 Ingrid Rekaa Nilssen
Ingrid Rekaa Nilssen Hege Svean Koksvik
Hege Svean Koksvik Bente Jakobsen
Bente Jakobsen Kjersti Grønning
Kjersti Grønning- 1Norwegian National Network for Pregnancy and Rheumatic Diseases, Department of Rheumatology, St Olavs Hospital Trondheim University Hospital, Trondheim, Norway
- 2Department of Research, Nord-Trøndelag Hospital Trust, Levanger, Norway
- 3Department of Public Health and Nursing, The Norwegian University of Science and Technology, Trondheim, Norway
Objective: Inflammatory arthritis (IA) often come with symptoms of pain, stiffness and fatigue, as well as fluctuating and unpredictable disease patterns. All of these symptoms can cause challenges in the role as a mother for women with IA. The main objective of this study is to gain a broader understanding of how mothers with IA experience motherhood and the challenges they encounter within a biopsychosocial framework.
Methods: The participants in this study were recruited through RevNatus, a Norwegian nationwide quality register. The sample consisted of women with IA who had given birth within the last 5 years. The data consisted of written answers to an open-ended question: “Is there anything, in particular, you have experienced as challenging with being a mother and having a rheumatic disease at the same time”? The data were analysed following Brinkmann and Kvale's qualitative content analysis.
Results: 186 women answered the open-ended question. The responses consisted of a total of 9,000 words. Motherhood with IA was described as a difficult balancing act, with practical and physical challenges affecting day-to-day life, medical dilemmas, as well as challenges on a deeper emotional level and worries for the future.
Conclusion: The main finding in this study is that the challenges these women meet are multifactorial and complex, including physical, mental and social issues that have a large impact on their everyday life. Focusing solely on improving medical treatment will not solve the challenges these women face. A multidisciplinary approach and focus on patient education and self-management strategies is important to help these women thrive in their role as mothers with IA.
1 Introduction
Inflammatory arthritis (IA) is a term used to describe a heterogeneous group of chronic autoimmune diseases characterised by joint inflammation, such as rheumatoid arthritis, juvenile idiopathic arthritis, spondyloarthritis and psoriatic arthritis (1). Pain, stiffness and fatigue are common symptoms in IA, as well as fluctuating and unpredictable disease patterns (1, 2). All of these symptoms can cause challenges in the role as a mother for women with IA (3).
Very few women with IA are advised against having children, as we now have more effective treatment and less severe disease manifestations (4). Still, several studies show that IA is associated with higher rates of childlessness, and many women with IA have fewer children than desired (5–8). The reason behind this may be multifaceted with physical, psychological, social, hormonal, immunological, medical and personal challenges contributing (8–10).
The biopsychosocial model, a well-established framework, describes how biological, psychological and social factors interact and affect one another, contributing to a person's experience of his or her overall health (11). This model can help us understand the complexity of living with chronic diseases, such as IA, where biological (e.g., inflammation, sleep deprivation, pain) psychological (e.g., worrying, unpredictability, vulnerability) and social (e.g., living situation, work, family, support) factors dynamically and reciprocally affect one another. In the same way, this model can also be useful to understand the experience of motherhood, regardless of chronic disease, as a multifaceted experience where biological/physical (e.g., physical changes due to pregnancy and labour, sleep deprivation), psychological (e.g., increased vulnerability, expectations) and social (social network, family, work) factors all come in to play.
The vast majority of research on pregnancy and rheumatic diseases focus on medical treatment, risk factors, and pregnancy outcomes. There are some qualitative studies focusing on women's experiences related to pregnancy and the postpartum period, and the number is growing (10, 12–18). The qualitative studies have provided important in-depth insight into how the women experience motherhood while living with IA, and the challenges these women have to cope with. However many of these studies are more than ten years old. There has been a massive development both within the field of rheumatology in general and specifically relating to pregnancy and rheumatic diseases. Access to medical treatment for people with IA, including biologics when indicated is much better than ten-twenty years ago (4, 19, 20).
Having better insight into the possible challenges these women face in their life as mothers with IA can potentially improve patient/clinician communication, and be of great value when developing health services and resources to best support and guide them through this very important part of life.
The aim of this study is thus to gain a broader understanding of how mothers with IA experience motherhood and the challenges they encounter in a biopsychosocial framework.
2 Materials and methods
2.1 Study population
This qualitative study is nested within a larger Norwegian study not yet published, looking at health related quality of life in mothers with IA. Patients were recruited through RevNatus, a nationwide quality register where 17 out of 20 rheumatology departments across Norway contribute with data (21). RevNatus consists of data from women who are 16 years or older with an inflammatory rheumatic disease, who are planning pregnancy or are pregnant. Participants were eligible for this study if they were included in the register and fulfilled the diagnostic- or classification criteria for one of the following diagnosis M05.8, M05.9, M06.0, M07.3+ L40.5, M45, M46.8, M46.9, M08.0 or M08.9, and had registered a live birth within 5 years from 19th of august 2019.
Eligible patients received a letter in the mail with an invitation to participate in the study. After signing an informed consent, the participants answered a questionnaire including an open-ended question aiming to collect in-depth information about perceived challenges related to motherhood and rheumatic disease: “Is there anything, in particular, you have experienced as challenging with being a mother and having a rheumatic disease at the same time?”.
Age, diagnosis and disease duration were retrieved from RevNatus while educational status, number of children and months since last childbirth were self-reported through the questionnaire.
The data collection found place autumn 2019.
