 Matthieu Bailly1*
Matthieu Bailly1* Frédérique Thibault1Maxime Courtehoux2
Frédérique Thibault1Maxime Courtehoux2 Gilles Metrard1Denis Angoulvant3,4†
Gilles Metrard1Denis Angoulvant3,4† Maria Joao Ribeiro2,5†
Maria Joao Ribeiro2,5†- 1Nuclear Medicine Department, CHR ORLEANS, Orleans, France
- 2Nuclear Medicine Department, CHRU TOURS, Tours, France
- 3Cardiology Department, CHRU TOURS, Tours, France
- 4EA4245 T2i, Tours University, Tours, France
- 5UMR 1253, iBrain, Université de Tours, Inserm, Tours, France
Purpose: The aim of this study was to assess the results of cadmium zinc telluride (CZT)- single-photon emission computed tomography (SPECT) myocardial flow reserve (MFR) in coronary artery disease (CAD) screening regarding clinical risk and its correlation to invasive coronary angiography (ICA).
Methods: A total of 137 patients (61 male and 76 female) referred for CAD screening myocardial perfusion imaging (MPI) between November 2018 and April 2020 were included in the CFR-OR prospective trial. The 10-year risk of cardiovascular death according to the European Society of Cardiology (SCORE) was calculated. SPECT 1-day 99mTc-tetrofosmin protocol was acquired on CZT cardiac-dedicated pinhole cameras. Low-dose thoracic CT was used for coronary calcium score (CCS) evaluation. ICA, when performed within 3 months, was also analyzed.
Results: Mean SCORE and mean global MFR were, respectively, 4 ± 3.1% and 2.50 ± 0.74; 34 patients had impaired CFR (using a threshold of 2). There was a significant inverse correlation between MFR and SCORE (p = 0.006), gender (p = 0.019), and number of cardiovascular risk factors (p = 0.01). MFR was significantly reduced in patients with CCS above 1 (p = 0.01). No significant correlation was found between MFR and individual cardiovascular risk factors (dyslipidemia, hypertension, diabetes, or family history of CAD). A total of 23 patients underwent ICA. Global MFR SPECT sensitivity and specificity were 83.3 and 100 %, respectively, with an area under the curve of 0.94.
Conclusion: Adding MFR to SPECT MPI for CAD screening on CZT camera may contribute to high-risk patient identification and enhance diagnostic performances. MFR could help physician decision to perform ICA.
Introduction
Stress single-photon emission computed tomography (SPECT) myocardial perfusion imaging (MPI) is commonly used for diagnosis and risk stratification of patients with suspected coronary artery disease (CAD) (1). Conventional SPECT MPI, using visual analysis and semi-quantitative parameters, assesses the presence, extent, and degree of myocardial ischemia and/or necrosis.
Myocardial blood flow (MBF) and myocardial flow reserve (MFR), calculated using Positron emission tomography (PET) MPI provide added diagnostic (2, 3) and prognostic (4) information than relative perfusion analysis alone. Cardiac PET is not as widely available as SPECT. The edge of cadmium zinc telluride (CZT) detectors in SPECT allow time–activity curve (TAC) acquisitions without any rotation, with higher sensitivity and temporal resolution (5). Some studies with experimental animal models demonstrated the capability to estimate absolute MBF and MFR estimation by SPECT (6). Several studies have shown that the clinical measurement of MBF and MFR using dynamic CZT-SPECT MPI with 99mTc radiopharmaceuticals is technically possible, resulting in similar MFR when compared to PET (7–10). One potential limit is the unfavorable properties of the currently available flow SPECT tracers, hampering accurate MBF quantification due to non-linear extraction fraction with roll-off at higher flow values.
CZT SPECT MPI quantitative flow parameters in the diagnosis of CAD have not been extensively reported until now. One recent study showed that MBF and MFR provided diagnostic information for patients with suspected or known CAD, in addition to the conventional analysis of qualitative and semi-quantitative parameters (11). We recently reported a case of MPI for CAD screening with normal relative MPI, high calcium score, and strongly impaired MBF and MFR. In this patient, coronary angiography confirmed extended CAD with three-vessel disease (12).
In this study, we prospectively evaluated the clinical correlations of SPECT MFR in patients referred for CAD screening and its correlation to invasive coronary angiography (ICA).
Materials and Methods
Patient Population
From October 2018 to June 2020, 137 patients without known CAD referred for SPECT MPI with MBF and MFR quantification and addressed to two Nuclear Medicine departments were prospectively enrolled in the CFR-OR trial (clinicaltrials.gov unique identifier NCT03586492). Every patient received information and gave informed consent. The study protocol was approved by the local and regional ethics committees (CPP Ouest III), and the procedures were in accordance with the Declaration of Helsinki. The inclusion criterion was CAD screening MPI.
The exclusion criteria included previously known CAD, absolute common contraindication to vasodilators (severe hypotension, second- or third-grade atrioventricular block, and recent myocardial infarction), previous cardiac surgery, pregnancy, or active breastfeeding.
Technical issues were reported for MBF and MFR measurement in two patients (late acquisition after injection) and for CCS evaluation in 35 patients (movement artifacts, CT breakdown). A flow chart of the study is displayed in Figure 1.
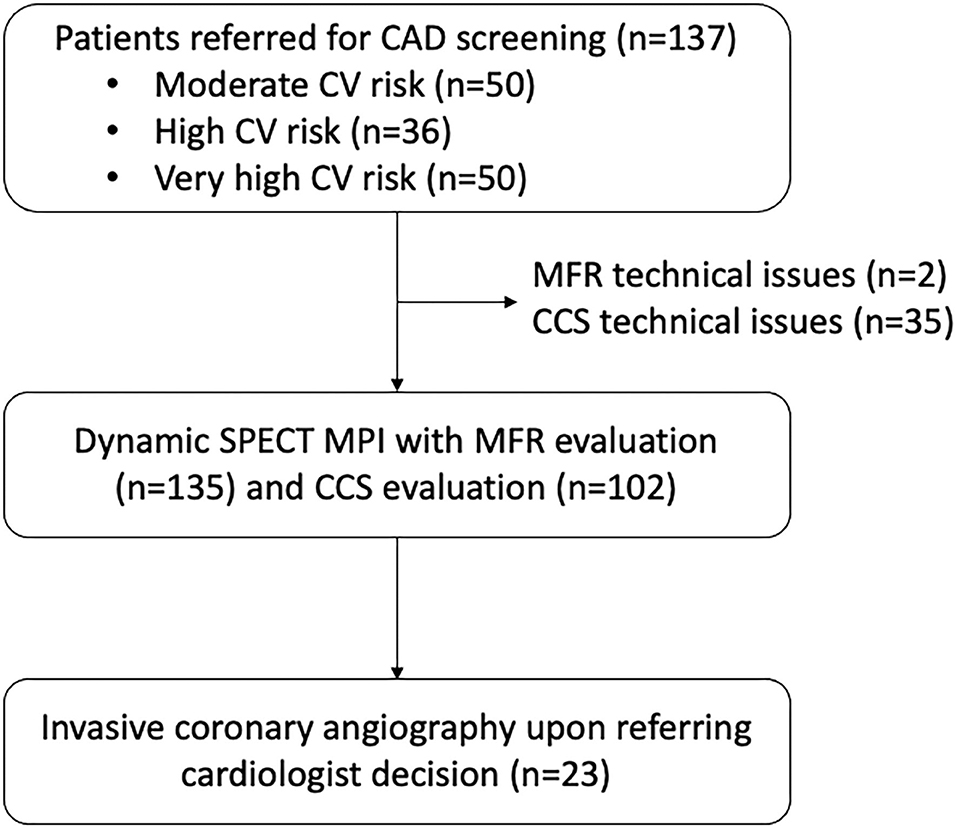
Figure 1. Flow chart of the study.
