 Margaux Damerval1Christine Fagnoni-Legat1Aurélien Louvrier2,3Sarah Fischer1Samuel Limat1,3Anne-Laure Clairet1Virginie Nerich1,3Isabelle Madelaine4
Margaux Damerval1Christine Fagnoni-Legat1Aurélien Louvrier2,3Sarah Fischer1Samuel Limat1,3Anne-Laure Clairet1Virginie Nerich1,3Isabelle Madelaine4 Marie Kroemer1,3*
Marie Kroemer1,3*- 1Department of Pharmacy, University Hospital of Besançon, Besançon, France
- 2Host-Graft Interactions Lab – Tumor - Cell and Tissue engineering (UMR 1098 INSERM/UFC/EFS), University of Franche-Comté, Besançon, France
- 3Department of Oral and Maxillofacial Surgery, University Hospital of Besançon, Besançon, France
- 4Department of Pharmacy, APHP, Hôpital Saint-Louis, Paris, France
Since 2007, a new class of biologic products for human use called “advanced therapy medicinal products (ATMP)” have been legally integrated in the European Medical Agency. They consist of recombinant nucleic acid, engineered cells, cells, or tissues. In the United States, ATMP fall under the regulatory framework of biological products and the term “cell and gene therapy product” is used in the legislative and regulatory documents. Potential clinical applications are broad, particularly, in the field of cancer, inherited genetic disease, and regenerative medicine. Indeed, the benefit conferred by CD19 chimeric antigen receptor T cells led to the first engineered cell therapy products to be approved by the Food and Drug Administration (FDA) in 2017. Gene therapy products to treat orphan diseases are also extensively developed with many clinical trials ongoing in the world. Nevertheless, the use of these therapeutic products is complex and requires careful considerations in the terms of regulatory and hospital setting requirements, such as storage, handling, administration, and disposal which justify the implementation of a secured medication circuit. Through this systematic review of the literature, the authors wanted to compile data on the assessment of environmental exposure related to the use of ATMP in healthcare setting to secure their medication circuit. A literature search was conducted on PubMed and Web of Science, and 32 publications dealing with environmental exposure assessment and ATMP were selected. In addition, marketed ATMPs were identified and data regarding the environmental concerns were extracted from product information sections from European Public Assessment Reports (EPAR). The environmental contamination assessments were mainly addressed in the reviews rather than in original articles related to the use of ATMP. Most of the product information sections from EPAR suggested precautions rather than requirements when dealing with environmental consideration following ATMP handling. Nevertheless, these precautions usually remain elusive especially concerning waste disposal and the detection of biological material on the work surfaces, and mainly relate to the genetically modified organisms (GMO) over non-GMO cellular products. Pharmaceutical oversight and adherence to the good preparation practices and good clinical practices are essential to ensure the safe use in term of environmental concern of these new therapeutic products in healthcare setting.
Introduction
Since 2007, a new class of biological products for human use called advanced therapy medicinal products (ATMP) are legally integrated in the European Medicines Agency (EMA) (1). These innovative biotechnological products consist of recombinant nucleic acids and engineered cells or tissues which are at the origin of the complexity of their pre-clinical and clinical development, handling, regulatory framework, and classification (2). In Europe, ATMP are divided into four subcategories known as somatic cell therapy medicinal products, gene therapy medicinal products, tissue engineered products, and combined ATMP (3). In the United States (US), ATMPs also fall under the regulatory framework of biological products but only encompass two subcategories called cellular and gene therapy (CGT) products (2). Indeed, the term “CGT product” is the one used in the US legislative and regulatory documents (4). Potential clinical applications of ATMP are broad, particularly in the field of cancer, inherited genetic diseases, and regenerative medicine (5, 6). More importantly, the use of these products is rapidly expanding in the clinical settings and sometimes they are used as last resort when conventional therapeutic approaches are ineffective (7, 8).
The successful clinical transition from bench to bedside of cellular and gene therapies in the early 2000s led to the start of early phase clinical trials (9, 10). Since, several gene and gene-modified cell-based therapies are approved by the Food and Drug Administration (FDA) and EMA. Imlygic® (talimogene laherparepvec, T-VEC), a genetically modified oncolytic vector, was the second gene therapy product approved in Europe in 2016 (5, 11). Then, the clinical benefit conferred by the CD19 chimeric antigen receptor (CAR)-T cells, led to the first engineered cell therapy products to be approved by the FDA in 2017 (8, 12). Pivotal studies showed a high rate of durable responses and an increase in the global survival despite high grade toxicities (8, 13, 14). These breakthrough in the field of cancer medicine prompted to the clinical development of CAR-T cells for other hematological malignancies, such as multiple myeloma and solid tumors, such as glioblastoma despite their immunosuppressive microenvironment and technological barriers preventing T-cell entry (15, 16). Beyond their successful development in the field of immuno-oncology, ATMP are currently extensively developed in orphan diseases addressing the unmet medical needs (17, 18). Another viral vector, Zolgensma® (onasemnogene abeparvovec), developed in the orphan disease spinal muscular atrophy proved its effectiveness in terms of overall survival, motor function, motor milestone achievements, and motor unit function (19). Furthermore, the development of cellular therapy products is illustrated by the approval of several ATMP in various diseases, such as limbal stem cell deficiency with Holoclar® (ex vivo expanded autologous human corneal epithelial cells containing stem cells), perianal fistulas in Crohn's disease with Alofisel® (Darvadstrocel), and cartilage defect in the knee with Spherox® (spheroids of human autologous matrix associated chondrocytes) (20–22). One common point between the studies involving ATMP is the lack of information concerning the assessment of environmental exposure. The use of these therapeutic products is complex and requires careful considerations in terms of regulatory and hospital setting requirements, such as storage, handling, administration, and disposal which justify the implementation of a secured medication circuit. In the framework of ATMP, the environmental risks are described mainly as the risk of transmission of the gene modified organisms to humans other than the patient, to animals or to the environment at large (23). In Europe, the marketing authorization of ATMP falls under the mandatory scope of a central authorization procedure. Among the data submitted by the developer, an environmental risk assessment (ERA) must be present. The specific guidelines dedicated to genetically modified organism (GMO) (EMEA/CHMP/BWP/473191/2006) for both the clinical trials and marketing authorization have recently been reviewed by Whomsley R. and colleagues (24). ERA for GMO should include six steps that are: (1) the identification of characteristics which may cause adverse effects, (2) the evaluation of the potential consequences of each adverse effect if it occurs, and of the magnitude of each identified consequence, (3) the evaluation of the likelihood of the occurrence of each identified potential adverse effect, (4) the estimation of the risk posed by each identified characteristic of the GMO, (5) the application of management strategies covering the risks from the marketing of the GMO, and (6) the determination of the overall risk of the GMO. These steps should be transposable to the cell therapy medicinal products. Routes through which ATMP could come in contact with the human beings other than the intended patient, or enter the environment, include dispersal of portions of product during normal handling and use; accidental dissemination during handling and use; disposal of unused or waste medicinal product; and dispersal of GMO containing patient excreta. Once released, the GMO may spread, undergo genetic or phenotypic change, compete with existing species, infect tissue, remain latent, reproduce, transfer genetic material to other micro-organisms, transfer genetic material to human beings, animal, or plant species, and degrade. Despite the necessity of ERA in both the clinical trials and marketing authorization, environmental exposure assessment related to ATMP handling in healthcare setting, notably in pharmacy preparation unit dedicated or not to their manipulation, deserves to be considered. Because of the heterogeneity of ATMP, it is difficult to define the general requirements for environmental exposure assessments that are applicable to all of them, apart from a dichotomous classification between the somatic cell therapy and gene therapy medicinal products.
