 Ping Xiao
Ping Xiao Tao Guo
Tao Guo Rutie Yin
Rutie Yin
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 02 November 2022
Sec. Obstetrics and Gynecology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.1018573
Background: Gestational trophoblastic neoplasia is an uncommon disease, whose clinical manifestations are similar to ectopic pregnancy, thus some rare pelvic lesion can be misdiagnosed as ectopic pregnancy.
Aims: This study was presented to investigate the characteristics of gestational trophoblastic neoplasia misdiagnosed as ectopic pregnancy and reduce the misdiagnosis.
Methods: The clinicopathological data for 14 cases of gestational trophoblastic neoplasia misdiagnosed as ectopic pregnancy at West China Second Hospital Sichuan University from January 2006 to December 2020 were retrospectively analyzed.
Results: The main clinical manifestations were amenorrhea, abnormal vaginal bleeding, and abdominal pain. At initial diagnosis, the serum hCG level was >10,000 mIU/mL in 5 patients and <10,000 mIU/mL in 7 patients, and a positive urine pregnancy test alone was found in 2 patients. Vaginal ultrasonography showed no abnormalities in 7 cases, adnexal mass in 5 cases, and tubal thickening in 2 cases. The patient's previous pregnancy was an abortion in 7 cases, full-term in 4 cases, and a hydatidiform mole in 3 cases. Clinical stage: 3 cases were stage I, 3 were stage II, 7 were stage III, and 1 case was stage IV (liver and spleen metastases). The median FIGO prognostic score was 13.5 points (12–21 points), with 9 cases having a score >13 points (very high risk). From 14 patients, only 3 had molar pregnancy previously. Only 3 patients had no metastasis at GTN diagnosis (from these 3, only one after molar pregnancy). After chemotherapy alone or in combination with surgery, all patients survived, with a median follow-up of 84 months (23–102 months).
Conclusion: If we have positive hCG, without a sonographic topic gestation confirmation, associated with metastatic lesions, the GTN diagnosis should be considered instead of ectopic pregnancy, if the patient have had a pregnancy once during her life.
Gestational trophoblastic disease (GTD) is a group of diseases caused by the abnormal proliferation of trophoblast cells in the placenta, which include benign mole and malignant trophoblast diseases. According to the WHO (5th Edition, 2020) pathological classification of the female reproductive system (1), GTD can be histologically divided into: (1) gestational trophoblastic neoplasia (GTN), including choriocarcinoma, placental site trophoblastic tumors (PSTT), epithelioid trophoblastic tumors (ETT), and mixed trophoblastic tumors; (2) hydatidiform mole pregnancy, including complete, partial, and invasive/metastatic hydatidiform mole; (3) tumor-like lesions (arterial-like lesions), including abnormal placental reactions and placental nodules/plaques; and (4) abnormal (non-hydatidiform mole) villous lesions. GTN can be secondary to any type of pregnancy, but has a low incidence ranging from 1–3/1,000 pregnancies for hydatidiform mole to (1–9)/40,000 pregnancies for choriocarcinoma (2).
The clinical manifestations of GTN include amenorrhea, abnormal vaginal bleeding, and elevated levels of serum human chorionic gonadotropin (hCG) in most patients, and these are also common clinical features in ectopic pregnancy. As only about 50% of GTN follows molar pregnancy, the rest can occur after an abortion, ectopic pregnancy, or a term pregnancy. Aside from abnormal vaginal bleeding, other clinical presentations may include bleeding from metastatic sites such as the lung, or brain, liver, spleen, intestines (3).
The incidence of ectopic pregnancy (EP) is ~1–2% (4). In particular, GTN patients with extrauterine lesions are more likely to be misdiagnosed with ectopic pregnancy. GTN is mainly treated with chemotherapy, while EP is treated with surgery or drug therapy, and misdiagnosis will lead to an incorrect treatment strategy for patients. The present paper reviews the clinicopathological data for GTN patients admitted to our hospital over the past 15 years, analyzes the clinical characteristics of patients misdiagnosed with EP, reviews the literature, and discusses the causes of misdiagnosis, with a view to facilitating correct clinical diagnosis and reducing misdiagnosis.
