
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Mater. , 11 May 2022
Sec. Biomaterials
Volume 9 - 2022 | https://doi.org/10.3389/fmats.2022.833427
 Mónica Fernández-Mafé1*
Mónica Fernández-Mafé1* Andrea Armengol-Olivares2Lucía Miralles-Jordá2Ángel Vicente-Escuder3
Andrea Armengol-Olivares2Lucía Miralles-Jordá2Ángel Vicente-Escuder3 Marcelino Pérez-Bermejo4
Marcelino Pérez-Bermejo4 Javier Narciso5,6Antonio Pallarés-Sabater7
Javier Narciso5,6Antonio Pallarés-Sabater7Silver diamine fluoride (SDF) has demonstrated its clinical success for years in the arrest of caries lesions; however, the influence it could have on the success of restorations after its application still remains unknown. The purpose of this research was to study the relationship between the use of SDF and the adhesive strength of the materials used in restorations made with glass ionomers and composite resin, as well as with different adhesive systems. A sample consisting of 240 teeth divided into eight groups with 30 teeth in each of them (n = 30) was used. In these groups, the use of restoration with composite resin and glass ionomer was compared using different adhesive systems, with and without prior application of SDF. Notable differences in adherence were observed among the different groups depending on the filling material. There is also a significant effect of tooth type on adhesion. We can conclude that there is a relationship between the use of SDF and the adhesion between the tooth and the restorative materials analyzed.
Resin restoration was introduced around the middle of the 20th century as a material for esthetic restoration (Leinfelder, 1988; Minguez et al., 2003). These resins are classified according to the size of the filler, which affects the polishability and esthetics, depth of polymerization, shrinkage that occurred during polymerization, and physical properties. Hybrid resins combine a mixture of particle sizes that improve both strength and esthetics (Burgess et al., 2002). The smaller size of the filler particles allows for greater polishability and esthetics, while a larger size provides greater strength and toughness. Thus, the more fluid resins have a lower volumetric filling than the hybrid resins (Pallav et al., 1989).
Materials used in dentistry based on glass ionomers have been used since 1970, as restorative material, cement, or pulp caps (Wilson and Kent, 1972). Initially, it was a difficult-to-handle material, with poor wear resistance and brittle. Advances in formulation allowed for improved properties, including the combination of resin-modified glass ionomers. This combination allowed us to improve the properties, improving the ease of handling of the material, the decrease in the setting time, the increase in strength, and the greater resistance (Mitra and Kedrowski, 1994). Generally, all materials with glass ionomers have properties that make them advantageous in pediatric dentistry, such as chemical bonding to the enamel and dentin, thermal expansion similar to that of the tooth, biocompatibility, absorption and release of fluoride, reduction of fluoride, and moisture sensitivity compared with resins (Author Anonymous, 2018). Glass ionomers can act as a reservoir for fluoride which can come from the use of toothpaste, rinses, as well as topical fluoride applications. This protection is a key advantage in pediatric dentistry, for patients with a high risk of caries (Donly et al., 1995; Donly and Nelson, 1997; Forsten, 1998; Author Anonymous, 2018).
Total embossing adhesive systems require a prior phase of conditioning the fabric with 37% orthophosphoric acid, which provides an irregular and porous surface that allows the infiltration of polymerizable resin monomers (Mithiborwala et al., 2012). On the other hand, self-etching systems composed of acid monomers do not require washing and act by conditioning, demineralizing, and infiltrating the enamel and dentin simultaneously (Pegado et al., 2010).
The use of adhesives in the enamel and dentin in the field of pediatric dentistry has increased considerably over the years. Mainly its use is justified to allow a more durable union of different restorative materials (García-Godoy and Donly, 2015). The selection of the most adequate material for coronary obturation in pediatric dentistry is a complex issue that must take into account many factors (Naulin-Ifi, 2011). Glass ionomer cement is one of the most used materials as it is a cariopreventive material, which makes it especially recommended for children at high risk of cavities since it has a special ability to release fluoride over a long period of time, which helps tooth remineralization and does not require very strict isolation as in composite resins (Wilde et al., 2006; American Academy of Pediatric Dentistry, 2008; Muller-Bolla, 2014). Its main disadvantage is low resistance, which is why it is not recommended as a long-term restorative material in permanent dentition (Tassery et al., 2006; American Academy of Pediatric Dentistry, 2008).
Resin-modified glass ionomer cement benefits from shorter bonding time and lower solubility than glass ionomer cement, improves resistance to fracture and abrasion, and maintains the biocompatibility and hydrodynamics of fluoride ions, preserving their physicochemical adherence to the tooth structure (Anderson-Wenckert et al., 2002; Roberts et al., 2005; Savin et al., 2016). Certain requirements must be considered for the successful use of resin composites, including the possibility of isolation of the cavity, the size of the lesion, and the need for periodic reviews. They are well suited for minimally invasive dentistry, yet extremely sensitive to any technical intervention, so they should only be used when adequate isolation can be achieved (Stoleriu et al., 2013).
Stoleriu et al. (2013) and Bansal et al. (2019) proposed that to achieve long-lasting clinical success, composite resin restorations should have as smooth a surface as possible to avoid the accumulation of bacterial plaque or extrinsic dyes, although subsequent studies have shown the impossibility of achieving a totally smooth surface because of the different coefficients of hardness and resistance to wear of both the organic and the inorganic matrixes (Mei et al., 2013; Andrian et al., 2017).
Silver diamine fluoride (SDF) has a positive effect in preventing the formation of new caries lesions and is able to effectively stop the caries process, with an 81% success rate in stopping caries in the active caries lesions (Gao et al., 2016; González Alarcón and Bakari Ndjidda, 2018; Horst, 2018). The clinical effects shown are the cariostatic effect on the temporary and permanent dentition, the reduction of the progression of the caries lesion, hardening of the carious dentin, the preventive effect on the occlusal and interproximal surfaces, and decreased tooth sensitivity (Zhao et al., 2018).
