
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Lupus , 05 September 2024
Sec. Clinical Research and Treatment in Lupus
Volume 2 - 2024 | https://doi.org/10.3389/flupu.2024.1462320
This article is part of the Research Topic Rheumatology Education without Borders - a global approach to basic instruction on the complex disease of SLE View all 6 articles
 Dzifa Dey1*
Dzifa Dey1* Rosetta Bobade2Bright Katso3Saudatu Issaka3,4Angela Charis4Abdul Aziz Can Tamakloe4Padiki Narh4
Rosetta Bobade2Bright Katso3Saudatu Issaka3,4Angela Charis4Abdul Aziz Can Tamakloe4Padiki Narh4
Rheumatic diseases like Lupus are complex autoimmune conditions with diverse manifestations presenting challenges for diagnosis and management globally. Access to rheumatology expertise and education varies significantly across different regions, particularly in low-resource settings. These diseases pose significant challenges to healthcare systems worldwide, including developing countries like Ghana. To address these resource gaps and optimise patient care, innovative solutions must be pursued. The Rheumatology Initiative (tRi) in Ghana aims to improve the understanding, diagnosis, and management of rheumatic conditions through educational activities, research projects, and targeted interventions. This article provides an overview of tRi's initiatives to bridge the rheumatology resource gap, focusing on educational efforts, project targets, and their outcomes, with specific attention to systemic lupus erythematosus (SLE) in the Ghanaian context. We highlight the progress made by tRi and underscore the importance of continued collaboration and support for rheumatology initiatives in resource-limited settings to improve management and awareness.
Rheumatic diseases cover a wide range of conditions that affect the joints, muscles, and connective tissues often causing significant morbidity and reduced quality of life (1). Historically, it was believed that the occurrence of rheumatic diseases was low in Africa (2). A study conducted in 1998 identified only 413 cases of Systemic Lupus Erythematosus (SLE) between 1971 and 1984 in several African countries (3), supporting the previously suggested “prevalence gradient hypothesis” (4). However, recent studies and increasing awareness have challenged this notion, revealing that systemic lupus erythematosus (SLE), is indeed prevalent in Africa (2, 5).
Over the past two decades, progress has been made in diagnosing and treating rheumatic diseases in Africa (5). However, this also highlights the many challenges that persist in managing these conditions, especially in Sub-Saharan Africa. More than half of the countries in Africa rank among the poorest in the world. Unfortunately, all in Sub-Saharan Africa, leading to issues such as limited access to education, low economic status, and restricted healthcare. This leads to intense competition for limited healthcare resources, resulting in non-communicable diseases such as rheumatic conditions being overlooked (2).
There is a severe shortage of rheumatologists in Africa. As of 2022, Africa identified 2,970 rheumatologists, serving 1·19 billion people residing in the 44 countries (0·25 rheumatologists per 100,000, yet is the second most populated continent in the world (6, 7). Nigeria, the most populated country in Africa, has approximately 30 rheumatologists serving its population of around 200 million people (8), compared to the ideal ratio of one rheumatologist for every 150,000 people (9). This has resulted in a situation where most people in rural areas only get to see rheumatologists when their conditions have already deteriorated (2). Additionally, some religious and cultural beliefs also contribute to challenges in identifying and managing rheumatic diseases leading to delays, especially in Sub-Saharan Africa (5, 10). The difficulty in obtaining the necessary tools and technologies for diagnosing and treating rheumatic disorders is also a challenge facing Africa. For instance, the ACR–EULAR SLE classification criteria (11), requiring a 1:80 ANA titer as an entry criterion, is often unaffordable or unavailable in many sub-Saharan African centres due to the high cost and limited access to autoantibody testing (12).