Clinicopathological data for GTN patients misdiagnosed with ectopic pregnancy, who were admitted to the West China Second Hospital of Sichuan University from January 2006 to December 2020, were collected. These included age, clinical manifestations, main treatment course after misdiagnosis, previous pregnancy type prior to the diagnosis of GTN, time since the previous pregnancy, serum hCG levels before treatment, International Federation of Obstetrics and Gynecology (FIGO) prognosis score and stage (2000), treatment, and prognosis were summarized and analyzed to elucidate the causes of misdiagnosis and suggest preventive measures.
Due to the small sample size, the distribution of continuous variables is described as the median and range. The present study was approved by the Ethics Committee of the West China Second Hospital of Sichuan University. Informed consent was obtained from all patients.
From January 2006 to December 2020, a total of 611 patients with GTN were admitted to our hospital, among which 14 (2.29%) were misdiagnosed as ectopic pregnancy. Thirteen cases were misdiagnosed at other hospitals and 1 case was misdiagnosed at our hospital. The median age of patients in this group was 32 years old (range: 21–49 years old). Ten patients were suffering from amenorrhea, with or without vaginal bleeding and abdominal pain; and 4 patients without a clear history of amenorrhea all had vaginal bleeding, with or without abdominal pain. At the time of misdiagnosis, the serum hCG level was >10,000 mIU/mL in 5 patients and <10,000 mIU/mL in 7 patients, and a positive urine pregnancy test alone was found in 2 patients. Vaginal ultrasonography showed no obvious abnormalities in 7 cases, adnexal mass in 5 cases, and tubal thickening in 2 cases. Details are shown in Table 1.
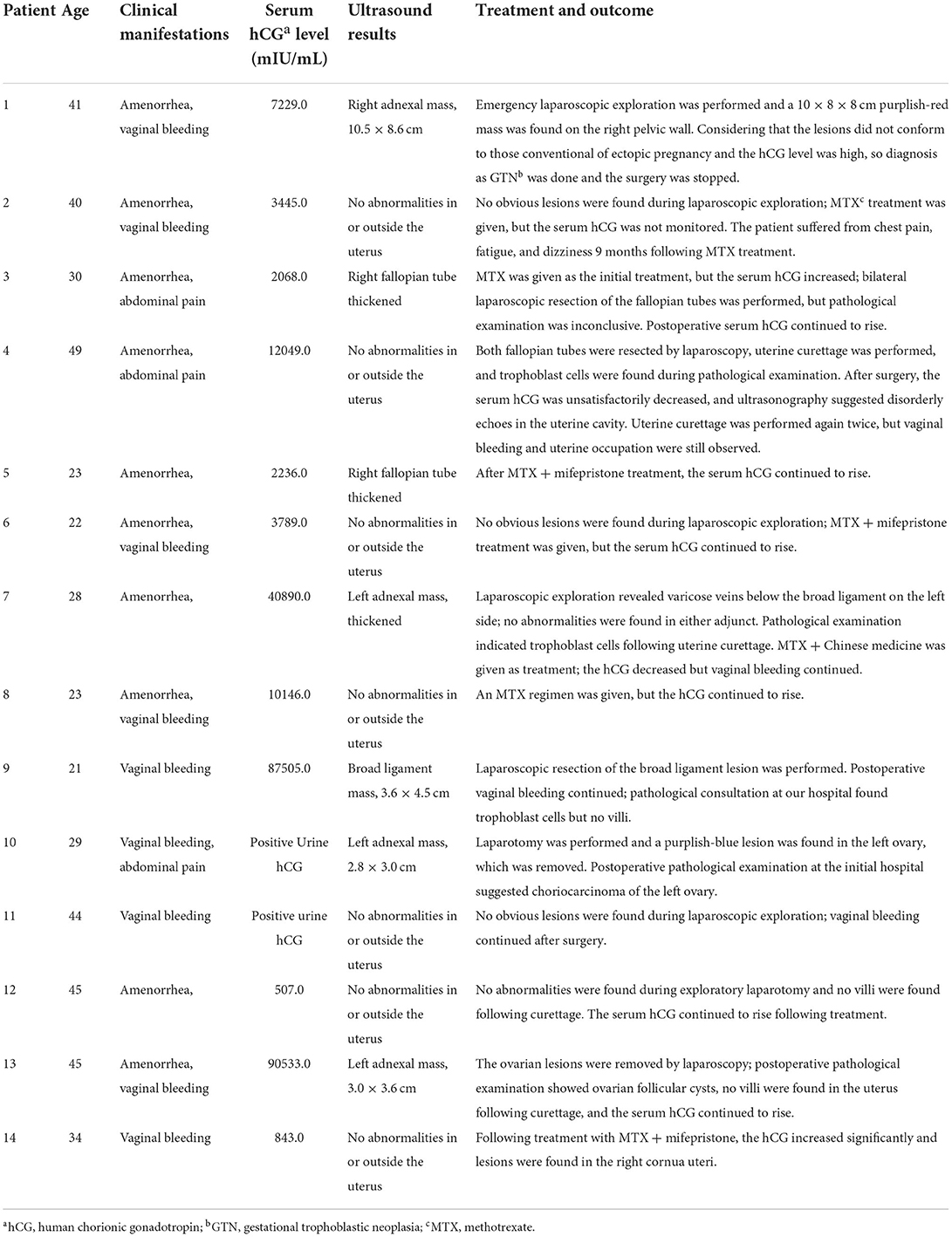
Table 1. Clinical characteristics of 14 misdiagnosed patients.
