
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Med. , 13 April 2021
Sec. Hematology
Volume 8 - 2021 | https://doi.org/10.3389/fmed.2021.577081
 Laura Hernández-Hernández1,2
Laura Hernández-Hernández1,2 Catalina Sanz2,3Elena Marcos-Vadillo2,4
Catalina Sanz2,3Elena Marcos-Vadillo2,4 Asunción García-Sánchez2,5Esther Moreno1,2,4,5Félix Lorente1,2,5
Asunción García-Sánchez2,5Esther Moreno1,2,4,5Félix Lorente1,2,5 David González-de-Olano6
David González-de-Olano6 Ignacio Dávila1,2,5*María Isidoro-García2,4,7
Ignacio Dávila1,2,5*María Isidoro-García2,4,7Background: Some recent familial studies have described a pattern of autosomal dominant inheritance for increased basal serum tryptase (BST), but no correlation with mRNA expression and gene dose have been reported.
Objective: We analyzed TPSAB1 mRNA expression and gene dose in a four-member family with high BST and in two control subjects.
Methods: Blood samples were collected from the family and control subjects. Complete morphologic, immunophenotypical, and molecular bone marrow mast cell (MC) studies were performed. mRNA gene expression and gene dose were performed in a LightCycler 480 instrument. Genotype and CNV were performed by quantitative real-time digital PCR (qdPCR).
Results: CNV analysis revealed a hereditary copy number gain genotype (3β2α) present in all the family members studied. The elevated total BST in the family members correlated with a significant increase in tryptase gene expression and dose.
Conclusions and Clinical Relevance: We present a family with hereditary α-tryptasemia and elevated BST which correlated with a high expression of tryptase genes and an increased gene dose. The family members presented with atypical MC-mediator release symptoms or were even asymptomatic. Clinicians should be aware that elevated BST does not always mean an MC disorder.
Mast cells (MCs) are tissue effector cells that participate in several physiologic and pathologic processes such as innate immunity, immunomodulation, allergy, autoimmunity, and neuroinflammation (1). Upon activation, MCs release preformed molecules stored in secretory granules, newly synthetized mediators, and several cytokines. On the stored proteases tryptase is a serine protease related to trypsin. Baseline serum tryptase (BST) levels correlate with MC burden and/or MC number in acute allergic reactions, thus providing a measure of MC activation (2).
Mast cell disorders (MCD) can be associated to an increased number of mast cells, activation of MCs, or both. A recent consensus (3) has classified MC activation (MCA) disorders in primary mast cell activation syndrome (MCAS)—when clonality is present—secondary MCAS, and idiopathic MCAS. The criteria indicative of systemic MCA are: (a) typical clinical signs and symptoms, (b) substantial and transient increase in an MC-derived mediator in biological fluids (being BST during or shortly after the acute event) compared to a baseline recorded either before the acute event or at least 24 h after all clinical signs and symptoms of the event have completely resolved, and (c) an objective major response of clinical symptoms to agents that attenuate the production or activity of MC-derived mediators (3). Recently, hereditary α-tryptasemia (HαT), which is associated with increased copy numbers of the TPSAB1 gene encoding α-tryptase, has been included in the last consensus report of MCD (4).
The tryptase comprises different proteases, so far α, β, γ, and δ, which show minor differences in terms of their enzymatic properties (5). To date, the best characterized tryptase is the β-tryptase. Three β-tryptase subtypes have been described (βI, βII, and βIII). β-tryptase is stored in its active form, though it is maintained with little or no activity within the secretory granules due to the low pH value and stabilization mediated by other proteins. In the absence of the factors needed for stabilization, the structure dissociates into monomers that were initially considered to be inactive, though several studies have demonstrated the existence of active β-tryptase monomers (6). Compared to β-tryptase, α-tryptase is in low levels in the circulation, without degranulation. Both enzymes have a 93–96% similarity in their amino acid sequences. In addition, other tryptases have been described: γ-tryptase, which is less related to other tryptases and δ-tryptase, which is similar to α-tryptase in its amino acid sequence and is also constitutively secreted.