Several authors (Chu et al., 2002; Zhao et al., 2018) have justified its use by finding evidence of its efficacy in active caries lesions and in the prevention of caries lesions. Some authors stated that the topical application of SDF did not interfere (either beneficially or detrimentally) with the subsequent adhesion of the restorative materials, either with composite resin or with glass ionomer cement; however, there is no consensus on this (Yamaga et al., 1972; Rosenblatt et al., 2009; Fung et al., 2013; Author Anonymous, 2018; Juneja et al., 2019). Later studies by Australian authors introduced potassium iodide (KI) to minimize and mask staining, obtaining similar long-term results in the effect of this treatment, as well as its acceptable interaction with various restorative materials (Knight et al., 2006; Knight et al., 2009; Craig et al., 2012). Knight et al. (2006) analyzed the influence of SDF/KI and adhesion between dentin and glass ionomer cement, and suggested that as long as there is a water wash of the SDF-treated surface, it will not influence the adhesive strength.
The exact mechanism of the SDF is still unknown. Although the interaction between SDF and the tooth has not been clearly demonstrated, some authors hypothesize that mainly fluorine ions react with the demineralized tooth surface, while silver ions, as with other heavy metals, cause its antimicrobial actions (Fung et al., 2013; Author Anonymous, 2018; Juneja et al., 2019). It has been observed that during the topical application of SDF, it reacts with hydroxyapatite minerals [Ca10 (PO4) 6 (OH) 2] on the tooth surface, and with this reaction, two compounds are mainly generated: calcium fluoride (CaF2) and phosphate of silver (Ag3PO4), by-products responsible for the arrest of caries, and the hardening of the dentin structure, in addition to producing an antimicrobial action against multiple types of cariogenic microbial flora (Yamaga et al., 1972; Wu et al., 2007; Chu and Lo, 2008; Chu et al., 2012; Mei et al., 2013).
Studies that have analyzed silver diamine fluoride differ widely in terms of objectives, hypotheses, methodologies, experimental conditions, model systems, and conclusions. There is evidence of the effectiveness of caries arrest by applying SDF at 38% (Mei et al., 2013; Gao et al., 2016; Horst, 2018). However, significant research has been continued on the recurrence of these unfilled lesions once the first six months have elapsed, since they continue to be patients at high risk of caries. Authors such as Crystal and Niederman (2016) suggested the alternative of using the glass ionomer cement as a filling material after the application of SDF, thereby further reducing the risk of caries recurrence and increasing dental esthetics.
The working hypothesis was that SDF has an effect on the adhesion between the different materials studied and the tooth. For this reason, this study focuses on knowing if the SDF influences the adhesion of the main reconstruction materials in pediatric dentistry (both with glass ionomer and with resins) since one of the alternatives in those candidate patients could be to stop caries with the application of SDF in the first line of action. Next, the second line of action would be the prevention of the reactivation of the said caries by sealing the cavity, either with glass ionomer cement or with resins. In this way, it would also facilitate the improvement of hygiene, thereby helping to prevent new caries lesions and reduce the risk of cavities.
On the other hand, with regard to candidate patients, those patients who cannot tolerate standard treatment for medical, psychological, or age reasons could be included. Similarly, patients with multiple caries lesions could be included, who at the moment cannot perform all the treatments in a short period of time (for medical, economic, psychological, or age reasons), thus slowing down caries lesions and cavities until the appropriate standard treatments can be performed.
Two hundred forty (240) extracted permanent human teeth were selected, with a total of 188 M (78.3%) and 52 premolars (21.7%). The proportion of premolars in each of the groups is similar, ranging between 20 and 30%. Homogeneity is confirmed by the chi2 association test (p = 0.980).
The teeth were divided into eight groups of 30 cases each (n = 30). Different combinations of pretreatment, bonding systems, and restorative materials were used in each of the groups (Table 1).
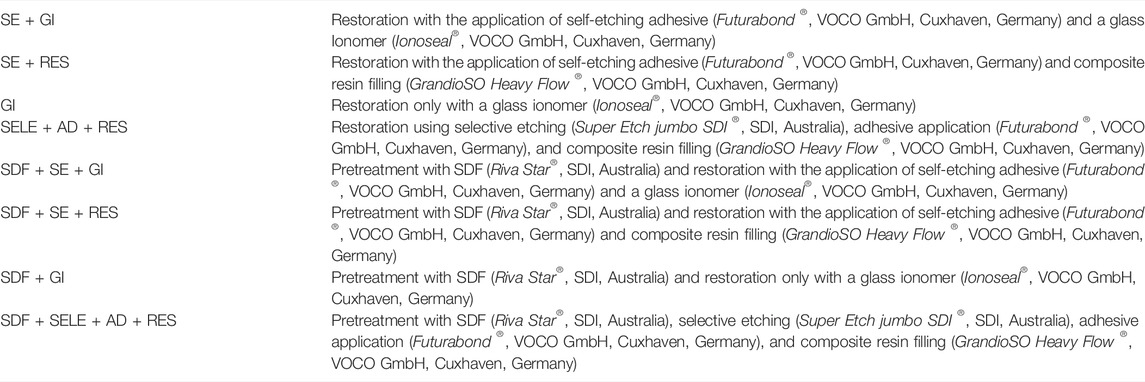
TABLE 1. Distribution of the sample in the different groups according to the use or non-use of pretreatment, and the use of the different adhesive systems and materials. In addition, the materials, commercial brands used in the study, and the country of manufacture are shown.
The inclusion criteria used in the sample were teeth without previous treatments extracted for periodontal and/or orthodontic reasons. Similarly, only premolars and molars were used. All teeth remained in a 0.9% sodium chloride container until their use in this study so as not to lose hydration.
Teeth with conservative treatments such as restorations, pulp treatments, or prostheses, as well as worn teeth or teeth with suspected cleft diagnosis, were excluded.
During the entire sample collection period, the teeth were immersed in a 0.9% sodium chloride solution to maintain hydration. This solution was changed routinely until the time of making the preparations. Once the entire sample had been collected, the selected teeth were immersed in 5% sodium hypochlorite for 10 min. Subsequently, they were individually grounded in plaster, numbered, and randomly distributed in the different groups.
All teeth were cleaned with ultrasound and/or curettes, thus removing the remains of tartar. In a similar manner, all the faces of the teeth were cleaned with a prophylaxis brush using the contra-angle to remove any traces of biofilm or dirt.
