 Nicola Principi
Nicola Principi Barbara Camilloni
Barbara Camilloni Anna Alunno2
Anna Alunno2 Ilaria Polinori
Ilaria Polinori Alberto Argentiero
Alberto Argentiero Susanna Esposito
Susanna Esposito
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Med., 28 May 2019
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 6 - 2019 | https://doi.org/10.3389/fmed.2019.00109
This article is part of the Research TopicRespiratory Virus Infection: Recent AdvancesView all 10 articles
Vaccines remain the best measure to reduce total influenza burden. However, presently available influenza vaccines have some limitations that cause a reduced efficacy compared to immunization practices with other respiratory pathogens. This paper shows the clinical roles of antiviral drugs against influenza that have been licensed in at least one country and the potential roles of compounds that are in development. Several attempts have been made to develop new agents against influenza viruses to overcome the supposed or demonstrated limitations of neuraminidase inhibitors (NAIs). Antibodies against the highly conserved stem region of the haemagglutinin molecule of influenza A viruses and drugs that target different stages of the influenza virus life cycle than NAIs in human cells have been developed and tested. Among these preparations, baloxavir marboxil (BAM), and favipiravir (FP) (i.e., polymerase inhibitors) are the only drugs that have reached the market (the first in Japan and the USA, and the second only in Japan). Other antiviral compounds and monoclonal antibodies are in advanced stage of development, but none of these new drugs and monoclonal antibodies in development have adequate characteristics to substitute for NAIs at present. However, although NAIs remain the drug of choice for influenza treatment, their overuse has to be avoided. Accurate selection of patients for whom treatment is truly needed is required.
Vaccines represent the best way to reduce the influenza impact (1–3). However, influenza viruses vary continuously through antigenic drifts and occasional antigenic shifts that help the virus evade pre-existing immunity (4). Therefore, continuous reformulation of vaccine compositions and annual immunization are needed. In the case of viral shifts, licensed vaccines are completely ineffective, and ad hoc vaccine preparations are generally available only several weeks after the emergence and spread of a pandemic influenza virus (5). Finally, the immune responses induced by the influenza vaccines are suboptimal in a number of subjects, especially in younger children and the elderly, who are at risk of severe influenza, which further reduces the protection offered by influenza vaccination (6).
In addition to the intrinsic limitations of influenza vaccines, a second problem limits the vaccine-induced prevention of influenza. Universal immunization against influenza in pediatric age is recommended only in a minority of countries (2). Healthy children and adults frequently are not included in the list of patients for whom official health authorities strongly suggest influenza immunization (7). Moreover, even when vaccines are recommended worldwide, for example, in the elderly, influenza vaccination coverage remains suboptimal (8, 9). The World Health Organization estimates that 5–10% of the global population suffers from influenza every year, 3–5 million people develop severe influenza and 290,000–650,000 people die (10); thus, developing safe and effective alternatives for prophylaxis and treatment is critical.
In this paper, the clinical roles of antiviral drugs against influenza that have been licensed in at least one country will be discussed. Additionally, the potential roles of the anti-influenza compounds in development are evaluated.
Antiviral drugs have been developed for a long time in an attempt to overcome the abovementioned problems and reduce the influenza-related risks. For years, the adamantane derivatives rimantadine and amantadine and the neuraminidase inhibitors (NAIs) oseltamivir, zanamivir (used worldwide) and, more recently, laninamivir and peramivir (used first in Japan and subsequently in China, Japan, South Korea, and the USA) have been the only drugs licensed for influenza prevention and control. However, these drugs have differences in their pharmacokinetic characteristics, routes of administration and ages of the targeted patients (11).
Starting from the 2004–2005 influenza season, use of adamantane derivatives was no longer recommended, mainly due to the emergence of resistance in most circulating influenza viruses. However, their activity was limited to influenza A viruses, and they showed poor tolerability, which could be considered sufficient reasons per se to avoid prescription of these drugs (12). In practice, only NAIs have been prescribed for influenza prevention and treatment since that time period. The emergence of influenza virus strains resistant to NAIs has been reported. Resistance to oseltamivir emerged only during the 2007–2008 and 2008–2009 influenza seasons, with up to 90% of circulating strains exhibiting resistance to this NAI (13–15). Fortunately, the influenza virus strains circulating during the 2009 pandemic and in the following years rarely contained the mutations in the neuraminidase viral surface glycoprotein that conferred resistance to oseltamivir. Localized clusters of oseltamivir-resistant influenza virus have been reported (16) and resistance to NAIs is increasing (17).
However, generally, an influenza virus resistant to oseltamivir is sensitive to the other NAIs, because cross resistance among oseltamivir and other NAIs has not been observed (18, 19). Patients with influenza due to an oseltamivir-resistant virus can be successfully treated with other NAIs, such as zanamivir (15). In patients undergoing treatment, the NAI-resistant viruses are found to be NA subtype–specific and drug-specific (16, 19, 20). These clinically-derived NAI-resistant variants of influenza A viruses of N1 NA subtype most frequently carry H274Y and N294S NA amino acid substitutions. Viruses of N2 NA subtype carry E119Vand R292K NA mutations, and NAI-resistant variants of influenza B viruses harbor R152K and D198N NA mutations. Another important point is that NAI-resistant viruses can emerge either under drug-selection pressure or naturally in the course of influenza virus evolution (without drug intervention). The high prevalence of oseltamivir-resistant A/Brisbane/59/2007(H1N1)-like viruses (subclade 2B) carrying the NA H274Y–resistance marker was reported worldwide during the 2007–2009 influenza seasons (16, 19, 20). Epidemiologic studies did not show evidence of an association between the development of resistance and oseltamivir use. Thus, H274Y NA amino acid substitution occurred naturally, and viruses with this mutation acquired remarkable transmissibility and superior fitness compared to their drug-sensitive counterparts (19, 20).
