 Majid Reza Ayatollahi1*
Majid Reza Ayatollahi1* Mohammad Hossein Davari
Mohammad Hossein Davari Hadi Asgharzadeh Shirazi
Hadi Asgharzadeh Shirazi Alireza Asnafi
Alireza Asnafi
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Mater. , 22 May 2019
Sec. Biomaterials
Volume 6 - 2019 | https://doi.org/10.3389/fmats.2019.00107
This article is part of the Research Topic Functional Materials for Bio-Applications View all 14 articles
One of the common issues that occur after total knee replacement surgery is the aseptic loosening. The problem usually occurs after about 15 years from the surgery. The destructive effects of residual particles due to wear, the stress shielding effect, and micro-movements are the causative factors for this type of loosening. In this research, using the advantages of functionally graded biomaterials (FGBM), it is tried to design a prosthetic system that can reduce the above-mentioned effects. For this purpose, the materials used in the most important part of the prosthesis system, i.e., the femoral part are redesigned so that the bioactivity between the prosthesis and bone, and the stress applied to the adjacent tissues increase simultaneously. In addition, to reduce the effect of wear at contact areas, wear-resistant biocompatible ceramics such as alumina and zirconia are used. The value of stress at the bone-prosthesis interface and adjacent tissues is the most important parameters. Two types of three-phase ceramic-based FGBMs are recommended. The prosthesis with three-phase hydroxyapatite-titanium-zirconia has increased the average stress in the bone tissues around high-risk areas up to 71.8% with respect to a commonly used Cr-Co prosthesis. The result for the prosthesis with three-phase hydroxyapatite-titanium-alumina is up to 65%, respectively. At bone-prosthesis interfaces, an increase of 92% in the stress for both zirconia-based and alumina-based is seen. Briefly, the recommended FGBMs can improve the bone-prosthesis performance in all desired indices.
The knee, as one of the complex joints in the body, connects the femur bone to the tibia and fibula. The kneecap patella is another component of this important joint. It is also surrounded by a joint capsule, synovial membrane (containing synovial fluid) and ligaments. Synovial fluid reduces joint friction and also plays a role in feeding the cartilages. In a knee replacement surgery, damaged cartilages, and bones are removed from the joint and replaced by a prosthesis system. Depending on the type of damage, the prosthesis system may include from one to three layers. In a total replacement of the knee, the lower part of the femur and the upper part of the tibia are connected with the prosthesis.
Due to any reason, the weakening of the connection between the prosthesis and the bone is a factor that in many cases results in a re-surgical procedure. In this case, there is a need to replace the prosthesis system with a newer one that has its own limitations with significantly lower success and more costs. In 2011, Bahraminasab and Jahan (2011) considered the challenge of aseptic loosening as the most important factor after the knee replacement operation. They showed that three factors of excessive wear, stress shielding effect, and development of soft tissue between the prosthesis and the bone are the most important reasons in the occurrence of this phenomenon.
The knee prosthesis has attracted the attention of many researchers, in terms of geometry and material. Saari et al. (2006) studied the geometry of the tibia-prosthesis component and showed how the posterior stabilization leads to bone loss. Wang et al. (2011) investigated the basic geometry of femoral knee prosthesis and considered eight different geometries to obtain the distribution of stress and type of bone destructions in the models. Zietz et al. (2012) focused their studies on the effects of different femoral bone segments on the behavior of bone-prosthesis systems to recommend the best model in terms of reduction in stress shielding effect.
As far as geometry is concerned for prostheses, there are numerous articles on the types and properties of the prostheses materials. Long and Rack (1998) focused on the comparison of Titanium alloy to stainless steel with a concentration on fatigue and wear and examined the advantages of Titanium alloys in this respect. Peterson et al. (1988) compared the behaviors of Titanium and Cobalt-Chromium-Molybdenum alloys in terms of wear for the femoral part of the knee prosthesis. McEwen et al. studied the effect of material, local movement and prosthesis geometry on the wear of an ultra-high molecular weight polyethylene (UHMWPE) prosthesis system. They showed that the backside motion contributes to an overall rate of UHMWPE wear in the system.
Due to the fact that several materials with different and sometimes contradictory properties can be used in the structure of functionally graded materials, these materials are recommended as suitable alternatives for the design of new generation of the knee prostheses. Also, in these materials, the properties between the components vary continuously; so, there is no need to worry about the disadvantages of composite laminated materials. For example, the prosthesis can be designed to reduce the effects of loosening, including wear, micro-motion and the effect of shielding stress simultaneously. At contact bearing surfaces, wear-resistant materials should be used while in areas close to bone tissues, materials with less elastic modulus are recommended to reduce the effect of shielding stress. Finally, at direct contact areas of the prosthesis and bone, a bioactive material to reduce the micro-motions is suggested. The use of functionally graded biomaterials in medical prosthetics has been considered in recent researches (Sadollah and Bahreininejad, 2011; Gong et al., 2012; Enab and Bondok, 2013). Some works on the use of these materials in knee prostheses have also been reported in the literature (Bahraminasab et al., 2013a,b); however, the bioactivity that prevents micro-motions, the reduction in the effects of shielding stress, and establishing strength have not been sufficiently taken into consideration.