In Ghana, the rheumatology landscape has been challenging for several reasons. According to the monthly statistics of the National Rheumatology Center located at the Korle Bu Teaching Hospital (KBTH), at least 7 new cases of SLE are diagnosed every month, totalling about 84 new cases annually. Diagnostic delays mean patients take a minimum of 39 months to receive a diagnosis from the onset of symptoms (13). This is because the diagnostic capacity in the country is severely limited to few specialist centres. The rheumatology referral process in Ghana often involves patients being seen by multiple general practitioners over time before being referred to a rheumatologist, causing significant delays. Currently, Ghana only has three rheumatologists, serving approximately 31 million people, meaning numerous patients only have access to rheumatologists when their conditions have significantly worsened. Furthermore, there is poor knowledge of these diseases among healthcare providers and the general population in Ghana. Like other African countries, diagnosing these diseases is complex and requires several costly serological tests, which can be a significant financial burden for the average Ghanaian (12). Despite these challenges, significant efforts are underway to improve the country's local care and management of rheumatic diseases.
This article provides an overview of The Rheumatology Initiative's (tRi's) efforts to bridge the rheumatology resource gap, focusing on educational initiatives, projects, and outcomes. The progress made by tRi underscores the importance of continued collaboration and support for rheumatology initiatives in resource-limited settings to improve disease management and patient outcomes.
The Rheumatology Initiative (tRi) was established in 2012 to enhance rheumatology care through various approaches. tRi is a not-for-profit organization based in Accra, Ghana, mainly run by volunteers, including doctors and patients, with self-funded initiatives. The organization conducts programs to bridge the knowledge gap, raise awareness about rheumatic conditions, and advocate for patients in rheumatology. tRi aims to increase public awareness of autoimmune rheumatological conditions in Ghana, develop educational resources, fund research, build strategic partnerships, and leverage technology. Key activities include public campaigns, educational activities, workshops, partnerships, online presence, and digital tools for patients and healthcare providers. The following sections discuss some of the projects undertaken by tRi.
The organization focuses on public awareness and educational campaigns to raise awareness about rheumatic diseases and promote early detection and treatment. It leverages social media platforms such as Facebook, Twitter, Instagram, and blogs to run regular campaigns and health awareness events such as concerts and media events.
Additionally, tRi has conducted community outreach initiatives. These involve engaging local communities in providing rheumatology services and educational programs in underserved areas, such as churches, schools, and workplaces, bringing education to their doorsteps.
The rheumatology initiative (tRi) prides itself in advocacy and support for patients, hence has engaged in successfully advocating for the addition of basic new medications like disease-modifying anti-rheumatic drugs (DMARDs) and steroids (prednisolone), on the essential drugs list in Ghana. This would improve access to essential medicines and specialised care for individuals with rheumatic disorders, especially lupus patients who tend to require emergency treatment for flares. tRi has advocated for a 25% drop in the prices of some biologics from pharma, making these drugs much more affordable to patients.
Through its patient assistance program, tRi provides free or discounted emergency medication to over 52 patients annually and also provides free or discounted lab tests to patients. tRi's advocacy efforts have also successfully raised funds to establish an infusion room at the Korle Bu Teaching Hospital in Accra, Ghana.
The Rheusolute Support Group established by tRi aims to provide sustainable solutions that empower individuals with rheumatic diseases in Ghana. The group focuses on connecting patients with social and community resources, educating them to advocate for themselves, and offering a supportive environment. Established in Accra, it supports individuals with diverse autoimmune rheumatic diseases, addressing concerns like disease management, lifestyle challenges, and coping with relapses and mortality. The group promotes cognitive well-being through counselling, enhancing physical health. With over 250 members, it includes subgroups for lupus, rheumatoid arthritis, and multiple autoimmune conditions, offering targeted support. Monthly meetings, attended by an average of 30 patients, feature activities such as hydrotherapy, soap-making, cooking competitions, eye screening, and oral hygiene sessions. These sessions provide information and healing interaction beyond the consulting room, fostering a resilient mindset and a supportive community (14). Details shown in Figure 1.