2.2 Data analysis
The responses consisted of a total of 9,000 words and were analysed as described by Brinkmann and Kvale (22). The first, third and last author inductively read and coded all the responses. The research team had several meetings to discuss the content and labels of the codes, during which different interpretations were developed until a consensus of interpretation was reached. The final analytical themes were agreed upon by comparing (finding similarities) and contrasting (searching for negative cases) codes. After reaching an agreement of the main themes, two of the authors went back and read thorough all written responses to see if all important aspects were covered by the themes as agreed upon, in addition to selecting quotes best illustrating the themes.
2.3 Research team
The research team consist of four females (3 MSc and one professor). All are trained nurses with extensive experience within rheumatology. Three out of four are currently working clinically specializing in pregnancy and rheumatic disease.
2.4 Ethics and patient involvement
Participation in the study was voluntary, and all participants signed a written informed consent. The study was approved by REK Sout/East Norway in April 2019 (2019/817/REK sor-ost). Continuous dialogue with two patient representatives have been important during the course of the project.
3 Results
Of the 375 questionnaires sent out, 233 questionnaires were returned, and three letters were returned because of incorrect address, i.e., 62% of eligible subjects responded. 186 of these 233 (80%) answered the open-ended question that this study is based upon. The remaining 47 (20%) left the open-ended question blank and only filled out the questions related to health related quality of life, which is investigated in a separate study.
Table 1 shows the demographic data of the women who responded to the open-ended question. Characteristics of the study population are presented as means and standard deviations or raw numbers and percentages.
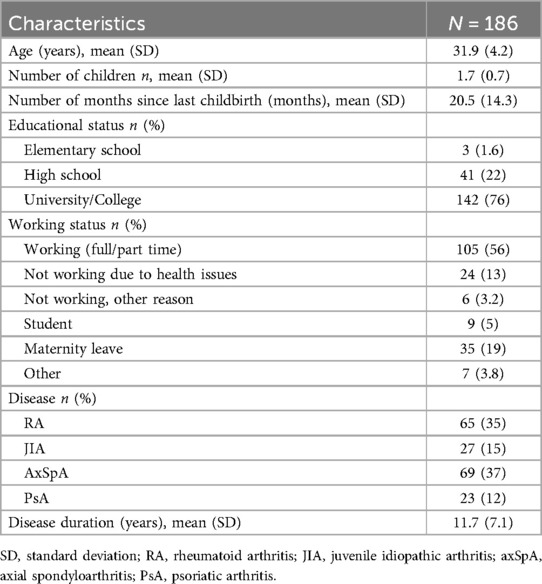
Table 1. Characteristics of study population.
3.1 Qualitative findings
The written answers from the open-ended question gave valuable insight to the challenges of motherhood for women with IA. Despite having focus on early diagnosis and good treatment options, mothers with rheumatic disease still describe many challenges related to motherhood.
When analysing the data it became apparent that being a mother with IA is a multifaceted experience. As both motherhood and having an IA diagnosis affects nearly all aspects of these women's lives, they sometimes experienced it as a balancing act. The women described practical and physical challenges that affected their day-to-day life, medical dilemmas, as well as challenges on a deeper emotional level and worries for the future.
One women described it in the following way, summing up many of the challenges these women encompassed, physically and emotionally:
“A lot of things. Where to start? Everything from not being able to breastfeed after giving birth (due to medications) and not being able to take care of the children (holding them,carrying them, picking them up at night). Dad had to take over. Of course it’s sad not being able to participate in activities and join them on trips to the extent I want when they’re growing up. Many thoughts on their dad. Afraid the kids will look back and think that I didn’t want to be involved” (#25, RA, three children- twins age 5 years and a baby age 1 month).
Two women described the difficult balancing act and feeling of “double trouble” when combining motherhood with a chronic disease as this:
“It’s challenging to be tired from having a toddler and being sick at the same time. I’m fully depended on my husband, who has been absolutely fantastic, not to break down” (#130, SpA, one child age 10 months).
“Lack of sleep is probably normal when having small children, but when the bechterew disease also wakes you up at night, it can be challenging” (#120, SpA, one child age 2 years).
The difficult balancing act stands out as an overarching main theme that is further divided into five sub-main themes as illustrated in Table 2, and described in further detail below.
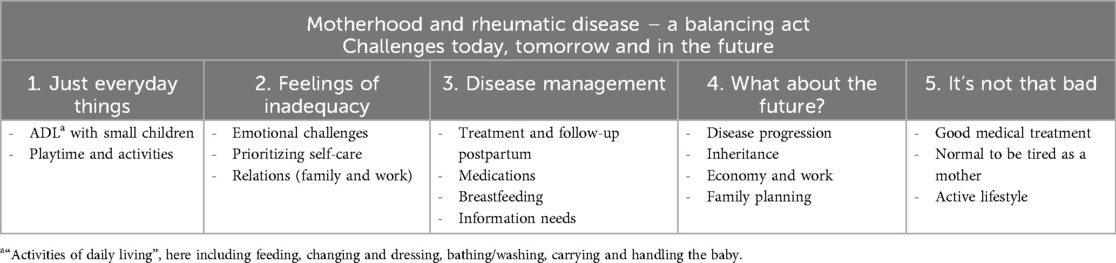
Table 2. Qualitative results- main and subthemes.
3.1.1 “Just everyday things”
Many women described how their disease, with symptoms such as pain, stiffness and fatigue, made everyday chores, as well as playtime and participating in activities with their children challenging. Having some physical limitations and difficulties with practical task was something that many of the women experienced to varying degrees since they developed IA. However, having challenges that affected their abilities to take care of their babies were described as a difficult and painful experience.