In this research, two types of ceramic-based prosthesis systems using three-phase functionally graded biomaterials are proposed by considering the effects of stress shielding, wear resistance, and bioactivity simultaneously. Also, the required strength and toughness are also investigated. The behavior and performance of the proposed prosthesis systems and the ones commonly used in previous works are compared to each other.
The mechanical strength of an artificial knee can effect both the performance and failure of the prosthesis system. If the osseointegration between the prosthesis and bone does not form well, soft fibrous tissues are formed in the connection, results in more relative movement between the implants and the bone. Initially, this causes increased pain in the patient and after a certain period, the implant loses its effectiveness and the need for implant replacement is inevitable (Geetha et al., 2009). It should be noted that the high strength of the prosthesis with the low elastic modulus is of great importance (Wang, 1996; Long and Rack, 1998). A high difference between the modulus of the implant's elasticity and the surrounding bone can contribute to the effect of shielding stress. This phenomenon may lead to a weakening of the bone and its connections to the implant and, consequently, the loosening of the prosthesis system. Additionally, the low elastic modulus means higher flexibility and damping capacity which directly increases the absorption energy of the impact and reduces the stress between the bones and the knee prosthesis. Therefore, the modulus of implant material elasticity is a major factor for the selection of materials for knee replacement prosthesis.
Low resistance to wear or high friction coefficient can also cause loosening in the implants (Ramsden et al., 2007). In addition, the remaining particles of wear are biologically active and may produce a severe inflammatory reaction. This may damage the immune supporting bone. Friction also increases the possibility of corrosion.
Another important requirement for orthopedic biomaterials is biocompatibility. Biocompatibility refers to the ability of prosthesis to communicate with the living tissue of the surrounding bones. Biocompatibility is not just about the implications of the implant and the surrounding tissues, and it is important to check its effects on the rest of the organic system (Navarro et al., 2008; Williams, 2008).
The osseointegration process is another major orthopedic necessity related to the bone improvement process. In some cases, for example, due to relative micro-movements, the implant cannot properly bind to the surrounding bone and tissues. This leads to the formation of fibrous tissues around the implant, and ultimately accelerates the loosening process (Viceconti et al., 2000).
In addition to the above, the corrosion which is an important factor in the field of biomaterials, and the issues related to the manufacturing process of biomaterials such as ductility, toughness, etc. should also be taken into account.
Titanium alloys are among the most popular orthopedic materials. Titanium alloys have excellent properties such as high strength, low density, good corrosion resistance, complete non-toxicity to the body, and moderate elastic modulus suitable for planting in the body (Nag et al., 2009). Titanium and its alloys can provide a relatively strong bond to the bone, which greatly improves the fixity of the implant and significantly prevents micro-movement. The elastic modulus of titanium alloys is about 110 GPa, less than steel and cobalt-chromium alloys. Therefore, a titanium implant is expected to reduce the shielding stress effect compared to a more elastic modulus material; however, the occurrence of this phenomenon is still possible due to the large difference between the modulus of elasticity of titanium alloys and human bones. Unfortunately, these alloys have a low wear resistance (one of the first factors in aseptic loosening) due to relative movements at bearing surfaces between themselves and other metals. Due to oxidation of titanium and the low adhesion of the oxidized layer, some particles are removed from the material and remain on the bearing surfaces. Based on experimental results, it has been shown that for the relative motion between UHMWPE and Ti-6Al-4V, the wear rate of both metal and polymer is much higher than that of stainless steel or cobalt-chromium-molybdenum alloy. In addition, the residual particles of wear from titanium alloys cause side effects like tissue discoloration indicative of metallosis (Nasser et al., 1990). Therefore, the use of titanium in areas with the high potential of wear i.e., knee and hip joints is limited (Nag et al., 2009). Also, there is concern about the release of aluminum and vanadium ions in titanium alloys that may lead to health problems (Okazaki and Gotoh, 2005; Navarro et al., 2008; Geetha et al., 2009).
Alumina (Al2O3) ceramics belongs to the group of oxide ceramics and polycrystalline materials with properties including high stiffness, good stability, high oxidation ability, very low friction coefficient (high wear resistance) and good biocompatibility (Hannouche et al., 2005). The earliest clinical use of pure ceramics was seen in 1970 for the hip prostheses (Boutin, 1971). It has been expected that the use of these materials for knee replacement can essentially improve in two aspects to minimize bone osteolysis: greater stability in biocompatibility and reduction of residual particles due to wear. Therefore, based on the results of the knee simulator, it was attempted to use a combination of alumina ceramics and UHMWPE as an alternative for knee prostheses (Heimke et al., 2002; Oonishi et al., 2006). The serious problem if the alumina ceramics is used alone is its high modulus of elasticity (350 GPa) which resulted in the effect of shielding stress and the aseptic loosening in the bone-prosthesis system (Boutin, 1971).