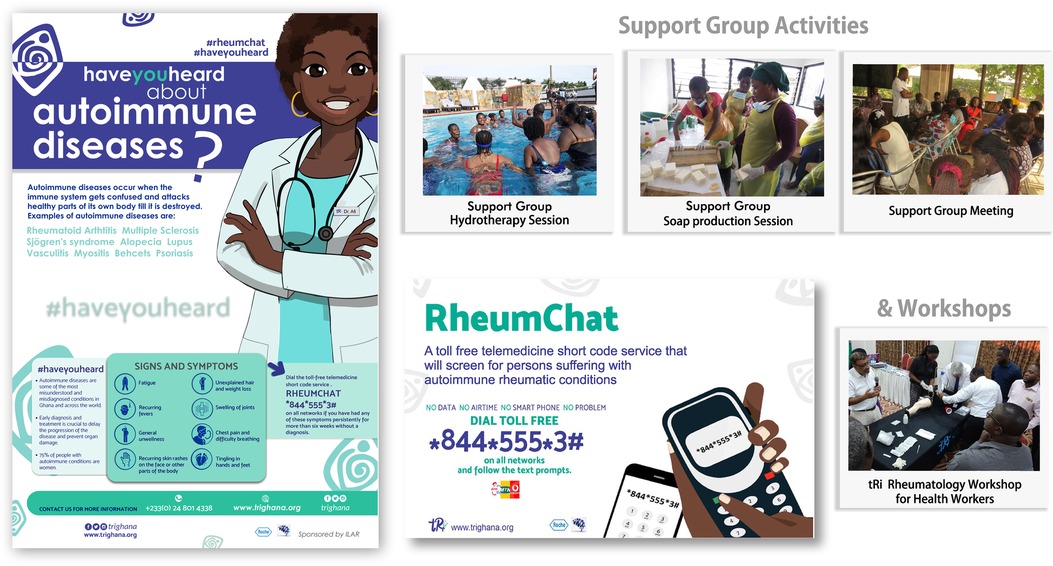
Figure 1. Rheusolute support group activities, the rheumChat project, and the HEARD project.
The cornerstone of the Rheumatology initiative (tRi) in Ghana centres on educational activities for healthcare professionals, patients, and the public. Historically, patient education has been an integral part of the clinical care. It was shown that simply providing patients with information or advice was insufficient to change health behaviors (15). Current patient education programs include activities designed and planned to result in adopting skills and behaviours beyond disease knowledge alone. Mobile technologies are assuming an emerging role in this scenario (16, 17).
The Heralding Education in Autoimmune Rheumatic Disorders (HEARD) project is a success story of tRi's patient educational activities. Conducted over 1 year, HEARD aimed to educate and raise awareness of Autoimmune Rheumatic Diseases using animated videos and communication materials in English, French, and local dialects such as Ewe, Twi, Ga, and Hausa. Targeting patients and Ghana's low health literacy population, this project used audiovisual formats to enhance disease awareness and comprehension, thereby facilitating early diagnosis. Education on autoimmune rheumatic diseases was presented in simple, culturally relevant languages, increasing interest and knowledge among patients and healthcare professionals.
The project included a radio campaign with jingles and interviews, despite challenges in measuring listenership. On social media, the Animation and E-flyer Campaign on Instagram reached 5,465 individuals and garnered 806 views, 722 likes, 2,410 impressions, 14 hashtags, and 66 shares. On Facebook, it received 32,995 views, 704 likes, 353 shares, and 43 comments. On Twitter, it generated 37,948 impressions, 220 retweets, 201 likes, 761 media views, and 984 engagements. The YouTube campaign obtained 76 views, and WhatsApp Status achieved widespread reach, though exact metrics were challenging to track. Brochures were distributed nationwide in healthcare centres, and a poster campaign was conducted in every district in Ghana.
tRi has implemented several educational activities to this effect. One significant educational activity tRi has implemented is the continuous medical education (CME) workshops. These regular workshops update healthcare providers on the latest advancements in rheumatology across various regions in Ghana reaching hundreds of doctors. Given the shortage of rheumatologists in Africa, training nurses and other health workers to identify common rheumatic conditions has been practical. This approach expands the responsibilities of health professionals like nurses to manage patients and provide treatment, education, monitoring, and referrals as needed. As of 2023, tRi has trained two rheumatology specialty nurses and updated over 300 medical doctors on rheumatology in Ghana. Supported by the International League of Associations for Rheumatology (ILAR), the Royal College of Physicians (RCP), the British Society for Rheumatology (BSR), the Ghana College of Physicians and Surgeons (GCPS), Korle Bu Teaching Hospital (KBTH), and pharmaceutical companies, tRi collaborated to conduct clinical training programs in Accra, Kumasi, and Cape Coast, aiming to improve patients’ access to skilled healthcare providers.
