch Dis Child Fetal Neonatal Ed. (2017) 102:F395–9. doi: 10.1136/archdischild-2016-312172
25. Sturrock S, Ambulkar H, Williams EE, Sweeney S, Bednarczuk NF, Dassios T, et al. A randomised crossover trial of closed loop automated oxygen control in preterm, ventilated infants. Acta Paediatr. (2021) 110:833–7. doi: 10.1111/apa.15585
26. Kaltsogianni O, Dassios T, Greenough A. Does closed-loop automated oxygen control reduce the duration of mechanical ventilation? A randomised controlled trial in ventilated preterm infants. Trials. (2022) 23:276. doi: 10.1186/s13063-022-06222-y
27. Morozoff E, Smyth JA, Saif M. Applying computer models to realize closed-loop neonatal oxygen therapy. Anesth Analg. (2017) 124:95–103. doi: 10.1213/ANE.0000000000001367
28. Gajdos M, Waitz M, Mendler MR, Braun W, Hummler H. Effects of a new device for automated closed loop control of inspired oxygen concentration on fluctuations of arterial and different regional organ tissue oxygen saturations in preterm infants. Arch Dis Child Fetal Neonatal Ed. (2019) 104:F360–5. doi: 10.1136/archdischild-2018-314769
29. Schwarz CE, Kidszun A, Bieder NS, Franz AR, König J, Mildenberger E, et al. Is faster better? A randomised crossover study comparing algorithms for closed-loop automatic oxygen control. Arch Dis Child Fetal Neonatal Ed. (2020) 105:369–74. doi: 10.1136/archdischild-2019-317029
30. Dargaville PA, Marshall AP, Ladlow OJ, Bannink C, Jayakar R, Eastwood-Sutherland C, et al. Automated control of oxygen titration in preterm infants on non-invasive respiratory support. Arch Dis Child Fetal Neonatal Ed. (2022) 107:39–44. doi: 10.1136/archdischild-2020-321538
31. Ali SK, Jayakar RV, Marshall AP, Gale TJ, Dargaville PA. Preliminary study of automated oxygen titration at birth for preterm infants. Arch Dis Child Fetal Neonatal Ed. (2022) 107:539–44. doi: 10.1136/archdischild-2021-323486
32. Plottier GK, Wheeler KI, Ali SK, Fathabadi OS, Jayakar R, Gale TJ, et al. Clinical evaluation of a novel adaptive algorithm for automated control of oxygen therapy in preterm infants on non-invasive respiratory support. Arch Dis Child Fetal Neonatal Ed. (2017) 102:F37–43. doi: 10.1136/archdischild-2016-310647
33. Salverda HH, Cramer SJE, Witlox RSGM, Gale TJ, Dargaville PA, Pauws SC, et al. Comparison of two devices for automated oxygen control in preterm infants: a randomised crossover trial. Arch Dis Child Fetal Neonatal Ed. (2022) 107:20–5. doi: 10.1136/archdischild-2020-321387
34. Schwarz CE, Kreutzer KB, Langanky L, Wolf NS, Braun W, O’Sullivan MP, et al. Randomised crossover trial comparing algorithms and averaging times for automatic oxygen control in preterm infants. Arch Dis Child Fetal Neonatal Ed. (2021) 107:425–30. doi: 10.1136/archdischild-2021-322096
35. Roca O, Caritg O, Santafé M, Ramos FJ, Pacheco A, García-de-Acilu M, et al. Closed-loop oxygen control improves oxygen therapy in acute hypoxemic respiratory failure patients under high flow nasal oxygen: a randomized cross-over study (the HILOOP study). Crit Care. (2022) 26:108. doi: 10.1186/s13054-022-03970-w
36. L’Her E, Jaber S, Verzilli D, Jacob C, Huiban B, Futier E, et al. Automated closed-loop versus standard manual oxygen administration after major abdominal or thoracic surgery: an international multicentre randomised controlled study. Eur Respir J. (2021) 57:2000182. doi: 10.1183/13993003.00182-2020