“To sit down/bend down to the child, both during play and when dressing the child. Carrying/lifting the child, fastening in the car seat. Sitting down on the floor to play with the child. It is emotionally difficult when the child (and myself) have an expectation to do something, which is not possible due to physical limitations and pain, but which really is just everyday tasks such as dressing, playing, bending down to the child and so on. Of course, in most situation you will find alternative ways to do things, which might be a bit untraditional, but that works. But it’s difficult at times to be a “different” mum, than “every other” mum. And baby-food, bottles, baby clothes should often have been more universally designed. I learned to avoid certain things because I had extra trouble with opening/buttoning etc.” (#61, JIA, one child age 2 years).
Some felt that the challenges in relation to handling the baby grew as the children grew bigger:
“Now that the child is bigger everything has gotten more difficult: holding her, putting her to bed, bathing her…yes, basically everything. Lack power and strength and get a lot of pain after various tasks with her” (#151, SpA, one child age 8 months).
Activities and playtime also change, as the children grow older. For mothers who are struggling with pain and fatigue it can be difficult to keep up with the high level of energy and physical demands, as this woman explained:
“Being tired, not having the energy to play, going for a walks, running after a bike and so on. This means there is less of these activities than what is normal. The child must be taken care of by others/their dad on days when everything is painful and tiring. It hurts not being able to take care of your own child all of the time” (#12, RA, one child age 4 years).
3.1.2 Feelings of inadequacy
Many women conveyed a strong feeling of inadequacy. This feeling was related to various aspects of their life as a mother with IA.
3.1.2.1 Emotional challenges
Not being able to be the mother they had pictured, and having trouble controlling their emotions due to pain and fatigue triggered many women to feel inadequate in their new role.
One mother expressed it like this:
“It’s a bit mentally challenging to realize you have limitations due to your illness that affect/will affect being a fully present mother. Feels like I'm failing somewhat in a role that I have chosen myself” (#130, SpA, one child age 10 months).
Another like this:
“You feel like you are never good enough, having to say no to things that the children wants to do because you're simply in too much pain, and are always tired and exhausted. Spend a lot of energy pulling yourself together, so that the children don't see how much you’re struggling with pain (…) You constantly have to pull yourself together on the worst days, so that you don't get angry with your kids and yell at them cause you are in pain. I often feel guilty because I feel I'm not patient enough and can get annoyed over little things” (#147, SpA, three children age 2, 5 and 8 years).
3.1.2.2 Relations – family and work
For some women the challenges and feelings of not being able to contribute and participate affected their relationship with their partner, and resulted in feelings of guilt and inadequacy.
These two women expressed it like this:
“Me and my partner can get a shorter fuse between us. He has to do more. I don't have the capacity I used to. He gets up every morning. Aching makes it difficult to fall asleep at times. Sometimes it can be hard on our partnership” (#131, RA, two children age 1 and 3 years).
“I often feel guilty that dad has to contribute more, especially in the mornings. And generally there’s a bit too much responsibility on dad” (#29, RA, one child age 2 years).
Being able to work full-time was described as important for many of the women. However, several expressed combining full-time work with family-life and a chronic disease as difficult. One women wrote that she often prioritized work to look good for her employer even though this made the afternoons with her family very hard. Another felt constantly tired/exhausted and experienced it as difficult to be present when being with her family and children because she worked fulltime. Being able to work fulltime was also depended on the type of job, possibilities for making adjustments and having some flexibility:
“If it wasn't for the fact that I have a very independent and flexible job (university-sector), I don’t think I would have been able to be both a mum and an employee. I hope this survey can contribute to increased political focus on us with rheumatic disease with “double responsibility”. For me, I think that only the possibility for rehabilitation in warm climate and/or some form of relief/childcare sometimes would make it possible to get enough a) rest and b) physical activity. I strongly want to work, also after giving birth to nr.2, but sometimes I worry that this won’t be possible. I often feel alone with my diagnosis in everyday life, and as a woman I think that one can experience very different expectations about being able to deal with both work and family-life compared to men, despite the fact that we are in 2019” (#32, SpA, one child age 2 years).
3.1.2.3 Self-care
Focusing on self-care, such as exercise and resting, were emphasised as important and as a way of keeping their disease under control. Many women experienced that it was difficult or impossible to prioritize self-care, which again had a negative impact on their health; as this mother described:
“I also feel/notice that to prioritize physical activity/exercise on my own has been difficult/non-existent, which in turn has a negative impact on my physical health and disease activity (…) With small children I also experience that there’s no time to relax and rest, and that sleep is limited. I notice that this also affects me and my disease negatively” (#74, PsA, two children age 3 years and 1 year).
3.1.3 Disease management
Pregnancy and the postpartum period led to some new dilemmas and problems regarding disease management and medication use. A few women felt that they did not get sufficient information from health professionals leading to unnecessary distress. Information about medication use during pregnancy and breastfeeding was described as inadequate and often conflicting. Some felt they had to do their own research, in addition to involving their partners:
“Decisions regarding medications, not enough knowledge among many of the doctors (especially regarding breastfeeding). I’ve used “tryggmammamedisin.no” (“Norwegian webpage with knowledge based information regarding medication in pregnancy and breastfeeding”) to check if it´s ok” (#160, RA, two children age 3 and 1 year).