Estimation of 10-Year Risk of Fatal Cardiovascular Events
A patient's individual estimation of 10-year risk of cardiovascular mortality was assessed using the ESC low-risk regions of Europe SCORE based on age, gender, smoking, systolic blood pressure, and total blood cholesterol concentration (13). Accordingly, very-high-risk patients were defined as having ≥10% risk, with high-risk patients having 5–9% and moderate-risk patients having 3–4%.
SPECT Acquisition
List-mode acquisitions were performed on two same Discovery NM530c cardiac CZT cameras (General Electric Healthcare, Haifa, Israel) in both departments. An initial injection of 37 MBq of 99m Tc-tetrofosmin was used to center the patient's heart in the field of view. Pharmacological stress was then performed using either a regadenoson (400 μg) injection or a dipyridamole perfusion (0.56 mg/kg), immediately followed with 250 MBq of 99mTc-tetrofosmin bolus injection at hyperemia peak and then flushed by 50 ml of saline to ensure the consistent delivery of a tight bolus. Rest dynamic acquisition was realized 3 h later, with a similar injection of 500 MBq of 99mTc-tetrofosmin, in agreement with the recent work of Zoccarato et al. (14). Non-ECG-gated, free-breathing low-dose CT was acquired on a conventional hybrid gamma-camera [Discovery NM670pro hybrid gamma-camera: 120 kV/20–120 mA, pitch 1.375:1, slice 1.25 mm (General Electric Healthcare, Haifa, Israel) or Symbia T2: 130 kV/30 mA, slice 2.5 mm (Siemens Healthineers, Erlangen, Germany)], placing the patient in the same position as on the CZT gamma-camera, with the arms above the head. Those parameters were in agreement with the recent best practices for CT-based attenuation correction (AC) and coronary calcium score (CCS) in nuclear cardiology (15). The procedure timeline is displayed in Figure 2. “Static” acquisitions could consist of supine and/or prone imaging for visual MPI analysis. Visual MPI analysis was performed by nuclear medicine board-certified physicians and checked by the principal investigator. Negative MPI was defined as no perfusion defect and no indirect sign of three-vessel disease (diminution of ejection fraction at stress, transient ischemic dilatation, and right ventricle visualization). No semi-quantitative analysis was performed, but defects (ischemia and/or necrosis when found) were quantified using the 17-segment model.
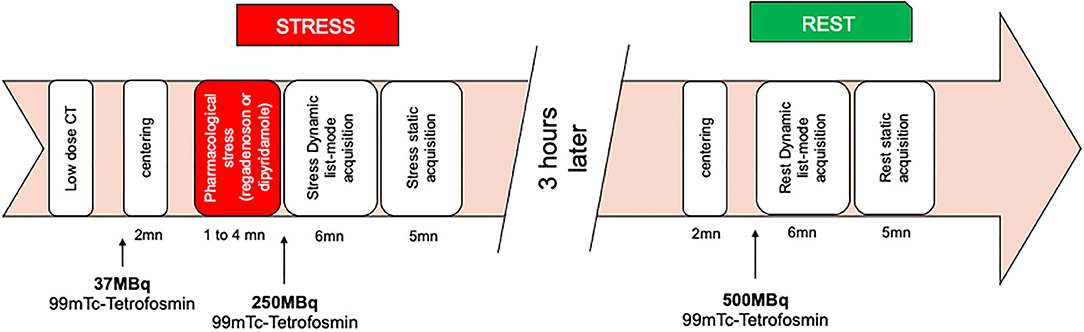
Figure 2. Dynamic cardiac myocardial perfusion imaging protocol.
SPECT MBF and MFR Quantification
Dynamic SPECT was reconstructed using Corridor 4DM(GE) software, v2015.0.2.66 (INVIA, Ann Arbor, MI, USA), on a Xeleris 4DR workstation (General Electric Healthcare, Haifa, Israel). SPECT initial list-mode was resampled into 12 × 10- and 8 × 30-s frames. Endocardial and epicardial left ventricle (LV) surfaces were algorithmically estimated from summed myocardial images after 2-min acquisition time. LV myocardial tissue TACs were nearest-neighbor-sampled at the center of each 460 polar map sectors at the midwall surface, on all time frames. Global and regional [left anterior descending artery (LAD), left circumflex (LCx), right coronary artery (RCA)] TACs were automatically generated by the software. A 3D box region of interest within the LV/left atrium (LA) blood pool was used for MBF estimation, placed on the valve plane, and centered across all time frames by the same physician. This region of interest was designed to sample both the LV and LA cavities (two pixels in width in the short axis and 30 mm in length in the long axis) (16). Retention rate R was calculated using the net retention model of Leppo and Meerdink (17) and Yoshida et al. (18) according to the following equation:
MBF, E, and P(t) were, respectively, the myocardial blood flow, the extraction fraction, and the total myocardial tracer concentration or tissue TAC. Ca(t) represents the arterial concentration of the tracer or blood TAC and PV the partial volume value (set to 0.6). We set the correction factor for myocardial density (CF) to 1. Sm and Sb represented, respectively, the spillover from the blood pool activity to the myocardium estimated from compartmental analysis (Sm set to 0.4) and the spillover from the myocardium to the blood pool activity (assuming this one was negligible, it was set to 0). Integration limits t1, t2, and t3 corresponded to the end of the blood pool phase at 1 min for t1 and to the average tissue activity, from 1 to 2 min for t2 and t3. Those limits were adjusted to the peak of the blood TAC. The uptake rate K1 was related to MBF using the following Renkin–Crone equation according to Leppo (17), where A = 0.874 and B = 0.443:
Because our previous results (19) showed no difference in terms of MFR whether attenuation correction was applied or not, we did not apply it in this study. All MBF and MFR values are presented without attenuation correction.
Coronary Calcium Score Evaluation
CCS was estimated on the low-dose CT as the sum of CCS in the three main coronary arteries according to the method described by Agatston et al. (20). This evaluation was made visually. Horos software was used only for training and to support the visual estimation (free and open-source code software program that is distributed free of charge under the LGPL license at Horosproject.org and sponsored by Nimble Co LLC d/b/a Purview in Annapolis, MD USA). Previous studies demonstrated a high agreement between CCS evaluated on attenuation correction CT for SPECT with the Agatston classical CCS and excellent inter-reader reproducibility (21, 22). The authors recommended that the degree of atherosclerosis should be assessed by means of estimating CCS on the CT for attenuation correction. In this study, the evaluation was performed by the same physician, and CCS score was classified in two categories: 0 CCS score and CCS ≥1.
