 Héloïse Prié1,2
Héloïse Prié1,2 Vanina Meyssonnier1,2
Vanina Meyssonnier1,2 Younes Kerroumi1
Younes Kerroumi1 Beate Heym1,3Olivier Lidove2
Beate Heym1,3Olivier Lidove2 Simon Marmor1,4
Simon Marmor1,4 Valérie Zeller1,2*
Valérie Zeller1,2*- 1Centre de Référence des Infections Ostéo-Articulaires Complexes, Groupe Hospitalier Diaconesses–Croix Saint-Simon, Paris, France
- 2Service de Médecine Interne et Infectiologie, Groupe Hospitalier Diaconesses–Croix Saint-Simon, Paris, France
- 3Laboratoire des Centres de Santé et Hôpitaux d’Île-de-France, Groupe Hospitalier Diaconesses–Croix Saint-Simon, Paris, France
- 4Service de Chirurgie Osseuse et Traumatologique, Groupe Hospitalier Diaconesses–Croix Saint-Simon, Paris, France
Objectives: Analysis the outcomes of Pseudomonas aeruginosa prosthetic joint infection (PJI), and of their clinical and microbiological characteristics, surgical strategies and antibiotic treatments.
Methods: Monocenter cohort study in a Bone-and-Joint-Infection Referral Center (08/2004 to 10/2018) including all consecutive P. aeruginosa PJIs. Data were extracted from the prospective database, including the following events: relapses, new PJIs, related deaths.
Results: Median [IQR]: among the 43 patients included (28 females; 72 [63–80] years old; 27 hip, 15 knee, and 1 shoulder PJIs), 29 (67%) had underlying comorbidities, 12 (28%) had previously been treated for another PJI and 9 (21%) had undergone previous surgeries for their P. aeruginosa PJI. Eleven (26%) PJIs were polymicrobial, 16 (37%) strains were wild type, 8 (19%) ciprofloxacin-resistant. PJIs were classified as late chronic (n = 33), early postoperative (n = 9) or acute hematogenous infection (n = 1). Forty patients underwent surgery: 27 one-stage and 5 two-stage exchanges, 3 debridement and implant retention, and 5 other surgical strategies. Antibiotic treatments were: 29 received 41 [37–43] days of combination therapy (IV anti-pseudomonal β-lactam and 3–5 days of amikacin, then β-lactam and oral ciprofloxacin), followed by oral ciprofloxacin for a total of 12 weeks; 10 received only IV antibiotics for 83 [77–86] days, including 37 [32–46] days of combination therapy; 49 days of ceftazidime alone for 1. During follow-up lasting 33 [24–64.5] months, 2 relapses, 3 new PJIs, and 2 related deaths occurred. Thirty-three (82%) patients and 93% of those managed with one-stage exchange experienced no event.
Conclusion: Outcomes of our cohort’s P. aeruginosa PJIs—predominantly monomicrobial, chronic, ciprofloxacin-susceptible, treated with one-stage exchange and prolonged IV antibiotics—were 82% favorable.
Introduction
Prosthetic joint infection (PJI) is a devastating complication of arthroplasty. The increasing number of joint replacements inevitably leads to increasing PJI incidence, with significant consequences on patients’ morbidity and economic concerns (1–3). Most PJIs are caused by Gram-positive pathogens, while Gram-negative bacilli are found less commonly (11–15%). Pseudomonas aeruginosa represents 3–5% of all PJIs (4, 5).
Treatment of P. aeruginosa PJIs is considered difficult because of the bacterium’s natural resistance to many antimicrobials, increasing acquired resistance, the nosocomial environment and patients’ comorbidities (6–8). The optimal antibiotic regimen and surgical strategy for P. aeruginosa PJIs are not well defined, guidelines are lacking and numerous questions remain.
Only a few retrospective studies focused on P. aeruginosa bone-and-joint infections (BJIs) (9–12). One reported 12 cases of early debridement, antibiotics, and implant retention (DAIR)-treated PJIs achieving 75% successes (11). More recently, a French National Referral Center for BJIs reported 90 cases of implant-associated P. aeruginosa infections, among which 30 were PJIs (12). Better outcome was associated with intravenous (IV) β-lactam administration for at least 3 weeks and oral ciprofloxacin for 3 months.
This prospective, observational study was undertaken to analyze the outcomes of P. aeruginosa PJIs, and to better characterize their clinical and microbiological characteristics, surgical strategies, and antibiotic treatments.
Methods
Study design and setting
This monocenter, observational, cohort study was conducted in a French Referral Center for BJIs from August 2004 to October 2018. All patients admitted for a PJI are registered in the Center’s PJI cohort (NCT 019635 and NCT 02801253). Each patient’s epidemiological, clinical, microbiological, therapeutic (surgical and antibiotics), adverse event, and outcome information was entered prospectively. We extracted P. aeruginosa-infected patients from the PJI-cohort database. The primary outcome was 2-year event-free survival (EFS).
Ethics
All patients gave written informed consent, and the cohort was approved by the Île-de-France Ethics Committee.
Population
All consecutive patients ≥18 years old with confirmed P. aeruginosa PJIs were included. P. aeruginosa had been isolated from at least two cultures of preoperative joint-fluid and/or intraoperative tissue specimens, and at least one of the following criteria was required: a sinus tract communicating with the prosthesis, local inflammatory signs (swelling, warmth, and erythema), C-reactive protein (CRP) >10 mg/L and/or radiological parameters (i.e., periosteal bone formation and subchondral osteolysis) of infection (3, 4, 13, 14). Polymicrobial infections with P. aeruginosa were included.