“I also had bad conscience for my child because I took some painkillers prescribed by a doctor (very little), that the child’s father meant wasn’t good for the foetus. I felt I was “in a squeeze” where I experienced that the partner should get more information from the doctors, not just passed on by me” (#70, SpA, one child age 2 years).
Several expressed that they received insufficient information, making it challenging to manage their IA. The women wanted clear and understandable information, not only that it was important to stop certain medications during pregnancy, but also about alternatives.
“I had been asked many times if I was planning to get pregnant, but that was just concerning that I had to stop my medications in time, never to tell me that there were alternatives if I did get pregnant. When I then got pregnant and came on a routine follow up appointment to the rheumatologist, I was met by a doctor who questioned why I hadn’t let them know earlier. I said it as it was, that I didn’t know that there was any reason to let them know – cause I didn’t know that there was anything that they could do to help. Now I’m pregnant again and I feel I’m much more informed this time” (#124,RA, two children age 10 and 2 years).
Others described struggles with taking care of their babies after giving birth due to disease flares and inadequate follow up or treatment plans.
“I would have appreciated a better plan regarding medication and treatment after birth and before stopping breastfeeding. I wasn't physically able to take care of the baby on my own until several months after birth, I wasn't prepared for this” (#77, PsA, one child age 1 year).
3.1.4 What about the future?
Naturally, having children and a family brought some new thoughts about the future. Several were concerned about the disease progress, and how their IA could affect their children and family in the future. The unpredictability of the disease worried them, making them questioning whether they were able to combine motherhood with a fulltime-job. If they could not work full-time, they were anxious about the economic consequences:
“Unpredictability with regards to daily fluctuations in disease burden. Worries about worsening of the disease and that I will not be able to follow up the children” (#193, JIA, 2 children age 5 and 1 year).
«Worry a lot about how the economic situation will be if I can’t work fulltime in the future2 (#1, SpA, one child age 1 year).
«I am dreading going back to work. I want to function as a mother and a girlfriend, and I think my work is going to take a lot of my energy” (#116,RA, one child age 1 year)
Several women also feared that their children would inherit their disease. Some described feelings of guilt if this would happen even though it was beyond their control. Whether to have more children or not is a life changing decision. Many of the women struggled to make such a decision because their prior pregnancy or post-partum periods were challenging, and they were unsure if they would go through it again:
«I’m scared that the children may have inherited the disease, don’t want them to be in pain just because I brought them into the world” (#209, PsA, two children age 2 years and 3 months).
“I want my child to have siblings, but having to go through a heavy pregnancy and the pain afterwards makes me doubt” (#116, RA, one child age 1 year).
3.1.5 It’s not so bad
Even though many women described difficulties in their role as a mother with IA, some described a more nuanced and positive picture of the situation. Better treatment, family-support and a perspective that normalised feeling tired a natural part of being a parent, independent of having a chronic disease, were mentioned.
Several women expressed that having a good medical treatment plan had significantly improved their lives with IA:
“I’m much better after starting biologics. I live more or less like normal” (#154, SpA, one child age 5 months).
“More challenges after the birth of my two first children (born 2011 and 2013), and in the first years, than after my last child (born 2018). Started biologics after giving birth in 2018, and this has given me a whole new life”(#10, RA, three children age 8, 6 and 2 years).
While some women were a bit concerned about whether their partner took too much responsibility, leading to stress on the relationship, others expressed that the support from their partner made the situation easier. Being a mother could be difficult and demanding at times regardless of having a chronic disease. Some women reflected on this, and that it could be difficult to know whether the challenges were due to their disease or to motherhood in general:
“I’ve been lucky when it comes to my arthritis, so I don’t think it affects me that much + I’m lucky to have a husband who takes care of the children when I’m tired (which doesn’t happen very often)” (#189, JIA, two children age 2 and 6 years).
“I think it’s difficult to tell what is due to the disease and what is “just being a mother with small kids”. Most people in this phase are tired” (#103, RA, three children age 12, 10 and 2 years).
Several also mention, despite the challenges, that having children led to a more active lifestyle, which had a positive impact on the disease symptoms:
“At the same time I’ve experienced that having an active lifestyle, which you do when your home with small kids, is overall a good thing for the joints. I notice little from the disease during the day when I’m carrying, going for walks, playing and running. Its first when I sit down at night and when I wake up in the morning that I notice that I have a rheumatic disease” (#88, RA, 2 children age 3 and 1 year).
4 Discussion
The aim of this study was to gain insight into the challenges that mothers with IA encounter in their daily life. Many describe difficulties, both physically, mentally and socially that have a large impact on their everyday life. They describe life as a mother with a chronic rheumatic disease as a balancing act, trying to live up to the needs and expectations of their children, family and workplace, at the same time as they try to take care of their own needs in order to function in everyday life.
Experiences and expectations surrounding motherhood are strongly influenced by the culture and society one lives in. Norway is a welfare state, with universal healthcare and a developed system for parents with paid parental leave for up to a year, a free infant healthcare-programme and highly subsidised child-care (23). Studies on Norwegian cohorts of women with psoriatic arthritis, juvenile idiopathic arthritis and spondyloarthritis found altogether low and stable disease activity during pregnancy and the first year after birth (24–26). These are all important factors that potentially influence how Norwegian women with IA experience motherhood. Still, our findings are in line with previous qualitative studies on similar patient groups from other countries, reporting many of the same challenges (10, 12–16). Also Barlow et.al study from 1999 (15), going 25 years back, describe many of the same challenges as our cohort when it comes to parenting with small children. Troubles with everyday tasks, and feelings of guilt for missing out on activities, as well as frustration and inadequacy were also described in this study. Considering the vast improvement in medical treatment for patients with IA in the last two decades, also during pregnancy and breastfeeding (4, 19, 20, 27), one could assume that the described experience of motherhood also should improve. It is however clear from the literature, that despite recent improvements in medical treatment, many IA patients, including those with low disease activity/in clinical remission, have residual symptoms and significant unmet needs (28, 29). Studies have also shown that women with IA overall have a higher disease burden and more unmet needs compared to men (30).
