 Blandine Rammaert1*†
Blandine Rammaert1*† Christophe Maunoury2
Christophe Maunoury2 Tioka Rabeony3Jean-Michel Correas4Caroline Elie3
Tioka Rabeony3Jean-Michel Correas4Caroline Elie3 Serge Alfandari5‡Pierre Berger6‡Marie-Thérèse Rubio7‡Thorsten Braun8‡Prissile Bakouboula3
Serge Alfandari5‡Pierre Berger6‡Marie-Thérèse Rubio7‡Thorsten Braun8‡Prissile Bakouboula3 Sophie Candon9‡Françoise Montravers10‡Olivier Lortholary1,11
Sophie Candon9‡Françoise Montravers10‡Olivier Lortholary1,11  on behalf of the Canhpari Study Group
on behalf of the Canhpari Study Group- 1Université de Paris Cité, APHP, Service des Maladies Infectieuses et Tropicales, Hôpital Necker-Enfants Malades, Centre d’Infectiologie Necker-Pasteur, Institut Imagine, Paris, France
- 2Université de Paris, APHP, Hôpital Européen Georges Pompidou, Service de Médecine Nucléaire, Paris, France
- 3APHP, URC Necker-Cochin, Paris, France
- 4Université de Paris Cité, APHP, Service de Radiologie Adulte, Hôpital Necker-Enfants Malades, Paris, France
- 5Centre Hospitalier Tourcoing, Service de Réanimation et Maladies Infectieuses, Tourcoing, France
- 6Institut Paoli-Calmettes, Infectiologie Transversale, Marseille, France
- 7CHU Nancy, Service d’Hématologie, Nancy, France
- 8Université de Paris Nord, APHP, Hôpital Avicenne, Service d’Hématologie, Bobigny, France
- 9Université de Rouen Normandie, INSERM U1234, CHU de Rouen Normandie, Rouen, France
- 10Sorbonne Université, APHP, Service de Médecine Nucléaire, Hôpital Tenon, Paris, France
- 11Institut Pasteur, CNRS, Unité de Mycologie Moléculaire, Centre National de Référence Mycoses Invasives et Antifongiques, UMR 2000, Paris, France
Background: Chronic disseminated candidiasis (CDC) classically occurs after profound and prolonged neutropenia. The aim of the CANHPARI study was to assess the clinical value of adding 18F-fluorodeoxyglucose PET/CT to conventional radiology for initial and subsequent evaluations of CDC.
Materials and methods: A pilot prospective study was conducted in 23 French onco-hematological centers from 2013 to 2017 (NCT01916057). Patients ≥ 18 y.o. suspected for CDC on abdominal conventional imaging (CT or MRI) were included. PET/CT and conventional imaging were performed at baseline and month 3 (M3). Follow-up was assessed until M12. The primary outcome measure was the global response at M3, i.e., apyrexia and complete response to PET/CT. The secondary outcome measure consists in comparison between responses to PET/CT and conventional imaging at diagnosis and M3.
Results: Among 52 included patients, 44 were evaluable (20 probable and 24 possible CDC); 86% had acute leukemia, 55% were male (median age 47 years). At diagnosis, 34% had fever and conventional imaging was always abnormal with microabscesses on liver and spleen in 66%, liver in 25%, spleen in 9%. Baseline PET/CT showed metabolic uptake on liver and/or spleen in 84% but did not match with lesion localizations on conventional imaging in 32%. M3 PET/CT showed no metabolic uptake in 13 (34%) patients, 11 still having pathological conventional imaging. Global response at M3 was observed in eight patients.
Conclusion: Baseline PET/CT does not replace conventional imaging for initial staging of CDC lesions but should be performed after 3 months of antifungal therapy.
Clinical trial registration: [www.clinicaltrials.gov], identifier [NCT01916057].
Introduction
Chronic disseminated candidiasis (CDC), often referred to as hepatosplenic candidiasis, is a rare disease occurring mostly in hematological malignancies with an incidence rate estimated at 1.53 per 100 patient-years (1, 2). Early and appropriate diagnosis and treatment of CDC are crucial, since anti-tumor chemotherapy or hematopoietic stem cell transplantation (HSCT) delay can negatively affect the underlying prognosis (3). Current IDSA Candida guidelines recommend for CDC a lipid formulation of amphotericin B or an echinocandin for several weeks followed by oral fluconazole in the case of azole-susceptible Candida isolate. Therapy should be protracted until lesions resolve on repeated imaging (4). It should at least last 8 weeks according to ESCMID guidelines (5). However, in a retrospective Taiwanese study 45.7% of CDC patients had residual liver and/or spleen abscesses on imaging at 6 months (2). Hence, prolonged treatments up to 3–6 months are frequent, leading to antifungal toxicity and cost increase (2, 6, 7). Finally, our group advocated that CDC belonged to the spectrum of fungal immune reconstitution inflammatory syndrome (IRIS), thereby raising questions on the tools most appropriate to evaluate the CDC-induced inflammatory reaction over time (8–10).
F18-fluorodeoxyglucose positron-emission tomography computed tomography (PET/CT) has shown a positive impact on reducing duration of antimicrobial therapy during febrile neutropenia in hematological patients (11). Lesions due to various fungi such as Aspergillus spp., Mucorales, Cryptococcus spp., Histoplasma spp., Coccidioides spp. are able to metabolize F18-fluorodeoxyglucose (12–15). Indeed, a preliminary study by our team has assessed PET/CT as a diagnostic tool for invasive fungal diseases (IFD), including CDC (16), its appropriateness being further documented by descriptive case reports or small case series uptake (17–21). PET/CT might therefore help to assess lesions at baseline and monitor antifungal treatment duration of CDC (9, 10). Through the largest prospective study on CDC ever performed (10), the aim was to determine whether the addition of PET/CT to conventional radiology added clinical value both at diagnosis and after 3 months of antifungal therapy.
Patients and materials and methods
Study design and population
CANHPARI was a multicenter pilot prospective interventional study designed to determine whether PET/CT is useful for treatment strategy for CDC. The study was registered on clinicaltrials.gov (NCT01916057) and approved by the ethic committee (CPP Ile de France 1, 2013-mai-13239).
Eligible patients met the following criteria: aged ≥ 18 years with a malignancy or HSCT, and profound, i.e., < 100 neutrophils/mm3, and prolonged, i.e., ≥ 10 days, neutropenia; and CDC defined by multiple abscesses in liver and/or spleen observed on abdominal CT or MRI (22). Exclusion criteria were described elsewhere (22). After file assessment by an independent committee, consisting in two infectious disease specialists, two hematologists, and two nuclear medicine specialists, patients were excluded if they had liver and/or lesions from an origin other than candidiasis. Since the definition of IFD changed long after the beginning of the study (23), CDC were categorized as proven, probable, or possible according to the previous 2008 EORTC/MSG criteria (22).
After providing written informed consent, all recruited patients benefited from PET/CT according to the European Association of Nuclear medicine guidelines within a week following inclusion and after 3 months of antifungal therapy (M3) (24). If PET/CT was performed for diagnosis before inclusion, no subsequent PET/CT was performed at baseline. Conventional imaging (CT or MRI) as part as routine follow-up was performed at diagnosis, M3, and M6. The follow-up was scheduled for 12 months.
Computed tomography (CT)-guided or ultrasonography-guided liver biopsy was performed at the physician’s discretion. Beta-1,3-D-glucans (BDG; Fungitell®, Beacon Diagnostics, East Falmouth, MA, USA) were considered present when one result was ≥ 80 pg/mL. Antifungal prophylaxis was considered if taken for at least 5 days, time corresponding of study state of most antifungal drugs.
Primary outcome measure
Global response at M3 was defined by a combined criterion, resolution of fever attributable to CDC and complete response to PET/CT. Criteria defining responses to therapy and study outcomes have been validated in interventional studies including therapeutic trials, therefore not applicable to the present study (10, 25). Consequently, clinical, biological and radiological criteria were adapted leading to the response definitions presented in Table 1. SUVs are not relevant in this study since PET/CT have been performed on different devices from different manufacturers, according to the high number of involved centers. To avoid this bias, we chose to perform a visual analysis to describe baseline PET/CT: any focal uptake above the uninvolved liver or splenic background activity was considered as a candidiasis lesion. Since there was no gold standard for PET/CT criteria to assess infectious complications, a complete response to PET/CT was defined by the visual disappearance of all target hypermetabolic lesions, according to PET Response Criteria in Solid Tumors (PERCIST) (26) (for more details see Supplementary Table 1). Global response at M3 was assessed by the independent committee. Each PET/CT was independently reviewed and analyzed by two experienced nuclear medicine physicians blinded to the patient’s history and any discrepancy was further resolved by consensus.
