 Guillermo Cuervo
Guillermo Cuervo Francesc Escrihuela-Vidal
Francesc Escrihuela-Vidal Carlota Gudiol
Carlota Gudiol Jordi Carratalà
Jordi Carratalà
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Med. , 22 February 2021
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.641243
This article is part of the Research Topic Spotlight on the Relationship between Sepsis and Infection: from Mechanisms to Therapy View all 26 articles
Infective endocarditis is a relatively rare, but deadly cause of sepsis, with an overall mortality ranging from 20 to 25% in most series. Although the classic clinical classification into syndromes of acute or subacute endocarditis have not completely lost their usefulness, current clinical forms have changed according to the profound epidemiological changes observed in developed countries. In this review, we aim to address the changing epidemiology of endocarditis, several recent advances in the understanding of the pathophysiology of endocarditis and endocarditis-triggered sepsis, new useful diagnostic tools as well as current concepts in the medical and surgical management of this disease. Given its complexity, the management of infective endocarditis requires the close collaboration of multidisciplinary endocarditis teams that must decide on the diagnostic approach; the appropriate initial treatment in the critical phase; the detection of patients needing surgery and the timing of this intervention; and finally the accurate selection of patients for out-of-hospital treatment, either at home hospitalization or with oral antibiotic treatment.
First described by the French physician Lazare Rivière more than 350 years ago, the clinicopathological manifestations of the infection of heart valves were better characterized through the enormous contributions of William Osler at the end of the 19th century (1). The infection affects the endocardial surface of the heart, most commonly the valves, but also may occur on mural endocardium, on cardiac septal defects, on arteriovenous or arterioarterial shunts and on intravascular devices. The current name of this infection, infective endocarditis, was popularized in the 1960s by Lerner and Weinstein to cover other possible, but infrequent etiologies in addition to bacterial infections (2).
Although the incidence of infective endocarditis seems to be slightly increasing (3), this disease continues to be a relatively rare, but severe cause of sepsis. Currently, up to 40–50% of affected patients require valve surgery at some point during the clinical course, with overall mortality remaining around 20–25% per year in most published series (4). Although the classic clinical syndromes of acute or subacute endocarditis are still observed to a certain degree, current clinical forms have changed. Furthermore, there have been profound epidemiological changes in high-income countries, with a clear and progressive increase in the number of cases associated with prosthetic valves and intravascular devices (3).
In this narrative review, we will address: (1) the epidemiological changes mentioned above; (2) several new advances in the understanding of the pathophysiology of infective endocarditis and in endocarditis-triggered sepsis; (3) new diagnostic tools; and finally (4) therapeutic aspects such as the relevance of early surgical treatment in selected cases, new available drugs and new useful treatment strategies.
The PubMed database was used to search medical literature published in English from 1st January 2010 to 30th October 2020, using the search terms “infective endocarditis” AND “epidemiology” OR “pathophysiology” OR “diagnosis” OR “treatment” OR “management.” We reviewed both original and review articles, excluding case reports and editorial articles. Some earlier published articles were also included due to their relevance to this review.
Infective endocarditis is considered an infrequent disease, with an annual incidence ranging from 1.5 to 15 cases per 100,000 inhabitants. It displays significant international variation (5, 6). The highest rates have been found in the United States, while the incidence is lower in Denmark. There is a significant lack of epidemiological information from Asia, Oceania and Latin America. Furthermore, the incidences can vary significantly even within the same country (7). Even though the scarcity of epidemiological data, particularly from low-income countries, a slight increase in the incidence of infective endocarditis has been noted since 2000. In this regard, controversy remains about the true impact of restricting antibiotic prophylaxis in high-risk patients, as recommended by NICE guidelines (8), with some investigations showing an increasing trend of infective endocarditis afterwards. The efficacy and impact of this strategy on antibiotic resistance are yet to be fully addressed (9).
A predisposing condition, such as rheumatic heart disease, is nowadays less commonly detected among cases of infective endocarditis, although the importance of such predisposing conditions persists in low-income countries (10). Cases associated with intravenous drug use have decreased globally, but a dramatic increase of this habit continues to affect the epidemiology of endocarditis in North America (11) and in some Eastern European countries (12). Other risk factors are being increasingly detected in high-income countries, such as degenerative valve disease, intracardiac devices (both cardiovascular implantable electronic devices as well as left ventricular assist devices), indwelling catheters and immunosuppression. This explains why the latest analyses of the demographics of endocarditis cases show a trend toward nosocomial characteristics in high-income countries: older patients, staphylococcal (both Staphylococcus aureus and coagulase-negative staphylococci) (13, 14) and enterococcal cases (15), and the involvement of prosthetic valves and cardiovascular implantable electronic devices (CIEDs) (3, 4, 11, 16, 17). By contrast, the oral streptococcal (so-called “subacute”) endocarditis classically associated with rheumatic heart disease has become less frequent (5, 18).
Other etiologies of endocarditis are infrequent: 2–5% of cases can be produced by Gram-negative bacilli (both aerobic Gram-negative bacilli or by the known HACEK group: Haemophilus spp., Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, Kingella kingae). Also uncommon are fungal endocarditis that can represent <2% of cases, mostly produced by yeasts of the Candida spp. genus or rarely by other yeasts or filamentous fungi.
Finally, a variable proportion (up to 10–20% of cases) without documented etiology are considered “culture-negative endocarditis,” mostly as a consequence of prior administration of antibiotics or caused either by fastidious slow-growing microorganisms or by truly non-cultivable intracellular bacteria (e.g., Coxiella burnetii, Chlamydophila spp, Bartonella spp, Tropheryma whippelii) (4, 19).
Transcatheter aortic valve implantation (TAVI) has led to a revolution in the management of valvular heart disease. This technique has become a suitable alternative to surgery in elderly patients with aortic valve stenosis who carry a high or moderate surgical risk (20). Therefore, the number of TAVI procedures has dramatically increased in recent years (21). The incidence of endocarditis associated with TAVI has been estimated to be 0.8–1.4% (22, 23). A meta-analysis comparing endocarditis following TAVI vs. surgical replacement found no difference in the overall incidence (24). Endocarditis after TAVI displays characteristics of healthcare-associated infections, with a high predominance of staphylococcal and enterococcal infections (23, 25, 26). In-hospital mortality of TAVI-associated endocarditis is elevated, strongly influenced by the epidemiological profile of the patients (27).
Sepsis and septic shock are severe complications that may arise from any type of infection, with poor early and late prognoses in the patients affected. A study on 894 episodes of infective endocarditis showed that 17.4% of the patients had septic shock at any time during hospitalization (28). A multivariate analysis suggested that S. aureus and signs of a persistent infection were independent predictors for the development of septic shock, alongside a previous diagnosis of diabetes mellitus and other systemic complications such as acute kidney injury and supraventricular tachycardia. Furthermore, the multivariate study indicated that the development of septic shock at any time during hospitalization was strongly associated with in-hospital mortality. Similar results were obtained in a study comparing endocarditis diagnosed “early” or “late” after the development of first symptoms. That study showed that the so-called “acute endocarditis” was more frequently presented as or complicated with septic shock (29). Sepsis and septic shock are associated with a 4-fold increase in the probability of death (28, 30).
Despite advances in diagnosis and therapeutics, infective endocarditis presents a significant morbidity burden and a remarkably high overall mortality (20–25% of cases). Endocarditis-related mortality has remained steadily high since 2000 and is strongly associated with several risk factors, such as advanced age, a high Charlson comorbidity index, non-community acquisition, prosthetic valves, staphylococcal infections, perivalvular complications, stroke, and the non-performance of surgery when indicated (3, 4, 11, 16, 31, 32). Of note, studies on psychological outcomes in survivors after an episode of endocarditis have demonstrated a reduction in quality of life and the occurrence of posttraumatic stress disorder (33).
The concurrence of several pathogenic events is required for the development of infective endocarditis, which partly explains the relatively low incidence of this disease.
From the seminal studies performed in animal models, it has been well known that inducing infective endocarditis in the absence of pre-existing endothelial damage is extremely difficult (34, 35). Important predisposing conditions are prior valvular involvement, classically rheumatic or currently due to degenerative disease (as well as the presence of prostheses or endovascular devices). These structural alterations induce turbulent blood flow that causes mechanical stress on the vascular wall, ultimately producing endothelial injury. More recently, the ability to induce experimental endocarditis in structurally healthy, but inflamed valves has been demonstrated (36). This mechanism could explain the development of endocarditis in previously normal hearts in patients with infections caused by aggressive microorganisms (e.g., S. aureus) and with endothelial inflammation caused by sepsis itself or by other agents that cause vascular damage.
After the initial endothelial damage or inflammation, the second key pathogenic event is the deposition of sterile fibrin-platelet aggregates in these injured areas. These lesions, leading to what is known as “non-bacterial thrombotic endocarditis,” have been described in up to 2.4% of the autopsies performed in patients with certain underlying diseases (37) and are the ideal niche for the subsequent anchoring of the bacteria seeded in the bloodstream. Not all bacteria from the bloodstream, however, have the same ability to colonize these lesions (38). Gram-negative bacilli, for example, are particularly susceptible to humoral innate immune responses (39). Furthermore, certain Gram-positive microorganisms, particularly some species of streptococci and S. aureus, have specific molecules on their surfaces called adhesins, such as “microbial surface components recognizing adhesive matrix molecules” (MSCRAMMs) and “secretable expanded repertoire adhesive molecules” (SERAMs). These adhesins recognize integrins, specific ligands located on the injured or inflamed endothelial surface. Since the 1980s to 1990s, a repertoire of molecules of the MSCRAMM and SERAM type have been described in detail for streptococci and S. aureus (40–44), which interact not only with the endothelium, but also with platelets and key proteins of the clotting cascade (45–47).
The last important pathogenic event is the maturation and growth of the fibrin-platelet aggregates, which clump together with bacteria at a high inoculum (more than 109 colony-forming units per gram of vegetation) in what is known as “vegetation.” Within this vegetation, bacterial communities are partly organized into complex biofilms, embedded in the fibrin-platelet aggregate and in a matrix of macromolecules produced by them. The arrival of phagocytes and antibiotics can be compromised in these structures, inside which bacteria can also modify their metabolism toward persistent phenotypes, with greater tolerance to antibiotics (48–50). The vegetation represents the pathological hallmark of infective endocarditis and determines its main clinical manifestations, namely: (1) the growth of this “full bacterial lesion” causes continuous bacteremia at a high inoculum that can seed distant septic metastases, (2) the invasion of the structures to which this vegetation is anchored can cause valvular destruction, negatively affecting the patient's hemodynamics, and finally (3) this friable mass can detach pieces that cause distant embolisms, which can significantly affect the function and prognosis of the affected patients. In recent years, intensive studies have been carried out in this field. Through pharmacological manipulation, successful attempts have been made to hinder the interactions between bacteria and the endothelium, effectively preventing the development or modulating the severity of infective endocarditis in animal models treated with antiplatelet and anticoagulant drugs (51, 52). Although the possible prophylactic role of some antiplatelet or anticoagulant drugs has been reinforced by observational clinical studies (53–55), the prophylactic use of these drugs has not been effectively transferred to clinical practice yet (56).
As described previously, a non-negligible proportion of patients with endocarditis may present with severe sepsis or septic shock (28), which can eventually lead to multi-organ failure. This complication appears to be associated with some characteristics of the patients (57) as well as with particularly virulent microorganisms such as S. aureus and beta-hemolytic streptococci (58). In addition to their invasive and destructive effects on the affected anatomical structures, these bacteria can seed distant septic metastases. Moreover, they display a repertoire of other virulence mechanisms, including the excretion of exotoxins that can act as superantigens, which overactivate the immune system (59–61). The systemic inflammation that is consequently triggered has an important hemodynamic impact, with generalized endothelial dysfunction and a drop in vascular resistance. Any increases in the compensatory cardiac output may be hampered by sepsis itself, a phenomenon known as “septic cardiomyopathy” (62), or by the destruction of the valve as a result of the infection. This extremely serious situation explains why the presence of septic shock is associated with a significant increase in the risk of mortality.