Invasive Coronary Angiography
ICA was performed upon the referring cardiologist's decision, after the MPI, MBF, and MFR results, according to clinical practice (the fractional flow reserve measurements were left at the angiographer's decision). Coronary angiograms were visually assessed by the experienced interventional cardiologist responsible for the procedure. The angiograms were assessed according to the clinical routine, taking into account available clinical data and patient history. According to the recent ESC guidelines defining very-high-risk patients in need of secondary prevention intervention, we considered all patients with significant coronary artery plaque according to the angiographer's conclusion, i.e., ≥50% narrowing of the diameter of the lumen of the arteries (13).
Statistical Analysis
Continuous variables are presented as means ± standard deviation. Categorical variables are provided as total numbers in percent. Gaussian distribution was assessed using the D'Agostino–Pearson normality test. When analyzing differences between the two groups, we applied independent-sample t-test when comparing continuous variables (SCORE, MFR) and the χ2 test or Fisher's exact test as appropriate when comparing categorical variables (CCS). ANOVA test was performed to compare multiple, not paired, groups with Gaussian distribution (clinical risk, number of risk factors, and CCS). The non-normal distributed variables were analyzed using the Mann–Whitney U test (some small groups regarding micro-albuminuria status or risk factors) and the Kruskal-Wallis test for multiple-group comparisons (MBF and MFR values in three CV risk groups). Pearson's correlation coefficients were computed between variables. Linear regression was used to analyze correlations between MFR, CCS, and other covariates (SCORE). Receiver operating characteristic (ROC) curves were calculated for MFR and stress MBF according to ICA results. p < 0.05 was considered statistically significant. All analyses were performed using Prism 9.
Results
MFR and CCS According to Clinical Findings
A total of 137 patients (61 male and 76 female) were included and classified in the three SCORE-estimated 10-year CV mortality risk groups: 50 moderate, 37 high, and 50 very high (Table 1).
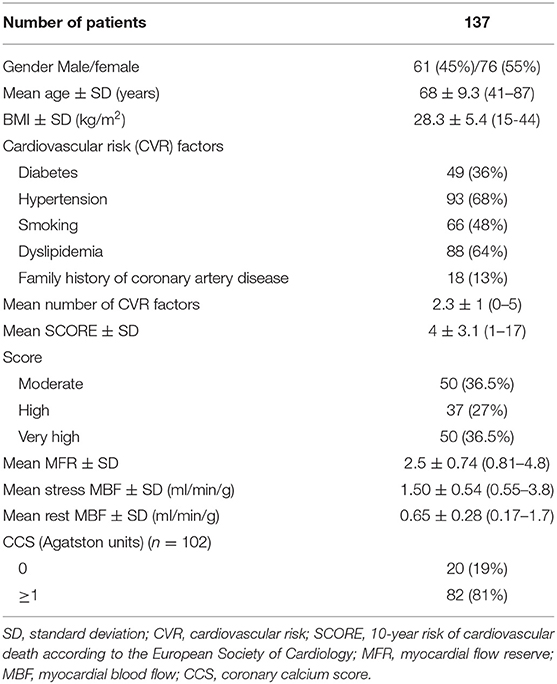
Table 1. Patients' demographics.
Mean SCORE and mean global MFR were, respectively, 4 ± 3.1% and 2.50 ± 0.74. The mean global stress MBF was 1.50 ± 0.54 ml/min/g. There were 35 patients who had impaired CFR (using a threshold of two), but only six of these patients also had impaired visual MPI.
MFR was significantly different between the three CV mortality risk groups (p = 0.03) (Figure 3), being significantly reduced in high- and very-high-risk patients. CCS was not different according to risk categories (p = 0.32) (Table 2).
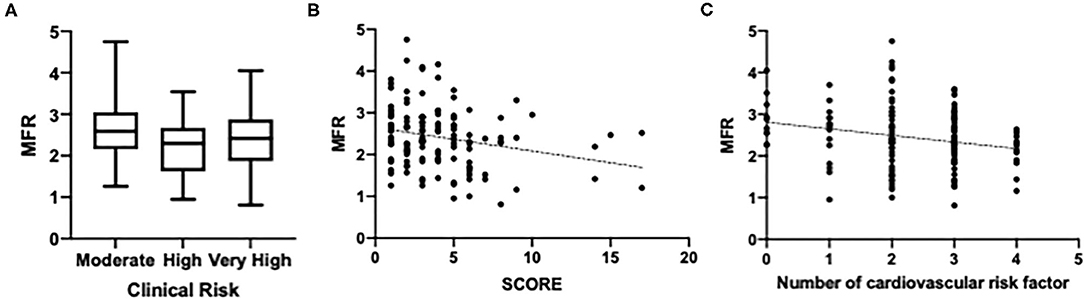
Figure 3. Myocardial flow reserve (MFR) according to clinical risk. (A) MFR according to CV mortality risk groups. (B) MFR correlated to SCORE-estimated 10-year cardiovascular (CV) mortality. (C) MFR correlated to the number of CV risk factors.
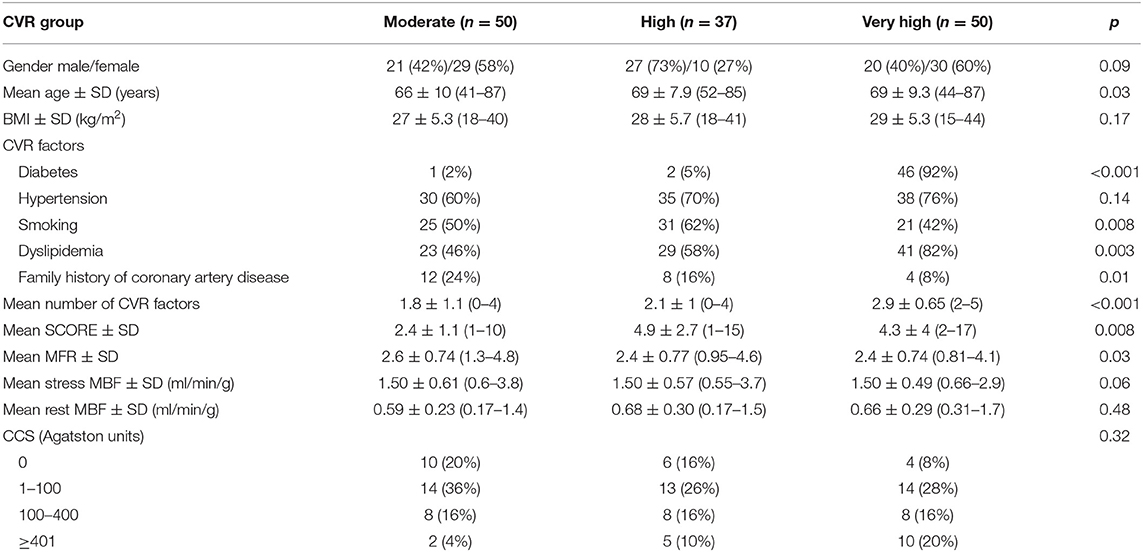
Table 2. Clinical findings, myocardial flow reserve (MFR), and coronary calcium score (CCS) according to cardiovascular risk (CVR) groups.