In 2018, the RCP and tRi assessed healthcare requirements for rheumatological services and the potential for broader training dissemination. This assessment recognized the need for leadership and a “train the trainer” component within the clinical training program to extend its reach to underserved communities. Applicants from regions outside Accra were given preference. The director of tRi, a rheumatologist, served as the course convenor, overseeing course development, design, and recruitment of local teaching faculty and participants. Initially, there was a gap in confidence and engagement between participants with prior rheumatology experience and general practitioners. However, participation and confidence improved significantly as the program progressed and incorporated more interactive sessions.
Given limited resources and funding, tRi adopted community-based participatory research to address health disparities. The shortage of specialists means many patients with autoimmune conditions are seen by general practitioners, leading to late diagnoses and poor prognoses. Therefore, doctors must integrate effective mobile education and monitoring systems into their practices to educate patients about their conditions and improve health outcomes.
The MEMTIP study (Mobile Technology for Education, Improving Hospital Follow-ups, and Medication Reminders) conducted by tRi received a grant from the International League of Associations for Rheumatology (ILAR). This study piloted mobile technology to improve literacy rates among patients with autoimmune rheumatic conditions, enabling timely health information delivery, especially for those living far from specialist care. This implementation research aimed to enhance knowledge, awareness, and sustained care, reducing complications and mortality. The study focused on patients with Systemic Lupus Erythematosus (SLE) and Rheumatoid Arthritis (RA). Participants, who consented and had access to mobile technology, were divided into intervention and control groups. Baseline demographic assessments and questionnaires including ACREU Rheumatoid Arthritis Questionnaire (18) and Lupus Knowledge Questionnaire (19), measured health literacy before and after the intervention. The intervention group received mobile applications with important health information, appointment reminders, and relevant messages please see Table 1.
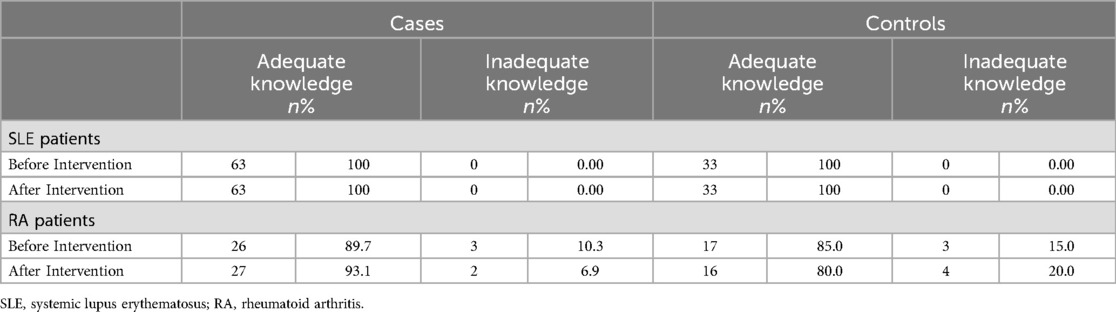
Table 1. Changes in the knowledge of participants before and after intervention.
Most participants had significant knowledge before the intervention, with RA cases and controls at 89.7% and 85% respectively, and SLE cases and controls at 100%. This high baseline knowledge was attributed to existing support groups like tRi and Global Lupus Outstanding Warriors (GLOW), which already disseminate health information via mobile phones. Additionally, many participants regularly used their phones to access information on their conditions, primarily from Google and healthline.com.