Moreover, all NAIs have been found to be safe and well tolerated. In particular, oseltamivir, which is the most frequently used NAI, can be administered not only to otherwise healthy adults and subjects with severe underlying disease but also to neonates, younger infants (18) and pregnant women (21) with age- and weight-appropriate doses without significant risks of severe adverse events.
Based on the results of several clinical trials, NAIs have been considered effective for the prevention and control of influenza infection (22, 23). Most available studies in this regard were carried out with oseltamivir and zanamivir, which were marketed before the other NAIs (24–28). Moreover, all of the data collected in younger children were derived from studies in which oseltamivir was used instead of zanamivir, which was licensed for use only in school-age patients. The effectiveness of NAIs has been documented in some meta-analyses, including those by Jefferson et al. (24) and Dobson et al. (25). A global evaluation of all of the studies analyzed in these meta-analyses suggests the conclusion that NAIs can limit the severity and duration of influenza in patients of any age with uncomplicated disease. However, the efficacy is time-dependent, because it is seen mainly in subjects who receive these drugs within the first 48 h of symptom onset. Jefferson et al. (24) and Dobson (25) calculated that administration of oseltamivir in adults with uncomplicated influenza decreased the time to first alleviation of symptoms of influenza-like illness (ILI) by 16.8 h [95% confidence interval [CI], 8.4–25.1] and 17.8 h (95% CI, 27.1 to −9.3), respectively. When only laboratory-confirmed influenza cases were considered, the advantage was slightly higher, because the time to perceived benefits was decreased by 25.2 h (95% CI, 16.0–36.2) (25). Similar results were reported for zanamivir, with the difference in time to alleviation of ILI symptoms reported as 14.4 h (95% CI, 9.36–19.44). No substantial differences were noted in the results obtained in children treated with oseltamivir (24). Regarding prophylaxis, it was calculated that oseltamivir could reduce the absolute risk for laboratory-confirmed influenza among community members and nursing home residents by 3.05% [relative risk [RR] 0.45; 95% CI, 0.30–0.67] and in a household setting by 13.6% (RR 0.20; 95% CI, 0.09–0.44) (21).
However, the available data do not permit firm conclusions regarding the effect of NAIs on severe cases (26–28). Although administration of NAIs was associated with a reduction of mortality during the recent 2009 pandemic (29), the impact on the development of serious influenza complications, hospitalization and mortality was not definitively demonstrated. The results of studies specifically planned to evaluate these problems were conflicting (30). A good example in this regard is given by studies that have measured the prevention of acute otitis media (AOM), which is a common complication of influenza in children. Jefferson et al. (24) did not find any statistically significant effect of oseltamivir on this disease (RR 0.8; 95% CI, 0.62–1.02), whereas Wang et al. (31) reported a statistically significant reduction in the AOM incidence with oseltamivir treatment in children 1–12 years of age (risk difference [RD] −0.09; 95% CI, −0.16 to −0.03). Moreover, in some cases, such as the meta-analysis by Muthuri et al. (32), NAI treatment was shown to be associated with an increased risk of severe outcomes, including pneumonia (OR 2.29; 95% CI, 1.16–4.53). Because laninamivir (33) and peramivir (34) do not seem to have substantially different efficacies compared to that of oseltamivir, these findings explain why the present possibility of treating influenza with NAIs cannot be considered completely satisfactory and the development of new drugs against influenza viruses has been deemed mandatory.
Several new approaches have been attempted to achieve influenza prevention and control. Antibodies against the highly conserved stem region of the haemagglutinin (HA) molecule of influenza A viruses and drugs that target different stages of the influenza virus life cycle than NAIs in human cells have been developed and tested (35). Among these preparations, baloxavir marboxil (BAM) and favipiravir (FP) are the only drugs that have reached the market (the first in Japan and the USA and the second only in Japan).
BAM was licensed in 2018 in Japan and the USA for the treatment of uncomplicated influenza in subjects aged ≥ 12 years with influenza clinical manifestations for ≤48 h (36). BAM is a prodrug that is given by mouth and is hydrolysed in the intestine, blood, and liver to form baloxavir acid (BXA), which is the active compound (37). The drug acts by inhibiting the cap-dependent endonuclease activity of the influenza A and B virus polymerase acidic protein (PA) to prevent the so-called cap snatching (i.e., the mechanism used by viruses to deviate the host mRNA transcription system and allow synthesis of viral RNAs) (37). In practice, BMA, in contrast to NAIs that reduce viral release from infected cells (38), inhibits viral replication. In vitro studies have shown that this activity is exerted without cytotoxicity even in cells infected with NAI-resistant influenza viruses. Moreover, BMA was shown to be effective not only against influenza viruses that usually infected humans but also against avian subtypes (39).