Unfortunately, alumina is not bioactive and cannot directly create a level of bone and implant interface, which results in micro-movements and thus aseptic loosening. It also has a low failure toughness than metal materials used in orthopedic applications. It shows brittle behavior i.e., no significant deformation is seen to fracture (Hannouche et al., 2003). To overcome the limitations of the mechanical properties of alumina, zirconia (ZrO2) was introduced. High strength, high toughness (about twice the alumina) and higher flexural strength (500-1,000 MPa) can be attributed to this ceramic. However, in contrast to alumina, zirconia has an unstable and multifaceted crystalline structure including monoclinic, tetragonal, and cubic. Therefore, phase transfer can occur from a crystalline structure to another, especially from the tetragonal phase to monoclinic. Phase transformation with shape and volume changes makes the material susceptible to cracking (Bal et al., 2006).
For optimal use of material properties, every advantage and every interest should be used in the right position and situation. To satisfy all conditions, a three-phase functionally graded biomaterial is proposed. At the site of bone bonding, hydroxyapatite (HA) is recommended for maximum biocompatibility. At bearing surfaces, alumina or zirconia ceramics is suggested to have maximum wear resistance. Titanium alloys are also offered in the middle of the material to provide both required strength and toughness. Figure 1 shows a schematic distribution of properties in a cross section of the material. The properties of materials used in this study to propose new FGBMs can be seen in Table 1. It should be noted that due to the almost same Poisson coefficient of materials used in the design of the FGBM, this coefficient is considered 0.3 in all simulations.
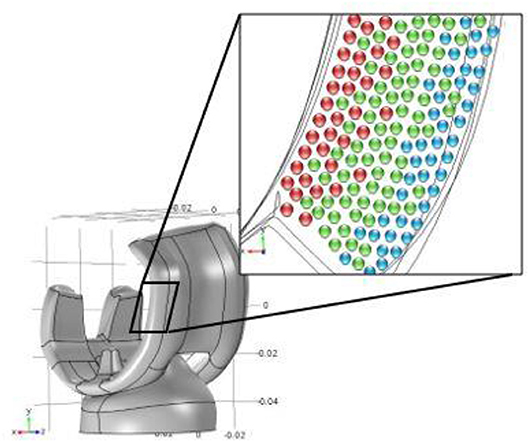
Figure 1. The schematic of material properties distribution in a cross section of the functionally graded biomaterial; red spheres: HA, green spheres: Ti, blue spheres: Al2O3 or ZrO2.
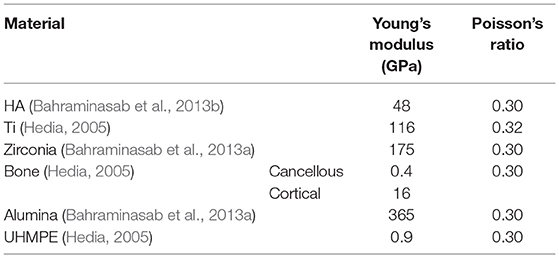
Table 1. The properties of materials used in this study.
The functions of how to change the properties including the modulus of elasticity and the Poisson coefficient are:
Where
In a finite element modeling, considering the desired function and selecting the material for each phase, a 3D model of the knee prosthesis and surrounding bone tissue was prepared and analyzed to obtain the distribution of stress and deformation in the system (see Figure 2).
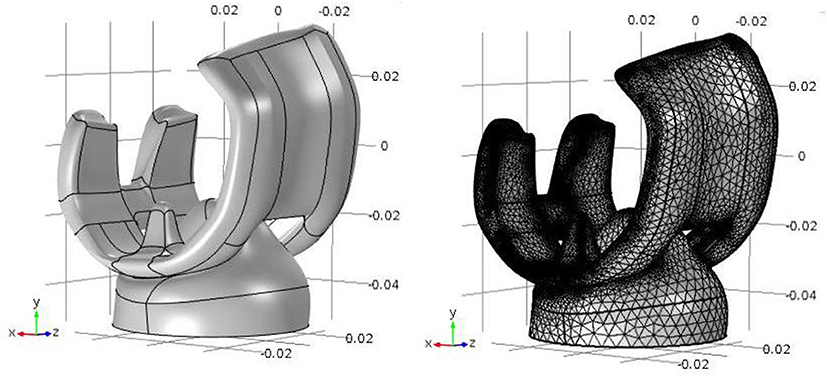
Figure 2. The geometry (left) and the generated mesh (right) for finite element analysis.
