 Kata Szemes1
Kata Szemes1 Alexandra Soós2,3
Alexandra Soós2,3 Péter Hegyi1,2,4,5*
Péter Hegyi1,2,4,5* Nelli Farkas2,6
Nelli Farkas2,6 Adrienn Erős2
Adrienn Erős2 Bálint Erőss2
Bálint Erőss2 Emese Mezősi1
Emese Mezősi1 Zsolt Szakács2,4
Zsolt Szakács2,4 Katalin Márta2,4
Katalin Márta2,4 Patrícia Sarlós1,4*
Patrícia Sarlós1,4*- 1First Department of Medicine, Medical School, University of Pécs, Pécs, Hungary
- 2Institute for Translational Medicine, Medical School, University of Pécs, Pécs, Hungary
- 3Doctoral School of Clinical Medicine, University of Szeged, Szeged, Hungary
- 4János Szentágothai Research Centre, University of Pécs, Pécs, Hungary
- 5Momentum Gastroenterology Multidisciplinary Research Group, Hungarian Academy of Sciences, University of Szeged, Szeged, Hungary
- 6Institute of Bioanalysis, Medical School, University of Pécs, Pécs, Hungary
Background: In steroid-refractory acute severe ulcerative colitis (ASUC), cyclosporine (CYS) or infliximab (IFX) may be considered as a second-line alternative to avoid colectomy. There are short-term data reported, but until now, there is no meta-analysis regarding long-term outcomes of CYS and IFX in patients with ASUC.
Aim: To compare long-term efficacy and safety of CYS and IFX in a meta-analysis.
Methods: Three electronic databases (PubMed, Embase, Cochrane Central Register of Controlled Trials) were searched for studies which compared CYS vs. IFX in adults with ASUC. Long-term colectomy-free rate from 1 to 10 years during CYS or IFX therapy was collected, last updated up to 22nd May 2019. Primary outcome was long-term colectomy-free rate, secondary outcomes were adverse events (AE), serious adverse events (SAE), and mortality. Long-term colectomy-free survival and safety measures were pooled with the random-effect model. Odds ratios (OR) with 95% confidence intervals (CI) were calculated.
Results: Data from 1,607 patients in 15 trials were extracted. In the first 3 years, pooled OR for colectomy-free survival was higher with IFX than with CYS (OR = 1.59, 95% CI: 1.11–2.29, p = 0.012; OR = 1.57, 95% CI: 1.14–2.18, p = 0.006; and OR = 1.75, 95% CI: 1.08–2.84, p = 0.024; at 1, 2, and 3 years, respectively). However, the significant difference remained undetected from the fourth year of follow-up and in subgroup of RCTs (OR = 1.35, 95% CI: 0.90–2.01, p = 0.143; OR = 1.41, 95% CI: 0.94–2.12, p = 0.096; and OR = 1.34, 95% CI: 0.89–2.00, p = 0.157; at 1, 2, and 3 years, respectively). No significant difference was detected regarding adverse events, serious adverse events and mortality between the groups. The neutral associations proved to be underpowered with trial sequential analysis.
Conclusion: However observational studies show IFX as a better choice, according to the RCTs, choosing either CYS or IFX as rescue therapy for ASUC, the long-term outcomes are not different, although further large RCTs are warranted.
Introduction
Ulcerative colitis (UC) is a lifelong inflammatory bowel disease that causes a continuous mucosal inflammation of the colon and occurs periodically in patients' life. Acute severe ulcerative colitis (ASUC) is a life-threatening condition which requires hospitalization and occurs in about 25% of patients with UC (1). ASUC is defined as patients with bloody diarrhea ≥6/day and any signs of systemic toxicity [pulse > 90/min, temperature > 37.8°C, hemoglobin < 105 g/l, erythrocyte sedimentation rate (ESR) > 30 mm/h, or C-reactive protein (CRP) > 30 mg/l] (2). In the case of ASUC, intravenous (IV) corticosteroids are the mainstay of first-line treatment, but up to 40% of the cases are resistant to this therapeutic modality (3). In steroid-refractory cases, second-line therapy is advised to be introduced to avoid colectomy. Cyclosporine (CYS) and infliximab (IFX) are widely used as rescue therapies.
Rationale
CYS is a calcineurin and cytochrome P450 inhibitor immunosuppressant blocking the transcription of cytokine genes (interleukin-2 and−4) in activated T cells, thereby reducing the inflammation in the intestine (4). In the 1990s, CYS was the first drug introduced as salvage therapy in steroid-refractory ASUC (5). In general, following 2 mg/kg/day IV CYS, 5 mg/kg oral CYS is recommended for up to 3 months as a bridge to an immunosuppressive agent [azathioprine (AZA) or 6-mercaptopurine (6-MP)] (6). Despite the fast response within 4–7 days and the reliable short-term effectiveness during CYS therapy, significant side effects may occur (7, 8). A close drug-level monitoring of CYS is required to avoid opportunistic infections, renal, vascular and neurological toxicity (9).
In the past 15 years, IFX, a chimeric IgG1 monoclonal antibody designed to bind tumor necrosis factor-alpha (TNFα) has become an alternative second-line therapeutic option in steroid-refractory ASUC (10). Regularly, a standard induction regimen of 5 mg/kg IFX is used, although recently accelerated dose intensification with 10 mg/kg IFX is often applied as well to counteract the increased intestinal clearance of IFX in ASUC (11). However, there is no data to support the benefit of 10 mg/kg. During IFX-linked immunosuppression, opportunistic infections, reactivation on latent tuberculosis or hepatitis may occur; therefore, careful screening is recommended before the initiation of IFX.
Objectives and Research Question
In the treatment of steroid-refractory ASUC, two randomized controlled trials (RCTs) demonstrated equal short-term efficacy and safety of IFX and CYS (CYSIF, CONSTRUCT) (12, 13). These results were opposed by a previous meta-analysis of observational studies, where IFX was associated with significantly higher rates of treatment response and a lower 12 months colectomy-rate compared to that with CYS (14). A lately reported network meta-analysis with benefit-risk analysis also suggested that there is a rank order of efficacy for colectomy-free rates favoring IFX over CYS, although the difference between the treatments was small (15).
Since new studies have been released and long-term survival data have become available. Therefore, we aimed to summarize the currently available evidence on the long-term efficacy and safety of IFX and CYS in steroid-refractory ASUC.
Methods
Study Design, Participants, Interventions, and Comparators
This meta-analysis was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement (Supplementary Table 1) (16). The protocol for this study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) a priori under number CRD42018115035.
Search Strategy
We searched MEDLINE via PubMed (http://www.ncbi.nlm.nih.gov/pubmed), Embase (https://www.embase.com) and Cochrane Central Register of Controlled Trials (CENTRAL) (http://www.cochranelibrary.com) databases from inception up to 22nd May 2019.
Our search followed the PICO concept. Studies discussed a population (P) of patients with steroid-refractory ASUC who received IFX (I) or CYS (C) as salvage therapy. The primary outcome (O) was long-term colectomy-free survival rate, defined as the follow-up period exceeding 12 months after therapy initiation. Secondary outcomes were adverse events (AE), serious adverse events (SAE) and mortality. AE and SAE were categorized in accordance with the definitions of the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human use—Good Clinical Practice (ICH-GCP) consensus guidelines (17).
The following query combining Medical Subject Headings (MeSH) and free text terms were used'. (“colitis, ulcerative”[MeSH Terms] OR (“colitis”[All Fields] AND “ulcerative”[All Fields]) OR “ulcerative colitis”[All Fields] OR (“ulcerative”[All Fields] AND “colitis”[All Fields])) AND (“infliximab”[MeSH Terms] OR “infliximab”[All Fields]) AND (“cyclosporine”[MeSH Terms] OR “cyclosporine”[All Fields] OR “cyclosporin”[All Fields]) AND (“colectomy”[MeSH Terms] OR “colectomy”[All Fields]). We imposed only “English-language” and “human” filters on the search.
Study Selection
After the database search, one author (KS) removed the overlapping records using a reference management software (EndNote X8, Clarivate Analytics, Philadelphia, PA, USA). Two investigators (KS and PS) independently screened titles, abstracts, and full-texts against the predefined eligibility criteria. Consensus involving a third party (PH) resolved discrepancies in each phase of selection.
We included any controlled studies (observational or experimental) that met the following criteria: (a) adult ASUC patients (aged ≥18 years) being refractory to IV or oral steroid treatment; (b) CYS and IFX was used as salvage therapy after 3–7 days of steroid treatment; (c) colectomy-free survival rate was assessed at 12 months or later; and (d) cytomegalovirus infection was not verified in the patients. There was no restriction for additional drugs used in UC treatment (e.g., AZA, 6-MP or methotrexate).
Data Extraction, Quality Assessment
The following data were extracted from each study (Table 1): first author, year of publication, study type (prospective/retrospective; randomized/non-randomized), drug regimen, the number of patients, age, gender distribution, rate of extensive colitis, concomitant, and maintenance therapy, follow-up period and the definition of ASUC. Intention-to-treat data were extracted from RCTs. If numerical data on long-term colectomy-free survival were not reported (13, 23, 26, 31), we extracted data from the Kaplan-Meier curves by identifying the values on the axes “x” and “y” with a software [GetData Graph Digitizer] according to the method proposed by Guyot et al. (32). Data collection was accomplished by two authors independently (KS and PS). Discrepancies were resolved by consensus. In the case of any disagreement, a third author was involved to resolve conflicts (PH).