Phase 1 clinical trials were carried out in a total of 55 healthy subjects aged 20–59 years and were mainly directed to evaluate the safety, tolerability, pharmacokinetics and food effects (40). BAM was well tolerated, as no serious adverse events or deaths were reported. Moreover, treatment-emergent adverse events, such as headache, stomatitis, an increased eosinophil count, and elevation of alanine aminotransferase (ALT) and aspartate aminotransferase (AST), emerged in a very small number of subjects, were mild and resolved spontaneously within a few days. Only one subject had an increased lactate dehydrogenase (LDH) serum concentration that did not disappear during the follow-up period (22 days). Pharmacokinetic data confirmed that the drug could be administered as a single dose because its half-life was very long (more than 70 h). Moreover, even the lowest dose of the drug used in these trials (6 mg of BAM) was associated with high BXA serum concentrations 24 h after the single dose. Finally, food could influence drug metabolism, since BXA concentrations were lower in subjects who were fed or when measured before meal states. However, the levels remained high enough to ensure significant viral inhibition (40).
Phase 2 and 3 studies involving subjects aged 12–64 years confirmed the efficacy and safety of BAM (41). Adverse events, such as diarrhea, bronchitis, nausea, common cold symptoms (nasopharyngitis), and headache, were reported in ~2% of patients and were not considered severe. Moreover, in otherwise healthy subjects with fever and mild to moderate uncomplicated respiratory disease for <48 h, administration of the drug could lead to a reduction of the mean time to alleviation of symptoms of ~50–65 h compared to the 77.7–80 h required for patients who received a placebo. However, the clinical efficacy was not different from that evidenced in patients receiving oseltamivir, although BAM administration was associated with a more rapid decline in the viral load and a shorter duration of infectious virus detection (41). Similar results were obtained with a double-blind, randomized, placebo-, and oseltamivir-controlled trial carried out in patients >12 years old suffering from influenza for <48 h with an underlying disease that was considered a risk factor for influenza-related complications. In this study, a shorter time to improvement of symptoms was also evidenced in the BAM group than in the placebo group (median 73.2 h vs. 102.3 h, p < 0.0001), whereas the efficacy of oseltamivir was quite similar (81.0 h, p = 0.8347). However, when the efficacy against the different types of influenza viruses was tested, BAM and oseltamivir demonstrated similar efficacies against the A/H3N2 virus, but the new drug was superior to oseltamivir against B viruses (time to symptom improvement 74.6 h vs. 101.6 h; p = 0.0251) (41). Moreover, despite the presence of severe underlying diseases, adverse events remained uncommon and did not differ from those found in patients receiving placebo or oseltamivir.
BAM has at least two important advantages over other available anti-influenza virus drugs. It is administered as a single dose by mouth, and it can overcome the problem of influenza viruses resistant to NAIs (39). Oseltamivir is also given by mouth, but to be effective it needs 5 days of administration, which can reduce compliance. Peramivir is given as a single dose by the intravenous route, requires administration by a nurse or a doctor and is more expensive than BAM. Zanamivir and laninamivir are administered by inhalation and are difficult to use in younger children.
However, despite obtaining a Food and Drug Administration (FDA) license, some unsolved problems seem to indicate that the use of BAM in clinical practice as an alternative to NAIs, particularly oseltamivir, for treatment of uncomplicated influenza cases can be debated. First, BAM is more expensive than oseltamivir. The cost of treatment with BAM has been calculated to be ~3 times higher than that of treatment with oseltamivir (42). Moreover, the epidemiological and clinical importance of resistance to BAM is not precisely defined. Before obtaining the license, almost all isolated influenza virus strains were susceptible to BAM. A study carried out in the USA showed that the frequency of genetic mutations (amino acid 38 substitutions for isoleucine in the endonuclease domain of the viral RNA polymerase PA subunit) that caused reduced susceptibility of influenza viruses to BAM was very low during the 2016/2017 and 2017/2018 seasons (43). Moreover, no mutated virus was detected in 2018/2019 before BAM was licensed (43). However, treatment was associated with a rapid and substantial emergence of resistant strains. Some of the studies used to obtain the license evidenced that mutated viruses could be identified in 2.2–9.7% of cases (41). Resistance to BAM was also evidenced in Japan after its introduction in clinical practice. A pediatric study showed that ~20% of treated children developed mutations (44). Recently, this problem was confirmed in strains isolated from adult patients (45). Although the mutated viruses remained sensitive to NAIs and had an impaired replicative capacity in vitro (44), patients with mutations shed the viruses and remained symptomatic for a longer period than those without the mutations (41), suggesting a potential negative effect of resistance to BAM.
These findings seem to suggest that emergence of resistance to BAM should be strictly monitored and that the clinical effects of BAM should be more carefully evaluated. Because definitive data in this regard are lacking, the routine use of BAM for treatment of uncomplicated influenza in adults seems premature. On the other hand, development of BAM is not complete. BAM is not licensed for complicated influenza cases. Moreover, data from children, pregnant women and patients at risk are rare or completely lacking, as are data concerning influenza prophylaxis.
FP is a prodrug. FP is a nucleoside analog that after oral ingestion requires intracellular phosphoribosylation to be transformed into its active form, FP ribofuranosyl-5′-triphosphate (FRTP). Similar to BAM, FRTP acts by reducing viral replication through inhibition of the RNA-dependent RNA polymerase (RdRp) of RNA viruses (46). However, its activity is not limited to influenza viruses but instead is extended to several other RNA viruses, including arenaviruses, phleboviruses, hantaviruses, flaviviruses, enteroviruses, respiratory syncytial virus, and noroviruses (47). In vitro studies have shown that FP is effective against all of the influenza virus subtypes, including the avian viruses and those that are poorly sensitive or insensitive to NAIs (48–50). In experimental animals, FP was found to be significantly more effective than oseltamivir in preventing influenza or reducing its severity in mice infected with lethal doses of influenza viruses, even when the treatment was started 72 h after infection (51). Moreover, when used in combination with oseltamivir, protection due to the NAI was increased and the treatment efficacy window was extended to 96 h after symptom onset (52).