The element type in the 3-D model is tetrahedron. The number of elements after the sensitivity analysis was 82,387 elements. It should be noted that the method of function assignment to a model is possible in two ways:
1- Partitioning the model into a number of layers (30 to 40 layers) proportional to the direction of changing the properties in the model and assigning the properties of the material with the approximation of its value from the desired function, or
2- Applying the function in the matrix of the properties of the material.
In this research, we try to use the function directly to assign material properties using the COMSOL Multiphysics5.2 software. The results of each route were only reported after a mesh study was done so that we ensured about the correctness of the outcomes and the convergence phenomenon.
The basis of knee and knee prosthesis modeling is based on dynamic analysis and a variety of created conditions caused by daily activities. In these activities, such as walking, running, climbing, etc. modeling the force applied to different points of the knee and prosthesis has a lot of complexity. This article focuses on the effect of changing the properties of the prosthesis on the surrounding bones, which can be generally examined for different loading conditions. In this research, the maximum value of the force at most dominant gait i.e., the walking is selected as a static load and then applied to the model. The amount of static load was considered to be 3110N (Bergmann et al., 2014) along the axial direction of the femur. This amount of load is reported in the literature for walking gait (Bergmann et al., 2014). The displacement of the lower surface of the tibia from the knee prosthesis is fixed in direction of the force applied, and in other directions are bounded by a point. Two contact constraints were defined; the first contact is associated with the area of the bone and prosthetic contact area, and the second contact is related to the prosthetic contact area and the tibia component. The contact between the prosthesis and the bone should be a constraint without any displacement; otherwise, the prosthesis is removed from the bone, which is not the basis of this research. Therefore, this constraint is considered as an all-inclusive fully fixed constraint between bone and prosthesis elements. The contact between the prosthesis and the tibia component is considered non-frictional. In fact, because of the absence of a specific friction coefficient in that environment between the prosthesis and the tibia component, which is subject to a variety of factors, the exact modeling has a particular complexity.
The values of Von Mises stress are evaluated along 12 directions in the prosthesis-bone system regarding a 3D model (see Figures 3A,B for more details). The center point is the midpoint of the prosthetic along-side its arms, with paths of 15, 20, 30 mm radius and at angles of 45, 135, 225, and 315 relative to the horizon line, and are numbered according to the Figure 3.
Figure 3. (A) Twelve assumed directions in the prosthesis-bone system; (B) The most important directions in 3-D model; (C) The most damaged areas due to stress shielding effect based on lateral radiograph of a distal femur showing distal anterior femoral osteopenia behind the femoral component (arrowheads) (Van Loon et al., 2001).
According to reports in the literature (Van Loon et al., 2001), the most damaged areas due to stress shielding effect are along directions 9 and 10; after that 5 and 6 and finally 1 and 2 (see Figures 3B,C). Here, the results are obtained in these directions for the commonly used cobalt-chromium prosthesis, also; alumina and zirconia-based three-phase FG biomaterials. Tables 2, 3 demonstrate the average and bone-prosthesis interface stresses along assumed paths at Cr-Co and alumina/zirconia-based proposed FG biomaterials. In Figure 4, one can follow the Von Mises stress vs. proximal distance from the interface in response to all paths for both Cr-Co and alumina-based proposed FG biomaterial. Figure 5 present the same results reported previously in Figure 4 except that the zirconia-based FGBM is used. Qualitatively, the same similarities are seen but there are some quantitative differences. It is again to be noted that the results presented in Figures 4, 5 and Tables 2–4 are based on the paths considered in Figures 3A,B.
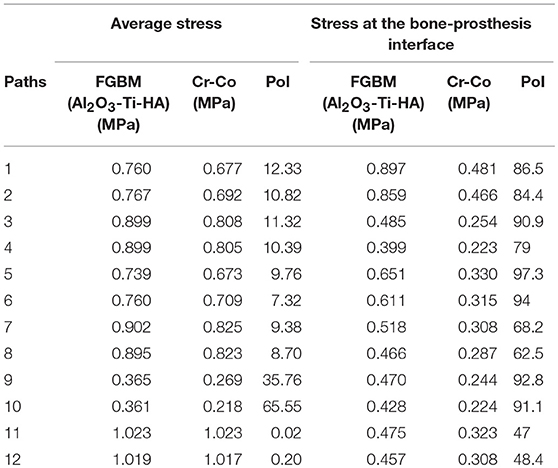
Table 2. Average and bone-prosthesis interface stresses along assumed paths at Cr-Co and alumina-based proposed FG biomaterial [PoI: Percent of increase (%)].