Among the 14 patients, 10 were initially treated with surgical exploration, including 1 case misdiagnosed at our hospital and 9 misdiagnosed at other hospitals. The patient misdiagnosed at our hospital was found to have massive and vascularized lesions on the lateral wall of the pelvis during laparoscopic exploration. GTN was considered, and the operation was stopped immediately. Among the 9 patients misdiagnosed at other hospitals, 5 had no intra- or extrauterine lesions detected by vaginal ultrasonography prior to surgery, and no exact lesions were found during surgery. In one case, both fallopian tubes were removed, and no abnormalities were found during the postoperative pathological examination. In the other 4 cases, the lesions all occurred at non-tubal sites: 2 ovaries, 1 broad ligament, and 1 pelvic wall. The first 3 patients received lesion resection; pathological examination indicated that one of the patients with an ovarian lesion had GTN and the other patient had an ovarian follicular cyst. No GTN features were found in the patient with broad ligament lesions. Surgery was stopped in the patient with lateral pelvic wall lesions due to the discovery of atypical lesions with tortuous vessels. Of the 9 patients misdiagnosed at other hospitals, only one (with an ovarian lesion) was corrected to a diagnosis of GTN following surgery. Among the remaining 8 patients, 3 received methotrexate (MTX) alone or in combination with mifepristone following surgery; however, the treatment was unsuccessful. The other 5 patients were transferred to our hospital due to continuously elevated serum hCG levels and/or continuous vaginal bleeding after surgery. Details are shown in Table 1.
The initial treatment in 4 patients was drug therapy, including MTX + mifepristone in 2 patients and MTX alone in the other 2 patients. Treatment failed in all 4 patients and the serum hCG continued to rise; GTN was then considered in 2 of these patients. Laparoscopic exploration was performed in one patient to remove both oviducts. Intraoperative findings and postoperative pathological examination were inconclusive. The serum hCG levels continued to rise after surgery, and GTN was considered following transfer to our hospital. The other patient received ultrasound examination again, which still showed no obvious intra- or extrauterine abnormalities; uterine curettage was subsequently performed. Postoperative pathological examination showed no GTN features, but the serum hCG levels continued to increase. GTN was considered following transfer to our hospital. Details are shown in Table 1.
Following GTN diagnosis, 5 patients progressed from no obvious intra- or extrauterine abnormalities to suspicious lesions detected by vaginal ultrasonography, including 2 cases in the uterine cavity, 2 cases in the intramural space, and 1 case in the cornua uteri. When diagnosed with GTN, the patient's previous pregnancy was an abortion in 7 cases, full-term in 4 cases, and a hydatidiform mole in 3 cases. The median interval from the first pregnancy to a diagnosis of GTN was 17.5 months (2–252 months), with the interval in 9 cases being >12 months. The median serum hCG level was 6077.5 mIU/mL (230.5–634960.1 mIU/mL), with the level in 3 patients being ≥100,000 mIU/mL. The clinical stage was stage I in 3 cases, stage II in 3 cases, stage III in 7 cases, and stage IV in 1 case with liver and spleen metastasis. The median FIGO (2000) prognostic score was 8 points (3–22 points), with 2 patients having a score ≥13 points (extremely high risk). Details are shown in Table 2.