Through this systematic review of the literature, the authors wanted to compile the data on environmental exposure assessment related to ATMP use especially in the healthcare settings to secure their medication circuit.
Materials and Methods
Eligibility Criteria
The population, interventions, comparison, and outcomes (PICO) model was used to formulate the questions for this study: (1) studies that considered environmental exposure assessment related to ATMP use (population), (2) studies dealing with the description of environmental exposure assessment related to ATMP use (interventions), (3) comparison criteria was not applicable, (4) studies that reported how to prevent environmental exposure in the use of ATMP and if there is a risk or not (outcomes).
Search Strategies
We searched Pubmed/Medline and Web of science databases for the studies published from January 1, 2000 to March 31, 2021. Selected keywords and Medical Subject Heading (MeSH) terms were individually selected by means of the National Library of Medicine controlled vocabulary thesaurus used for indexing articles for PubMed. The keywords and MeSH terms were combined to conduct the literature search as described in Table 1. This study was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (25).
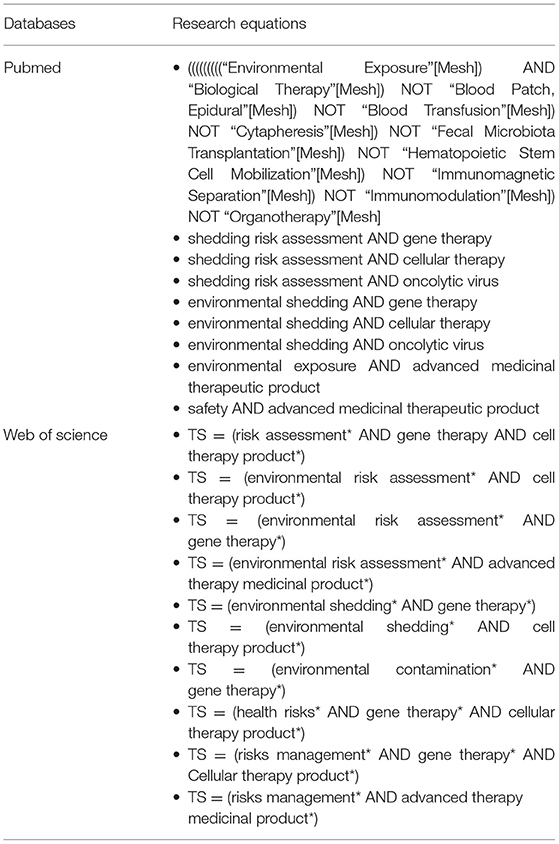
Table 1. The keywords and MeSH terms to conduct the literature search.
Inclusion and Exclusion Criteria
Article reporting environmental concerns related to the use of ATMP in healthcare setting written in English or French were included in this review. Exclusion criteria included translational research using the cells or animals and congress poster.
Study Selection and Data Extraction
The articles were submitted to a public reference manager (Zotero® software) to eliminate the repeated articles. Then, possible relevant articles were screened using the title and abstract by two reviewers (MK and MD) and articles that did not meet the inclusion criteria were excluded. Subsequently, the remaining full-text articles were examined by two reviewers (MK and MD). Any disagreement was resolved through discussion until a consensus was reached. The following items were extracted from each full text article that met the inclusion criteria, if available: year of publication, journal type, main location of first author, sponsor, conflicts of interest (yes, no, and not reported), type of article (original research or literature review), type of ATMP (cellular, gene therapy, and both), aim of the paper, examination of environmental exposure assessment (production, preparation, disposal), what's being watched (ATMP handling, excreta, and not reported), technique use to assess environmental exposure (PCR, sequencing, monitoring, and not reported), regulatory framework (yes or no), how to avoid environmental exposure (quarantined treated patients, disinfectants/decontamination, hygiene measures, sterilization, and not reported), and environmental risk (yes, potential, and not reported). In addition, marketed ATMP were identified and data dealing with environmental concerns were extracted from product information sections from the European Public Assessment Reports (EPAR).
Risk of Bias Assessment
Two reviewers (MK and MD) independently assessed the methodological quality of articles. The selected articles were categorized into three groups: relevant, irrelevant, and unsure. The articles categorized as irrelevant by both the reviewers were eliminated from the study. Second, the full text of each selected article was independently analyzed by both the reviewers that make a list of articles to be included. The two list were compared, and a consensus was found in the case of disagreements between the two reviewers. When an agreement was not reached, a third reviewer made the final decision. The main reason for each article exclusion was recorded.
Additionally, the reference lists of all the selected articles were screened to identify other potentially relevant articles that were not identified by means of the electronic source. Pivotal studies of ATMP actually and previously marketed in Europe and their product information sections from EPAR were screened and analyzed.
Results
Article Selection
The literature search conducted on PubMed and Web of Science identified 708 articles, among which 71 were duplicate articles and 569 were excluded after reviewing the titles and abstracts that did not match the eligibility criteria (Figure 1). A total of 68 articles were included for full text review, among which 42 were excluded because they were off topic, or they did not match the eligibility criteria. Two ATMP pivotal studies have been added (26, 27). Overall, 32 articles were eligible for the present systematic review.
