 Layla Honorato1
Layla Honorato1 Steven S. Witkin1,2
Steven S. Witkin1,2 Maria Cássia Mendes-Correa1
Maria Cássia Mendes-Correa1 Ana Luiza Castro Conde Toscano3
Ana Luiza Castro Conde Toscano3 Iara Moreno Linhares4Anderson Vicente de Paula1
Iara Moreno Linhares4Anderson Vicente de Paula1 Heuder Gustavo Oliveira Paião1Vanessa Salete de Paula5Amanda de Oliveira Lopes5Silvia Helena Lima1
Heuder Gustavo Oliveira Paião1Vanessa Salete de Paula5Amanda de Oliveira Lopes5Silvia Helena Lima1 Vanessa de Cássia Raymundi1
Vanessa de Cássia Raymundi1 Noely Evangelista Ferreira1
Noely Evangelista Ferreira1 Almir Ribeiro da Silva Junior1Karim Yaqub Abrahim1
Almir Ribeiro da Silva Junior1Karim Yaqub Abrahim1 Paulo Henrique Braz-Silva1,6
Paulo Henrique Braz-Silva1,6 Tania Regina Tozetto-Mendoza1*
Tania Regina Tozetto-Mendoza1*- 1Laboratory of Virology (LIM 52), Department of Infectious Diseases, Instituto de Medicina Tropical de São Paulo, Universidade de São Paulo, São Paulo, Brazil
- 2Department of Obstetrics and Gynecology, Weill Cornell Medicine, New York, NY, United States
- 3Hospital Dia, Instituto de Infectologia Emílio Ribas, São Paulo, Brazil
- 4Departamento de Ginecologia e Obstetrícia, Universidade de São Paulo, São Paulo, Brazil
- 5Laboratory of Molecular Virology, Instituto Oswaldo Cruz, Fundação Oswaldo Cruz, Rio de Janeiro, Brazil
- 6Faculdade de Odontologia da Universidade de São Paulo, São Paulo, Brazil
Introduction: Torque teno virus (TTV) is a non-pathogenic virus present in body fluids. Its titer in the circulation increases in association with immune suppression, such as in HIV-infected individuals. We evaluated if the TTV titer in saliva from HIV-positive individuals undergoing antiretroviral therapy (ART) was related to the circulating CD4+ T lymphocyte concentration and the HIV titer.
Methods: Saliva was collected from 276 asymptomatic individuals undergoing ART, and an additional 48 individuals positive for AIDS-associated Kaposi's Sarcoma (AIDS-KS). The salivary TTV titer was measured by gene amplification analysis. The circulating CD4+ T lymphocyte and HIV levels were obtained by chart review.
Results: TTV was detectable in saliva from 80% of the asymptomatic subjects and 87% of those with AIDS-KS. In the asymptomatic group the median log10 TTV titer/ml was 3.3 in 200 males vs. 2.4 in 76 females (p < 0.0001). TTV titer/ml was 3.7 when HIV was acquired by intravenous drug usage, 3.2 when by sexual acquisition and 2.4 when blood transfusion acquired. The salivary TTV titer was inversely correlated with the circulating CD4+ T lymphocyte level (p < 0.0001) and positively correlated with the circulating HIV concentration (p = 0.0005). The median salivary TTV titer and circulating HIV titer were higher, and the CD4+ count was lower, in individuals positive for AIDS-KS than in the asymptomatic subjects (p < 0.0001).
Conclusion: The TTV titer in saliva is a potential biomarker for monitoring immune status in individuals undergoing ART.
Introduction
Torque teno virus (TTV), first described in 1997, is a non-enveloped DNA virus (1) belonging to the Anelloviridae family and the Alphatorquetenovirus genus (2). There are at least 29 major TTV species that exhibit a high degree of genomic heterogeneity (1–4). TTV is recognized as a commensal non-pathogenic virus with a worldwide distribution. It is ubiquitously detected in body fluids in up to 90% of healthy individuals (2, 4, 5). It has been suggested that the TTV level in saliva may be elevated as compared to its level in the circulation, peripheral blood mononuclear cells or in body sites such as in liver or bone marrow (6–9). Therefore, the utility of salivary TTV determination may be of clinical value for evaluating immune status.
