
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Med. , 19 August 2021
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.675282
This article is part of the Research Topic Infectious Disease Surveillance: Applying Cooperative Research to Recent Outbreaks including COVID-19 View all 50 articles
 Matias Moragas1
Matias Moragas1 Sandra Gomez2María Florencia Fernández1Marcelo Dario Golemba1
Sandra Gomez2María Florencia Fernández1Marcelo Dario Golemba1 Marcela Palladino3Daniela Borgnia1
Marcela Palladino3Daniela Borgnia1 Silvina Ruvinsky2Lidia Fraquelli4Ana Buchovsky5
Silvina Ruvinsky2Lidia Fraquelli4Ana Buchovsky5 Rosa Bologna2
Rosa Bologna2 Andrea Mangano1*
Andrea Mangano1*Coronavirus disease 2019 (COVID-19) is spreading throughout the world. Limited data are available for the dynamics of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) viral load (VL) in immunocompromised pediatric patients. Here, we report the clinical characteristics and the dynamics of SARS-CoV-2 VL of a pediatric patient with acute myeloid leukemia who developed a hyperinflammatory status mimicked MIS-C. The clinical course was characterized by the late onset of fever, GI symptoms, rash, and respiratory distress, including oxygen requirement with sustained VL of SARS-CoV-2 around 7 log10 RNA copies/mL for 6 weeks. It is important to note that the hyperinflammatory status developed early at the third week of hospitalization—in a context of high VL and immunocompromised status. All these characteristics make this clinical case unique. On the other hand, while many reports have characterized the dynamics of SARS-CoV-2 VL in adults and immunocompetent hosts, it remains unreported in pediatrics—even less in immunosuppressed children.
In April 2020, serious cases of children with systemic hyperinflammatory status with a temporary association with SARS-CoV-2 infection were reported in the United Kingdom (UK) (1). Since then, pediatric cases with a similar condition have been reported in Europe, South Africa, and America (2–4). This entity identified as multisystem inflammatory syndrome in children (MIS-C) has a spectrum of manifestations similar to Kawasaki disease, toxic shock syndrome, sepsis, and macrophage activation syndrome. The World Health Organization (WHO), the Center for Disease Prevention and Control (CDC), and the Royal College of Pediatrics and Child Health (RCPCH) in the UK issued definitions for case identification (5–7). Although MIS-Cs were reported in immunocompetent patients, so far there are no records in the literature about this condition in immunosuppressed children.
Here, we report a case of an immunosuppressed child who developed a hyperinflammatory status temporally associated with SARS-CoV-2 infection in the presence of sustained high viral load (VL).
A 3-year-old male patient diagnosed with M7 acute myeloid leukemia in January 2020 in Paraguay was admitted to the Hospital de Pediatria Garrahan (Buenos Aires, Argentina) in February 2020 for treatment and follow-up. By the end of July, the child had completed the first and second intensification block of chemotherapy with cytarabine and etoposide to keep the patient in complete remission, awaiting a bone marrow transplant. On August 4th, due to a close contact with a person with COVID-19, the child and his mother were tested. A reverse-transcriptase–polymerase-chain-reaction (RT-PCR) assay for SARS-CoV-2 in nasopharyngeal swab specimen was performed with detectable results in both cases. The child was asymptomatic for COVID-19, but he was immediately hospitalized for isolation following national health policies at that time.
The child remained asymptomatic for 28 days, when beginning with febrile neutropenia. Peripheral blood and urine cultures were negative for bacterial and fungal infection. Galactomannan antigen tests in serum were negative. Other respiratory viruses including influenza A and B, adenovirus, parainfluenza 1, 2, 3, and 4, respiratory syncytial virus, metapneumovirus, rhinovirus, enterovirus, and pan-coronavirus (NL63, 229E, OC43, and HKU1) were also negative by molecular tests. He started broad-spectrum antibiotic treatment with piperacillin tazobactam associated with amikacin. On day 31, the child started coughing and had dysphonia. Twenty-four hours later, he started getting abdominal pain, diarrhea, and a maculopapular rash affecting the face and high upper thoracic area without compromised hand and feet. Laboratory tests showed that pancytopenia (white blood cells 100/mm3, hemoglobin 6.2 g/dl, platelets 8,000/mm3), fibrinogen 526 mg/dl, ferritin 4489.3 ng/ml, CPK (creatine phosphokinase) 14 UI/l, NT-PROBNP (N-terminal portion of pro-B-type natriuretic peptide) 226 pg/ml, C-reactive protein 136.14 mg/l, procalcitonin 1.22 ng/ml, normal hepatogram, and anti SARS-CoV-2 antibodies were negative. Detailed laboratory markers are shown in Table 1. No evidence of coagulopathy was shown. Myocardial dysfunction, pericarditis, valvulitis, or coronary abnormalities were discarded by echocardiography. In the presence of high inflammatory laboratory markers, acute SARS-CoV-2 severe infection or MIS-C was suspected. Gamma globulin treatment with a dose of 2 g/kg was immediately administered.