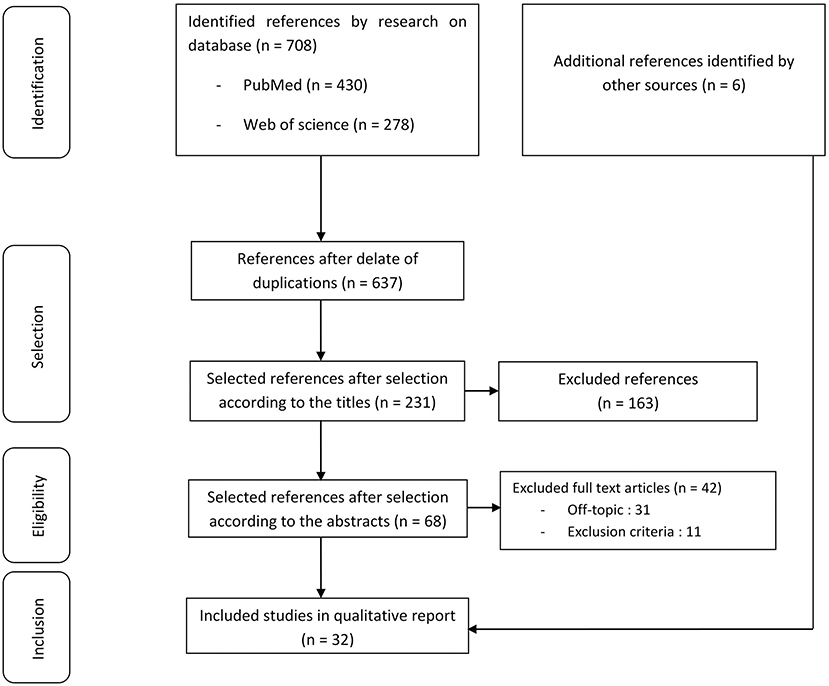
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart for the study selection.
Characteristics of Selected Articles
The characteristics of the 32 selected articles are summarized in Table 2. Few of them were published in the early 2000s, and there has been a considerable increase in the published articles ever since 2010 (75%, n = 24). Only four articles were original research, not including pivotal studies (28–31). Other were mainly state of the art or literature review.
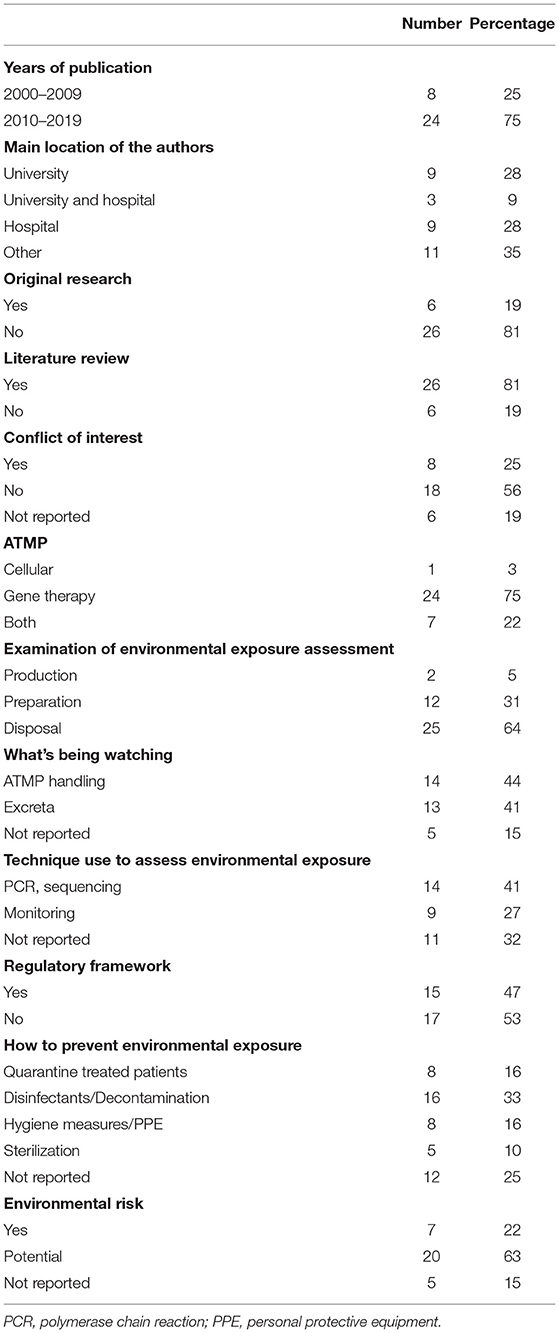
Table 2. Synthesis of basic elements of 32 included articles.
Synthesis of the Basic Elements of Selected Article Dealing With ATMP Environmental Exposure Assessment
The synthesis of basic elements from the 32 selected articles is summarized in Table 3. Among the selected articles, 75% (n = 24) deal with gene therapy and 3% (n = 1) with cellular therapy. Remaining articles concerned ATMP regardless of their classification. Among the selected articles, environmental exposure assessment related to ATMP was examined during manufacturing (5%, n = 2), handling and manipulation (31%, n = 12), and waste disposal (64%, n = 25).