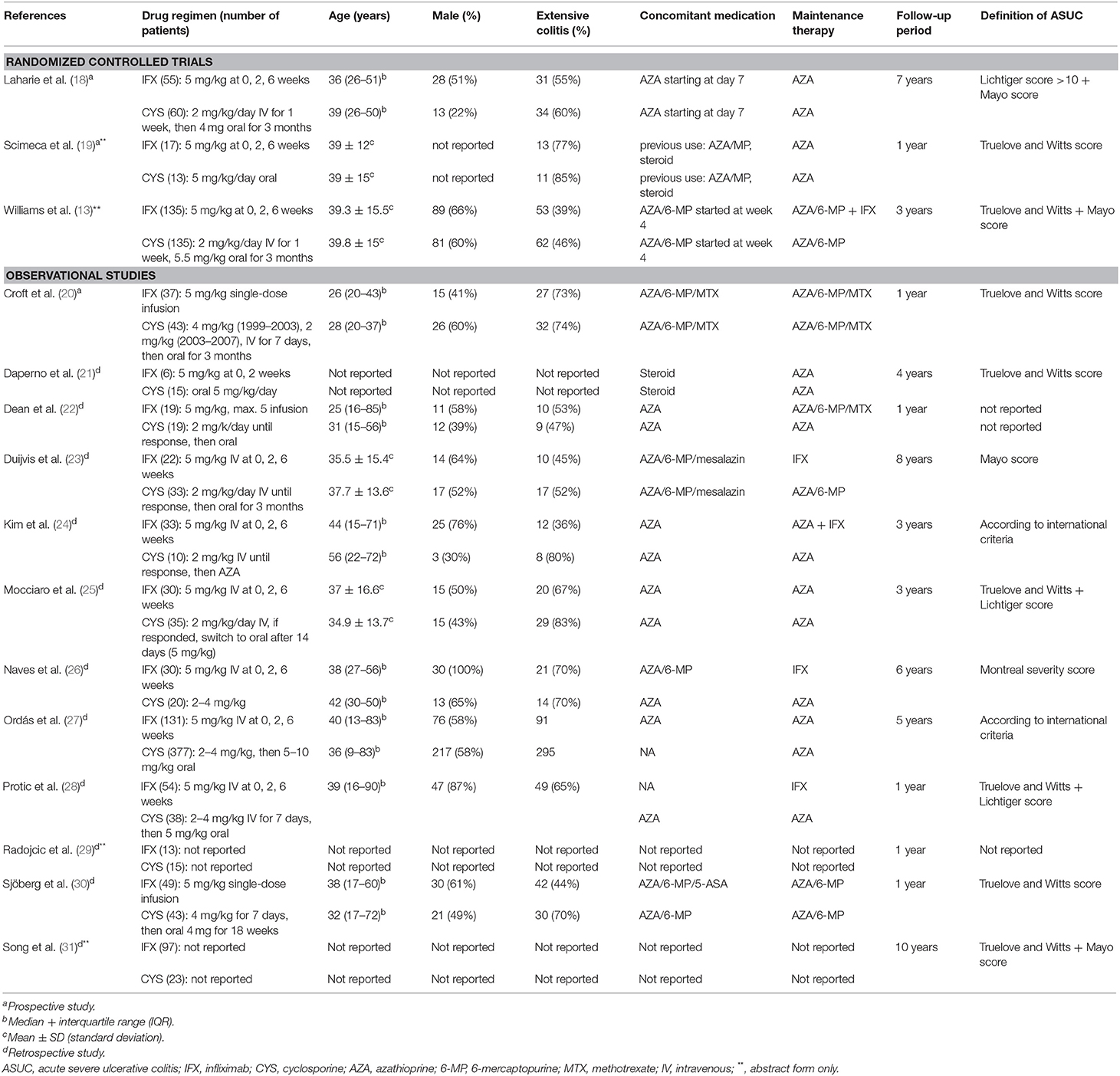
Table 1. Study characteristics.
We assessed the risk of bias of observational studies using the Newcastle-Ottawa scale (NOS) (Table 2) (33). There is a reliable “star system” that has three broad perspectives to secure a simple tool for quality assessment: selection and comparability of the groups, and the ascertainment of the outcome. The quality of the included RCTs was assessed with the Cochrane Risk of Bias Tool along seven domains (34). After the assessment, low, high and unclear risks of bias were indicated with green, red and yellow symbols.
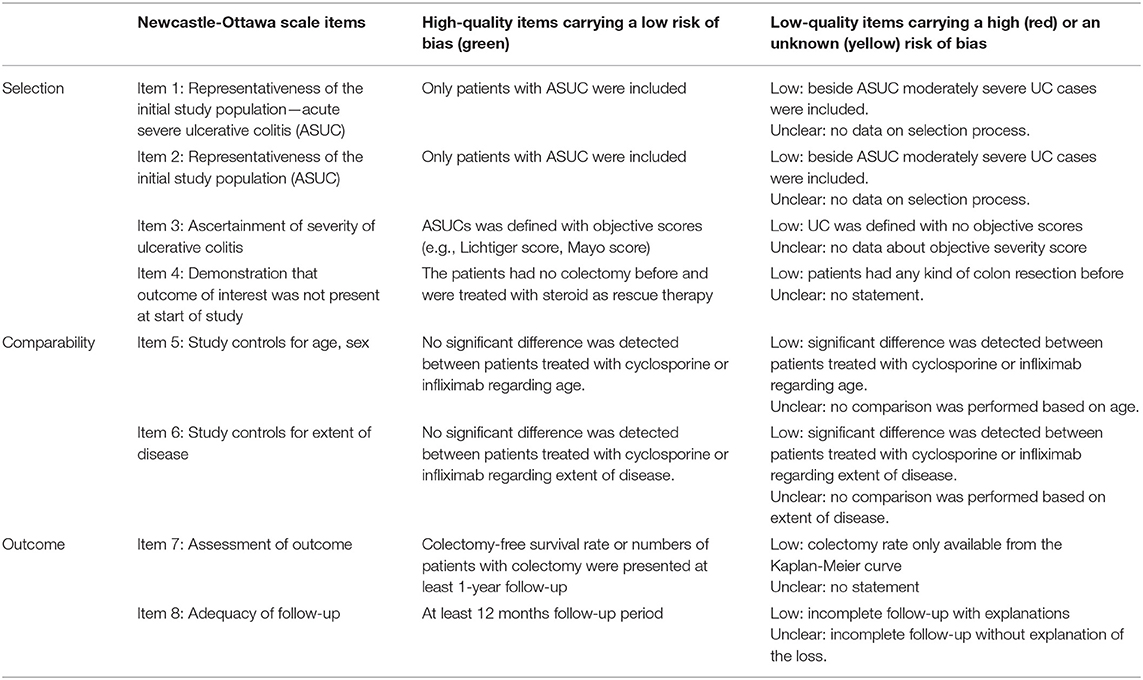
Table 2. Modified Newcastle-Ottawa Scale.
Data Analysis
Data on colectomy-free survival were extracted with IFX and CYS. Odds ratios (ORs) were calculated with 95% confidence intervals using the random effects model with the DerSimonian–Laird estimation (35). Results of the meta-analysis were displayed graphically using Forest plots. All analyses were two-tailed and p < 0.05 was considered as significant.
Subgroup analyses were performed to examine different effects in a 10 years interval. We carried out subgroup analyses only for the first 4 years based on the study design because data from RCTs were lacking for longer follow-up. Heterogeneity was tested by using the Cochrane's Q and the I2 statistics, where I2 = 100% × (Q – df)/Q and represents the magnitude of the heterogeneity (moderate: 30–60%, substantial: 50–90%, considerable: 75–100%) (34). All meta-analytical calculations were performed with Stata 15.1 data analysis and statistical software (Stata Corp LLC, College Station, TX, USA).
Trial Sequential Analysis
Trial sequential analysis (TSA) was performed to assess the risk of type-I error and to estimate the required information size for an adequate statistical power if only RCTs were included (36). TSA was interpreted with an overall five percent of risk of type-I error (α = 0.05) and with a power of 80% (Figures 1–3). Crossing of the constructed cumulative Z-curves (blue) and the two-sided Z = 1.96 provides a traditionally significant result. To obtain reliable evidence, crossing of the trial sequential monitoring boundaries (red) is needed. We conducted TSA using Trial Sequential Analysis software 0.9 (Copenhagen Trials Unit, Denmark).