In clinical practice, class V cavities were performed in all of them, with an approximately similar depth and extension of 2 and 5 mm, respectively (Puckett et al., 1995). All the margins were beveled so that the cavities were expulsive and the adhesion could be adequately assessed.
For the application of different materials, the manufacturer’s recommendations were followed according to the different groups during the application of self-etching adhesive. In the case of the glass ionomer cement and the composite resin, it was applied to the cavity and polymerized. In those groups where a previous selective etching was carried out, 37% orthophosphoric acid was applied to condition the enamel. Then, it was washed with water, and the surface was dried. In those cases where SDF pretreatment was used, it was carefully applied throughout the entire cavity of the Riva Star® (silver diamine fluoride) silver capsule solution. Immediately afterward, liberal application of the Riva Star® green capsule solution (potassium iodide) was carried out until the white cream became clear. Subsequently, profuse washing with water to remove the remains of material and drying the cavity was performed. The materials used are reflected in Table 1.
In all the teeth and during the last step (application of the composite resin or the glass ionomer cement), the pull button was inserted before the polymerization of the glass ionomer cement or the composite resin.
The steps performed after making the class V cavity are as follows:
For the homogenous application of the Futurabond ® self-etching adhesive in the cavity for 20 s, air was applied to remove the solvents for 5 s, and polymerization was carried out for 10 s. The cavity was then filled with glass ionomer (Ionoseal®) and polymerized for 20 s.
For the homogenous application of the Futurabond ® self-etching adhesive in the cavity for 20 s, air was applied to remove the solvents for 5 s, and polymerization was carried out for 10 s. The cavity was then filled with GrandioSO Heavy Flow ® fluid resin and polymerized for 20 s.
No prior conditioning or pretreatment was performed. Only the cavity was filled with glass ionomer (Ionoseal®) and polymerized for 20 s.
First, 37% orthophosphoric acid was applied for 15–20 s to condition the enamel. It was then washed with water for 15 s, and the surface was dried. Next, Futurabond ® self-etching adhesive was applied homogenously in the cavity for 20 s, with subsequent application of air to remove solvents for 5 s and polymerization for 10 s. Finally, it was filled with GrandioSO Heavy Flow ® fluid resin and polymerized for 20 s.
Careful application along the entire cavity of the Riva Star® silver capsule solution (diamine fluoride) was carried out. Immediately afterward, copious application of the Riva Star® green capsule solution (potassium iodide) was performed until the white cream became transparent. Then, profuse washing with water to remove the remains of the material and to drying the cavity for 20 s was carried out. Next, the Futurabond ® self-etching adhesive was applied homogenously in the cavity for 20 s; air was applied to remove the solvents for 5 s and polymerization for 10 s. To fill the cavity, a glass ionomer (Ionoseal ®) was applied and polymerized for 20 s.
Careful application along the entire cavity of the Riva Star® silver capsule solution (diamine fluoride) was performed. Immediately afterward, the copious application of the Riva Star® green capsule solution (potassium iodide) was carried out until the white cream became transparent. Then, profuse washing with water was performed to remove the remains of the material and to drying the cavity for 20 s. Next, the Futurabond ® self-etching adhesive was applied homogenously in the cavity for 20 s; air was applied to remove the solvents for 5 s, and polymerization was carried out for 10 s. Finally, it was filled with GrandioSO Heavy Flow ® fluid resin and polymerized for 20 s.
Careful application along the entire cavity of the Riva Star® silver capsule solution (diamine fluoride) was carried out. Immediately afterward, copious application of the Riva Star® green capsule solution (potassium iodide) was performed until the white cream became transparent. Then, profuse washing with water was done to remove the remains of the material and to drying the cavity for 20 s. The cavity was then filled with a glass ionomer (Ionoseal®) and polymerized for 20 s.
Careful application along the entire cavity of the Riva Star® silver capsule solution (diamine fluoride) was performed. Immediately afterward, copious application of the Riva Star® green capsule solution (potassium iodide) was carried out until the white cream became transparent. Then, profuse washing with water was carried out to remove the remains of the material and to drying the cavity for 20 s. First, 37% orthophosphoric acid was applied for 15–20 s to condition the enamel. Then, it was washed with water for 15 s, and the surface was dried. Next, the Futurabond® self-etching adhesive was applied homogeneously in the cavity for 20 s; air was applied to remove the solvents for 5 s, and polymerization was performed for 10 s. Finally, it was sealed with GrandioSO Heavy Flow ® fluid resin and polymerized for 20 s.
Once the entire sample was prepared, a tensile test was carried out using the universal testing machine SHIMADZU Autograph AG-X plus Series ® (Shimadzu, Nakagyo-ku, Kyoto, Japan). A continuous tensile force of 1 mm/s was applied to each of the tooth, assessing the maximum applied force necessary to remove the restoration and the maximum displacement that occurred in each of them.
After the restoration process, a tensile test was performed on a universal testing machine, and the separation force of the restored fragment was obtained (Figure 1). This force or strength, measured in Newton, is the primary response variable of the study. In addition, the displacement of the sample was recorded in millimeters (mm). One of the graphs obtained in the test where the force–displacement curve can be observed (Figure 2) is included as an example.

FIGURE 1. Photo of the tensile strength test setup.
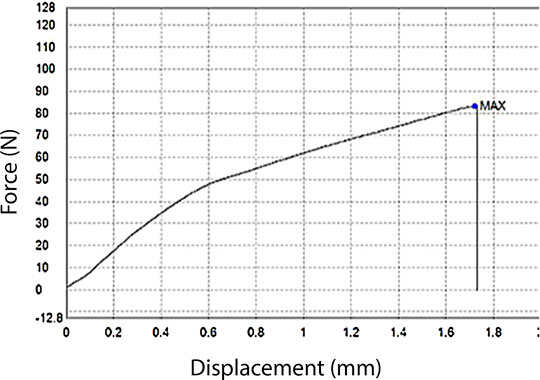
FIGURE 2. Force–displacement curve.
Statistical analysis was performed with the SPSS 15.0 computer program (IBM, Armonk, New York, EE.UU.). The sample size ensures a power of 80% for an average effect size. The reference significance level was 5%. Before the statistical analysis, the Kolmogorov–Smirnov test was applied to check if the variables were normally distributed in the different groups. Levene’s test was used to compare the variances. By means of the chi2 test, the homogeneity of the groups in terms of types of teeth included was verified.