A higher prevalence of TTV and a wider range of TTV genotypes has been reported to be present in the circulation of HIV-infected individuals as compared to uninfected healthy people (10, 11). In addition, there appears to be an inverse correlation between the CD4+ T lymphocyte count and the plasma level of TTV in the context of HIV infection (10, 12, 13).
The aim of the present study was to investigate the presence and titer of TTV in saliva samples from asymptomatic HIV-positive individuals undergoing anti-retroviral therapy (ART), as well as in AIDS patients being treated for Kaposi's Sarcoma (AIDS-KS), and to determine if this analysis could serve as a potential biomarker of immune status, in addition to the circulating CD4+ T lymphocyte and HIV level.
Materials and Methods
Subjects and Study Sites
The current protocol is a component of our previous studies on HIV-infected patients with and without Kaposi sarcoma (CAAE: 55771116.0.1001.0065) (14, 15). Saliva samples from HIV-infected subjects undergoing ART were collected as part of a 2008 study of molecular characterization of herpesvirus human type 8 (HHV-8), the causal agent of Kaposi's sarcoma. However, saliva samples from the AIDS-KS patients were scarce, all consumed and necessitated collection of new salivary samples from AIDS-KS patients between 2016 and 2018. The primary subjects in this cross-sectional study were 276 asymptomatic and HIV-positive who were all outpatients at the Hospital das Clínicas, of the Faculdade de Medicina of the Universidade de São Paulo, São Paulo, Brazil. An additional 48 saliva samples were collected from subjects with AIDS-KS at Dia Hospital of the Instituto de Infectologia Emílio Ribas (IIER), São Paulo, Brazil. All clinical information as well as each subject's circulating HIV and CD4+ T lymphocyte concentration, were obtained by chart review. The HIV level was determined by a standard real time polymerase chain reaction with an analytical sensitivity of 50 copies/ml; the circulating CD4+ concentration was measured by routine Fluorescence Activated Cell Sorting (FACS) analysis. All subjects were taking combination ART. The chemotherapy (CT) regime for AIDS-KS was based on the available regimen (IIER), ABV, Daunorubicin or Doxorubicin, alternatively.
Saliva Collection and Molecular Analysis of TTV
Saliva was obtained within 30 days of blood collection for CD4+ and HIV analysis. The saliva collection protocol was as described previously (16, 17) and a 2 ml sample was cryopreserved at-−80°C until used. Nucleic acid was extracted and purified by using a DNA extraction kit (Real Genomics Biotech Corp.), according to the manufacturer's instructions. The quality of the total DNA was monitored by PCR amplification of the human β-globin sequence (18), prior to investigation of viral DNA. All samples were suitable for viral DNA amplification as judged by the results of this internal control.
The primers and probe sequences for DNA TTV amplification were as described previously: Forward primer 5′-GTGCCGIAGGTGAGTTTA-3′; Reverse primer 5′-AGCCCGGCCAGTCC-3′; Probe: FAM5′- TCAAGGGGCAATTCGGGCT-3′ (3, 5). For real time quantitative PCR reaction (qPCR), a standard curve was generated, as described previously, with known amounts of the synthetic oligonucleotide: 5′TTCGT AGCCCGGCCAGTCC CGTAT AGCCCGAATTGCCCCTTGA ATGCGT TAAACTCACCTTCGGCAC CTGATA−3′ (16, 19). The qPCR mix was prepared with forward and reverse primers at 250 nM and the probe at 62 nM and a standard input of ~100 ng of DNA template per reaction in 12.5 μl of 2X TaqMan™ Universal Master Mix (Thermo Fisher Scientific, Warrington, UK). Thermocycling conditions consisted of two initial heat activation steps of 50°C for 2 min and 95°C for 15 s, followed by 50 cycles of 15 s at 95°C and 1 min at 60°C, in a Quantstudio™ 5 instrument. The data were analyzed using QuantStudio Design & Analysis Software v.1.4.1. The limit of sensitivity of TTV qPCR was 40 copies/ml at a >95% detection rate (16, 19).