There was a significant inverse correlation between MFR and SCORE (r = −0.24; p = 0.006), gender (r = −0.20; p = 0.019), and number of cardiovascular risk factors (r = −0.22; p = 0.01). A significant correlation was also found between CCS and SCORE (r = 0.25; p = 0.013) and gender (r = 0.22; p = 0.027). MFR was significantly reduced in patients with CCS ≥1 (p = 0.002) (Figure 4), with a mean global LV. MFR was 2.8 ± 0.67 and 2.3 ± 0.76, respectively, for patients with 0 CCS score and CCS score ≥1.
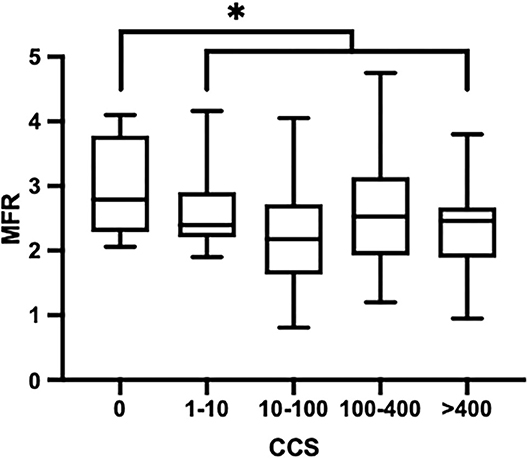
Figure 4. Myocardial flow reserve according to coronary calcium score. *p < 0.05.
Regarding CV risk factors, CCS was significantly higher in smokers (p = 0.05), but we did not find other significant correlations between MFR or CCS and individual risk factors (dyslipidemia, hypertension, diabetes, or family history of coronary artery disease; p of at least 0.18) (Table 3). We noticed a significant inverse correlation between smoking and stress MBF (p = 0.02).
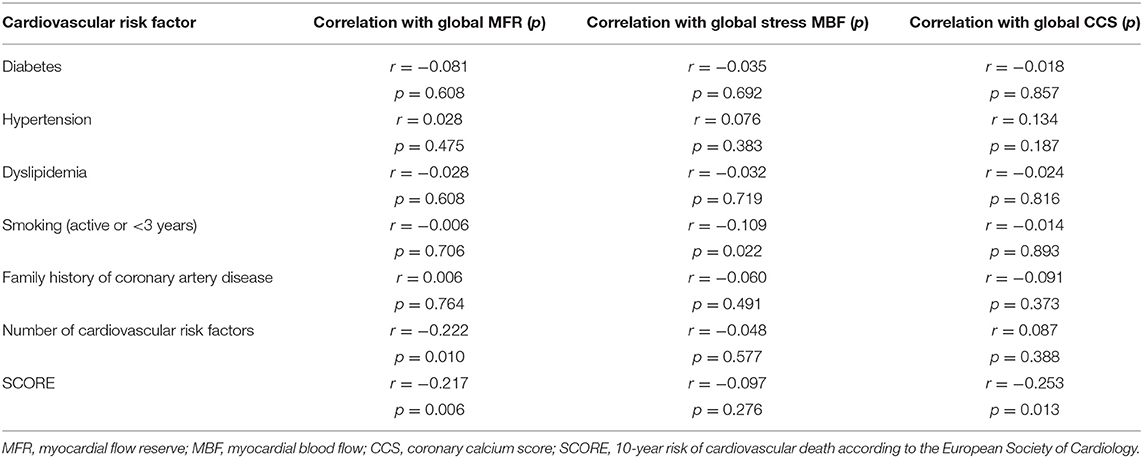
Table 3. Correlation between cardiovascular risk factors, MFR, stress MBF, and CCS.
There were 77 patients who reported cardiovascular symptoms [chest pain (typical or atypical) or dyspnea]. MFR was not significantly different according to symptoms (p = 0.25).
Finally, MFR tend to be reduced in patients with high microalbuminuria (Table 4). Mean global MFR was 2.4 ± 0.76 and 2.2 ± 0.78 when albuminuria/creatinuria ratio was, respectively, ≤20 and >20 mg/g (all of these patients considered with high microalbuminuria were diabetic and/or hypertensive patients).

Table 4. MFR and MBF according to microalbuminuria.
Coronary Angiography Findings
A total of 23 ICA were performed: five were considered normal, 18 showed significant coronary artery plaques qualifying for high-risk patients (four one-vessel, six two-vessel, and eight three-vessel disease). All normal ICA had normal visual MPI, and only one patient had a global MFR <2 (diabetic and symptomatic patient). Considering the 18 patients with significant coronary artery plaques, 16 had impaired MFR (two patients had global and regional MFR >2, but their stenosis was moderate, with negative FFR: 0.9 and 0.95), whereas only four patients had impaired visual MPI (Figure 5). CCS was significantly higher in patients with CAD: 90 ± 150 and 480 ± 660, respectively, for patients without CAD and with CAD (p = 0.02). The mean global MFR was also significantly lower in patients with CAD; stress MBF and MFR were both significantly lower in vessel territories with CAD (Table 5).
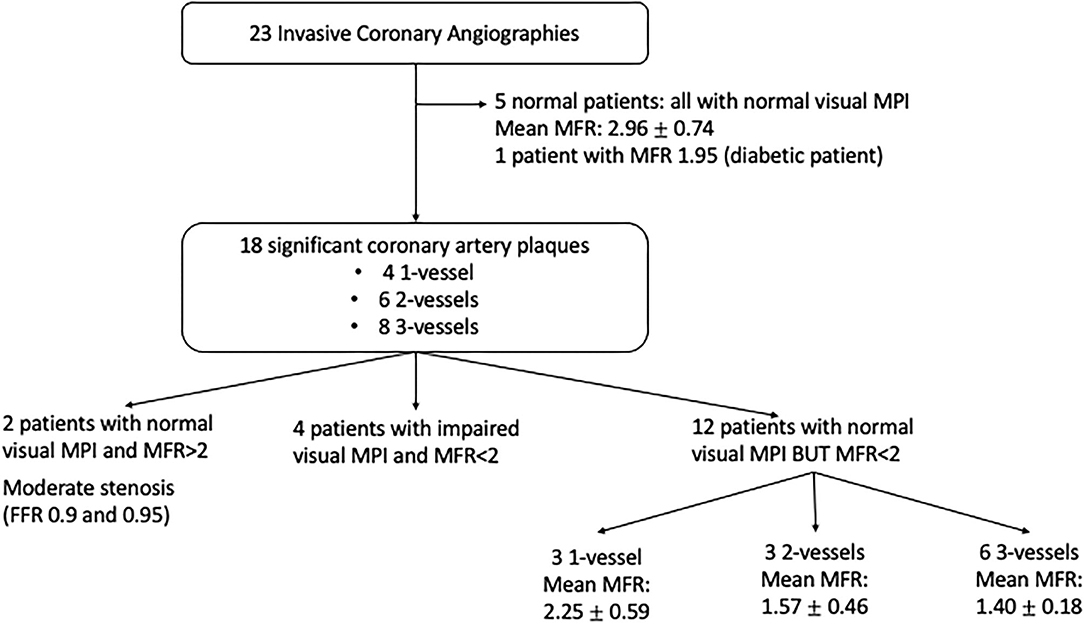
Figure 5. Myocardial perfusion imaging and myocardial flow reserve according to invasive coronary angiography results.