Similarly, the one-way ANOVA model was used to determine if there were statistically significant differences between the strength means of the different groups. For multiple comparisons, the Tamhane T2 test was performed, which is suitable when the variances are unequal. The effect of the tooth type is studied with a two-way model extension.
In Figure 3, different patterns are shown. Both with and without the application of SDF, the differences by the groups are notable, appreciating the low resistance offered by the glass ionomer cement, without pretreatment or adhesion system, compared with the rest. On the other hand, the application of SDF slightly raises the distributions (improves adhesion moderately). Furthermore, it tends to increase the variability within each group.
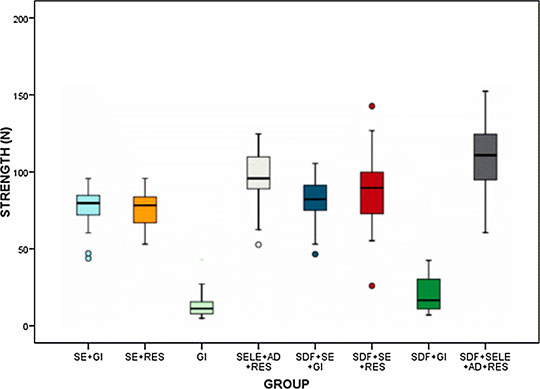
FIGURE 3. Distributions of force values of the different groups. The sample names were represented as follows: SE + GI: restoration with the application of self-etching adhesive and glass ionomer, SE + RES: restoration with the application of self-etching adhesive and composite resin, GI: restoration only with a glass ionomer, SELE + AD + RES: restoration using selective etching, adhesive application, and composite resin filling, SDF + SE + GI: pretreatment with SDF and restoration with the application of self-etching adhesive and a glass ionomer, SDF + SE + RES: pretreatment with SDF and restoration with application of self-etching adhesive and composite resin, SDF + GI: pretreatment with SDF and restoration only with glass ionomer, SDF + SELE + AD + RES: pretreatment with SDF, selective etching, adhesive application, and composite resin filling.
The Kolmogorov test allowed accepting the adjustment to the normal distribution in all groups, except the glass ionomer cement without pretreatment or selective etching. However, the homogeneity of the variances (p = 0.00087, Levene) could not be accepted. Thus, the ANOVA model was applied, controlling the problem and using a specific multiple comparison test for this type of situation, such as Tamhane’s T2 (Table 2), finding significant differences in the mean strength of the eight groups (p = 0.000723).
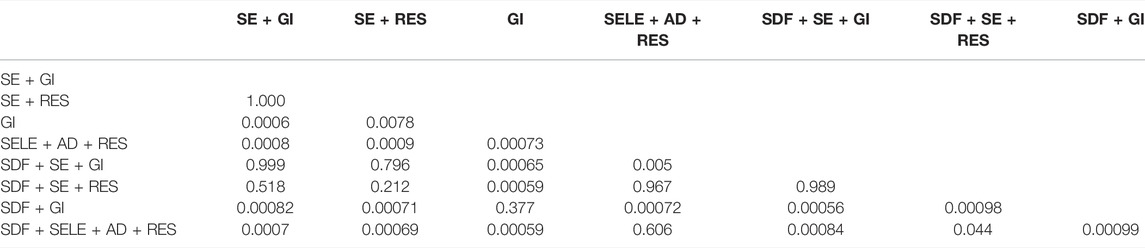
TABLE 2. Comparison of mean strength according to group: Tamhane post hoc test results. The gray area is not shown for symmetry.
The application of SDF did not significantly modify the adherence of the groups where restoration was applied with the application of self-etching adhesive and glass ionomer cement, restoration with application of self-etching adhesive and composite resin filling, restoration only with glass ionomer cement, and restoration using selective etching, adhesive application, and composite resin filling. In the SELE + AD + RES group (restoration using selective etching, adhesive application, and composite resin filling), where SDF was not applied, a detachment force was observed to be significantly higher than that in any of the other groups. The groups with the application of self-etching adhesive were similar to each other (p = 1.000) and significantly stronger than the ionomer alone. On the other hand, in the groups where SDF was applied, the results were quite similar. The SELE + AD + RES group was superior in terms of medium adhesion, equaled only with the SE + RES group (restoration with the application of self-etching adhesive and composite resin). The SE + GI (restoration with the application of self-etching adhesive and glass ionomer cement) and SE + RES groups were similar to each other (p = 0.989) and significantly stronger than the glass ionomer cement alone.
The data indicated that there is a significant tooth type effect on strength (p = 0.027). On average and without differentiating by groups, molars offered significantly higher strength than premolars (Figure 4).
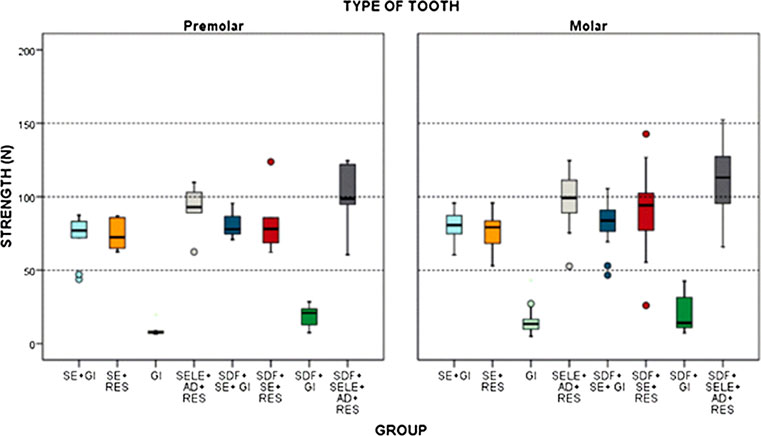
FIGURE 4. Strength (N) according to the group and tooth type. The sample names were represented as follows: SE + GI: restoration with the application of self-etching adhesive and a glass ionomer, SE + RES: restoration with the application of self-etching adhesive and composite resin, GI: restoration only with a glass ionomer, SELE + AD + RES: restoration using selective etching, adhesive application, and composite resin filling, SDF + SE + GI: pretreatment with SDF and restoration with the application of self-etching adhesive and a glass ionomer, SDF + SE + RES: pretreatment with SDF and restoration with the application of self-etching adhesive and composite resin, SDF + GI: pretreatment with SDF and restoration only with a glass ionomer, SDF + SELE + AD + RES: pretreatment with SDF, selective etching, adhesive application, and composite resin filling.