The biopsychosocial model is helpful for clinicians to understand the complexity of how women with IA experience motherhood, and why improvement in medical treatment does not solve all of their challenges. Figure 1 illustrates various elements that has an impact on how women experience motherhood. The relations between the underlying factors are dynamic and intertwined. Many of these factors are relevant for how people with IA experience life with a chronic disease in all life stages, and pregnancy and motherhood can affect and intensify many of these elements contributing to the overall experience. When it comes to the psychological impact of having IA, studies have shown that people with IA are generally more at risk of both depression and anxiety disorders (31) and mothers with IA are more at risk of developing postpartum depression compared to mothers without IA (32, 33). In addition, poor mental health is linked to worse outcomes in IA (34, 35). We do not know if any of the women in this study had a comorbidity of anxiety or depression, but it is plausible that some did, and that this potentially affected their experience of motherhood.
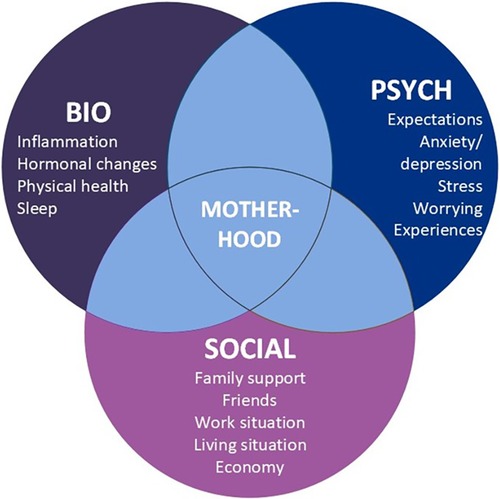
Figure 1. Illustration of elements affecting how women with IA experience motherhood, in a biopsychosocial framework.
Many women in our study expressed difficulties with prioritizing self-care and exercise, which had a detrimental effect on their function and disease activity, also contributing to the experience of inadequacy. The majority of the women in our study were also working, making prioritizing self-care even more challenging. The cultural expectations of motherhood in the western society, and how this affects women with various health challenges is thoroughly discussed in several studies (14, 36, 37). Attending to and prioritizing own needs, e.g., with exercise and resting, rather than always attending to their children and others needs first, means that the women might not live up to their own and their perceived expectations of others in the role as a mother.
A study by Bar and colleagues (38) gave some interesting insight from men with IA, and their experience of fatherhood. Despite arthritis interfering with specific tasks for these men in the same way that mothers in our study describe, it did not affect the way they perceived themselves as fathers. Strong social support, ability and possibility to prioritize themselves in regards to things such as exercise and rest, and taking ownership of their disease by changing priorities, pacing activities and normalizing their disease were all factors that contributed to a predominantly positive experience of fatherhood. Going back to the biopsychosocial model, these men expressed many positive experiences in the psychosocial domains, illustrating how these can be protective and positive factors in the overall experience of being a parent with IA. It is interesting that several women in our study felt guilty when the dad had to step in and at times do more, such as get up in the morning. No men in Bar et al. study mentioned feelings of guilt and they were not hesitant about seeking and accepting help and support, possibly a result of cultural expectations and differences in parenteral role of mothers vs. fathers (39).
Challenges with disease management and follow-up in relation to pregnancy and the post-partum period, as well as insufficient/contradictory information from various health professionals was brought up as problematic by many women in our study. This can lead to uncertainty and increased stress and worrying, non-compliance, increased disease activity and feelings of inadequacy, illustrating how everything is connected. The findings in this study adds to an already extensive number of studies highlighting problems with unmet information and support needed for this patient group (17, 40–42).
Empowering these women, and learning them good self-management strategies in order to deal with the practical, physical and psychological challenges they encounter in their role as a mother with a chronic disease is vital. Pregnancy and the post-partum period represents a massive life-changing event. EULARs recommendations on patient education (PE) for patients with IA (43) states that PE should be provided as an integral part of their care to increase patient involvement in disease management. They also highlight that the need for education and support might be more prominent when the disease interferes with daily activities, life-events and family roles, and that PE should include discussion on emotional issues and support. Increased focus on PE and self-management interventions in relation to pregnancy and the postpartum period is thus something that should be prioritized (3, 43, 44).
The findings in this study highlights the importance of providing high quality multidisciplinary care with a holistic and individualized approach for this group of patients, where the health care professionals have insights into the common challenges these women encounter. The team of health care professionals should provide advice and guidance on practical aspects of childcare, physical activity, exercise, patient rights, adjustments in work life, patient information, self-management and optimal medical treatment (17). Also encouraging the women to get in touch with peers through i.e., patient organisations, can be of great value (44).
4.1 Strengths and limitations
One of the main strengths in this study is that 186 of the 233 women responded to the open-ended question providing us with a rich material of written descriptions of experienced challenges among mothers with IA. On the other hand, a possible limitation with the written responses is that we were not able to ask the respondents to elaborate, as qualitative interviews could have, limiting the depth of the data (45). The open-ended question encouraged the respondents to write about their challenges related to being a mother with IA, and positive experiences might not be captured.