Table 5. MFR and MBF findings in patients with and without obstructive coronary artery disease (CAD).
Based on global MFR and with a threshold of 2, sensitivity and specificity were, respectively, 83.3 and 100%, and area under the curve (AUC) was 0.94 (Figure 6). Regarding regional MFR for the per-vessel analysis, using the same threshold of 2, sensitivity and specificity were, respectively, 85 and 62%, and AUC was 0.79. Based on the ROC curve, the best MFR threshold appeared to be 2.28 on a per-patient analysis, resulting in the best sensitivity and specificity compromise of 88.9% (IC 95%: 67.20–98.03%) and 80% (IC 95%: 37.55–98.87%), with a likelihood ratio of 4.44. The best threshold for regional MFR was 1.92, and this resulted in sensitivity and specificity of 84.4% (IC 95%: 68.25–93.14%) and 56.76% (IC 95%: 40.91–71.33%), with a likelihood ratio of 1.95. Based on global stress MBF, the best threshold appeared to be 1.28, resulting in the best sensitivity and specificity compromise of 61.1% (IC 95%: 38.62–79.69%) and 80% (IC 95%: 37.55–98.87%), with a likelihood ratio of 3.1. The same threshold for regional stress MBF resulted in sensitivity and specificity of 70% (IC 95%: 54.57–81.93%) and 65.52% (IC 95%: 47.35–80.06%), with a likelihood ratio of 2.03.
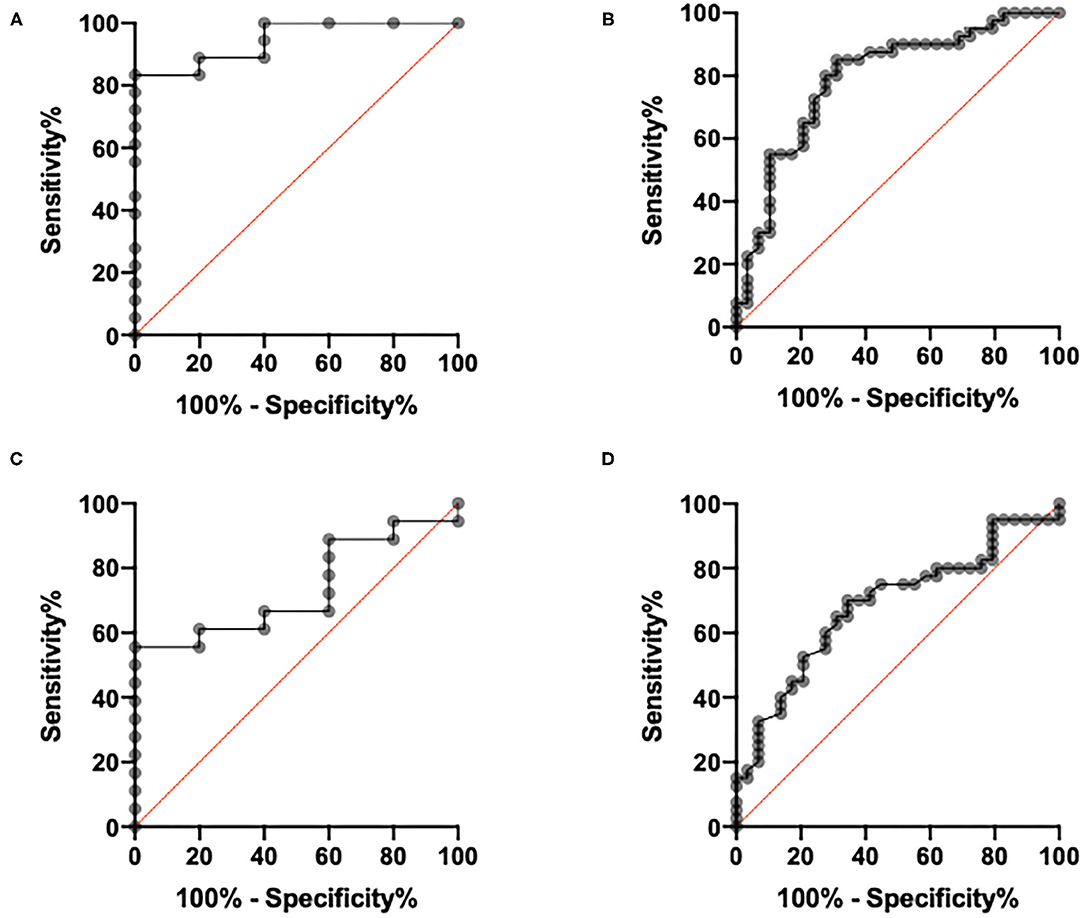
Figure 6. Receiver operating characteristic curves per vessel analysis and per patient analysis. (A) Per patient analysis, based on global myocardial flow reserve (MFR). (B) Per vessel analysis, based on regional MFR. (C) Per patient analysis, based on global stress myocardial blood flow (MBF). (D) Per vessel analysis, based on regional stress MBF.
Discussion
In this study, we found a significant reduction of global SPECT MFR in patients with high SCORE-estimated 10-year CV mortality risk, high number of CV risk factors, and CCS ≥ 1. In addition, our data suggest that global SPECT MFR may be a good predictor of angiographically significant coronary artery lesions.
Our SPECT results are consistent with the reported PET findings. MFR above 2 as assessed by PET has been recognized as a normal value, resulting in a very low rate of cardiac events (4, 23). With an excellent negative predictive value of nearly 1.0, independently of semi-quantitative perfusion results, it could safely exclude patients at high CV risk (24). However, despite of other risk factors, patients with MFR below 1.5 were shown to have a significantly worse prognosis (25). Our findings are also consistent with the recent SPECT studies from Acampa et al. the authors demonstrated a relationship between MPI findings and both hyperemic MBF and MFR obtained by CZT-SPECT, yet global MFR resulted as an independent predictor of CAD, and regional MFR was useful for the identification of obstructive CAD in the corresponding coronary artery. Their best thresholds were 2.6 for global MFR and 2.1 for regional MFR (26).
Although MFR appears to be a strong predictor of cardiovascular mortality, better than stress MBF, it is dependent on both hyperemic and rest flows. For example, low stress MBF with low rest MBF, in case of hibernating myocardium, could result in normal MFR; abnormal MFR could be found with normal stress MBF and high rest MBF. Thus, the integrated assessment of stress MBF and MFR helps to improve diagnostic performances (27, 28). According to our results, the best threshold seemed to be 1.28, but this finding should be put into perspective, knowing the great variability in the described flow values. Our MFR values are similar to other SPECT studies. Giubbini et al., Acampa, and Agostini et al. reported mean global MFR values of 2.18 ± 0.83, 2.44 ± 0.7, 2.60 ± 0.8, and 2.84 ± 0.81, respectively (8–10, 26). Regarding stress MBF values, results from previous works are quite heterogeneous. Our stress MBF values are consistent with those reported by Fang et al., with mean stress MBF of 1.77 ± 0.46 (29), but some authors reported higher values, with mean stress MBF of 3.18 ± 0.95, 2.40 ± 0.7, 3.27 ± 1.1, and 2.3 ± 0.97, respectively, for Agostini et al. (8), Acampa et al. (9, 26), and Giubbini et al. (10), whereas others observed lower values, with stress MBF of 1.11 (interquartile range, IQR: 1.00–1.26) for Nkoulou et al. (7) or 0.67 (IQR, 0.55–0.81) for Zavadovsky et al. (30). This discrepancy between values might result from a lack of standardization in terms of software and corrections (31).