In an audit of referrals to the Korlebu Teaching Hospital rheumatology unit to evaluate the impact of previous educational efforts on general practitioners’ referral patterns for autoimmune diseases in Ghana. Preliminary findings from this ongoing audit reveal that, during the first quarters of 2018, 2021, and 2022, there was a successive increase of referrals from 48 in 2018 to 80 in 2021 and 81 in 2022. This persistent increase indicates that general practitioners in Ghana are becoming more aware of autoimmune diseases and have improved their skills in identifying patients with suspected rheumatic conditions.
tRi collaborates with governmental and non-governmental entities to advocate for policies promoting rheumatology care and improving accessibility. Collaborations with the Royal College of Physicians and the International League of Associations for Rheumatology facilitate training opportunities for local rheumatologists and allied health professionals. Over the past few years, tRi has lobbied locally for government support for individuals with lupus and other rheumatic conditions and has made some progress. tRi was invited to provide input into the Ghana standard treatment guidelines list, allowing drugs needed to treat Lupus to be in the guidelines, hence improving access through health insurance schemes. In 2017, tRi was part of efforts to ratify World Lupus Day in Ghana by the Ministry of Health, officially recognizing it as an existing disease.
One of the most innovative solutions implemented by tRi is Rheumchat, a cost-effective and scalable telemedicine platform designed to improve access to care for individuals with autoimmune conditions across Ghana. The Rheumchat service was developed to address the significant barriers to healthcare access in remote and underserved areas of Ghana. Rheumchat operates via a toll-free short code, enabling users to access the service through simple text messaging. Users follow a text prompt and answer these questions when they dial the short code (*844*555*3#) options for screening or education. Their telephone numbers and responses are then automatically forwarded to a call center via an instant text message and email. Upon receiving a text, the system provides an initial set of prompts to screen users for symptoms related to autoimmune rheumatic diseases. These prompts include questions about joint pain, swelling, fatigue, skin rashes, and other common symptoms associated with conditions such as Systemic Lupus Erythematosus (SLE) and Rheumatoid Arthritis (RA). Persons with symptoms highly suggestive of a rheumatic disease via the screening tools algorithm are contacted and referred to rheumatologists at the Department of Rheumatology or GPs in various regions. Should the need arise, referrals are made to other departments. Out of 144 shortlisted beneficiaries from tRi organized conferences and workshops, 25 Doctors volunteered their services with the project. Patients identified as having a rheumatological problem from engaging with the shortcode and being selected by the algorithm are referred to these networks of doctors for evaluation and follow-up. An average of 20 patients were screened every month.
Rheumchat streamlines the rheumatology referral process in Ghana and reduces delays in receiving care. It offers a cost-effective solution by minimizing the need for initial in-person consultations and lowering patient travel expenses. Rheumchat represents a significant advancement in leveraging technology to expand access to rheumatology care in resource-limited settings. By providing a straightforward, accessible platform for initial screening and referrals, Rheumchat helped to bridge the gap between remote communities and specialized healthcare, ultimately improving patient outcomes and reducing the burden of untreated autoimmune diseases in Ghana.
Education is extremely important for improving the early detection and management of rheumatic disorders, particularly in limited-resource settings like Sub-Saharan Africa. Providing physicians with training on diagnostic criteria empowers them to evaluate patients and begin necessary investigations effectively. Research emphasizes the critical importance of prompt diagnosis and proactive treatment in improving outcomes for rheumatic disease patients. These interventions highlight the significant impact of tRi's interventions in improving awareness, diagnosis, and management of rheumatic diseases in Ghana, while also underscoring the ongoing challenges in resource-limited settings.
Language diversity and cultural barriers can hinder the dissemination of rheumatology-related information effectively. In some cases, medical terminologies may not exist in local languages, making it challenging to convey important information to the general public or healthcare providers, these gaps have been addressed so patients and carers have gained insights into the disease, making it easier to manage.
The rheumatology health capacity in Ghana has been enhanced, and the training programs have strengthened the knowledge and skills of local healthcare professionals. This has improved the quality of rheumatology care, enhancing patient outcomes and quality of life. Various activities, including the education and training of GPs, have resulted in significant referral changes. Diagnosis time has decreased, and referrals are now more accurate than before. These comprehensive care and patient education initiatives have led to better disease management and treatment adherence.