The model also showed that this “superiority” of molars over premolars should be admitted as similar in all the groups evaluated; that is, there is no interaction effect (p = 0.958). The differences between groups (p 0.00073) could be extrapolated to any of the two tooth types (p = 0.958).
In the previous models, the eight groups were considered independent combinations of SDF (yes/no) and the adhesive system. The effect of both variables was evaluated separately to know if one or the other variable is to a greater or lesser extent responsible for the variability of the strength measurements.
When comparing the mean strength of the four systems (with 60 teeth each), significant differences were found (p = 0.00055), showing that SDF had an effect on the measured mean strength (p = 0.00078).
From a general point of view, the bonding system is the most important source of strength variability, followed by SDF and, last, the tooth type. No significant interactions were found between these factors according to our study results.
To know the relationship between the different materials and the resistance, a selection of samples has been made to carry out a fractographic analysis. The groups with the greatest resistance (G8) and with the least resistance (G3) have been analyzed. As can be seen in the G3 sample, the cavity is completely clean with no traces of restorative material. Some cracks are observed, but the highlight is that the beach marks produced by the materials used for the preparation of the cavity continue to be observed. This shows that there is no rest of the material used (Figure 5).
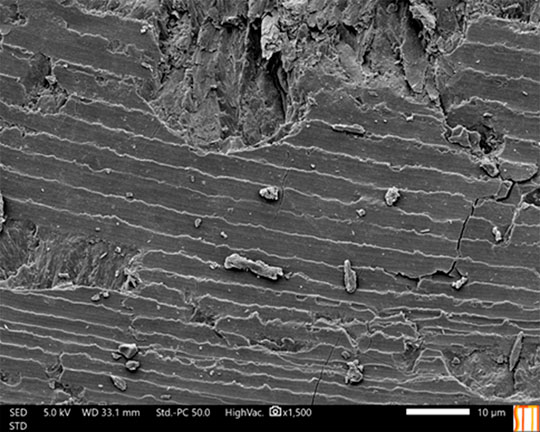
FIGURE 5. Image extracted from the fractographic analysis of the G3 sample.
Unlike the G3 sample, in the G8 sample, it can be seen that the fracture has been through the restoration material, which shows that there is great adhesion with the tooth (Figure 6).
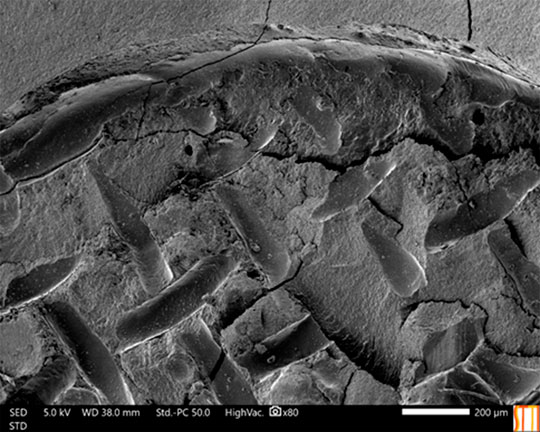
FIGURE 6. Image extracted from the fractographic analysis of the G8 sample.
The study has been completed by a superficial analysis using the EDX and XPS techniques, which simply corroborate the aforementioned ones, since they only detect hydroxyapatite in the G3 sample and the components of the G8 restoration material.
Performing a dental restoration after stopping caries by applying SDF could be a possible solution in pediatric patients or in special patients. It seems promising to incorporate this material in the management of caries lesions together with restorative treatment. In these cases, esthetic restorative materials could be used to restore the caries-derived cavity and thus cover the darkened area caused by SDF (Jiang et al., 2020).
Previous studies differ greatly in terms of methodology. Studies to date have used various bond strength-testing methods, including the tensile bond strength test (TBS), shear bond strength test (SBS), micro-tensile bond strength test (mTBS), and micro-tensile bond strength test (mSBS) (Jiang et al., 2020) or the tensile strength method (Kucukyilmaz et al., 2016), similar to that performed in this study. A meta-analysis carried out in 2020 (Fröhlich et al., 2020) is recommended for future studies to carefully carry out and describe all the methodological parameters involved in carrying out the studies, since in those carried out to date, there is great heterogeneity in the methodology, making it difficult to compare the results.
Whenever SDF is used for the arrest of caries lesions, the possible staining of the enamel or dentin must be taken into account, especially in the marginal zone of restorations or in its application in the anterior sector (Nguyen et al., 2017; Zhao et al., 2017). As an alternative to solve this esthetic problem, it has been proposed to apply a KI solution immediately after the application of SDF to minimize the darkened area. Iodide ions in the KI solution can react with silver ions to form silver iodide which appears as a yellowish precipitate providing enhanced esthetics (Knight et al., 2006).
In some studies, it has been observed that the bonding strength has not been adversely compromised after the application of SDF/KI, provided there is a subsequent rinse with water because without such rinsing, the bonding strength is significantly reduced (Knight et al., 2006; Selvaraj et al., 2016; Gupta et al., 2019; Zhao et al., 2019). However, other authors observed that the application of SDF followed by immediate rinsing with water did not have a significant influence on the bond strength (Quock et al., 2012; Wu et al., 2016; Gupta et al., 2019; Van Duker et al., 2019).
Some of the studies published to date focused their objective on assessing this influence of adherence according to the use of different materials. On the one hand, some studies mainly evaluate adhesive systems with previous etching and self-etching (Selvaraj et al., 2016), using glass ionomer cement restorations (Chu et al., 2012; Wang et al., 2016; Puwanawiroj et al., 2018; Zhao et al., 2019) or evaluating the use of composite resins as a restorative material (Quock et al., 2012; Kucukyilmaz et al., 2016; Wu et al., 2016; Lutgen et al., 2018). In the present study, it was decided to carry out different groups to observe the possible difference between the adhesive system (selective etching and adhesive application, or only self-etching adhesive) and the use of glass ionomer cement and composite resins.