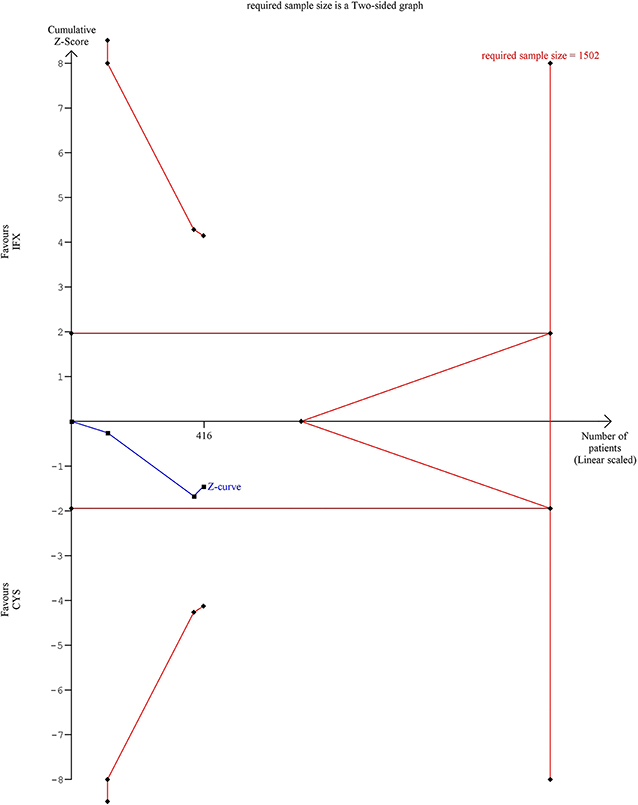
Figure 1. Results of the trial sequential analysis of the risks of 1 year colectomy-free rate. The required sample size of 1,502 patients was estimated using α = 0.05 (two-sided) and ß = 0.02 (power of 80%). Crossing of the constructed cumulative Z-curves (blue) and the two-sided Z = 1.96 provides a traditionally significant result. To obtain reliable evidence, crossing of the trial sequential monitoring boundaries (red) is needed. In the case of 1 year colectomy-free rate outcome, the cumulative Z-curve (blue) did not crossed the conventional boundary and neither the trial sequential monitoring boundary nor the required sample size line was surpassed.
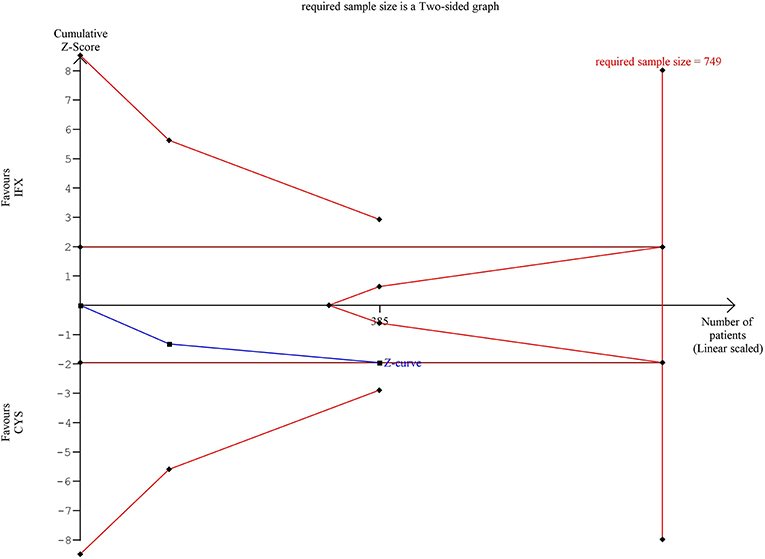
Figure 2. Results of the trial sequential analysis of the risks of adverse events. The required sample size was calculated with α = 0.05 (two-sided) and ß = 0.02 (power of 80%). Although cumulative Z-curve (blue) reached the conventional boundary, it did not cross through. Number of participants (385) did not reach the information size (749) and the cumulative Z-curve does not cross the monitoring boundary either.
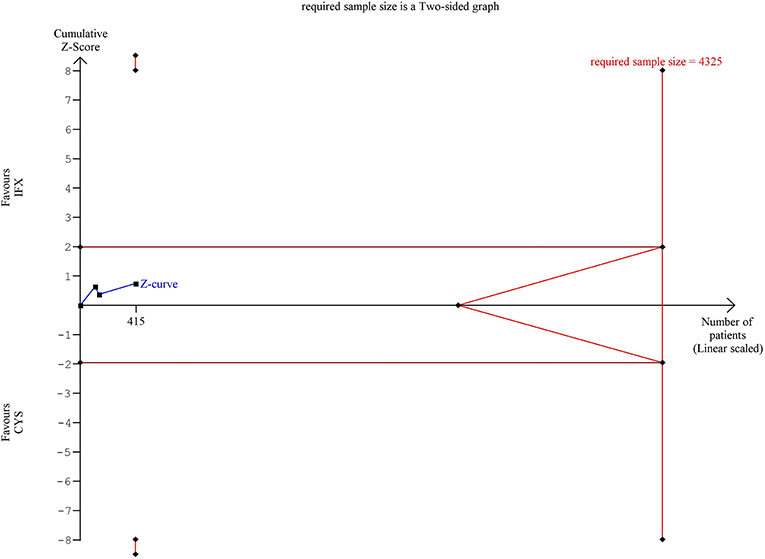
Figure 3. Results of the trial sequential analysis of the risks of serious adverse events. The required sample size was calculated using α = 0.05 (two-sided) and ß = 0.02 (power of 80%). The cumulative Z-curve (blue) did not cross the monitoring boundary (red) and not reached the required information size (4,325 patients). There is insufficient information about the evidence of significance.
Quality of Evidence
The GRADE system was constructed for the assessment of the quality of the evidence for the main outcomes in a review (37). The rating extends from very low to high quality, wherein RCTs starting from a high, non-randomized studies starting from a low quality of evidence. After the assessment of study design, outcomes were tested against five criteria including risk of bias, inconsistency, indirectness, imprecision and publication bias. Finally, the overall quality of the evidence for each outcome was graded as high, moderate, low or very low. Grading was performed independently by two of the authors (KS and PS) and disagreements were discussed by involving a third party (AE).
Results
Search Results
A total of 731 records were identified from the databases with our systematic search strategy (121 records in PubMed, 597 ones in EMBASE and 13 ones in CENTRAL) (as shown in the PRISMA flow diagram; Figure 4). Two additional articles were found from the reference lists of the included studies (19, 38). After the removal of duplicates, 594 records remained, 565 of which were excluded by titles and abstracts. The remaining 29 articles were assessed for eligibility by full-text and further 10 studies were excluded due to the following reasons: three studies reported only short-term follow-up data (39–41), one study did not report on the timing and rate of colectomy (38) and two studies were uncontrolled (42, 43). In two studies, the number of patients treated with CYS and IFX was not reported (44, 45), one study included patients pre-treated with either CYS or IFX (46) and one study evaluated patients with Crohn's colitis (47). Nineteen studies remained, but four additional studies were excluded from the quantitative synthesis because they investigated overlapping study population (12, 48–50). Thus, 15 studies fulfilled all inclusion criteria and were included in the meta-analysis.
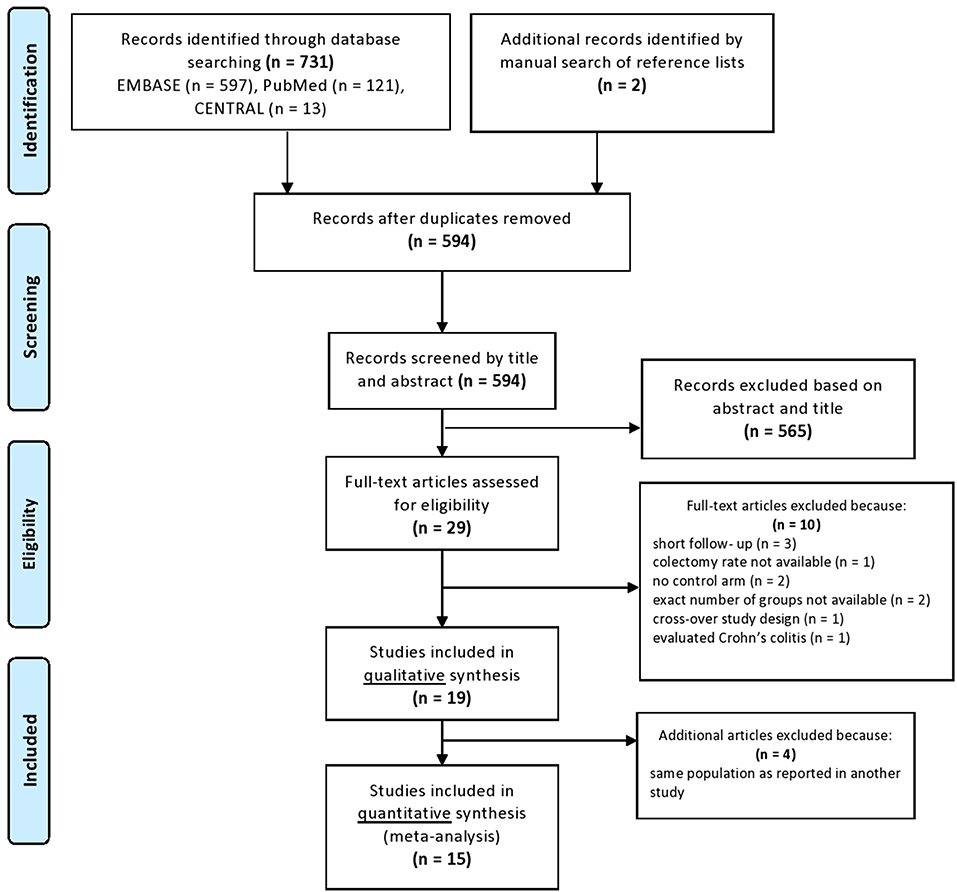
Figure 4. PRISMA flowchart.