Prosthetic joint infections were classified on the initial clinical presentation according to three, previously described clinical settings (4, 13) derived from Tsukayama’s classification (15): early-postoperative: onset of symptoms within 30 days after arthroplasty; late-chronic: progressive symptoms occurring ≥30 days after surgery; and acute-hematogenous: defined as sudden onset of local and general symptoms after a symptom-free interval of ≥30 days postsurgery, with identification of a portal of entry or not.
Duration of PJI was calculated from the first day of PJI symptoms to curative surgery in our center, or for non-operated patients to the first day of prolonged suppressive antibiotic surgery.
Microbiology
Pseudomonas aeruginosa and other microorganisms isolated from PJIs were identified in intraoperative sample and/or preoperative joint-fluid aspirate cultures, handled as previously described (4, 14). Bacteria were identified to species with the rapid ID 32 API system (bioMérieux, Marcy-l’Étoile, France) and, since 2012, by mass spectrometry (MALDI Biotyper, Bruker Daltonik GmbH, Bremen, Germany). Antibiotic susceptibilities were determined with the standard disk-diffusion method, according to the recommendations of the French Society of Microbiology (CaSFM) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST).
Pseudomonas aeruginosa multidrug resistance (MDR) was defined as previously described (16). When a patient had several different isolates, the most resistant strain was retained for description and choice of treatment.
Surgery and antibiotic treatments
Medical–surgical management strategies were decided during multidisciplinary consensus meetings, according to the algorithm described in Supplementary Figure 1.
Antibiotics were usually started during surgery after tissue sampling. Preoperative antibiotic therapy was administered systematically until December 2016, and, since January 2017, for selected cases only (clinical sepsis, bacteremia, large local inflammation or abscess, and/or CRP ≥50 mg/L).
Antibiotic therapy lasted 84 days for all patients from 2004 to 2012; 42 days after DAIR; and 84 days after exchange-arthroplasty-treated patients from 2013 to 2016. Since 2017, all patients have received 42 days of antibiotics, except those at high risk of relapse (multiple operations, severe immunosuppression, sickle-cell anemia, irradiated bone, and large bone graft) who were treated for 84 days.
First-line, IV-administered, combination antibiotic therapy (CAT) was ceftazidime–amikacin for 3–5 days, followed by IV ceftazidime and oral ciprofloxacin to complete 28–42 days. Patients treated for 84 days received an additional 42–56 days course of oral ciprofloxacin. In the case of contraindication or resistance to ciprofloxacin, IV CAT with an anti-pseudomonal β-lactam (ceftazidime, cefepime, or meropenem) and fosfomycin, colistin, or aminoglycoside (maximum 2 weeks) was given. High-dose β-lactams (ceftazidime, 100 mg/kg/day, after a 2-g loading dose) were administered by continuous IV infusion to all patients. Drug-monitoring assured reaching target, plasma ceftazidime concentrations of 50–70 mg/L.
Adverse drug-reaction severity was graded according to the Common Terminology Criteria for Adverse Events (CTCAE) (17).
Outcomes
The primary endpoint was 2-year follow-up event-free-survival (EFS), considering the following events: relapse with the same bacteria, new infection (microorganism different than the initial PJI) and infection- or treatment-related death.
Patients were prospectively followed after discharge at 3, 6, 12, and 24 months, then every 2 years. Patients unable to attend follow-up visits were contacted by phone to assess their health and prosthesis evolution.
Statistical analyses
Categorical variables are expressed as number (%) and quantitative variables as median [interquartile range (IQR)]. Fisher’s exact test, Student’s t-test, or Mann–Whitney U-test, as appropriate, were used to compare PJI baseline admission to our center characteristics and outcomes. The Kaplan–Meier method was used to estimate cumulative EFS incidence and 95% confidence intervals (CIs).
Results
Study population and prosthetic joint infection characteristics
During the 14-year study period, among 1,539 managed PJIs, 170 (11%) Gram-negative and 43 (2.8%) P. aeruginosa PJIs occurred. Table 1 reports their clinical and laboratory characteristics. Among these 43 patients, 32 (74%) were monomicrobial PJIs. Most were hip and knee PJIs. Patients had undergone a median [IQR] of 2 (1–3) surgeries on the affected joint. More than one-quarter had a previous, other-site PJI. Two-third of the patients had underlying comorbidities detailed in Table 1.