Physician and patient education, self-help programs, and shared decision-making are essential clinic best practices. Both physician and patient education improve overall outcomes in chronic diseases like SLE, and measures to improve these can improve care even in the context of minimal resources (20). Recent endeavours to enhance the treatment of Systemic Lupus Erythematosus (SLE) have yielded results across various African regions. South Africa has achieved notable progress in managing SLE, marked by enhanced healthcare accessibility, specialized clinics, and heightened awareness among healthcare providers (21). Programs focused on patient education and establishing multidisciplinary care teams have notably bolstered outcomes for individuals with SLE. Morocco has also seen improvements in SLE care, with the establishment of dedicated lupus clinics and the implementation of national treatment guidelines (5). Increased research collaborations and efforts to enhance early diagnosis and treatment have positively impacted patient outcomes (5). The rapid adoption of mobile phones and smartphones among populations more likely to have low health literacy presents a tremendous opportunity for improving access to health information and tools to improve health (16).
The increasing availability of technology and digital tools presents an opportunity for tRi, Ghana, to expand its reach and impact. The organisation can leverage its partnerships to influence policy decisions and improve access to care for SLE patients. There is also the potential to collaborate with international organisations and researchers to advance knowledge and research in the field.
Ghana's Rheumatology Initiative (tRi) has significantly improved SLE care through educational activities and targeted projects. While challenges persist, the collaborative efforts of tRi and its partners have contributed to enhanced awareness, capacity building, and research advancements in care. Continued support and investment in such initiatives are crucial for addressing the evolving burden of rheumatic diseases like SLE in resource-limited settings like Ghana.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
DD: Project administration, Formal Analysis, Data curation, Conceptualization, Writing – review & editing, Writing – original draft, Supervision, Methodology. RB: Methodology, Formal Analysis, Data curation, Conceptualization, Writing – original draft, Writing – review & editing. BK: Writing – review & editing, Writing – original draft, Methodology, Formal Analysis, Data curation, Conceptualization. SI: Writing – review & editing, Writing – original draft, Data curation, Conceptualization. AC: Writing – review & editing, Writing – original draft, Methodology, Conceptualization. AC: Writing – review & editing, Writing – original draft, Data curation, Conceptualization. PN: Writing – review & editing, Writing – original draft, Data curation, Conceptualization.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors wish to extend their heartfelt appreciation to The Rheumatology Initiative (tRi) members, whose valuable insights and thoughtful discussions significantly enriched this work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wolfe F, Michaud K, Li T, Katz RS. Chronic conditions and health problems in rheumatic diseases: comparisons with rheumatoid arthritis, noninflammatory rheumatic disorders, systemic lupus erythematosus, and fibromyalgia. J Rheumatol. (2010) 37(2):305–15. doi: 10.3899/jrheum.090781
2. Adelowo O, Mody GM, Tikly M, Oyoo O, Slimani S. Rheumatic diseases in Africa. Nat Rev Rheumatol (Review). (2021) 17:363–74. doi: 10.1038/s41584-021-00603-4
3. Bae SC, Fraser P, Liang MH. The epidemiology of systemic lupus erythematosus in populations of African ancestry: a critical review of the “prevalence gradient hypothesis” Arthritis Rheum. (1998) 41:2091–9. doi: 10.1002/1529-0131(199812)41:12%3C2091::AID-ART2%3E3.0.CO;2-D
4. Symmons DP. Frequency of lupus in people of African origin. Lupus. (1995) 4:176–8. doi: 10.1177/096120339500400303
5. Mody GM. Rheumatology in Africa—challenges and opportunities. Arthritis Res Ther. (2017) 19:49. doi: 10.1186/s13075-017-1259-3