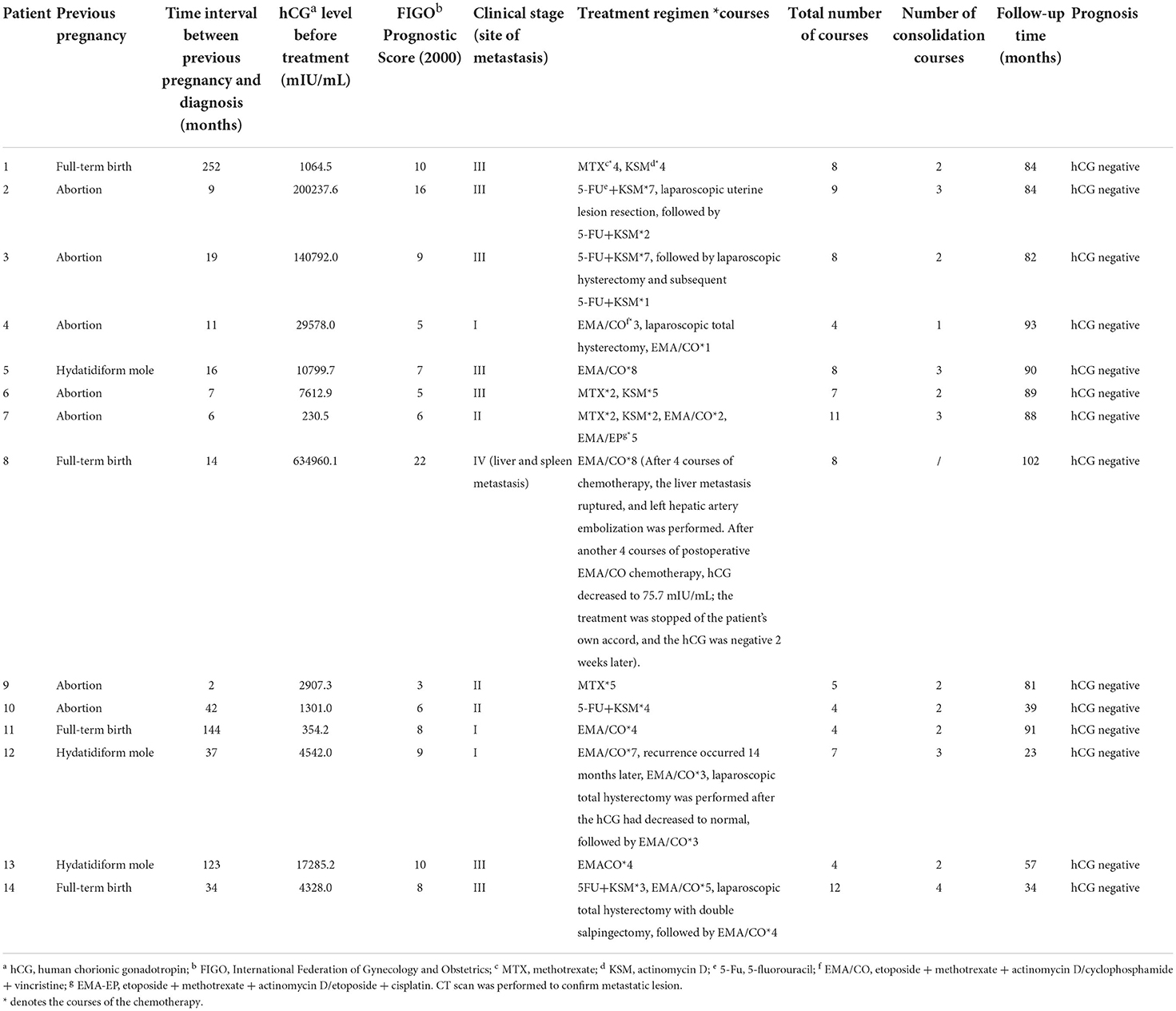
Table 2. The clinical characteristics, treatment, and prognosis of 14 patients diagnosed with GTN.