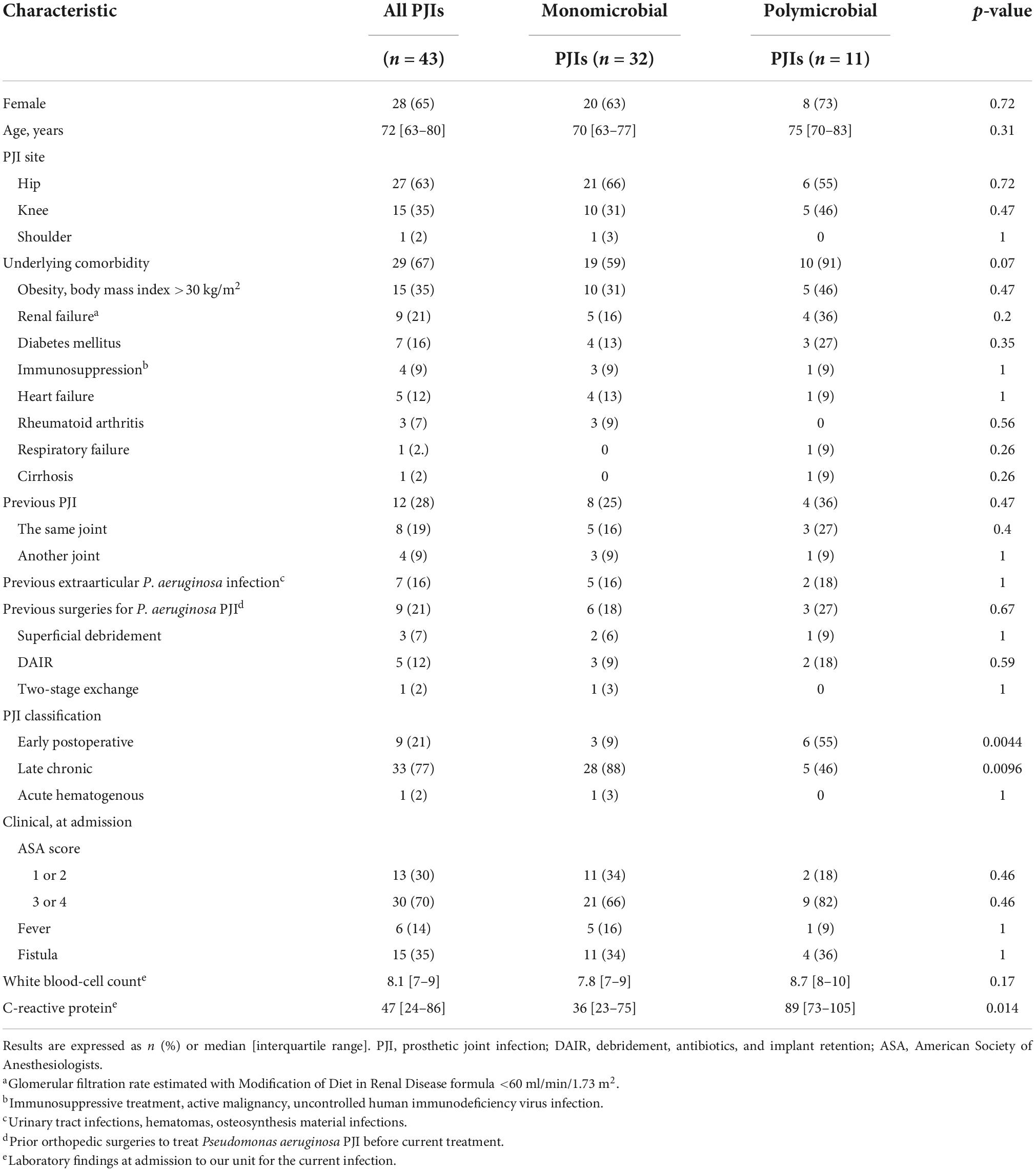
Table 1. Baseline characteristics of 43 patients with P. aeruginosa PJIs and according to type of infection.
Only one acute-hematogenous infection was observed. The source of infection was the urinary tract, as the patient experienced urinary sepsis, fever, and bacteremia with the same P. aeruginosa, 3 weeks before the onset of PJI signs. Nine other patients developed an early postoperative PJI. Most patients (n = 33, 77%) had a late-chronic PJI. The source of infection was considered to be the surgical site, but 7 patients had previous extra articular P. aeruginosa infection or colonization. Four involved the urinary tract in the 6 months prior to PJI (pyelonephritis, cystitis, and two urinary tract colonization), two experienced an infected hematoma following arthroplasty and one patient had had an implant-associated infection after osteosynthesis of a femoral fracture infection 25 years ago.
Median [IQR] duration of PJI symptoms before curative surgery or prolonged suppressive antibiotic therapy in our center, was 176 [60–342] days for the total population. It was 53 [20–136] days for early-postoperative and 251 [136–371] days for late-chronic PJIs. For the only hematogenous infection, symptoms lasted 104 days before surgical treatment.
Microbiological findings
Among 37 joint-fluid cultures of preoperative aspirates, 36 yielded P. aeruginosa and one Staphylococcus simulans. Cultures of intraoperative samples taken from 40 patients isolated P. aeruginosa exclusively in 28 (70%) patients, 11 (28%) were polymicrobial, and 1 from a patient given preoperative antibiotic therapy remained sterile.
Susceptibility testing of the 43 strains showed that 16 (37%) were wild-type P. aeruginosa, 35 (81%) were ciprofloxacin-susceptible (Supplementary Table 1), and 4 (9%) were MDR.
The 11 (26%) patients with polymicrobial PJIs were slightly older, had more comorbidities, higher CRP levels and more frequent early-postoperative PJIs (Table 1). Other coinfecting microorganisms were mostly Gram-positive cocci [five each: methicillin-susceptible (MS) coagulase-negative staphylococci (CNS) or Enterococcus spp.; four each: MS Staphylococcus aureus (MSSA) or Enterobacteriaceae; and two each: methicillin-resistant CNS, Streptococcus spp. or Gram-positive bacilli].
Surgical strategies
Three patients with early-postoperative PJIs underwent DAIR 13, 28 or 30 days after prosthesis implantation.
Thirty-two patients underwent prosthesis exchange. Twenty-seven were one-stage exchanges: 5 were polymicrobial PJIs, 24 ciprofloxacin-susceptible, and 2 MDR P. aeruginosa strains.
Other surgical treatments were knee arthrodeses and hip resections (two each), in patients with previous, same-site PJIs. One patient underwent transfemoral amputation for knee PJI with sepsis and extensive skin necrosis.
Polymicrobial infections were more frequently managed with DAIR or other surgery (6/11, 55%), rather than with prosthesis exchange (5/11, 46%), compared to monomicrobial PJIs (7 and 93%, respectively, p = 0.003).
The four MDR-P. aeruginosa PJI patients underwent one-stage for 2, and two-stage exchange or hip-resection, for one each.
Three non-operated patients were treated with prolonged suppressive antibiotic therapy (PSAT).
Antibiotic strategy
Preoperative antibiotics
Among 30 (75%) patients given preoperative IV antibiotics, 24 (80%) received combined β-lactam and aminoglycoside (mostly ceftazidime and amikacin, for 21) for a median [IQR] of 4.5 (2–6) days. The others received β-lactam monotherapy or association with fosfomycin or colistin.