37. Harper JC, Kearns NA, Maijers I, Bird GE, Braithwaite I, Shortt NP, et al. Closed-loop oxygen control using a novel nasal high-flow device: a randomized crossover trial. Respir Care. (2021) 66:416–24. doi: 10.4187/respcare.08087
38. Kofod LM, Westerdahl E, Kristensen MT, Brocki BC, Ringbæk T, Hansen EF. Effect of automated oxygen titration during walking on dyspnea and endurance in chronic hypoxemic patients with COPD: a randomized crossover trial. J Clin Med. (2021) 10:4820. doi: 10.3390/jcm10214820
39. Malli F, Boutlas S, Lioufas N, Gourgoulianis KI. Automated oxygen delivery in hospitalized patients with acute respiratory failure: a pilot study. Can Respir J. (2019) 2019:4901049. doi: 10.1155/2019/4901049
40. Lellouche F, L’Her E. Automated oxygen flow titration to maintain constant oxygenation. Respir Care. (2012) 57:1254–62. doi: 10.4187/respcare.01343
41. Hansen EF, Hove JD, Bech CS, Jensen JS, Kallemose T, Vestbo J. Automated oxygen control with O2matic(®) during admission with exacerbation of COPD. Int J Chron Obstruct Pulmon Dis. (2018) 13:3997–4003. doi: 10.2147/COPD.S183762
42. Lellouche F, Bouchard PA, Roberge M, Simard S, L’Her E, Maltais F, et al. Automated oxygen titration and weaning with FreeO2 in patients with acute exacerbation of COPD: a pilot randomized trial. Int J Chron Obstruct Pulmon Dis. (2016) 11:1983–90. doi: 10.2147/COPD.S112820
43. Poder TG, Kouakou CRC, Bouchard PA, Tremblay V, Blais S, Maltais F, et al. Cost-effectiveness of FreeO(2) in patients with chronic obstructive pulmonary disease hospitalised for acute exacerbations: analysis of a pilot study in Quebec. BMJ Open. (2018) 8:e018835.
44. Cirio S, Nava S. Pilot study of a new device to titrate oxygen flow in hypoxic patients on long-term oxygen therapy. Respir Care. (2011) 56:429–34. doi: 10.4187/respcare.00983
45. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. (2007) 39:175–91. doi: 10.3758/BF03193146
46. van Zanten HA, Pauws SC, Beks EC, Stenson BJ, Lopriore E, Te Pas AB. Improving manual oxygen titration in preterm infants by training and guideline implementation. Eur J Pediatr. (2017) 176:99–107. doi: 10.1007/s00431-016-2811-x
47. Armbruster J, Schmidt B, Poets CF, Bassler D. Nurses’ compliance with alarm limits for pulse oximetry: qualitative study. J Perinatol. (2010) 30:531–4. doi: 10.1038/jp.2009.189
48. Claure N, Gerhardt T, Everett R, Musante G, Herrera C, Bancalari E. Closed-loop controlled inspired oxygen concentration for mechanically ventilated very low birth weight infants with frequent episodes of hypoxemia. Pediatrics. (2001) 107:1120–4. doi: 10.1542/peds.107.5.1120
49. Claure N, D’Ugard C, Bancalari E. Automated adjustment of inspired oxygen in preterm infants with frequent fluctuations in oxygenation: a pilot clinical trial. J Pediatr. (2009) 155:640–5.e1-2. doi: 10.1016/j.jpeds.2009.04.057
50. Hallenberger A, Poets CF, Horn W, Seyfang A, Urschitz MS, CLAC Study Group. Closed-loop automatic oxygen control (CLAC) in preterm infants: a randomized controlled trial. Pediatrics. (2014) 133:e379–85. doi: 10.1542/peds.2013-1834
51. Johannigman JA, Branson R, Lecroy D, Beck G. Autonomous control of inspired oxygen concentration during mechanical ventilation of the critically injured trauma patient. J Trauma. (2009) 66:386–92. doi: 10.1097/TA.0b013e318197a4bb