A region containing the human tryptase locus has been described in chromosome 16p13.3, containing at least four genes (7). The TPSG1 gene, encoding for γ-tryptase, is followed by the TPSB2 gene, which encodes for tryptases βII/βIII, and by the TPSAB1 gene, which encodes for α-tryptase and β-tryptase. Lastly, the TPSD1 gene encodes for δ-tryptase. Although the genes encoding for tryptases βI and βIII have been previously localized within the aforementioned chromosome, there is some controversy regarding their precise position. CpG islands have been identified in this region, a fact that complicates the cloning and sequencing processes (7).
Familial occurrence of increased serum BST has been rarely described. Lyons et al. (8) reported that increases in the TPSAB1 gene, which codes for α-tryptase, were associated with BST levels >8 ng/mL. This trait is inherited, and the condition is called hereditary α-tryptasemia (HαT). We had the opportunity to study four members of a family with elevated BST for 16 years (2003–2019) which correlated with a high expression of tryptase and gene dose.
The study was approved by the local Ethics Committee of the University Hospital of Salamanca (PI120913) and an informed consent form was signed in all cases.
The index case was a patient in her fifties who in 3 years presented six events, without identifying known triggers, consisting of sudden episodes of shivering, abdominal pain, nausea, vomiting, and diarrhea, followed by muscular cramps; no cutaneous lesions, hypotension, or other symptoms appeared. The patient required hospitalization for these episodes, but symptoms resolved with supportive therapy. The index case had been studied by Internal Medicine where gastrointestinal, thyroid, suprarenal or celiac disease, carcinoid syndrome, neuroendocrine syndromes, autoimmunity, and porphyria were ruled out. The patient was then referred to the Department of Allergy. Physical exploration was unremarkable. Skin prick tests to aeroallergens and food extracts were negative. Total serum IgE was 21.6 kU/L, C3, C4, CH100, and C1-INH levels were normal, and parasite infections were ruled out. BST was 47.4 ng/ml (Thermo Scientific Phadia AB, Uppsala, Sweden). When repeated 2 months later, BST showed a value of 48.4 ng/ml. A bone marrow (BM) study was later performed strictly following the proposed criteria (9): BM MCs morphology was analyzed in toluidine blue and May-Grünwald-Giemsa-stained smears (10) and disclosed no abnormalities. Immunophenotypical analysis of CD25 expression on BM MCs was performed by flow cytometry using a multiparameter 4-color immunofluorescence technique according to consensus procedures and criteria previously defined by the Spanish Network on mastocytosis (REMA) (11, 12). Flow cytometry showed 0.006% of MCs on BM and <1/105 cells on peripheral blood. Mast cells showed a normal phenotype (CD117++, CD45+, CD25–, CD2–, CD69low, and IgE+). Study of somatic activating codon Asp816-Val KIT mutation or other KIT mutations was performed in genomic DNA from fluorescence-activated cell-sorting purified populations of BM mast cells, neutrophils, eosinophils, monocytes, lymphocytes, CD34+ hematopoietic progenitor and precursor cells, and nucleated red cells, as described elsewhere (13). No mutations were detected. Meanwhile, antihistamines were prescribed on a daily basis, but six new episodes appeared. During one of these episodes, acute serum tryptase could be determined, showing no significant increase (35.9 ng/ml), even when considering the rule of an increase in BST exceeding 20% of baseline value plus absolute 2 ng/ml. The patient could fulfill one of the diagnostic criteria of MCAS (3), although clinical symptoms were not typical. Nevertheless, she had permanently increased BST without variation during acute episodes—although the participation of other putative mediators cannot be excluded—and she did not respond to anti-mast cell mediator treatment and, thus, a MCAS diagnosis was discarded. After these initial episodes, the index case has been asymptomatic up to date. In January 2019, her tryptase levels were 38.8 ng/ml.