Even though the experiences described in this study do not apply to all women with IA, they provide great insights that are beneficial for clinical practice in further development of follow-up care.
This study only included Norwegian mothers. This might limit the reproduction of these results in other locations, especially less developed countries.
4.2 Recommendations for future research
This study gives valuable insights into the experienced challenges among mothers with IA. Hence, further studies should focus on the positive experiences of motherhood; on beneficial strategies to improve different challenging situations, and how health care personnel can best support women in planning their pregnancy, during pregnancy, and in the post-partum period. The experiences of becoming a father when living with IA is also less studied, and what kind of support they need in this phase of life.
Comparing the experiences and challenges of mothers with IA to women with other chronic diseases, or to healthy mothers could also give important insight into what challenges are unique to those living with IA, and what challenges are common for mothers regardless of diagnosis.
5 Conclusion
The main finding in this study is that the women with IA experience several challenges related to motherhood. The challenges are multifactorial and complex, including physical, mental and social issues that have a large impact on their everyday life. Focusing solely on improving medical treatment will not solve the challenges these women face. A multidisciplinary approach and focus on patient education and self-management strategies is important to help these mothers thrive in their role as a mother with chronic disease.
Data availability statement
The datasets presented in this article are not readily available because The data cannot be shared publicly due to the requirements of the involved register holders and the general data protection regulation, to protect the privacy of individuals. Requests to access the datasets should be directed toaW5ncmlkLnJla2FhLm5pbHNzZW5Ac3RvbGF2Lm5v.
Ethics statement
The studies involving humans were approved by Regional Committee for Medical and Health Research Ethics South/East Norway. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
IN: Conceptualization, Data curation, Methodology, Project administration, Writing – original draft, Writing – review & editing, Formal Analysis, Investigation, Visualization. HK: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Writing – original draft, Writing – review & editing. BJ: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Writing – original draft, Writing – review & editing. KG: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by The Norwegian Rheumatism Association with a research grant from Trondheim revmatikerforening. They were not involved in the collection, analysis, or interpretation of the data, nor the writing or submission for publication.
Acknowledgments
The authors would like to express our gratitude to the patients who responded to our questionnaire and we also thank the participating departments of rheumatology at the following hospitals for including patients in RevNatus: Betanien Hospital, Skien; Diakonhjemmet Hospital, Oslo; Haugesund hospital for rheumatic diseases (HSR), Haugesund; Haukeland University Hospital, Bergen; Førde Hospital, Førde; Ålesund hospital, Ålesund; Lillehammer Hospital for Rheumatic Diseases, Nordland Hospital Trust, Bodø; St. Olavs hospital Trondheim University Hospital, Trondheim; Sørlandet Hospital Trust, Kristiansand; University Hospital of North Norway, Tromsø; Vestre Viken Hospital Trust, Drammen; Østfold Hospital, Moss; The Helgeland Hospital Trust, Mo i Rana, Nord-Trøndelag Hospital Trust, Levanger.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Al Maini M, Adelowo F, Al Saleh J, Al Weshahi Y, Burmester GR, Cutolo M, et al. The global challenges and opportunities in the practice of rheumatology: white paper by the world forum on rheumatic and musculoskeletal diseases. Clin Rheumatol. (2015) 34(5):819–29. doi: 10.1007/s10067-014-2841-6
2. Studenic P, Aletaha D, de Wit M, Stamm TA, Alasti F, Lacaille D, et al. American College of Rheumatology/EULAR remission criteria for rheumatoid arthritis: 2022 revision. Ann Rheum Dis. (2023) 82(1):74–80. doi: 10.1136/ard-2022-223413
3. Kristiansen TM, Primdahl J, Antoft R, Hørslev-Petersen K. Everyday life with rheumatoid arthritis and implications for patient education and clinical practice: a focus group study. Musculoskeletal Care. (2012) 10(1):29–38. doi: 10.1002/msc.224