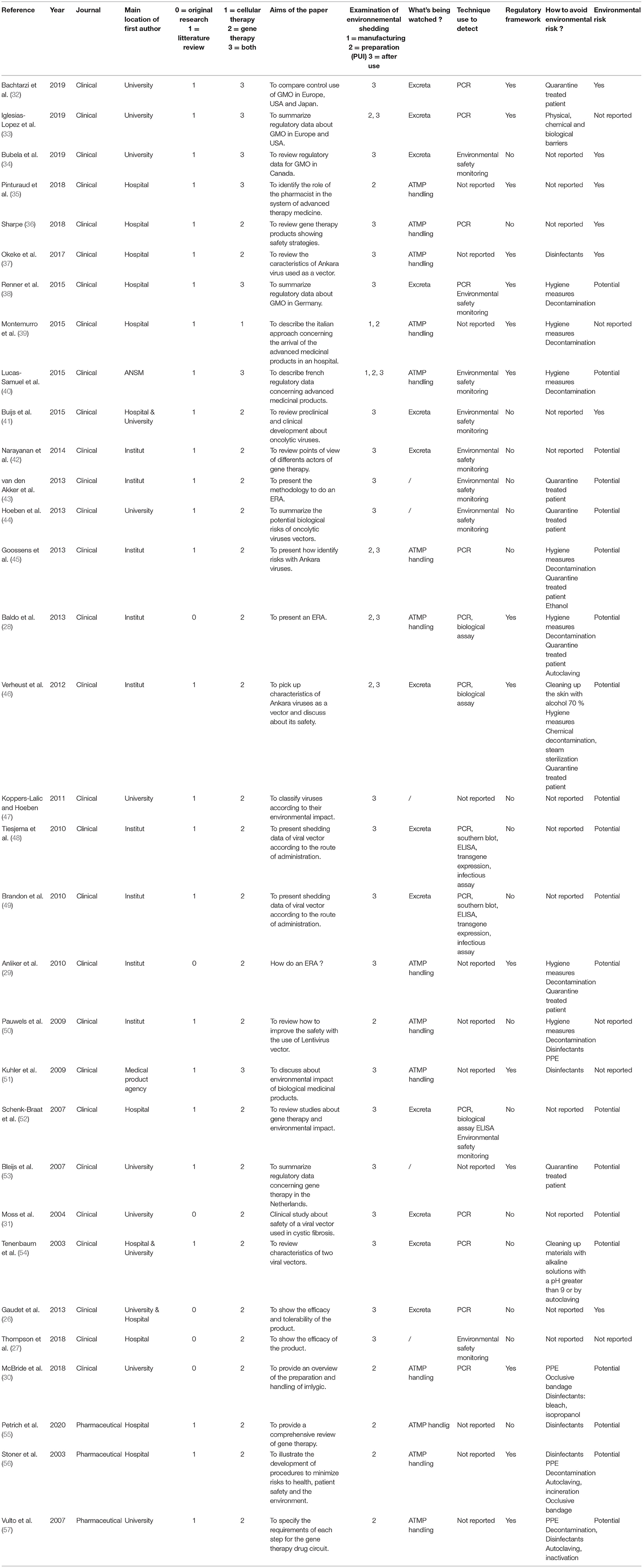
Table 3. The characteristics of the 32 selected articles.
Almost half of the articles (47%, n = 15) involve regulatory framework, such as good manufacturing practices, good preparation practices, and/or European Union (EU) legislation. PCR was used as a main technique to detect ATMP on work surfaces and the excreta or blood of a patient (26, 28, 31–33, 36, 38, 45, 46, 48, 49, 52, 54). The follow-up of a patient after treatment was approached by nine articles to evaluate the potential risk of dissemination of the ATMP (27, 34, 38, 40–44, 52). Yet, different ways of disposal were described to prevent the environmental shedding and quarantine of patients was mainly proposed (n = 8; 16%). Hygiene measures using the disinfectants to decontaminate and clean work surfaces and equipment as sodium hypochlorite, ethanol, or alkaline solutions following the use of ATMP were described (28–30, 33, 37–40, 45, 46, 50, 51, 54–57). Waste sterilization and especially waste autoclaving was addressed within five articles (28, 46, 54, 56, 57). Excreta, such as urine and feces were tested to assess the environmental shedding of ATMP following their administration to the patients (48, 49, 52, 54). Thus, the route of ATMP administration as well as the viral vector characteristics in case of GMO might impact the environmental shedding of ATMP.
Overall, 85% of the selected articles reported a potential environmental risk of dissemination following the use of ATMP. This risk was proven (26, 32, 34–37, 41) or considered to be potential (28–31, 38, 40, 42–49, 52–57) and concerns mainly GMO.
ATMP Product Information Sections From EPAR
Marketed ATMPs in EU are presented in Table 4. Among all EPAR studied (15/15), waste disposal following the local guidelines was recommended. Other information was found inconsistently, such as what to do in case of accidental exposure, the necessity to wear a personal protective equipment during ATMP handling, and the use of certain disinfectants after handling the clean work surfaces.

Table 4. Environmental exposure assessment consideration from the European Public Assessment Reports (EPAR) of advanced therapy medicinal products (ATMP) in Europe.
Discussion
ATMP represent a breakthrough in the field of medicines whose active substance is produced from living tissue and demonstrate the culmination of fundamental research in biotechnology. They provide the opportunity of bringing the most innovative projects coming from translational research to the clinical setting. In line with their medication status, their management in hospital depends on the pharmacies of the hospitals (58). Their complexity and technical specificity in terms of supply, reception, storage, handling, administration, and disposal imply the creation of a dedicated medication circuit. The rapidly growing area of ATMP leads to the implementation of risk minimization measures by the pharmacists to prevent environmental and occupational exposure. This work allowed to establish a state of the art of environmental exposure assessments related to the use of ATMP in healthcare settings through the analysis of both the literature and, for ATMP with marketing authorizations in Europe, their pivotal studies, and their product information section from the EPAR. Through our literature research, 32 articles dealing with the environmental risk assessment of ATMP were selected. Among the 32 articles selected, more than three quarter were published over the last 10 years, demonstrating the rapidly growing area of ATMP.