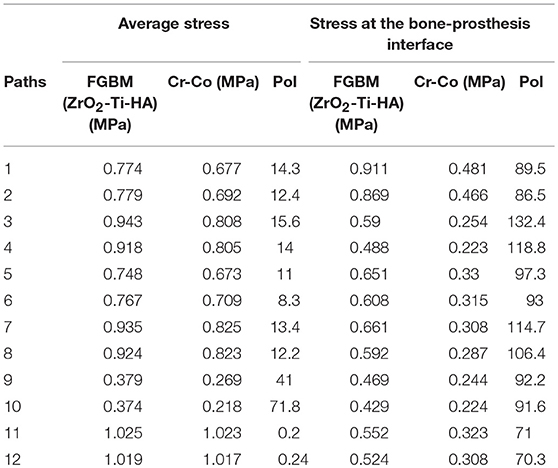
Table 3. Average and bone-prosthesis interface stresses along assumed paths at Cr-Co and zirconia-based proposed FG biomaterial [PoI: Percent of increase (%)].
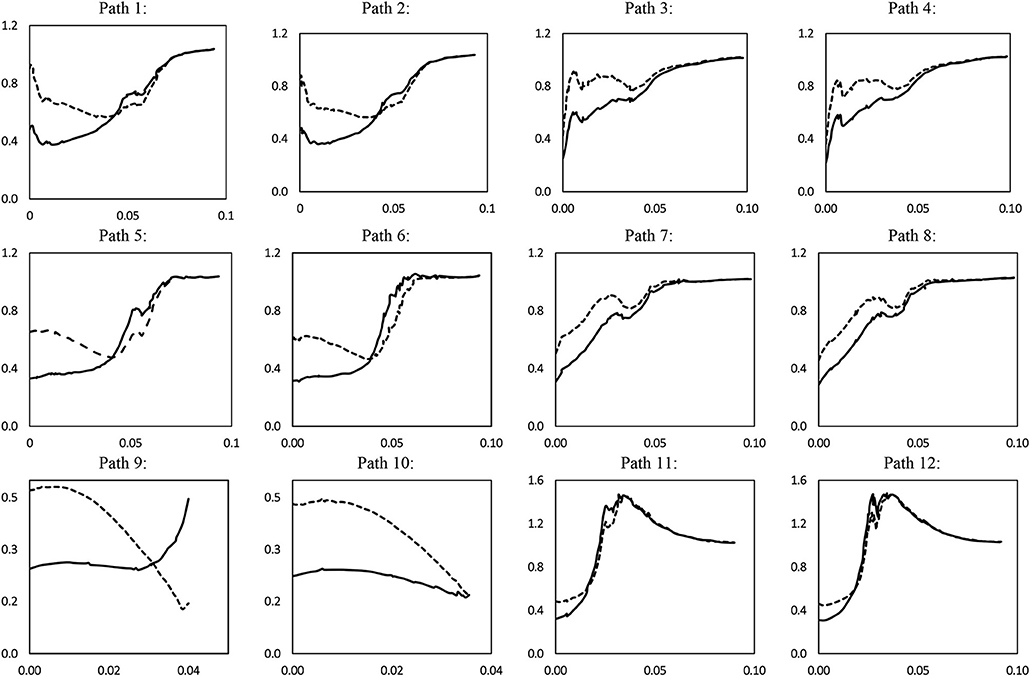
Figure 4. Von Mises stress (MPa) vs. proximal distance from the interface (m) in response to the all paths for both Cr-Co (solid line) and alumina-based proposed FG biomaterial (dashed line).
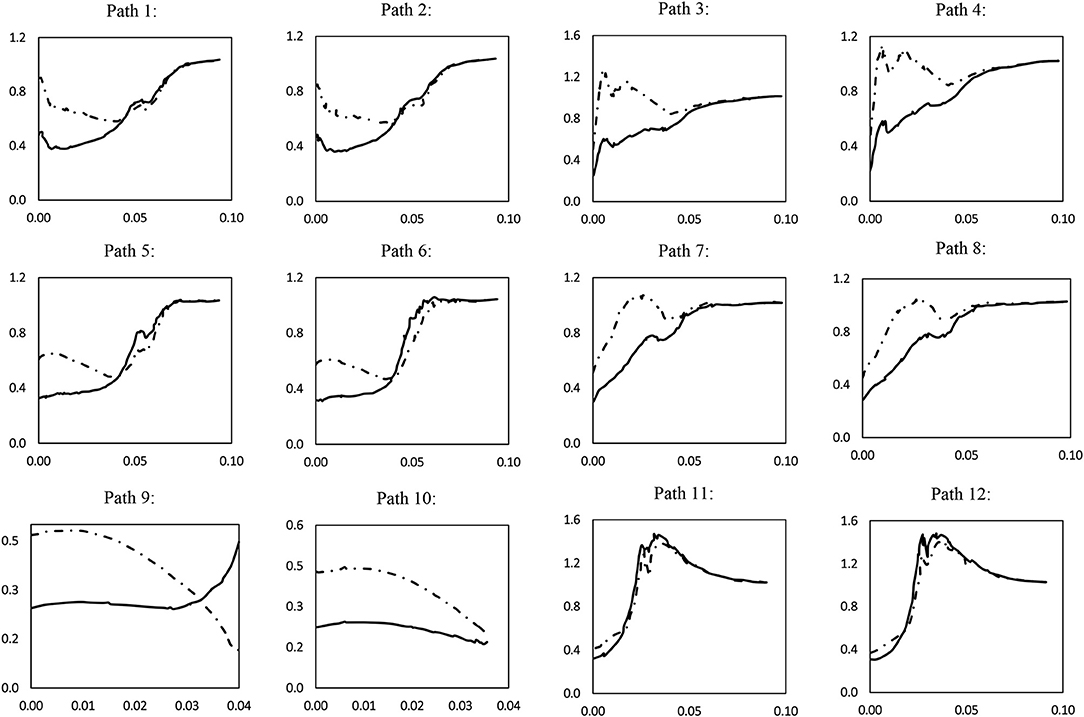
Figure 5. Von Mises stress (MPa) vs. proximal distance from the interface (m) in response to the all paths for both Cr-Co (solid line) and zirconia-based proposed FG biomaterial (dashed line).
