 Aleksandra Antovic1*†
Aleksandra Antovic1*† Daniele Lini2,†
Daniele Lini2,† Nida Soutari3
Nida Soutari3 Sanja Lalic-Cosic4Agneta Zickert1Andrea Mc Nicholas1Katarina Bremme5Maria Sennström5
Sanja Lalic-Cosic4Agneta Zickert1Andrea Mc Nicholas1Katarina Bremme5Maria Sennström5 Franco Franceschini2
Franco Franceschini2 Elisabet Svenungsson1
Elisabet Svenungsson1 Laura Andreoli2,†Iva Gunnarsson1,†
Laura Andreoli2,†Iva Gunnarsson1,†
- 1Division of Rheumatology, Department of Medicine Solna, Karolinska Institutet and Rheumatology, Karolinska University Hospital, Stockholm, Sweden
- 2Rheumatology Unit, Department of Medicine, ASST Spedali Civili of Brescia and University of Brescia, Brescia, Italy
- 3Department of Molecular Medicine and Surgery, Karolinska Institutet and Clinical Chemistry, Karolinska University Hospital, Stockholm, Sweden
- 4Department of Medical Biochemistry, Faculty of Pharmacy, University of Belgrade, Belgrade, Serbia
- 5Department of Women’s and Children’s Health, Karolinska Institutet, Stockholm, Sweden
Objectives: This study aimed to investigate hemostatic parameters in pregnant patients with systemic lupus erythematosus (SLE) in relation to the use of antithrombotic prophylaxis, preeclampsia (PE), and antiphospholipid antibody status.
Patients and methods: In total, 34 pregnant patients with SLE and 80 pregnant healthy controls (HC) without PE were included. Patients with SLE were sampled during the first and third trimester of gestation. We analyzed fibrinogen, D-dimer, and global hemostatic parameters including the overall coagulation potential (OCP), overall hemostatic potential (OHP), and the overall fibrinolysis potential (OFP). Fibrin structure was visualized using scanning electron microscopy.
Results: The median age of the patients with SLE was 33 (range 23–42) years and 31 (26–38) years in the HC. The median disease duration was 10 (range 0–26) years. All but two patients with SLE received prophylaxis with low-dose acetylsalicylic acid (LDASA) and 11 received low-molecular-weight heparin (LMWH). OCP and OHP were significantly increased in the patients with SLE compared to HC (p < 0.01). The levels of fibrinogen and D-dimer increased throughout the pregnancies in the patients with SLE, but no differences were found in the third trimester compared to controls. Among the patients treated with LMWH, OCP, OHP, and OFP were undetectable in two, both of whom were on high prophylactic dosage, and one developed PE. OCP, OHP, and OFP levels were not affected by low prophylactic doses of LMWH. Despite LDASA, preeclampsia occurred in four patients with SLE (12.5%); of whom two received a high prophylactic LMWH dose. Five of 32 (15.6%) patients had major bleeding complications at delivery. There were no thromboembolic complications.
Conclusions: In this pilot study, pregnant patients with SLE developed a hypercoagulable state throughout pregnancy, as demonstrated by the global hemostatic parameters OCP and OHP, except for two patients who were treated with a full dosage of LMWH. The alterations in the coagulation system in SLE pregnancy need to be further studied with the aim of optimizing treatment strategies.
Introduction
Systemic lupus erythematosus (SLE) predominantly affects women of reproductive age, constituting a significant gestational risk factor. Women with SLE are at increased risk of severe pregnancy complications, such as preeclampsia (PE), preterm delivery, fetal death, and several other adverse pregnancy outcomes (APOs) (1–4). Further, pregnancy can exacerbate disease manifestations leading to SLE flares and irreversible organ damage, contributing to considerable maternal morbidity (5–7).
Thromboembolic manifestations are common during SLE pregnancy, as shown by several studies (8–10). The underlying hemostatic disturbances during SLE pregnancy are poorly studied, despite the known propensity to develop a hypercoagulable state during the gestation period, as also shown in healthy women (11). Recently, in a study on the global hemostatic potential, we demonstrated enhanced coagulation and impaired fibrinolysis in healthy women suffering from PE during the third gestational trimester (12). As patients with SLE have an increased risk for PE development, we hypothesized that similar findings could contribute to adverse pregnancy outcomes in SLE pregnancy.
Antiphospholipid antibodies (aPL) and lupus nephritis (LN) significantly contribute to fetal and maternal complications and are known risk factors for the development of PE (13, 14). In addition, positivity for aPL further enhances the risk for thromboembolic complications during pregnancy (15). In a previous study, we demonstrated an increased risk of PE specifically in women with LN compared to patients with non-renal SLE (26 vs. 3%), regardless of the presence of concurrent antenatal flares (16).
This study aimed to investigate hemostatic variables in pregnant women with SLE in relation to the use of anticoagulant prophylaxis, aPL status, and development of thromboembolic complications and PE.
Patients and methods
In total, 34 pregnant patients with SLE followed between 2019 and 2022 at the Rheumatology Clinic, Karolinska University Hospital, were included in the study. All the patients fulfilled the American College of Rheumatology (ACR) criteria and/or the Systemic Lupus International Collaborating Clinics for SLE (17, 18). Patients older than 18 years of age with an SLE diagnosis prior to conception who were followed during pregnancy at the SLE outpatient clinic were included. Clinical and laboratory data were collected and the patients were sampled during the first (weeks 10–12, T1) and the third (weeks 32–34, T3) trimester of gestation for research purposes.
Thus, 22 of the patients had samples taken during T1, of whom 2 miscarried, 28 patients were sampled in T3, and 16 patients had samples taken at both study timepoints.
As a control population, 80 pregnant healthy controls (HCs) who had been sampled during T3 of gestation were included (12). HCs scheduled for routine prenatal care visits during T3 were included in the study. All HCs had uncomplicated pregnancies and had no history of cardiovascular disease (CVD), venous thromboembolism (VTE), or treatment with antithrombotic or anticoagulant drugs.
All the participants had given their oral and written consent to participate, and the study was performed according to the Declaration of Helsinki. The study was approved by the Swedish Ethical Review Authority (2021-02559) and the local Ethics Committee of Gynaecology and Obstetrics Clinic “Narodni Front,” Belgrade, Serbia (24/5-1).
Clinical variables were retrieved from electronic medical records. This included age at conception, disease duration, occurrence of lupus nephritis (ever), ongoing immunosuppressing therapy, and a special focus on the use of anticoagulant therapy. The occurrence of secondary antiphospholipid syndrome (sAPS) defined according to the Sapporo criteria (19) was recorded.