The diagnosis of infective endocarditis relies on a combination of clinical, microbiological and imaging information, as specified by the modified Duke criteria (63, 64). The classic combination of clinical features of infective endocarditis remains a critical feature in diagnosis, particularly for subacute or chronic endocarditis. The mainstay of diagnosis involves the information provided by blood cultures and different imaging techniques that can detect anatomical changes such as valve vegetations or associated complications. However, a shift toward more acute infections and the involvement of prosthetic materials have decreased, to some extent, the usefulness of applying these classic clinical features in diagnosis. The performance of the modified Duke criteria has been thus compromised in the era of non-community acquired infective endocarditis. Therefore, modifications have been proposed to improve their sensitivity (65, 66). Nowadays, the diagnostic accuracy of these criteria seems to largely rely on the development of new and more sensitive non-invasive imaging techniques (Table 1).
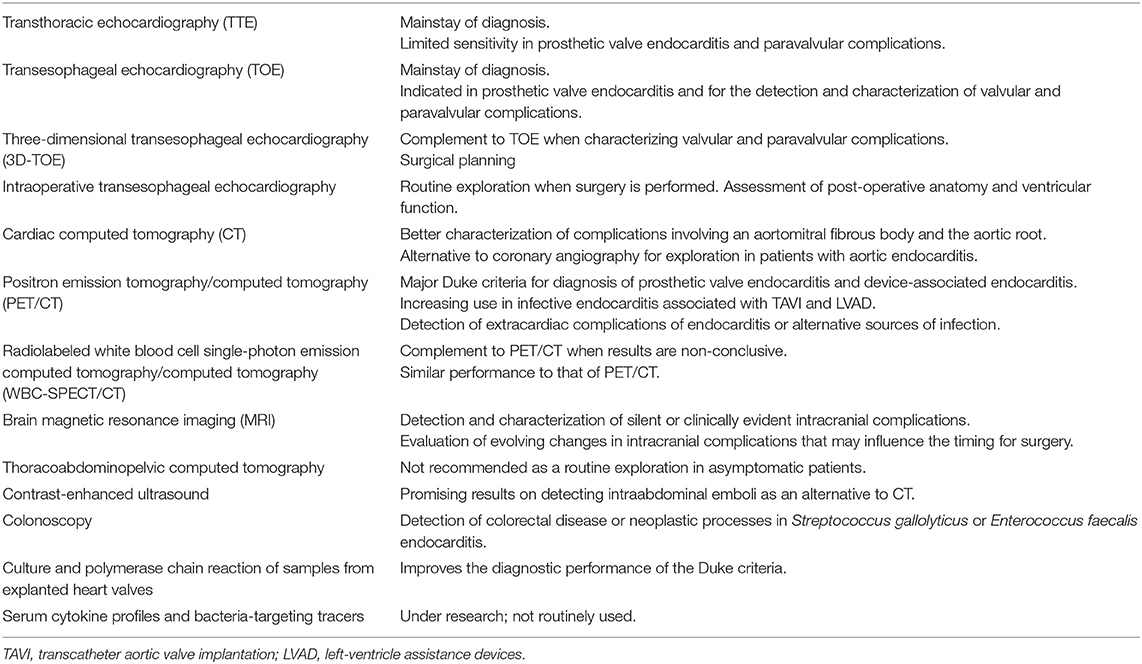
Table 1. Imaging and laboratory techniques used in the diagnosis of infective endocarditis.
Transthoracic echocardiography (TTE) is the main imaging method in the diagnosis of endocarditis, with varying sensitivity rates for valvular and paravalvular abnormalities such as vegetations (sensitivity around 65%), a new regurgitation or dehiscence of a prosthetic valve, perforations, abscesses and fistulae (64). Transesophageal echocardiography (TOE) provides a better detection and characterization of local abnormalities (sensitivity for intracardiac vegetations of ~95%), particularly when TTE is negative, in the case of valvular or paravalvular complications as well as in prosthetic valve endocarditis (PVE) and endocarditis associated with CIEDs (67).
Three-dimensional TOE (3D-TOE) may complement conventional TOE. Although its contribution to the diagnosis of endocarditis is not clearly established (68, 69), its main value is in providing a detailed description of vegetations, regurgitations and abscesses in both native (70) and prosthetic valve endocarditis (71). This technique can also differentiate vegetations from thrombi (72) and can be used in surgical planning. Intraoperative TOE has been demonstrated to be useful in the surgeries for endocarditis and has been proposed for use in routine exploration (73, 74).
Although TOE remains the mainstay in the diagnosis of infective endocarditis, there is growing interest in the application of cardiac computed tomography (CT). This tool shows good anatomical correlation, especially when diagnosing a perivalvular abscess of the aortomitral intervalvular fibrous body and other structures surrounding the aortic root, thus overcoming the limitations of TOE (75–77). Recent data support cardiac CT as an adjuvant exploration technique when a better depiction of valvular complications is needed or when echocardiography proves to be insufficient in both native (77) and prosthetic valve endocarditis (78–80). Furthermore, cardiac CT is frequently used to preoperatively assess the presence of coronary artery disease in aortic endocarditis where performing a coronary angiography carries a prohibitive high risk of the dislodgment of vegetations (74). A recent study from Wang and colleagues added a prognostic value to cardiac CT, suggesting a synergistic role with TOE in surgery planning and in predicting early and late mortality (81).
To complement the detection of anatomic abnormalities, progress has been made in measuring biological activity through 18F-fluorodeoxyglucose positron emission/computed tomography (FDG-PET/CT) and radiolabeled white blood cell single-photon emission CT/CT (WBC-SPECT/CT). Their use has been recommended by the European Society of Cardiology in patients with suspected PVE for valves implanted for more than 3 months (74), with a positive result included as a major criterion for the diagnosis of prosthetic valve and device-related endocarditis. Prospective studies of patients with suspected PVE have revealed a remarkable performance of FDG-PET/CT and WBC-SPECT/CT in the diagnosis of PVE (82, 83). They suggest that these two imaging techniques can be used in a stepwise fashion when evaluating the presence of endocarditis. FDG-PET/CT should be used first, since it has higher sensitivity, and when the results are not conclusive, WBC-SPECT/CT may be performed. Similar results have been obtained with both FDG-PET/CT (84, 85) and WBC-SPECT/CT (86–89) for suspected CIEDs endocarditis. Controversy remains on the use of FDG-PET/CT in patients with aortic root grafts with a prosthetic valve, since a high rate of false positives has been observed in relation to surgical adhesives (82, 90). FDG-PET/CT performs very well in the diagnosis of PVE when adjusting for confounders such as the low inflammatory activity caused by the initiation of antibiotic treatment (82, 90, 91), suggesting that FDG-PET/CT should be performed as soon as possible when infective endocarditis is suspected. Furthermore, FDG-PET/CT has proven prognostic value in PVE by correlating with major cardiac events (92).
The role of FDG-PET/CT in the diagnosis of native valve endocarditis has not been fully established and may be limited to cases where endocarditis is strongly suspected but the Duke criteria are not totally met. Studies on the use of FDG-PET/CT in native valve endocarditis are mostly retrospective and might overestimate the sensitivity of this technique (93, 94). In such cases, FDG-PET/CT may have an impact on diagnosis by detecting extracardiac complications of endocarditis (95).
The increasing use of TAVI and left ventricular assist devices (LVAD) have led to challenges in diagnosing the infective complications associated with their use. A recent study in patients with suspected TAVI-related endocarditis showed that the inclusion of FDG-PET/CT led to the reclassification of 36% of the patients diagnosed with “possible endocarditis” by the modified Duke criteria (96). Moreover, FGD-PET/CT and WBC-SPECT/CT have been used in cases of endocarditis associated with LVADs, showing variable rates of sensitivity and specificity (97–100). WBC-SPECT/CT and FDG-PET/CT show similar sensitivity and specificity, but the former may be more challenging to perform since it uses a more difficult protocol and requires the manipulation of blood specimens.
FDG-PET/CT is also useful in revealing unexpected sources of primary infections and detecting extracardiac complications of endocarditis. Thus, its use can lead to changes in treatment plans (101). However, no recommendations have been made in international guidelines regarding the detection of extracardiac complications.
Recommendations for neuroimaging in infective endocarditis remain unclear. Brain CT is often used when neurological symptoms are present, although brain magnetic resonance imaging (MRI) has better sensitivity in defining lesions. Clinically silent complications of the central nervous system, such as embolisms, may occur in up to 60% of patients (102). Some centers routinely perform brain MRI when infective endocarditis is diagnosed since it may provide additional diagnostic findings for fulfilling the modified Duke criteria and may change therapeutic plans (103) or the timing for surgery (104). However, while major intracranial hemorrhages and extensive ischemic stroke worsen prognosis after valve surgery, brain MRI findings of clinically silent complications do not affect postoperative mortality (105). In this sense, the clinical significance of cerebral microbleeds, one of the most frequently encountered silent lesions, remains to be elucidated (106, 107).
Systematic thoracoabdominopelvic CT has not demonstrated a clear utility in the diagnosis of left-sided endocarditis in asymptomatic patients. Furthermore, it increases the risk of kidney toxicity (108). Nevertheless, the finding of pulmonary embolisms in chest CT may be useful in the diagnostic workup of right-sided endocarditis either on the tricuspid native valve in intravenous drug addicts or associated with pacemakers (109). Contrast-enhanced ultrasound may be useful as an alternative for the detection of abdominal complications, mostly spleen infarctions (110).
Regarding the detection of the portals of bacterial entry, colonoscopy has proved to be very useful. The relationship between Streptococcus gallolyticus and colon cancer has been well known since the 1950s (111). Two observational studies on infective endocarditis caused by Enterococcus faecalis found a high rate of colorectal disease when a colonoscopy was performed, with a high incidence of neoplastic disease particularly in those with an unknown source of bacteremia (112, 113). A systematic and multidisciplinary search for portals of bacterial entry has been proposed, suggesting that a meticulous physical examination should be performed when evaluating patients with infective endocarditis (114).
Procedures involving polymerase chain reaction (PCR) using samples from explanted heart valves could improve diagnostic performance (115) in comparison with conventional cultures. Although interesting from a theoretical point of view, those molecular techniques applied to the detection of genetic material in blood samples for cases of culture-negative endocarditis have shown low sensitivity so far (116). Finally, there is an increasing interest in finding new predictors of mortality in patients with endocarditis through the use of serum cytokine profiles (117) or bacteria-targeting tracers alongside diverse nuclear imaging techniques (118). Regarding acute-phase reactants and biomarkers of severe infection, procalcitonin levels are significantly increased in the cases of endocarditis complicated with sepsis or septic shock when compared to cases without these complications (119). No other biomarker has demonstrated a good predictive value in this setting. Current research of biomarkers in endocarditis is focused on proteomic analysis of some molecules that are not yet in routine clinical use (120).
To conclude, progress has been made through the development of new diagnostic techniques and improvements in known ones. However, for a complex and systemic disease such as infective endocarditis, it seems that diagnosis will be further improved by using a refined combination of clinical, microbiological and multimodal imaging information.
The available evidence to guide antibiotic treatment of infective endocarditis is composed mostly of data from observational studies and some from experimental animal models. A recent Cochrane review analyzed the evidence from six small clinical trials evaluating various antibiotic regimens for endocarditis with a range of etiologies. After an in-depth analysis, the authors of the review concluded that given the high risk of bias, insufficient data, or underpowered designs, the evidence offered by these trials did not support or reject any of the regimens evaluated (121). This poor evidence may partly explain the significant heterogeneity in the management of this disease observed in some surveys (122) and the lack of adherence to some recommendations of the European guidelines even among those who developed them (123).