Postoperative curative antibiotics
Types, molecules and durations of antibiotic treatments are reported in Table 2. Among 29 (73%) patients receiving first-line antibiotics, 24 (83%) underwent prosthesis exchange, 22 of which were one-stage. Eleven patients were prescribed alternative antibiotic regimens: seven with ciprofloxacin-resistant strains and four with ciprofloxacin contraindications. Thirty-one (78%) patients received antibiotics for 84 days and nine (23%, including the three DAIR-treated) for 42 days.
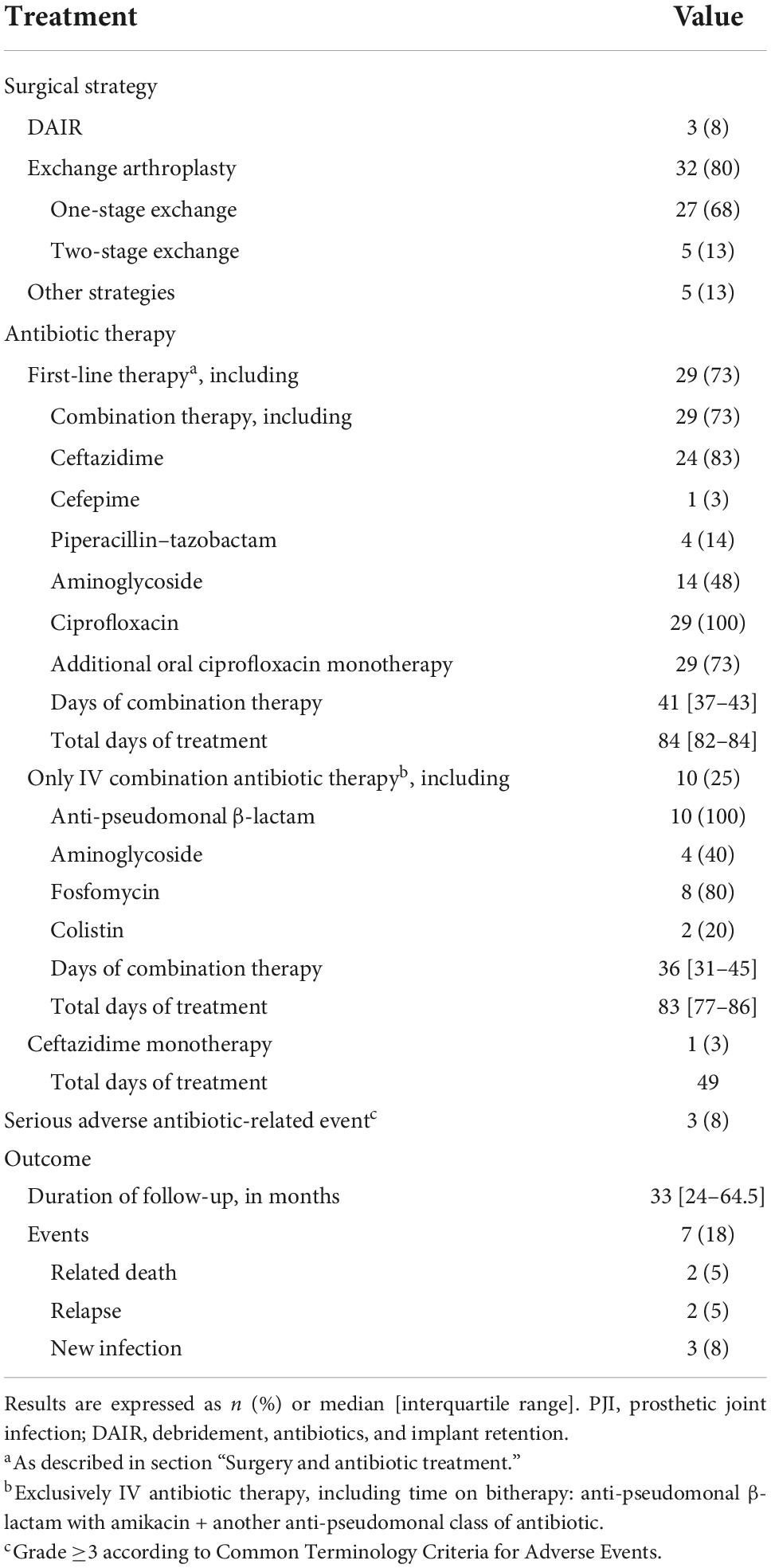
Table 2. Post-operative antibiotic therapies and outcomes of 40 P. aeruginosa PJIs after curative surgery.
Three patients experienced antibiotic serious adverse events (grade ≥3): acute renal failure, esophageal candidiasis, and Clostridium difficile colitis. None required antibiotic discontinuation.
Prolonged suppressive antibiotic therapy
Three very old and frail patients received PSAT comprising oral ciprofloxacin after 19–28 days of IV ceftazidime with amikacin or without. Drug-induced peripheral neuropathy forced two to stop ciprofloxacin after 6 and 18 months.
Outcomes
Median [IQR] follow-up lasted 33 [24–64.5] months for the 40 patients managed with a curative strategy; two were lost-to-follow-up before 24 months.
Seven events occurred: two related deaths, three new PJIs, and two relapses (Table 3). The 2-year and end-of-follow-up crude EFS rates were 85 and 82%, respectively. The estimated 2-year and end-of-follow-up cumulative EFS rates (CIs) were 84% (73–96.7%) and 79.4% (66.3–95%), respectively (Figure 1). For patients managed with one-stage exchange arthroplasty, the 2-year and end-of-follow-up crude EFS rates were 96 and 92%, respectively.