Two articles addressed the manufacturing step of ATMP in terms of regulatory framework, manufacturing, and quality control guidelines. The manufacturing step mostly focused on environmental concern related to the prevention of cross contamination and the establishment of process and standard operating procedures (SOP) to maintain a clean working environment to protect the ATMP. However, the measures taken to protect the ATMP indirectly apply to protect the environment. Twelve selected articles addressed the preparation steps of the ATMP in healthcare setting. Hygiene measures and decontamination were systematically mentioned with, among others, the use of bactericidal or virucidal agents to prevent environmental shedding. In an original article of McBride, T-VEC handling was presented (30). To prevent environmental shedding, the authors recommended the use of personal protective equipment during T-VEC preparation and administration and the use of disinfectants to clean work and room surfaces exposed to T-VEC. Similar recommendations were made by Stoner N et al. and Pietrich J et al. (55, 56). Nevertheless, the realization of a dedicated test, such as PCR to assess the presence of the GMO following its utilization and cleaning was not suggested. In 2007, Vulto AG et al. published general guidance about gene therapy handling within hospital pharmacy and suggested similar precautions should be taken in the handling of gene medicine and cytotoxic agents, especially concerning the prevention of cross-contamination (57). Unlike antineoplastic drugs, the existence of dedicated kits to assess environmental contamination on the work surfaces were not mentioned. In a study realized by Moss RB et al. that aimed to assess the safety and efficacy of a viral vector for the treatment of cystic fibrosis, the authors analyzed excreta of the patients using PCR assays to assess environmental shedding of the virus (31). Despite detection of the virus in the sputum samples of a patient, no minimal recommendations were proposed by the authors to prevent environmental shedding. Similar observations were related in the study of Baldo et al., which deals with gene therapy having a potential risk of dissemination depending on the vector used (28). According to the authors, it is important to analyze environmental shedding with regards to the capacity of the virus to replicate and resist within “the environment” and to quarantine the treated patients, if necessary. Environmental shedding may also depend on the route of administration of the ATMP. Indeed, Tiesjema et al. indicated that the routes of shedding for HAdV-5 depend on the route of administration (48). In the Glybera® 's (alipogene tiparvovec) pivotal study, the authors specified that following its administration, the treatment may result in a low risk of dissemination in the environment (26). Indeed, the genetically modified viruses were detected in blood, urine, and saliva of the treated patients by qualitative PCR until several weeks following the ATMP injections. Nevertheless, no recommendations regarding the management of these excreta were formalized by the authors. No information concerning storage, handling, the detection of ATMP on the work surfaces and waste disposal were mentioned in original articles from our literature search except for T-VEC (30). As previously described, original research articles mainly deal with investigational medicinal product safety and efficacy.
Most of product information sections from EPAR suggest that specific precautions should be taken regarding environmental consideration following ATMP handling. Thus, in a section entitled “clinical particular,” the summary of product characteristics (SPC) of tisagenlecleucel indicates the precautions that might be taken by the healthcare professionals before handling or administering the medicinal product to prevent transmission. The precautions to be taken during transport and for wastes disposal are also mentioned in a section entitled “Special precautions for disposal and other handling.” Thus, tisagenlecleucel “should be transported within the facility in closed, break-proof, and leak-proof containers.” Waste disposal is not much discussed. Yet, it is advisable to follow the local guidelines for biological wastes disposal. Concerning axicabtagene ciloleucel, the precautions suggested were identical. Overall, there are dedicated precautions for the disposal and handling of CAR-T cells products in the SPC but no information about the risk of surface contamination and product detection were specified. In the T-VEC section “special precautions for disposal and other handling,” recommendations concerning handling and administration, personal protective equipment, accidental spills, and waste disposal were specified. The same recommendations were specified in the product section information for Luxturna® (voretigene neparvovec), onasemnogene abeparvovec, Zolgensma®, Provenge® (Sipuleucel-T), Zalmoxis®, and Strimvelis®. Nevertheless, information still remains elusive especially concerning waste disposal and the detection of medicinal product on work surfaces. Finally, we noticed that the procedure to follow in case of accidental exposure was also detailed in the same section referring to use virucidal agent in case of spill(s). As far as cell therapy is concerned, the environmental exposure assessment is once again a poorly discussed subject. Yet, among cell therapy products, only the SPC of Chondrocelect® specifies, without any further details, that any drug or waste material must be disposed of in accordance with the current regulations.
Management of ATMP is complex, preventing the establishment of a single standardized pharmaceutical circuit for all of them. Furthermore, their specific storage and preparation as well as their classification as GMO or not determine how they need to be handled. Regarding GMO, the assessment of the probability that a potential hazard occurs that determines the level of risk. The level of risk then allows to determine ways to control them to ensure the protection of humans and the environment. As discussed above, antineoplastic drug handling implies a strict aseptic process to prevent cross-contamination within the pharmacy preparation units. Indeed, the experience of pharmacists, justified by the centralization of the reconstitution of antineoplastic drugs, provides an adequate basis for the handling of ATMP in health settings (55, 58, 59). Environmental concern regarding the use ATMP and not only GMO, as previously described, require adaptation in the pharmacies in terms of facilities, equipment, SOP, and waste disposal (57). Storage and manipulation of ATMP need to be performed in a dedicated area. The manipulation of GMO must be conducted in contained cabinet or isolator in negative pressure relative to the pressure of the immediate environment to protect the worker and the environment as well as the product itself. A dedicated high-efficiency particulate air (HEPA) filtering of the extracted air to protect the environment and input air to protect the product is necessary in area of both GMO and non-GMO ATMP manipulation. The establishment of SOP for storage, cleaning, preparation, personal protective clothing dedicated to preparation and administration, transport, accidental exposure, disinfection and decontamination, and disposal of waste is a minimum requirement to prevent environmental shedding. Obviously, these SOPs might be interconnected. Thus, whatever the ATMP, and considering the GMO risk group, disposable personal protective clothing, handling, and administration equipment directly in contact with the ATMP should be autoclaved (sterilization at 134°C during 20–30 min in air saturated with water vapor) if possible, using appropriate sealed container and then incinerated. Non-disposable equipment and material should be cleaned according to institutional SOP and manufacturer instruction to prevent environmental shedding. As mentioned above, the instructions present within EPAR, when they exist, always remain elusive. However, because of their diversity, GMO and especially viruses may have heterogeneous sensitivity to liquid chemical disinfectants. In that context, the recombinant associated viruses that are already used as gene delivery vehicles for approved ATMP have been described as the good virus models for testing the virucidal efficacy of disinfectants. Two studies evaluating the chemical sensitivity of different human adenovirus serotypes have concluded that the inactivation method varies according to each virus serotype demonstrating the need for knowledge and thus providing clear instructions for inactivation methods suitable for each ATMP using a viral vector (60, 61). Additionally, both studies demonstrated that complete inactivation using suitable disinfectants can be done safely and quickly.
This manuscript has several deficiencies. The articles included were limited to English and French only. In addition, the abstract or meeting articles as well as congress posters were excluded although their scientific contribution could have been taken into consideration. This systematic review has not been registered online. Bias due to selective non-reporting (or incomplete reporting) that were measured and analyzed by the trial investigators are likely not to be disclosed. This literature review and data collected from EPAR are biased to published data that may not reflect the actual knowledge on the environmental impact of ATMP. Beyond existing undisclosed data, key considerations, such as dispersal of GMO from patient excreta in the clinical trials may not be known or planned in clinical trial development.