4. Skorpen CG, Hoeltzenbein M, Tincani A, Fischer-Betz R, Elefant E, Chambers C, et al. The EULAR points to consider for use of antirheumatic drugs before pregnancy, and during pregnancy and lactation. Ann Rheum Dis. (2016) 75(5):795–810. doi: 10.1136/annrheumdis-2015-208840
5. de Jong PH, Dolhain RJ. Fertility, pregnancy, and lactation in rheumatoid arthritis. Rheum Dis Clin North Am. (2017) 43(2):227–37. doi: 10.1016/j.rdc.2016.12.004
6. Wallenius M, Skomsvoll JF, Irgens LM, Salvesen KA, Nordvag BY, Koldingsnes W, et al. Fertility in women with chronic inflammatory arthritides. Rheumatology (Oxford). (2011) 50(6):1162–7. doi: 10.1093/rheumatology/keq458
7. Wallenius M, Skomsvoll JF, Irgens LM, Salvesen KA, Nordvag BY, Koldingsnes W, et al. Parity in patients with chronic inflammatory arthritides childless at time of diagnosis. Scand J Rheumatol. (2012) 41(3):202–7. doi: 10.3109/03009742.2011.641582
8. Clowse ME, Chakravarty E, Costenbader KH, Chambers C, Michaud K. Effects of infertility, pregnancy loss, and patient concerns on family size of women with rheumatoid arthritis and systemic lupus erythematosus. Arthritis Care Res (Hoboken). (2012) 64(5):668–74. doi: 10.1002/acr.21593
9. Østensen M. New insights into sexual functioning and fertility in rheumatic diseases. Best Pract Res Clin Rheumatol. (2004) 18(2):219–32. doi: 10.1016/j.berh.2004.01.002
10. Meade T, Sharpe L, Hallab L, Aspanell D, Manolios N. Navigating motherhood choices in the context of rheumatoid arthritis: women’s stories. Musculoskeletal Care. (2013) 11(2):73–82. doi: 10.1002/msc.1031
11. Borrell-Carrió F, Suchman AL, Epstein RM. The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Ann Fam Med. (2004) 2(6):576–82. doi: 10.1370/afm.245
12. Backman CL, Smith Ldel F, Smith S, Montie PL, Suto M. Experiences of mothers living with inflammatory arthritis. Arthritis Rheum. (2007) 57(3):381–8. doi: 10.1002/art.22609
13. Feddersen H, Mechlenborg Kristiansen T, Tanggaard Andersen P, Horslev-Petersen K, Primdahl J. Juggling identities of rheumatoid arthritis, motherhood and paid work - a grounded theory study. Disabil Rehabil. (2019) 41(13):1536–44. doi: 10.1080/09638288.2018.1433723
14. Parton C, Ussher JM, Perz J. Mothers’ experiences of wellbeing and coping while living with rheumatoid arthritis: a qualitative study. BMC Womens Health. (2022) 22(1):185. doi: 10.1186/s12905-022-01767-1
15. Barlow JH, Cullen LA, Foster NE, Harrison K, Wade M. Does arthritis influence perceived ability to fulfill a parenting role? Perceptions of mothers, fathers and grandparents. Patient Educ Couns. (1999) 37(2):141–51. doi: 10.1016/S0738-3991(98)00136-0
16. Mitton DL, Treharne GJ, Hale ED, Williams RA, Kitas GD. The health and life experiences of mothers with rheumatoid arthritis: a phenomenological study. Musculoskeletal Care. (2007) 5(4):191–205. doi: 10.1002/msc.116
17. Rebić N, Garg R, Ellis U, Kitchin V, Munro S, Hazlewood G, et al. “Walking into the unknown…” key challenges of pregnancy and early parenting with inflammatory arthritis: a systematic review and thematic synthesis of qualitative studies. Arthritis Res Ther. (2021) 23(1):123. doi: 10.1186/s13075-021-02493-z
18. Williams D, Pell B, Grant A, Sanders J, Taylor A, Edwards A, et al. Identities of women who have an autoimmune rheumatic disease [ARD] during pregnancy planning, pregnancy and early parenting: a qualitative study. PLoS One. (2022) 17(11):e0263910. doi: 10.1371/journal.pone.0263910
19. Russell MD, Dey M, Flint J, Davie P, Allen A, Crossley A, et al. British Society for rheumatology guideline on prescribing drugs in pregnancy and breastfeeding: immunomodulatory anti-rheumatic drugs and corticosteroids. Rheumatology (Oxford). (2023) 62(4):e48–88. doi: 10.1093/rheumatology/keac551
20. Schreiber K, Frishman M, Russell MD, Dey M, Flint J, Allen A, et al. British Society for rheumatology guideline on prescribing drugs in pregnancy and breastfeeding: comorbidity medications used in rheumatology practice. Rheumatology (Oxford). (2023) 62(4):e89–e104. doi: 10.1093/rheumatology/keac552
21. Meissner Y, Fischer-Betz R, Andreoli L, Costedoat-Chalumeau N, De Cock D, Dolhain R, et al. EULAR recommendations for a core data set for pregnancy registries in rheumatology. Ann Rheum Dis. (2021) 80(1):49–56. doi: 10.1136/annrheumdis-2020-218356
22. Brinkmann S, Kvale S. InterViews: Learning the Craft of Qualitative Research Interviewing. 3rd ed. Thousand Oaks, Calif: Sage Publications (2015). p. 204–46.
23. Helsedirektoratet. Nytt liv og trygg barseltid for familien. Nasjonal faglig retningslinje for barselomsorgen (2014).