The safety and tolerability of FP were found to be good, although some data regarding the potential teratogenicity of FP were collected in all animal species assessed (53). Interestingly, the exposure causing teratogenicity was quite similar to that found in humans receiving the dosage of the drug that was useful for influenza treatment. Finally, although in vitro studies have shown that viral mutations associated with non-viable viral phenotypes rapidly develop in influenza viruses exposed to this drug, in vivo use of FP is only rarely associated with influenza virus mutations (54).
Some phase 2 and 3 studies in adults have been carried out in Japan, the USA and Europe (NCT01068912, NCT02026349, NCT02008344, NCT01728753, and NCT03394209). Generally, the drug was administered by mouth two times per day for 5 days even when different dosages were used. Most studies were completed several months ago, but the results are not available with the exception of those from NCT01068912, which aimed to identify the most effective and best tolerated drug dosage. The reasons for the unavailability of the study results are unknown. However, FP is licensed for use in humans in Japan. Its use is authorized only in patients infected by a novel or re-emerging influenza virus (i.e., a pandemic virus?) that is resistant to all other available influenza drugs. To avoid irrational prescriptions, FP is distributed only upon request by the Minister of Health, Labor and Welfare of Japan. Moreover, the guidelines clearly establish that pregnant women are excluded from use of FP, and females of childbearing potential have to avoid pregnancy in the 7 days following drug use to obtain the complete elimination of the FP concentration from the plasma (55).
Pimodivir is an oral drug that inhibits the polymerase basic protein 2 (PB2) subunit of the influenza A virus polymerase complex. Consequently, it inhibits viral replication (56). In vitro and experimental animal studies have shown that pimodivir is effective against influenza A virus, even when strains resistant to NAIs are tested. Compared to oseltamivir, it was more effective in improving body weight and reducing the severity of lung infection. However, its activity can significantly vary according to the influenza A virus subtype, probably as a consequence of differences in the PB2 structure among various A viruses (57). Positive results were also obtained when the drug was tested in humans with uncomplicated influenza, for whom pimodivir reduced viral shedding and influenza symptoms. Generally, adverse events (mainly diarrhea) were mild and spontaneously resolved within a few days (58). These findings were confirmed by a double-blinded phase 2b study involving adults with uncomplicated influenza A in whom different pimodivir dosages were given 2 times per day for 5 days alone or in combination with oseltamivir (59). This study showed that 600 mg of the drug per dose was adequate to obtain the best results. In the treated groups, both the viral load titer and the time to symptom resolution were reduced compared to those of the placebo group. Moreover, combined therapy was more effective than administration of pimodivir alone (59, 60).
However, the use of pimodivir has been associated with the emergence of mutations leading to viruses with a several fold decrease in susceptibility to the drug. In particular, emergence of PB2 substitutions or phenotypic resistance to pimodivir was evidenced in 11 of 172 patients (6.4%) (59, 60). The mutations included S324K/N/R, F325L, S337P, K376N/R, T378S, and N510K (59, 60). Although the mutated viruses were not associated with a deterioration of clinical conditions and the patients did not shed the virus after treatment, this finding deserves attention.
Studies of natural immune responses to influenza virus infection evidenced that N-linked glycosylation sites in the haemagglutinin stem region of influenza A viruses were relatively well conserved and that antibodies against these sites were effective against a large number of influenza viruses (61–64). Starting from this evidence, a number of monoclonal antibodies targeting the HA conserved regions was developed and tested for the treatment of influenza A.
Preparations identified as MHAA4549A, MEDI8852, and VIS 410 have reached the phase II stage of development. All of these preparations were found to be safe and well tolerated and were able to reduce the peak viral load, duration of viral shedding, and influenza symptom scores compared to those of the placebo group (65–67). Moreover, no mutated virus was evidenced after monoclonal antibody administration (65–67). Compared to those of oseltamivir, all of these preparations have superior pharmacokinetic properties and a longer therapeutic window. The half-life is ~3 weeks, one dose can be sufficient to control infection and efficacy can be obtained even if administration occurs after 48 h from symptom onset (65, 68, 69). However, two clinical trials (NCT02293863 and NCT02603952) in which the efficacy of oseltamivir alone was compared to that of the combination oseltamivir/MHAA4549A or MEDI8852 in adults with influenza A infection revealed that addition of the monoclonal antibody did not add any significant clinical advantage to those offered by the old NAI. When these results are considered together with the fact that the activity is limited to influenza A viruses, this finding seems to be a relevant limitation that may preclude extensive use of monoclonal antibodies. However, a definitive conclusion in this regard can only be drawn when studies in patients with severe influenza illnesses and those at high risk, including children and pregnant women, are performed.