We also retrieved data regarding disease activity 12 months before conception where active disease was defined as having a SLE Disease Activity Index 2000 (SLEDAI-2K) score >4 (20).
Blood sampling
Peripheral venous blood was collected in tubes containing clot activator or trisodium citrate. Serum and platelet-poor plasma (PPP) were obtained within 60 min of sampling by centrifugation at 2,000 g for 20 min at room temperature and then aliquoted and frozen at −80°C. The analyses of hemostatic parameters were performed at Karolinska Institutet, Department of Molecular Medicine and Surgery, Coagulation Laboratory.
Analysis of hemostatic parameters
Determination of overall hemostatic potential and turbidimetric parameters of fibrin clots in plasma
To assess overall hemostatic potential (OHP) in plasma, a modified assay described by He et al. was employed (21). The assay is based on the spectrophotometric registration of Absorbance (Abs) at 405 nm every 12 s for 60 min in recalcified plasma after the addition of a small amount of thrombin and tissue plasminogen activator (t-PA). Fibrin formation is calculated as the area under the curve (Abs-sum) and expressed as the OHP. Two additional parameters were also analyzed—overall coagulation potential (OCP), determined as the area under the fibrin aggregation curve obtained without the addition of t-PA, and the overall fibrinolytic potential (OFP), calculated as the difference between the two areas as OFP (%) = [(OCP − OHP)/OCP] × 100. The intra- and inter-assay coefficients of variation for OHP were 1.6% and 6.8% and for OCP were 1.2% and 5.7%, respectively. The reference range for OCP, OHP, and OFP was established at our laboratory and presented as 25th–75th percentile.
The turbidimetric curve for determination of OCP was used to assess fibrin clot density by the following parameters: “lag time,” measuring clotting time as the time-point when exponential growth of the curve starts; “max absorbance,” reflecting clot density calculated as the average value of three consecutive points where the curve reached a plateau; and the “slope,” measuring the polymerization rate of fibrin (22).
Determination of clot lysis time
The turbidimetric curve for the determination of OHP was used for the calculation of clot lysis time (CLT) and was defined as the time from the midpoint of the clear-to-maximum turbid transition to the midpoint of the maximum turbid-to-clear transition.
To study the effects of thrombin activatable fibrinolysis inhibitor (TAFI) on CLT, a specific TAFI potato tuber carboxy-peptidase inhibitor (PTCI) was added to plasma samples, to a final concentration of 50 μg/ml, and the OHP assay was performed. CLT was measured before and after PTCI addition and the difference (dCLT) was calculated.
Scanning electron microscopy of fibrin clots
The clots formed during fibrin generation were washed, fixed in 2.5% glutaraldehyde, and stored at 4°C. The specimens were analyzed in an Ultra 55 field emission scanning electron microscope (Carl Zeiss) and individual fiber thickness was measured as previously described (22). To visualize fibrin clots, two different magnifications were used, 1 µM and 300 nm, respectively.
Analyses of fibrinogen and D-dimer levels
Dade Thrombin Reagent Siemens, Germany, was used for the determination of fibrinogen concentration using the Caluss method in the patient group, while the modified Caluss method with Multifibren U reagent, Siemens, Germany, was used for measuring fibrinogen concentration in the control group. The INNOVANCE® (Siemens, Germany) D-Dimer Assay, a particle-enhanced immunoturbidimetric assay, was used for the quantitative determination of cross-linked fibrin degradation products (D-dimers).
Serology
Serologic analyses were performed in Clinical Immunology and Clinical Chemistry at the Karolinska University Hospital according to clinical routine. The panel for aPL assays comprised IgG and IgM isotypes for both anti-cardiolipin (aCL) and anti-beta2glycoprotein I (anti-beta2GPI) antibodies, and the functional lupus anticoagulant (LA) test. Anti-dsDNA antibodies were analyzed by immunofluorescence microscopy using Crithidia luciliae as the source of antigen.
Pregnancy outcome
Information regarding the development of PE or thrombotic or major bleeding events was retrieved from the medical records. PE was defined as gestational hypertension and new onset of proteinuria (≥300 mg/24 h) after 20 weeks of gestation (23). A major bleeding at delivery was defined as a hemorrhage of >500 ml in cases of vaginal delivery and >1,000 ml in C-section patients (24).
Statistics
Descriptive statistics was used for presentation of patient's characteristics as median (IQR). Fisher's exact test was used for testing continuous variables. The Mann–Whitney U-test was used for group comparisons and the results are presented as median (IQR). For comparison between two related groups, the Wilcoxon signed ranks test was used. Spearman's analysis was performed to examine correlations. For comparison between more than two groups, the Kruskal–Wallis test was computed. The p-value was significant if <0.05. Analyses were performed using the GraphPad program.
Results
The general characteristics of the patients and controls are presented in Table 1.
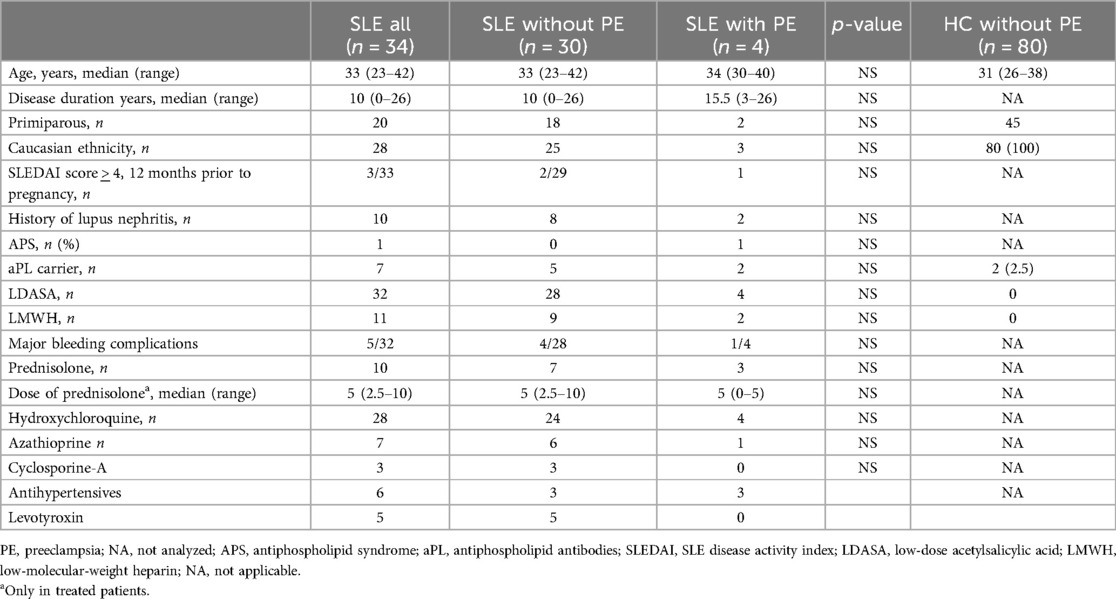
Table 1. Baseline characteristics of pregnant patients with SLE and pregnant healthy controls.