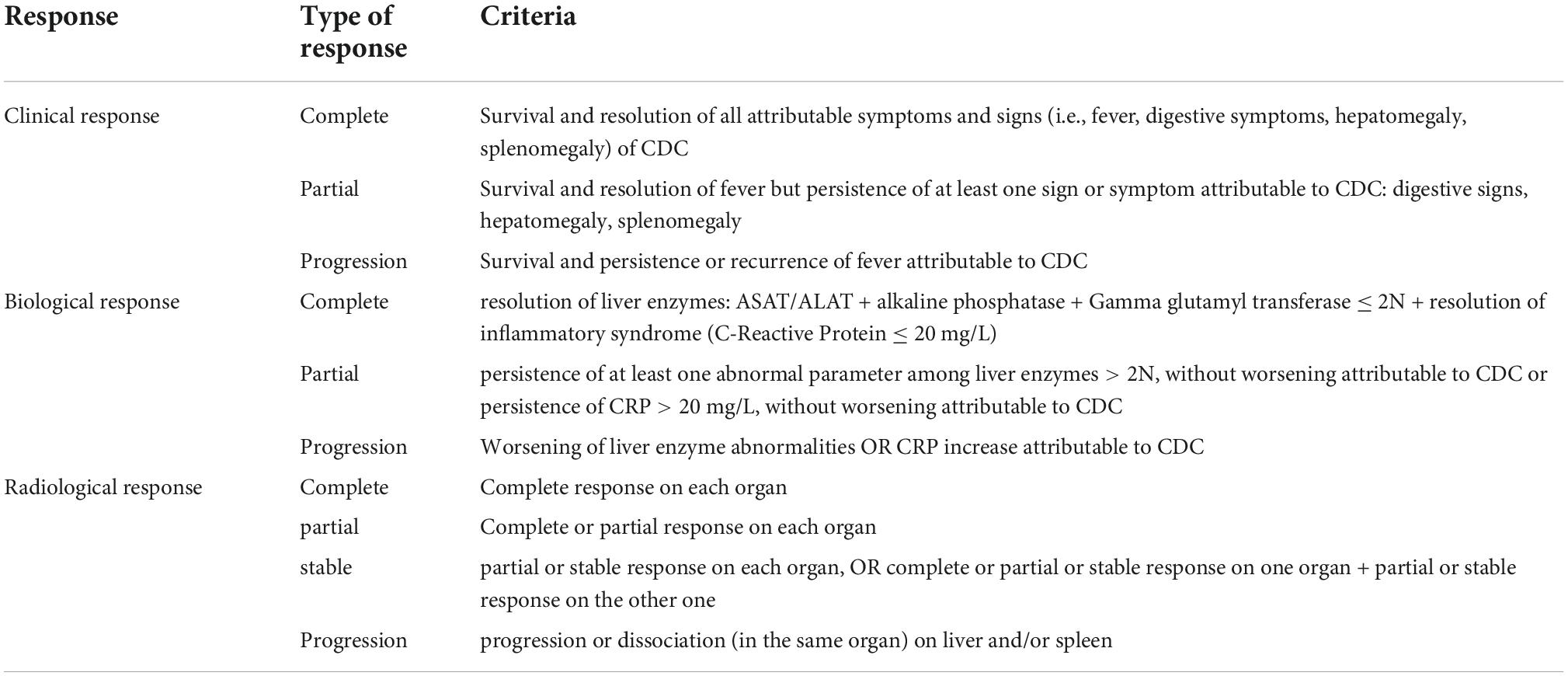
Table 1. Adapted criteria for chronic disseminated candidiasis (CDC) outcome.
Secondary outcome measure
Secondary outcome measure consists in comparison between responses to PET/CT and conventional imaging at diagnosis and M3. Responses to radiography were defined according to the Response Evaluation Criteria in Solid Tumors (RECIST1.1) (27) (for more details see Supplementary Table 2).
Statistical analysis
The original design required a total of 100 patients with CDC. Quantitative variables were described as mean ± standard deviation (SD) in the case of normal distribution or median and interquartile range [IQR 25-75] otherwise. Comparisons for continuous data were performed through Wilcoxon test and for categorical data through Fisher’s exact test.
Results
Population characteristics
Among 52 patients included between November 2013 and March 2017 in 23 French onco-hematology centers, 6 were secondarily excluded for alternative diagnosis and 2 for lack of available PET/CT at diagnosis. Among 44 analyzable patients, 43 had a hematological malignancy and one underwent autologous HSCT for solid cancer (Table 2). Most of the cases (27; 61.4%) were diagnosed during the induction phase. Other comorbidities are presented in Table 2. One case had had splenectomy. Corticosteroids were prescribed for 21 (47.7%) patients in the month prior to inclusion, included in the anti-tumor chemotherapy protocol for 17 patients. The mean cumulative dose of equivalent-prednisone corticosteroids was 1264 ± 843 mg. In the month preceding CDC diagnosis, an antifungal drug was prescribed for at least 5 days in 41 patients (93.2%), 16 patients receiving it as primary or secondary prophylaxis; 18 patients were still receiving an antifungal treatment at inclusion (see Supplementary Figure 1). Invasive pulmonary aspergillosis was previously diagnosed as probable in four cases and possible in three others.
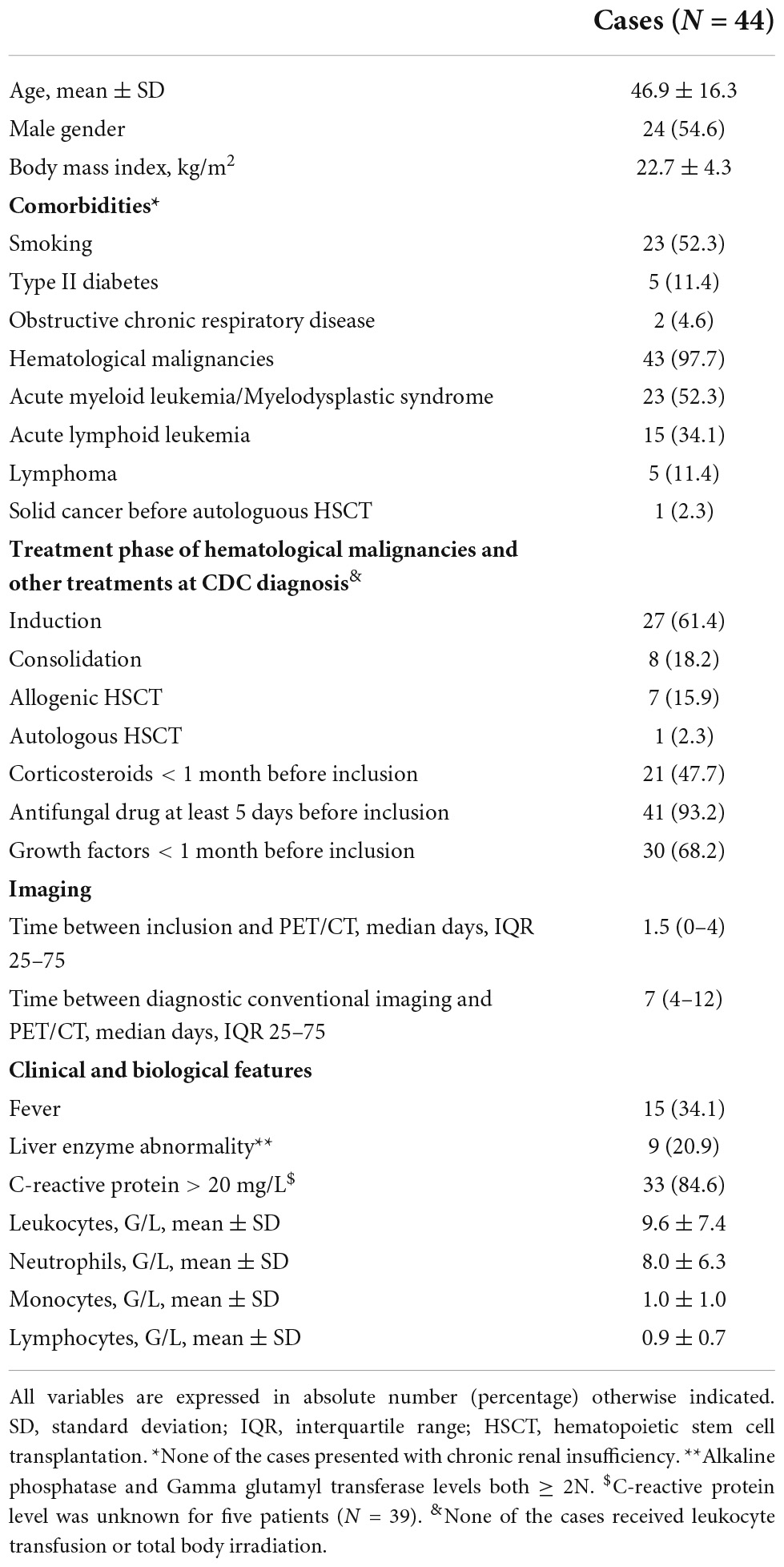
Table 2. Characteristics of 44 patients with chronic disseminated candidiasis (CDC) having a positron-emission tomography computed tomography (PET/CT) at inclusion.