Statistical Analysis
The Mann-Whitney test or the Kruskal-Wallis test were used to compare results between groups, as appropriate. Associations between the TTV titer and the CD4 or HIV concentration were analyzed by the Spearman rank correlation test. A p-value < 0.05 was considered significant. The GraphPad Prism 9 software (San Diego, CA) was used for all analyses.
Ethical Approval
The Institutional Review Board committees at Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo CAPPESP 0290/07 and Emilio Ribas CC No. 48/2016 previously approved the project (CAAE: 55771116.0.1001.0065). All subjects provided written informed consent before their participation and saliva collection. An amendment to waive the informed consent for the current protocol on salivary TTV titer and immune status was approved by the same committees (5.054.321 and 5.065.362) in October, 2021.
Results
Characteristics of the Asymptomatic Subjects and Relation to TTV Titer in Saliva
The mean age of the study subjects was 44.8 +/−9.2 years and usage of ART was for 4.0 +/−0.9 years. Characteristics of the asymptomatic group and the relationship to the salivary TTV titer is shown in Table 1. The majority of the subjects were male (72.5%) and their median log10 TTV titer/ml (3.3) was higher than in the female subjects (2.4) (p < 0.0001, Mann-Whitney test). The racial distribution was 60.5% White and 39.5% non-White and there was no association between race and TTV titer. The mode of HIV acquisition was 42.4% in men having sex with men, 27.9% from blood transfusion, 16.7% by heterosexual sex and 13.0% by intravenous (IV) drug ingestion. The median log10 TTV titer/ml was different in each group (p < 0.0001, Kruskal-Wallis test), being highest in the IV drug users (3.7) and lowest in the transfusion group (2.4). However, there were no differences in the CD4 or HIV levels by source of infection (p > 0.05, Kruskal-Wallis test).
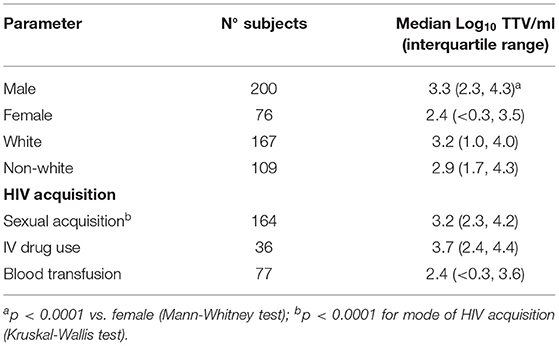
Table 1. Association between characteristics of study subjects and TTV in saliva.
Association Between TTV in Saliva and Circulating CD4+lymphocytes
The salivary TTV titer was inversely related to the circulating CD4+ T lymphocyte concentration (p < 0.0001, Spearman rank correlation test). The log10 TTV titer/ml at different CD4+ concentrations is shown in Table 2. The TTV titer decreased from 5.7 when the CD4+ level was <200 cells/mm3, to 3.7 when CD4+ was between 201 and 350 cells/mm3, to 3.4 when the level was between 351 and 500 cells/mm3, to 2.9 when CD4+ was >500 cells/mm3 (p < 0.0001 Kruskal-Wallis test).
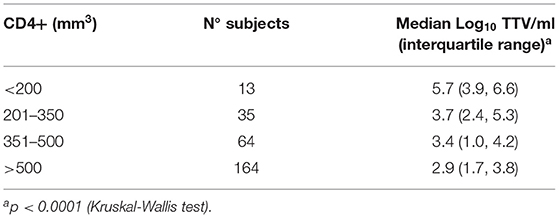
Table 2. Association between CD4+ cell count and TTV in saliva.