We carried out a determination of BST levels and genetic analysis to the index case, her sister, her two daughters, and her husband. All of them gave informed written consent to perform these procedures. Serum baseline tryptase levels were as follows: 50.2 ng/ml (index case, I.2); 30.5 ng/ml (daughter #1, II.1); 28.5 ng/ml (daughter #2, II.2), 46 ng/ml (sister, I.3), and 4.22 ng/ml (husband, I.1; Figure 1). The sister and the two daughters were completely asymptomatic, as well as the husband, so no BM biopsy was performed. Furthermore, the index case and his family has been followed for 14 years and they have all remained asymptomatic up to date. Two individuals were included as controls for the expression and gene dose analyses. The inclusion criteria were (i) no symptoms or history of allergy; (ii) no symptoms or history of asthma or other pulmonary diseases; (iii) negative skin prick tests to a battery of common aeroallergens; (iv) absence of first-degree relatives with a history of asthma or atopy; and (v) BST lower than 11.4 ng/ml.
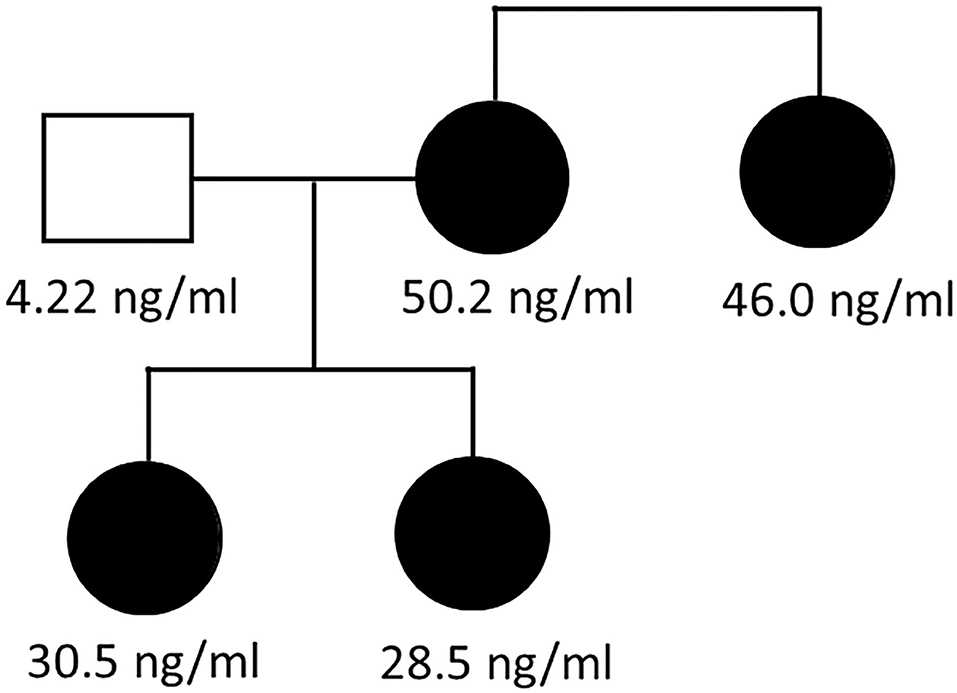
Figure 1. Family pedigree. Family pedigree showing hereditary alpha-tryptasemia syndrome. Numbers indicate serum baseline tryptase concentration (in ng/ml) in the index case (I.2), her sister (I.3), and two daughters (II.1 and II.2); values were normal in her husband (I.1).
RNA was obtained with the RiboPureTM-Blood Kit (Ambion, Life Technologies, Paisley, UK) according to the manufacturer's instructions. cDNA samples were obtained with SuperscriptTM First-Strand Synthesis System for RT-PCR (Invitrogen, Life Technologies, Carlsbad, California, USA).
Quantitative expression experiments were performed in the control group and in family members following MIQE recommendations (14). The efficiency analysis of primers was previously performed for TPS (tryptase gene) forward 5′-GCGATGTGGACAATGATGAG-3′ and reverse 5′-TTCCATTATGGGGACCTTCA-3′ primers as well as for TBP (TATA box binding protein) forward 5′-ATAGGGATTCCGGGAGTCAT-3′ and reverse 5′-GAACATCATGGATCAGAACAACA-3′ primers (TBP was used as reference). Relative quantitative PCR (qPCR) was performed in a LightCycler 480 Instrument and using SYBR Green I Master (Roche, Indianapolis, IN, USA). The luminescence signal acquisition was obtained in the last cycle of amplification (unique acquisition) and in the melting curve (continuous acquisition). Two negative control samples were included and three replications per sample were performed.