The median duration of neutropenia before CDC diagnosis was 18 [14–24] days. The median time between CDC diagnosis by imaging and the previous period of neutropenia was 34 [24–41] days. Two (4.5%) patients were still neutropenic < 500/mm3 at diagnosis. Liver biopsy was performed in 13 patients in median 9 [6–12] days after CDC diagnosis; 21 (48%) patients received corticosteroids in the month before or at the time of biopsy. No granuloma or yeasts were observed. CDC was considered as probable in 20 patients on one positive BDG (n = 13) or recent candidemia (n = 7), and 24 patients had possible CDC without BDG.
Lesions were detected in liver and spleen in 29 (66%) patients, liver only in 11 (25%) patients and spleen only in 4 (9%) patients. Although the study protocol was not designed to screen for localizations other than liver and spleen, involvement of lungs and kidneys was detected in 11 and 6 patients, respectively. Antifungal treatment for CDC was ongoing at inclusion in 37 patients (84.1%). The 44 patients received antifungal drugs for CDC during the week following inclusion.
Baseline PET/CT and conventional imaging
Positron-emission tomography computed tomography (PET/CT) was performed in median 7 [4–12] days after diagnostic imaging, while the abdominal MRI (n = 4) or CT (n = 40) was performed in median 5.5 [2.3–10] days before inclusion. All the patients had PMN ≥ 500/mm3 at initial PET/CT [median 5,626/mm3 (3,240–11,270)], except two who had leucocytes less than 1,000/mm3. These two patients had positive PET/CT.
Positron-emission tomography computed tomography (PET/CT) showed metabolic uptake in liver and/or spleen at CDC diagnosis in 37 (84.1%) patients. In addition to hepatosplenic lesions, 4 patients had metabolic uptake in lungs; uptake in kidneys was not interpretable due to renal excretion of 18F-FDG. Among 37 positive PET/CT, metabolic uptake matched with lesion localizations on conventional imaging in 30 (68.2%) patients (Figure 1). For 7 patients, there were discrepancies between metabolic uptake and conventional imaging. There was a lack of detection of liver and spleen lesions in one and 5 patients, respectively, but detection was better for liver lesions in one patient.
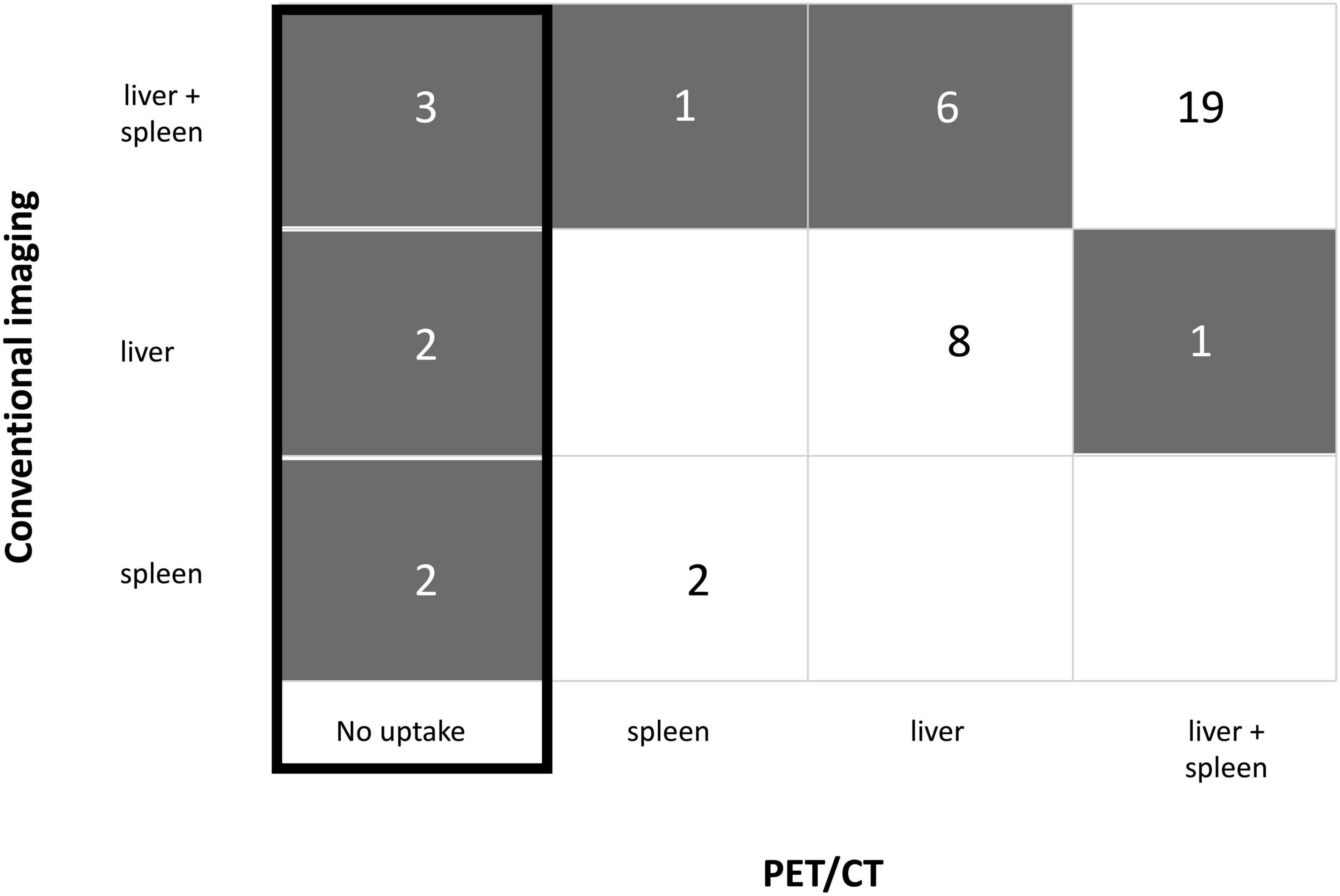
Figure 1. Discrepancies between baseline positron-emission tomography computed tomography (PET/CT) and conventional imaging regarding lesion localization. The number of patients is represented in each box. Gray color flags a discrepancy between PET/CT and conventional imaging.
Positron-emission tomography computed tomography (PET/CT) was negative in 7 patients for whom no metabolic uptake was detected, whereas conventional imaging showed lesions on liver and/or spleen (Figure 1). There was a trend toward a longer time to implementation for the 7 negative PET/CT [15(8–17.5) days] compared to the positive PET/CT [6(4–10) days; p = 0.079]: 3 negative PET/CT were performed in the first week following conventional imaging and 4 PET/CT were performed at 15, 15, 20, and 23 days, respectively (see Supplementary Table 3). Among the seven patients without initial metabolic uptake, 5 had probable, and 2 had possible CDC. They had median PMN at 4,300/mm3 [2,510–6,425]. None had severe neutropenia. Two patients received corticosteroids in the month before inclusion and 4 patients were diabetic. Glycemia was normal at the time of PET/CT for all patients. Taking into account the fact that some data were missing in both groups, C-reactive protein (CRP) was in median 31[20–130] mg/L in the negative PET/CT group, twice lower than CRP in the positive PET/CT group [78(39–159); p = 0.21], three patients having CRP ≤ 20 mg/L (see Supplementary Table 3).