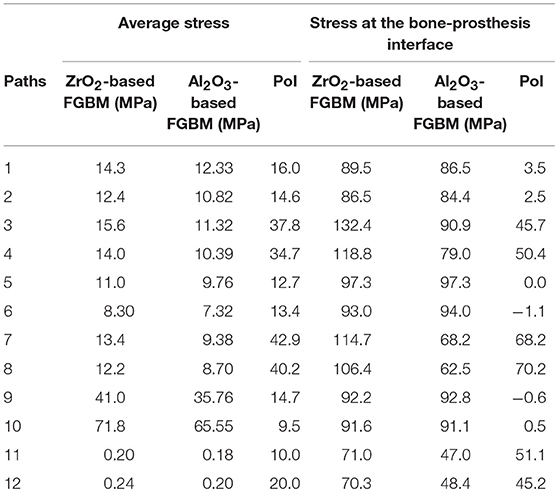
Table 4. Average and bone-prosthesis interface stresses along assumed paths at alumina-based and zirconia-based proposed FG biomaterials [PoI: Percent of increase (%)].
The Von Mises stress is considered as an indicator to be obtained in both the prosthesis and surrounding bones in our simulations. This measure is related to other factors such as wear, strength, and shielding stress effect; so, one can use it to have an almost precise look at the global and local behavior and performance of the prosthesis system. To show the performance of the recommended FGBM prosthesis, three comparisons were made; the first two are between the commonly used cobalt-chromium prosthesis with the three-phase FG biomaterials proposed in this study, one is based on alumina and the other on zirconia. The third comparison was also made between the two proposed FG biomaterials.
According to the results presented in Table 2, for the three-phase FG biomaterial (alumina-titanium-hydroxyapatite), all routes in the design of FGM have shown moderate stress in bone tissue, which means a reduction in stress shielding effect. The paths on which the stress values were calculated are the same as those shown in Figures 3A,B. Reference (Van Loon et al., 2001) indicated that paths 9 and 10 played a more important role in the shielding stress phenomenon; thus, the study of these two paths is more important. According to Table 2, the proposed material has been able to increase the average stress by 65.55% and 35.76% in these pathways, which reduces the effect of shielding stress and, consequently, aseptic loosening. In major paths such as 1, 2, 5 and 6, and most of the paths, stress in the bone has increased. Only on the 11th and 12th routes, little changes are observed. In fact, the change in properties of the prosthesis has not had a significant change in the stress of these two paths, which can be concluded that stress in these two paths is independent of the properties of the prosthetic material.
In Figure 4, it can be noted that the stress in the bone-prosthesis interfaces has increased significantly. The percent values of increase at interfaces along each path are listed in Table 2. As previously indicated, moderate values of stress at bone- prosthesis interfaces are important to reduce the shielding stress effect and consequently the aseptic loosening. The maximum increase occurred on route 9, with the lowest increase in path 11. Using this FG biomaterial, the maximum change in the stresses is seen at the bone-prosthesis interfaces which are quite desirable and valuable.
In the same way previously indicated in section Three-Phase Alumina-Based FG Biomaterial vs. Cr-Co One, the average stresses along the assumed paths together with the bone-prosthesis interface stresses are obtained for a zirconia-based FG biomaterial and compared to the ones of the commonly used cobalt-chromium prosthesis. Same qualitative similarities are seen while the quantitative values are different. There is again a significant increase in stresses in all directions except the average stresses along paths 11 and 12. More important paths 9 and 10 show an average increase of 41 and 71.8%, respectively. The values of stress are greater in comparison with the amount in the same path for the alumina-based FGBM. One can follow the values of average and interface stresses for this case in Table 3.