Expression differences were calculated by the Livak method (15). The process was carried out in an accredited laboratory following ISO-15189.
A relative qPCR was carried out to determine the gene-dose of TPSAB1, TPSB2, and TPSD1 genes. The efficiency of TPSAB1 primers: forward 5′-CCAAAACACCACTGCTTCCT-3′ and reverse 5′-AGGATAGGGAAGGGTCCTCA-3′; TPSB2 primers: forward 5′-CAGCGAGTGGGCATCGTT-3′, and reverse 5′-TGCATCCAGTATCGGTCGC-3′, and TPSD1 primers: forward 5′-GGGGTTTGGAGAGTCCCTTA-3′ and reverse 5′-TCCACATAGCAAGTCCGTGA-3′ was tested by generation of a standard curve with serial dilutions, using the slope of the regression line [E = 10(1–slope)]. Reactions were performed in triplicate in a final volume of 15 μl, including 50 ng of genomic DNA, SYBR Green I Master (Roche Applied Science, IN, USA), and 0.4 μM of each primer. Amplification was performed using the LightCycler 480 Instrument (Roche Applied Science, IN, USA). The qPCR protocol used an initial denaturation step (95°C for 10 s) followed by amplification and quantification steps repeated for 45 cycles (95°C for 30 s, 60°C for 30 s, and 72°C for 30 s). GAPDH was considered as the reference gene and the copy number was estimated from the normalized ratio 2 × 2–(ΔΔCt) using a DNA control obtained from a healthy subject. qPCR product quality was monitored using post-PCR melt curve analysis.
Genotyping of the TPSAB1 gene was performed by quantitative real-time digital PCR (qdPCR) using the Biomark™ HD system (Fluidigm, South SanFrancisco, CA, USA). To detect copy number variation (CNV) in α and β alleles, specific probes, as previously described in Lyons et al. (8), were used for qdPCR reaction according to the 37 K digital PCR protocol (Fluidigm). Data were analyzed using Digital PCR Analysis software (Fluidigm). Hereditary α-tryptasemia (HαT) was defined as three or more α-tryptase copies or two α-tryptase copies in the presence of three β-tryptase copies.
The databases consulted to analyze the Tryptase genes were the Genome Browser of California University (http://genome.ucsc.edu/), Aceview (http://www.ncbi.nlm.nih.gov/IEB/Research/Acembly/), Genecards (http://www.genecards.or), and NCBI from the National Center for Biotechnology Information (http://www.ncbi.nlm.nih.gov/projects/SNP/).
Statistical analysis was performed using SPSS 19.0 software (Chicago, Illinois, USA), the statistical power was analyzed with available software in http://www.dssresearch.conm/toolkit/sscalc/size_a2.asp and http://statpages.org/proppowr.html.
We had the opportunity to study four members of a family with elevated BST for 16 years. The four members of the same family were the index case (I.2), her sister (I.3), and her two daughters (II.1 and II.2). BST values were normal in her husband (I.1) and controls (Figure 1 and Table 1). Additionally, KIT mutations were negative, and a clonal MCD was discarded after the performance of a BM biopsy. Furthermore, the patient has been followed for 14 years, and has been asymptomatic for the last 9 years (except for pruritus sine materia) despite the persistence of elevated BST (Table 1). The rest of the family has also been asymptomatic all this time. We consider that this family with elevated BST, in the absence of clinical symptoms, and without clonal MCs, has an asymptomatic HαT.