Characteristics of the Studies Included
The main characteristics of the included studies are listed in Table 1. The studies were published between 2004 and 2018 and the follow-up period ranged at least from 1 year to maximum of 10 years. In the quantitative analysis, we used data from three RCTs (13, 18, 19) and 12 cohort studies (20–31). A total number of 1,607 patients with steroid-refractory ASUC were included, 879 of which (54.7%) were treated with CYS and the other 728 (45.3%) with IFX. The most common definitions of ASUC used in the studies were the Truelove and Witts criteria, the Mayo and the Lichtiger scores (7, 51, 52). Three of the 15 articles were published only in conference abstract form (19, 29, 31).
In most of the studies, the standard 2 mg/kg/day IV CYS regimen was applied, oral CYS was used for induction of remission only in two studies (19, 21). After the oral CYS bridging, AZA maintenance therapy was continued in all studies. Standard 5 mg/kg dose of IFX was administered in multiple IV infusions (at 0, 2, and 6 weeks) following the induction protocol. Only two studies reported a single infusion of IFX (20, 30). In the IFX treatment groups, AZA was the most commonly administered maintenance drug, albeit recent studies continued IFX (13, 23, 24, 26, 28). Due to the lack of available safety data during long-term follow-up in an RCT, the CYSIF trial (18), AE and SAE results reported in the original study were used in the meta-analysis (12).
Long-Term Colectomy-Free Survival
Fifteen, eight, five, and one studies reported 1, 3, 5, and 10 years colectomy-free survival rate. In the first 3 years, colectomy-free survival rate was higher with IFX compared to that with CYS (OR = 1.59, 95% CI: 1.11 −2.29, p = 0.012 for 1 year; OR = 1.57, 95% CI: 1.14–2.18, p = 0.006 for 2 years; and OR = 1.75, 95% CI: 1.08–2.84, p = 0.024 for 3 years), with moderate heterogeneity across the studies (I2 = 44.3%, p = 0.033; I2 = 0.0%, p = 0.74, and I2 = 42.6%, p = 0.093, respectively) (Figure 5). From the fourth year of follow-up, no significant difference regarding the colectomy-free rates was found between the two treatment groups (Figure 6). At 9 and 10 years of follow-up, only one small, retrospective study remained in the analysis, where the colectomy-free survival was higher with IFX compared to that with CYS (31).
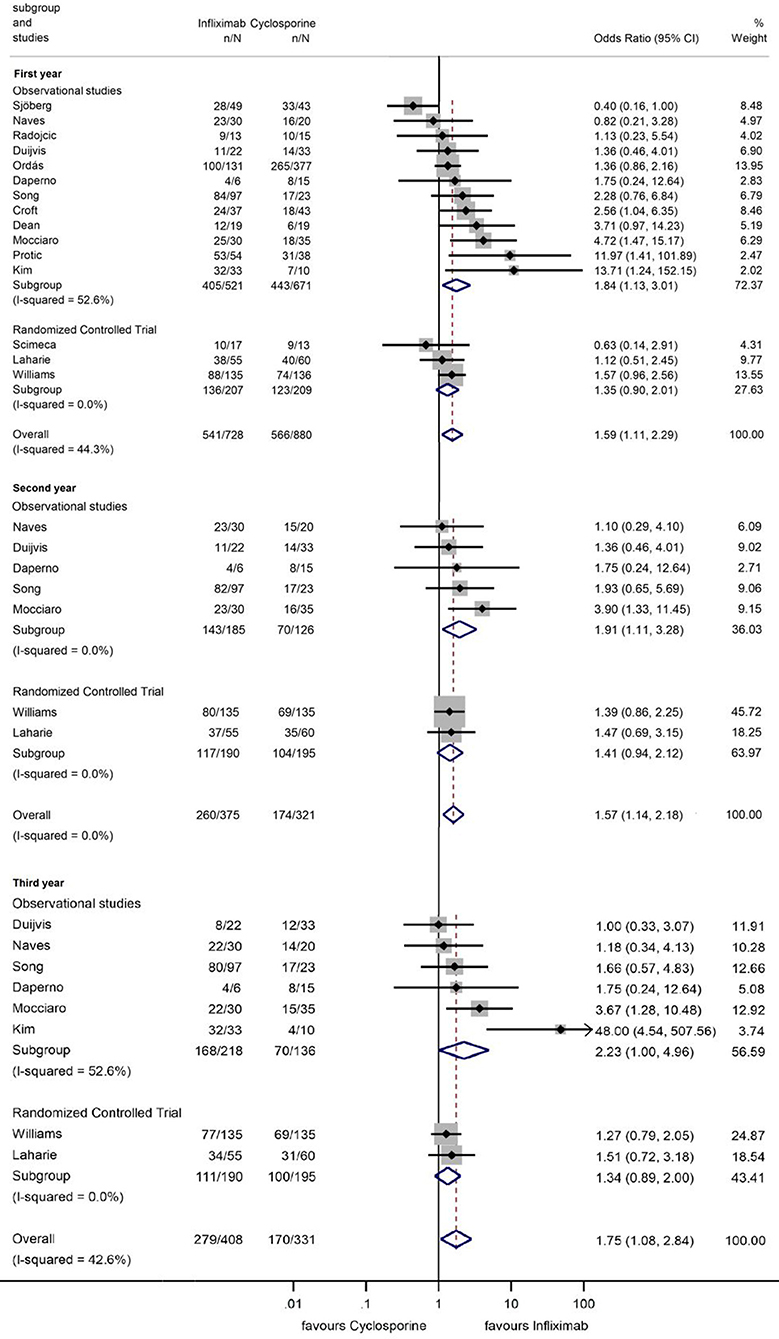
Figure 5. Odds ratios of colectomy-free survival with infliximab (vs. cyclosporine) in the first, second, and third year in steroid-refractory acute severe ulcerative colitis.
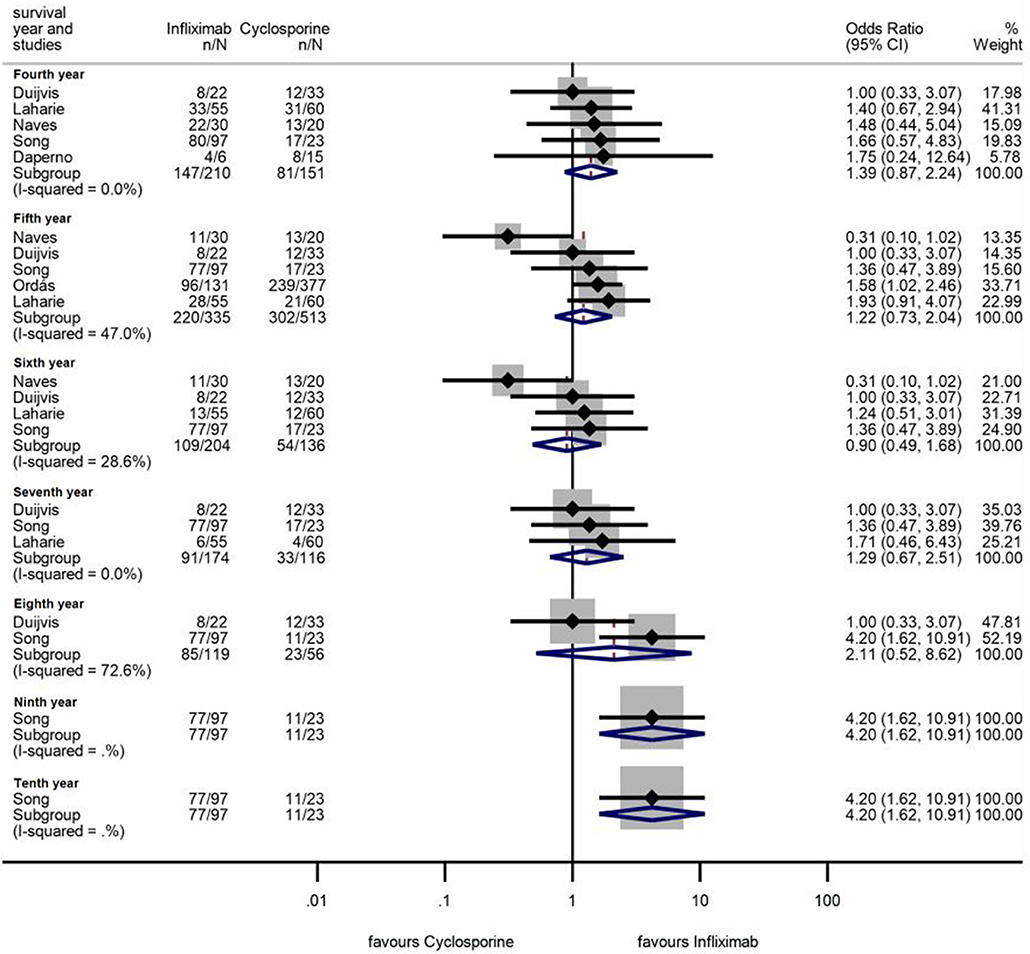
Figure 6. Odds ratios of colectomy-free survival with infliximab (vs. cyclosporine) between the fourth and tenth year in steroid-refractory acute severe ulcerative colitis.