Of the 14 patients, 10 received combination chemotherapy and 4 received monotherapy. In the combined treatment group, the chemotherapy regimen was 5-fluorouracil and actinomycin D (5FU+KSM) in 4 patients, among which 1 patient changed regimen due to drug resistance, and EMA/CO in 6 patients. The median number of chemotherapy courses was 7.5 (4–12 courses), and that of consolidation courses was 2 (1–4 courses). Four patients received a total hysterectomy, and one underwent uterine lesion resection. Nine patients achieved complete remission (CR). One patient with liver and spleen metastasis gave up treatment after her serum hCG level dropped to 75.7 mIU/mL, which returned to normal 2 weeks later. Four patients received MTX monotherapy, and 1 patient achieved CR after initial treatment. Three patients changed regimen due to drug resistance, and all achieved CR. The median follow-up time was 84 months (23–102 months), and all 14 patients survived.
The most common GTD lesions occur in the uterus, and primary lesions outside the uterus are rare and occur in the fallopian tubes, accounting for 0.2–0.8% of cases (5, 6). GTN secondary to hydatidiform mole is relatively easy to diagnose by monitoring serum hCG levels, especially if the interval is shorter. GTN secondary to non-hydatidiform pregnancy, especially without uterine lesions, is more likely to be misdiagnosed. HCG level plateau for 4 consecutive values over 3 weeks or rise ≥10% for 3 values over 2 weeks after hydatidiform mole evacuation indicate GTN diagnosis (7). HCG level normalized within 14 weeks after evacuation in 95% of these patients (8). GTN occurring after hCG normalization is a rare event, which increases the difficulty of diagnosis in these patients.
Studies have shown that the sensitivity and specificity of serum hCG levels combined with transvaginal ultrasound imaging in diagnosing ectopic pregnancy is 97 and 95%, respectively (9). At a serum hCG level of 1,000–2,000 mIU /mL, evidence of ectopic pregnancy can be found in most vaginal ultrasound images (4, 10). At a serum hCG level >3,000 mIU/mL, most intrauterine pregnancy sacs can be detected by vaginal ultrasonography (11, 12). Some scholars have recommended a cut-off value for serum hCG at 3,500 mIU/mL to avoid misdiagnosis or termination of a pregnancy that may be normal (4, 9). If the serum hCG is greater than this level and no pregnancy sac is found by vaginal ultrasound, intrauterine pregnancy is extremely rare. Patients with a positive hCG but no imaging evidence confirming intra- or extrauterine pregnancy should be followed up closely if their hemodynamics are stable (13). If the serum hCG is >3,500 mIU/mL and no evidence of intrauterine pregnancy is found, GTN or other hCG-secreting tumors should be considered. In the present study, there were 7 patients with vaginal color doppler ultrasonography indicating no obvious intra- or extrauterine abnormalities, four of whom had a serum hCG level >2,000 mIU/mL, essentially excluding ectopic pregnancy. Two patients had a serum hCG level >10,000 mIU/mL; therefore, GTN or other hCG-secreting tumors should be considered. The other 2 cases had a serum hCG level <1,000 mIU/mL and should be followed up closely.
Difficult diagnosis by ultrasound imaging in some patients can be assisted by magnetic resonance imaging (MRI) (14). In addition, since most GTN patients have lung metastasis, chest radiographs and lung CT examination can also be used as a differentiator in suspected GTN patients. In some patients with differential diagnosis difficulties, laparoscopy or hysteroscopy is necessary to confirm the diagnosis (15).
Ultrasound image is important criteria for diagnosis of EP, hCG positive and uterine cavity empty, the diagnosis of ectopic pregnancy is usually indicated. However, as hCG is at a low level, it is not casually to make a diagnosis when the condition is stable. HCG and ultrasound images should be closely monitored to avoid misdiagnosis and missed diagnosis. While the hCG level is at a high level, a comprehensive assessment should be make, especially searching for metastatic lesion. HCG positive and metastatic lesion indicate diagnosis of GTN.
The low incidence and non-specific clinical manifestations of GTN are the main reasons for misdiagnosis. GTN is sensitive to chemotherapy, and the vast majority of patients can be cured. It has been reported that the prognosis of GTN with extrauterine lesions is still good (5); however, hematogenous metastasis is the main transfer route of this disease. If distant metastasis such as liver or brain occurs, the prognosis is poor; thus, early diagnosis and treatment should be carried out to avoid delay.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The present study was approved by the Ethics Committee of the West China Second Hospital of Sichuan University. Informed consent was obtained from all patients.