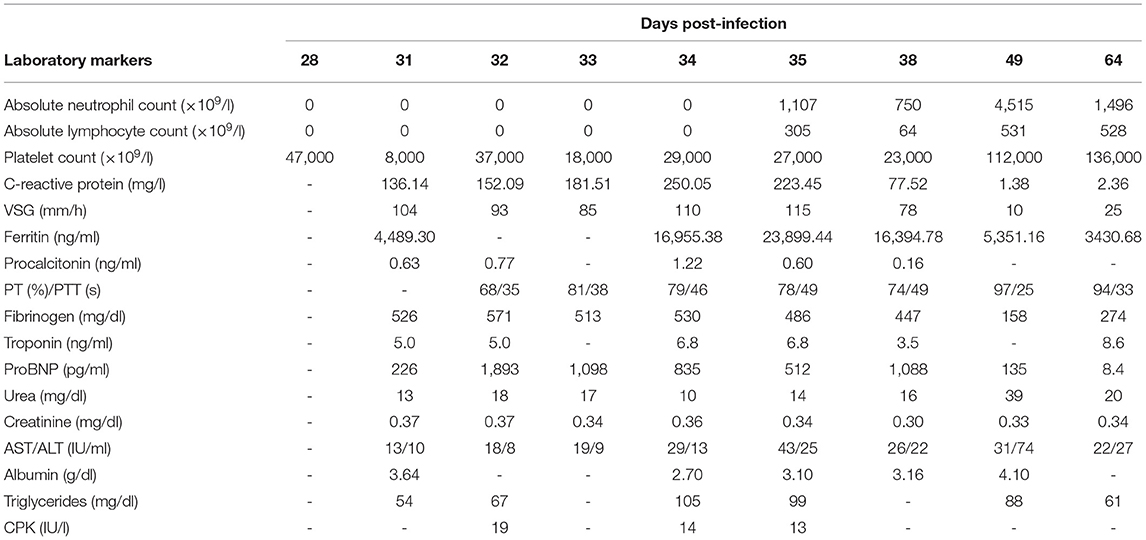
Table 1. Laboratory characteristics along SARS-CoV-2 infection.
On day 33, febrile neutropenia persisted, and the child started bronchospasms and hypoxemia requiring oxygen therapy by nasal cannula. Blood cultures were performed, and antibiotics were switched to meropenem, vancomycin, and lipid formulation of amphotericin B. A chest CT scan showed (i) patched areas of airspace occupation with confluent sectors and ground glass opacity in both upper lobes and (ii) extensive areas of consolidation with bronchogram in both lower lobes. A second echocardiogram showed no abnormal findings. On day 34, the patient remained feverish with diarrhea and abdominal pain and started with hypoxemia and vomits.
At day 35, the patient had a normal neutrophil count but remained lymphopenic. Due to worsening rash and respiratory symptoms, the child required a non-rebreathing mask and was admitted to the pediatric intensive unit (PICU). During the PICU stay, the patient did not require inotropic drugs or mechanical respiratory support. A 10-day treatment with dexamethasone 0.6 mg/kg per day was started, and convalescent plasma at a dose of 5 ml/kg was administered with good tolerance. The administration of convalescent plasma was in the context of institutional approved protocol. On day 38, the child was without fever and decreased oxygen requirements, going from PICU to an intermediate care unit. At day 53, the child was discharged with normalized laboratory markers, except for lymphopenia and high ferritin (Table 1).
SARS-CoV-2 VL monitoring was performed in nasopharyngeal swabs using an in-house quantitative RT-PCR, which was validated according to the guidelines proposed by Burd et al. (8) and Bustin et al. (9). It is important to mention that our assay included the measure of a housekeeping gene (RNase P) cycle threshold (Ct) to correct the specific-SARS-CoV-2 Ct—before its extrapolation from the standard curve—according to the number of cells in the samples and as recommended by Han et al. (10). The dynamic of SARS-CoV-2 VL was reconstructed in six samples along the 64 days of hospitalization (Figure 1). In summary, the child had a VL of 8.34 log10 copies per milliliter on the first day of symptom onset and remained above 8 log10 copies per milliliter and close to 7 log10 copies per milliliter until days 29 and 42 from admission, respectively. Then, VL decreased, reaching a value of 3.29 log10 copies per milliliter at day 49, and remained detectable but below the limit of quantification at day 64.