However, separating the data of RCTs revealed that the significant association can only be seen if observational studies are included (ORs for observational studies = 1.84, 95% CI: 1.13–3.01, p = 0.015 in the first year; OR = 1.91, 95% CI: 1.11–3.28, p = 0.020 in the second year; and OR = 2.23, 95% CI: 1.00–4.96, p = 0.049 in the third year; ORs for RCTs = 1.35, 95% CI: 0.90–2.01, p = 0.143 in the first year; OR = 1.41, 95% CI: 0.94–2.12, p = 0.096 in the second year; and OR = 1.34, 95% CI: 0.89–2.00, p = 0.157 in the third year) (Figure 5). The heterogeneity remained substantial in the analysis from observational studies but was negligible if RCTs were included exclusively (in the first year I2 = 52.6%, p = 0.016 and I2 = 0.0%, p = 0.466, respectively). TSA indicated that the analysis on colectomy-free survival at 1 year was underpowered, since the monitoring boundaries were not crossed, and the required information size was not reached (Figure 1). According to TSA, at least 1,502 patients would be required for drawing final conclusion while only 416 patients were included in the current analysis.
Based on our strict and consistent grading, the quality of the evidence for colectomy-free survival rates at 1, 3, 5, and 10 years proved to be low for the subgroups of RCTs and very low if non-randomized studies were included as well (Table 3).
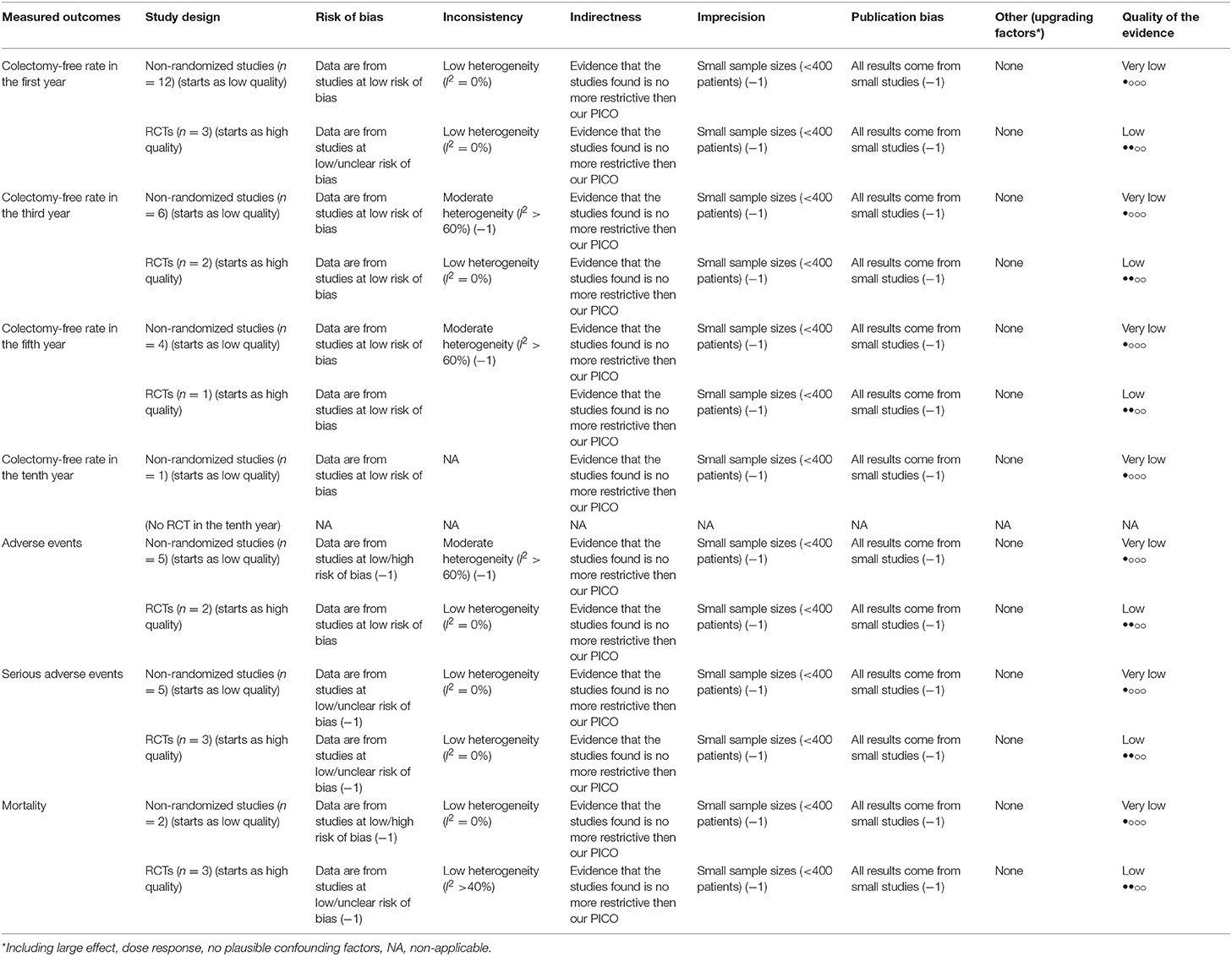
Table 3. Investigation of quality of the evidence for all included outcomes (GRADE).
Safety
Seven studies assessed AE (Figure 7) (12, 13, 20, 22, 25, 28, 30). Sixty-seven (18.1%) AEs were reported with CYS and 72 (18.9%) with IFX. The pooled OR of AEs was 0.93 (95% CI: 0.45–1.92, p = 0.847), demonstrating no significant difference between groups (Figure 7).
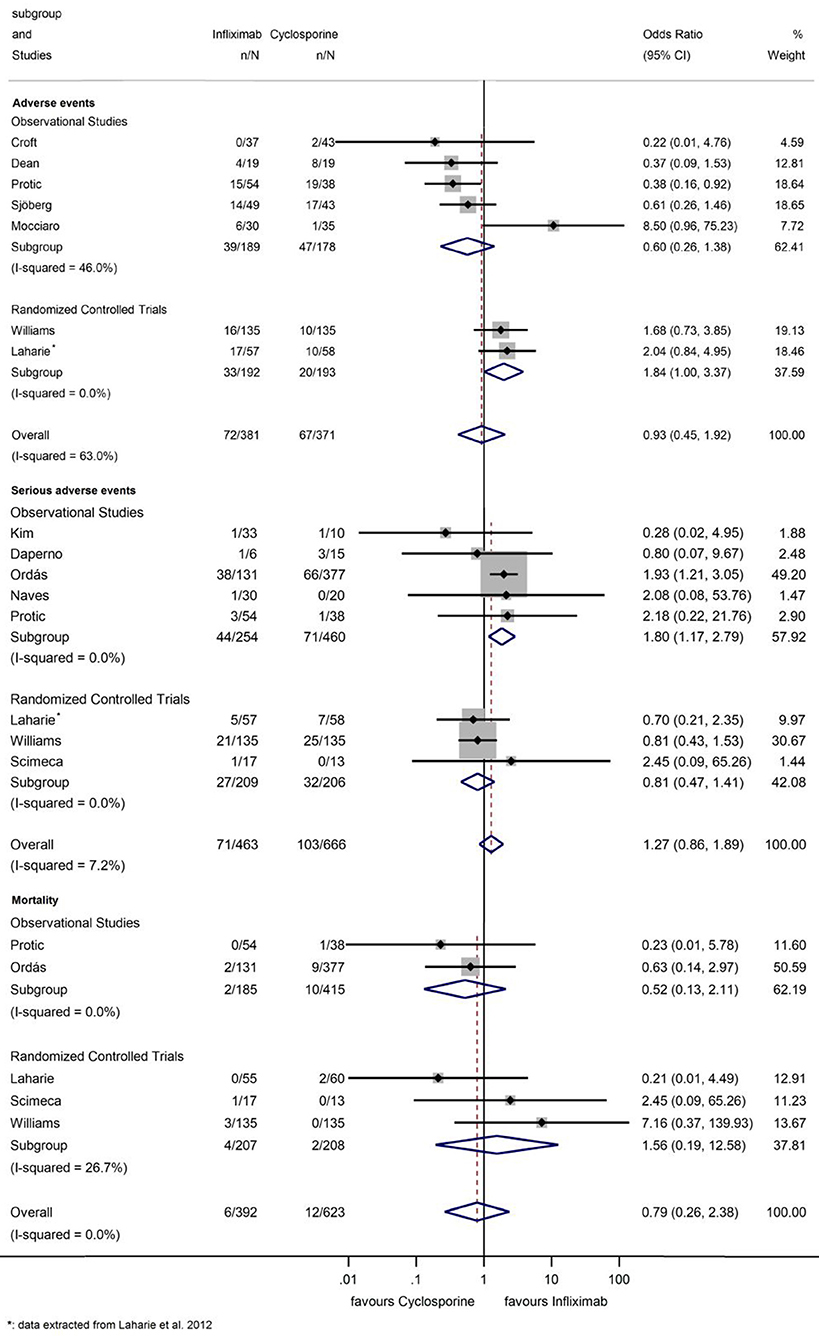
Figure 7. Odds ratios of studies evaluating adverse events, serious adverse events, and mortality during infliximab treatment compared to the cyclosporine group in steroid-refractory acute severe ulcerative colitis.