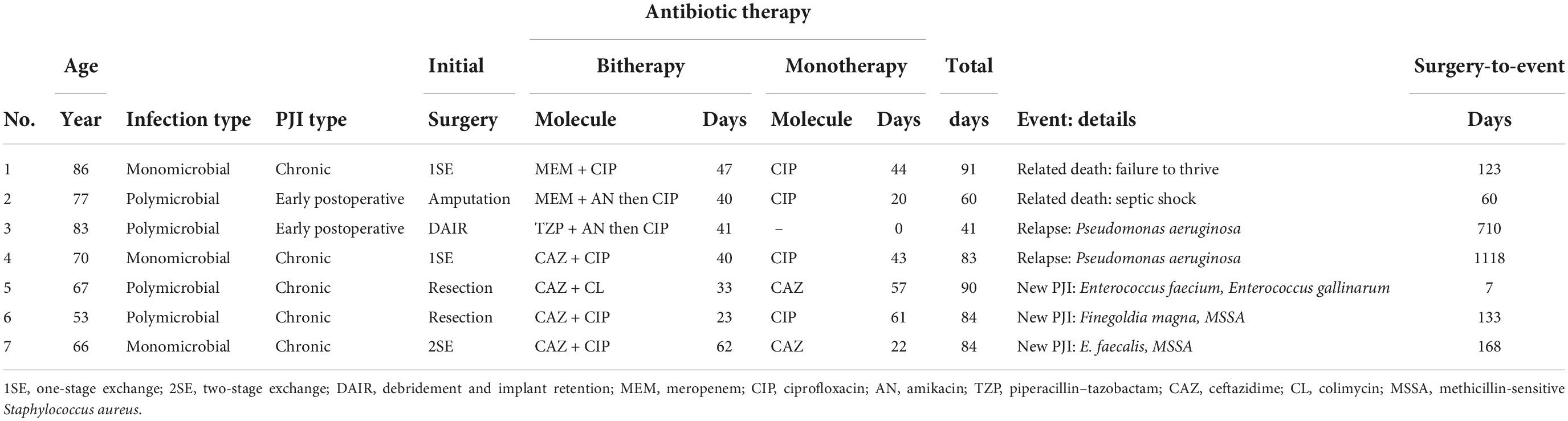
Table 3. Details of the reported events.
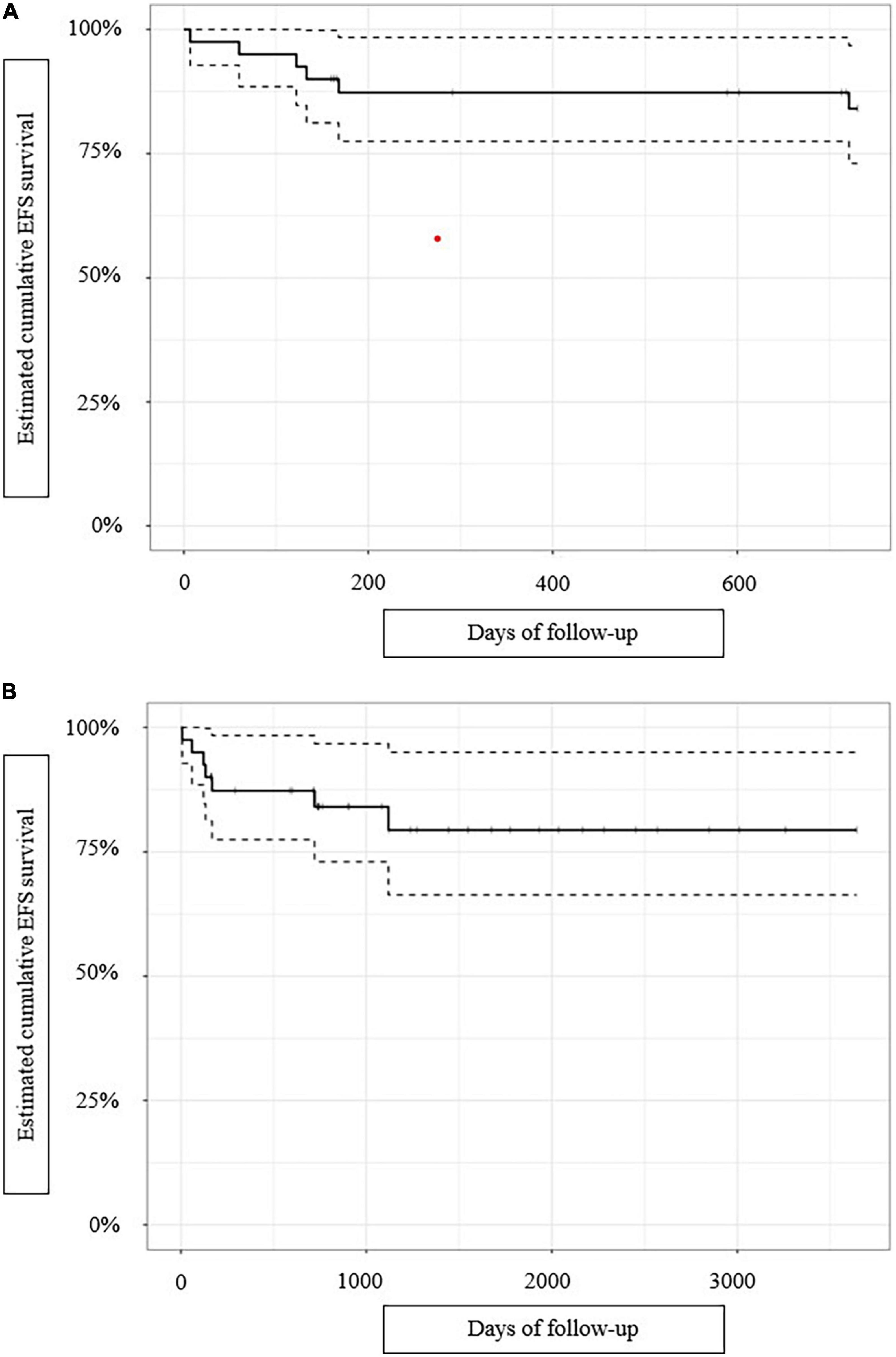
Figure 1. For 40 patients curatively treated for P. aeruginosa prosthetic joint infections, Kaplan–Meier-estimated: (A) cumulative 2-year event-free survival (EFS), and (B) cumulative end-of-follow-up event-free survival. The dashed lines indicated the confidence intervals.