24. Ursin K, Lydersen S, Skomsvoll JF, Wallenius M. Disease activity of juvenile idiopathic arthritis during and after pregnancy: a prospective multicenter study. J Rheumatol. (2018) 45(2):257–65. doi: 10.3899/jrheum.161410
25. Ursin K, Lydersen S, Skomsvoll JF, Wallenius M. Disease activity during and after pregnancy in women with axial spondyloarthritis: a prospective multicentre study. Rheumatology (Oxford). (2018) 57(6):1064–71. doi: 10.1093/rheumatology/key047
26. Ursin K, Lydersen S, Skomsvoll JF, Wallenius M. Disease activity of psoriatic arthritis during and after pregnancy: a prospective multicenter study. Arthritis Care Res (Hoboken). (2019) 71(8):1092–100. doi: 10.1002/acr.23747
27. Sammaritano LR, Bermas BL, Chakravarty EE, Chambers C, Clowse MEB, Lockshin MD, et al. 2020 American College of Rheumatology guideline for the management of reproductive health in rheumatic and musculoskeletal diseases. Arthritis Care Res (Hoboken). (2020) 72(4):461–88. doi: 10.1002/acr.24130
28. Ishida M, Kuroiwa Y, Yoshida E, Sato M, Krupa D, Henry N, et al. Residual symptoms and disease burden among patients with rheumatoid arthritis in remission or low disease activity: a systematic literature review. Mod Rheumatol. (2018) 28(5):789–99. doi: 10.1080/14397595.2017.1416940
29. Taylor PC, Moore A, Vasilescu R, Alvir J, Tarallo M. A structured literature review of the burden of illness and unmet needs in patients with rheumatoid arthritis: a current perspective. Rheumatol Int. (2016) 36(5):685–95. doi: 10.1007/s00296-015-3415-x
30. Michelsen B, Berget KT, Loge JH, Kavanaugh A, Haugeberg G. Sex difference in disease burden of inflammatory arthritis patients treated with tumor necrosis factor inhibitors as part of standard care. PLoS One. (2022) 17(5):e0266816. doi: 10.1371/journal.pone.0266816
31. Nagy Z, Szigedi E, Takács S, Császár-Nagy N. The effectiveness of psychological interventions for rheumatoid arthritis (RA): a systematic review and meta-analysis. Life (Basel). (2023) 13(3):849. doi: 10.3390/life13030849
32. Shridharmurthy D, Lapane KL, Nunes AP, Baek J, Weisman MH, Kay J, et al. Postpartum depression in reproductive-age women with and without rheumatic disease: a population-based matched cohort study. J Rheumatol. (2023) 50(10):1287–95. doi: 10.3899/jrheum.2023-0105
33. Luan M, Yang F, Miao M, Yuan W, Gissler M, Arkema EV, et al. Rheumatoid arthritis and the risk of postpartum psychiatric disorders: a nordic population-based cohort study. BMC Med. (2023) 21(1):126. doi: 10.1186/s12916-023-02837-3
34. Lwin MN, Serhal L, Holroyd C, Edwards CJ. Rheumatoid arthritis: the impact of mental health on disease: a narrative review. Rheumatol Ther. (2020) 7(3):457–71. doi: 10.1007/s40744-020-00217-4
35. Santos EF, Duarte CM, Ferreira RO, Pinto AM, Geenen R, da Silva JP. Multifactorial explanatory model of depression in patients with rheumatoid arthritis: a structural equation approach. Clin Exp Rheumatol. (2019) 37(4):641–8.30418126
36. Parton C, Ussher JM, Natoli S, Perz J. Being a mother with multiple sclerosis: negotiating cultural ideals of mother and child. Fem Psychol. (2017) 28(2):212–30. doi: 10.1177/0959353517732591
37. Liss M, Schiffrin HH, Rizzo KM. Maternal guilt and shame: the role of self-discrepancy and fear of negative evaluation. J Child Fam Stud. (2013) 22(8):1112–9. doi: 10.1007/s10826-012-9673-2
38. Bar MA, Dao TT, DeBlock Vlodarchyk LR, Backman CL. Fatherhood experiences of men with inflammatory arthritis: a preliminary grounded theory. Arthritis Care Res (Hoboken). (2021) 73(6):885–92. doi: 10.1002/acr.24189
39. Schmidt EM, Décieux F, Zartler U, Schnor C. What makes a good mother? Two decades of research reflecting social norms of motherhood. J Fam Theory Rev. (2023) 15(1):57–77. doi: 10.1111/jftr.12488
40. Phillips R, Pell B, Grant A, Bowen D, Sanders J, Taylor A, et al. Identifying the unmet information and support needs of women with autoimmune rheumatic diseases during pregnancy planning, pregnancy and early parenting: mixed-methods study. BMC Rheumatol. (2018) 2:21. doi: 10.1186/s41927-018-0029-4
41. Chew C, Rebić N, Baldwin C, Amiri N, Proulx L, De Vera MA. “R/thritis”, pregnancy, and parenting: a qualitative descriptive study of reddit forums to explore information needs and concerns of women with rheumatoid arthritis. ACR Open Rheumatol. (2019) 1(8):485–92. doi: 10.1002/acr2.11069
42. Ackerman IN, Jordan JE, Van Doornum S, Ricardo M, Briggs AM. Understanding the information needs of women with rheumatoid arthritis concerning pregnancy, post-natal care and early parenting: a mixed-methods study. BMC Musculoskelet Disord. (2015) 16:194. doi: 10.1186/s12891-015-0657-4
43. Zangi HA, Ndosi M, Adams J, Andersen L, Bode C, Boström C, et al. EULAR recommendations for patient education for people with inflammatory arthritis. Ann Rheum Dis. (2015) 74(6):954–62. doi: 10.1136/annrheumdis-2014-206807
44. Nikiphorou E, Santos EJF, Marques A, Böhm P, Bijlsma JW, Daien CI, et al. 2021 EULAR recommendations for the implementation of self-management strategies in patients with inflammatory arthritis. Ann Rheum Dis. (2021) 80(10):1278–85. doi: 10.1136/annrheumdis-2021-220249
Keywords: motherhood, rheumatic diseases, arthritis, inflammatory joint disease, women's health
Citation: Nilssen IR, Koksvik HS, Jakobsen B and Grønning K (2024) Motherhood and rheumatic disease – a balancing act. A qualitative study on the challenges of mothers with inflammatory arthritis. Front. Lupus 2:1497518. doi: 10.3389/flupu.2024.1497518
Received: 17 September 2024; Accepted: 30 October 2024;
Published: 12 November 2024.
Edited by:
Laura Andreoli, University of Brescia, ItalyReviewed by:
Guilherme Ramires De Jesús, Rio de Janeiro State University, BrazilMadhuri Radhakrishna, AIG Hospitals, India
Copyright: © 2024 Nilssen, Koksvik, Jakobsen and Grønning. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ingrid Rekaa Nilssen, aW5ncmlkLnJla2FhLm5pbHNzZW5Ac3RvbGF2Lm5v