Association Between TTV in Saliva and HIV in the Circulation
HIV was below the level of detection (<50 particles/ml) in 189 (68.5%) of the subjects. The association between log10 HIV titer in the circulation and the log10 TTV titer in saliva is shown in Table 3. The salivary TTV level increased in proportion to the circulating HIV level. The median log10 TTV titer/ml was 2.9 when HIV was not detected, 3.5 when the log10 HIV titer/ml was between 1.8–3.0 and 3.8 when it was between 3.1–4.0 and 4.1 when the log10 HIV level/ml was >4.0 (p = 0.0005, Kruskal-Wallis test). As expected, the HIV titer was negatively correlated with the CD4+ concentration (p < 0.0001, Spearman rank correlation test).
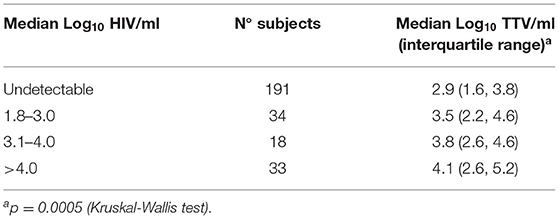
Table 3. Association between TTV in saliva and HIV in the circulation.
TTV in Individuals With AIDS-KS
The 47 subjects with AIDS-KS were younger than the asymptomatic individuals (38.2 vs. 44.8 years, p < 0.0001), had a lower median log10 CD4+ level (127 vs. 559 mm3, p < 0.0001) and a higher circulating median log10 HIV titer/ml (2.4 vs. <1.0, p < 0.0001). The median log10 TTV titer/ml in saliva was also greatly elevated in the AIDS-KS group (5.3) as compared to the asymptomatic group (3.1) (p < 0.0001). The time using ART was similar in the AIDS-KS and asymptomatic groups (4.6 vs. 4.0 years, respectively). All analyses were by the Mann-Whitney test. Similar to findings in the asymptomatic group, the circulating CD4+ concentration was inversely related to the salivary TTV titer in the group with AIDS-KS (p < 0.0001, Spearman rank correlation test). Regardless of the CT regimen or ART combination, the TTV was inversely proportional to the CD4+ count in 40 patients with AIDS-KS receiving CT (Supplementary Table 1, Description of characteristics of AIDS-KS subjects).
TTV and HIV Titers in Relation to the CD4+ Lymphocyte Count
An inverse relation between the CD4+ level and titers of both TTV/HIV was also observed in this study (Figure 1), demonstrating a suitable sensitivity for TTV analysis in the saliva. The TTV titer in saliva was higher than the HIV titer in the circulation in relation to the CD4 + level of <250, 250–350 and >500 cells/mm3 (****p < 0.0001, Mann Whitney test).
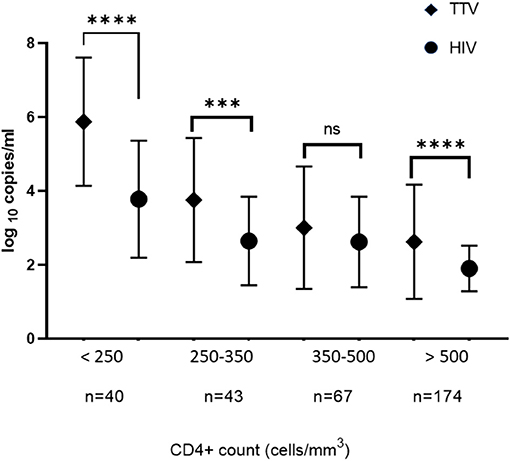
Figure 1. Means of titers of TTV in the saliva and HIV in the circulation in relation to the CD4+ lymphocytes count from all subjects being treated with antiretroviral therapy. The TTV and HIV titers were proportionately increased when CD4+ count was decreased. The vertical bar indicates the Standard Deviation value of the titer of TTV and HIV in log10 copies/ml. ****p < 0.0001; ***p < 0.0005; ns, statistically not significant.