Regarding the number of lesions in each organ, 27 patients had > 10 metabolic lesions on liver and/or spleen and had significantly more CRP > 100 mg/L than patients with ≤ 10 lesions (respectively 54.3% vs. 20.0%; p = 0.049). There were no other significant differences between patients who had > 10 lesions compared to those without (Table 3). Overall, the present data do not concur to perform systematically PET/CT in the setting of suspected CDC.
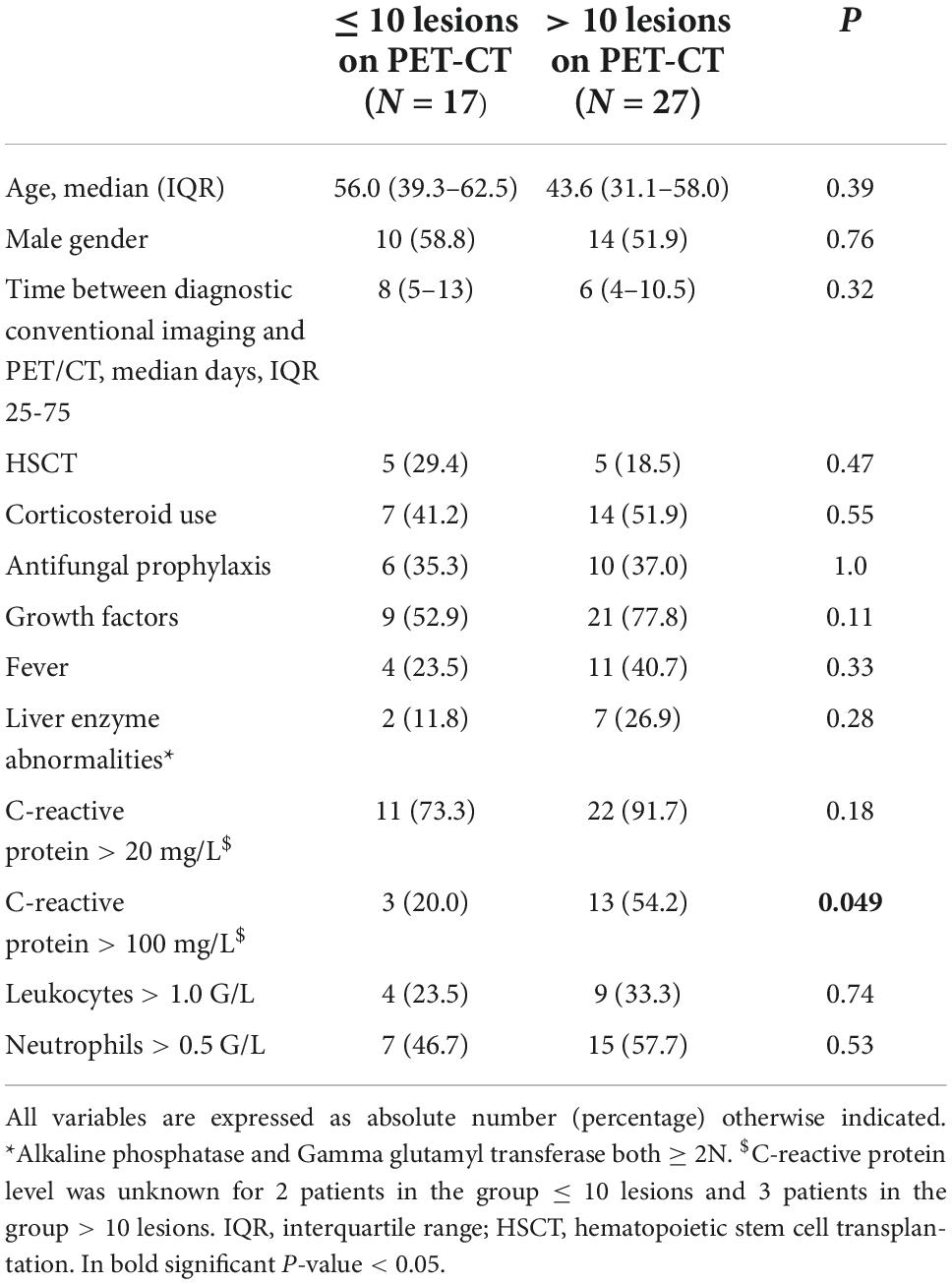
Table 3. Comparison of clinical and biological parameters in patients with > 10 lesions vs. ≤ 10 lesions on baseline positron-emission tomography computed tomography (PET-CT).
M3 PET/CT and conventional imaging
M3 PET/CT was performed in 38 patients (3 patients died before M3,3 PET/CT were missing among which 2 were negative at baseline). Figure 2 shows clinical, biological, and radiological responses according to PET/CT responses at M3.
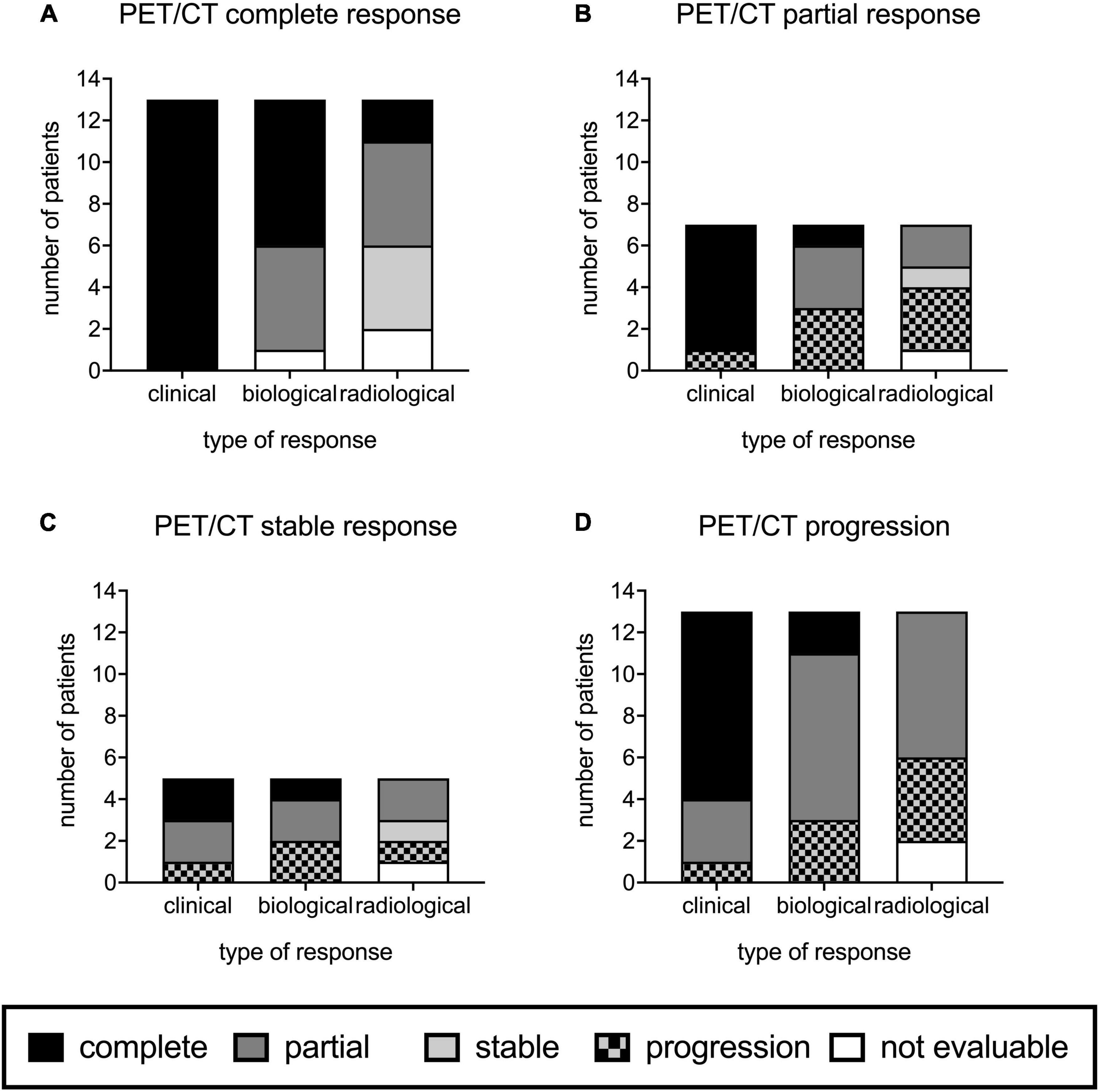
Figure 2. Positron-emission tomography computed tomography (PET/CT) responses at M3 compared to those of conventional imaging, clinical examination, and biology in 38 onco-hematology patients. M3 PET/CT showed complete response in 13 patients (A), partial response in 7 (B), stable response in 5 (C), and progression in 13 patients (D).