Table 1 summarizes antiviral drugs against influenza available on the market. Several attempts have been made to develop new agents against influenza viruses that are able to overcome the supposed or demonstrated limitations of NAIs. These drugs, mainly oseltamivir, are discussed in terms of the risk of emergence of resistant strains and doubts regarding their efficacy in severe influenza cases and prevention of bacterial complications or death. Some of the new drugs have been licensed or are in the advanced stages of development. However, none of them has been completely developed, and the lack of data regarding patients for whom oseltamivir is recommended is discussed. Moreover, in some cases, use of the new drugs has been associated with emergence of resistance. In practice, none of these new drugs and monoclonal antibodies that are in development has adequate characteristics to substitute for NAIs at present. However, although NAIs (especially oseltamivir due to its greater ease of administration) remain the drug of choice for influenza treatment, their overuse has to be avoided. Accurate selection of patients for whom treatment is truly needed is necessary. Finally, the limitations of antivirals can be overcome with more extensive use of influenza vaccines.
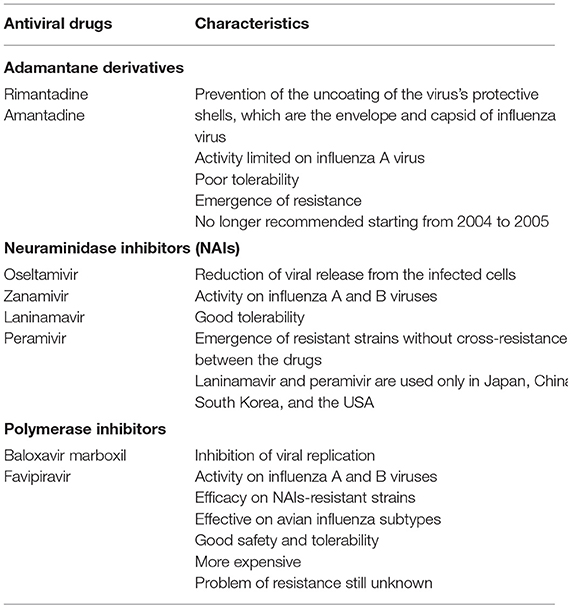
Table 1. Antiviral drugs against influenza available on the market.
NP wrote the first draft of the manuscript. BC and AAl gave scientific contributions. IP and AAr performed the literature review. SE co-wrote the manuscript and supervised all activities. All authors approved the final submitted version of the manuscript.
This work has received funding from the European Union's Horizon 2020 research and innovation programme under grant agreement No. 701088.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
2. Principi N, Senatore L, Esposito S. Protection of young children from influenza through universal vaccination. Hum Vaccin Immunother. (2015) 11:2350–8. doi: 10.1080/21645515.2015.1055428
3. Principi N, Esposito S, Marchisio P, Gasparini R, Crovari P. Socioeconomic impact of influenza on healthy children and their families. Pediatr Infect Dis J. (2003) 22(10 Suppl):S207–10. doi: 10.1097/01.inf.0000092188.48726.e4
4. Kim H, Webster RG, Webby RJ. Influenza virus: dealing with a drifting and shifting pathogen. Viral Immunol. (2018) 31:174–83. doi: 10.1089/vim.2017.0141
5. Chua JV, Chen WH. Bench-to-bedside review: vaccine protection strategies during pandemic flu outbreaks. Crit Care. (2010) 14:218. doi: 10.1186/cc8891
6. Sano K, Ainai A, Suzuki T, Hasegawa H. The road to a more effective influenza vaccine: up to date studies and future prospects. Vaccine. (2017) 35:5388–95. doi: 10.1016/j.vaccine.2017.08.034
7. Principi N, Camilloni B, Esposito S. Influenza immunization policies: which could be the main reasons for differences among countries? Hum Vaccin Immunother. (2018) 14:684–92. doi: 10.1080/21645515.2017.1405188
8. European Center for Disease prevention and Control. Seasonal Influenza Vaccination in Europe Vaccination Recommendations and Coverage Rates in the EU Member States for Eight Influenza Seasons 2007–2008 to 2014–2015. Available online at: https://ecdc.europa.eu/sites/portal/files/documents/seasonal-influenza-antiviral-use-2018.pdf (accessed May 15, 2019).
9. Chiu APY, Dushoff J, Yu D, He D. Patterns of influenza vaccination coverage in the United States from 2009 to 2015. Int J Infect Dis. (2017) 65:122–7. doi: 10.1016/j.ijid.2017.10.004
10. World Health Organization. Influenza (Seasonal). Available online at: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed January 25, 2019).