6. Dey D, Paruk F, Mody GM, Kalla AA, Adebajo A, Akpabio A, et al. Women in rheumatology in Africa. Lancet Rheumatol. (2022) 4(10):e657–60. doi: 10.1016/S2665-9913(22)00255-7
7. Eastin J, Dey D, Amissah-Arthur MB, Chaudhuri K, Jawad A. Capacity building for the provision of rheumatological services in sub-Saharan Africa. Clin Rheumatol. (2021) 40:3439–43. doi: 10.1007/s10067-020-05058-8
8. Tickly M, McGill P. Epidemiology: the challenge of practicing rheumatology in Africa. Nat Rev Rheumatol. (2016) 12(11):630–1. doi: 10.1038/nrrheum.2016.170
9. Meenan R. Rheumatology manpower — the US perspective. Br J Rheumatol. (1991) 30:81. doi: 10.1093/rheumatology/30.2.81
10. Amissah-Arthur MB, Gyaban-Mensah A, Boima V, Yorke E, Dey D, Ganu V, et al. Health-seeking behavior, referral patterns, and associated factors among patients with autoimmune rheumatic diseases in Ghana: a cross-sectional mixed method study. PLoS One. (2022) 17(9):e0271892. doi: 10.1371/journal.pone.0271892
11. Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R., et al. European league against rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol. (2019) 71(9):1400–12. doi: 10.1002/art.40930
12. Dey D. Juggling art: making critical clinical decisions without vital laboratory support in autoimmune rheumatic patients in a resource-poor setting. Ghana Med J. (2017) 51(2): 119–21. doi: 10.4314/gmj.v51i2.1
13. Dey D, Oduro-Afriyie A, Okine R. Rheumatoid arthritis in Ghana—a description of an inception cohort. Afr J Rheumatol. (2020) 8(2). Available online at: https://www.ajol.info/index.php/ajr/article/view/198904.
14. Narh PP, Can-Tamakloe AAAA, Dey ID. Support groups and patient centred care; making a difference in the lives of people with autoimmune and rheumatic conditions in Ghana. Arthritis Rheumatol. (2018) 70(suppl 9). Available online at: https://acrabstracts.org/abstract/support-groups-and-patient-centred-care-making-a-difference-in-the-lives-of-people-with-autoimmune-and-rheumatic-conditions-in-ghana/ (accessed August 10, 2024).
15. Marengo MF, Suarez-Almazir ME. Improving treatment adherence in patients with rheumatoid arthritis: what are the options? Int J Clin Rheumtol. (2015) 10(5):345–56. doi: 10.2217/ijr.15.39
16. Kwabara A, Su S, Krauss J. Utilizing digital health technologies for patient education in lifestyle medicine. Am J Lifestyle Med. (2019) 14(20):137–42. doi: 10.1177/1559827619892547
17. Mackert M, Mabry-Flynn A, Champlin S, Donovan EE, Pounders K. Health literacy and health information technology adoption: the potential for a new digital divide. J Med Internet Res. (2016) 18(10):e6349. doi: 10.2196/jmir.6349
18. Lineker SC, Badley EM, Hughes EA, Bell MJ. Development of an instrument to measure knowledge in individuals with rheumatoid arthritis: the ACREU rheumatoid arthritis knowledge questionnaire. J Rheumatol. (1997) 24(4):647–53. PMID: 9101496.9101496
19. Sullivan SL. Development of a Systemic Lupus Erythematosus Knowledge Questionnaire: The Relationship among Disease Proximity, Educational Exposure, and Knowledge. Milwaukee: The University of Wisconsin (2016).
20. Navarra SV, Zamora LD, Collante MTM. Lupus education for physicians and patients in a resource-limited setting. Clin Rheumatol. (2020) 39(3):697–702. doi: 10.1007/s10067-019-04795-9
Keywords: systemic lupus erythematosus (SLE), education, intervention, research, Africa, the rheumatology initiative (tRi), rheumatic diseases
Citation: Dey D, Bobade R, Katso B, Issaka S, Charis A, Can Tamakloe AA and Narh P (2024) Enhancing systemic lupus erythematosus care and outcomes through innovative interventions by the rheumatology initiative (tRi) in Ghana. Front. Lupus 2:1462320. doi: 10.3389/flupu.2024.1462320
Received: 9 July 2024; Accepted: 22 August 2024;
Published: 5 September 2024.
Edited by:
Cindy Hilary Flower, The University of the West Indies, BarbadosReviewed by:
Sharon Dowell, NEA Baptist Memorial Hospital, United StatesCopyright: © 2024 Dey, Bobade, Katso, Issaka, Charis, Can Tamakloe and Narh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dzifa Dey, ZHppZmFrYXlAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.