With these caveats in mind, when treating this infection, the pathophysiological peculiarities of infective endocarditis must be taken into account, such as the presence of very high concentrations of bacteria protected from immune responses within vegetations and the potential existence of bacteria with reduced metabolism embedded in biofilms. For these reasons, it has been postulated that to achieve microbiological eradication, the treatment of infective endocarditis must involve bactericidal antibiotics administered parenterally in high doses and for prolonged periods (124).
The selection of the antibiotic regimen for a particular case of endocarditis is often complex and beyond the scope of this review. All the details on this are available in the published guidelines (74, 125). However, in the next few paragraphs, we will offer a brief overview of the common regimens that are used against the most frequent microorganisms that cause infective endocarditis.
The cornerstone of the antibiotic treatment of endocarditis is the use of beta-lactams in high doses: penicillin or ceftriaxone for the viridans group streptococci, ampicillin for E. faecalis, and antistaphylococcal penicillins or first-generation cephalosporins for methicillin-sensitive S. aureus or coagulase-negative staphylococci. In allergic patients or in those with infections caused by strains resistant to beta-lactams, the alternative is usually another cell wall-active agent, such as vancomycin for the viridans group streptococci and E. faecalis or vancomycin or daptomycin for staphylococci. Due to the limited amount of evidence, treatment regimens for endocarditis caused by coagulase-negative staphylococci are usually extrapolated from those recommended for treating endocarditis caused by S. aureus (126).
The synergistic combination of aminoglycosides and beta-lactams demonstrates rapid bactericidal action, allowing treatment to be shortened to 2 weeks for native valve endocarditis caused by susceptible viridans group streptococci (127). This antibiotic combination is also recommended for treating infections caused by the viridans group streptococci that are partially or fully resistant to penicillin, although this recommendation is based on less robust evidence (128, 129).
The combination of ampicillin and aminoglycosides is essential for at least the first 2 weeks of treatment (130) to reduce the risk of relapse in endocarditis caused by E. faecalis, given the relative tolerance of these bacteria to beta-lactams (which is also observed in other species such as Granulicatella adiacens and Abiotrophia defectiva). When this combination cannot be used due to high-level aminoglycoside resistance or an unacceptable risk of toxicity, combination with ceftriaxone (so-called “double beta-lactam”) is recommended, which achieves bactericidal action presumably through the complementary saturation of penicillin-binding proteins (PBPs) (131, 132).
In endocarditis caused by S. aureus, the combination of beta-lactams and aminoglycosides is currently not recommended for native valve infections due to the increased risk of renal toxicity without any relevant clinical benefit (133, 134). It is only recommended for PVE according to experimental data, although some retrospective series question its usefulness even in that scenario (135).
The use of rifampicin in a combination treatment for native valve endocarditis caused by S. aureus is discouraged (136), but could be useful in PVE, given its potent activity in infections involving biofilms. Guidelines recommend this regimen for PVE, but only after clearing blood cultures to avoid the emergence of resistant mutants during treatment (136). In any case, this drug may not be essential after valve replacement surgery in patients operated during the active phase of treatment (137).
There is enormous interest in the potential utility of the combination of beta-lactams with daptomycin or fosfomycin in endocarditis caused by methicillin-susceptible S. aureus. Experimental evidence shows that combinations of both drugs with cloxacillin produce greater sterilization of vegetations on the left-sided valves in animal models (138). However, this potential beneficial effect of the combination with daptomycin was not observed in a retrospective study conducted in our center (139) or in a recent clinical trial of bacteremia caused by susceptible S. aureus (140), although it is worth mentioning that there was an underrepresentation of infective endocarditis as a cause of bacteremia in both studies (9 and 10% of patients, respectively). The combination of cloxacillin with fosfomycin in bacteremia and endocarditis caused by susceptible S. aureus is an attractive alternative. In an ongoing multicenter clinical trial (SAFO trial) we are testing this combination for bacteremia caused by methicillin-susceptible S. aureus (141).
In the case of endocarditis caused by methicillin-resistant S. aureus (MRSA), combination therapy is likely to be more effective given the relatively poor results of both vancomycin and daptomycin monotherapy. The possible synergistic effect of vancomycin and beta-lactams in MRSA bacteremia suggested by in vitro studies, retrospective studies (142, 143) and a pilot clinical trial (144) could not be confirmed in the international multi-center CAMERA 2 clinical trial. This trial had to be prematurely discontinued due to greater renal toxicity in the combination arm, which was associated with a shorter duration of bacteremia, but no differences in mortality between the groups (145).
The combination of daptomycin and fosfomycin has produced promising results in animal models of MRSA endocarditis (146). This combination has also shown good microbiological results and clinical benefits in patients aged under 70 years in our recent clinical trial of MRSA bacteremia (BACSARM trial) (147), which again had a poor representation of endocarditis cases (diagnosed in 12% of the cases).
Finally, combinations of daptomycin and beta-lactams without and with intrinsic anti-MRSA activity for the treatment of MRSA bacteremia have been shown to be effective in a retrospective study (148) and in a pilot clinical trial (149), respectively, although with little specific information for endocarditis cases.
Even in infections caused by susceptible microorganisms, the risk of microbiological relapse is plausible in endocarditis. For this reason, long treatments are typically recommended, generally 4 weeks for native valve endocarditis and 6 weeks for PVE. Exceptions to this general rule are the abbreviated 2-week treatments that have proved to be effective for right-sided endocarditis (150) and the combination treatment of beta-lactams and aminoglycosides for native valve endocarditis caused by penicillin-susceptible viridans group streptococci (127). Furthermore, there are clinical trials currently underway that aim to demonstrate the efficacy of shorter-than-standard therapeutic regimens (151).
In native valve endocarditis caused by E. faecalis, 4-week aminoglycoside treatment courses are recommended for cases with a clinical evolution shorter than 3 months (152). In cases with a longer symptomatic duration and in those using the double beta-lactam combination, a 6-week treatment course is recommended (153).
The decision of the total duration of antibiotic therapy in patients undergoing surgery during the active phase of treatment is affected by the result of the valve culture (154). According to the findings of a retrospective study, an antibiotic treatment duration of 2 weeks after surgery may be sufficient for valve culture-negative streptococcal endocarditis (155). Management guidelines recommend completing the pre-stipulated duration of the antibiotic treatment course when the valve culture is negative and, conversely, restarting a complete cycle if the valve is not sterile at the time of surgery.
Infective endocarditis requires long and expensive hospitalizations for its management given the need to administer parenteral antibiotics for several weeks. Outpatient parenteral antibiotic treatment (OPAT) has been shown to be efficient and cost-effective in the management of endocarditis. A series of specific criteria must be met by the patients for them to be considered safe candidates for OPAT (156). Generally, this option is considered suitable for patients who have overcome the critical phase of the disease (first 2 weeks), provided that they remain stable. Recent studies have demonstrated the safety of this strategy, even expanding the restrictive criteria proposed in the guidelines (157).
In recent years, new antibiotics targeting Gram-positive microorganisms (and, therefore, potentially useful for treating endocarditis) have been incorporated. The fifth-generation cephalosporins ceftaroline and ceftobiprole represent the first beta-lactams with intrinsic anti-MRSA activity. Although infective endocarditis is not among the approved indications based on pivotal clinical trials, there are case series that have reported that its off-label use is an effective salvage treatment in patients with endocarditis (158, 159). Ceftaroline and, in particular, ceftobiprole also have anti-enterococcal activity (160), which makes them attractive as candidates for combination treatments with ampicillin or daptomycin in managing enterococcal infective endocarditis (161).
Another interesting new molecule is the lipoglycopeptide dalbavancin, a bactericidal drug with a chemical structure and antibacterial spectrum similar to those of teicoplanin, but with a very long half-life that allows its administration every week or every 2 weeks. Dalbavancin is a potentially useful option for OPAT in selected patients. In vitro studies have demonstrated its potent activity against endocarditis-producing strains (162). Furthermore, recently published series of cases indicate that it shows efficacy as a continuation drug in endocarditis cases of diverse etiology (163, 164).
The effectiveness of oral treatment for endocarditis has been demonstrated for cases involving right-sided valves (165), as stated in the management guidelines. For left-sided endocarditis, retrospective studies (166), a small clinical trial of endocarditis caused by the viridans group streptococci (167) and a recent randomized clinical trial (168) of endocarditis with diverse etiologies (streptococci, enterococci, and staphylococci) have demonstrated that partial oral regimens are effective in treating selected patients who have overcome the critical phase.
In that recent randomized clinical trial, the POET trial, 1,954 patients were evaluated, of whom 400 were finally selected. After a minimum of 10 days of intravenous antibiotic therapy, the patients were randomized to continue intravenous therapy or to complete treatment with a combination of oral drugs. The clinical endpoint was a composite of all-cause mortality, unplanned cardiac surgery, embolic events, and relapse of bacteremia with the primary pathogen from the time of randomization until 6 months after the completion of antibiotic treatment. This endpoint was found to be similar between the groups. Due to the diverse etiologies included in the trial and the various combinations of oral antibiotics administered, the results of the POET trial cannot be used to make specific therapeutic recommendations. However, this trial has raised the possibility of including oral sequential treatment as a suitable option for treatment completion in selected patients.
Antifungal treatment for Candida spp. endocarditis is usually based on the use of drugs with fungicidal activity, either based on regimens with liposomal amphotericin B (or other lipid formulations) with or without flucytosine or on regimens based on echinocandins in high doses. Although the evidence is scarce, based mostly on retrospective experiences and expert consensus, the use of combined treatments and long-term azole suppressive treatments is frequent. A high number of cases will require surgical intervention as part of the management (169). On the other hand, in the rare cases of endocarditis due to Aspergillus species (often responsible for culture-negative endocarditis), the most commonly used antifungal is voriconazole and the surgery requirements is also high (74, 125).
The appropriate selection of an empirical antibiotic treatment for patients with culture-negative endocarditis is a difficult task and so expert consultation is recommended. The decision is often conditioned by the clinical presentation of the disease, the presence or absence of prosthetic material and other epidemiological data such as other comorbidities, dental hygiene, alcoholism, contact with animals, etc. Thus, for patients with native valves and subacute presentation, empirical treatment should cover viridans group streptococci, enterococci and HACEK (e.g., ampicillin plus either gentamicin or ceftriaxone) whereas in cases with acute clinical presentation and/or presence of prosthetic valves it seems reasonable to cover Staphylococcus aureus, coagulase-negative staphylococci, β-hemolytic streptococci and aerobic gram-negative bacilli (e.g., cloxacillin plus ceftriaxone plus either vancomycin or daptomycin) (170, 171) The details on directed treatment options for specific pathogens are available in the published guidelines (74, 125).
More than 50% of patients with endocarditis will need valve surgery. Among these, a significant proportion will require it during the active phase (that is, during the initial hospitalization and before the end of antibiotic treatment), which is known as early valve surgery (EVS). Although both the American and European guidelines have the same indications for EVS (Table 2) (74, 125), the latter guideline goes further in terms of recommending the timing of surgery. It suggests emergent surgery (within the first 24–48 h) in the case of refractory heart failure secondary to valve regurgitation, and an urgent surgery (during the first week) in almost all other clinical settings.
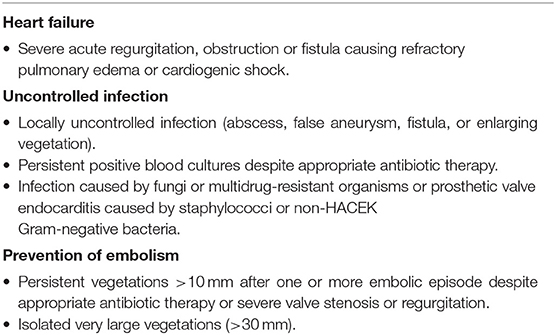
Table 2. Indications for surgery in left-sided valve endocarditis (74).