Among the three DAIR-treated patients, an 83-year-old diabetic man, with chronic renal insufficiency, and wild-type P. aeruginosa and MSSA hip PJI operated 28 days after prosthesis implantation, relapsed with a persistent wild-type strain.
Among 32 patients who underwent prosthesis exchange, three (9%) experienced events: a 70-year-old woman with no comorbidity after chronic P. aeruginosa knee PJI relapsed with the same wild-type P. aeruginosa; one related death (multiple prolonged decubitus complications within 1 year) and a new PJI (MSSA and Enterococcus faecalis).
One 77-year-old patient died of septic shock after urgent knee amputation for necrotizing polymicrobial PJI. Two patients who underwent hip resection for chronic polymicrobial PJIs developed new polymicrobial PJIs.
Event-free survival tended to be lower for patients with polymicrobial than monomicrobial PJIs (64 vs. 90%, p = 0.075). It was comparable for patients with ciprofloxacin-susceptible (84%; five events: two relapses, one new PJI, and two related deaths) and ciprofloxacin-resistant PJIs (75%; two new PJIs).
Two of the three PSAT-treated patients relapsed 7 months and 2 years after having stopped ciprofloxacin for adverse events; their relapsing strains remained ciprofloxacin-susceptible.
Discussion
We described 43 P. aeruginosa-PJI patients extracted from a prospective cohort and managed in a BJI Referral Center over 14 years. The cohort’s strength is its focus on PJIs and its prospective, prolonged follow-up.
These patients included a high percentage with previous PJIs and surgeries, as also observed by others, partly explained by the nosocomial origin of P. aeruginosa (9, 10, 18). Unlike previous studies, three-quarters of our observed PJIs were late-chronic, monomicrobial infections, whereas Gram-negative and P. aeruginosa PJIs are often early-postoperative and polymicrobial (5, 11, 12, 19). Our Referral Center’s BJI activity has certainly contributed to the selection of this different PJI population, because 21% of our patients had been transferred from primary-care centers after undergoing a first surgical intervention that failed. These late chronic PJIs seem to be acquired per or postoperatively, but among them 7 had a history of previous extra articular, especially urinary, P. aeruginosa infection or colonization. This raises the question of whether these extra articular infections are not the PJI source, finally acquired by hematogenous route or by contiguity with the infectious site.
Overall, 85 and 82% of the operated patients had not experienced any event at 2-years and the end-of-follow-up, respectively; rates higher than the 68–75% previously reported (9, 12, 20). Our patients’ outcomes differed according to the surgical strategy. For prosthesis exchange, the most frequent strategy applied in our cohort, EFS reached 91% and even 93% when considering only one-stage exchanges. Only one patient relapsed. These results are highly satisfying and encouraging, especially when compared to the largest P. aeruginosa-PJI population described by Shah et al. (9). Those authors had a 5-year 71% failure-free rate after one-stage and 39% after two-stage exchange. Among our three DAIR-treated patients with early-postoperative PJIs, one relapsed. No definitive conclusions can be drawn based on such small numbers, but post-DAIR failure-free survival reported by others ranged between 26 and 79%, close to our values (9, 11, 20).
We prescribed prolonged antibiotic therapy with 42-days-long CAT with IV β-lactam and oral ciprofloxacin for nearly three-quarters of our patients. Ceftazidime was the first-choice β-lactam, because of its excellent bactericidal activity against P. aeruginosa (21, 22). Data on ceftazidime bone diffusion are scarce, reportedly 20–40% of the serum concentration (23). To optimize ceftazidime’s time-dependent activity and reach therapeutic concentration, we used continuous, high-dose infusion adapted by drug-monitoring, as previously supported about antipseudomonal β-lactam in general (24).
Amikacin was combined for the first few days to avoid development of drug resistance and enhance bactericidal activity, followed by oral ciprofloxacin, also controlled by drug-monitoring. Ciprofloxacin alone was prescribed for 42 additional days, to patients treated for 84 days.
In their recent study, Cerioli et al. (12) observed that effective IV β-lactam lasting at least 3 weeks and ciprofloxacin for at least 3 months were independently associated with better outcomes. Other authors also observed better outcomes when fluoroquinolones were prescribed to treat P. aeruginosa and Gram-negative PJIs (12, 20, 25), attributed to their high bone diffusion and activity in biofilm (26, 27). Optimal durations of initial IV and CAT remain unknown, but Cerioli et al.’s findings and our results support prolonged, combined, IV β-lactam and ciprofloxacin, longer than that usually accepted for fluoroquinolone-susceptible Enterobacteriaceae PJIs (20, 25).
The 20% ciprofloxacin-resistance rate observed in our population was not high and close to that reported for invasive P. aeruginosa strains in France (28). No standard treatment is recommended for ciprofloxacin-resistant P. aeruginosa PJIs. The eight patients with ciprofloxacin-resistant strains received 12 weeks of IV antibiotics, including 5 weeks of CAT; none relapsed but two developed new PJIs.
The three PSAT-treated patients had favorable clinical and microbiological outcomes until they stopped ciprofloxacin because of adverse events. Fluoroquinolone-susceptible strains were also found at relapse. This suppressive therapeutic option should be chosen only when curative strategies are contraindicated. Indeed, ciprofloxacin is the only fluoroquinolone available, and its use is limited by potential resistance emergence and adverse events under prolonged monotherapy. More data are needed to determine whether PSAT with ciprofloxacin is indeed a therapeutic option (29, 30).