Discussion
In our study of HIV-infected individuals who were currently on ART, the majority had detectable levels of TTV in their saliva. In both asymptomatic subjects and those positive for AIDS-KS, the TTV level was significantly elevated in parallel to the concentration of HIV in the circulation and significantly reduced as the concentration of CD4+ lymphocytes increased in the circulation. These fluctuations in the TTV level strongly suggest that analysis of the salivary TTV level is a sensitive biomarker for CD4+ status and HIV production in HIV-positive individuals currently undergoing ART. Our findings are consistent with earlier studies that demonstrated an association between the extent of TTV viremia in the systemic circulation and immune dysfunction in HIV-positive individuals (12, 13, 20–22). The analysis of TTV titers in bone marrow and spleen tissues also confirmed that elevations in TTV parallel AIDS progression (22). Serial analyses of TTV concentrations in plasma from individuals living with HIV further reinforces the inverse correlation between TTV titer and CD4 count (10, 12, 13, 20). Our observation of elevated salivary TTV levels in HIV-positive subjects with AIDS-KS as compared to asymptomatic HIV-positive individuals is also consistent with this association.
Investigations of the rate of TTV detection in blood from HIV-positive individuals have varied from <50% to >90% (13, 20, 21, 23). This discordance is likely due in large part to the choice of primers utilized for TTV detection (11, 13, 24, 25). For the quantitation of the TTV titer in saliva in our study we utilized primers and probes specific for the untranslated regions of the TTV genome in a protocol yielding an analytical sensitivity (LOD >95%) of 40 copies/ml (5, 16). The resulting detection of TTV in saliva from 80% of asymptomatic HIV-positive individuals supports the high sensitivity of our analysis.
The salivary TTV titer in women in our study was lower than in men. This is consistent with reports of higher circulating TTV levels in men than in women (26, 27). Differences in hormone levels between men and women have been implicated in influencing TTV titers and responses to HIV infection (28, 29).
The salivary TTV titer in our study subjects was highest in individuals who acquired HIV from IV drug use and lowest in those with transfusion-acquired HIV. A study of TTV in blood from individuals infected with HIV also reported the highest levels in IV drug users (11). There were no differences in the CD4 or HIV levels by source of infection in the asymptomatic individuals in our study. We propose that the TTV titer in saliva will vary with the level of physiological stress and immune suppression, and that this may very well differ between individuals with different modes of HIV acquisition. For example, IV drug users are at increased risk to acquire other infectious diseases as well as multiple TTV genotypes. However, we agree that this interpretation requires direct support and so the reasons for the observed disparity in TTV titer remains to be determined. Possibly, additional immune-related variables other than the CD4+ T lymphocyte level are responsible for the observed variations in TTV titer.
Study limitations should be acknowledged. Subjects' blood samples were not available to us for TTV analysis and thus we are unable to comment on the relative titers of TTV in saliva and in blood. Our study also only analyzed salivary TTV at a single time point. Sequential analyses might have led to a more accurate correlation between TTV abundance in saliva and variation in T cell immune responses. Patient knowledge and recall of the event responsible for HIV acquisition may be incomplete or faulty. Lastly, the absence of information on the possible influence of ART or CT on the TTV titer remains to be determined.