This contentious issue of the timing of surgery in the guidelines is partly due to the limited and conflicting evidence published to date that is difficult to interpret. There is only one randomized clinical trial that has demonstrated a clinical benefit in terms of a reduction in embolic events for “very” EVS in young patients (median age of 48 years) with native mitral valve endocarditis and mostly caused by streptococcal bacteria (172). It is unclear to what extent this evidence can be extrapolated to older patients and to endocarditis with other etiologies.
Most of the available evidence consists of findings from retrospective studies that require laborious statistical adjustments in order to mitigate indication and survival biases and draw valid conclusions. According to these studies, the benefit of EVS can only be demonstrated for native valve endocarditis with surgical requirement (173). The benefit is less evident in the case of PVE (only demonstrated in patients who are more likely to require surgery) (174) and could be present in some carefully selected patients with PVE caused by S. aureus (175).
It seems reasonable to conclude that the decision to proceed with an emergency or urgent valve surgery during the active phase of endocarditis cannot be recommended systematically or routinely. Instead, this decision should be based on an individualized assessment (176).
The management of septic shock in patients with endocarditis does not seem to differ from that recommended for sepsis from other sources (59). In addition to volume expansion, vasoactive drugs in some cases and the early initiation of appropriate bactericidal antibiotic treatment, there is still no clinical evidence about the possible effectiveness of additional immunomodulatory treatments in cases of endocarditis and suspected toxic shock (61). It seems appropriate to point out that early valve surgery may be necessary in some cases as a source control measure (30), such as in cases with uncontrolled infection despite correct antibiotic treatment.
It is evident that the management of infective endocarditis requires the close collaboration of a multidisciplinary team that includes experts in critical care for patients with severe sepsis or septic shock. The training of endocarditis teams is recommended by the guidelines, while some studies have demonstrated the beneficial impact of their performance on patient outcomes (177, 178).
It seems reasonable to conclude that patients with endocarditis should be evaluated preferentially by these multidisciplinary teams in the critical phase of the disease, at which time the most appropriate initial intravenous antibiotic therapy should be chosen. New therapeutics and possible new synergistic combinations of antibiotics are of very high interest. After a thorough clinical and anatomical cardiac evaluation, patients eligible for surgical treatment should be selected and the timing of the intervention decided. It is possible that in coming years, an increasing proportion of appropriately selected patients will be able to continue their antibiotic treatment in home hospitalization regimens with OPAT, using long half-life parenteral antibiotics or combinations of oral antibiotics (Figure 1).
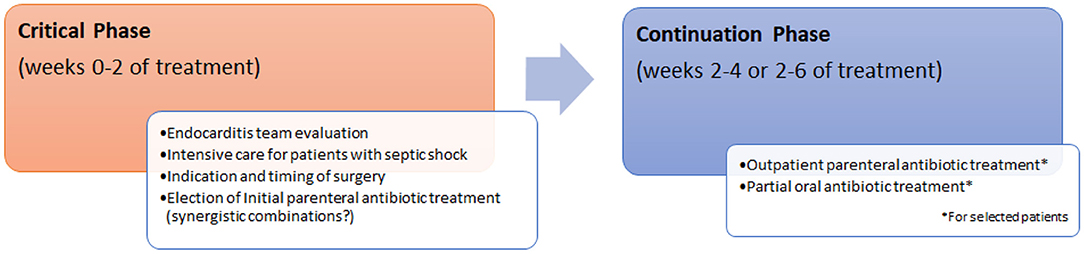
Figure 1. Management of infective endocarditis.
There is a need for international and multi-center working groups to establish a common work agenda in order to scientifically address all the unresolved diagnostic and therapeutic aspects of infective endocarditis.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Our group was supported by Plan Nacional de I+D+i 2013-2016 and the Instituto de Salud Carlos III, the Subdirección General de Redes y Centros de Investigación Cooperativa, the Ministerio de Ciencia, Innovación y Universidades, the Spanish Network for Research in Infectious Diseases (REIPI RD16/0016/0005) co-financed by the European Regional Development Fund A Way to Achieve Europe, and the Operative program Intelligent Growth 2014-2020.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank the CERCA Programme/Generalitat de Catalunya for institutional support. Members of Bellvitge University Hospital Endocarditis Team: GC, FE-V, JC, Inmaculada Grau, Sara Grillo, Carmen Ardanuy, Dámaris Berbel, Miriam Torecillas-Muelas, Jose Carlos Sánchez-Salado, Oriol Alegre, Alejandro Ruiz-Majoral, Fabrizio Sbraga, Arnau Blasco, Laura Gracia-Sánchez, Iván Sánchez-Rodríguez, Ariadna Padullés, Paola Sastre, Pere Cardona, Ignasi Anguera, Joan Peris, Joan Guillamont.
1. Geller SA. Infective endocarditis : a history of the development of its understanding. Autops Case Rep. (2013) 3:5–12. doi: 10.4322/acr.2013.033
2. Lerner PI, Weinstein L. Infective endocarditis in the antibiotic era. N Engl J Med. (1966) 274:199–206. doi: 10.1056/NEJM196601272740407
3. Tleyjeh IM, Steckelberg JM, Murad HS, Anavekar NS, Ghomrawi HMK, Mirzoyev Z, et al. Temporal trends in infective endocarditis: a population-based study in Olmsted County, Minnesota. J Am Med Assoc. (2005) 293:3022–8. doi: 10.1001/jama.293.24.3022
4. Habib G, Erba PA, Iung B, Donal E, Cosyns B, Laroche C, et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: a prospective cohort study. Eur Heart J. (2019) 40:3222–32B. doi: 10.1093/eurheartj/ehz620
5. Pant S, Patel NJ, Deshmukh A, Golwala H, Patel N, Badheka A, et al. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J Am Coll Cardiol. (2015) 65:2070–6. doi: 10.1016/j.jacc.2015.03.518
6. Muñoz P, Kestler M, De Alarcón A, Miro JM, Bermejo J, Rodríguez-Abella H, et al. Current epidemiology and outcome of infective endocarditis: a multicenter, prospective, cohort study. Medicine. (2015) 94:e1816. doi: 10.1097/MD.0000000000001816
7. Bin Abdulhak AA, Baddour LM, Erwin PJ, Hoen B, Chu VH, Mensah GA, et al. Global and regional burden of infective endocarditis, 1990–2010. Glob Heart. (2014) 9:131–43. doi: 10.1016/j.gheart.2014.01.002
8. Prophylaxis Against Infective Endocarditis: Antimicrobial Prophylaxis Against Infective Endocarditis in Adults and Children Undergoing Interventional Procedures (CG64). (2015). Available online at: https://www.nice.org.uk/guidance/cg64/resources/prophylaxis-against-infective-endocarditis-antimicrobial-prophylaxis-against-infective-endocarditis-in-adults-and-children-undergoing-interventional-procedures-pdf-975567956677 (accessed December 12, 2020).
9. Cahill TJ, Harrison JL, Jewell P, Onakpoya I, Chambers JB, Dayer M, et al. Antibiotic prophylaxis for infective endocarditis: a systematic review and meta-analysis. Heart. (2017) 103:937–44. doi: 10.1136/heartjnl-2015-309102
10. Yew H Sen, Murdoch DR. Global trends in infective endocarditis epidemiology. Curr Infect Dis Rep. (2012) 14:367–72. doi: 10.1007/s11908-012-0265-5
11. Slipczuk L, Codolosa JN, Davila CD, Romero-Corral A, Yun J, Pressman GS, et al. Infective endocarditis epidemiology over five decades: a systematic review. PLoS ONE. (2013) 8:e82665. doi: 10.1371/journal.pone.0082665
12. European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Trends in Injecting Drug Use in Europe. Luxembourg: Publications Office of the European Union. (2010).
13. Fowler VG, Miro JM, Hoen B, Cabell CH, Abrutyn E, Rubinstein E, et al. Staphylococcus aureus endocarditis: a consequence of medical progress. J Am Med Assoc. (2005) 293:3012–21. doi: 10.1001/jama.293.24.3012
14. Benito N, Miro JM, De Lazzari E, Cabell CH, Del Rio A, Altclas J, et al. Health care-associated native valve endocarditis: importance of non-nosocomial acquisition. Ann Intern Med. (2009) 150:586–94. doi: 10.7326/0003-4819-150-9-200905050-00004
15. Escolà-Vergé L, Fernández-Hidalgo N, Larrosa MN, Fernandez-Galera R, Almirante B. Secular trends in the epidemiology and clinical characteristics of Enterococcus faecalis infective endocarditis at a referral center (2007–2018). Eur J Clin Microbiol Infect Dis. (2021). doi: 10.1007/s10096-020-04117-x. [Epub ahead of print].
16. Cuervo G, Rombauts A, Caballero Q, Grau I, Pujol M, Ardanuy C, et al. Twenty-year secular trends in infective endocarditis in a teaching hospital. Open Forum Infect Dis. (2018) 5:1–7. doi: 10.1093/ofid/ofy183
17. Olmos C, Vilacosta I, Fernández-Pérez C, Bernal JL, Ferrera C, García-Arribas D, et al. The evolving nature of infective endocarditis in Spain: a population-based study (2003 to 2014). J Am Coll Cardiol. (2017) 70:2795–804. doi: 10.1016/j.jacc.2017.10.005
18. Ambrosioni J, Hernandez-Meneses M, Téllez A, Pericàs J, Falces C, Tolosana J, et al. The changing epidemiology of infective endocarditis in the twenty-first Century. Curr Infect Dis Rep. (2017) 19:21. doi: 10.1007/s11908-017-0574-9
19. Murdoch DR, Corey RG, Hoen B, Miró M, Fowler VG, Bayer AS, et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century the international collaboration on endocarditis-prospective cohort study. Arch Intern Med. (2009) 169:463–73. doi: 10.1001/archinternmed.2008.603
20. Siontis GCM, Overtchouk P, Cahill TJ, Modine T, Prendergast B, Praz F, et al. Transcatheter aortic valve implantation vs. surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: an updated meta-analysis. Eur Heart J. (2019) 40:3143–53. doi: 10.1093/eurheartj/ehz275
21. Fernández D, Cevallos J, Brugaletta S, Martín-Yuste V, Freixa X, Andrea R, et al. Percutaneous transcatheter aortic valve implantation: present and future perspective. Expert Rev Med Devices. (2013) 10:185–99. doi: 10.1586/erd.12.78
22. Regueiro A, Linke A, Latib A, Ihlemann N, Urena M, Walther T, et al. Association between transcatheter aortic valve replacement and subsequent infective endocarditis and in-hospital death. J Am Med Assoc. (2016) 316:1083–92. doi: 10.1001/jama.2016.12347
23. Latib A, Naim C, De Bonis M, Sinning JM, Maisano F, Barbanti M, et al. TAVR-associated prosthetic valve infective endocarditis: results of a large, multicenter registry. J Am Coll Cardiol. (2014) 64:2176–8. doi: 10.1016/j.jacc.2014.09.021
24. Ando T, Ashraf S, Villablanca PA, Telila TA, Takagi H, Grines CL, et al. Meta-Analysis comparing the incidence of infective endocarditis following transcatheter aortic valve implantation vs. surgical aortic valve replacement. Am J Cardiol. (2019) 123:827–32. doi: 10.1016/j.amjcard.2018.11.031
25. Pericas JM, Llopis J, Cervera C, Sacanella E, Falces C, Andrea R, et al. Infective endocarditis in patients with an implanted transcatheter aortic valve: clinical characteristics and outcome of a new entity. J Infect. (2015) 70:565–76. doi: 10.1016/j.jinf.2014.12.013
26. Amat-Santos IJ, Messika-Zeitoun D, Eltchaninoff H, Kapadia S, Lerakis S, Cheema AN, et al. Infective endocarditis after transcatheter aortic valve implantation results from a large multicenter registry. Circulation. (2015) 131:1566–74. doi: 10.1161/CIRCULATIONAHA.114.014089
27. Bjursten H, Rasmussen M, Nozohoor S, Götberg M, Olaison L, Rück A, et al. Infective endocarditis after transcatheter aortic valve implantation: a Nationwide study. Eur Heart J. (2019) 40:3263–9. doi: 10.1093/eurheartj/ehz588
28. Olmos C, Vilacosta I, Fernández C, López J, Sarriá C, Ferrera C, et al. Contemporary epidemiology and prognosis of septic shock in infective endocarditis. Eur Heart J. (2012) 34:1999–2006. doi: 10.1093/eurheartj/ehs336
29. N'Guyen Y, Duval X, Revest M, Saada M, Erpelding ML, Selton-Suty C, et al. Time interval between infective endocarditis first symptoms and diagnosis: relationship to infective endocarditis characteristics, microorganisms and prognosis. Ann Med. (2017) 49:117–25. doi: 10.1080/07853890.2016.1235282
30. Krajinovic V, Ivancic S, Gezman P, Barsic B. Association between cardiac surgery and mortality among patients with infective endocarditis complicated by sepsis and septic shock. Shock. (2018) 49:536–42. doi: 10.1097/SHK.0000000000001013
31. Armiñanzas C, Fariñas-Alvarez C, Zarauza J, Muñoz P, González Ramallo V, Martínez Sellés M, et al. Role of age and comorbidities in mortality of patients with infective endocarditis. Eur J Intern Med. (2019) 64:63–71. doi: 10.1016/j.ejim.2019.03.006
32. Bikdeli B, Wang Y, Kim N, Desai MM, Quagliarello V, Krumholz HM. Trends in hospitalization rates and outcomes of endocarditis among medicare beneficiaries. J Am Coll Cardiol. (2013) 62:2217–26. doi: 10.1016/j.jacc.2013.07.071
33. Bagnasco MS, Núñez-Gil IJ. Infective endocarditis and thoracic aortic disease: a review on forgotten psychological aspects. World J Cardiol. (2017) 9:620. doi: 10.4330/wjc.v9.i7.620
34. Angrist AA, Oka M. Pathogenesis of bacterial endocarditis. J Am Med Assoc. (1963) 183:249–52. doi: 10.1001/jama.1963.63700040009010b
35. Durack DT, Beeson PB. Experimental bacterial endocarditis. I. Colonization of a sterile vegetation. Br J Exp Pathol. (1972) 53:44–9.