12. Duwe S. Influenza viruses - antiviral therapy and resistance. GMS Infect Dis. (2017) 5:Doc04. doi: 10.3205/id000030y
13. Dharan NJ, Gubareva LV, Meyer JJ, Okomo-Adhiambo M, McClinton RC, Marshall SA, et al. Infections with oseltamivir-resistant influenza A(H1N1) virus in the United States. JAMA. (2009) 301:1034–41. doi: 10.1001/jama.2009.294
14. Hurt AC, Ernest J, Deng YM, Iannello P, Besselaar TG, Birch C, et al. Emergence and spread of oseltamivir-resistant A(H1N1) influenza viruses in Oceania, South East Asia and South Africa. Antiviral Res. (2009) 83:90–3. doi: 10.1016/j.antiviral.2009.03.003
15. Esposito S, Molteni CG, Colombo C, Daleno C, Daccò V, Lackenby A, et al. Oseltamivir-induced resistant pandemic A/H1N1 influenza virus in a child with cystic fibrosis and Pseudomonas aeruginosa infection. J Clin Virol. (2010) 48:62–5. doi: 10.1016/j.jcv.2010.02.019
16. Webster RG, Govorkova EA. Continuing challenges in influenza. Ann N Y Acad Sci. (2014) 1323:115–39. doi: 10.1111/nyas.12462
17. Hurt AC, Hardie K, Wilson NJ, Deng YM, Osbourn M, Gehrig N, et al. Community transmission of oseltamivir-resistant A(H1N1)pdm09 influenza. N Engl J Med. (2011) 365:2541–2. doi: 10.1056/NEJMc1111078
18. McKimm-Breschkin JL. Influenza neuraminidase inhibitors: antiviral action and mechanisms of resistance. Influenza Other Respir Viruses. (2013) 7 (Suppl 1):25–36. doi: 10.1111/irv.12047
19. Writing Committee of the WHO Consultation on Clinical Aspects of Pandemic (H1N1) 2009 Influenza Bautista E, Chotpitayasunondh T, Gao Z, Harper SA, Shaw M, et al. Clinical aspects of pandemic 2009 influenza A (H1N1) virus infection. N Engl J Med. (2010) 362:1708–19. doi: 10.1056/NEJMra1000449
20. Fraaij PL, Heikkinen T. Seasonal influenza: the burden of disease in children. Vaccine. (2011) 29:7524–8. doi: 10.1016/j.vaccine.2011.08.010
21. Reece PA. Neuraminidase inhibitor resistance in influenza viruses. J Med Virol. (2007) 79:1577–86. doi: 10.1002/jmv.20951
22. Esposito S, Principi N. Oseltamivir for influenza infection in children: risks and benefits. Expert Rev Respir Med. (2016) 10:79–87. doi: 10.1586/17476348.2016.1126182
23. Oboho IK, Reed C, Gargiullo P, Leon M, Aragon D, Meek J, et al. Benefit of early initiation of influenza antiviral treatment to pregnant women hospitalized with laboratory-confirmed influenza. J Infect Dis. (2016) 214:507–15. doi: 10.1093/infdis/jiw033
24. Jefferson T, Jones MA, Doshi P, Del Mar CB, Hama R, Thompson MJ, et al. Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children. Cochrane Database Syst Rev. (2014) 4:CD008965. doi: 10.1002/14651858.CD008965.pub4
25. Dobson J, Whitley RJ, Pocock S, Monto AS. Oseltamivir treatment for influenza in adults: a meta-analysis of randomised controlled trials. Lancet. (2015) 385:1729–37. doi: 10.1016/S0140-6736(14)62449-1
26. Parra-Rojas C, Nguyen VK, Hernandez-Mejia G, Hernandez-Vargas EA. Neuraminidase inhibitors in influenza treatment and prevention. Is it time to call it a day? Viruses. (2018) 10:E454. doi: 10.3390/v10090454
27. Kmietowicz Z. WHO downgrades oseltamivir on drugs list after reviewing evidence. BMJ. (2017) 357:j2841. doi: 10.1136/bmj.j2841
28. Doll MK, Winters N, Boikos C, Kraicer-Melamed H, Gore G, Quach C. Safety and effectiveness of neuraminidase inhibitors for influenza treatment, prophylaxis, and outbreak control: a systematic review of systematic reviews and/or meta-analyses. J Antimicrob Chemother. (2017) 72:2990–3007. doi: 10.1093/jac/dkx271
29. Muthuri SG, Venkatesan S, Myles PR, Leonardi-Bee J, Al Khuwaitir TS, Al Mamun A, et al. Effectiveness of neuraminidase inhibitors in reducing mortality in patients admitted to hospital with influenza A H1N1pdm09 virus infection: a meta-analysis of individual participant data. Lancet Resp Med. (2014) 2:395–404. doi: 10.1016/S2213-2600(14)70041-4
30. European Center for Disease Prevention and Control. Expert Opinion on Neuraminidase Inhibitors for the Prevention and Treatment of Influenza. Review of Recent Systematic Reviews and Meta-Analyses. Available online at: https://ecdc.europa.eu/sites/portal/files/documents/Scientific-advice-neuraminidase-inhibitors-2017.pdf (accessed January 23, 2019).
31. Wang K, Shun-Shin M, Gill P, Perera R, Harnden A. Neuraminidase inhibitors for preventing and treating influenza in children (published trials only). Cochrane Database Syst Rev. (2012) 4:CD002744. doi: 10.1002/14651858.CD002744.pub4
32. Muthuri SG, Myles PR, Venkatesan S, Leonardi-Bee J, Nguyen-Van-Tam JS. Impact of neuraminidase inhibitor treatment on outcomes of public health importance during the 2009-2010 influenza A(H1N1) pandemic: a systematic review and meta-analysis in hospitalized patients. J Infect Dis. (2013) 207:553–63. doi: 10.1093/infdis/jis726
33. Higashiguchi M, Matsumoto T, Fujii T. A meta-analysis of laninamivir octanoate for treatment and prophylaxis of influenza. Antivir Ther. (2018) 23:157–65. doi: 10.3851/IMP3189
34. Wester A, Shetty AK. Peramivir injection in the treatment of acute influenza: a review of the literature. Infect Drug Resist. (2016) 9:201–14. doi: 10.2147/IDR.S86460
35. Davidson S. Treating Influenza Infection, from now and into the future. Front Immunol. (2018) 9:1946. doi: 10.3389/fimmu.2018.01946
36. Roche, Announces FDA Approval of Xofluza (baloxavir marboxil) for Influenza,. Available online at: https://www.roche.com/media/releases/med-cor-2018-10-24.htm. (accessed March 27, 2019).