MFR evaluation in SPECT MPI could be considered as an important tool to identify high-risk patients and patients with false negative visual SPECT MPI. Similarly, the SCOTHEART study showed that performing systematic CT coronary angiography in patients referred for CAD screening with suspected angina clearly clarified the diagnostic and resulted in a reduction of fatal and non-fatal coronary events. This helped to identify patients with ongoing CAD even if they were free from ischemia (32). Indeed in those very high-risk patients, pharmacological interventions targeting thrombotic risk and lipid risk were shown to reduce cardiovascular events (13, 33). Aspirin or other antiplatelet drugs are protective in most types of patients who are at an increased risk of atherothrombotic events, including patients with acute myocardial infarction or ischemic stroke, angina (unstable or stable), previous myocardial infarction, stroke or cerebral ischemia, peripheral arterial disease, or atrial fibrillation (34). Its use in primary prevention is more controversial. While in Europe aspirin is not recommended for primary prevention (35), it might be considered in the US (36). Lipid-lowering agents, such as statins, also play a major role in CV prevention. The benefit of lipid-lowering therapy depends on the initial levels of risk; it appears to be greater in patients with a higher risk. There are no differences in the relative reduction between men and women and between younger and older age or between those with and without diabetes (35). Thus, by helping to identify those high-risk patients and improving their prevention strategies, MFR could be a useful tool.
CCS appears to be an independent predictor of CAD (37). It has shown a very high negative predictive value since an Agatston score of 0 has a negative predictive value of nearly 100% for ruling out significant coronary stenosis (38). CCS score and SPECT have already been demonstrated as independent predictors of MACE in patients with suspected coronary artery disease (39). In our study, MFR was significantly reduced in patients with CCS score ≥1. Usually, a CCS score ≥300 Agatston units or ≥75 th percentile for age, sex, and ethnicity is considered to indicate increased CV risk. The Euro-CCAD study showed that the CCS score was a more accurate predictor of significant coronary stenosis than conventional risk factors, with a greater accuracy for predicting >50% stenosis (AUC 0.85) (40). The inclusion of CCS in the Multi-Ethnic Study of Atherosclerosis risk score also offered significant improvements in risk prediction (41). In the European guidelines, CCS scoring should be considered in patients with calculated SCORE risks at around the 5 or 10% thresholds (35). The addition of MFR to CCS could help to better classify patients, especially those with lower or moderate clinical risk.
The combination of MFR, CCS, and myocardial scintigraphy had already been studied by Mentjes et al. (42) and Zampella et al. (43) and showed that the addition of MFR and CCS provided better sensitivity (95%) and better negative predictive value (97%) in the detection of coronary stenosis, supporting the suggestion of Schenker et al. (44) that an imaging approach combining functional and quantitative information offered a clear diagnostic benefit compared to conventional approaches solely based on MPI.
Regarding our dynamic SPECT protocol, we injected 250 and 500 MBq for stress and rest acquisition, respectively, such that even if our total injected dose is higher than those used in some studies [185 and 370 MBq, respectively, at stress and rest for Giubbini et al. (10) and 155 and 370 MBq, respectively, at stress and rest for Acampa et al. (9)], it is still significantly lower than those used by Agostini et al. (3 MBq/kg at rest and 9 MBq/kg at stress) or Nkoulou et al. (330 and 990 MBq) (7, 8). Unlike some authors, our exam protocol consisted in a same-day stress/rest protocol that had the disadvantage of being long for the patients but offered the possibility of multiple prone and/or supine “static” acquisitions, improving the MPI visual image quality by making a definite difference/impact on the inferior wall, with often less digestive uptake or parietal attenuation.
Our study has some limitations that need to be acknowledged; first of all, the small number of patients, especially those having ICA, and the absence of follow-up. Only 102 patients had a successful evaluation of CCS: 89% of the patients scanned in the department equipped with Discovery NM670pro hybrid SPECT and 33% of patients explored in the unit with Symbia T2. This higher failure rate was explained by technological issues inherent to the system technology gap. Then, we have not compared our results to MFR calculated in PET, which remains the gold standard, but as mentioned before, several studies have shown a similar quantification of MBF and MFR using dynamic CZT-SPECT MPI with 99mTc-sestamibi compared to PET (7–10). We also chose to compare our SPECT flow results, which remains a functional test, to an anatomical test used as a reference standard (ICA). This choice may have affected the evaluation of the diagnostic performance of the index test because it is known that the correlation between stenosis severity and myocardial ischemia is poor. The choice to perform ICA or not was left at the cardiologist's decision and might have been influenced by the results of the MPI and flow parameters. Regarding our protocol, the pharmacological stress agent was either dipyridamole or regadenoson, but we previously demonstrated that those two agents induced equivalent hyperemia with similar stress MBF and MFR in comparable patients (45). We did not apply attenuation correction because, in our experience like in other studies, MFR was not different whether it was applied or not (10, 19, 46) and also because most of CZT-SPECT cameras are not equipped with CT, so it may not be achievable in routine. We did not apply motion correction, but before analysis, all our data were screened for motion detection. Finally, we did not perform inter- and intra-observer variability and reproducibility evaluation for MBF and MFR measurements.
Conclusion
In this study, we showed a significant inverse correlation of MFR with SCORE-estimated 10-year CV mortality risk and number of CV risk factors. MFR also showed excellent performances to predict lesions at ICA.
This suggest that MFR evaluation should be added to SPECT in high- and very-high-risk patients. Thus, even without ischemia on MPI, patients with abnormal MFR might be considered as high-risk patients that need to be confirmed by ICA to further benefit from active secondary prevention. Larger studies with clinical follow-up might be useful to confirm our findings.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by CPP Ouest III, France. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MB, MC, and GM contributed to the conception and design of the study. MB and FT analyzed and interpreted the data. MB drafted the manuscript. MR and DA revised it critically for important intellectual content. All authors have contributed to this work and have read and approved the manuscript.
Funding
This study was supported by CHR Orleans.
Conflict of Interest
MB and GM received honoraria and travel grants from General Electric Healthcare (from previous and other works). DA received honoraria and travel grants from Astra Zeneca, MSD, Amgen, Servier, Sanofi, Bayer, BMS, Pfizer, Boehringer, Novartis, and Novo Nordisk (from previous and other works).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We express our deepest gratitude to the cardiologists and the technical and radiopharmaceutical staff from CHR of Orleans and CHRU of Tours. This study is part of the French network of University Hospitals HUGO (Hôpitaux Universitaires du Grand Ouest).