M3 PET/CT was normalized in 13 (34.2%) patients (Figure 2A). M3 PET/CT still showed metabolic uptake at M3 in 25 (65.8%) cases: 7 had a partial response (Figure 2B), 5 had stable lesions (Figure 2C), and 13 had worsening of their lesions (Figure 2D).
M3 conventional imaging was performed in 35 patients (3 patients died before M3,6 were missing). A complete response was observed in 3 (8.6%) patients, a partial response in 18 (51.4%), stabilization of the lesions in 6 (17.1%), and worsening of abnormalities in 8 (22.9%) patients.
Among the 13 patients with normalized M3 PET/CT, 11 had still pathological conventional imaging (Figure 2A). When M3 PET/CT showed metabolic uptake (n = 25), no or partial improvement of the lesions on conventional imaging was noted (Figures 2B–D).
Clinical and biological responses according to M3 PET/CT
Among the 13 patients with normalized M3 PET/CT, all had a complete clinical response and 7 had a complete biological response (Figure 2A). Corticosteroids were given for CDC treatment in 7/13 patients between inclusion and M3, and were still ongoing at M3 in 3 patients. Antifungal drugs were given less than 3 months in 5/13 patients; the median duration of treatment was 60 [50–63] days.
Among the 25 patients with persistent metabolic uptake on M3 PET/CT, a complete clinical response was observed in 17/25 (68.0%) and a complete biological response in 4 (16.0%) (Figures 2B–D). One patient had severe neutropenia < 500/mm3. A total of 12 patients received corticosteroids for CDC treatment and 2 received an antifungal treatment less than 3 months. PET/CT responses were not linked to hematological malignancy outcome since only one patient failed to respond to chemotherapy at M3.
Global response at M3
Global response at M3, i.e., apyrexia and complete response to M3 PET/CT, was observed in eight patients. Among them, a complete response was also found with conventional imaging and biology in 2 and 4 cases, respectively. Of note, 5 PET/CT performed at baseline had no metabolic uptake, and stayed identical at M3. The 5 patients had a complete clinical response.
There were no significant differences between patients who had a global response at M3 and the other patients evaluable at inclusion in terms of age, gender, hematological malignancies, corticosteroids use, antifungal prophylaxis, G-CSF use, fever, liver enzyme abnormalities, CRP, white blood cell count (Supplementary Table 4).
Evolution of radiography at M6 according to M3 PET/CT results
Among the 13 patients with normalized M3 PET/CT, 9 were evaluable for conventional imaging at M6: 5 kept an abnormal imaging and 4 had a no more lesions. Regarding the 17 patients who had persistent abnormalities on M3 PET/CT and were evaluable at M6, 12 (70.6%) still had lesions on conventional imaging.
Outcome
Among the 44 patients, 11 (25.0%) died during the study period, 3 in the first 3 months of follow-up, 2 between M3 and M6. None of the patients with complete response to PET/CT at M3 died during the monitoring. None of the deaths were attributable to CDC: 3 were due to other infectious causes and 8 to refractory hematological malignancy.
Regarding the impact of CDC on hematological malignancy, 10 patients had allogenic HSCT during the follow-up with a median time from CDC diagnosis of 138 [102–192] days. They still received an antifungal drug at the time of HSCT in 80% of the cases. Two of them died at 38 days and 286 days, both from refractory hematological malignancy. Subsequent antitumoral chemotherapy courses were delayed in 13 patients, with a median time of 17 [8–38] days. Among the eight patients who died due to refractory hematological malignancy, only one had had a delay in chemotherapy.
Discussion
This study is the first prospective multicentric study gathering clinical, biological, radiological and PET/CT data on a cohort of patients with CDC, now becoming as a rare disease. We did not meet our recruitment objectives, as the initial number of patients to be included in this study was 100. Changes in recommendations regarding antifungal prophylaxis in 2011 may have influenced the recruitment in our study (28). Nevertheless, data provided here allows us to get a better insight on CDC diagnosis and management.
At CDC diagnosis, discrepancies existed between conventional imaging and positive PET/CT. Indeed, PET/CT either increased sensitivity or could miss some lesions. Of note, CT was widely used in our study, although MRI is considered, at least by some authors, as the best conventional imaging to screen for hepatosplenic candidiasis lesions (29). Moreover, 16% of patients had no metabolic uptake on the initial PET/CT. PET/CT performed for infection screening can be falsely negative in the case of low inflammation due to previous prolonged anti-infectious therapy (30). In our study, 84.1% had had previous antifungal drugs before PET/CT, including the seven patients with negative baseline PET/CT, and all patients received antifungal treatment within a week following CDC diagnosis. Two other known factors that could influence 18F-FDG metabolic uptake are hyperglycemia and corticosteroid use. Diabetes mellitus did not seem to be associated with more negative PET/CT in the literature (31). By contrast, hyperglycemia did. Even if four patients in the negative PET/CT group were diabetic, all seven patients had normal glycemia at the time of PET/CT. Corticosteroids may attenuate 18F-FDG uptake in inflammatory diseases depending on treatment duration ≥ 10 days, but have a limited effect on PET/CT diagnostic accuracy (32–34). Corticosteroid were prescribed in 47.7% of our patients in the month prior to inclusion, including 2 patients with negative baseline PET/CT. Since the proportion of corticosteroid use was lower in the PET/CT negative group, corticosteroids were unlikely to have been responsible for attenuated metabolic uptake. Circulating neutrophils seemed not to influence positivity of PET/CT since all patients with negative PET/CT had full recovery of neutropenia and neutropenic patients had increased metabolic uptake. Activation of neutrophils is not always reflected by their expansion. Consequently, activated resident liver neutrophils could also play a role in increasing metabolic uptake. Low inflammatory state assessed by CRP may have led to negative PET/CT. For instance, CRP < 40 mg/L was a statistically significant predictor of negative PET/CT in suspicion of prosthetic valve endocarditis (30, 35). Our series of patients with negative PET/CT was a bit small to formally conclude whether low CRP influences metabolic uptake. However, a high CRP > 100 mg/L seemed to be associated with the presence of more lesions with metabolic uptake, and patients with negative PET/CT at baseline had lower CRP than those with positive PET/CT. PET/CT is known to have poor sensitivity for small lesions such as hepatic metastasis less than 1 cm due to a lack of resolution, which can result in false negative results (36). Criteria of inclusion in our study were based on small abscesses < 1 cm on liver and/or spleen, and were checked at inclusion. Finally, the interval between initial CDC diagnosis and PET/CT may have increased the number of negative PET/CT. There was a trend toward a longer interval between negative PET/CT and initial diagnostic imaging with a PET/CT performed in median 9 days after conventional imaging. However, a delayed PET/CT has had no impact for diagnosis of other infections such as vertebral osteomyelitis (37).
Our findings suggest that PET/CT is useful for follow-up at 3 months. Only 25% of patients with complete M3 PET/CT and clinical responses had concordant conventional imaging. In addition, liver enzyme abnormalities and inflammatory syndrome could last for months.