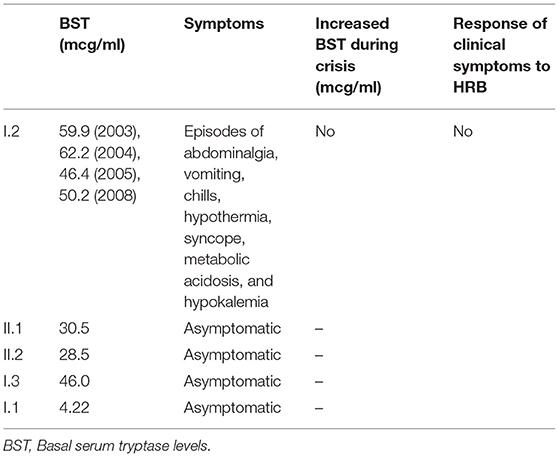
Table 1. Family clinical features.
We aimed to interrogate whether BST could correlate with mRNA expression and gene dose in this family. We detected an increase in the mRNA expression of tryptase genes in the family members compared to controls. Thus, patient I.2 showed a dramatic increment in fold change compared to control average (Table 2). Both patients I.2 and I.3 showed BST > 20 ng/ml, which was higher (average 54.67 ng/ml) for I.2 than for I.3 (46 ng/ml). The index case also presented the highest levels of tryptase gene expression. These levels correlated with a highly increased tryptase mRNA expression in those patients (Pearson 0.977, p = 0.004).
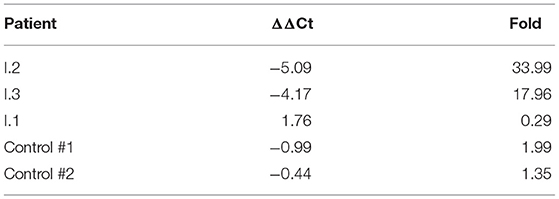
Table 2. TPSAB1 mRNA expression levels.
In addition, we detected an increase of the TPSAB1 gene dose in the family members, which correlated with BST levels (Pearson 0.868, p = 0.011), whereas TPSB2 and TPSD1 showed a normal gene dose. The index case (I.2) and their relatives I.3, II.1, and II.2 had a higher copy number than the controls for TPSAB1. Considering two as the normal number of copies, we found: patient I.2 = 4.13; patient I.3 = 4.47; patient II.1 = 4.57; and patient II.2 = 4.04. These results of CNV were confirmed, with qdPCR revealing a hereditary copy number gain genotype (3β2α) present in all family members studied (Table 3).
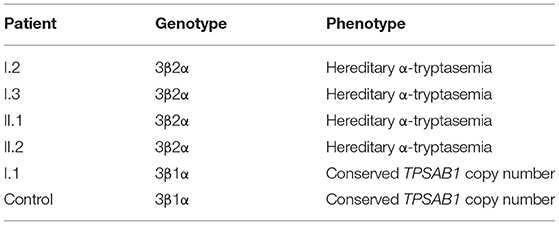
Table 3. Identified tryptase genotypes encoded at TPSAB1 and TPSB2.
We found four members of the same family with elevated BST that were followed-up for 16 years. The index case presented the highest BST and some symptoms that could be compatible with atypical symptoms of the release of MC mediators, but the patient did not fulfill all the diagnostic criteria of MCAS (3). Additionally, a clonal mast cell disorder was discarded in the index case by performing a BM biopsy, and KIT mutations studied were negative. Some cases of familial mastocytosis have been described (16–19). Molderings et al. (20) described a familial occurrence of systemic MC activation disease reporting that mutated disease-related operator and/or regulator genes could be responsible for the development of somatic mutations in KIT and other proteins involved in the regulation of mast cell activity. Recently, the entity known as hereditary alpha-hypertryptasemia has emerged. Lyons et al. (21) identified nine atopic subjects with persistent increases in BST in the absence of evidence for a clonal MCD. They found an autosomal dominant inheritance pattern of increased BST, which is in agreement with our family. Although they observed an increase in MC numbers on BM, none of the five index patients that underwent BM biopsy met the World Health Organization established criteria for the diagnosis of systemic mastocytosis (22) or the ones proposed for monoclonal MCA (3). Nevertheless, all of the patients were symptomatic. In addition, these authors also found that elevated BST identified a multisystem disorder associated with increased TPSAB1 copy number (8). Finally, Sabato et al. (23) reported a family with elevated BST and MCAS. They found elevated BST in seven relatives of three consecutive generations, suggesting a monogenic form of hypertryptasemia with autosomal dominant inheritance. Two patients were completely asymptomatic and a third one only had apathy and migraine with a normal BM biopsy. These three patients are similar to the two daughters (II.1, II.2) and the sister (I.3) of our index case.