36. Liesenborghs L, Meyers S, Lox M, Criel M, Claes J, Peetermans M, et al. Staphylococcus aureus endocarditis: distinct mechanisms of bacterial adhesion to damaged and inflamed heart valves. Eur Heart J. (2019) 40:3248–59. doi: 10.1093/eurheartj/ehz175
37. Chino F, Kodama A, Otake M, Dock DS. Nonbacterial thrombotic endocarditis in a Japanese autopsy sample. A review of eighty cases. Am Heart J. (1975) 90:190–8. doi: 10.1016/0002-8703(75)90119-2
38. Gould K, Ramirez Ronda CH, Holmes RK, Sanford JP. Adherence of bacteria to heart valves in vitro. J Clin Invest. (1975) 56:1364–70. doi: 10.1172/JCI108216
39. Yersin B, Glauser MP, Guze PA, Guze LB, Freedman LR. Experimental Escherichia coli endocarditis in rats: roles of serum bactericidal activity and duration of catheter placement. Infect Immun. (1988) 56:1273–80. doi: 10.1128/IAI.56.5.1273-1280.1988
40. Burnette-Curley D, Wells V, Viscount H, Munro CL, Fenno JC, Fives-Taylor P, et al. FimA, a major virulence factor associated with Streptococcus parasanguis endocarditis. Infect Immun. (1995) 63:4669–74. doi: 10.1128/IAI.63.12.4669-4674.1995
41. Vernachio J, Bayer AS, Le T, Chai YL, Prater B, Schneider A, et al. Anti-clumping factor A immunoglobulin reduces the duration of methicillin-resistant Staphylococcus aureus bacteremia in an experimental model of infective endocarditis. Antimicrob Agents Chemother. (2003) 47:3400–6. doi: 10.1128/AAC.47.11.3400-3406.2003
42. Heying R, van de Gevel J, Que Y-A, Moreillon P, Beekhuizen H. Fibronectin-binding proteins and clumping factor A in Staphylococcus aureus experimental endocarditis: FnBPA is sufficient to activate human endothelial cells. Thromb Haemost. (2007) 97:617–26. doi: 10.1160/TH06-11-0640
43. Hauck CR, Ohlsen K. Sticky connections: extracellular matrix protein recognition and integrin-mediated cellular invasion by Staphylococcus aureus. Curr Opin Microbiol. (2006) 9:5–11. doi: 10.1016/j.mib.2005.12.002
44. Chavakis T, Wiechmann K, Preissner KT, Herrmann M. Staphylococcus aureus interactions with the endothelium. The role of bacterial “Secretable Expanded Repertoire Adhesive Molecules” (SERAM) in disturbing host defense systems. Thromb Haemost. (2005) 94:278–85. doi: 10.1160/TH05-05-0306
45. Nallapareddy SR, Sillanpää J, Mitchel J, Singh K V., Chowdhury SA, Weinstock GM, et al. Conservation of Ebp-type pilus genes among enterococci and demonstration of their role in adherence of Enterococcus faecalis to human platelets. Infect Immun. (2011) 79:2911–20. doi: 10.1128/IAI.00039-11
46. Liesenborghs L, Peetermans M, Claes J, Veloso TR, Vandenbriele C, Criel M, et al. Shear-resistant binding to von Willebrand factor allows staphylococcus lugdunensis to adhere to the cardiac valves and initiate endocarditis. J Infect Dis. (2016) 213:1148–56. doi: 10.1093/infdis/jiv773
47. Liesenborghs L, Verhamme P, Vanassche T. Staphylococcus aureus, master manipulator of the human hemostatic system. J Thromb Haemost. (2018) 16:441–54. doi: 10.1111/jth.13928
48. Stewart PS, Costerton JW. Antibiotic resistance of bacteria in biofilms. Lancet. (2001) 358:135–8. doi: 10.1016/S0140-6736(01)05321-1
49. Elgharably H, Hussain ST, Shrestha NK, Blackstone EH, Pettersson GB. Current hypotheses in cardiac surgery: biofilm in infective endocarditis. Semin Thorac Cardiovasc Surg. (2016) 28:56–9. doi: 10.1053/j.semtcvs.2015.12.005
50. Di Domenico EG, Rimoldi SG, Cavallo I, D'Agosto G, Trento E, Cagnoni G, et al. Microbial biofilm correlates with an increased antibiotic tolerance and poor therapeutic outcome in infective endocarditis. BMC Microbiol. (2019) 19:228. doi: 10.1186/s12866-019-1596-2
51. Veloso TR, Que YA, Chaouch A, Giddey M, Vouillamoz J, Rousson V, et al. Prophylaxis of experimental endocarditis with antiplatelet and antithrombin agents: a role for long-term prevention of infective endocarditis in humans? in J Infect Dis. 211:72–9. doi: 10.1093/infdis/jiu426
52. Lerche CJ, Christophersen LJ, Goetze JP, Nielsen PR, Thomsen K, Enevold C, et al. Adjunctive dabigatran therapy improves outcome of experimental left-sided Staphylococcus aureus endocarditis. PLoS ONE. (2019) 14:e0215333. doi: 10.1371/journal.pone.0215333
53. Eisen DP, Corey GR, McBryde ES, Fowler VG, Miro JM, Cabell CH, et al. Reduced valve replacement surgery and complication rate in Staphylococcus aureus endocarditis patients receiving acetyl-salicylic acid. J Infect. (2009) 58:332–8. doi: 10.1016/j.jinf.2009.03.006
54. Peetermans M, Liesenborghs L, Peerlinck K, Wijngaerden E Van, Gheysens O, Goffin KE, et al. Targeting coagulase activity in Staphylococcus aureus bacteraemia: a randomized controlled single-centre trial of staphylothrombin inhibition. Thromb Haemost. (2018) 118:818–29. doi: 10.1055/s-0038-1639586
55. Anavekar NS, Tleyjeh IM, Anavekar NS, Mirzoyev Z, Steckelberg JM, Haddad C, et al. Impact of prior antiplatelet therapy on risk of embolism in infective endocarditis. Clin Infect Dis. (2007) 44:1180–6. doi: 10.1086/513197
56. Chan KL, Dumesnil JG, Cujec B, Sanfilippo AJ, Jue J, Turek MA, et al. A randomized trial of aspirin on the risk of embolic events in patients with infective endocarditis. J Am Coll Cardiol. (2003) 42:775–80. doi: 10.1016/S0735-1097(03)00829-5
57. Olmos C, Vilacosta I, Pozo E, Fernández C, Sarriá C, López J, et al. Prognostic implications of diabetes in patients with left-sided endocarditis. Medicine. (2014) 93:114–9. doi: 10.1097/MD.0000000000000023
58. Ruch Y, Hansmann Y, Riegel P, Lefebvre N, Mazzucotelli JP, Douiri N, et al. Virulence of beta-hemolytic streptococci in infective endocarditis. Infection. (2020) 48:91–7. doi: 10.1007/s15010-019-01358-7
59. Werdan K, Dietz S, Löffler B, Niemann S, Bushnaq H, Silber RE, et al. Mechanisms of infective endocarditis: pathogen-host interaction and risk states. Nat Rev Cardiol. (2014) 11:35–50. doi: 10.1038/nrcardio.2013.174
60. Salgado-Pabón W, Breshears L, Spaulding AR, Merriman JA, Stach CS, Horswill AR, et al. Superantigens are critical for Staphylococcus aureus infective endocarditis, sepsis, and acute kidney injury. mBio. (2013) 4:e00494-13. doi: 10.1128/mBio.00494-13
61. Stach CS, Vu BG, Merriman JA, Herrera A, Cahill MP, Schlievert PM, et al. Novel tissue level effects of the Staphylococcus aureus enterotoxin gene cluster are essential for infective endocarditis. PLoS ONE. (2016) 11:e0154762. doi: 10.1371/journal.pone.0154762
62. Werdan K, Oelke A, Hettwer S, Nuding S, Bubel S, Hoke R, et al. Septic cardiomyopathy: hemodynamic quantification, occurrence, and prognostic implications. Clin Res Cardiol. (2011) 100:661–8. doi: 10.1007/s00392-011-0292-5
63. Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. J Oral Maxillofac Surg. (1994) 52:1225. doi: 10.1016/0278-2391(94)90556-8
64. Li JS, Sexton DJ, Mick N, Nettles R, Fowler VG, Ryan T, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. (2000) 30:633–8. doi: 10.1086/313753
65. Lamas CC, Eykyn SJ. Suggested modifications to the Duke criteria for the clinical diagnosis of native valve and prosthetic valve endocarditis: analysis of 118 pathologically proven cases. Clin Infect Dis. (1997) 25:713–9. doi: 10.1086/513765
66. Pérez-Vázquez A, Fariñas MC, Garcia-Palomo JD, Bernal JM, Revuelta JM, González-Macías J. Evaluation of the duke criteria in 93 episodes of prosthetic valve endocarditis: could sensitivity be improved? Arch Intern Med. (2000) 160:1185–91. doi: 10.1001/archinte.160.8.1185
67. Doherty JU, Kort S, Mehran R, Schoenhagen P, Soman P. ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2017 Appropriate Use Criteria for Multimodality Imaging in Valvular Heart Disease: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery. J Am Coll Cardiol. (2017) 70:1647–72. doi: 10.1016/j.jacc.2017.07.732
68. Liu YW, Tsai WC, Lin CC, Hsu CH, Li WT, Lin LJ, et al. Usefulness of real-time three-dimensional echocardiography for diagnosis of infective endocarditis. Scand Cardiovasc J. (2009) 43:318–23. doi: 10.1080/14017430902737940
69. Pfister R, Betton Y, ten Freyhaus H, Jung N, Baldus S, Michels G. Three-dimensional compared to two-dimensional transesophageal echocardiography for diagnosis of infective endocarditis. Infection. (2016) 44:725–31. doi: 10.1007/s15010-016-0908-9
70. Hansalia S, Biswas M, Dutta R, Hage FG, Hsiung MC, Nanda NC, et al. The value of live/real time three-dimensional transesophageal echocardiography in the assessment of valvular vegetations. Echocardiography. (2009) 26:1264–73. doi: 10.1111/j.1540-8175.2009.01042.x
71. Anwar AM, Nosir YFM, Alasnag M, Chamsi-Pasha H. Real time three-dimensional transesophageal echocardiography: a novel approach for the assessment of prosthetic heart valves. Echocardiography. (2014) 31:188–96. doi: 10.1111/echo.12327
72. Singh P, Inamdar V, Hage FG, Kodali V, Karakus G, Suwanjutah T, et al. Usefulness of live/real time three-dimensional transthoracic echocardiography in evaluation of prosthetic valve function: research from the university of alabama at birmingham. Echocardiography. (2009) 26:1236–49. doi: 10.1111/j.1540-8175.2009.01079.x
73. Shapira Y, Weisenberg DE, Vaturi M, Sharoni E, Raanani E, Sahar G, et al. The impact of intraoperative transesophageal echocardiography in infective endocarditis. Isr Med Assoc J. (2007) 9:299–302.
74. Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. 2015 ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European Society of Cardiology (ESC) endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. (2015) 36, 3075–28. doi: 10.1093/eurheartj/ehv319
75. Kim IC, Chang S, Hong GR, Lee SH, Lee S, Ha JW, et al. Comparison of cardiac computed tomography with transesophageal echocardiography for identifying vegetation and intracardiac complications in patients with infective endocarditis in the era of 3-dimensional images. Circ Cardiovasc Imaging. (2018) 11:e006986. doi: 10.1161/CIRCIMAGING.117.006986
76. Sifaoui I, Oliver L, Tacher V, Fiore A, Lepeule R, Moussafeur A, et al. Diagnostic performance of transesophageal echocardiography and cardiac computed tomography in infective endocarditis. J Am Soc Echocardiogr. (2020) 33:1442–53. doi: 10.1016/j.echo.2020.07.017
77. Ye W, Ren G, Zhong X, Jian X, Chen O, Ma Q, et al. ECG-gated CT in aortic perivalvular abscess: comparison with transesophageal echocardiography and intraoperative findings. Radiology. (2020) 297:334–41. doi: 10.1148/radiol.2020200685
78. Hryniewiecki T, Zatorska K, Abramczuk E, Zakrzewski D, Szymański P, Kuśmierczyk M, et al. The usefulness of cardiac CT in the diagnosis of perivalvular complications in patients with infective endocarditis. Eur Radiol. (2019) 29:4368–76. doi: 10.1007/s00330-018-5965-2
79. Fagman E, Flinck A, Snygg-Martin U, Olaison L, Bech-Hanssen O, Svensson G. Surgical decision-making in aortic prosthetic valve endocarditis: the influence of electrocardiogram-gated computed tomography. Eur J Cardio-thoracic Surg. (2016) 50:1165–71. doi: 10.1093/ejcts/ezw177
80. Habets J, Tanis W, Van Herwerden LA, Van Den Brink RBA, Mali WPTM, De Mol BAJM, et al. Cardiac computed tomography angiography results in diagnostic and therapeutic change in prosthetic heart valve endocarditis. Int J Cardiovasc Imaging. (2014) 30:377–87. doi: 10.1007/s10554-013-0335-2
81. Wang TKM, Bin Saeedan M, Chan N, Obuchowski NA, Shrestha N, Xu B, et al. Complementary diagnostic and prognostic contributions of cardiac computed tomography for infective endocarditis surgery. Circ Cardiovasc Imaging. (2020) 13:e011126. doi: 10.1161/CIRCIMAGING.120.011126
82. Saby L, Laas O, Habib G, Cammilleri S, Mancini J, Tessonnier L, et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: increased valvular 18F- fluorodeoxyglucose uptake as a novel major criterion. J Am Coll Cardiol. (2013) 61:2374–82. doi: 10.1016/j.jacc.2013.01.092
83. Rouzet F, Chequer R, Benali K, Lepage L, Ghodbane W, Duval X, et al. Respective performance of 18F-FDG PET and radiolabeled leukocyte scintigraphy for the diagnosis of prosthetic valve endocarditis. J Nucl Med. (2014) 55:1980–5. doi: 10.2967/jnumed.114.141895
84. Bensimhon L, Lavergne T, Hugonnet F, Mainardi JL, Latremouille C, Maunoury C, et al. Whole body [18F]fluorodeoxyglucose positron emission tomography imaging for the diagnosis of pacemaker or implantable cardioverter defibrillator infection: a preliminary prospective study. Clin Microbiol Infect. (2011) 17:836–44. doi: 10.1111/j.1469-0691.2010.03312.x
85. Pizzi MN, Roque A, Fernández-Hidalgo N, Cuéllar-Calabria H, Ferreira-González I, Gonzàlez-Alujas MT, et al. Improving the diagnosis of infective endocarditis in prosthetic valves and intracardiac devices with 18F-fluordeoxyglucose positron emission tomography/computed tomography angiography: initial results at an infective endocarditis referral center. Circulation. (2015) 132:1113–26. doi: 10.1161/CIRCULATIONAHA.115.015316
86. Małecka BA, Zabek A, Debski M, Szot W, Holcman K, Boczar K, et al. The usefulness of SPECT-CT with radioisotope-labeled leukocytes in diagnosing lead-dependent infective endocarditis. Adv Clin Exp Med. (2019) 28:113–9. doi: 10.17219/acem/92315
87. Erba PA, Conti U, Lazzeri E, Sollini M, Doria R, De Tommasi SM, et al. Added value of 99mTc-HMPAO-labeled leukocyte SPECT/ CT in the characterization and management of patients with infectious endocarditis. J Nucl Med. (2012) 53:1235–43. doi: 10.2967/jnumed.111.099424
88. Erba PA, Sollini M, Conti U, Bandera F, Tascini C, De Tommasi SM, et al. Radiolabeled WBC scintigraphy in the diagnostic workup of patients with suspected device-related infections. JACC Cardiovasc Imaging. (2013) 6:1075–86. doi: 10.1016/j.jcmg.2013.08.001
89. Juneau D, Golfam M, Hazra S, Zuckier LS, Garas S, Redpath C, et al. Positron emission tomography and single-photon emission computed tomography imaging in the diagnosis of cardiac implantable electronic device infection. Circ Cardiovasc Imaging. (2017) 10:e005772. doi: 10.1161/CIRCIMAGING.116.005772
90. Swart LE, Gomes A, Scholtens AM, Sinha B, Tanis W, Lam MGEH, et al. Improving the diagnostic performance of 18F-fluorodeoxyglucose positron-emission tomography/computed tomography in prosthetic heart valve endocarditis. Circulation. (2018) 138:1412–27. doi: 10.1161/CIRCULATIONAHA.118.035032
91. Scholtens AM, Van Aarnhem EEHL, Budde RP. Effect of antibiotics on FDG-PET/CT imaging of prosthetic heart valve endocarditis. Eur Heart J Cardiovasc Imaging. (2015) 16:1223. doi: 10.1093/ehjci/jev186
92. San S, Ravis E, Tessonier L, Philip M, Cammilleri S, Lavagna F, et al. Prognostic value of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in infective endocarditis. J Am Coll Cardiol. (2019) 74:1031–40. doi: 10.1016/j.jacc.2019.06.050
93. De Camargo RA, Sommer Bitencourt M, Meneghetti JC, Soares J, Gonçalves LFT, Buchpiguel CA, et al. The role of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in the diagnosis of left-sided endocarditis: native vs prosthetic valves endocarditis. Clin Infect Dis. (2020) 70:583–94. doi: 10.1093/cid/ciz267
94. Kouijzer IJE, Berrevoets MAH, Aarntzen EHJG, De Vries J, Van Dijk APJ, Oyen WJG, et al. 18F-fluorodeoxyglucose positron-emission tomography combined with computed tomography as a diagnostic tool in native valve endocarditis. Nucl Med Commun. (2018) 39:747–52. doi: 10.1097/MNM.0000000000000864
95. Duval X, Le Moing V, Tubiana S, Esposito-Farèse M, Ilic-Habensus E, Leclercq F, et al. Impact of systematic whole-body 18F-Fluorodeoxyglucose PET/CT on the management of patients suspected of infective endocarditis: the prospective multicenter TEPvENDO study. Clin Infect Dis. (2020). doi: 10.1093/cid/ciaa666. [Epub ahead of print].
96. Wahadat AR, Tanis W, Swart LE, Scholtens A, Krestin GP, van Mieghem NMDA, et al. Added value of 18F-FDG-PET/CT and cardiac CTA in suspected transcatheter aortic valve endocarditis. J Nucl Cardiol. (2019). doi: 10.1007/s12350-019-01963-x. [Epub ahead of print].