Dissociation between conventional imaging, clinical, and biological responses in CDC led to issues when applying criteria defining responses to therapy and study outcomes in clinical trials for IFD (25). Success was defined by complete or partial responses with radiological resolution or significant improvement or stabilization. Other studies have heterogenous combined criteria for success and failure. For instance, Kauffman et al. defined failure as persistent fever, persistence or worsening of liver lesions on CT and persisting or progressing clinical symptoms (38). Anaissie et al. added to these criteria persistence or progression of biochemical parameters (39). Finally, failure criteria in the Cornely et al. study were open to interpretation since they had been defined as unresponsive or progressing infection (40). Since responses in CDC patients could be dissociated, the response criteria chosen in this study were divided into four categories instead of success/failure, i.e., clinical, biological, radiological, PET/CT responses. New criteria to assess CDC response to treatment should be implemented to consider dissociated responses without impact on CDC prognosis.
Conventional imaging, mainly represented by abdominal CT in this study, showed long-term persistent liver and/or splenic lesions, more than 6 months for some patients, whereas clinical symptoms resolved at M3 for 75.8% of the patients. Persistent lesions on conventional imaging may encourage clinicians to continue antifungal treatment more than 3 months; as was the case for 82.9% of the patients in our study. This result is consistent with other retrospective studies with median duration of antifungal drug ranging from 96 to 210 days (2, 6, 7, 41). The recommended treatment duration in IDSA guidelines for CDC is to continue until lesions resolve on repeated imaging, which usually takes several months (4). The main reason for long-term antifungal treatment was mainly the risk of “relapse” if the treatment was withdrawn too early. Growing evidence for IRIS may explain “inflammatory rebounds” independently of fungal persistence, occurring in more than 15% of our patients. Our team has recently demonstrated that expansion of Candida-specific IFNγ-producing T cells together with features of T-cell activation and systemic inflammation supported IRIS in patients with CDC (10). Consequently, corticosteroids are more and more widely used to treat IRIS-related CDC symptoms after the initial fungal disease (6, 8, 42–44). In addition, lesions due to IRIS have shown a high metabolic uptake on PET/CT in HIV patients, possibly due to increased Glut-1 expression on T cells and monocytes (45). In this context, response to treatment in patients without symptoms of CDC at 3 months should be evaluated with PET/CT, and not CT.
Positron-emission tomography computed tomography (PET/CT) could be used to stop antifungal treatment at M3 in various IFD (46, 47). A few case reports and one retrospective study on 25 children showed the feasibility of antifungal treatment discontinuation in CDC patients using PET/CT (21, 41).
Although no death was attributable directly to CDC, chemotherapy for hematological malignancy was delayed in 20.4% of the patients. However, delayed chemotherapy could have an impact on cancer prognosis. In a recent study on 29 CDC in 639 acute myeloid leukemia patients, the long-term probability for survival was higher in CDC patients than in CDC-free patients (3). Allograft was performed despite CDC with no significant difference on overall survival between CDC and CDC-free patients. Similar conclusions arose from an older publication underlying the necessity to continue chemotherapy while treating CDC (48).
Our study had some limitations. Although it was the largest series of CDC patients, the number of patients remained small, showing scarcity of the disease. It was not surprising that half of the patients had possible CDC. CDC belonging to IRIS spectrum, mycological investigations were often performed too late compared to the initial fungal triggering event, which was most of the time undocumented during neutropenia. In our population, CDC diagnosis was performed in median more than a month after the initial neutropenic period and only 16% of the patients had initial candidemia. The now widely use of antifungal prophylaxis could have explained the longer time to diagnosis compared to ancient series (49). Even if our population had various hematological malignancies, the common point for CDC occurrence was the profound and prolonged neutropenia mainly due to intensive chemotherapy. Heterogenous time between conventional imaging and baseline PET/CT could have overrated the discrepancies.
To conclude, owing to discrepancies with conventional imaging, further studies are needed to use PET/CT for initial staging of CDC lesions. In contrast, PET/CT add clinical value in the follow-up of CDC patients. We recommend to perform a PET/CT at M3 to assess antifungal treatment response. Its usefulness for earlier, but safe, antifungal treatment discontinuation should be evaluated in further prospective studies. Whether or not PET/CT is useful before M3 is to be demonstrated.
Data availability statement
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by CPP Ile de France 1, 2013-mai-13239. The patients/participants provided their written informed consent to participate in this study.
Author contributions
BR and OL contributed to the conception and design of the work. CM, J-MC, SC, FM, and PrB contributed to the acquisition of the data. CE, TR, OL, and BR analyzed the data. CM, FM, SA, PiB, M-TR, TB, BR, and OL contributed to the interpretation of the data. BR, CM, CE, FM, and OL drafted the manuscript. All authors read and approved the final version of the manuscript.
Funding
This work was supported by the French Ministry of Health (PHRC AOM12047).
Acknowledgments
The authors thank Jeffrey Arsham for editing the manuscript and the Canhpari Study Group Members, first all participating clinicians who recruited patients in the study: Fanny Lanternier (Hôpital Necker-Enfants Malades -APHP, Paris), Felipe Suarez (Hôpital Necker-Enfants Malades-APHP, Paris), Emmanuel Raffoux (Hôpital Saint-Louis-APHP, Paris), Jean-Pierre Marolleau (CHU Amiens), Aline Schmidt (CHU Angers), Ana Berceanu (CHU Besançon), Arnaud Pigneux (CHU Bordeaux), Sylvain Chantepie (CHU La Côte de Nacre–Caen), Johanna Konopacki (Hôpital militaire de Percy–Clamart), Cécile Chabrot (CHU Clermont-Ferrand), Anne Thiebaut-Bertrand (CHU Albert Michalon–Grenoble), Pascal Turlure (CHU Limoges), Michallet Mauricette (Hôpital Edouard Herriot–Hospices civils de Lyon), PiB (Institut Paoli-Calmettes–Marseille), Thomas Gastinne (CHU Nantes), TB (CHU Avicenne–APHP, Bobigny), Madalina Uzunov (Hôpital Pitié-Salpêtriére–APHP, Paris), Lise Willems (Hôpital Cochin–APHP, Paris), Françoise Isnard (Hôpital St Antoine–Paris), Natacha Maillard, José Miguel Torregrosa Diaz, Maria-Pilar Gallego Hernanz, Mathieu Puyade (CHU Poitiers), SA (CH Tourcoing), Valérie Coiteux (CHRU Lille), Raoul Herbrecht (Hôpital de Hautepierre-CHRU Strasbourg), Juliette Lambert (CH Versailles), Fanny Lanternier-Dessap (Hôpital Necker-Enfants Malades–APHP, Paris), Patrick Ceballos (Hôpital Saint-Eloi-CHRU Montpellier), Catherine Lechiche (Hôpital Carémeau-CHU Nîmes); second all the mycologists from the participating centers: Marie-Elisabeth Bougnoux (Hôpital Necker-Enfants Malades-APHP, Paris), Alexandre Alanio (Hôpital Saint-Louis-APHP, Paris), Tayeb Chouaki (CHU Amiens), Jean-Philippe Bouchara (CHU Angers), Laurence Millon (CHU Besançon), Laurence Delhaes (CHU Bordeaux), Julie Bonhomme (CHU La Côte de Nacre–Caen), Charles Soler (Hôpital militaire de Percy–Clamart), Philippe Poirier (CHU Clermont-Ferrand), Danièle Maubon (CHU Albert Michalon–Grenoble), Marie-Fleur Durieux (CHU Limoges), Damien Dupont (Hôpital Edouard Herriot–Hospices civils de Lyon), Stéphane Ranque (IHU Méditerranée–Marseille), Florent Morio (CHU Nantes), Sophie Brun (CHU Avicenne–APHP, Bobigny), Arnaud Fekkar (Hôpital Pitié-Salpêtriére–APHP, Paris), André Paugam (Hôpital Cochin–APHP, Paris), Christophe Hennequin (Hôpital St Antoine–Paris), Estelle Peyraud (CHU Poitiers), Boualem Sendid (CHRU Lille), Valérie Letscher (Hôpital de Hautepierre-CHRU Strasbourg), Odile Eloy (CH Versailles), Philippe Rispail (Hôpital Saint-Eloi-CHRU Montpellier), and Miléne Sasso (Hôpital Carémeau-CHU Nîmes). The authors are thankful to the CANHPARI scientific committee (Felipe Suarez, Emmanuel Raffoux, Nathalie de Castro, Marie-Elisabeth Bougnoux, Grégory Jouvion, CM, Boualem Sendid, J-MC, and Pierre-Yves Bochud), the CANHPARI adjudication committee M-TR, TB, SA, PiB, FM, CM, and J-MC, as well as the clinical research unit (URC) of Hôpital Necker-Enfants Malades (CE, PrB, Thouraya Saadoun Bensefta, Sandrine Albert, Kelly Cheung, Fawzia Aissat, Meriem Imarazene, Liza Belkessam, Laetitia Desjardins, Claire Mathely, Anne-Marine Lenzotti, Fabrice Gourmelon, and Rabeony Tioka). The authors are also grateful to the radiologists who independently reviewed conventional imaging: Sarah Sillou, Jonathan Dbjay, Jean-Baptiste Quere (Hôpital Necker-Enfants Malades–APHP, Paris).