The median age at inclusion was 33 (range 23–42) years, and the median disease duration was 10 (range 0–26) years in the patients with SLE. The median age in the controls was 31 (26–38) years. In total, 29 patients (85%) were of Caucasian origin. None of the patients were smokers but one patient used smokeless tobacco (snuff). None of the patients developed gestational diabetes.
Furthermore, 20 of the patients were primiparous, 13 had one previous delivery, and 1 patient had two. One patient had a previous episode of hepatic vein thrombosis during a previous pregnancy and diagnosis of SLE/APS was established. Her pregnancy was medically terminated in the second trimester of pregnancy (here regarded as primiparous). Otherwise, there were no cases of PE during the previous pregnancies in the parous patients.
Three of 33 (10%) patients with available data were defined as having active disease the year before the pregnancy, of whom 1 developed PE. There was no association with active disease within 12 months of gestation and development of PE. Finally, 10/34 (29.4%) had a history of LN confirmed by a kidney biopsy in all but one case.
Treatment
Low-molecular-weight heparin (LMWH) was given in 11 cases. High-dose thromboprophylaxis was given twice daily to three patients and was guided by measurement of the nadir level of anti-factor Xa concentration according to clinical routines.
Eight patients received prophylactic LMWH once daily, the so-called low prophylactic dosage. Twenty-eight patients (82%) received hydroxychloroquine (HCQ) treatment and 32 (94%) low-dose acetylsalicylic acid (LDASA) (75 mg/day) during pregnancy. Ten patients were treated with prednisolone at a median dose of 5 mg/day (range 2.5–10). There was no statistical difference regarding the use of prednisolone when comparing PE and non-PE patients (p = 0.16). Ten of the patients (29%) were on immunosuppressing therapy, of whom seven received azathioprine and three cyclosporine-A (Table 1). Data on patients receiving LMWH are presented in Table 2.
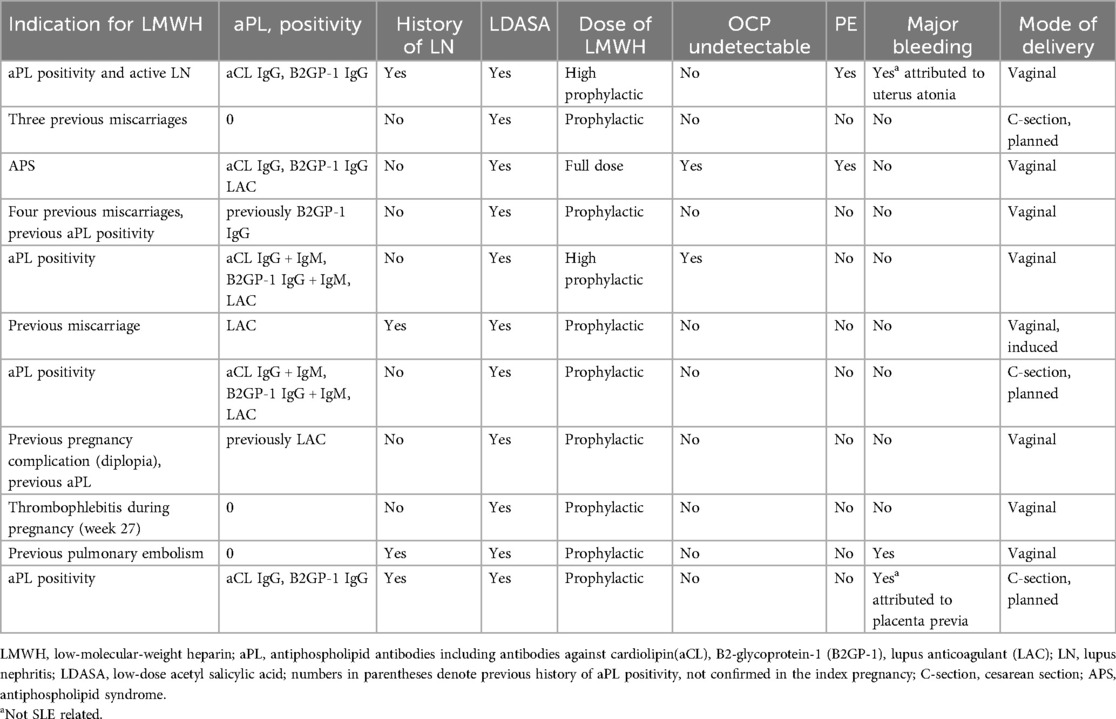
Table 2. Characteristics and complications in 11 patients treated with low-molecular-weight heparin.
Coagulation analyses
Data on coagulation variables were available in 22 patients in T1 and 28 in T3. In 16 cases, data was available in both T1 and T3. Of these 16 patients, 5 received LMWH prophylaxis.
Figure 1 presents the levels of coagulation parameters in 80 healthy pregnant women (HC) sampled during T3 and pregnant women with SLE in T1 and T3, while separate graphs show the same parameters in the 16 patients sampled in both T1 and T3.