The previously mentioned meta-analysis (Fröhlich et al., 2020) concluded that there is no evidence regarding the possible influence of the previous application of 38% SDF in relation to the bond strength of glass ionomer cement restorations to dentin, although it observed a significant decrease in the bond strength relative to dentin adhesive systems. In the present study, the results showed that the bond strength between the materials used and the dentin without the application of SDF/KI was slightly lower and increased in those groups with the application of SDF/KI. This was reflected in all the groups and globally, both in the different adhesive systems (acid etching—adhesive application and self-etching) and in the different materials (glass ionomer cement and composite resin), while in the restoration with glass ionomer cement, it follows the line of results of different authors who affirm this improvement in the bond strength between the glass ionomer cement and the dentin after the use of SDF.
The SDF is used mainly for the arrest of caries lesions, so it is proposed as a possible future research line to study its possible application in other types of treatments, such as orthodontic and periodontic treatments. It would be interesting to know how its application on smooth surfaces influences the remineralization of the enamel before the cementation of brackets or before the cementation of splints in periodontics.
Based on the results of this study, there is a relationship between the use of SDF and the bond between the tooth and the materials. It can be affirmed that the previous conditioning of the enamel with selective etching had a significant influence. Similarly, a statistically significant improvement was observed by previously applying self-etched adhesive to glass ionomer cement restorations. The application of SDF improved the adhesion between the tooth and the restoration material, being the group SDF + SELE + AD + RES (pretreatment with SDF, selective etching, adhesive application, and composite resin filling), which showed the best results. The most important source of variability in the bond strength of the material was the bonding system, followed by the application or not of SDF and, last, the type of tooth.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Conceptualization: MF and AP. Methodology: MF, AA, LM, AV-E, MP-B, JN, and AP. Validation: MF, AA, LM, and AP. Formal analysis: MF, AV-E, and AP. Investigation: MF, AV-E, JN, and AP. Data curation: MF and AV-E. Writing—original draft preparation: MF and AP. Writing—review and editing: MF, MP-B, and AP. Supervision: AA, LM, MP-B, and AP.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors thank the Catholic University of Valencia San Vicente Mártir for their contribution and help in the payment of the Open Access publication fee under grant number 2021-196-001.
American Academy of Pediatric Dentistry (2008). Comprehensive Review of Pediatric Dentistry [Internet]. Available from: www.cmeinfo.com (Accessed Aug 23, 2016).
Anderson-Wenckert, I. E., van Dijken, J. W., and Hörstedt, P. (2002). Modified Class II Open Sandwich Restorations: Evaluation of Interfacial Adaptation and Influence of Different Restorative Techniques. Eur. J. Oral Sci. 110 (3), 270–275. doi:10.1034/j.1600-0447.2002.11210.x
Andrian, S., Munteanu, B., Tărăboanţă, I., Negraia, D., Nica, P. E., Stoleriu, S., et al. (2017). “Surface Roughness after Finishing and Polishing of a Restorative Nanocomposite Material,” in The 6th IEEE International Conference on E-Health and Bioengineering Conference (EHB), Sinaia, Romania, June 22-24, 2017, 101–104.
Bansal, K., Gupta, S., Nikhil, V., Jaiswal, S., Jain, A., and Aggarwal, N. (2019). Effect of Different Finishing and Polishing Systems on the Surface Roughness of Resin Composite and Enamel: An in vitro Profilometric and Scanning Electron Microscopy Study. Int. J. Appl. Basic Med. Res. 9 (3), 154–158. doi:10.4103/ijabmr.IJABMR_11_19
Burgess, J. O., Walker, R., and Davidson, J. M. (2002). Posterior Resin-Based Composite: Review of the Literature. Pediatr. Dent 24 (5), 465–479.
Chu, C., and Lo, E. (2008). Promoting Caries Arrest in Children with Fluoride : A Review. Oral Heal Prev. Dent 6, 315–322.
Chu, C. H., Lo, E. C. M., and Lin, H. C. (2002). Effectiveness of Silver Diamine Fluoride and Sodium Fluoride Varnish in Arresting Dentin Caries in Chinese Pre-School Children. J. Dental Res. 81 (11), 767–770. doi:10.1177/154405910208101109
Chu, C. H., Mei, L., Seneviratne, C. J., and Lo, E. C. M. (2012). Effects of Silver Diamine Fluoride on Dentine Carious Lesions Induced by Streptococcus Mutans and Actinomyces Naeslundii Biofilms. Int. J. Paediatr. Dent 22 (1), 2–10. doi:10.1111/j.1365-263x.2011.01149.x
Council on Clinical Affairs (2018). Policy on the Use of Silver Diamine Fluoride for Pediatric Dental Patients. Pediatr. Dent 40 (6), 51–54.
Craig, G., Knight, G., and McIntyre, J. (2012). Clinical Evaluation of Diamine Silver Fluoride/Potassium Iodide as a Dentine Desensitizing Agent. A Pilot Study. Aust. Dent J. 57 (3), 308–311. doi:10.1111/j.1834-7819.2012.01700.x
Crystal, Y. O., and Niederman, R. (2016). Silver Diamine Fluoride Treatment Considerations in Children's Caries Management. Pediatr. Dent 38 (7), 466–471.
Donly, K. J., and Nelson, J. J. (1997). Fluoride Release of Restorative Materials Exposed to a Fluoridated Dentifrice. ASDC J. Dent Child. 64 (4), 249–250.