The cumulative Z-curve of the risk of AE during TSA reached but not crossed the conventional boundary (Figure 2). The number of participants included (n = 385) did not reach the required information size (n = 749), the cumulative Z-curve does not cross the monitoring boundary either.
Eight studies reported on SAE, such as opportunistic infections, sepsis, anaphylactic reaction and hepato- and nephrotoxicity (Figure 7) (12, 13, 19, 21, 24, 26–28). One hundred and three (15.5%) SAEs were reported with CYS and 72 (15.3%) with IFX. Rate of SAE was not elevated with IFX compared to that with CYS (OR = 1.27, 95% CI: 0.86–1.89, p = 0.236); although in the subgroup analysis of observational studies (21, 24, 26–28), IFX was associated with a higher SAE rate (OR = 1.80, 95% CI: 1.17–2.79, p = 0.008). However, in the three RCTs (13, 18, 19), no statistically significant difference could be detected between the two groups (OR = 0.81, 95% CI: 0.47–1.41, p = 0.461), data proved to be homogeneous (I2 = 0.0%, p = 0.712; I2 = 0.0%, p = 0.781, and I2 = 7.2%, p = 0.374 for observational and randomized studies and overall, respectively).
TSA of SAE showed that the number of patients in the analysis of RCTs did not reach the required information size and the cumulative Z-curve did not cross the monitoring boundary (Figure 3).
There was also no significant difference between treatment groups regarding mortality (OR: 0.79, 95% CI: 0.26–2.38, p = 0.678; I2 = 0.0%, p = 0.411) (Figure 7) (13, 18, 19, 27, 28).
The GRADE assessment of safety outcomes (AE, SAE, and mortality) showed low quality of evidence for the analyses of RCTs and very low quality of evidence for that of non-randomized studies (Table 3).
Risk of Bias Assessment
Assessments of the risk of bias of the included studies are shown in Figure 8. In the observational studies, the representativeness of the exposed and the selection of the non-exposed cohort was judged to be at high risk in multiple studies (23, 28, 30). In the studies of Daperno, Protic, and Radojcic, no comparison was performed between groups regarding age, sex, and extent of disease (21, 28, 29).
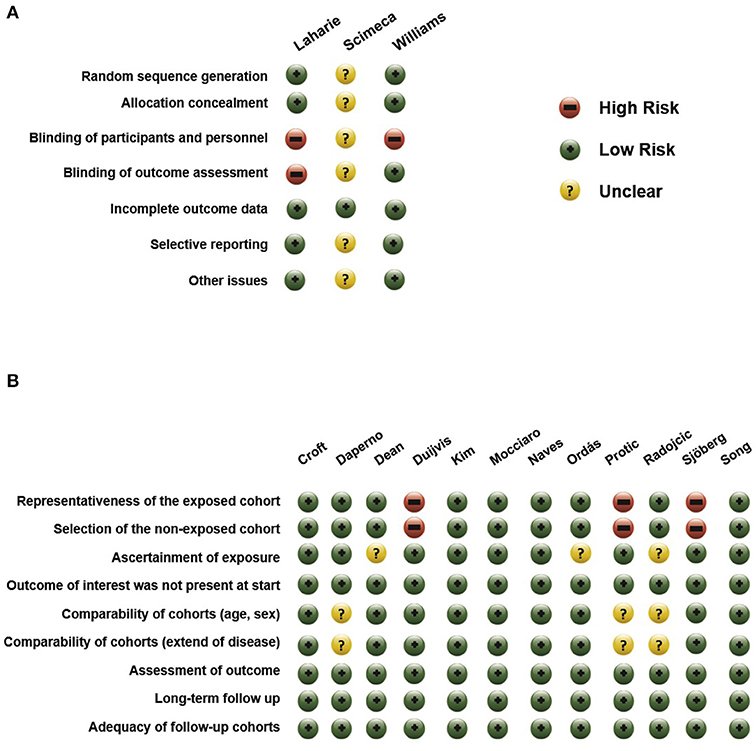
Figure 8. Risk of bias in (A) RCTs and in (B) non-randomized studies.
Among the RCTs, the studies of Williams and Laharie carried the lowest risk of bias (13, 18). As they were open trials, participants and personnel were not blinded; however, in the study of Williams, outcome assessment remained blinded. Because the study of Scimeca et al., was only published in a conference abstract form, almost all domains were judged as carrying “unclear” risk of bias (19).
Discussion
Summary of Main Findings
ASUC is a medical emergency and should be managed in high-volume tertiary centers with a multidisciplinary approach. In patients failing to respond to parenteral corticosteroids, medical rescue therapy including CYS or IFX is needed. Recently, a meta-analysis has covered the short-term efficacy of the two drugs in treatment response and 12 months colectomy rates but failed to discuss long-term outcomes (14).
In our meta-analysis, we collected RCTs and observational studies to perform long-term statistics focusing on colectomy-free survival rates and drug safety. Our combined data from all the studies showed that there was a significantly higher colectomy-free survival rate with IFX compared to that with CYS. This difference was only seen within the first 3 years after rescue therapy was initiated and it disappeared after the fourth year of follow-up. Additionally, we performed a subgroup analysis by study design to reveal selection bias when comparing RCTs and observational studies. Higher colectomy-free survival was found in observational studies with IFX but not in RCTs. It should be noted that the level of heterogeneity was moderate to substantial in the analysis from observational studies whilst data from RCTs were homogenous. When evaluating safety outcomes, no significant difference was detected between CYS and IFX treatment groups regarding AE, SAE, and mortality. The neutral association calculated from RCTs proved to be underpowered (indicated by TSA) and therefore insufficient to draw a final conclusion (36).
During ASUC treatment, early identification of steroid refractoriness and early introduction of rescue treatments are crucial to avoid morbidity and mortality. A variety of risk prediction tools have been developed to identify patients with ASUC being suitable for second-line medical therapy, these tools are used in clinical practice (such as the Oxford criteria and the Ho index) (53, 54). In a retrospective study, older age, severe endoscopic lesions, high CRP, low albumin levels and low serum IFX levels were identified as predictors of IFX failure in ASUC (30). Due to increased intestinal loss of IFX in ASUC, the serum IFX levels could be decreased; therefore, a modified IFX induction strategy can be considered (55). However, the results of other studies have opposed this association. Dose optimization based on IFX drug level monitoring may result in better patient outcomes (56, 57). In a retrospective study and meta-analysis, no association was found between accelerated IFX induction therapy and lower rates of colectomy in patients with ASUC, compared to standard induction therapy (58). The benefit of intensified induction regimen, i.e., shorter dosing intervals and/or higher doses of IFX is still not proven.
Limitations and Strengths
However, we are aware that our findings suffer from several limitations. First, most of the studies were non-randomized, retrospective studies, and the number of RCTs was low. Second, the use of maintenance therapy after the initial response was not uniform in all studies and must have contributed to the variation in the long-term outcomes. Third, the definitions of AE and SAE were often mixed together and were unclear in the reports; therefore, an internationally accepted guide has been adopted (17). Fourth, in two RCTs (13, 18), there is switch reported in some cases between CYS and IFX or IFX and CYS as third-line rescue therapy. The switch was necessary to avoid colectomy and achieve clinical remission. However, this can cause a difficulty defining the effect of the drug and may affect the long-term outcome.
We deviated from the PROSPERO protocol regarding an important point. Originally, the primary outcome was planned to be the 5 years colectomy-free survival. However, we thought that investigating the same outcome at multiple time points may improve the clinical yield of!!break the results.
Last, conference abstracts with limited information were also included in the meta-analysis, containing a high amount of unclear information and an increasing possibility of risk of bias.
There are several strengths of our meta-analysis that worth being highlighted. Altogether, a high number of patients with ASUC was investigated. Our meta-analysis is the first reporting more than 1 year colectomy free-survival rates with a high number of studies providing even seven or 10 years of colectomy-free survival data. Another strength of our meta-analysis is that the certainty of the evidence was examined for all outcomes according to the GRADE approach (37). Moreover, TSA was used to test whether the analyses are sufficiently powered; therefore, can be considered conclusive.
Conclusions
In summary, our meta-analysis has shown that there is no definitive evidence for any difference regarding long-term efficacy and safety between CYS and IFX in patients with steroid-refractory ASUC based on RCTs. Considering second-line treatment options in ASUC, the choice of drug depends on several factors other than efficacy and safety. Since the introduction of IFX, as rescue therapy for ASUC and a proxy for CYS, the length of hospital stay and in-hospital costs have been reduced significantly (59). On the other hand, the total costs up to 3 months after initiation of rescue therapy were significantly higher in the IFX group (59). However, since 2013 lower-cost IFX biosimilars are available, which may result in large cost savings in the future. In addition to safety and efficacy, other components of evidence-based medicine, such as the experience of treating physicians and patient preferences, should also be highlighted. In thiopurine-naïve patients, CYS can be preferred as a bridge to thiopurine maintenance treatment. IFX is a reasonable option for patients who have previously failed thiopurine maintenance therapy. Results of TSA and the lack of high-quality evidence in our meta-analysis highlight that further large RCTs are warranted to decide which therapy is the preferable rescue therapy in ASUC.