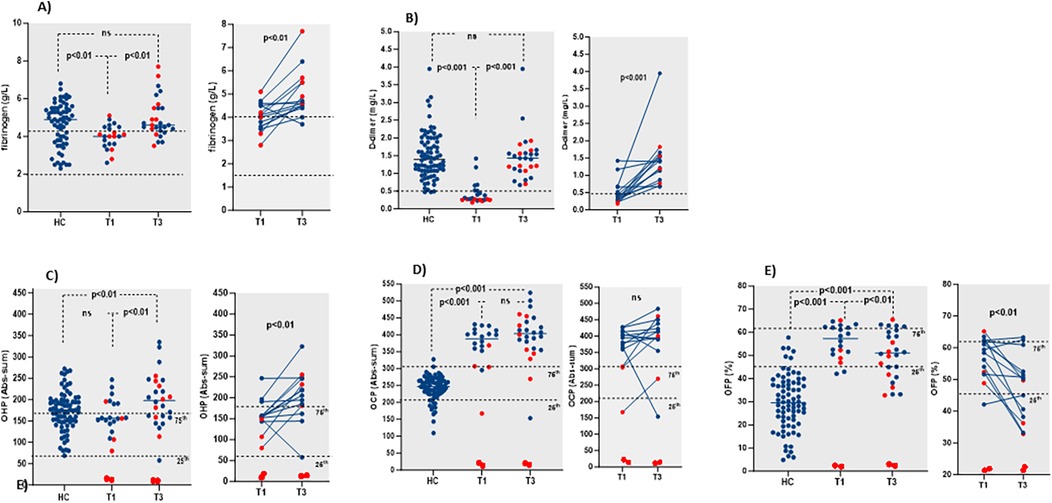
Figure 1. Hemostatic parameters (fibrinogen - (A), D-dimer - (B), OHP - (C), OCP - (D) and OFP - (E)) in all patients compared to healthy controls and in relation to LMWH treatment (left). Separate graphs in 16 patients with samples from both T1 and T3 (right). LMWH treated patients marked in red.
There was a significant increase in fibrinogen and D-dimer levels along with the pregnancy stage (p < 0.001, respectively). Fibrinogen levels in T1 (median 4.06; IQR 3.6–4.5) were within the reference range (2–4.5 g/L), while D-dimer (median 0.34; IQR 0.26–0.59) was under the cut-off (<0.5 mg/L) in most of the patients (Figures 1A,B). In T3, both fibrinogen (4.65; IQR 4.5–5.5) and D-dimer levels (1.41; IQR 1.0–1.56) increased above the upper reference ranges in all patients, since these parameters are unaffected by anticoagulant treatment. A significant increase was seen in both fibrinogen and D-dimer levels in patients sampled at both T1 and T3 (p < 0.01 and p < 0.001, respectively).
The OHP assay detected two completely anticoagulated patients with undetectable levels, both treated with high prophylactic doses of LMWH (Figure 1C, LMWH patients marked in red). In all patients treated with low prophylactic doses of LMWH, OHP was within the reference range in T1 (88–158) and increased above the upper reference range in T3. In the patients with detectable OHP levels, there was a significant increase of OHP from T1 to T3 (155.7; IQR 146.2–174.2 vs. 211.8; IQR 171.5–246.7, p < 0.01). A significant increase was seen in patients sampled at both pregnancy timepoints (p < 0.01) (right panel of Figure 1C).
OCP was also undetectable in two patients, as described above. In most of the patients with detectable OCP levels, OCP was above the reference range (213–304) in both T1 and T3 and increased along with the pregnancy stage (387.6; IQR 333.2–414.7 vs. 407.1; IQR 372.3–444.2), however, the increase was not significant (p = 0.15) (Figure 1D).
OFP decreased significantly from T1 to T3 (59; IQR 52%–62% vs. 50; IQR 37%–57%, p < 0.01), while the levels remained within the reference range (45%–61%) in most of the patients (Figure 1E).
CLT increased from T1 to T3, though not significantly (1,490; IQR 1,310–1,710 vs. 1,630; IQR 1,400–1,960, p = 0.2) and within the reference range (1,180–1,850 s). There was no difference between CLT in the HCs (1,533; IQR 1,338–1,685) compared to CLT in the SLE pregnancies in T1 and T3 (Table 3).
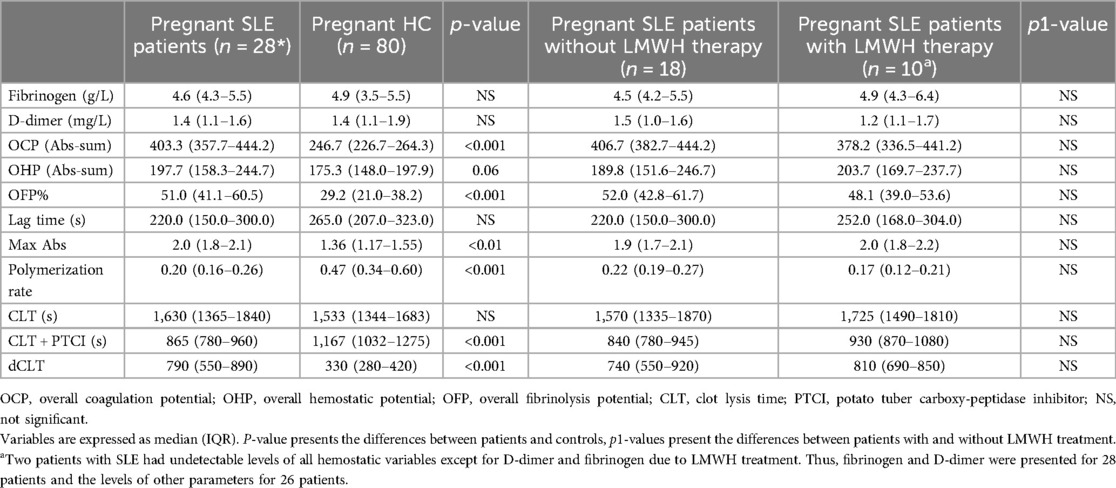
Table 3. Coagulation parameters in patients with SLE and HCs in the third trimester.
Coagulation parameters in 28 patients sampled in T3 compared to 80 healthy controls
Table 3 displays the levels of coagulation parameters in 28 pregnant women with SLE sampled in the third trimester and in 80 healthy pregnant women during the same gestational stage.
Ten patients (of a total of 11) treated with LMWH were sampled in T3. As described above, in two patients with a high prophylactic dosage of LMWH, all the investigated coagulation parameters were undetectable, except for fibrinogen and D-dimer. Thus, the results of fibrinogen and D-dimer are presented for a total of 28 patients, and the remaining parameters in 26 patients.
Fibrinogen and D-dimer did not differ between the whole group of patients and the controls. OCP was significantly increased in the patients with SLE (p < 0.001), while OHP was similar in both groups. OFP was higher in the patients with SLE (p < 0.001), however the CLT was not significantly prolonged. When PTCI was added, CLT was significantly shorter in the patient group compared to the control group (p < 0.001), thus dCLT was significantly higher (p < 0.001). There was a significant inverse correlation between dCLT and OFP in the patient group (r = −0.60; p < 0.01).
In total, the levels of all the investigated coagulation parameters did not differ between the patients receiving low-dose LMWH prophylaxis and those without Table 3.