References
1. Hendel RC, Berman DS, Di Carli MF, Heidenreich PA, Henkin RE, Pellikka PA, et al. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 appropriate use criteria for cardiac radionuclide imaging: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the American Society of Nuclear Cardiology, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the Society of Cardiovascular Computed Tomography, the Society for Cardiovascular Magnetic Resonance, and the Society of Nuclear Medicine. Circulation. (2009) 119:e561–87. doi: 10.1161/CIRCULATIONAHA.109.192519
2. Camici PG, Rimoldi OE. The clinical value of myocardial blood flow measurement. J Nucl Med. (2009) 50:1076–87. doi: 10.2967/jnumed.108.054478
3. Valenta I, Dilsizian V, Quercioli A, Ruddy TD, Schindler TH. Quantitative PET/CT measures of myocardial flow reserve and atherosclerosis for cardiac risk assessment and predicting adverse patient outcomes. Curr Cardiol Rep. (2013) 15:344. doi: 10.1007/s11886-012-0344-0
4. Herzog BA, Husmann L, Valenta I, Gaemperli O, Siegrist PT, Tay FM, et al. Long-term prognostic value of 13N-ammonia myocardial perfusion positron emission tomography added value of coronary flow reserve. J Am Coll Cardiol. (2009) 54:150–6. doi: 10.1016/j.jacc.2009.02.069
5. Bocher M, Blevis IM, Tsukerman L, Shrem Y, Kovalski G, Volokh L. A fast cardiac gamma camera with dynamic SPECT capabilities: design, system validation and future potential. Eur J Nucl Med Mol Imaging. (2010) 37:1887–902. doi: 10.1007/s00259-010-1488-z
6. Wells RG, Timmins R, Klein R, Lockwood J, Marvin B, deKemp RA, et al. Dynamic SPECT measurement of absolute myocardial blood flow in a porcine model. J Nucl Med. (2014) 55:1685–91. doi: 10.2967/jnumed.114.139782
7. Nkoulou R, Fuchs TA, Pazhenkottil AP, Kuest SM, Ghadri JR, Stehli J, et al. Absolute myocardial blood flow and flow reserve assessed by gated spect with cadmium-zinc-telluride detectors using 99mTc-tetrofosmin: head-to-head comparison with 13N-Ammonia PET. J Nucl Med. (2016) 57:1887–92. doi: 10.2967/jnumed.115.165498
8. Agostini D, Roule V, Nganoa C, Roth N, Baavour R, Parienti JJ, et al. First validation of myocardial flow reserve assessed by dynamic (99m)Tc-sestamibi CZT-SPECT camera: head to head comparison with (15)O-water PET and fractional flow reserve in patients with suspected coronary artery disease. The WATERDAY study. Eur J Nucl Med Mol Imaging. (2018) 45:1079–90. doi: 10.1007/s00259-018-3958-7
9. Acampa W, Zampella E, Assante R, Genova A, De Simini G, Mannarino T, et al. Quantification of myocardial perfusion reserve by CZT-SPECT: a head to head comparison with (82)Rubidium PET imaging. J Nucl Cardiol. (2020). doi: 10.1007/s12350-020-02129-w. [Epub ahead of print].
10. Giubbini R, Bertoli M, Durmo R, Bonacina M, Peli A, Faggiano I, et al. Comparison between N(13)NH3-PET and (99m)Tc-Tetrofosmin-CZT SPECT in the evaluation of absolute myocardial blood flow and flow reserve. J Nucl Cardiol. (2019). doi: 10.1007/s12350-019-01939-x. [Epub ahead of print].
11. Pang Z, Wang J, Li S, Chen Y, Wang X, Li J. Diagnostic analysis of new quantitative parameters of low-dose dynamic myocardial perfusion imaging with CZT SPECT in the detection of suspected or known coronary artery disease. Int J Cardiovasc Imaging. (2020) 37:367–78. doi: 10.1007/s10554-020-01962-x
12. Bailly M, Thibault F, Courtehoux M, Metrard G, Ribeiro MJ. Added value of myocardial blood flow quantification and calcium scoring during CZT SPECT myocardial perfusion imaging for coronary artery disease screening. Clin Nucl Med. (2019) 44:e617–e9. doi: 10.1097/RLU.0000000000002709
13. Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J. (2019) 41:111–88. doi: 10.1093/eurheartj/ehz826
14. Zoccarato O, Matheoud R, Lecchi M, Scabbio C, Claudio M, Brambilla M. Optimal (99m)Tc activity ratio in the single-day stress-rest myocardial perfusion imaging protocol: a multi-SPECT phantom study. J Nucl Cardiol. (2021) 28:338–49. doi: 10.1007/s12350-020-02290-2
15. Camoni L, Santos A, Attard M, Mada MO, Pietrzak AK, Rac S, et al. Best practice for the nuclear medicine technologist in CT-based attenuation correction and calcium score for nuclear cardiology. Eur J Hybrid Imaging. (2020) 4:11. doi: 10.1186/s41824-020-00080-0
16. Lortie M, Beanlands RS, Yoshinaga K, Klein R, Dasilva JN, DeKemp RA. Quantification of myocardial blood flow with 82Rb dynamic PET imaging. Eur J Nucl Med Mol Imaging. (2007) 34:1765–74. doi: 10.1007/s00259-007-0478-2
17. Leppo JA, Meerdink DJ. Comparison of the myocardial uptake of a technetium-labeled isonitrile analogue and thallium. Circ Res. (1989) 65:632–9. doi: 10.1161/01.RES.65.3.632
18. Yoshida K, Mullani N, Gould KL. Coronary flow and flow reserve by PET simplified for clinical applications using rubidium-82 or nitrogen-13-ammonia. J Nucl Med. (1996) 37:1701–12.
19. Bailly M, Thibault F, Courtehoux M, Metrard G, Ribeiro MJ. Impact of attenuation correction for CZT-SPECT measurement of myocardial blood flow. J Nucl Cardiol. (2020). doi: 10.1007/s12350-020-02075-7. [Epub ahead of print].
20. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. (1990) 15:827–32. doi: 10.1016/0735-1097(90)90282-T
21. Engbers EM, Timmer JR, Mouden M, Jager PL, Knollema S, Oostdijk AH, et al. Visual estimation of coronary calcium on computed tomography for attenuation correction. J Cardiovasc Comput Tomogr. (2016) 10:327–9. doi: 10.1016/j.jcct.2016.04.002
22. Einstein AJ, Johnson LL, Bokhari S, Son J, Thompson RC, Bateman TM, et al. Agreement of visual estimation of coronary artery calcium from low-dose CT attenuation correction scans in hybrid PET/CT and SPECT/CT with standard Agatston score. J Am Coll Cardiol. (2010) 56:1914–21. doi: 10.1016/j.jacc.2010.05.057
23. Ziadi MC, Dekemp RA, Williams KA, Guo A, Chow BJ, Renaud JM, et al. Impaired myocardial flow reserve on rubidium-82 positron emission tomography imaging predicts adverse outcomes in patients assessed for myocardial ischemia. J Am Coll Cardiol. (2011) 58:740–8. doi: 10.1016/j.jacc.2011.01.065
24. Naya M, Murthy VL, Taqueti VR, Foster CR, Klein J, Garber M, et al. Preserved coronary flow reserve effectively excludes high-risk coronary artery disease on angiography. J Nucl Med. (2014) 55:248–55. doi: 10.2967/jnumed.113.121442
25. Murthy VL, Naya M, Foster CR, Hainer J, Gaber M, Di Carli G, et al. Improved cardiac risk assessment with noninvasive measures of coronary flow reserve. Circulation. (2011) 124:2215–24. doi: 10.1161/CIRCULATIONAHA.111.050427
26. Acampa W, Assante R, Mannarino T, Zampella E, D'Antonio A, Buongiorno P, et al. Low-dose dynamic myocardial perfusion imaging by CZT-SPECT in the identification of obstructive coronary artery disease. Eur J Nucl Med Mol Imaging. (2020) 47:1705–12. doi: 10.1007/s00259-019-04644-6
27. Cho SG, Lee SJ, Na MH, Choi YY, Bom HH. Comparison of diagnostic accuracy of PET-derived myocardial blood flow parameters: a meta-analysis. J Nucl Cardiol. (2018) 27:1955–66. doi: 10.1007/s12350-018-01476-z
28. Gupta A, Taqueti VR, van de Hoef TP, Bajaj NS, Bravo PE, Murthy VL, et al. Integrated noninvasive physiological assessment of coronary circulatory function and impact on cardiovascular mortality in patients with stable coronary artery disease. Circulation. (2017) 136:2325–36. doi: 10.1161/CIRCULATIONAHA.117.029992
29. Fang YD, Liu YC, Ho KC, Kuo FC, Yang CF, Yen TC, et al. Single-scan rest/stress imaging with 99mTc-Sestamibi and cadmium zinc telluride-based SPECT for hyperemic flow quantification: A feasibility study evaluated with cardiac magnetic resonance imaging. PLoS ONE. (2017) 12:e0183402. doi: 10.1371/journal.pone.0183402
30. Zavadovsky KV, Mochula AV, Boshchenko AA, Vrublevsky AV, Baev AE, Krylov AL, et al. Absolute myocardial blood flows derived by dynamic CZT scan vs invasive fractional flow reserve: correlation and accuracy. J Nucl Cardiol. (2019) volume 28:249–59. doi: 10.1007/s12350-019-01678-z
31. Giubbini R, Cerudelli E, Camoni L. Myocardial blood flow reserve and absolute myocardial blood flow for the assessment of patients with coronary artery disease with or without microvascular dysfunction. J Nucl Cardiol. (2020). doi: 10.1007/s12350-020-02297-9. [Epub ahead of print].
32. investigators S-H. CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet. (2015) 385:2383–91. doi: 10.1016/S0140-6736(15)60291-4
33. Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. (2020) 41:407–77. doi: 10.1093/eurheartj/ehz425
34. Antithrombotic Trialists C. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. (2002) 324:71–86. doi: 10.1136/bmj.324.7329.71
35. Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the sixth joint task force of the european society of cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. (2016) 37:2315–81. doi: 10.1093/eurheartj/ehw106
36. Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. (2019) 74:1376–414. doi: 10.1016/j.jacc.2019.03.009
37. Hecht HS, Superko HR. Electron beam tomography and National Cholesterol Education Program guidelines in asymptomatic women. J Am Coll Cardiol. (2001) 37:1506–11. doi: 10.1016/S0735-1097(01)01211-6
38. Haberl R, Becker A, Leber A, Knez A, Becker C, Lang C, et al. Correlation of coronary calcification and angiographically documented stenoses in patients with suspected coronary artery disease: results of 1,764 patients. J Am Coll Cardiol. (2001) 37:451–7. doi: 10.1016/S0735-1097(00)01119-0
39. Engbers EM, Timmer JR, Mouden M, Knollema S, Jager PL, Ottervanger JP. Prognostic value of myocardial perfusion imaging with a Cadmium-Zinc-Telluride SPECT camera in patients suspected of having coronary artery disease. J Nucl Med. (2017) 58:1459–63. doi: 10.2967/jnumed.116.188516
40. Nicoll R, Wiklund U, Zhao Y, Diederichsen A, Mickley H, Ovrehus K, et al. The coronary calcium score is a more accurate predictor of significant coronary stenosis than conventional risk factors in symptomatic patients: Euro-CCAD study. Int J Cardiol. (2016) 207:13–9. doi: 10.1016/j.ijcard.2016.01.056
41. McClelland RL, Jorgensen NW, Budoff M, Blaha MJ, Post WS, Kronmal RA, et al. 10-year coronary heart disease risk prediction using coronary artery calcium and traditional risk factors: derivation in the MESA (Multi-Ethnic Study of Atherosclerosis) With Validation in the HNR (Heinz Nixdorf Recall) study and the DHS (Dallas Heart Study). J Am Coll Cardiol. (2015) 66:1643–53. doi: 10.1016/j.jacc.2015.08.035
42. Meintjes M, Sathekge M, Makanjee CR, Dickson JC, Endozo R, Rheeder P, et al. Comparison of rubidium-82 myocardial blood flow quantification with coronary calcium score for evaluation of coronary artery stenosis. Nucl Med Commun. (2016) 37:197–206. doi: 10.1097/MNM.0000000000000410
43. Zampella E, Acampa W, Assante R, Nappi C, Gaudieri V, Mainolfi CG, et al. Combined evaluation of regional coronary artery calcium and myocardial perfusion by (82)Rb PET/CT in the identification of obstructive coronary artery disease. Eur J Nucl Med Mol Imaging. (2018) 45:521–9. doi: 10.1007/s00259-018-3935-1
44. Schenker MP, Dorbala S, Hong EC, Rybicki FJ, Hachamovitch R, Kwong RY, et al. Interrelation of coronary calcification, myocardial ischemia, and outcomes in patients with intermediate likelihood of coronary artery disease: a combined positron emission tomography/computed tomography study. Circulation. (2008) 117:1693–700. doi: 10.1161/CIRCULATIONAHA.107.717512
45. Brana Q, Thibault F, Courtehoux M, Metrard G, Ribeiro MJ, Angoulvant D, et al. Regadenoson versus dipyridamole: Evaluation of stress myocardial blood flow response on a CZT-SPECT camera. J Nucl Cardiol. (2020). Epub 2020/07/12. doi: 10.1007/s12350-020-02271-5. [Epub ahead of print].
Keywords: myocardial blood flow, myocardial flow reserve, CZT-SPECT, cardiovascular risk, invasive coronary angiography
Citation: Bailly M, Thibault F, Courtehoux M, Metrard G, Angoulvant D and Ribeiro MJ (2021) Myocardial Flow Reserve Measurement During CZT-SPECT Perfusion Imaging for Coronary Artery Disease Screening: Correlation With Clinical Findings and Invasive Coronary Angiography—The CFR-OR Study. Front. Med. 8:691893. doi: 10.3389/fmed.2021.691893
Received: 07 April 2021; Accepted: 03 May 2021;
Published: 04 June 2021.
Edited by:
Domenico Albano, University of Brescia, ItalyReviewed by:
Luca Camoni, University of Brescia, ItalyRoberta Assante, University of Naples Federico II, Italy
Yen-Wen Wu, Far Eastern Memorial Hospital (FEMH), Taiwan
Copyright © 2021 Bailly, Thibault, Courtehoux, Metrard, Angoulvant and Ribeiro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthieu Bailly, bWF0dGhpZXUuYmFpbGx5QGNoci1vcmxlYW5zLmZy; orcid.org/0000-0001-6526-0813
†These authors have contributed equally to this work and share senior authorship