In this section, a comparison is done between two proposed FG biomaterials. Based on the results listed in Table 4, Zirconia-based FG biomaterial has a better performance in terms of stress shielding effect reduction in the bone tissues. It is due to the fact that the Young modulus of zirconia which is equal to 175 GPa is much less than the modulus of alumina which is equal to 365 GPa. The greatest increase in terms of both average stress and interface one occurred in routes 7 and 8. Along important paths 9 and 10, zirconia-based FG biomaterial shows better performance in terms of average stress whereas no significant change in terms of stress in the interface is seen for these two paths. As shown in Table 4, the stress values in bone tissues for all paths are higher when the zirconia-based FG biomaterial is employed. The largest differences are seen for paths 7 and 8.
To improve the performance of the bone-prosthesis system and prevent the aseptic loosening in a total knee replacement surgery, two types of ceramic-based functionally graded biomaterials were proposed in this article. To have a right investigation, 12 directions in a 3D finite element model of the prosthesis system were considered. The Von Mises stress values along the paths, as an important indicator, were obtained for proposed materials and then compared to commonly-used Cr-Co prosthesis. Specifically, the average values and the stress at the bone-prosthesis interfaces along the paths were compared to each other. Along all the paths, both the alumina-based and zirconia-based FG biomaterials showed significantly better performance. The average stress when the zirconia-based FGBM was used was higher than that of alumina-based one. Generally, both recommended FGBMs can reduce the effect of shielding stress, while the zirconia-based one shows better performance in this respect.
The datasets for this manuscript are not publicly available because There is no public link related to this data but the raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher. Requests to access the datasets should be directed to Pr. MA (bS5heWF0QGl1c3QuYWMuaXI=).
MRA gave the idea, interpreted the results, and checked the final version of the article. MHD surveyed the literature in this respect and prepared the history of the research and the first version of the article and also helped derive and solve the equations. HAS derived and solved the equations and drew the figures in corresponding software. AA wrote the main text of the article together with the abstract and conclusion and investigated the correctness of the equations and text of the article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Bahraminasab, M., and Jahan, A. (2011). Material selection for femoral component of total knee replacement using comprehensive VIKOR. Mater. Design 32, 4471–4477. doi: 10.1016/j.matdes.2011.03.046
Bahraminasab, M., Sahari, B., Edwards, K. L., Farahmand, F., and Arumugam, M. (2013a). Aseptic loosening of femoral components–materials engineering and design considerations. Mater. Design. 44, 155–163. doi: 10.1016/j.matdes.2012.07.066
Bahraminasab, M., Sahari, B., Edwards, K. L., Farahmand, F., and Hong, T. (2013b). Material tailoring of the femoral component in a total knee replacement to reduce the problem of aseptic loosening. Mater. Design. 52, 441–451. doi: 10.1016/j.matdes.2013.05.066
Bal, B. S., Garino, J., Ries, M., and Rahaman, M. N. (2006). Ceramic materials in total joint arthroplasty. Semi. Arthroplasty 17, 94–101. doi: 10.1053/j.sart.2006.09.002
Bergmann, G., Bender, A., Graichen, F., Dymke, J., Rohlmann, A., Trepczynski, A., et al. (2014). Standardized loads acting in knee implants. PLoS ONE. 9:e86035. doi: 10.1371/journal.pone.0086035
Boutin, P. (1971). Alumina and its use in surgery of the hip.(Experimental study). La Presse. Med. 79, 639.
Enab, T. A., and Bondok, N. E. (2013). Material selection in the design of the tibia tray component of cemented artificial knee using finite element method. Mater. Design. 44, 454–460. doi: 10.1016/j.matdes.2012.08.017
Geetha, M., Singh, A., Asokamani, R., and Gogia, A. (2009). Ti based biomaterials, the ultimate choice for orthopaedic implants–a review. Prog. Mater. Sci. 54, 397–425. doi: 10.1016/j.pmatsci.2008.06.004
Gong, H., Wu, W., Fang, J., Dong, X., Zhao, M., and Guo, T. (2012). Effects of materials of cementless femoral stem on the functional adaptation of bone. J. Bionic. Eng. 9, 66–74. doi: 10.1016/S1672-6529(11)60098-X
Hannouche, D., Hamadouche, M., Nizard, R., Bizot, P., Meunier, A., and Sedel, L. (2005). Ceramics in total hip replacement. Clin. Orthop. Relat. Res. 430, 62–71. doi: 10.1097/01.blo.0000149996.91974.83