There were no differences in the investigated hemostatic variables between the subgroups of patients with a history of LN and those without (data not shown). One patient with active proteinuria received high-dose LMWH prophylaxis and had undetectable levels of parameters investigated by OHP assay.
Pregnancy outcomes and coagulation parameters in patients with preeclampsia
Two patients had early miscarriages and were only studied at T1. Of the remaining 32 patients, four (12.5%) developed PE of whom two had a history of previous LN, one had sAPS, and the fourth had no known predisposition for PE development. Two of the PE patients were primiparous. The two parous patients had a history of gestational hypertension in their previous pregnancies but no further manifestations of PE.
The patient with sAPS was treated with a high prophylactic LMWH dose. One of the LN patients had active proteinuria and was also treated with a high prophylactic dose of LMWH. Two PE patients received LDASA only.
The levels of OCP, OHP, and OFP were undetectable in the patient with sAPS anticoagulated with a high prophylactic LMWH dose. One PE patient receiving a low prophylactic LMWH dose had levels of OCP within the reference range in both T1 and T3, with increasing tendency at T3. In the remaining two patients without LMWH, the OCP levels were above the reference range in both T1 and T3 (Figure 2D).
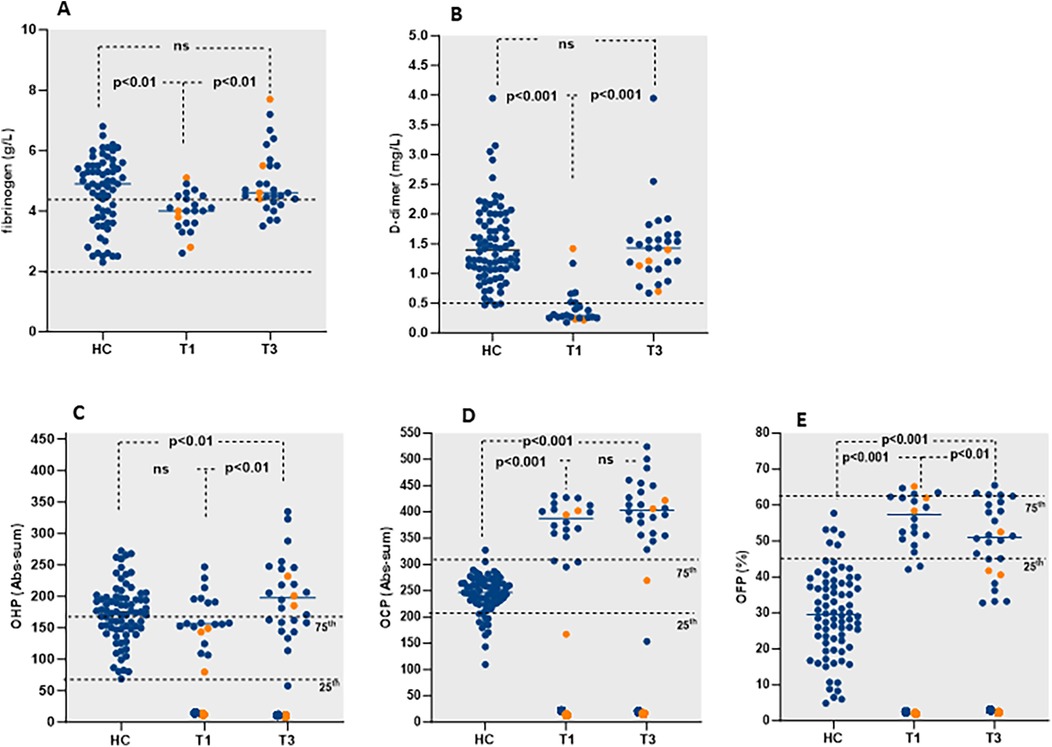
Figure 2. Fibrinogen (A), D-dimer (B), OHP (C), OCP (D) and OFP (E) levels in pregnant patients with SLE during first and third trimester of pregnancy and healthy controls. Patients with preeclampsia are marked in orange.
In T1, OHP was within the reference range in three patients (one with low-dose prophylactic LMWH) and increased above the reference range in T3 (Figure 2C). OFP levels decreased from T1 to T3 as demonstrated in Figure 2E.
There was no difference between the occurrence of LN, APS, or active disease prior to pregnancy when comparing patients with and without PE (data not shown). No thromboembolic episodes occurred during pregnancy.
Analysis of fibrin clot parameters clot structure
The parameters of fibrin clot formation indicated significantly increased Max Abs values and fibrin polymerization rate in the patients with SLE sampled in T3 compared to the HCs (Table 3).
Fibrin clots were analyzed in T1 and T3 in three representative patients with SLE. Scanning electron microscopy (SEM) showed that the fibrin clots in T3 had thinner fibers (mean density 0.28 ± 0.05 μm/fiber) with a denser structure and smaller intrinsic pores compared to the clots created from plasma samples taken during T1 (mean density 0.33 ± 0.02 μm/fiber). The fibrin clot from a patient receiving high-dose prophylactic LMWH during T3 was comprised of thick fibers (mean density 0.63 ± 0.10 μm/fiber) and as such was more prone to fibrinolysis (Figure 3).
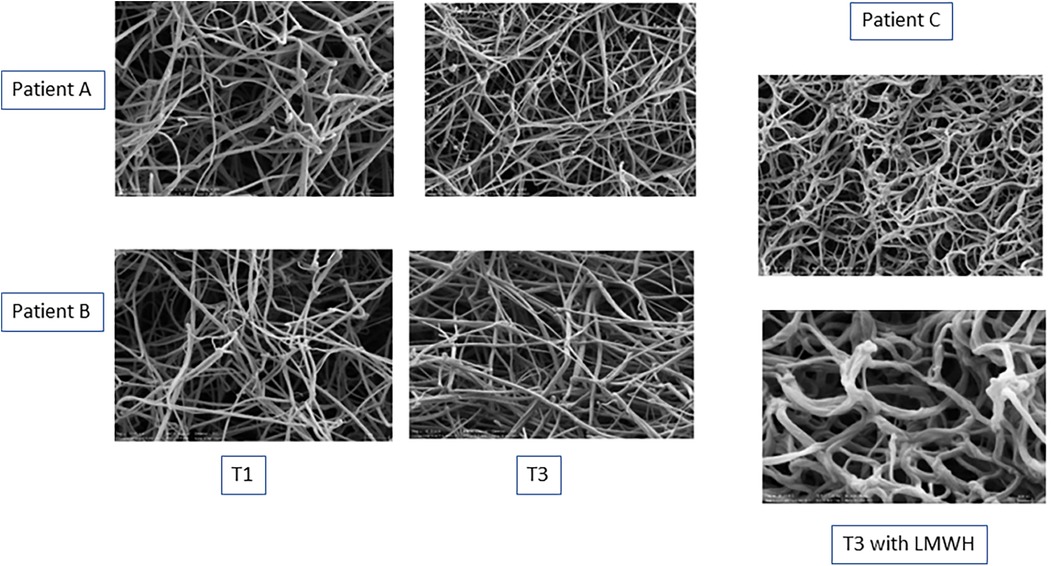
Figure 3. SEM images of representative fibrin clots in two pregnant women with SLE during T1 and T3 (patients A and B). A magnification of 1 μm was used for these images. SEM images of a fibrin clot from a patient treated with a prophylactic dose of LMWH during T3 (patient C). A magnification of 1 μm and 200 nm was used for these images.