We consider that this family with high BST in the absence of clinical symptoms and without clonal MCs has an asymptomatic familial hypertryptasemia or HαT. We detected an increase in the mRNA expression of tryptase genes in the family members compared to controls. The index case also presented the highest BST levels which correlated with a highly increased tryptase mRNA expression. In addition, we detected an increase of TPSAB1 gene dose in patients which correlated with high BST levels in those patients. This agrees with Sabato et al. (24) that recently reported a TPSAB1 quintuplication in a highly symptomatic patient with clonal MC disease, remarking that individuals carrying three or more copies of α-tryptase had higher BST and more symptoms than those carrying two copies.
We performed CNV analysis revealing a hereditary copy number gain phenotype (3β2α) present in the index case (I.2), her sister (I.3), and her daughters (II.1 and II.2). Although the mRNA of patients II.1 and II.2 was not available, a good correlation between gene expression and BST levels was shown in the rest of the samples. Finally, other factors capable of modulating gene expression can be involved, such as epigenetic factors (25).
In conclusion, we present a family with HαT, elevated BST, and mRNA gene expression in the absence of MC clonality. Unlike what has been reported to date, nearly all of them have remained asymptomatic during a long follow-up period. Typically, BSTs have been associated with having an MCD. However, HαT associates with increased copy numbers of the TPSAB1 gene, which leads to high BSTs (4) and may not be associated with the presence of usual MC-mediator release symptoms or may even be asymptomatic. Since an estimated 4–6% of the population has high levels of BST (26, 27), HαT should be taken into account in the differential diagnosis of patients with symptoms of mastocyte activation and increased BST levels, not only to achieve a correct diagnosis and treatment but also to advise on prognosis and recommendations.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the local Ethics Committee of the University Hospital of Salamanca (PI120913) and an informed consent was signed in all cases. The patients/participants provided their written informed consent to participate in this study.
LH-H, CS, ID, and MI-G conceived and planned the experiments. LH-H, EM-V, and AG-S carried out the experiments. EM, FL, and ID collect the samples. LH-H, CS, EM-V, AG-S, DG-O, ID, and MI-G contributed to the interpretation of the results. All authors provided critical feedback and helped shape the research, analysis, and manuscript. All authors agree to be accountable for the content of the work.
This research received funding from the Spanish Foundation of the Spanish Association of Allergy and Clinical Immunology (Sociedad Española de Alergologia e Inmunologia Clínica), the Council of Castilla y León, Education Counseling in the context of Regional Strategy of Scientist Research, Technological Development and Innovation 2007–2013, co-financing from the European Social Fund, the Immunoallergic Association of Salamanca, and the Asthma, Allergic, and Adverse Reactions networks for Cooperative Research in Health (ARADyAL) in association with the Instituto de Salud Carlos III (RD16/0006/0019), co-funding from the European Regional Development Fund (ERDF).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
BST, basal serum tryptase; HAT or HαT, hereditary α-tryptasemia; BM, bone marrow; MC, mast cell; MCD, mast cell disorder; MCAS, mast cell activation syndrome.