Conclusion
Many challenges remain to be fulfilled in environmental contamination assessment related to the use of ATMP within the pharmacy preparation units, healthcare settings, and beyond. Because the use of these new treatments is a rapidly expanding field with increasing use in the clinical trials and routine practice, the guidelines are eagerly awaited. Even though environmental contamination assessment is poorly addressed in original articles related to the use of ATMP, most of the product information sections from EPAR suggested precautions rather than requirements when dealing with environmental consideration following ATMP handling. Nevertheless, information usually remains elusive especially concerning waste disposal and the detection of biological material on work surfaces, and mainly relate to the GMO than non-GMO cellular products. Pharmaceutical oversight and adherence to good preparation practices and good clinical practices are essential to ensure the safe use of these new therapeutics in healthcare setting in term of environmental concern. Additionally, this work demonstrates the necessity to adopt a multidisciplinary approach involving the clinicians, nurses, pharmacists, and biologists to assess and control environmental exposure to ATMP in the healthcare settings at all steps, from their reception to their administration, and suggest the importance to monitor excreta of a patient during the clinical trials to define recommendations to prevent environmental shedding following their use.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author/s.
Author Contributions
MK and IM: Conceptualization. MK and AL: Methodology. MD, CF-L, and MK: Writing. MK, MD, and AL: Literature search. MD, CF-L, AL, SF, A-LC, SL, and VN: Critically revised work. MK: Supervision. All authors were involved in the design, data collection, analysis, and manuscript preparation.
Funding
This work was supported by the Region Bourgogne Franche-Comté (PERSONALISE, subvention #2019-0077).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank Mihail Turcanu and Camille Hosotte for English writing assistance.
Abbreviations
ATMP, advanced therapy medicinal products; CGT, cellular and gene therapy; EMA, European Medicines Agency; EPAR, European Public Assessment Reports; FDA, Food and Drug Administration; GMO, genetically modified organisms; PCR, polymerase chain reaction; SOP, standard operation procedure; SPC, summary of product characteristics; T-VEC, Talimogene laherparep VEC.
References
1. Journal Officiel de l'Union Européenne (2007). Règlement (CE) n°1394-2007 (L324/121). Available online at: https://eur-lex.europa.eu/legal-content/FR/TXT/PDF/?uri=CELEX:32007R1394
2. Iglesias-López C, Agustí A, Obach M, Vallano A. Regulatory framework for advanced therapy medicinal products in Europe and United States. Front Pharmacol. (2019) 10:921. doi: 10.3389/fphar.2019.00921
3. European Medicines Agency (2015). Reflection paper on classification of advanced therapy medicinal products (EMA/CAT/600280/2010). Available online at: https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-classification-advanced-therapy-medicinal-products_en-0.pdf
4. U.S. Food and Drug Administration (2021). Research C for BE and. Cellular & Gene Therapy Products. Available online at: https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products
5. Carvalho M, Sepodes B, Martins AP. Regulatory and scientific advancements in gene therapy: state-of-the-art of clinical applications and of the supporting European Regulatory Framework. Front Med. (2017) 4:182. doi: 10.3389/fmed.2017.00182
6. Farkas AM, Mariz S, Stoyanova-Beninska V, Celis P, Vamvakas S, et al. Advanced therapy medicinal products for rare diseases: state of play of incentives supporting development in Europe. Front Med. (2017) 4:53. doi: 10.3389/fmed.2017.00053
7. Hoy SM. Onasemnogene abeparvovec: first global approval. Drugs. (2019) 79:1255–62. doi: 10.1007/s40265-019-01162-5
8. Maude SL, Laetsch TW, Buechner J, Rives S, Boyer M, Bittencourt H, et al. Tisagenlecleucel in children and young adults with B- kemia. N Engl J Med. (2018) 378:439–48. doi: 10.1056/NEJMoa1709866
9. Dunbar CE, High KA, Joung JK, Kohn DB, Ozawa K, Sadelain M. Gene therapy comes of age. Science. (2018) 359:eaan4672. doi: 10.1126/science.aan4672
10. Rousseau CF, Mačiulaitis R, Sladowski D, Narayanan G. Cell and gene therapies: european view on challenges in translation and how to address them. Front Med. (2018) 5:158. doi: 10.3389/fmed.2018.00158
11. Andtbacka RHI, Kaufman HL, Collichio F, Amatruda T, Senzer N, Chesney J, et al. Talimogene laherparepvec improves durable response rate in patients with advanced melanoma. J Clin Oncol Off J Am Soc Clin Oncol. (2015) 33:2780–8. doi: 10.1200/JCO.2014.58.3377
12. U.S. Food and Drug Administration (2017). Commissioner O of the. FDA approval brings first gene therapy to the United States. Available online at: https://www.fda.gov/news-events/press-announcements/fda-approval-brings-first-gene-therapy-united-states
13. Locke FL, Ghobadi A, Jacobson CA, Miklos DB, Lekakis LJ, Oluwole OO, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1-2 trial. Lancet Oncol. (2019) 20:31–42. doi: 10.1016/S1470-2045(18)30864-7
14. Schuster SJ, Bishop MR, Tam CS, Waller EK, Borchmann P, McGuirk JP, et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med. (2019) 380:45–56. doi: 10.1056/NEJMoa1804980
15. Martínez Bedoya D, Dutoit V, Migliorini D. Allogeneic CAR T cells: an alternative to overcome challenges of CAR T cell therapy in glioblastoma. Front Immunol. (2021) 12:506. doi: 10.3389/fimmu.2021.640082