Serology
Anti-dsDNA antibodies were positive in 12/34 (35%) patients in T1 and continued to be persistently positive during the pregnancies (one missing data and one miscarried). None of the patients negative for anti-dsDNA antibodies in T1 had increasing titers during their pregnancy. Positive anti-dsDNA antibodies were found in one of the patients who developed PE.
aPL was positive in seven patients, of whom only one was diagnosed with APS due to a previous arterial thrombotic event. Two patients had a previous history of aPL positivity at low titers but were negative during the current pregnancy. All patients with aPL but one received prophylactic treatment with LMWH: the patient not receiving treatment was the single positive at a low titer for IgG anti-B2GP-I.
Delivery mode and bleeding complications at delivery
Of the 32 patients with full term pregnancies, 23 delivered vaginally (one instrumentally) and 9 by C-section, either planned (n = 6) or emergent (n = 3). Major bleeding as defined above occurred in 5 of all 32 (15.6%) successful pregnancies. Of these bleeding events, 3/23 (13%) were seen in patients with vaginal delivery, of which two were on LMWH. One patient had received a low prophylactic dose of LMWH and the other patient, with a high prophylactic dose, had a bleeding attributed to uterus atonia. Two out of nine (22.2%) patients with C-sections suffered from major bleeding complications. Of these, one was on LMWH and had a C-section due to placenta previa (Table 2).
Discussion
In this study, we investigated hemostatic parameters in pregnant women with SLE in early and late gestation in association with the use of anticoagulant therapy and the development of PE and thrombotic complications. To the best of our knowledge, this is the first study investigating hemostatic variables during SLE pregnancy. In general, hemostatic alterations toward enhanced coagulation were found in SLE pregnancy compared to healthy pregnant women. In contrast to the parameters of the OHP assay, routine analyses of fibrinogen and D-dimer were not useful for monitoring the effect of LMWH in treated patients.
Pregnancy is recognized as a major risk factor for thromboembolism, with pregnant women being up to six times more likely to develop VTE compared with the general population (25). Thromboembolic complications during pregnancy contribute significantly to maternal morbidity and treatment burden in SLE. A large meta-analysis demonstrated a risk ratio of 11 for the occurrence of thromboembolism during SLE pregnancy as compared to pregnant women without SLE (8). None of the patients included in our study developed thrombotic complications, though enhanced coagulation was found already in early pregnancy and increased over time.
A large proportion of the patients had significantly elevated OCP, OHP, and OFP levels in the third trimester compared to the healthy pregnant women. Yet, the women with SLE had comparably lower OHP during early pregnancy than the healthy controls in the third trimester, pointing toward the importance of sample timing for the interpretation of results. The levels of fibrinogen and D-dimer also increased during pregnancy, yet without differences between the patients with SLE and healthy women in the third trimester of pregnancy. Not unexpectedly, a large individual variation was noted in the markers as we have chosen to display the results of all hemostatic parameters from real-life settings during SLE pregnancies without omitting outliers.
Despite a high prophylactic LMWH dose and LDASA in risk individuals, PE occurred in two cases of which one did not achieve a significant reduction of OCP, OHP, and OFP (for detailed information on the LMWH-treated patients, see Table 2). Overall, the response to the prophylactic LMWH regimen was variable and none of the patients treated with low prophylactic doses achieved a significant anticoagulation measured by the parameters of the OHP assay. The routine coagulation parameters fibrinogen and D-dimer were not affected by LMWH prophylaxis.
The representative fibrin clot images of two patients showed denser clots composed of thinner fibers in T3 compared to T1, revealing the formation of prothrombotic clots during pregnancy in patients with SLE. The increased fibrin polymerization rate indicated faster fibrin formation and Max Abs confirmed higher fibrin density in T3 compared to the healthy controls sampled at the same gestation stage. These clots were more difficult to lyse, however, the CLT did not differ between the healthy pregnant women and SLE pregnancy in our study. This might be due to the increased TAFI activation demonstrated by increased dCLT in the patients with SLE compared to the controls. TAFI (carboxy-peptidase B) is an enzyme involved in both coagulation and fibrinolysis (26) and TAFI activation due to enhanced thrombin formation inhibits fibrinolysis, as reflected by the inverse association between dCLT and OFP in the pregnant patients with SLE. However, OFP levels in patients with SLE were elevated compared to the HCs, indicating that other factors may be involved in the overall regulation of the fibrinolytic process during SLE pregnancy, which should be an objective of a larger study.
In one patient treated with a high prophylactic dose of LMWH, SEM images revealed a fibrin clot formed of thicker fibers and larger intrinsic pores. LMWH and LDASA are known to influence fibrin structure and may lead to increased porosity of fibrin clots and enhanced fibrinolysis (27, 28). However, we could not observe a difference in OFP and CLT between patients treated prophylactically with LMWH and the rest of the patients in our study. Further, despite LDASA, fibrin structure was changed toward a prothrombotic pattern during gestation. This may further support our observation that LDASA and prophylactic LMWH are not sufficient to achieve significant anticoagulation in pregnant patients with SLE.
We found a prevalence of PE of 12.5%, thus a similar frequency as previously reported in pregnant women with SLE (4, 6), although higher frequencies (13%–35%) have also been reported (29). A history of lupus nephritis, chronic hypertension, disease activity before and at conception, and sAPS are known risk factors for PE development in SLE (14). In our cohort, the patient with sAPS with significant anticoagulation developed PE despite full dose LMWH, LDASA, and HCQ treatment. Thus, additional treatment modalities are still warranted to prevent PE development.