37. Tomassini J, Selnick H, Davies ME, Armstrong ME, Baldwin J, Bourgeois M, et al. Inhibition of cap (m7GpppXm)-dependent endonuclease of influenza virus by 4-substituted 2,4-dioxobutanoic acid compounds. Antimicrob Agents Chemother. (1994) 38:2827–37. doi: 10.1128/AAC.38.12.2827
38. Shtyrya YA, Mochalova LV, Bovin NV. Influenza virus neuraminidase: structure and function. Acta Naturae. (2009) 1:26–32.
39. Noshi T, Kitano M, Taniguchi K, Yamamoto A, Omoto S, Baba K, et al. In vitro characterization of baloxavir acid, a first-in-class cap-dependent endonuclease inhibitor of the influenza virus polymerase PA subunit. Antiviral Res. (2018) 160:109–17. doi: 10.1016/j.antiviral.2018.10.008
40. Koshimichi H, Ishibashi T, Kawaguchi N, Sato C, Kawasaki A, Wajima T. Safety, tolerability, and pharmacokinetics of the novel anti-influenza agent baloxavir marboxil in healthy adults: phase I study findings. Clin Drug Investig. (2018) 38:1189–96. doi: 10.1007/s40261-018-0710-9
41. Hayden FG, Sugaya N, Hirotsu N, Lee N, de Jong MD, Hurt AC, et al. Baloxavir marboxil for uncomplicated influenza in adults and adolescents. N Engl J Med. (2018) 379:913–23. doi: 10.1056/NEJMoa1716197
42. Yang T. Baloxavir marboxil: the first cap-dependent endonuclease inhibitor for the treatment of influenza. Ann Pharmacother. (2019) 53:754–9. doi: 10.1177/1060028019826565
43. Gubareva LV, Mishin VP, Patel MC, Chesnokov A, Nguyen HT, De La Cruz J, et al. Assessing baloxavir susceptibility of influenza viruses circulating in the United States during the 2016/17 and 2017/18 seasons. Euro Surveill. (2019) 24:1800666. doi: 10.2807/1560-7917.ES.2019.24.3.1800666
44. Omoto S, Speranzini V, Hashimoto T, Noshi T, Yamaguchi H, Kawai M, et al. Characterization of influenza virus variants induced by treatment with the endonuclease inhibitor baloxavir marboxil. Sci Rep. (2018) 8:9633. doi: 10.1038/s41598-018-27890-4
45. Takashita E, Kawakami C, Morita H, Ogawa R, Fujisaki S, Shirakura M, et al. Detection of influenza A(H3N2) viruses exhibiting reduced susceptibility to the novel cap-dependent endonuclease inhibitor baloxavir in Japan, December 2018. Euro Surveill. (2019) 24:1800698. doi: 10.2807/1560-7917.ES.2019.24.3.1800698
46. Furuta Y, Komeno T, Nakamura T. Favipiravir (T-705), a broad spectrum inhibitor of viral RNA polymerase. Proc Jpn Acad Ser B Phys Biol Sci. (2017) 93:449–63. doi: 10.2183/pjab.93.027
47. Furuta Y, Gowen BB, Takahashi K, Shiraki K, Smee DF, Barnard DL. Favipiravir (T-705), a novel viral RNA polymerase inhibitor. Antiviral Res. (2013) 100:446–54. doi: 10.1016/j.antiviral.2013.09.015
48. Kiso M, Mitamura K, Sakai-Tagawa Y, Shiraishi K, Kawakami C, Kimura K, et al. Resistant influenza A viruses in children treated with oseltamivir: descriptive study. Lancet. (2004) 364:759–65. doi: 10.1016/S0140-6736(04)16934-1
49. Stephenson I, Democratis J, Lackenby A, McNally T, Smith J, Pareek M, et al. Neuraminidase inhibitor resistance after oseltamivir treatment of acute influenza A and B in children. Clin Infect Dis. (2009) 48:389–96. doi: 10.1086/596311
50. Sleeman K, Mishin VP, Deyde VM, Furuta Y, Klimov AI, Gubareva LV. In vitro antiviral activity of favipiravir (T-705) against drug-resistant influenza and 2009 A(H1N1) viruses. Antimicrob Agents Chemother. (2010) 54:2517–24. doi: 10.1128/AAC.01739-09
51. Sidwell RW, Barnard DL, Day CW, Smee DF, Bailey KW, Wong MH, et al. Efficacy of orally administered T-705 on lethal avian influenza A (H5N1) virus infections in mice. Antimicrob Agents Chemother. (2007) 51:845–51. doi: 10.1128/AAC.01051-06
52. .Marathe BM, Wong SS, Vogel P, Garcia-Alcalde F, Webster RG, Webby RJ, et al. Combinations of oseltamivir and T-705 extend the treatment window for highly pathogenic influenza A(H5N1) virus infection in mice. Sci Rep. (2016) 6:26742. doi: 10.1038/srep26742
53. Nagata T, Lefor AK, Hasegawa M, Ishii M. Favipiravir: a new medication for the Ebola virus disease pandemic. Disaster Med Public Health Prep. (2015) 9: 79-81. doi: 10.1017/dmp.2014.151
54. Furuta Y, Takahashi K, Shiraki K, Sakamoto K, Smee DF, Barnard DL, et al. T-705 (favipiravir) and related compounds: novel broad-spectrum inhibitors of RNA viral infections. Antiviral Res. (2009) 82:95–102. doi: 10.1016/j.antiviral.2009.02.198