52. Arnal JM, Wysocki M, Novotni D, Demory D, Lopez R, Donati S, et al. Safety and efficacy of a fully closed-loop control ventilation (IntelliVent-ASV(R)) in sedated ICU patients with acute respiratory failure: a prospective randomized crossover study. Intensive Care Med. (2012) 38:781–7. doi: 10.1007/s00134-012-2548-6
53. Lellouche F, Bouchard PA, Simard S, L’Her E, Wysocki M. Evaluation of fully automated ventilation: a randomized controlled study in post-cardiac surgery patients. Intensive Care Med. (2013) 39:463–71. doi: 10.1007/s00134-012-2799-2
54. Johannigman JA, Branson RD, Edwards MG. Closed loop control of inspired oxygen concentration in trauma patients. J Am Coll Surg. (2009) 208:763–8; discussion768–9. doi: 10.1016/j.jamcollsurg.2009.01.033
55. Saihi K, Richard JC, Gonin X, Krüger T, Dojat M, Brochard L. Feasibility and reliability of an automated controller of inspired oxygen concentration during mechanical ventilation. Crit Care. (2014) 18:R35–35. doi: 10.1186/cc13734
56. De Bie AJR, Neto AS, van Meenen DM, Bouwman AR, Roos AN, Lameijer JR, et al. Fully automated postoperative ventilation in cardiac surgery patients: a randomised clinical trial. Br J Anaesth. (2020) 125:739–49. doi: 10.1016/j.bja.2020.06.037
57. Mao C, Wong DT, Slutsky AS, Kavanagh BP. A quantitative assessment of how Canadian intensivists believe they utilize oxygen in the intensive care unit. Crit Care Med. (1999) 27:2806–11. doi: 10.1097/00003246-199912000-00033
58. Roué JM, Delpeut J, d’Hennezel A, Tierrie T, Barzic A, L’Her E, et al. Automatic oxygen flow titration in spontaneously breathing children: an open-label randomized controlled pilot study. Pediatr Pulmonol. (2020) 55:3180–8. doi: 10.1002/ppul.25035
59. Tarnow-Mordi WO, Hau C, Warden A, Shearer AJ. Hospital mortality in relation to staff workload: a 4-year study in an adult intensive-care unit. Lancet. (2000) 356:185–9. doi: 10.1016/S0140-6736(00)02478-8
60. Darbyshire JL, Young JD. An investigation of sound levels on intensive care units with reference to the WHO guidelines. Crit Care. (2013) 17:R187. doi: 10.1186/cc12870
61. Smith HAB, Besunder JB, Betters KA, Johnson PN, Srinivasan V, Stormorken A, et al. 2022 society of critical care medicine clinical practice guidelines on prevention and management of pain, agitation, neuromuscular blockade, and delirium in critically ill pediatric patients with consideration of the ICU environment and early mobility. Pediatr Crit Care Med. (2022) 23:e74–110. doi: 10.1097/PCC.0000000000002873
Keywords: intensive care, pediatric [MeSH], hypoxemia, oxygen therapy, high flow (NHF), automation, closed-loop, oxygen controller
Citation: Sandal O, Ceylan G, Topal S, Hepduman P, Colak M, Novotni D, Soydan E, Karaarslan U, Atakul G, Schultz MJ and Ağın H (2022) Closed–loop oxygen control improves oxygenation in pediatric patients under high–flow nasal oxygen—A randomized crossover study. Front. Med. 9:1046902. doi: 10.3389/fmed.2022.1046902
Received: 17 September 2022; Accepted: 26 October 2022;
Published: 16 November 2022.
Edited by:
Zhongheng Zhang, Sir Run Run Shaw Hospital, ChinaReviewed by:
Sung-Min Cho, The Johns Hopkins Hospital, Johns Hopkins Medicine, United StatesAndrás Lovas, Kiskunhalas Semmelweis Hospital, Hungary
Copyright © 2022 Sandal, Ceylan, Topal, Hepduman, Colak, Novotni, Soydan, Karaarslan, Atakul, Schultz and Ağın. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gokhan Ceylan, ZHJnb2toYW5jZXlsYW5AZ21haWwuY29t