No previous PE had occurred in the 14 parous patients. In the two patients who developed PE in their second pregnancy, gestational hypertension was present in the late stages of the previous pregnancies, of whom one also had a previous history of LN. Neither of these two cases had been given LMWH as prophylactic therapy, and LDASA treatment was here not found to be protective for PE development. The use of HCQ, given here to most patients, was in a recent publication not confirmed to decrease the risk for PE development (30).
Prevention of PE and close monitoring of patients at risk are central in the care of pregnant patients with SLE. Furthermore, in a long-term follow-up, women with SLE experiencing hypertensive disorders of pregnancy, including PE, are at increased risk of developing CVD later in life (31). Thus, women with SLE who have developed PE should be closely monitored for hypertension and other CVD risk factors and subjected to vigorous prophylactic treatment to protect them from later vascular events (32, 33).
Major bleeding complications were seen in 5/32 (15.6%) in the total patient population, of which three were treated with LMWH, in all cases given in combination with LDASA. However, other obstetric complications could also have contributed to the hemorrhages and despite anticoagulant treatment, we found no clear signal of increased bleeding risks in our study population. A majority of patients were on LDASA which was not found to increase the rate of severe hemorrhage. However, the numbers are small, and firm conclusions cannot be drawn from the present study.
The major limitation of this study is the small sample size, as larger studies in all trimesters may increase our understanding of the effects of anticoagulation on the risk for bleeding complications, PE development, and prevention of thromboembolism. Our study was performed in a single center, where most of the patients were of Caucasian ethnicity, thus hemostatic alterations may differ between different ethnic groups. In addition, patient data were sourced from clinical records retrospectively, which may have affected data consistency and follow-up compliance. Furthermore, we did not analyze whether the altered hemostatic balance had an impact on fetal outcomes, and no comparison between conventional assays and the OHP/OCP results was performed.
Although all the patients were closely monitored by specialists in obstetrics and rheumatologists in collaboration, compliance to treatment must be considered when evaluating the effects of treatment. The method for the coagulation analysis used in the present study is not routinely available and needs to be automatized to be used in clinical practice to fully monitor the effects of anticoagulant treatment. However, by using this method, we clearly demonstrate that a prothrombotic condition is present among pregnant patients with SLE, which was not captured by conventional assays.
In summary, in this exploratory pilot study aiming at investigating hemostatic alteration in a pregnant SLE population, we found a clear procoagulant state which may have an impact on the risk for the development of PE and thromboembolism. Prophylactic treatment with LMWH was safe regarding bleeding complications but did not ameliorate the hemostatic disturbances. Monitoring of hemostatic alterations may improve personalized treatment strategies in patients at risk.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Swedish Ethical Review Authority and Ethics Committee of Gynaecology and Obstetrics Clinic “Narodni Front”, Belgrade, Serbia. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AA: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Writing – original draft, Writing – review & editing. DL: Formal Analysis, Investigation, Methodology, Writing – review & editing. NS: Formal Analysis, Investigation, Methodology, Writing – review & editing. SL-C: Formal Analysis, Investigation, Methodology, Writing – review & editing. AZ: Writing – review & editing. AM: Writing – review & editing. KB: Conceptualization, Writing – review & editing. MS: Conceptualization, Investigation, Writing – review & editing. FF: Writing – review & editing. ES: Conceptualization, Supervision, Writing – review & editing. LA: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing. IG: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Peart E, Clowse ME. Systemic lupus erythematosus and pregnancy outcomes: an update and review of the literature. Curr Opin Rheumatol. (2014) 26(2):118–23. doi: 10.1097/BOR.0000000000000030
2. Andreoli L, Fredi M, Nalli C, Reggia R, Lojacono A, Motta M, et al. Pregnancy implications for systemic lupus erythematosus and the antiphospholipid syndrome. J Autoimmun. (2012) 38(2–3):J197–208. doi: 10.1016/j.jaut.2011.11.010
3. Clowse ME, Jamison M, Myers E, James AH. A national study of the complications of lupus in pregnancy. Am J Obstet Gynecol. (2008) 199(2):127e1–6. doi: 10.1016/j.ajog.2008.03.012
4. Arkema EV, Palmsten K, Sjowall C, Svenungsson E, Salmon JE, Simard JF. What to expect when expecting with systemic lupus erythematosus (SLE): a population-based study of maternal and fetal outcomes in SLE and Pre-SLE. Arthritis Care Res. (2016) 68(7):988–94. doi: 10.1002/acr.22791
5. Ruiz-Irastorza G, Lima F, Alves J, Khamashta MA, Simpson J, Hughes GR, et al. Increased rate of lupus flare during pregnancy and the puerperium: a prospective study of 78 pregnancies. Br J Rheumatol. (1996) 35(2):133–8. doi: 10.1093/rheumatology/35.2.133
6. Smyth A, Oliveira GH, Lahr BD, Bailey KR, Norby SM, Garovic VD. A systematic review and meta-analysis of pregnancy outcomes in patients with systemic lupus erythematosus and lupus nephritis. Clin J Am Soc Nephrol. (2010) 5(11):2060–8. doi: 10.2215/CJN.00240110
7. Moroni G, Doria A, Giglio E, Imbasciati E, Tani C, Zen M, et al. Maternal outcome in pregnant women with lupus nephritis. A prospective multicenter study. J Autoimmun. (2016) 74:194–200. doi: 10.1016/j.jaut.2016.06.012
8. Bundhun PK, Soogund MZ, Huang F. Impact of systemic lupus erythematosus on maternal and fetal outcomes following pregnancy: a meta-analysis of studies published between years 2001–2016. J Autoimmun. (2017) 79:17–27. doi: 10.1016/j.jaut.2017.02.009