Hannouche, D., Nich, C., Bizot, P., Meunier, A., Nizard, R., and Sedel, L. (2003). Fractures of ceramic bearings: history and present status. Clin. Orthop. Relat. Res. 417, 19–26. doi: 10.1097/01.blo.0000096806.78689.50
Hedia, H. (2005). Comparison of one-dimensional and two-dimensional functionally graded materials for the backing shell of the cemented acetabular cup. J. Biomed. Mater. Res. Part B: Appl. Biomater. 74, 732–739. doi: 10.1002/jbm.b.30258
Heimke, G., Leyen, S., and Willmann, G. (2002). Knee arthoplasty: recently developed ceramics offer new solutions. Biomaterials 23, 1539–1551. doi: 10.1016/S0142-9612(01)00262-9
Long, M., and Rack, H. J. (1998). Titanium alloys in total joint replacement—a materials science perspective. Biomaterials 19, 1621–1639. doi: 10.1016/S0142-9612(97)00146-4
Nag, S., Samuel, S., Puthucode, A., and Banerjee, R. (2009). Characterization of novel borides in Ti–Nb–Zr–Ta+ 2B metal-matrix composites. Mater. Charac. 60, 106–113. doi: 10.1016/j.matchar.2008.07.011
Nasser, S., Campbell, P. A., Kilgus, D., Kossovsky, N., and Amstutz, H. C. (1990). Cementless total joint arthroplasty prostheses with titanium-alloy articular surfaces: a human retrieval analysis. Clin. Orthop. Relat. Res. 261, 171–185. doi: 10.1097/00003086-199012000-00020
Navarro, M., Michiardi, A., Castano, O., and Planell, J. (2008). Biomaterials in orthopaedics. J. R. Soc. Interf. 5, 1137–1158. doi: 10.1098/rsif.2008.0151
Okazaki, Y., and Gotoh, E. (2005). Comparison of metal release from various metallic biomaterials in vitro. Biomaterials 26, 11–21. doi: 10.1016/j.biomaterials.2004.02.005
Oonishi, H., Kim, S. C., Kyomoto, M., Iwamoto, M., and Ueno, M. (2006). “PE wear in ceramic/PE bearing surface in total knee arthroplasty: clinical experiences of more than 24 years,” in Bioceramics and Alternative Bearings in Joint Arthroplasty (Steinkopff), 101–110.
Peterson, C., Hillberry, B., and Heck, D. (1988). Component wear of total knee prostheses using Ti-6Al-4V, titanium nitride coated Ti-6Al-4V, and cobalt-chromium-molybdenum femoral components. J. Biomed. Mater. Res. Part A. 22, 887–903. doi: 10.1002/jbm.820221005
Ramsden, J. J, Allen, D. M, Stephenson, D. J., et al. (2007). The design and manufacture of biomedical surfaces. CIRP Ann. Manuf. Technol. 56, 687–711,. doi: 10.1016/j.cirp.2007.10.001
Saari, T., Uvehammer, J., Carlsson, L. V., Regnér, L., and Kärrholm, J. (2006). Posterior stabilized component increased femoral bone loss after total knee replacement. 5-year follow-up of 47 knees using dual energy X-ray absorptiometry. The Knee 13, 435–439. doi: 10.1016/j.knee.2006.08.002
Sadollah, A., and Bahreininejad, A. (2011). Optimum gradient material for a functionally graded dental implant using metaheuristic algorithms. J. Mech. Behav. Biomed. Mater. 4, 1384–1395. doi: 10.1016/j.jmbbm.2011.05.009
Van Loon, C., Oyen, W., de Waal Malefijt, M., and Verdonschot, N. (2001). Distal femoral bone mineral density after total knee arthroplasty: a comparison with general bone mineral density. Arch. Orthop. Trauma Surg. 121, 282–285. doi: 10.1007/s004020000232
Viceconti, M., Muccini, R., Bernakiewicz, M., Baleani, M., and Cristofolini, L. (2000). Large-sliding contact elements accurately predict levels of bone–implant micromotion relevant to osseointegration. J. Biomech. 33, 1611–1618. doi: 10.1016/S0021-9290(00)00140-8
Wang, C. J., Shi, J. F, Morgan, C., and Mynors, D. J. (2011). Design and simulation of a femoral component peg in total knee replacement. Key Eng. Mater. 450, 111–114. doi: 10.4028/www.scientific.net/KEM.450.111
Wang, K. (1996). The use of titanium for medical applications in the USA. Mater. Sci. Eng. A. 213, 134–137. doi: 10.1016/0921-5093(96)10243-4
Williams, D. F. (2008). On the mechanisms of biocompatibility. Biomaterials 29, 2941–2953. doi: 10.1016/j.biomaterials.2008.04.023
Keywords: ceramic-based FGBM, finite element method, stress shielding effect, bone-prosthesis system, orthopedic prosthesis, femoral diseases
Citation: Ayatollahi MR, Davari MH, Shirazi HA and Asnafi A (2019) To Improve Total Knee Prostheses Performance Using Three-Phase Ceramic-Based Functionally Graded Biomaterials. Front. Mater. 6:107. doi: 10.3389/fmats.2019.00107
Received: 24 February 2019; Accepted: 24 April 2019;
Published: 22 May 2019.
Edited by:
Laura Maria Vergani, Politecnico di Milano, ItalyReviewed by:
Sergey V. Dorozhkin, Independent Researcher, Moscow, RussiaCopyright © 2019 Ayatollahi, Davari, Shirazi and Asnafi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Majid Reza Ayatollahi, bS5heWF0QGl1c3QuYWMuaXI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.