In conclusion, our findings suggest that the analysis of TTV titers in saliva may be of value as an additional and sensitive tool for monitoring the immune status in HIV-infected patients on ART. Similarly, a salivary TTV assay may also be beneficial as a non-invasive procedure to model the level of immunosuppression in other infectious or non-infectious disorders.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics and Research Committee local CAPPEsq (number 1.560.798) and Emilio Ribas (CC No 48/2016). CAAE: 55771116.0.1001.0065, parecer number 5.054.321 and 5.065.362. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
TT-M, LH, SW, and MM-C: conceptualization. LH, AC, VP, AL, HP, SL, VR, NF, AS, and PB-S: methodology. TT-M, SW, MM-C, IL, and PB-S: validation. TT-M, LH, and SW: formal analysis. AC, LH, TT-M, KA, HP, VP, SL, VR, AL, NF, AS, and PB-S: investigation. TT-M and LH: resources. TT-M, KA, LH, SW, IL, MM-C, and PB-S: data curation. TT-M, LH, AC, and SW: writing—original draft preparation. SW: writing—review and editing. SW and LH: visualization. TT-M: supervision. TT-M and MM-C: project administration and funding acquisition. All authors contributed to the article and approved the submitted version.
Funding
The research was supported by CNPq (Conselho Nacional de Desenvolvimento Cientifico e Tecnológico), an agency of the Brazilian Ministry of Science and Technology (Grants - 423401/2018-1- Universal Project Modality). Additional financial support was provided by the Laboratory of Virology (LIM52) of Department of Infectious Diseases of Hospital das Clínicas of the Faculdade de Medicina of the Universidade de São Paulo.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the staff of the Laboratory of Medical Research in Virology (LIM52) for technical support - Instituto de Medicina Tropical of the Faculdade de Medicina of the Universidade de São Paulo.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.809312/full#supplementary-material
References
1. Nishizawa T, Okamoto H, Konishi K, Yoshizawa H, Miyakawa Y, Mayumi M. A novel DNA virus (TTV) associated with elevated transaminase levels in posttransfusion hepatitis of unknown etiology. Biochem Biophys Res Commun. (1997) 241:92–7. doi: 10.1006/bbrc.1997.7765
2. Biagini P. Classification of TTV and related viruses (Anelloviruses). Current Topics Microbiol Immunoly. (2009) 331:21–33. doi: 10.1007/978-3-540-70972-5_2
3. Maggi F, Fornai C, Zaccaro L, Morrica A, Vatteroni ML, Isola P, et al. TT virus (TTV) loads associated with different peripheral blood cell types and evidence for TTV replication in activated mononuclear cells. J Med Virol. (2001) 64:190–4. doi: 10.1002/jmv.1035
4. Spandole S, Cimponeriu D, Berca LM, Mihăescu G. Human anelloviruses: an update of molecular, epidemiological and clinical aspects. Arch Virol. (2015) 160:893–908. doi: 10.1007/s00705-015-2363-9
5. Maggi F, Pifferi M, Tempestini E, Fornai C, Lanini L, Andreoli E, et al. TT virus loads and lymphocyte subpopulations in children with acute respiratory diseases. J Virol. (2003) 77:9081–3. doi: 10.1128/JVI.77.16.9081-9083.2003
6. Albert E, Torres I, Talaya A, Giménez E, Piñana JL, Hernández-Boluda JC, et al. Kinetics of torque teno virus DNA load in saliva and plasma following allogeneic hematopoietic stem cell transplantation. J Med Virol. (2018) 90:1438–43. doi: 10.1002/jmv.25218