9. Nili F, McLeod L, O'Connell C, Sutton E, McMillan D. Maternal and neonatal outcomes in pregnancies complicated by systemic lupus erythematosus: a population-based study. J Obstet Gynaecol Can. (2013) 35(4):323–8. doi: 10.1016/S1701-2163(15)30959-2
10. Wallenius M, Salvesen KA, Daltveit AK, Skomsvoll JF. Systemic lupus erythematosus and outcomes in first and subsequent births based on data from a national birth registry. Arthritis Care Res. (2014) 66(11):1718–24. doi: 10.1002/acr.22373
11. Kilkenny K, Frishman W. Venous thromboembolism in pregnancy: a review of diagnosis, management, and prevention. Cardiol Rev. (2024). doi: 10.1097/CRD.0000000000000756
12. Lalic-Cosic S, Dopsaj V, Kovac M, Pruner I, Littmann K, Mandic-Markovic V, et al. Evaluation of global haemostatic assays and fibrin structure in patients with pre-eclampsia. Int J Lab Hematol. (2020) 42(3):322–30. doi: 10.1111/ijlh.13183
13. Gamba A, Zen M, Depascale R, Calligaro A, Gatto M, Iaccarino L, et al. Modern management of pregnancy in systemic lupus erythematosus: from prenatal counseling to postpartum support. J Clin Med. (2024) 13(12):3454. doi: 10.3390/jcm13123454
14. Wind M, Fierro JJ, Bloemenkamp KWM, de Leeuw K, Lely AT, Limper M, et al. Pregnancy outcome predictors in systemic lupus erythematosus: a systematic review and meta-analysis. Lancet Rheumatol. (2024) 6(10):e667–e83. doi: 10.1016/S2665-9913(24)00160-7
15. Andreoli L, Bertsias GK, Agmon-Levin N, Brown S, Cervera R, Costedoat-Chalumeau N, et al. EULAR Recommendations for women’s health and the management of family planning, assisted reproduction, pregnancy and menopause in patients with systemic lupus erythematosus and/or antiphospholipid syndrome. Ann Rheum Dis. (2017) 76(3):476–85. doi: 10.1136/annrheumdis-2016-209770
16. Bremme K, Honkanen S, Gunnarsson I, Chaireti R. The presence of lupus nephritis additionally increases the risk of preeclampsia among pregnant women with systemic lupus erythematosus. Lupus. (2021) 30(7):1031–8. doi: 10.1177/09612033211004716
17. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF, et al. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. (1982) 25(11):1271–7. doi: 10.1002/art.1780251101
18. Petri M, Orbai AM, Alarcon GS, Gordon C, Merrill JT, Fortin PR, et al. Derivation and validation of the systemic lupus international collaborating clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. (2012) 64(8):2677–86. doi: 10.1002/art.34473
19. Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL, Cervera R, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. (2006) 4(2):295–306. doi: 10.1111/j.1538-7836.2006.01753.x
20. Gladman DD, Ibanez D, Urowitz MB. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. (2002) 29(2):288–91.11838846
21. He S, Antovic A, Blomback M. A simple and rapid laboratory method for determination of haemostasis potential in plasma. II. Modifications for use in routine laboratories and research work. Thromb Res. (2001) 103(5):355–61. doi: 10.1016/S0049-3848(01)00332-2
22. Pruner I, Farm M, Tomic B, Gvozdenov M, Kovac M, Miljic P, et al. The silence speaks, but we do not listen: synonymous c.1824C>T gene variant in the last exon of the prothrombin gene as a new prothrombotic risk factor. Clin Chem. (2020) 66(2):379–89. doi: 10.1093/clinchem/hvz015
23. Brown MA, Lindheimer MD, de Swiet M, Van Assche A, Moutquin JM. The classification and diagnosis of the hypertensive disorders of pregnancy: statement from the international society for the study of hypertension in pregnancy (ISSHP). Hypertens Pregnancy. (2001) 20(1):IX–XIV. doi: 10.1081/PRG-100104165
24. Lalonde A, International Federation of G, Obstetrics. Prevention and treatment of postpartum hemorrhage in low-resource settings. Int J Gynaecol Obstet. (2012) 117(2):108–18. doi: 10.1016/j.ijgo.2012.03.001
25. Nichols KM, Henkin S, Creager MA. Venous thromboembolism associated with pregnancy: JACC focus seminar. J Am Coll Cardiol. (2020) 76(18):2128–41. doi: 10.1016/j.jacc.2020.06.090
26. Redlitz A, Tan AK, Eaton DL, Plow EF. Plasma carboxypeptidases as regulators of the plasminogen system. J Clin Invest. (1995) 96(5):2534–8. doi: 10.1172/JCI118315
27. Li N, He S, Blomback M, Hjemdahl P. Platelet activity, coagulation, and fibrinolysis during exercise in healthy males: effects of thrombin inhibition by argatroban and enoxaparin. Arterioscler Thromb Vasc Biol. (2007) 27(2):407–13. doi: 10.1161/01.ATV.0000253906.19648.ac
28. Antovic A, Perneby C, Ekman GJ, Wallen HN, Hjemdahl P, Blombäck M, et al. Marked increase of fibrin gel permeability with very low dose ASA treatment. Thromb Res. (2005) 116(6):509–17. doi: 10.1016/j.thromres.2005.02.007
29. Clowse ME. Lupus activity in pregnancy. Rheum Dis Clin North Am. (2007) 33(2):237–52. doi: 10.1016/j.rdc.2007.01.002
30. Rector A, Maric I, Chaichian Y, Chakravarty E, Cantu M, Weisman MH, et al. Hydroxychloroquine in lupus pregnancy and risk of preeclampsia. Arthritis Rheumatol. (2024) 76(6):919–27. doi: 10.1002/art.42793
31. Simard JF, Rossides M, Arkema EV, Svenungsson E, Wikstrom AK, Mittleman MA, et al. Maternal hypertensive disorders in pregnant women with systemic lupus erythematosus and future cardiovascular outcomes. Arthritis Care Res. (2021) 73(4):574–9. doi: 10.1002/acr.24160
32. Gustafsson JT, Simard JF, Gunnarsson I, Elvin K, Lundberg IE, Hansson LO, et al. Risk factors for cardiovascular mortality in patients with systemic lupus erythematosus, a prospective cohort study. Arthritis Res Ther. (2012) 14(2):R46. doi: 10.1186/ar3759
Keywords: systemic lupus erythematosus, pregnancy, anticoagulant treatment, preeclampsia, global hemostasis assay
Citation: Antovic A, Lini D, Soutari N, Lalic-Cosic S, Zickert A, Mc Nicholas A, Bremme K, Sennström M, Franceschini F, Svenungsson E, Andreoli L and Gunnarsson I (2025) Altered hemostatic balance in favor of a procoagulant state in pregnant women with systemic lupus erythematosus. Front. Lupus 2:1511382. doi: 10.3389/flupu.2024.1511382
Received: 14 October 2024; Accepted: 26 December 2024;
Published: 30 January 2025.
Edited by:
Alessandra Bettiol, University of Florence, ItalyCopyright: © 2025 Antovic, Lini, Soutari, Lalic-Cosic, Zickert, Mc Nicholas, Bremme, Sennström, Franceschini, Svenungsson, Andreoli and Gunnarsson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aleksandra Antovic, YWxla3NhbmRyYS5hbnRvdmljQGtpLnNl
†These authors have contributed equally to this work