16. Munshi NC, Anderson LD, Shah N, Madduri D, Berdeja J, Lonial S, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloMA. N Engl J Med. (2021) 384:705–16. doi: 10.1056/NEJMoa2024850
17. Yu JX, Upadhaya S, Tatake R, Barkalow F, Hubbard-Lucey VM. Cancer cell therapies: the clinical trial landscape. Nat Rev Drug Discov. (2020) 19:583–4. doi: 10.1038/d41573-020-00099-9
18. Aiuti A, Roncarolo MG, Naldini L. Gene therapy for ADA-SCID, the first marketing approval of an ex vivo gene therapy in Europe: paving the road for the next generation of advanced therapy medicinal products. EMBO Mol Med. (2017) 9:737–40. doi: 10.15252/emmm.201707573
19. Al-Zaidy SA, Kolb SJ, Lowes L, Alfano LN, Shell R, Church KR, et al. AVXS-101 (Onasemnogene Abeparvovec) for SMA1. J Neuromusc Dis. (2019) 6: 307–17. doi: 10.3233/JND-190403
20. Rama P, Matuska S, Paganoni G, Spinelli A, De Luca M, Pellegrini G. Limbal stem-cell therapy and long-term corneal regeneration. N Engl J Med. (2010) 363:147–55. doi: 10.1056/NEJMoa0905955
21. Panés J, García-Olmo D, Van Assche G, Colombel JF, Reinisch W, Baumgart DC, et al. Expanded allogeneic adipose-derived mesenchymal stem cells (Cx601) for complex perianal fistulas in Crohn's disease: a phase 3 randomised, double-blind controlled trial. Lancet Lond Engl. (2016) 388:1281–90. doi: 10.1016/S0140-6736(16)31203-X
22. Niemeyer P, Laute V, John T, Becher C, Diehl P, Kolombe T, et al. The effect of cell dose on the early magnetic resonance morphological outcomes of autologous cell implantation for articular cartilage defects in the knee: a randomized clinical trial. Am J Sports Med. (2016) 44:2005–14. doi: 10.1177/0363546516646092
23. European Medicines Agency (2008). Guideline on Scientific Requirements for the Environmental Risk Assessment of Gene Therapy Medicinal Products (EMEA/CHMP/GTWP/125491/2006). Available online at: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-scientific-requirements-environmental-risk-assessment-gene-therapy-medicinal-products_en.pdf
24. Whomsley R, Palmi Reig V, Hidalgo-Simon A. Environmental risk assessment of advanced therapies containing genetically modified organisms in the EU. Br J Clin Pharmacol. (2021) 87:2450–8. doi: 10.1111/bcp.14781
25. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg Lond Engl. (2010) 8:336–41. doi: 10.1016/j.ijsu.2010.02.007
26. Gaudet D, Méthot J, Déry S, Brisson D, Essiembre C, Tremblay G, et al. Efficacy and long-term safety of alipogene tiparvovec (AAV1-LPLS447X) gene therapy for lipoprotein lipase deficiency: an open-label trial. Gene Ther. (2013) 20:361–9. doi: 10.1038/gt.2012.43
27. Thompson AA, Walters MC, Kwiatkowski J, Rasko JEJ, Ribeil J-A, Hongeng S, et al. Gene therapy in patients with transfusion-dependent β-thalassemia. N Engl J Med. (2018) 378:1479–93. doi: 10.1056/NEJMoa1705342
28. Baldo A, van den Akker E, Bergmans HE, Lim F, Pauwels K. General considerations on the biosafety of virus-derived vectors used in gene therapy and vaccination. Curr Gene Ther. (2013) 13:385–94. doi: 10.2174/15665232113136660005
29. Anliker B, Longhurst S, Buchholz CJ. Environmental risk assessment for medicinal products containing genetically modified organisms. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz. (2010) 53:52–7. doi: 10.1007/s00103-009-0986-2
30. McBride A, Valgus J, Parsad S, Sommermann EM, Nunan R. Pharmacy operationalization of the intralesional oncolytic immunotherapy talimogene laherparepvec. Hosp Pharm. (2018) 53:296–302. doi: 10.1177/0018578717749926
31. Moss RB, Rodman D, Spencer LT, Aitken ML, Zeitlin PL, Waltz D, et al. Repeated adeno-associated virus serotype 2 aerosol-mediated cystic fibrosis transmembrane regulator gene transfer to the lungs of patients with cystic fibrosis: a multicenter, double-blind, placebo-controlled trial. Chest. (2004) 125:509–21. doi: 10.1378/chest.125.2.509
32. Bachtarzi H, Farries T. The genetically modified organism medicinal framework in europe, united states, and japan: underlying scientific principles and considerations toward the development of gene therapy and genetically modified cell-based products. Hum Gene Ther Clin Dev. (2019) 30:114–28. doi: 10.1089/humc.2019.042
33. Iglesias-Lopez C, Cortadellas M, Vallano A, Agusti A, Montane Mogas J. Hurdles of environmental risk assessment procedures for advanced therapy medicinal products: comparison between the European Union and the United States. Crit Rev Toxicol. (2019) 49:580–96. doi: 10.1080/10408444.2019.1689380
34. Bubela T, Boch R, Viswanathan S. Recommendations for regulating the environmental risk of shedding for gene therapy and oncolytic viruses in Canada. Front Med. (2019) 6:58. doi: 10.3389/fmed.2019.00058
35. Pinturaud M, Vasseur M, Odou P. Rôle du pharmacien hospitalier dans le circuit d'une catégorie de medicament de thérapie innovante: les lymphocytes T exprimant un récepteur chimérique à l'antigène. Bull Cancer (Paris). (2018) 105 Suppl 2:S205–13. doi: 10.1016/S0007-4551(19)30051-7
36. Sharpe ME. T-cell immunotherapies and the role of nonclinical assessment: the balance between efficacy and pathology. Toxicol Pathol. (2018) 46:131–46. doi: 10.1177/0192623317752101
37. Okeke MI, Okoli AS, Diaz D, Offor C, Oludotun TG, Tryland M, et al. Hazard characterization of modified vaccinia virus ankara vector: what are the knowledge gaps? Viruses-Basel. (2017) 9:318. doi: 10.3390/v9110318
38. Renner M, Anliker B, Sanzenbacher R, Schuele S. Regulation of clinical trials with advanced therapy medicinal products in Germany. Adv Exp Med Biol. (2015) 871:87–101. doi: 10.1007/978-3-319-18618-4_5