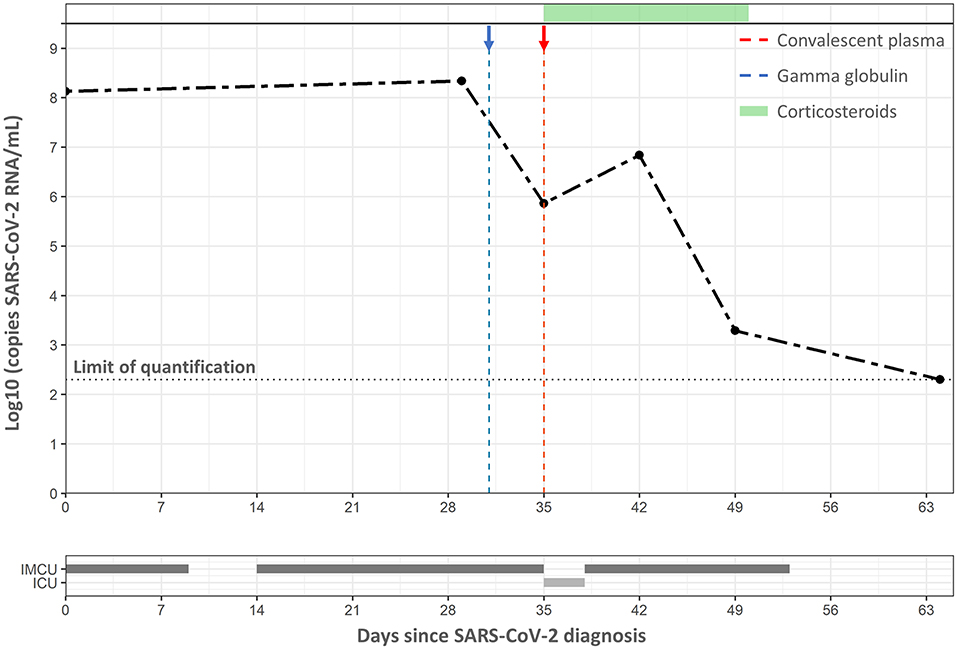
Figure 1. Dynamic of SARS-CoV-2 since admission. Dashed lines in gray, blue, and red represent the limit of quantification value, gamma globulin treatment, and convalescent plasma treatment, respectively, whereas the green bar represents the days under corticosteroids therapy. The bars below the VL curve show the period in which the child stayed in the intermediate care unit (IMCU) and intensive care unit (ICU).
During the whole hospitalization, the patient did not show signs of hemodynamic instability or shock. After 3 months from hospital discharge, the patient received unrelated hematopoietic stem cells transplantation with normal clinical and laboratory markers. At present (June 2021), 6 months after transplantation, the child was in remission of his underlying disease with good clinical evolution.
The study was approved by the Institutional Review Board, and written informed consent was obtained from the parents.
Recently, a case report showed persistent infection of SARS-CoV-2 in an immunocompromised adult with confirmed infectious virus in nasopharyngeal samples from days 75 and 143 (11). Our case adds new evidence about persistently high VL of SARS-CoV-2 in an immunocompromised child, with diagnosis of acute severe infection of SARS-CoV-2 with hyperinflammatory status mimicking MIS-C. In acute severe infection and MIS-C, common features are gastrointestinal manifestations (abdominal pain, diarrhea), cutaneous signs (rash), inflammatory markers, and lymphopenia. However, children with severe COVID-19 mimicking MIS-C present more frequently with respiratory symptoms (e.g., cough, respiratory distress) while gastrointestinal symptoms are less common. Also, comorbidities (e.g., malignancy, chronic lung diseases, neurological disorders) are frequently associated with severe forms of disease as in the case reporting here (12). On the other hand, the clinical presentation of the inflammatory status in this patient appeared at the same time that MIS-C were usually diagnosed (3rd/4th week since SARS-CoV-2 diagnosis) (5–7). The majority of MIS cases—in children and adults—were diagnosed with negative SARS-CoV-2 RT-PCR, and detectable antibodies. It is important to highlight that in our case, the specific SARS-CoV-2 antibodies were negative, but it is an immunocompromised host (13). Up to our knowledge, this is the first immunocompromised child, with persistent high VL who developed a hyperinflammatory status mimicked MIS-C. Further studies are needed to unravel the host–virus interaction that led to hyperinflammatory status in an immunocompromised host.
There are no restrictions to apply to the data generated in this article. Requests to access the datasets should be directed to YW5kcmVhbW1hbmdhbm9AZ21haWwuY29t.