Data Availability Statement
The datasets analyzed in this article are not publicly available. Requests to access the datasets should be directed to KS, c3plbWVza0BnbWFpbC5jb20=.
Author Contributions
PS and KS designed the research. PS, KS, NF, and AS performed the research and statistical analyses, analyzed and interpreted the data. KS and PS wrote the article. BE, EM, KM, AE, and ZS made the critical revisions related to important intellectual content of the manuscript. PS and PH gave the final approval of the version of the article to be published.
Funding
This study was supported by the Economic Development and Innovation Operative Programme Grant (GINOP 2.3.2-15-2016-00048) and the Grant of the Hungarian Science Foundation (FK 132834).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2019.00338/full#supplementary-material
Abbreviations
AE, adverse events; ASUC, acute severe ulcerative colitis; AZA, azathioprine; CRP, C-reactive protein; CYS, cyclosporine; ESR, erythrocyte sedimentation rate; IFX, infliximab; IV, intravenous; OR, odds ratio; RCT, randomized controlled trial; SAE, serious adverse events; TNFα, tumor necrosis factor-alpha; TSA, trial sequential analysis; UC, ulcerative colitis.
References
1. Dinesen LC, Walsh AJ, Protic MN, Heap G, Cummings F, Warren BF, et al. The pattern and outcome of acute severe colitis. J Crohns Colitis. (2010) 4:431–7. doi: 10.1016/j.crohns.2010.02.001
2. Harbord M, Eliakim R, Bettenworth D, Karmiris K, Katsanos K, Kopylov U, et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. part 2: current management. J Crohns Colitis. (2017) 11:769–84. doi: 10.1093/ecco-jcc/jjx009
3. Jarnerot G, Rolny P, Sandberg-Gertzen H. Intensive intravenous treatment of ulcerative colitis. Gastroenterology. (1985) 89:1005–13. doi: 10.1016/0016-5085(85)90201-X
4. Herold KC, Lancki DW, Moldwin RL, Fitch FW. Immunosuppressive effects of cyclosporin A on cloned T cells. J Immunol. (1986) 136:1315–21.
5. Lichtiger S, Daniel H. Preliminary report: cyclosporin in treatment of severe active ulcerative colitis. Lancet. (1990) 336:16–9. doi: 10.1016/0140-6736(90)91521-B
6. Dulai PS, Jairath V. Acute severe ulcerative colitis: latest evidence and therapeutic implications. Ther Adv Chronic Dis. (2018) 9:65–72. doi: 10.1177/2040622317742095
7. Lichtiger S, Present DH, Kornbluth A, Gelernt I, Bauer J, Galler G, et al. Cyclosporine in severe ulcerative colitis refractory to steroid therapy. N Engl J Med. (1994) 330:1841–5. doi: 10.1056/NEJM199406303302601
8. Rolny P, Vatn M. Cyclosporine in patients with severe steroid refractory ulcerative colitis in the era of infliximab. Review article Scand J Gastroenterol. (2013) 48:131–5. doi: 10.3109/00365521.2012.733954
9. Lee J. Use of antioxidants to prevent cyclosporine a toxicity. Toxicol Res. (2010) 26:163–70. doi: 10.5487/TR.2010.26.3.163
10. Jarnerot G, Hertervig E, Friis-Liby I, Blomquist L, Karlen P, Granno C, et al. Infliximab as rescue therapy in severe to moderately severe ulcerative colitis: a randomized, placebo-controlled study. Gastroenterology. (2005) 128:1805–11. doi: 10.1053/j.gastro.2005.03.003
11. Brandse JF, Mathot RA, van der Kleij D, Rispens T, Ashruf Y, Jansen JM, et al. Pharmacokinetic features and presence of antidrug antibodies associate with response to infliximab induction therapy in patients with moderate to severe ulcerative colitis. Clin Gastroenterol Hepatol. (2016) 14:251–8.e1–2. doi: 10.1016/j.cgh.2015.10.029
12. Laharie D, Bourreille A, Branche J, Allez M, Bouhnik Y, Filippi J, et al. Ciclosporin versus infliximab in patients with severe ulcerative colitis refractory to intravenous steroids: a parallel, open-label randomised controlled trial. Lancet. (2012) 380:1909–15. doi: 10.1016/S0140-6736(12)61084-8
13. Williams JG, Alam MF, Alrubaiy L, Clement C, Cohen D, Grey M, et al. Comparison of iNfliximab and ciclosporin in STeroid resistant ulcerative colitis: pragmatic randomised trial and economic evaluation (CONSTRUCT). Health Technol Assess. (2016) 20:1–320. doi: 10.3310/hta20440
14. Narula N, Marshall JK, Colombel JF, Leontiadis GI, Williams JG, Muqtadir Z, et al. Systematic review and meta-analysis: infliximab or cyclosporine as rescue therapy in patients with severe ulcerative colitis refractory to steroids. Am J Gastroenterol. (2016) 111:477–91. doi: 10.1038/ajg.2016.7
15. Komaki Y, Komaki F, Micic D, Yamada A, Suzuki Y, Sakuraba A. Pharmacologic therapies for severe steroid refractory hospitalized ulcerative colitis: a network meta-analysis. J Gastroenterol Hepatol. (2017) 32:1143–51. doi: 10.1111/jgh.13674
16. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. (2010) 8:336–41. doi: 10.1016/j.ijsu.2010.02.007
17. ICH. Guideline for good clinical practice E6 (R2). In: The International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). (2019). Available online at: https://www.ich.org/products/guidelines/efficacy/article/efficacy-guidelines.html (accessed May 5, 2019).
18. Laharie D, Bourreille A, Branche J, Allez M, Bouhnik Y, Filippi J, et al. Long-term outcome of patients with steroid-refractory acute severe UC treated with ciclosporin or infliximab. Gut. (2018) 67:237–43. doi: 10.1136/gutjnl-2016-313060
19. Scimeca D, Bossa F, Annese V, Biscaglia G, Caruso N. Infliximab vs oral cyclosporin in patients with severe ulcerative colitis refractory to intravenous steroids. A controlled, randomized study. United European Gastroenterology week. Gut. (2012) 61(Suppl. 3):A165.
20. Croft A, Walsh A, Doecke J, Cooley R, Howlett M, Radford-Smith G. Outcomes of salvage therapy for steroid-refractory acute severe ulcerative colitis: ciclosporin vs. infliximab. Aliment Pharmacol Ther. (2013) 38:294–302. doi: 10.1111/apt.12375
21. Daperno M, Sostegni R, Scaglione N, Ercole E, Rigazio C, Rocca R, et al. Outcome of a conservative approach in severe ulcerative colitis. Dig Liver Dis. (2004) 36:21–8. doi: 10.1016/j.dld.2003.04.001
22. Dean KE, Hikaka J, Huakau JT, Walmsley RS. Infliximab or cyclosporine for acute severe ulcerative colitis: a retrospective analysis. J Gastroenterol Hepatol. (2012) 27:487–92. doi: 10.1111/j.1440-1746.2011.06958.x
23. Duijvis NW, Ten Hove AS, Ponsioen CI, van den Brink GR, Buskens CJ, Bemelman WA, et al. Similar short- and long-term colectomy rates with ciclosporin and infliximab treatment in hospitalised ulcerative colitis patients. J Crohns Colitis. (2016) 10:821–7. doi: 10.1093/ecco-jcc/jjw031
24. Kim EH, Kim DH, Park SJ, Hong SP, Kim TI, Kim WH, et al. Infliximab versus cyclosporine treatment for severe corticosteroid-refractory ulcerative colitis: a Korean, retrospective, single center study. Gut Liver. (2015) 9:601–6. doi: 10.5009/gnl14120
25. Mocciaro F, Renna S, Orlando A, Rizzuto G, Sinagra E, Orlando E, et al. Cyclosporine or infliximab as rescue therapy in severe refractory ulcerative colitis: early and long-term data from a retrospective observational study. J Crohns Colitis. (2012) 6:681–6. doi: 10.1016/j.crohns.2011.11.021
26. Naves JE, Llao J, Ruiz-Cerulla A, Romero C, Manosa M, Lobaton T, et al. Long-term comparative efficacy of cyclosporine- or infliximab-based strategies for the management of steroid-refractory ulcerative colitis attacks. Inflamm Bowel Dis. (2014) 20:1375–81. doi: 10.1097/MIB.0000000000000101
27. Ordás I, Domènech E, Mañosa M, García-Sánchez V, Iglesias-Flores E, Peñalva M, et al. Long-term efficacy and safety of cyclosporine in a cohort of steroid-refractory acute severe ulcerative colitis patients from the ENEIDA registry (1989–2013): a nationwide multicenter study. Am J Gastroenterol. (2017) 112:1709–18. doi: 10.1038/ajg.2017.180
28. Protic M, Seibold F, Schoepfer A, Radojicic Z, Juillerat P, Bojic D, et al. The effectiveness and safety of rescue treatments in 108 patients with steroid-refractory ulcerative colitis with sequential rescue therapies in a subgroup of patients. J Crohns Colitis. (2014) 8:1427–37. doi: 10.1016/j.crohns.2014.05.004
29. Radojcic M, Macrae F, Viney B. Infliximab versus cyclosporine in severe steroid-refractory ulcerative colitis; a comparison of clinical outcomes. J Gastroenterol Hepatol. (2014) 29:116–7.