Outcomes of polymicrobial PJIs were poorer than monomicrobial infections. Although not previously identified as a risk factor for treatment failure, polymicrobial infections were mostly treated with DAIR or non-conservative surgery, strategies that have poorer outcomes than prosthesis exchange.
This study had several limitations, especially the small size of the population. However, P. aeruginosa PJIs are quite rare and the single-center design precluded multivariate analyses. Because of Referral Center selection bias, results are difficult to extrapolate to other populations, particularly those with higher MDR rates. We did not collect the ambulatory status of the patients during the follow-up, which prevent us from evaluating the functional results of medico-surgical treatment. Notably, the study period was long and procedures evolved over time, leading to different PJI treatments. However, observational studies can yield precise data on rare and specific situations, helping to optimize management of this devastating nosocomial complication.
Conclusion
In addition to global favorable outcomes for 82% of these difficult-to-treat PJIs, we observed >90% favorable outcomes for the main population managed with one-stage exchange and prolonged IV antibiotics for chronic ciprofloxacin-susceptible P. aeruginosa PJIs. Additional larger studies are needed to better specify optimal surgical strategies and antibiotics.
Data availability statement
The raw data are not publicly available because French regulatory and Ethics Committees do not authorize the deposition of personal patient data in a public database. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the Île-de-France Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
Author contributions
HP, VM, VZ, YK, and SM conceived the study. HP, VM, YK, and VZ analyzed the data. HP, VM, and VZ wrote the original draft of the manuscript and performed the literature review. VM and VZ reviewed and edited the manuscript. VZ, SM, and YK were the investigators of the prospective cohort. VM, VZ, BH, OL, and SM participated in the patient care and the review of the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
We thank Prof. Patrick Plesiat (Pseudomonas aeruginosa National Reference Center, Besançon) for his microbiological and pharmacological review about P. aeruginosa treatment, Janet Jacobson for English language support. Preliminary findings were presented at the RICAI Congress, Paris, on 17 December 2019.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1039596/full#supplementary-material
References
1. Putman S, Argenson J, Bonnevialle P, Ehlinger M, Vie P, Leclercq S, et al. Ten-year survival and complications of total knee arthroplasty for osteoarthritis secondary to trauma or surgery: a French multicentre study of 263 patients. Orthop Traumatol Surg Res. (2018) 104:161–4. doi: 10.1016/j.otsr.2017.11.019
2. Kurtz S, Ong K, Schmier J, Mowat F, Saleh K, Dybvik E, et al. Future clinical and economic impact of revision total hip and knee arthroplasty. J Bone Joint Surg Am. (2007) 89(Suppl. 3):144–51. doi: 10.2106/JBJS.G.00587
3. Osmon D, Berbari E, Berendt A, Lew D, Zimmerli W, Steckelberg J, et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the infectious diseases society of America. Clin Infect Dis. (2013) 56:e1–25. doi: 10.1093/cid/cis803
4. Zeller V, Kerroumi Y, Meyssonnier V, Heym B, Metten M, Desplaces N, et al. Analysis of postoperative and hematogenous prosthetic joint-infection microbiological patterns in a large cohort. J Infect. (2018) 76:328–34. doi: 10.1016/j.jinf.2017.12.016
5. Triffault-Fillit C, Ferry T, Laurent F, Pradat P, Dupieux C, Conrad A, et al. Microbiologic epidemiology depending on time to occurrence of prosthetic joint infection: a prospective cohort study. Clin Microbiol Infect. (2019) 25:353–8. doi: 10.1016/j.cmi.2018.04.035
6. Cunningham D, Kavolus J, Bolognesi M, Wellman S, Seyler T. Specific infectious organisms associated with poor outcomes in treatment for hip periprosthetic infection. J Arthroplasty. (2017) 32:1984–90.e5. doi: 10.1016/j.arth.2017.01.027
7. Tornero E, Martínez-Pastor J, Bori G, García-Ramiro S, Morata L, Bosch J, et al. Risk factors for failure in early prosthetic joint infection treated with debridement. Influence of etiology and antibiotic treatment. J Appl Biomater Funct Mater. (2014) 12:129–34. doi: 10.5301/jabfm.5000209
8. Ascione T, Pagliano P, Balato G, Mariconda M, Rotondo R, Esposito S. Oral therapy, microbiological findings, and comorbidity influence the outcome of prosthetic joint infections undergoing 2-stage exchange. J Arthroplasty. (2017) 32:2239–43. doi: 10.1016/j.arth.2017.02.057
9. Shah N, Osmon D, Steckelberg J, Sierra R, Walker R, Tande A, et al. Pseudomonas prosthetic joint infections: a review of 102 episodes. J Bone Jt Infect. (2016) 1:25–30. doi: 10.7150/jbji.15722
10. Laghmouche N, Compain F, Jannot A, Guigui P, Mainardi J, Lonjon G, et al. Successful treatment of Pseudomonas aeruginosa osteomyelitis with antibiotic monotherapy of limited duration. J Infect. (2017) 75:198–206. doi: 10.1016/j.jinf.2017.06.006