97. Kim J, Feller ED, Chen W, Liang Y, Dilsizian V. FDG PET/CT for early detection and localization of left ventricular assist device infection: impact on patient management and outcome. JACC Cardiovasc Imaging. (2019) 12:722–9. doi: 10.1016/j.jcmg.2018.01.024
98. Tam MC, Patel VN, Weinberg RL, Hulten EA, Aaronson KD, Pagani FD, et al. Diagnostic accuracy of FDG PET/CT in suspected LVAD infections: a case series, systematic review, and meta-analysis. JACC Cardiovasc Imaging. (2020) 13:1191–202. doi: 10.1016/j.jcmg.2019.04.024
99. Litzler PY, Manrique A, Etienne M, Salles A, Edet-Sanson A, Vera P, et al. Leukocyte SPECT/CT for detecting infection of left-ventricular-assist devices: preliminary results. J Nucl Med. (2010) 51:1044–8. doi: 10.2967/jnumed.109.070664
100. de Vaugelade C, Mesguich C, Nubret K, Camou F, Greib C, Dournes G, et al. Infections in patients using ventricular-assist devices: Comparison of the diagnostic performance of 18 F-FDG PET/CT scan and leucocyte-labeled scintigraphy. J Nucl Cardiol. (2019) 26:42–55. doi: 10.1007/s12350-018-1323-7
101. Orvin K, Goldberg E, Bernstine H, Groshar D, Sagie A, Kornowski R, et al. The role of FDG-PET/CT imaging in early detection of extra-cardiac complications of infective endocarditis. Clin Microbiol Infect. (2015) 21:69–76. doi: 10.1016/j.cmi.2014.08.012
102. Snygg-Martin U, Gustafsson L, Rosengren L, Alsiö Å, Ackerholm P, Andersson R, et al. Cerebrovascular complications in patients with left-sided infective endocarditis are common: a prospective study using magnetic resonance imaging and neurochemical brain damage markers. Clin Infect Dis. (2008) 47:23–30. doi: 10.1086/588663
103. Duval X, Iung B, Klein I, Brochet E, Thabut G, Arnoult F, et al. Effect of early cerebral magnetic resonance imaging on clinical decisions in infective endocarditis: a prospective study. Ann Intern Med. (2010) 152:497–504. doi: 10.7326/0003-4819-152-8-201004200-00006
104. Nakamura M, Uzuka T, Sato H, Kondo M, Sakata J, Kodama F, et al. Early surgery with aggressive surgical approach to improve 6-month outcomes in patients with active infective endocarditis: contribution of cerebral preoperative magnetic resonance imaging. Gen Thorac Cardiovasc Surg. (2019) 67:427–35. doi: 10.1007/s11748-018-1040-9
105. Chakraborty T, Scharf E, DeSimone D, El Rafei A, Brinjikji W, Baddour LM, et al. Variable significance of brain mri findings in infective endocarditis and its effect on surgical decisions. Mayo Clin Proc. (2019) 94:1024–32. doi: 10.1016/j.mayocp.2018.09.015
106. Haller S, Vernooij MW, Kuijer JPA, Larsson EM, Jäger HR, Barkhof F. Cerebral microbleeds: imaging and clinical significance. Radiology. (2018) 287:11–28. doi: 10.1148/radiol.2018170803
107. Chakraborty T, Scharf E, Rabinstein AA, DeSimone D, El Rafei A, Brinjikji W, et al. Utility of brain magnetic resonance imaging in the surgical management of infective endocarditis. J Stroke Cerebrovasc Dis. (2017) 26:2527–35. doi: 10.1016/j.jstrokecerebrovasdis.2017.05.047
108. Lecomte R, Issa N, Gaborit B, Le Turnier P, Deschanvres C, Asseray N, et al. Risk-benefit assessment of systematic thoracoabdominal-pelvic computed tomography in infective endocarditis. Clin Infect Dis. (2019) 69:1605–12. doi: 10.1093/cid/ciz014
109. Shmueli H, Thomas F, Flint N, Setia G, Janjic A, Siegel RJ. Right-sided infective endocarditis 2020: challenges and updates in diagnosis and treatment. J Am Heart Assoc. (2020) 9:e017293. doi: 10.1161/JAHA.120.017293
110. Paul G, Michels G, Hohmann C, Pfister R, Mader N, Blanke L, et al. Contrast-enhanced ultrasound for the detection of abdominal complications in infective endocarditis: first experience from a prospective cohort. Ultrasound Med Biol. (2020) 46:2965–71. doi: 10.1016/j.ultrasmedbio.2020.07.027
111. Boleij A, Van Gelder MMHJ, Swinkels DW, Tjalsma H. Clinical importance of streptococcus gallolyticus infection among colorectal cancer patients: systematic review and meta-analysis. Clin Infect Dis. (2011) 53:870–8. doi: 10.1093/cid/cir609
112. Pericàs JM, Corredoira J, Moreno A, García-País MJ, Falces C, Rabuñal R, et al. Relationship between Enterococcus faecalis infective endocarditis and colorectal neoplasm: preliminary results from a cohort of 154 patients. Rev Esp Cardiol. (2017) 70:451–8. doi: 10.1016/j.recesp.2016.09.055
113. Escolà-Vergé L, Peghin M, Givone F, Pérez-Rodríguez MT, Suárez-Varela M, Meije Y, et al. Prevalence of colorectal disease in Enterococcus faecalis infective endocarditis: results of an observational multicenter study. Rev Esp Cardiol. (2020) 73:711–7. doi: 10.1016/j.recesp.2019.07.016
114. Delahaye F, M'Hammedi A, Guerpillon B, De Gevigney G, Boibieux A, Dauwalder O, et al. Systematic search for present and potential portals of entry for infective endocarditis. J Am Coll Cardiol. (2016) 67:151–8. doi: 10.1016/j.jacc.2015.10.065
115. Vollmer T, Piper C, Horstkotte D, Körfer R, Kleesiek K, Dreier J. 23S rDNA real-time polymerase chain reaction of heart valves: A decisive tool in the diagnosis of infective endocarditis. Eur Heart J. (2010) 31:1105–13. doi: 10.1093/eurheartj/ehp600
116. Fournier PE, Thuny F, Richet H, Lepidi H, Casalta JP, Arzouni JP, et al. Comprehensive diagnostic strategy for blood culture-negative endocarditis: a prospective study of 819 new cases. Clin Infect Dis. (2010) 51:131–40. doi: 10.1086/653675
117. Ris T, Teixeira-Carvalho A, Coelho RMP, Brandao-de-Resende C, Gomes MS, Amaral LR, et al. Inflammatory biomarkers in infective endocarditis: machine learning to predict mortality. Clin Exp Immunol. (2019) 196:374–82. doi: 10.1111/cei.13266
118. Chen W, Dilsizian V. Molecular imaging of cardiovascular device infection: targeting the bacteria or the host-pathogen immune response? J Nucl Med. (2020) 61:319–26. doi: 10.2967/jnumed.119.228304
119. Snipsøyr MG, Ludvigsen M, Petersen E, Wiggers H, Honoré B. A systematic review of biomarkers in the diagnosis of infective endocarditis. Int J Cardiol. (2016) 202:564–70. doi: 10.1016/j.ijcard.2015.09.028
120. Snipsøyr MG, Wiggers H, Ludvigsen M, Stensballe A, Vorum H, Poulsen SH, et al. Towards identification of novel putative biomarkers for infective endocarditis by serum proteomic analysis. Int J Infect Dis. (2020) 96:73–81. doi: 10.1016/j.ijid.2020.02.026
121. Martí-Carvajal AJ, Dayer M, Conterno LO, Gonzalez Garay AG, Martí-Amarista CE. A comparison of different antibiotic regimens for the treatment of infective endocarditis. Cochrane Database Syst Rev. (2020) 5:CD009880. doi: 10.1002/14651858.CD009880.pub3
122. Béraud G, Pulcini C, Paño-Pardo JR, Hoen B, Beovic B, Nathwani D. How do physicians cope with controversial topics in existing guidelines for the management of infective endocarditis? Results of an international survey. Clin Microbiol Infect. (2016) 22:163–70. doi: 10.1016/j.cmi.2015.10.013
123. Tissot-Dupont H, Casalta JP, Gouriet F, Hubert S, Salaun E, Habib G, et al. International experts' practice in the antibiotic therapy of infective endocarditis is not following the guidelines. Clin Microbiol Infect. (2017) 23:736–9. doi: 10.1016/j.cmi.2017.03.007
124. Luque Paz D, Lakbar I, Tattevin P. A review of current treatment strategies for infective endocarditis. Expert Rev Anti Infect Ther. (2020). doi: 10.1080/14787210.2020.1822165. [Epub ahead of print].
125. Baddour LM, Wilson WR, Bayer AS, Fowler VG, Tleyjeh IM, Rybak MJ, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation. (2015) 132:1435–86. doi: 10.1161/CIR.0000000000000296
126. Carugati M, Petti CA, Arnold C, Miro JM, Pericàs JM, De La Maria CG, et al. Antistaphylococcal β-lactams vs. vancomycin for treatment of infective endocarditis due to methicillin-susceptible coagulase-negative staphylococci: a prospective cohort study from the international collaboration on endocarditis. Antimicrob Agents Chemother. (2016) 60:6341–9. doi: 10.1128/AAC.01531-16
127. Francioli P, Ruch W, Stamboulian D. Treatment of streptococcal endocarditis with a single daily dose of ceftriaxone and netilmicin for 14 Days: a prospective multicenter study. Clin Infect Dis. (1995) 21:1406–10. doi: 10.1093/clinids/21.6.1406
128. Knoll B, Tleyjeh IM, Steckelberg JM, Wilson WR, Baddour LM. Infective endocarditis due to penicillin-resistant viridans group streptococci. Clin Infect Dis. (2007) 44:1585–92. doi: 10.1086/518174
129. Lebeaux D, Fernández-Hidalgo N, Pilmis B, Tattevin P, Mainardi JL. Aminoglycosides for infective endocarditis: time to say goodbye? Clin Microbiol Infect. (2020) 26:723–8. doi: 10.1016/j.cmi.2019.10.017
130. Dahl A, Rasmussen RV, Bundgaard H, Hassager C, Bruun LE, Lauridsen TK, et al. Enterococcus faecalis infective endocarditis a pilot study of the relationship between duration of gentamicin treatment and outcome. Circulation. (2013) 127:1810–7. doi: 10.1161/CIRCULATIONAHA.112.001170
131. Gavaldà J, Len O, Miró JM, Muñoz P, Montejo M, Alarcón A, et al. Brief communication: treatment of Enterococcus faecalis endocarditis with ampicillin plus ceftriaxone. Ann Intern Med. (2007) 146:574–9. doi: 10.7326/0003-4819-146-8-200704170-00008
132. Fernández-Hidalgo N, Almirante B, Gavaldà J, Gurgui M, Peña C, De Alarcón A, et al. Ampicillin plus ceftriaxone is as effective as ampicillin plus gentamicin for treating enterococcus faecalis infective endocarditis. Clin Infect Dis. (2013) 56:1261–8. doi: 10.1093/cid/cit052
133. Korzeniowski O, Sande MA. Combination antimicrobial therapy for Staphylococcus aureus endocarditis in patients addicted to parenteral drugs and in nonaddicts. A prospective study. Ann Intern Med. (1982) 97:496–503. doi: 10.7326/0003-4819-97-4-496
134. Cosgrove SE, Vigliani GA, Campion M, Fowler VG, Abrutyn E, Ralph Corey G, et al. Initial low-dose gentamicin for staphylococcusaureus bacteremia and endocarditis is nephrotoxic. Clin Infect Dis. (2009) 48:713–21. doi: 10.1086/597031
135. Ramos-Martínez A, Muñoz Serrano A, de Alarcón González A, Muñoz P, Fernández-Cruz A, Valerio M, et al. Gentamicin may have no effect on mortality of staphylococcal prosthetic valve endocarditis. J Infect Chemother. (2018) 24:555–62. doi: 10.1016/j.jiac.2018.03.003
136. Riedel DJ, Weekes E, Forrest GN. Addition of rifampin to standard therapy for treatment of native valve infective endocarditis caused by Staphylococcus aureus. Antimicrob Agents Chemother. (2008) 52:2463–7. doi: 10.1128/AAC.00300-08
137. Shrestha NK, Shah SY, Wang H, Hussain ST, Pettersson GB, Nowacki AS, et al. Rifampin for surgically treated staphylococcal infective endocarditis: a propensity score-adjusted cohort study. Ann Thorac Surg. (2016) 101:2243–50. doi: 10.1016/j.athoracsur.2015.11.015
138. García-de-la-Mària C, Gasch O, Castañeda X, García-González J, Soy D, Cañas MA, et al. Cloxacillin or fosfomycin plus daptomycin combinations are more active than cloxacillin monotherapy or combined with gentamicin against MSSA in a rabbit model of experimental endocarditis. J Antimicrob Chemother. (2020) 75:3586–92. doi: 10.1093/jac/dkaa354
139. Grillo S, Cuervo G, Carratalà J, Grau I, Pallarès N, Tebé C, et al. Impact of β-Lactam and daptomycin combination therapy on clinical outcomes in methicillin-susceptible Staphylococcus aureus bacteremia: a propensity score-matched analysis. Clin Infect Dis. (2019) 69:1480–8. doi: 10.1093/cid/ciz018
140. Cheng MP, Lawandi A, Butler-Laporte G, De l'Etoile-Morel S, Paquette K, Lee TC. Adjunctive daptomycin in the treatment of methicillin-susceptible staphylococcus aureus bacteremia: a randomized controlled trial. Clin Infect Dis. (2020). doi: 10.1093/cid/ciaa1000. [Epub ahead of print].
141. ClinicalTrials.gov. 2000 Feb 29 -. Identifier: NCT03959345, Efficacy of Cloxacillin and Fosfomycin Combination VS. Cloxacillin Monotherapy in Patients With MSSA Bacteremia (SAFO). Bethesda, MD: National Library of Medicine (2019). Available from: https://clinicaltrials.gov/ct2/show/NCT03959345 (accessed December 12, 2020).