1. Theoharides TC, Valent P, Akin C. Mast cells, mastocytosis, and related disorders. N Engl J Med. (2015) 373:163–72. doi: 10.1056/NEJMra1409760
2. Vega-Castro A, Alonso-Llamazares A, Cárdenas R, Beitia JM, Mateo B, Alvarez-Twose I, et al. An increase in tryptase on the first day of hymenoptera venom immunotherapy might be a predictor of future systemic reactions during treatment. J Investig Allergol Clin Immunol. (2018) 28:305–11. doi: 10.18176/jiaci.0258
3. Valent P, Akin C, Bonadonna P, Hartmann K, Brockow K, Niedoszytko M, et al. Proposed diagnostic algorithm for patients with suspected mast cell activation syndrome. J Allergy Clin Immunol Pract. (2019) 7:1125–33.e1. doi: 10.1016/j.jaip.2019.01.006
4. Weiler CR, Austen KF, Akin C, Barkoff MS, Bernstein JA, Bonadonna P, et al. AAAAI Mast Cell Disorders Committee Work Group Report: Mast cell activation syndrome (MCAS) diagnosis and management. J Allergy Clin Immunol. (2019) 144:883–96. doi: 10.1016/j.jaci.2019.08.023
5. Sommerhoff CP, Schaschke N. Mast cell tryptase beta as a target in allergic inflammation: an evolving story. Curr Pharm Des. (2007) 13:313–32. doi: 10.2174/138161207779313579
6. Fukuoka Y, Schwartz LB. Active monomers of human beta-tryptase have expanded substrate specificities. Int Immunopharmacol. (2007) 7:1900–8. doi: 10.1016/j.intimp.2007.07.007
7. Caughey GH. New developments in the genetics and activation of mast cell proteases. Mol Immunol. (2002) 38:1353–7. doi: 10.1016/S0161-5890(02)00087-1
8. Lyons JJ, Yu X, Hughes JD, Le QT, Jamil A, Bai Y, et al. Elevated basal serum tryptase identifies a multisystem disorder associated with increased TPSAB1 copy number. Nat Genet. (2016) 48:1564–9. doi: 10.1038/ng.3696
9. Valent P, Akin C, Escribano L, Födinger M, Hartmann K, Brockow K, et al. Standards and standardization in mastocytosis: consensus statements on diagnostics, treatment recommendations and response criteria. Eur J Clin Invest. (2007) 37:435–53. doi: 10.1111/j.1365-2362.2007.01807.x
10. Sperr WR, Escribano L, Jordan JH, Schernthaner GH, Kundi M, Horny HP, et al. Morphologic properties of neoplastic mast cells: delineation of stages of maturation and implication for cytological grading of mastocytosis. Leuk Res. (2001) 25:529–36. doi: 10.1016/S0145-2126(01)00041-8
11. Escribano L, Diaz-Agustin B, López A, Núñez López R, García-Montero A, Almeida J, et al. Immunophenotypic analysis of mast cells in mastocytosis: when and how to do it. Proposals of the Spanish Network on Mastocytosis (REMA). Cytometry B Clin Cytom. (2004) 58:1–8. doi: 10.1002/cyto.b.10072
12. Escribano L, Orfao A, Díaz-Agustin B, Villarrubia J, Cerveró C, López A, et al. Indolent systemic mast cell disease in adults: immunophenotypic characterization of bone marrow mast cells and its diagnostic implications. Blood. (1998) 91:2731–6. doi: 10.1182/blood.V91.8.2731.2731_2731_2736
13. Garcia-Montero AC, Jara-Acevedo M, Teodosio C, Sanchez ML, Nunez R, Prados A, et al. KIT mutation in mast cells and other bone marrow hematopoietic cell lineages in systemic mast cell disorders: a prospective study of the Spanish Network on Mastocytosis (REMA) in a series of 113 patients. Blood. (2006) 108:2366–72. doi: 10.1182/blood-2006-04-015545
14. Taylor S, Wakem M, Dijkman G, Alsarraj M, Nguyen M. A practical approach to RT-qPCR-Publishing data that conform to the MIQE guidelines. Methods. (2010) 50:S1–S5. doi: 10.1016/j.ymeth.2010.01.005
15. Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods. (2001) 25:402–8. doi: 10.1006/meth.2001.1262