30. Sjöberg M, Walch A, Meshkat M, Gustavsson A, Järnerot G, Vogelsang H, et al. Infliximab or cyclosporine as rescue therapy in hospitalized patients with steroid-refractory ulcerative colitis: a retrospective observational study. Inflamm Bowel Dis. (2012) 18:212–8. doi: 10.1002/ibd.21680
31. Song EM, Lee SH, Chang K, Hwang SW, Park SH, Yang DH, et al. Long-term outcomes of cyclosporine A and infliximab treatment for the management of steroid-refractory acute severe ulcerative colitis. J Crohn's and Colitis. (2018) 12:S182. doi: 10.1093/ecco-jcc/jjx180.294
32. Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. (2012) 12:9. doi: 10.1186/1471-2288-12-9
33. Wells GA, Shea B, O'Connell D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. (2019). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed May 5, 2019).
34. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
35. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. (1986) 7:177–88. doi: 10.1016/0197-2456(86)90046-2
36. Thorlund K, Engstrom J, Wetterslev J. User Manual for Trial Sequential Analysis (TSA). Copenhagen: Copenhagen Trial Unit, Centre for Clinical Intervention Research (2019). Available online at: www.ctu.dk/tsa (accessed June 15, 2019).
37. Schünemann H, Brozek J, Guyatt G, Oxman A. Handbook for Grading the Quality of Evidence and the Strength of Recommendations Using The GRADE Approach. (2013). Available online at: https://gdt.gradepro.org/app/handbook/handbook.html#h.svwngs6pm0f2 (accessed May 5, 2019).
38. Lynch RW, Lowe D, Protheroe A, Driscoll R, Rhodes JM, Arnott ID. Outcomes of rescue therapy in acute severe ulcerative colitis: data from the United Kingdom inflammatory bowel disease audit. Aliment Pharmacol Ther. (2013) 38:935–45. doi: 10.1111/apt.12473
39. Govani SM, Waljee AK, Stidham RW, Higgins PD. Infliximab reduces 90 day colectomy rate versus cyclosporine for acute severe ulcerative colitis. Gastroenterology. (2014) 146:S464. doi: 10.1016/S0016-5085(14)61661-9
40. Nelson R, Liao C, Fichera A, Rubin DT, Pekow J. Rescue therapy with cyclosporine or infliximab is not associated with an increased risk for postoperative complications in patients hospitalized for severe steroid-refractory ulcerative colitis. Inflamm Bowel Dis. (2014) 20:14–20. doi: 10.1097/01.MIB.0000437497.07181.05
41. Yoshimura N, Tadami T, Kawaguchi T, Sako M, Saniabadi A, Takazoe M. Comparative short-term efficacy of cyclosporine, tacrolimus and infliximab in hospitalized patients with severe corticosteroid-refractory ulcerative colitis: a retrospective study. Gastroenterology. (2013) 144:S209–10. doi: 10.1016/S0016-5085(13)60738-6
42. Cunningham G, Macisaac M, Ding N, Spizzo P, Connell W, Wright E, et al. Colectomy rates remain high in the era of rescue therapy for acute severe ulcerative colitis: a single-center experience. J Gastroenterol Hepatol. (2017) 32:124. doi: 10.1111/jgh.13895
43. Chaparro M, Burgueño P, Iglesias E, Panés J, Muñoz F, Bastida G, et al. Infliximab salvage therapy after failure of ciclosporin in corticosteroid-refractory ulcerative colitis: a multicentre study. Aliment Pharmacol Therapeut. (2012) 35:275–83. doi: 10.1111/j.1365-2036.2011.04934.x
44. Motoya S, Miyakawa M, Nasuno M, Tanaka H. Short-and long-term outcomes of infliximab and calcineurin inhibitor treatment for steroidrefractory ulcerative colitis. J Crohn's Colitis. (2016) 10:S291–2. doi: 10.1093/ecco-jcc/jjw019.502
45. Patrick D, Ballard E, O'Rourke P, Howlett M, Radford-Smith GL. Comparing colectomy rates in treatment naïve vs. Treatment experienced patients with acute severe ulcerative colitis (ASUC). J Gastroenterol Hepatol. (2015) 30:135. doi: 10.1111/jgh.13094
46. Leblanc S, Allez M, Seksik P, Flourie B, Peeters H, Dupas JL, et al. Successive treatment with cyclosporine and infliximab in steroid-refractory ulcerative colitis. Am J Gastroenterol. (2011) 106:771–7. doi: 10.1038/ajg.2011.62
47. Shepherd S, Wright EK, Holmes JA, Brown SJ, Lust M, Kamm MA, et al. Outcomes of salvage therapy for acute severe colitis treatment in a single tertiary center: infliximab v. cyclosporine. J Gastroenterol Hepatol. (2014) 29:123. doi: 10.1111/jgh.12736-6
48. Protic M, Frei P, Radojicic ZA, Schoepfer A, Juillerat P, Mottet C, et al. Comparative long-term outcomes of tacrolimus, cyclosporine and infliximab for steroid-refractory ulcerative colitis-week 52 results swiss IBD cohort study. Gastroenterology. (2013) 144:S428–9. doi: 10.1016/S0016-5085(13)61578-4
49. Duijvis N, Ten Hove A, Ponsioen C, Van Den Brink G, Te Velde A, D'Haens G, et al. Lower long-term colectomy rates with IFX than with CsA treatment in moderate to severe UC. J Crohns Colitis. (2015) 9:S53–4. doi: 10.1093/ecco-jcc/jju027.080
50. Seibold F, Protic M, Frei P, Mottet C, Juillerat P, Knezevic T, et al. Colectomy rate two years after sequential rescue treatments in steroid refractory ulcerative colitis. Gastroenterology. (2017) 152:S409. doi: 10.1016/S0016-5085(17)31597-4
51. Truelove SC, Witts LJ. Cortisone in ulcerative colitis; preliminary report on a therapeutic trial. Br Med J. (1954) 2:375–8. doi: 10.1136/bmj.2.4884.375
52. Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med. (1987) 317:1625–9. doi: 10.1056/NEJM198712243172603
53. Travis SP, Farrant JM, Ricketts C, Nolan DJ, Mortensen NM, Kettlewell MG, et al. Predicting outcome in severe ulcerative colitis. Gut. (1996) 38:905–10. doi: 10.1136/gut.38.6.905
54. Ho GT, Mowat C, Goddard CJ, Fennell JM, Shah NB, Prescott RJ, et al. Predicting the outcome of severe ulcerative colitis: development of a novel risk score to aid early selection of patients for second-line medical therapy or surgery. Aliment Pharmacol Ther. (2004) 19:1079–87. doi: 10.1111/j.1365-2036.2004.01945.x
55. Brandse JF, van den Brink GR, Wildenberg ME, van der Kleij D, Rispens T, Jansen JM, et al. Loss of infliximab into feces is associated with lack of response to therapy in patients with severe ulcerative colitis. Gastroenterology. (2015) 149:350–5.e2. doi: 10.1053/j.gastro.2015.04.016
56. Dotan I, Ron Y, Yanai H, Becker S, Fishman S, Yahav L, et al. Patient factors that increase infliximab clearance and shorten half-life in inflammatory bowel disease: a population pharmacokinetic study. Inflamm Bowel Dis. (2014) 20:2247–59. doi: 10.1097/MIB.0000000000000212
57. Seow CH, Newman A, Irwin SP, Steinhart AH, Silverberg MS, Greenberg GR. Trough serum infliximab: a predictive factor of clinical outcome for infliximab treatment in acute ulcerative colitis. Gut. (2010) 59:49–54. doi: 10.1136/gut.2009.183095
58. Nalagatla N, Falloon K, Tran G, Borren NZ, Avalos D, Luther J, et al. Effect of accelerated infliximab induction on short- and long-term outcomes of acute severe ulcerative colitis: a retrospective multicenter study and meta-analysis. Clin Gastroenterol Hepatol. (2019) 17:502–9.e1. doi: 10.1016/j.cgh.2018.06.031
Keywords: steroid-refractory, ulcerative colitis, cyclosporine, infliximab, colectomy, meta-analysis
Citation: Szemes K, Soós A, Hegyi P, Farkas N, Erős A, Erőss B, Mezősi E, Szakács Z, Márta K and Sarlós P (2020) Comparable Long-Term Outcomes of Cyclosporine and Infliximab in Patients With Steroid-Refractory Acute Severe Ulcerative Colitis: A Meta-Analysis. Front. Med. 6:338. doi: 10.3389/fmed.2019.00338
Received: 30 October 2019; Accepted: 23 December 2019;
Published: 21 January 2020.
Edited by:
Fernando Gomollón, University of Zaragoza, SpainReviewed by:
Juan Ricardo Marquez, Instituto de Coloproctología ICO S.A.S., ColombiaHiroshi Nakase, Sapporo Medical University, Japan
Copyright © 2020 Szemes, Soós, Hegyi, Farkas, Erős, Erőss, Mezősi, Szakács, Márta and Sarlós. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Péter Hegyi, aGVneWkucGV0ZXJAcHRlLmh1; Patrícia Sarlós, c2FybG9zLnBhdHJpY2lhQHB0ZS5odQ==