Donly, K. J., Istre, S., and Istre, T. (1995). In Vitro Enamel Remineralization at Orthodontic Band Margins Cemented with Glass Ionomer Cement. Am. J. Orthod. Dentofacial Orthop. 107 (5), 461–464. doi:10.1016/s0889-5406(95)70112-5
Forsten, L. (1998). Fluoride Release and Uptake by Glass-Ionomers and Related Materials and its Clinical Effect. Biomaterials 19 (6), 503–508. doi:10.1016/s0142-9612(97)00130-0
Fröhlich, T. T., Rocha, R. d. O., and Botton, G. (2020). Does Previous Application of Silver Diammine Fluoride Influence the Bond Strength of Glass Ionomer Cement and Adhesive Systems to Dentin? Systematic Review and Meta‐Analysis. Int. J. Paediatr. Dent 30 (1), 85–95. doi:10.1111/ipd.12571
Fung, M., Wong, M., Lo, E., and Chu, C. (2013). Arresting Early Childhood Caries with Silver Diamine Fluoride-A Literature Review. J. Oral Hyg. Health 1, 117–223. doi:10.4172/2332-0702.1000117
Gao, S. S., Zhao, I. S., Hiraishi, N., Duangthip, D., Mei, M. L., Lo, E. C. M., et al. (2016). Clinical Trials of Silver Diamine Fluoride in Arresting Caries Among Children: A Systematic Review. JDR Clin. Translational Res. 1 (3), 201–210. doi:10.1177/2380084416661474
García-Godoy, F., and Donly, K. J. (2015). Dentin-Enamel Adhesives in Pediatric Dentistry: An Update. Pediatr. Dent 37 (2), 133–135.
González Alarcón, D., and Bakari Ndjidda, W. (2018). “Update Report on Silver Diamine Fluoride,” in Mindja Paul Health and Emancipation Research Center. Cameroon: University of Yaounde.
Gupta, J., Thomas, M. S., Radhakrishna, M., Srikant, N., and Ginjupalli, K. (2019). Effect of Silver Diamine Fluoride-Potassium Iodide and 2% Chlorhexidine Gluconate Cavity Cleansers on the Bond Strength and Microleakage of Resin-Modified Glass Ionomer Cement. J. Conserv Dent 22 (2), 201–206. doi:10.4103/JCD.JCD_485_18
Horst, J. A. (2018). Silver Fluoride as a Treatment for Dental Caries. Adv. Dent Res. 29 (1), 135–140. doi:10.1177/0022034517743750
Jiang, M., Mei, M. L., Wong, M. C. M., Chu, C. H., and Lo, E. C. M. (2020). Effect of Silver Diamine Fluoride Solution Application on the Bond Strength of Dentine to Adhesives and to Glass Ionomer Cements: A Systematic Review. BMC Oral Health 20 (1), 40–11. doi:10.1186/s12903-020-1030-z
Juneja, A., Sultan, A., Siddiqui, M., and Kaur, G. (2019). Silver Diamine Fluoride as a Proactive Anti-Caries Tool: A Review. Int. J. Oral Heal Dent 5 (2), 63–68. doi:10.18231/j.ijohd.2019.016
Knight, G. M., Mcintyre, J. M., Craig, G. G., Mulyani, P. S., Zilm, P. S., and Gully, N. J. (2009). Inability to Form a Biofilm of Streptococcus Mutans on Silver Fluoride- and Potassium Iodide-Treated Demineralized Dentin. Quintessence Int. 40 (2), 155–161.
Knight, G., McIntyre, J., and Mulyani, (2006). The Effect of Silver Fluoride and Potassium Iodide on the Bond Strength of Auto Cure Glass Ionomer Cement to Dentine. Aust. Dental J. 51 (1), 42–45. doi:10.1111/j.1834-7819.2006.tb00399.x
Kucukyilmaz, E., Savas, S., Akcay, M., and Bolukbasi, B. (2016). Effect of Silver Diamine Fluoride and Ammonium Hexafluorosilicate Applications with and without Er:YAG Laser Irradiation on the Microtensile Bond Strength in Sound and Caries-Affected Dentin. Lasers Surg. Med. 48 (1), 62–69. doi:10.1002/lsm.22439
Leinfelder, K. F. (1988). Clinical Restorative Materials and Techniques. Philadelphia: Lea & Febiger.
Lutgen, P., Chan, D., and Sadr, A. (2018). Effects of Silver Diammine Fluoride on Bond Strength of Adhesives to Sound Dentin. Dent. Mater. J. 37 (6), 1003–1009. doi:10.4012/dmj.2017-401
Mei, M. L., Li, Q. L., Chu, C. H., Lo, E. C., and Samaranayake, L. P. (2013). Antibacterial Effects of Silver Diamine Fluoride on Multi-Species Cariogenic Biofilm on Caries. Ann. Clin. Microbiol. Antimicrob. 12 (1), 4. doi:10.1186/1476-0711-12-4
Minguez, N., Ellacuria, J., Soler, J. I., Triana, R., and Ibaseta, G. (2003). Advances in the History of Composite Resins. J. Hist. Dent 51 (3), 103–105.
Mithiborwala, S., Chaugule, V., Munshi, A., and Patil, V. (2012). A Comparison of the Resin Tag Penetration of the Total Etch and the Self-Etch Dentin Bonding Systems in the Primary Teeth: An In Vitro Study. Contemp. Clin. Dent 3 (2), 158–163. doi:10.4103/0976-237X.96818
Mitra, S. B., and Kedrowski, B. L. (1994). Long-Term Mechanical Properties of Glass Ionomers. Dental Mater. 10 (2), 78–82. doi:10.1016/0109-5641(94)90044-2
Muller-Bolla, M. (2014). Fiches Practiques D Odontolgiepe- Diatrique. Paris (France): Malakoff: Edition CdP.
Nguyen, V., Neill, C., Felsenfeld, O., and Primus, C. (2017). Potassium Iodide. The Solution to Silver Diamine Fluoride Discoloration? ADOH 5 (1), 1. doi:10.19080/adoh.2017.05.555655
Pallav, P., De Gee, A. J., Davidson, C. L., Erickson, R. L., and Glasspoole, E. A. (1989). The Influence of Admixing Microfiller to Small-Particle Composite Resin on Wear, Tensile Strength, Hardness, and Surface Roughness. J. Dent Res. 68 (3), 489–490. doi:10.1177/00220345890680031101
Pegado, R. E., do Amaral, F. L., Flório, F. M., and Basting, R. T. (2010). Effect of Different Bonding Strategies on Adhesion to Deep and Superficial Permanent Dentin. Eur. J. Dent 4 (2), 110–117. doi:10.1055/s-0039-1697818
Puckett, A. D., Fitchie, J. G., Bennett, B., and Hembree, J. H. (1995). Microleakage and thermal Properties of Hybrid Ionomer Restoratives. Quintessence Int. 26 (8), 577–581.