7. Deng X, Terunuma H, Handema R, Sakamoto M, Kitamura T, Ito M, et al. Higher prevalence and viral load of TT virus in saliva than in the corresponding serum: another possible transmission route and replication site of TT virus. J Med Virol. (2000) 62:531–7. doi: 10.1002/1096-9071(200012)62:4<531::AID-JMV20>3.0.CO;2-C
8. Hettmann A, Demcsák A, Bach Á, Decsi G, Dencs Á, Pálinkó D, et al. Detection and phylogenetic analysis of torque teno virus in salivary and tumor biopsy samples from head and neck carcinoma patients. Intervirol. (2016) 59:123–9. doi: 10.1159/000452974
9. Ross RS, Viazov S, Runde V, Schaefer UW, Roggendorf M. Detection of TT virus DNA in specimens other than blood. J Clin Virol. (1999) 13:181–4. doi: 10.1016/S1386-6532(99)00015-3
10. Elesinnla AR, Adeleye IA, Ayolabi CI, Bessong PO. Prevalence of torque viruses in HIV-infected and non-HIV-infected Nigerian subjects: analysis of near-full-length genome sequences. Arch Virol. (2020) 165:571–82. doi: 10.1007/s00705-020-04538-1
11. Sherman KE, Rouster SD, Feinberg J. Prevalence and genotypic variability of TTV in HIV-infected patients. Digest Dis Scie. (2001) 46:2401–7. doi: 10.1023/A:1012307416122
12. Christensen JK, Eugen-Olsen J, Sørensen M, Ullum H, Gjedde SB, Pedersen BK, et al. Prevalence and prognostic significance of infection with TT virus in patients infected with human immunodeficiency virus. J Infect Dis. (2000) 181:1796–9. doi: 10.1086/315440
13. Shibayama T, Masuda G, Ajisawa A, Takahashi M, Nishizawa T, Tsuda F, et al. Inverse relationship between the titre of TT virus DNA and the CD4 cell count in patients infected with HIV. AIDS. (2001) 15:563–70. doi: 10.1097/00002030-200103300-00004
14. Tozetto-Mendoza TR, Ibrahim KY, Tateno AF, de Oliveira CM, Sumita LM, Sanchez MCA, et al. Genotypic distribution of HHV-8 in AIDS individuals without and with Kaposi sarcoma. Medicine. (2016) 95:e5291. doi: 10.1097/MD.0000000000005291
15. De Oliveira Lopes A, Spitz N, Martinelli KG, de Paula AV, de Castro Conde Toscano AL, Braz-Silva PH, et al. Introduction of human gammaherpesvirus 8 genotypes A, B and C into Brazil from multiple geographic regions. Virus Res. (2020) 276:197828. doi: 10.1016/j.virusres.2019.197828
16. Mendes-Correa MC, Tozetto-Mendoza TR, Freire WS, Paiao HGO, Ferraz ABC, Mamana AC, et al. Torquetenovirus in saliva: a potential biomarker for SARS-CoV-2 infection? PLoS ONE. (2021) 16:e0256357. doi: 10.1371/journal.pone.0256357
17. Tozetto-Mendoza TR, Sumita LM, Palmieri M, Ornaghi M, Canto AM, Braz-Silva PH. No detectable human herpesvirus-8 oral shedding in seronegative-healthy, immunocompetent individuals from non-endemic regions for Kaposi's sarcoma: A pilot study. J Invest Clin Dentistry. (2018) 9:1–6. doi: 10.1111/jicd.12278
18. Saiki R, Scharf S, Faloona F, Mullis K, Horn G, Erlich H, et al. Enzymatic amplification of beta-globin genomic sequences and restriction site analysis for diagnosis of sickle cell anemia. Science. (1985) 230:1350–4. doi: 10.1126/science.2999980
19. Tozetto-Mendoza TR, Bongiovanni AM, Minis E, Linhares IM, Boester A, Freire WS, et al. Torquetenovirus titer in vaginal secretions from pregnant and postpartum women: association with absence of lactobacillus crispatus and levels of lactic acid and matrix metalloproteinase-8. Reprod Sci. (2020) 27:2075–81. doi: 10.1007/s43032-020-00227-1