142. Dilworth TJ, Ibrahim O, Hall P, Sliwinski J, Walraven C, Mercier RC. β-Lactams enhance vancomycin activity against methicillin-Resistant staphylococcus aureus bacteremia compared to vancomycin alone. Antimicrob Agents Chemother. (2014) 58:102–9. doi: 10.1128/AAC.01204-13
143. Casapao AM, Jacobs DM, Bowers DR, Beyda ND, Dilworth TJ. Early administration of adjuvant β-lactam therapy in combination with vancomycin among patients with methicillin-resistant Staphylococcus aureus bloodstream infection: a retrospective, multicenter analysis. Pharmacotherapy. (2017) 37:1347–56. doi: 10.1002/phar.2034
144. Davis J, Sud A, O'Sullivan MVN, Robinson JO, Ferguson PE, Foo H, et al. Combination of vancomycin and β-lactam therapy for methicillin-resistant Staphylococcus aureus bacteremia: a pilot multicenter randomized controlled trial. Clin Infect Dis. (2016) 62:173–80. doi: 10.1093/cid/civ808
145. Tong SYC, Lye DC, Yahav D, Sud A, Robinson JO, Nelson J, et al. Effect of vancomycin or daptomycin with vs without an antistaphylococcal β-lactam on mortality, bacteremia, relapse, or treatment failure in patients with MRSA bacteremia: a randomized clinical trial. J Am Med Assoc. (2020) 323:527–37. doi: 10.1001/jama.2020.0103
146. Del Río A, García-de-la-Mària C, Entenza JM, Gasch O, Armero Y, Soy D, et al. Fosfomycin plus β-lactams as synergistic bactericidal combinations for experimental endocarditis due to methicillin-resistant and glycopeptide-intermediate Staphylococcus aureus. Antimicrob Agents Chemother. (2016) 60:478–86. doi: 10.1128/AAC.02139-15
147. Pujol M, Miró J-M, Shaw E, Aguado J-M, San-Juan R, Puig-Asensio M, et al. Daptomycin plus fosfomycin vs. daptomycin alone for methicillin-resistant Staphylococcus aureus bacteremia and endocarditis: a randomized clinical trial. Clin Infect Dis. (2020). doi: 10.1093/cid/ciaa1081. [Epub ahead of print].
148. Jorgensen SCJ, Zasowski EJ, Trinh TD, Lagnf AM, Bhatia S, Sabagha N, et al. Daptomycin plus ß-lactam combination therapy for methicillin-resistant Staphylococcus aureus bloodstream infections: a retrospective, comparative cohort study. Clin Infect Dis. (2020) 71:1–10. doi: 10.1093/cid/ciz746
149. Geriak M, Haddad F, Rizvi K, Rose W, Kullar R, LaPlante K, et al. Clinical data on daptomycin plus ceftaroline vs. standard of care monotherapy in the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Antimicrob Agents Chemother. (2019) 63:e02483-18. doi: 10.1128/AAC.02483-18
150. Ribera E, Gómez-Jimenez J, Cortes E, Del Valle O, Planes A, Teresa Gonzalez-Alujas M, et al. Effectiveness of cloxacillin with and without gentamicin in short-term therapy for right-sided Staphylococcus aureus endocarditis: a randomized, controlled trial. Ann Intern Med. (1996) 125:969–74. doi: 10.7326/0003-4819-125-12-199612150-00005
151. Olmos C, Vilacosta I, López J, Sáez C, Anguita M, García-Granja PE, et al. Short-course antibiotic regimen compared to conventional antibiotic treatment for gram-positive cocci infective endocarditis: randomized clinical trial (SATIE). BMC Infect Dis. (2020) 20:417. doi: 10.1186/s12879-020-05132-1
152. Wilson WR, Wilkowske CJ, Wright AJ, Sande MA, Geraci JE. Treatment of streptomycin-susceptible and streptomycin-resistant enterococcal endocarditis. Ann Intern Med. (1984) 100:816–23. doi: 10.7326/0003-4819-100-6-816
153. Ramos-Martínez A, Pericàs JM, Fernández-Cruz A, Muñoz P, Valerio M, Kestler M, et al. Four weeks vs. six weeks of ampicillin plus ceftriaxone in Enterococcus faecalis native valve endocarditis: a prospective cohort study. PLoS ONE. (2020) 15:e0237011. doi: 10.1371/journal.pone.0237011
154. Morris AJ, Drinković D, Pottumarthy S, MacCulloch D, Kerr AR, West T. Bacteriological outcome after valve surgery for active infective endocarditis: implications for duration of treatment after surgery. Clin Infect Dis. (2005) 41:187–94. doi: 10.1086/430908
155. Muñoz P, Giannella M, Scoti F, Predomingo M, Puga D, Pinto A, et al. Two weeks of postsurgical therapy may be enough for high-risk cases of endocarditis caused by Streptococcus viridans or Streptococcus bovis. Clin Microbiol Infect. (2012) 18:293–9. doi: 10.1111/j.1469-0691.2011.03594.x
156. Andrews MM, Von Reyn CF. Patient selection criteria and management guidelines for outpatient parenteral antibiotic therapy for native valve infective endocarditis. Clin Infect Dis. (2001) 33:203–9. doi: 10.1086/321814
157. Pericà S JM, Llopis J, González-Ramallo V, Goenaga MA, Muñoz P, García-Leoni ME, et al. Outpatient parenteral antibiotic treatment for infective endocarditis: a prospective cohort study from the GAMES Cohort. Clin Infect Dis. (2019) 69:1690–700. doi: 10.1093/cid/ciz030
158. Destache CJ, Guervil DJ, Kaye KS. Ceftaroline fosamil for the treatment of Gram-positive endocarditis: CAPTURE study experience. Int J Antimicrob Agents. (2019) 53:644–9. doi: 10.1016/j.ijantimicag.2019.01.014
159. Tascini C, Attanasio V, Ripa M, Carozza A, Pallotto C, Bernardo M, et al. Ceftobiprole for the treatment of infective endocarditis: a case series. J Glob Antimicrob Resist. (2020) 20:56–9. doi: 10.1016/j.jgar.2019.07.020
160. Rodríguez-García R, Rodríguez-Esteban MÁ, García-Carús E, Telenti M, Fernández J. In vitro activity of ceftaroline and ceftobiprole against clinical isolates of Gram-positive bacteria from infective endocarditis: are these drugs potential options for the initial management of this disease? Diagn Microbiol Infect Dis. (2020) 98:115153. doi: 10.1016/j.diagmicrobio.2020.115153
161. Werth BJ, Barber KE, Tran KNT, Nonejuie P, Sakoulas G, Pogliano J, et al. Ceftobiprole and ampicillin increase daptomycin susceptibility of daptomycin-susceptible and -resistant vre. J Antimicrob Chemother. (2015) 70:489–93. doi: 10.1093/jac/dku386
162. Sader HS, Mendes RE, Pfaller MA, Flamm RK. Antimicrobial activity of dalbavancin tested against Gram-positive organisms isolated from patients with infective endocarditis in US and European medical centres. J Antimicrob Chemother. (2019) 74:1306–10. doi: 10.1093/jac/dkz006
163. Tobudic S, Forstner C, Burgmann H, Lagler H, Ramharter M, Steininger C, et al. Dalbavancin as primary and sequential treatment for gram-positive infective endocarditis: 2-year experience at the general hospital of vienna. Clin Infect Dis. (2018) 67:795–8. doi: 10.1093/cid/ciy279
164. Hidalgo-Tenorio C, Vinuesa D, Plata A, Martin Dávila P, Iftimie S, Sequera S, et al. DALBACEN cohort: Dalbavancin as consolidation therapy in patients with endocarditis and/or bloodstream infection produced by gram-positive cocci. Ann Clin Microbiol Antimicrob. (2019) 18:30. doi: 10.1186/s12941-019-0329-6
165. Heldman AW, Hartert T V., Ray SC, Daoud EG, Kowalski TE, Pompili VJ, et al. Oral antibiotic treatment of right-sided staphylococcal endocarditis in injection drug users: prospective randomized comparison with parenteral therapy. Am J Med. (1996) 101:68–76. doi: 10.1016/S0002-9343(96)00070-8
166. Mzabi A, Kernéis S, Richaud C, Podglajen I, Fernandez-Gerlinger MP, Mainardi JL. Switch to oral antibiotics in the treatment of infective endocarditis is not associated with increased risk of mortality in non–severely ill patients. Clin Microbiol Infect. (2016) 22:607–12. doi: 10.1016/j.cmi.2016.04.003
167. Stamboulian D, Bonvehi P, Arevalo C, Bologna R, Cassetti I, Scilingo V, et al. Antibiotic management of outpatients with endocarditis due to penicillin-susceptible streptococci. Rev Infect Dis. (1991) 13:S160–S3. doi: 10.1093/clinids/13.Supplement_2.S160
168. Iversen K, Ihlemann N, Gill SU, Madsen T, Elming H, Jensen KT, et al. Partial oral vs. intravenous antibiotic treatment of endocarditis. N Engl J Med. (2019) 380:415–24. doi: 10.1056/NEJMoa1808312
169. Arnold CJ, Johnson M, Bayer AS, Bradley S, Giannitsioti E, Miró JM, et al. Candida infective endocarditis: an observational cohort study with a focus on therapy. Antimicrob Agents Chemother. (2015) 59:2365–73. doi: 10.1128/AAC.04867-14
170. Katsouli A, Massad MG. Current issues in the diagnosis and management of blood culture-negative infective and non-infective endocarditis. Ann Thorac Surg. (2013) 95:1467–74. doi: 10.1016/j.athoracsur.2012.10.044
171. Tattevin P, Watt G, Revest M, Arvieux C, Fournier PE. Update on blood culture-negative endocarditis. Med Mal Infect. (2015) 45:1–8. doi: 10.1016/j.medmal.2014.11.003
172. Kang D-H, Kim Y-J, Kim S-H, Sun BJ, Kim D-H, Yun S-C, et al. Early surgery vs. conventional treatment for infective endocarditis. N Engl J Med. (2012) 366:2466–73. doi: 10.1056/NEJMoa1112843
173. Lalani T, Cabell CH, Benjamin DK, Lasca O, Naber C, Fowler VG, et al. Analysis of the impact of early surgery on in-hospital mortality of native valve endocarditis: use of propensity score and instrumental variable methods to adjust for treatment-selection bias. Circulation. (2010) 121:1005–13. doi: 10.1161/CIRCULATIONAHA.109.864488
174. Lalani T, Chu VH, Park LP, Cecchi E, Corey GR, Durante-Mangoni E, et al. In-hospital and 1-year mortality in patients undergoing early surgery for prosthetic valve endocarditis. JAMA Intern Med. (2013) 173:1495–504. doi: 10.1001/jamainternmed.2013.8203
175. Chirouze C, Alla F, Fowler VG, Sexton DJ, Corey GR, Chu VH, et al. Impact of early valve surgery on outcome of staphylococcus aureus prosthetic valve infective endocarditis: analysis in the international collaboration of endocarditis-prospective cohort study. Clin Infect Dis. (2015) 60:741–9. doi: 10.1093/cid/ciu871
176. Wang A, Chu VH, Athan E, Delahaye F, Freiberger T, Lamas C, et al. Association between the timing of surgery for complicated, left-sided infective endocarditis and survival. Am Heart J. (2019) 210:108–16. doi: 10.1016/j.ahj.2019.01.004
177. Botelho-Nevers E, Thuny F, Casalta JP, Richet H, Gouriet F, Collart F, et al. Dramatic reduction in infective endocarditis-related mortality with a management-based approach. Arch Intern Med. (2009) 169:1290–8. doi: 10.1001/archinternmed.2009.192
Keywords: infective endocarditis, transesophageal echocardiography - three-dimensional echocardiography, positron - emission tomography, Staphycoccus aureus, viridans group streptococci, Enterococcus
Citation: Cuervo G, Escrihuela-Vidal F, Gudiol C and Carratalà J (2021) Current Challenges in the Management of Infective Endocarditis. Front. Med. 8:641243. doi: 10.3389/fmed.2021.641243
Received: 13 December 2020; Accepted: 01 February 2021;
Published: 22 February 2021.
Edited by:
Alessandro Russo, University of Pisa, ItalyCopyright © 2021 Cuervo, Escrihuela-Vidal, Gudiol and Carratalà. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guillermo Cuervo, Z3VpbGxlcm1vLmN1ZXJ2b0BiZWxsdml0Z2Vob3NwaXRhbC5jYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.