55. Delang L, Abdelnabi R, Neyts J. Favipiravir as a potential countermeasure against neglected and emerging RNA viruses. Antiviral Res. (2018) 153:85–94. doi: 10.1016/j.antiviral.2018.03.003
56. Clark MP, Ledeboer MW, Davies I, Byrn RA, Jones SM, Perola E, et al. Discovery of a novel, first-in-class, orally bioavailable azaindole inhibitor (VX-787) of influenza PB2. J Med Chem. (2014) 57:6668–78. doi: 10.1021/jm5007275
57. Smee DF, Barnard DL, Jones SM. Activities of JNJ63623872 and oseltamivir against influenza A H1N1pdm and H3N2 virus infections in mice. Antiviral Res. (2016) 136:45–50. doi: 10.1016/j.antiviral.2016.10.009
58. Trevejo JM, Asmal M, Vingerhoets J, Polo R, Robertson S, Jiang Y, et al. Pimodivir treatment in adult volunteers experimentally inoculated with live influenza virus: a Phase IIa, randomized, double-blind, placebo-controlled study. Antivir Ther. (2018) 23:335–44. doi: 10.3851/IMP3212
59. Finberg RW, Lanno R, Anderson D, Fleischhackl R, van Duijnhoven W, Kauffman RS, et al. Phase 2b Study of pimodivir (JNJ-63623872) as monotherapy or in combination with oseltamivir for treatment of acute uncomplicated seasonal iInfluenza A: TOPAZ Trial. J Infect Dis. (2018) 219:1026–34. doi: 10.1093/infdis/jiy547
60. Medina RA, Stertz S, Manicassamy B, Zimmermann P, Sun X, Albrecht RA, et al. Glycosylations in the globular head of the hemagglutinin protein modulate the virulence and antigenic properties of the H1N1 influenza viruses. Sci Transl Med. (2013) 5:187ra170. doi: 10.1126/scitranslmed.3005996
61. Corti D, Voss J, Gamblin SJ, Codoni G, Macagno A, Jarrossay D, et al. A neutralizing antibody selected from plasma cells that binds to group 1 and group 2 influenza A hemagglutinins. Science. (2011) 333:850–6. doi: 10.1126/science.1205669
62. Dilillo DJ, Tan GS, Palese P, Ravetch JV. Broadly neutralizing hemagglutinin stalk-specific antibodies require FcgammaR interactions for protection against influenza virus in vivo. Nat Med. (2014) 20:143–51. doi: 10.1038/nm.3443
63. Dilillo DJ, Palese P, Wilson PC, Ravetch JV. Broadly neutralizing antiinfluenza antibodies require Fc receptor engagement for in vivo protection. J Clin Invest. (2016) 126:605–10. doi: 10.1172/JCI84428
64. McBride JM, Lim JJ, Burgess T, Deng R, Derby MA, Maia M, et al. Phase 2 randomized trial of the safety and efficacy of MHAA4549A, a broadly neutralizing monoclonal antibody, in a human influenza A virus challenge model. Antimicrob Agents Chemother. (2017) 61:e01154–17. doi: 10.1128/AAC.01154-17
65. Ali O, Takas T, Andrew BS, Nyborg C, Kathryn D, Jensen N. A Phase 2a study to evaluate the safety of MEDI8852 in outpatient adults with acute, uncomplicated influenza A. Open Forum Infect Dis. (2017) 4 (Suppl. 1):S519. doi: 10.1093/ofid/ofx163.1352
66. Hershberger E, Sloan S, Narayan K, Hay CA, Smith P, Engler F, et al. Safety and efficacy of monoclonal antibody VIS410 in adults with uncomplicated influenza A infection: results from a randomized, double-blind, phase-2, placebo-controlled study. EBioMedicine. (2019). 40:574–82. doi: 10.1016/j.ebiom.2018.12.051
67. Gupta P, Kamath AV, Park S, Chiu H, Lutman J, Maia M, et al. Preclinical pharmacokinetics of MHAA4549A, a human monoclonal antibody to influenza A virus, and the prediction of its efficacious clinical dose for the treatment of patients hospitalized with influenza A. MAbs. (2016) 8:991–7. doi: 10.1080/19420862.2016.1167294
68. Kallewaard NL, Corti D, Collins PJ, Neu U, Mcauliffe JM, Benjamin E, et al. Structure and function analysis of an antibody recognizing all influenza A subtypes. Cell. (2016) 166:596–608. doi: 10.1016/j.cell.2016.05.073
Keywords: antiviral drugs, baloxavir marboxil, favipiravir, influenza, monoclonal antibodies, neuraminidase inhibitors
Citation: Principi N, Camilloni B, Alunno A, Polinori I, Argentiero A and Esposito S (2019) Drugs for Influenza Treatment: Is There Significant News? Front. Med. 6:109. doi: 10.3389/fmed.2019.00109
Received: 14 February 2019; Accepted: 02 May 2019;
Published: 28 May 2019.
Edited by:
Ville Peltola, Turku University Hospital, FinlandReviewed by:
Elena A. Govorkova, St. Jude Children's Research Hospital, United StatesCopyright © 2019 Principi, Camilloni, Alunno, Polinori, Argentiero and Esposito. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susanna Esposito, c3VzYW5uYS5lc3Bvc2l0b0B1bmltaS5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.