11. Veltman E, Vos F, Meis J, Goosen J. Debridement, antibiotics and implant retention in early postoperative infection with Pseudomonas aeruginosa. J Infect. (2015) 70:307–9. doi: 10.1016/j.jinf.2014.10.002
12. Cerioli M, Batailler C, Conrad A, Roux S, Perpoint T, Becker A, et al. Pseudomonas aeruginosa implant-associated bone and joint infections: experience in a regional reference center in France. Front Med. (2020) 7:513242. doi: 10.3389/fmed.2020.513242
13. Zimmerli W, Trampuz A, Ochsner P. Prosthetic-joint infections. N Engl J Med. (2004) 351:1645–54. doi: 10.1056/NEJMra040181
14. Zeller V, Letembet V, Meyssonnier V, Heym B, Ziza J, Marmor S. Cutibacterium (formerly Propionibacterium) avidum: a rare but avid agent of prosthetic hip infection. J Arthroplasty. (2018) 33:2246–50. doi: 10.1016/j.arth.2018.02.008
15. Tsukayama D, Estrada R, Gustilo R. Infection after total hip arthroplasty. A study of the treatment of one hundred and six infections. J Bone Joint Surg Am. (1996) 78:512–23. doi: 10.2106/00004623-199604000-00005
16. Magiorakos A, Srinivasan A, Carey R, Carmeli Y, Falagas M, Giske C, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. (2012) 18:268–81. doi: 10.1111/j.1469-0691.2011.03570.x
17. Trotti A, Colevas A, Setser A, Rusch V, Jaques D, Budach V, et al. CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol. (2003) 13:176–81. doi: 10.1016/S1053-4296(03)00031-6
18. Zeller V, Lhotellier L, Marmor S, Leclerc P, Krain A, Graff W, et al. One-stage exchange arthroplasty for chronic periprosthetic hip infection: results of a large prospective cohort study. J Bone Joint Surg Am. (2014) 96:e1. doi: 10.2106/JBJS.L.01451
19. Hsieh P, Lee M, Hsu K, Chang Y, Shih H, Ueng S. Gram-negative prosthetic joint infections: risk factors and outcome of treatment. Clin Infect Dis. (2009) 49:1036–43. doi: 10.1086/605593
20. Rodríguez-Pardo D, Pigrau C, Lora-Tamayo J, Soriano A, del Toro M, Cobo J, et al. Gram-negative prosthetic joint infection: outcome of a debridement, antibiotics and implant retention approach. A large multicentre study. Clin Microbiol Infect. (2014) 20:911–9. doi: 10.1111/1469-0691.12649
21. Bonfiglio G, Marchetti F. In vitro activity of ceftazidime, cefepime and imipenem on 1,005 Pseudomonas aeruginosa clinical isolates either susceptible or resistant to beta-lactams. Chemotherapy. (2000) 46:229–34. doi: 10.1159/000007294
22. Van Laethem Y, Klastersky J. Serum bactericidal activity of mezlocillin, ceftazidime, mezlocillin/ceftazidime and mezlocillin/amikacin against Klebsiella pneumoniae and Pseudomonas aeruginosa. Eur J Clin Microbiol. (1986) 5:110–4. doi: 10.1007/BF02013479
23. Leigh D, Griggs J, Tighe C, Powell H, Church J, Wise K, et al. Pharmacokinetic study of ceftazidime in bone and serum of patients undergoing hip and knee arthroplasty. J Antimicrob Chemother. (1985) 16:637–42. doi: 10.1093/jac/16.5.637
24. Bassetti M, Vena A, Russo A, Croxatto A, Calandra T, Guery B. Rational approach in the management of Pseudomonas aeruginosa infections. Curr Opin Infect Dis. (2018) 31:578–86. doi: 10.1097/QCO.0000000000000505
25. Martínez-Pastor J, Muñoz-Mahamud E, Vilchez F, García-Ramiro S, Bori G, Sierra J, et al. Outcome of acute prosthetic joint infections due to gram-negative bacilli treated with open debridement and retention of the prosthesis. Antimicrob Agents Chemother. (2009) 53:4772–7. doi: 10.1128/AAC.00188-09
26. Tanaka G, Shigeta M, Komatsuzawa H, Sugai M, Suginaka H, Usui T. Effect of the growth rate of Pseudomonas aeruginosa biofilms on the susceptibility to antimicrobial agents: beta-lactams and fluoroquinolones. Chemotherapy. (1999) 45:28–36. doi: 10.1159/000007162
27. Fong I, Ledbetter W, Vandenbroucke A, Simbul M, Rahm V. Ciprofloxacin concentrations in bone and muscle after oral dosing. Antimicrob Agents Chemother. (1986) 29:405–8. doi: 10.1128/AAC.29.3.405
28. European Centre for Disease Prevention and Control [ECDC] Surveillance of antimicrobial resistance in Europe 2018. Stockholm: ECDC (2019).
29. Prendki V, Ferry T, Sergent P, Oziol E, Forestier E, Fraisse T, et al. Prolonged suppressive antibiotic therapy for prosthetic joint infection in the elderly: a national multicentre cohort study. Eur J Clin Microbiol Infect Dis. (2017) 36:1577–85. doi: 10.1007/s10096-017-2971-2
Keywords: prosthetic joint infection, one-stage exchange, debridement and implant retention, ciprofloxacin, Pseudomonas aeruginosa, ceftazidime
Citation: Prié H, Meyssonnier V, Kerroumi Y, Heym B, Lidove O, Marmor S and Zeller V (2022) Pseudomonas aeruginosa prosthetic joint-infection outcomes: Prospective, observational study on 43 patients. Front. Med. 9:1039596. doi: 10.3389/fmed.2022.1039596
Received: 08 September 2022; Accepted: 21 November 2022;
Published: 08 December 2022.
Edited by:
Eric Denes, Polyclinique de Limoges, FranceReviewed by:
Mousumi Chaudhury, Arkansas Children’s Nutrition Center, Agricultural Research Service (USDA), United StatesFabrice Fiorenza, Centre Hospitalier Universitaire de Limoges, France
Copyright © 2022 Prié, Meyssonnier, Kerroumi, Heym, Lidove, Marmor and Zeller. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Valérie Zeller, dnplbGxlckBob3BpdGFsLWRjc3Mub3Jn