PX: data collecting and manuscript writing. TG: data collecting. RY: supervision manuscript review and editing. All authors have read and approved the final manuscript.
This work was supported by The Key Project of Sichuan Provincial Department of Science and Technology, Study on the key factors affecting the diagnosis and treatment of major diseases in obstetrics and gynecology (19ZDYF) (Approved by Medical Ethics Committee of West China Second University Hospital, Sichuan University. Ethical Lot Number: 20200076).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. WHO Classification of Tumours Editorial Board. Female Genital Tumours. WHO Classification of Tumours. 5th ed. Lyon. (2020).
2. Ngan HYS, Seckl MJ, Berkowitz RS, Xiang Y, Golfier F, Sekharan PK, et al. Update on the diagnosis and management of gestational trophoblastic disease. Int J Gynaecol Obstet. (2018) 143:79–85. doi: 10.1002/ijgo.12615
3. Lurain JR. Gestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole. Am J Obset Gynecol. (2010) 203:531–9. doi: 10.1016/j.ajog.2010.06.073
4. Hendriks E, Rosenberg R, Prine L. Ectopic pregnancy: diagnosis and management. Am Fam Phys. (2020) 101:599–606.
5. Hassadia A, Kew FM, Tidy JA, Wells M, Hancock BW. Ectopic gestational trophoblastic disease: a case series review. J Reprod Med. (2012) 57:297–300.
6. Muto MG, Lage JM, Berkowitz RS, Goldstein DP, Bernstein MR. Gestational trophoblastic disease of the fallopian tube. J Reprod Med. (1991) 36:57–60.
7. Ngan HY BH, Benedet JL, Jones H, Montruccoli GC, Pecorelli S, et al. Gestational trophoblastic neoplasia, FIGO 2000 staging and classification. Int J Gynecol Obstet. (2003) 83(Suppl. 1):175–7. doi: 10.1016/S0020-7292(03)90120-2
8. Eysbouts Y, Brouwer R, Ottevanger P, Massuger L, Sweep F, Thomas C, et al. Serum human chorionic gonadotropin normogram for the detection of gestational trophoblastic neoplasia. Int J Gynecol Cancer. (2017) 27:1035–41. doi: 10.1097/IGC.0000000000000966
10. Rana P, Kazmi I, Singh R, Afzal M, Al-Abbasi FA, Aseeri A, et al. Ectopic pregnancy: a review. Arch Gynecol Obstet. (2013) 288:747–57. doi: 10.1007/s00404-013-2929-2
11. Dart R, Kaplan B, Ortiz L, Cloherty J, Lavoie T. Normal intrauterine pregnancy is unlikely in emergency department patients with either menstrual days >38 days or β-hCG>3,000 mIU/mL, but without a gestational sac on ultrasonography. Acad Emerg Med. (1997) 4:967–71. doi: 10.1111/j.1553-2712.1997.tb03660.x
12. Kadar N, Bohrer M, Kemmann E, Shelden R. The discriminatory human chorionic gonadotropin zone for endovaginal sonography: a prospective, randomized study. Fertil Steril. (1994) 61:1016–20. doi: 10.1016/S0015-0282(16)56749-1
13. Doubilet PM, Benson CB. Further evidence against the reliability of the human chorionic gonadotropin discriminatory level. J Ultrasound Med. (2011) 30:1637–42. doi: 10.7863/jum.2011.30.12.1637
14. Suzuki H, Chigusa Y, Hamanishi J, Mandai M, Kondoh E. Two cases of ectopic pregnancy mimicking gestational trophoblastic disease. Case Rep Obstet Gynecol. (2020) 2020:2417428. doi: 10.1155/2020/2417428
Keywords: gestational trophoblastic neoplasia, ectopic pregnancy, human chorionic gonadotropin, misdiagnosis, retrospective study
Citation: Xiao P, Guo T and Yin R (2022) Misdiagnosis of gestational trophoblastic neoplasia as ectopic pregnancy: A 15-year retrospective study. Front. Med. 9:1018573. doi: 10.3389/fmed.2022.1018573
Received: 13 August 2022; Accepted: 18 October 2022;
Published: 02 November 2022.
Edited by:
Lawrence Hsu Lin, New York University, United StatesCopyright © 2022 Xiao, Guo and Yin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rutie Yin, eXJ0dDIwMTNAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.