The studies involving human participants were reviewed and approved by Comité Revisor y de Ética en la Investigación, Hospital de Pediatría Garrahan. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
AM, DB, and MM conceived the study. SG, MP, DB, SR, LF, AB, and RB collected and analyzed the clinical data. MM, MF, and MG developed and performed the VL of SARS-CoV-2. MM, MF, MG, DB, and AM drafted the manuscript. All authors contributed and approved the final manuscript.
This work was supported by Fondo Sectorial Argentino, Ministerio de Ciencia, Tecnología e Innovación (Argentina) (grant name: Convocatoria Ideas Proyectos IP –COVID-19; grant number: IP N° 402 and N° 0012).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank Fundación Garrahan for sponsoring the publication fees of this paper.
1. Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet. (2020) 395:1607–8. doi: 10.1016/S0140-6736(20)31094-1
2. Verdoni L, Mazza A, Gervasoni A, Martelli L, Ruggeri M, Ciuffreda M, et al. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. Lancet. (2020) 395:1771–8. doi: 10.1016/S0140-6736(20)31103-X
3. Feldstein LR, Rose EB, Horwitz SM, Collins JP, Newhams MM, Son MBF, et al. Multisystem inflammatory syndrome in U.S. children and adolescents. N Engl J Med. (2020) 383:334–46. doi: 10.1056/NEJMoa2021680
4. Webb K, Abraham DR, Faleye A, McCulloch M, Rabie H, Scott C. Multisystem inflammatory syndrome in children in South Africa. Lancet Child Adolesc Heal. (2020) 4:e38. doi: 10.1016/S2352-4642(20)30272-8
5. World Health Organization. Multisystem inflammatory syndrome in children and adolescents temporally related to COVID-19. (2020). Available online at: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (accessed January 26, 2021).
6. Centers for Disease Control and Prevention. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19). (2020). Available online at: https://emergency.cdc.gov/han/2020/han00432.asp (accessed January 26, 2021).
7. The Royal College of Paediatrics and Child Health. Guidance: paediatric multisystem inflammatory syndrome temporally associated with COVID-19. (2020). Available online at: https://www.rcpch.ac.uk/resources/paediatric-multisystem-inflammatory-syndrome-temporally-associated-covid-19-pims-guidance (accessed January 26, 2021).
8. Burd EM. Validation of laboratory-developed molecular assays for infectious diseases. Clin Microbiol Rev. (2010) 23:550–76. doi: 10.1128/CMR.00074-09
9. Bustin SA, Benes V, Garson JA, Hellemans J, Huggett J, Kubista M, et al. The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments. Clin Chem. (2009) 55:611–22. doi: 10.1373/clinchem.2008.112797
10. Han MS, Byun JH, Cho Y, Rim JH. RT-PCR for SARS-CoV-2: quantitative versus qualitative. Lancet Infect Dis. (2020) 21:165. doi: 10.1016/S1473-3099(20)30424-2
11. Choi B, Choudhary MC, Regan J, Sparks JA, Padera RF, Qiu X, et al. Persistence and evolution of SARS-CoV-2 in an immunocompromised host. N Engl J Med. (2020) 383:2291–3. doi: 10.1056/NEJMc2031364
12. Kabeerdoss J, Pilania RK, Karkhele R, Kumar TS, Danda D, Singh S. Severe COVID-19, multisystem inflammatory syndrome in children, and Kawasaki disease: immunological mechanisms, clinical manifestations and management. Rheumatol Int. (2020) 21:1–14. doi: 10.1007/s00296-020-04749-4
Keywords: SARS-CoV-2, COVID-19, viral load, immunocompromised state, hyperinflammatory status, pediatrics
Citation: Moragas M, Gomez S, Fernández MF, Golemba MD, Palladino M, Borgnia D, Ruvinsky S, Fraquelli L, Buchovsky A, Bologna R and Mangano A (2021) Case Report: Hyperinflammatory Status in an Immunocompromised Child With a Highly Sustained Viral Load of SARS-CoV-2. Front. Med. 8:675282. doi: 10.3389/fmed.2021.675282
Received: 02 March 2021; Accepted: 09 July 2021;
Published: 19 August 2021.
Edited by:
Roger Hewson, Public Health England, United KingdomReviewed by:
Audrey Ragan Odom John, Children's Hospital of Philadelphia, United StatesCopyright © 2021 Moragas, Gomez, Fernández, Golemba, Palladino, Borgnia, Ruvinsky, Fraquelli, Buchovsky, Bologna and Mangano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Mangano, YW1hbmdhbm9AZ2FycmFoYW4uZ292LmFy; YW5kcmVhbW1hbmdhbm9AZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.