Conflict of interest
BR has travel grants from Pfizer and MSD, speaker’s fees from MSD, Gilead, Astellas, and Iqone. SA has travel grants from MSD and Gilead, and speaker’s fee from Gilead. PiB has travel grants from Astellas, Pfizer, MSD, and Gilead, and speaker’s fee from MSD. OL speaker’s fees from MSD, Gilead, Astellas, Pfizer, and F2G, consultant Gilead.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.1026067/full#supplementary-material
References
1. Rammaert B, Desjardins A, Lortholary O. New insights into hepatosplenic candidosis, a manifestation of chronic disseminated candidosis. Mycoses. (2012) 55:e74–84. doi: 10.1111/j.1439-0507.2012.02182.x
2. Chen C-Y, Cheng A, Tien F-M, Lee PC, Tien HF, Sheng WH, et al. Chronic disseminated candidiasis manifesting as hepatosplenic abscesses among patients with hematological malignancies. BMC Infect Dis. (2019) 19:635. doi: 10.1186/s12879-019-4260-4
3. Grateau A, Le Maréchal M, Labussière-Wallet H, Ducastelle-Leprêtre S, Nicolini FE, Thomas X, et al. Chronic disseminated candidiasis and acute leukemia: impact on survival and hematopoietic stem cell transplantation agenda. Med Mal Infect. (2018) 48:202–6. doi: 10.1016/j.medmal.2017.12.004
4. Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the infectious diseases society of America. Clin Infect Dis. (2016) 62:e1–50.
5. Ullmann AJ, Akova M, Herbrecht R, Viscoli C, Arendrup MC, Arikan-Akdagli S, et al. ESCMID* guideline for the diagnosis and management of Candida diseases 2012: adults with haematological malignancies and after haematopoietic stem cell transplantation (HCT). Clin Microbiol Infect. (2012) 18(Suppl 7):53–67. doi: 10.1111/1469-0691.12041
6. Jang Y-R, Kim M-C, Kim T, Chong YP, Lee SO, Choi SH, et al. Clinical characteristics and outcomes of patients with chronic disseminated candidiasis who need adjuvant corticosteroid therapy. Med Mycol. (2018) 56:782–6. doi: 10.1093/mmy/myx110
7. De Castro N, Mazoyer E, Porcher R, Raffoux E, Suarez F, Ribaud P, et al. Hepatosplenic candidiasis in the era of new antifungal drugs: a study in Paris 2000-2007. Clin Microbiol Infect. (2012) 18:E185–7. doi: 10.1111/j.1469-0691.2012.03819.x
8. Legrand F, Lecuit M, Dupont B, Bellaton E, Huerre M, Rohrlich PS, et al. Adjuvant corticosteroid therapy for chronic disseminated candidiasis. Clin Infect Dis. (2008) 46:696–702.
9. Dellière S, Guery R, Candon S, Rammaert B, Aguilar C, Lanternier F, et al. Understanding pathogenesis and care challenges of immune reconstitution inflammatory syndrome in fungal infections. J Fungi. (2018) 4:E139.
10. Candon S, Rammaert B, Foray AP, Moreira B, Gallego Hernanz MP, Chatenoud L, et al. Chronic disseminated candidiasis during hematological malignancies: an immune reconstitution inflammatory syndrome with expansion of pathogen-specific T helper type 1 cells. J Infect Dis. (2020) 221:1907–16. doi: 10.1093/infdis/jiz688
11. Koh KC, Slavin MA, Thursky KA, Lau E, Hicks RJ, Drummond E, et al. Impact of fluorine-18 fluorodeoxyglucose positron emission tomography on diagnosis and antimicrobial utilization in patients with high-risk febrile neutropenia. Leuk Lymphoma. (2012) 53:1889–95. doi: 10.3109/10428194.2012.677533
12. Chamilos G, Macapinlac HA, Kontoyiannis DP. The use of 18F-fluorodeoxyglucose positron emission tomography for the diagnosis and management of invasive mould infections. Med Mycol. (2008) 46: 23–9.
13. Wang S-Y, Chen G, Luo D-L, Shao D, Liu ET, Sun T, et al. 18F-FDG PET/CT and contrast-enhanced CT findings of pulmonary cryptococcosis. Eur J Radiol. (2017) 89:140–8. doi: 10.1016/j.ejrad.2017.02.008
14. Mohan M, Fogel B, Eluvathingal T, Schinke C, Kothari A. Gastrointestinal histoplasmosis in a patient after autologous stem cell transplant for multiple myeloma. Transpl Infect Dis. (2016) 18:939–41. doi: 10.1111/tid.12619
15. Reyes N, Onadeko OO, Luraschi-Monjagatta MDC, Knox KS, Rennels MA, Walsh TK, et al. Positron emission tomography in the evaluation of pulmonary nodules among patients living in a coccidioidal endemic region. Lung. (2014) 192:589–93. doi: 10.1007/s00408-014-9589-2
16. Hot A, Maunoury C, Poiree S, Lanternier F, Viard JP, Loulergue P, et al. Diagnostic contribution of positron emission tomography with [18F]fluorodeoxyglucose for invasive fungal infections. Clin Microbiol Infect. (2011) 17:409–17.
17. Rammaert B, Candon S, Maunoury C, Bougnoux ME, Jouvion G, Braun T, et al. Thalidomide for steroid-dependent chronic disseminated candidiasis after stem cell transplantation: a case report. Transpl Infect Dis. (2017) 19:e12637. doi: 10.1111/tid.12637
18. Teyton P, Baillet G, Hindié E, Filmont JE, Sarandi F, Toubert ME, et al. Hepatosplenic candidiasis imaged with F-18 FDG PET/CT. Clin Nucl Med. (2009) 34:439–40. doi: 10.1097/RLU.0b013e3181a7cfba
19. Jennane S, Eddou H, Mahtat E-M, Konopacki J, Souleau B, Malfuson JV, et al. [Contribution of PET/CT for the management of hepatosplenic candidiasis in hematology]. Med Mal Infect. (2014) 44:281–3.
20. Albano D, Bosio G, Bertoli M, Petrilli G, Bertagna F. Hepatosplenic candidiasis detected by (18)F-FDG-PET/CT. Asia Ocean J Nucl Med Biol. (2016) 4:106–8. doi: 10.7508/aojnmb.2016.02.007
21. Xu B, Shi P, Wu H, Guo X, Wang Q, Zhou S. Utility of FDG PET/CT in guiding antifungal therapy in acute leukemia patients with chronic disseminated candidiasis. Clin Nucl Med. (2010) 35:567–70. doi: 10.1097/RLU.0b013e3181e4db84
22. De Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE, Calandra T, et al. Revised definitions of invasive fungal disease from the European organization for research and treatment of cancer/invasive fungal infections cooperative group and the national institute of allergy and infectious diseases mycoses study group (EORTC/MSG) consensus group. Clin Infect Dis. (2008) 46:1813–21. doi: 10.1086/588660
23. Donnelly JP, Chen SC, Kauffman CA, Steinbach WJ, Baddley JW, Verweij PE, et al. Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin Infect Dis. (2020) 71:1367–76. doi: 10.1093/cid/ciz1008
24. Boellaard R, Delgado-Bolton R, Oyen WJG, Giammarile F, Tatsch K, Eschner W, et al. /CT: EANM procedure guidelines for tumour imaging: version 2.0. Eur J Nucl Med Mol Imaging. (2015) 42:328–54.
25. Segal BH, Herbrecht R, Stevens DA, Ostrosky-Zeichner L, Sobel J, Viscoli C, et al. Defining responses to therapy and study outcomes in clinical trials of invasive fungal diseases: mycoses study group and european organization for research and treatment of cancer consensus criteria. Clin Infect Dis. (2008) 47:674–83. doi: 10.1086/590566
26. Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST to PERCIST: evolving considerations for PET response criteria in solid tumors. J Nucl Med. (2009) 50(Suppl 1):122S–50S. doi: 10.2967/jnumed.108.057307
27. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. (2009) 45:228–47.