Puwanawiroj, A., Trairatvorakul, C., Dasanayake, A. P., and Auychai, P. (2018). Microtensile Bond Strength between Glass Ionomer Cement and Silver Diamine Fluoride-Treated Carious Primary Dentin. Pediatr. Dent 40 (4), 291–295.
Quock, R., Barros, J., Yang, S., and Patel, S. (2012). Effect of Silver Diamine Fluoride on Microtensile Bond Strength to Dentin. Oper. Dent 37 (6), 610–616. doi:10.2341/11-344-l
Roberts, J. F., Attari, N., and Sherriff, M. (2005). The Survival of Resin Modified Glass Ionomer and Stainless Steel crown Restorations in Primary Molars, Placed in a Specialist Paediatric Dental Practice. Br. Dent J. 198 (7), 427–431. doi:10.1038/sj.bdj.4812197
Rosenblatt, A., Stamford, T. C. M., and Niederman, R. (2009). Silver Diamine Fluoride: A Caries "Silver-Fluoride Bullet". J. Dent Res. 88 (2), 116–125. doi:10.1177/0022034508329406
Savin, C., Petcu, A., Gavrilă, L., Mârţu- Ştefanache, M. A., and Balan, A. (2016). Dental Materials for Coronary Obturation Utilized in Pedodontics. Int. J. Med. Dentistry 6 (3), 171–176.
Selvaraj, K., Sampath, V., Sujatha, V., and Mahalaxmi, S. (2016). Evaluation of Microshear Bond Strength and Nanoleakage of Etch-And-Rinse and Self-Etch Adhesives to Dentin Pretreated with Silver Diamine Fluoride/Potassium Iodide: An In Vitro Study. Indian J. Dent Res. 27 (4), 421–425. doi:10.4103/0970-9290.191893
Stoleriu, S., Iovan, G., Pancu, G., Nica, I., and Andrian, S. (2013). Study Concerning the Influence of the Finishing and Polishing Systems on the Surface State of Various Types of Composite Resins. Rom. J. Oral Rehabilit. 5 (3), 78–83.
Tassery, H., Koubi, S., Raskin, A., Bukiet, F., Pignoly, C., Toca, E., et al. (2006). One-Year Clinical Evaluation of Two Resin Composites, Two Polymerization Methods, and a Resin-Modified Glass Ionomer in Non-Carious Cervical Lesions. J. Contemp. Dent Pract. 7 (5), 42–53. doi:10.5005/jcdp-7-5-42
Van Duker, M., Hayashi, J., Chan, D. C., Tagami, J., and Sadr, A. (2019). Effect of Silver Diamine Fluoride and Potassium Iodide on Bonding to Demineralized Dentin. Am. J. Dent 32 (3), 143–146.
Wang, A. S., Botelho, M. G., Tsoi, J. K. H., and Matinlinna, J. P. (2016). Effects of Silver Diammine Fluoride on Microtensile Bond Strength of GIC to Dentine. Int. J. Adhes. Adhesives 70, 196–203. doi:10.1016/j.ijadhadh.2016.06.011
Wilde, M. G., Delfino, C. S., Sassi, J. F., Garcia, P. P., and Palma-Dibb, R. G. (2006). Influence of 0.05% Sodium Fluoride Solutions on Microhardness of Resin-Modified Glass Ionomer Cements. J. Mater. Sci. Mater. Med. 17 (9), 869–873. doi:10.1007/s10856-006-9847-9
Wilson, A. D., and Kent, B. E. (1972). A New Translucent Cement for Dentistry. The Glass Ionomer Cement. Br. Dent J. 132 (4), 133–135. doi:10.1038/sj.bdj.4802810
Wu, D. I., Velamakanni, S., Denisson, J., Yaman, P., Boynton, J. R., and Papagerakis, P. (2016). Effect of Silver Diamine Fluoride (SDF) Application on Microtensile Bonding Strength of Dentin in Primary Teeth. Pediatr. Dent 38 (2), 148–153.
Wu, M. Y., Suryanarayanan, K., van Ooij, W. J., and Oerther, D. B. (2007). Using Microbial Genomics to Evaluate the Effectiveness of Silver to Prevent Biofilm Formation. Water Sci. Technol. 55 (8-9), 413–419. doi:10.2166/wst.2007.285
Yamaga, R., Nishino, M., Yoshida, S., and Yokomizo, I. (1972). Diammine Silver Fluoride and its Clinical Application. J. Osaka Univ. Dent Sch. 12, 1–20.
Zhao, I. S., Chu, S., Yu, O. Y., Mei, M. L., Chu, C. H., and Lo, E. C. M. (2019). Effect of Silver Diamine Fluoride and Potassium Iodide on Shear Bond Strength of Glass Ionomer Cements to Caries-Affected Dentine. Int. Dental J. 69 (5), 341–347. doi:10.1111/idj.12478
Zhao, I. S., Gao, S. S., Hiraishi, N., Burrow, M. F., Duangthip, D., Mei, M. L., et al. (2018). Mechanisms of Silver Diamine Fluoride on Arresting Caries: A Literature Review. Int. Dent J. 68 (2), 67–76. doi:10.1111/idj.12320
Keywords: silver diamine fluoride, adhesive strength, adhesive systems, glass ionomer, composite resin
Citation: Fernández-Mafé M, Armengol-Olivares A, Miralles-Jordá L, Vicente-Escuder Á, Pérez-Bermejo M, Narciso J and Pallarés-Sabater A (2022) In Vitro Study on the Influence of Silver Diamine Fluoride on the Adhesion Strength of Dental Restorative Materials. Front. Mater. 9:833427. doi: 10.3389/fmats.2022.833427
Received: 11 December 2021; Accepted: 04 April 2022;
Published: 11 May 2022.
Edited by:
Senentxu Lanceros-Mendez, Basque Center for Materials, Applications and Nanostructures, SpainReviewed by:
Abdul Samad Khan, Imam Abdulrahman Bin Faisal University, Saudi ArabiaCopyright © 2022 Fernández-Mafé, Armengol-Olivares, Miralles-Jordá, Vicente-Escuder, Pérez-Bermejo, Narciso and Pallarés-Sabater. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mónica Fernández-Mafé, bW9uaWNhLmZlcm5hbmRlekB1Y3YuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.