16. Broesby-Olsen S, Kristensen TK, Møller MB, Bindslev-Jensen C, Vestergaard H; Mastocytosis Centre, Odense University Hospital (MastOUH). Adult-onset systemic mastocytosis in monozygotic twins with KIT D816V and JAK2 V617F mutations. J Allergy Clin Immunol. (2012) 130:806–8. doi: 10.1016/j.jaci.2012.04.013
17. Wöhrl S, Moritz KB, Bracher A, Fischer G, Stingl G, Loewe R. A c-kit mutation in exon 18 in familial mastocytosis. J Invest Dermatol. (2013) 133:839–41. doi: 10.1038/jid.2012.394
18. Zanotti R, Simioni L, Garcia-Montero AC, Perbellini O, Bonadonna P, Caruso B, et al. Somatic D816V KIT mutation in a case of adult-onset familial mastocytosis. J Allergy Clin Immunol. (2013) 131:605–7. doi: 10.1016/j.jaci.2012.11.040
19. Zhang LY, Smith ML, Schultheis B, Fitzgibbon J, Lister TA, Melo JV, et al. A novel K509I mutation of KIT identified in familial mastocytosis-in vitro and in vivo responsiveness to imatinib therapy. Leuk Res. (2006) 30:373–8. doi: 10.1016/j.leukres.2005.08.015
20. Molderings GJ, Haenisch B, Bogdanow M, Fimmers R, Nöthen MM. Familial occurrence of systemic mast cell activation disease. PLoS One. (2013) 8:e76241. doi: 10.1371/journal.pone.0076241
21. Lyons JJ, Sun G, Stone KD, Nelson C, Wisch L, O'Brien M, et al. Mendelian inheritance of elevated serum tryptase associated with atopy and connective tissue abnormalities. J Allergy Clin Immunol. (2014) 133:1471–4. doi: 10.1016/j.jaci.2013.11.039
22. Valent P, Akin C, Hartmann K, Nilsson G, Reiter A, Hermine O, et al. Advances in the classification and treatment of mastocytosis: current status and outlook toward the future. Cancer Res. (2017) 77:1261–70. doi: 10.1158/0008-5472.CAN-16-2234
23. Sabato V, Van De Vijver E, Hagendorens M, Vrelust I, Reyniers E, Fransen E, et al. Familial hypertryptasemia with associated mast cell activation syndrome. J Allergy Clin Immunol. (2014) 134:1448–50.e3. doi: 10.1016/j.jaci.2014.06.007
24. Sabato V, Chovanec J, Faber M, Milner JD, Ebo D, Lyons JJ. First identification of an inherited TPSAB1 quintuplication in a patient with clonal mast cell disease. J Clin Immunol. (2018) 38:457–9. doi: 10.1007/s10875-018-0506-y
25. Molderings GJ. Transgenerational transmission of systemic mast cell activation disease-genetic and epigenetic features. Transl Res. (2016) 174:86–97. doi: 10.1016/j.trsl.2016.01.001
26. Fellinger C, Hemmer W, Wöhrl S, Sesztak-Greinecker G, Jarisch R, Wantke F. Clinical characteristics and risk profile of patients with elevated baseline serum tryptase. Allergol Immunopathol (Madr). (2014) 42:544–52. doi: 10.1016/j.aller.2014.05.002
Keywords: tryptase, β-tryptase, hereditary α-tryptasemia, mast cells, basal serum tryptase
Citation: Hernández-Hernández L, Sanz C, Marcos-Vadillo E, García-Sánchez A, Moreno E, Lorente F, González-de-Olano D, Dávila I and Isidoro-García M (2021) Increased TPSAB1 Copy Number in a Family With Elevated Basal Serum Levels of Tryptase. Front. Med. 8:577081. doi: 10.3389/fmed.2021.577081
Received: 28 June 2020; Accepted: 19 March 2021;
Published: 13 April 2021.
Edited by:
Evi X. Stavrou, Case Western Reserve University, United StatesReviewed by:
Long-Sheng Lu, Taipei Medical University, TaiwanCopyright © 2021 Hernández-Hernández, Sanz, Marcos-Vadillo, García-Sánchez, Moreno, Lorente, González-de-Olano, Dávila and Isidoro-García. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ignacio Dávila, aWRnQHVzYWwuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.