28. Maertens J, Marchetti O, Herbrecht R, Cornely OA, Flückiger U, Frêre P, et al. European guidelines for antifungal management in leukemia and hematopoietic stem cell transplant recipients: summary of the ECIL 3–2009 update. Bone Marrow Transplant. (2011) 46:709–18. doi: 10.1038/bmt.2010.175
29. Anttila VJ, Lamminen AE, Bondestam S, Korhola O, Färkkilä M, Sivonen A, et al. Magnetic resonance imaging is superior to computed tomography and ultrasonography in imaging infectious liver foci in acute leukaemia. Eur J Haematol. (1996) 56:82–7. doi: 10.1111/j.1600-0609.1996.tb00300.x
30. Swart LE, Gomes A, Scholtens AM, Sinha B, Tanis W, Lam MGEH, et al. Improving the diagnostic performance of 18F-fluorodeoxyglucose positron-emission tomography/computed tomography in prosthetic heart valve endocarditis. Circulation. (2018) 138:1412–27.
31. Rabkin Z, Israel O, Keidar Z. Do hyperglycemia and diabetes affect the incidence of false-negative 18F-FDG PET/CT studies in patients evaluated for infection or inflammation and cancer? A Comparative analysis. J Nucl Med. (2010) 51:1015–20. doi: 10.2967/jnumed.109.074294
32. Nielsen BD, Gormsen LC, Hansen IT, Keller KK, Therkildsen P, Hauge E-M. Three days of high-dose glucocorticoid treatment attenuates large-vessel 18F-FDG uptake in large-vessel giant cell arteritis but with a limited impact on diagnostic accuracy. Eur J Nucl Med Mol Imaging. (2018) 45:1119–28. doi: 10.1007/s00259-018-4021-4
33. Fuchs M, Briel M, Daikeler T, Walker UA, Rasch H, Berg S, et al. The impact of 18F-FDG PET on the management of patients with suspected large vessel vasculitis. Eur J Nucl Med Mol Imaging. (2012) 39:344–53. doi: 10.1007/s00259-011-1967-x
34. Hay B, Mariano-Goulart D, Bourdon A, Benkiran M, Vauchot F, De Verbizier D, et al. Diagnostic performance of 18F-FDG PET-CT for large vessel involvement assessment in patients with suspected giant cell arteritis and negative temporal artery biopsy. Ann Nucl Med. (2019) 33:512–20. doi: 10.1007/s12149-019-01358-5
35. San S, Ravis E, Tessonier L, Philip M, Cammilleri S, Lavagna F, et al. Prognostic value of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in infective endocarditis. J Am Coll Cardiol. (2019) 74:1031–40.
36. Sivesgaard K, Larsen LP, Sørensen M, Kramer S, Schlander S, Amanavicius N, et al. Diagnostic accuracy of CE-CT, MRI and FDG PET/CT for detecting colorectal cancer liver metastases in patients considered eligible for hepatic resection and/or local ablation. Eur Radiol. (2018) 28:4735–47.
37. Smids C, Kouijzer IJE, Vos FJ, Sprong T, Hosman AJ, de Rooy JW, et al. A comparison of the diagnostic value of MRI and 18F-FDG-PET/CT in suspected spondylodiscitis. Infection. (2017) 45:41–9.
38. Kauffman CA, Bradley SF, Ross SC, Weber DR. Hepatosplenic candidiasis: successful treatment with fluconazole. Am J Med. (1991) 91:137–41.
39. Anaissie E, Bodey GP, Kantarjian H, David C, Barnett K, Bow E, et al. Fluconazole therapy for chronic disseminated candidiasis in patients with leukemia and prior amphotericin B therapy. Am J Med. (1991) 91:142–50. doi: 10.1016/0002-9343(91)90006-j
40. Cornely OA, Lasso M, Betts R, Klimko N, Vazquez J, Dobb G, et al. Caspofungin for the treatment of less common forms of invasive candidiasis. J Antimicrob Chemother. (2007) 60:363–9.
41. Madney Y, Shalaby L, Elanany M, Adel N, Nasr E, Alsheshtawi K, et al. Clinical features and outcome of hepatosplenic fungal infections in children with haematological malignancies. Mycoses. (2020) 63:30–7. doi: 10.1111/myc.13002
42. Shkalim-Zemer V, Levi I, Fischer S, Tamary H, Yakobovich J, Avrahami G, et al. Response of symptomatic persistent chronic disseminated candidiasis to corticosteroid therapy in immunosuppressed pediatric patients: case study and review of the literature. Pediatr Infect Dis J. (2018) 37:686–90. doi: 10.1097/INF.0000000000001844
43. Fox TA, Halsey R, Pomplun S, Gant V, Grandage V, Mansour MR, et al. Rapid clinical response to adjuvant corticosteroids in chronic disseminated candidiasis complicated by granulomas and persistent fever in acute leukemia patients. Leuk Lymphoma. (2020) 61:944–9. doi: 10.1080/10428194.2019.1691198
44. Chaussade H, Bastides F, Lissandre S, Blouin P, Bailly E, Chandenier J, et al. Usefulness of corticosteroid therapy during chronic disseminated candidiasis: case reports and literature review. J Antimicrob Chemother. (2012) 67:1493–5. doi: 10.1093/jac/dks044
45. Hammoud DA, Boulougoura A, Papadakis GZ, Wang J, Dodd LE, Rupert A, et al. Increased metabolic activity on 18F-fluorodeoxyglucose positron emission tomography-computed tomography in human immunodeficiency virus-associated immune reconstitution inflammatory syndrome. Clin Infect Dis. (2018) 68:229–38. doi: 10.1093/cid/ciy454
46. Ankrah AO, Span LFR, Klein HC, de Jong PA, Dierckx RAJO, Kwee TC, et al. Role of FDG PET/CT in monitoring treatment response in patients with invasive fungal infections. Eur J Nucl Med Mol Imaging. (2019) 46:174–83.
47. Leroy-Freschini B, Treglia G, Argemi X, Bund C, Kessler R, Herbrecht R, et al. 18F-FDG PET/CT for invasive fungal infection in immunocompromised patients. QJM. (2018) 111:613–22.
48. Walsh TJ, Whitcomb PO, Revankar SG, Pizzo PA. Successful treatment of hepatosplenic candidiasis through repeated cycles of chemotherapy and neutropenia. Cancer. (1995) 76:2357–62. doi: 10.1002/1097-0142(19951201)76:11<2357::aid-cncr2820761126>3.0.co;2-h
Keywords: invasive fungal disease, Candida, candidiasis, hematological malignancy, immune reconstitution inflammatory syndrome, acute leukemia, hematopoietic stem cell transplantation
Citation: Rammaert B, Maunoury C, Rabeony T, Correas J-M, Elie C, Alfandari S, Berger P, Rubio M-T, Braun T, Bakouboula P, Candon S, Montravers F and Lortholary O (2022) Does 18F-FDG PET/CT add value to conventional imaging in clinical assessment of chronic disseminated candidiasis? Front. Med. 9:1026067. doi: 10.3389/fmed.2022.1026067
Received: 23 August 2022; Accepted: 28 November 2022;
Published: 20 December 2022.
Edited by:
Carlo Tascini, University of Udine, ItalyReviewed by:
Anna Candoni, Ospedale Santa Maria della Misericordia di Udine, ItalyAlfred Ankrah, Korle Bu Teaching Hospital, Ghana
Copyright © 2022 Rammaert, Maunoury, Rabeony, Correas, Elie, Alfandari, Berger, Rubio, Braun, Bakouboula, Candon, Montravers and Lortholary. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Blandine Rammaert, YmxhbmRpbmUucmFtbWFlcnQucGFsdHJpZUB1bml2LXBvaXRpZXJzLmZy
†Present Address: Blandine Rammaert, Faculté de Médecine et Pharmacie, Université de Poitiers, Poitiers, France; CHU Poitiers, Service de Maladies Infectieuses et Tropicales, Poitiers, France; INSERM U1070, Poitiers, France
‡These authors have contributed equally to this work