39. Montemurro T, Vigano M, Budelli S, Montelatici E, Lavazza C, Marino L, et al. How we make cell therapy in Italy. Drug Des Devel Ther. (2015) 9:4825–34. doi: 10.2147/DDDT.S80403
40. Lucas-Samuel S, Ferry N, Trouvin J-H. Overview of the regulatory oversight implemented by the french regulatory authorities for the clinical investigation of gene therapy and cell therapy products. Adv Exp Med Biol. (2015) 871:73–85. doi: 10.1007/978-3-319-18618-4_4
41. Buijs PRA, Verhagen JHE, van Eijck CHJ, van den Hoogen BG. Oncolytic viruses: from bench to bedside with a focus on safety. Hum Vaccines Immunother. (2015) 11:1573–84. doi: 10.1080/21645515.2015.1037058
42. Narayanan G, Cossu G, Galli MC, Flory E, Ovelgonne H, Salmikangas P, et al. Clinical development of gene therapy needs a tailored approach: a regulatory perspective from the European Union. Hum Gene Ther Clin Dev. (2014) 25:1–6. doi: 10.1089/humc.2013.230
43. van den Akker E, van der Vlugt CJB, Bleijs DA, Bergmans HE. Environmental risk assessment of replication competent viral vectors applied in clinical trials: potential effects of inserted sequences. Curr Gene Ther. (2013) 13:395–412. doi: 10.2174/156652321306140103221621
44. Hoeben RC, Louz D, Koppers-Lalic D. Biosafety of non-human therapeutic viruses in clinical gene therapy. Curr Gene Ther. (2013) 13:492–9. doi: 10.2174/156652321306140103224907
45. Goossens M, Pauwels K, Willemarck N, Breyer D. Environmental risk assessment of clinical trials involving modified vaccinia virus ankara (MVA)-based vectors. Curr Gene Ther. (2013) 13:413–20. doi: 10.2174/156652321306140103221941
46. Verheust C, Goossens M, Pauwels K, Breyer D. Biosafety aspects of modified vaccinia virus Ankara (MVA)-based vectors used for gene therapy or vaccination. Vaccine. (2012) 30:2623–32. doi: 10.1016/j.vaccine.2012.02.016
47. Koppers-Lalic D, Hoeben RC. Non-human viruses developed as therapeutic agent for use in humans. Rev Med Virol. (2011) 21:227–39. doi: 10.1002/rmv.694
48. Tiesjema B, Hermsen HPH, van Eijkeren JCH, Brandon EFA. Effect of administration route on the biodistribution and shedding of replication-deficient HAdV-5: a qualitative modelling approach. Curr Gene Ther. (2010) 10:107–27. doi: 10.2174/156652310791111038
49. Brandon EFA, Hermsen HPH, van Eijkeren JCH, Tiesjema B. Effect of administration route on the biodistribution and shedding of replication-deficient AAV2: a qualitative modelling approach. Curr Gene Ther. (2010) 10:91–106. doi: 10.2174/156652310791111047
50. Pauwels K, Gijsbers R, Toelen J, Schambach A, Willard-Gallo K, Verheust C, et al. State-of-the-art lentiviral vectors for research use: risk assessment and biosafety recommendations. Curr Gene Ther. (2009) 9:459–74. doi: 10.2174/156652309790031120
51. Kuhler TC, Andersson M, Carlin G, Johnsson A, Akerblom L. Do Biological Medicinal Products Pose a Risk to the environment? A Current View on ecopharmacovigilance. Drug Saf. (2009) 32:995–1000. doi: 10.2165/11316540-000000000-00000
52. Schenk-Braat EAM, van Mierlo MMKB, Wagemaker G, Bangma CH, Kaptein LCM. An inventory of shedding data from clinical gene therapy trials. J Gene Med. (2007) 9:910–21. doi: 10.1002/jgm.1096
53. Bleijs R, Haenen I, Bergmans H. Assessment of clinical gene therapy trials and environmental risk analysis. Hum Gene Ther. (2007) 18:1060–1060. doi: 10.1002/jgm.1095
54. Tenenbaum L, Lehtonen E, Monahan PE. Evaluation of risks related to the use of adeno-associated virus-based vectors. Curr Gene Ther. (2003) 3:545–65. doi: 10.2174/1566523034578131
55. Petrich J, Marchese D, Jenkins C, Storey M, Blind J. Gene replacement therapy: a primer for the health-system pharmacist. J Pharm Pract. (2020) 33:846–55. doi: 10.1177/0897190019854962
56. Stoner NS, Gibson RN, Edwards J. Development of procedures to address health and safety issues in the administration of gene therapy within the clinical setting. J Oncol Pharm Pract. (2003) 9:21–35. doi: 10.1191/1078155203jp101oa
57. Vulto AG, Stoner N, Cercos A-C, Hoppe-Tichy T, Genestar JLV, Kontra K, et al. European Association of Hospital Pharmacists (EAHP) guidance on the pharmacy handling of gene medicines. Eur J Hosp Pharm Sci(EAHP). (2007) 13:29–39. Available online at: https://www.genetherapynet.com/download/EAHP-Guideline.pdf
58. Roth RI, Fleischer NM. Gene therapy: applications to pharmacy practice. J Am Pharm Assoc. (2002) 42:694–698. doi: 10.1331/108658002764653478
59. Stoner N. Are UK hospital pharmacy departments ready for the rise of gene therapy medicinal products? Expert Opin Biol Ther. (2018) 18:837–40. doi: 10.1080/14712598.2018.1495192
60. Sauerbrei A, Sehr K, Eichhorn U, Reimer K, Wutzler P. Inactivation of human adenovirus genome by different groups of disinfectants. J Hosp Infect. (2004) 57:67–72. doi: 10.1016/j.jhin.2004.01.029
Keywords: advanced therapy medicinal products (ATMP), cell and gene therapy (CGT), environmental exposure, environmental shedding, cellular therapy, healthcare settings
Citation: Damerval M, Fagnoni-Legat C, Louvrier A, Fischer S, Limat S, Clairet A-L, Nerich V, Madelaine I and Kroemer M (2021) ATMP Environmental Exposure Assessment in European Healthcare Settings: A Systematic Review of the Literature. Front. Med. 8:713047. doi: 10.3389/fmed.2021.713047
Received: 21 May 2021; Accepted: 18 October 2021;
Published: 01 December 2021.
Edited by:
Nuno M. Neves, University of Minho, PortugalReviewed by:
Zhenjian Zhuo, Guangzhou Medical University, ChinaJoaquim Vives, Banc de Sang i Teixits, Spain
Copyright © 2021 Damerval, Fagnoni-Legat, Louvrier, Fischer, Limat, Clairet, Nerich, Madelaine and Kroemer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie Kroemer, bWtyb2VtZXJAY2h1LWJlc2FuY29uLmZy