20. Nasser TF, Brajão de Oliveira K, Vissoci Reiche EM, Amarante MK, Pelegrinelli Fungaro MH, Watanabe MAE. Detection of TT virus in HIV-1 exposed but uninfected individuals and in HIV-1 infected patients and its influence on CD4+ lymphocytes and viral load. Microbial Pathogenesis. (2009) 47:33–7. doi: 10.1016/j.micpath.2009.04.010
21. Schmidt L, Jensen B-EO, Walker A, Keitel-Anselmino V, di Cristanziano V, et al. Torque Teno Virus plasma level as novel biomarker of retained immunocompetence in HIV-infected patients. Infection. (2021) 49:501–9. doi: 10.1007/s15010-020-01573-7
22. Thom K, Petrik J. Progression towards AIDS leads to increased torque teno virus and torque teno minivirus titers in tissues of HIV infected individuals. J Med Virol. (2007) 79:1–7. doi: 10.1002/jmv.20756
23. Puig-Basagoiti F, Cabana M, Guilera M, Giménez-Barcons M, Sirera G, Tural C, et al. Prevalence and route of transmission of infection with a novel DNA virus (TTV), hepatitis C virus, and hepatitis G virus in patients infected with HIV. J Acquired Immune Deficiency Syndromes. (2000) 23:89–94. doi: 10.1097/00126334-200001010-00012
24. Okamoto H, Takahashi M, Nishizawa T, Ukita M, Fukuda M, Tsuda F, et al. Marked genomic heterogeneity and frequent mixed infection of TT virus demonstrated by PCR with primers from coding and noncoding regions. Virology. (1999) 259:428–36. doi: 10.1006/viro.1999.9770
25. Okamoto H, Takahashi M, Kato N, Fukuda M, Tawara A, Fukuda S, et al. Sequestration of TT virus of restricted genotypes in peripheral blood mononuclear cells. J Virol. (2000) 74:10236–9. doi: 10.1128/JVI.74.21.10236-10239.2000
26. Brassard J, Gagné M-J, Leblanc D, Poitras É, Houde A, et al. Association of age and gender with torque teno virus detection in stools from diarrheic and non-diarrheic people. J Clin Virol. (2015) 72:55–9. doi: 10.1016/j.jcv.2015.08.020
27. Haloschan M, Bettesch R, Görzer I, Weseslindtner L, Kundi M, Puchhammer-Stöckl E. TTV DNA plasma load and its association with age, gender, and HCMV IgG serostatus in healthy adults. AGE. (2014) 36:9716. doi: 10.1007/s11357-014-9716-2
28. Brundin PMA, Landgren BM, Fjällström P, Johansson AF, Nalvarte I. Blood hormones and torque teno virus in peripheral blood mononuclear cells. Heliyon. (2020) 6:e05535. doi: 10.1016/j.heliyon.2020.e05535
Keywords: CD4+ lymphocytes, HIV, Kaposi's Sarcoma, saliva, torque teno virus, anellovirus
Citation: Honorato L, Witkin SS, Mendes-Correa MC, Conde Toscano ALC, Linhares IM, de Paula AV, Paião HGO, de Paula VS, Lopes AO, Lima SH, Raymundi VC, Ferreira NE, da Silva Junior AR, Abrahim KY, Braz-Silva PH and Tozetto-Mendoza TR (2022) The Torque Teno Virus Titer in Saliva Reflects the Level of Circulating CD4+ T Lymphocytes and HIV in Individuals Undergoing Antiretroviral Maintenance Therapy. Front. Med. 8:809312. doi: 10.3389/fmed.2021.809312
Received: 09 November 2021; Accepted: 22 December 2021;
Published: 14 January 2022.
Edited by:
Zhiliang Hu, Nanjing Second Hospital, ChinaReviewed by:
Denis V. Rebrikov, Gynecology and Perinatology Named After Academician V.I. Kulakova, RussiaBjörn Jensen, Heinrich Heine University of Düsseldorf, Germany
Salwa Bdour, The University of Jordan, Jordan
Copyright © 2022 Honorato, Witkin, Mendes-Correa, Conde Toscano, Linhares, de Paula, Paião, de Paula, Lopes, Lima, Raymundi, Ferreira, da Silva Junior, Abrahim, Braz-Silva and Tozetto-Mendoza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tania Regina Tozetto-Mendoza, dG96ZXR0byYjeDAwMDQwO3VzcC5icg==