 Melinda Nagy-Vincze1,2*
Melinda Nagy-Vincze1,2* Dorottya Szinay1,2
Dorottya Szinay1,2 Katalin Szabó1,2Sarolta Molnár Deliné3László Balkay4Tibor Béldi1,2,†
Katalin Szabó1,2Sarolta Molnár Deliné3László Balkay4Tibor Béldi1,2,† Zoltán Griger1,2
Zoltán Griger1,2
- 1Division of Clinical Immunology, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
- 2Gyula Petrányi Doctoral School of Allergy and Clinical Immunology, University of Debrecen, Debrecen, Hungary
- 3Pathology Institute, University of Debrecen, Debrecen, Hungary
- 4Department of Medical Imaging, Division of Nuclear Medicine, University of Debrecen, Debrecen, Hungary
Background: Several systemic autoimmune rheumatic diseases may affect both fetal and maternal outcomes during pregnancy. However, little information is available regarding pregnancy outcomes in women with idiopathic inflammatory myopathy. Previously published articles stated that the activity of maternal disease may worsen pregnancy outcomes. A former multicenter study suggested that anti-Jo1 antibody positivity and joint involvement could distinguish a more vulnerable group regarding pregnancy complications. Our aim was to identify prognostic factors among clinical symptoms at disease onset and auto-antibody profiles for identifying a high-risk group for poor pregnancy outcome.
Methods: The clinical data of the myositis cohort of the Division of Clinical Immunology, University of Debrecen, Hungary, were reviewed retrospectively. IIM diagnoses were made by Bohan and Peter's criteria or European Alliance of Associations for Rheumatology/American College of Rheumatology (EULAR/ACR) criteria. Disease activity was evaluated based on physician opinion. Gynecological definitions were used to evaluate fetal outcomes.
Results: Reviewing clinical data of overall 763 patients (542 women and 221 men) revealed that 5.2% of female patients had pregnancies in the same time or after myositis onset. Among these, 71.4% of the mothers suffered from polymyositis (PM) and 28.6% suffered from dermatomyositis (DM). Their mean age at the time of myositis diagnosis was 25.28 years, and the average interval between myositis diagnosis and first pregnancy was 55.4 months. Maternal complications included preeclampsia in one case and pregnancy-induced myositis in 25% of cases. All cases of pregnancy-induced myositis improved after immunosuppressive treatment. Twenty-eight patients reported 60 pregnancies overall, with multiple pregnancies occurring in 57% of cases. Early or late fetal loss was detected in 41.7% of the pregnancies, and stillbirth occurred in 18.3% of deliveries. Although late fetal loss was observed mainly due to placental insufficiency in patients with anti-Jo1 positivity and complications seemed more frequent in PM cases, logistic regression analysis only confirmed that multiple pregnancies could be an independent risk factor for fetal (p = 0.0112) and interstitial lung disease of maternal complications (p = 0.02).
Conclusion: Internal organ involvement and the number of pregnancies could influence pregnancy outcomes in myositis patients. Patients’ family planning should be well organized and counseled by myositis experts. Prospective, multicenter collaborations are needed to precisely identify high-risk groups and state managing guidelines.
Introduction
Idiopathic inflammatory myopathies (IIMs) are a heterogeneous group of systemic autoimmune rheumatic diseases (SARDs) characterized by progressive muscle weakness and specific skin symptoms. Internal organs, including the skin, joints, lungs, heart, and gastrointestinal tract, can also be affected in both skin-dominant [dermatomyositis (DM)] and muscle-dominant forms [polymyositis (PM)] (1).
Like other SARDs, idiopathic inflammatory myopathies may affect both fetal and maternal outcomes during pregnancy. Probably due to the rarity of the disease or its later onset, there is only one short consensus guideline for planning and managing pregnancy in these patients (2). Correlations between clinical and pathological alterations have been barely studied. Based on previous studies, only 12%–29% of IIM cases are recognized during the reproductive years (3–6). A couple of retrospective cohort studies revealed that the activity of maternal disease could worsen pregnancy outcomes (3–10). Complete remission refers to a better fetal outcome (1), while high disease activity increases abortion rates above 50% (7) and increases the risk of stillbirth or neonatal death (5). Our former multicenter study suggested that anti-Jo1 antibody positivity and joint involvement could distinguish a more vulnerable group considering fetal pregnancy complications (8). Except pregnancy induced myositis cases maternal outcome is generally favorable (9). Based on several case series and reports, “pregnancy-induced” myositis could be a leading risk factor considering maternal outcomes (3–11). A population-based study reported an increased risk of hypertensive disorders of pregnancy in patients with DM/PM compared with the general population (OR = 2.18, 95% CI: 1.37–3.46) (10). No data are available concerning medication risks during and after pregnancy or the effect of myositis on breastfeeding.
Our aims were to evaluate the frequency of maternal and fetal pregnancy complications in myositis, find prognostic factors of maternal and fetal complications among clinical symptoms and auto-antibody profiles, and identify high-risk groups for unfavorable pregnancy outcomes.
Materials and methods
A retrospective data analysis of the myositis cohort at the University of Debrecen was used to assess the frequency and outcome of pregnancies after IIM onset. Clinical data from 763 patients (542 women and 221 men) diagnosed between 2000 and 2022 were reviewed.
IIM diagnoses were made using Bohan and Peter's criteria or EULAR/ACR diagnostic criteria. Myositis-specific and associated auto-antibodies were identified by ELISA and immunoblot techniques; anti-phospholipid (APL) antibodies, including anti-b2glycoprotein IgG and IgM, anti-cardiolipine IgG and IgM, and thyroid-specific antibodies [anti-thyroperoxidase (TPO)], were detected using the ELISA technique. Detection of lupus anticoagulant (LAC) was made by dilute Russell's viper venom time (dRVVT) test. Disease activity was evaluated and recorded in medical files based on clinical symptoms, muscle enzyme levels, and physician opinion before 2011 and using International Myositis Assessment and Clinical Studies Group (IMACS) core set measures thereafter. As this is a retrospective cohort study when disease activity was evaluated with different methods for statistical analysis, patients were categorized into active and inactive groups. Pregnancy data were self-reported by the mother and supplemented with medical records. Pregnancy-induced myositis was defined as IIM symptoms that began during pregnancy or within 6 months following delivery or termination.
Data on general maternal complications, such as gestational diabetes, hypertension, preeclampsia, eclampsia, and excessive bleeding, were recorded. Also, disease-specific complications, such as weak contractions, pregnancy-induced myositis, relapses, or worsening of clinical symptoms, were collected.
Gynecological definitions were used to evaluate fetal outcomes. Normal labor was defined as the delivery of a healthy newborn weighing >2,500 g after 37 weeks of pregnancy. Stillbirth was defined as the end of a pregnancy between gestational weeks 28 and 37. Abortion or miscarriage was defined as a pregnancy ending before 28 weeks, without specification as spontaneous or induced. Early pregnancy losses occurred in the first trimester, and late losses occurred in the second trimester. We considered pregnancy losses observed in the third trimester as fetal deaths.
After descriptive statistics, Fisher's exact test was used to prove univariate associations and logistic regression analysis was conducted to identify independent risk factors for fetal and maternal complications. Myositis subset, maternal age, organ involvement, auto-antibodies, number of pregnancies, and disease activity were included in the analysis.
Results
General myositis characteristics
Data collection revealed that 5.2% (n = 28) of the 542 female patients had pregnancies either concurrently with or after myositis onset. Among these, 71.4% (n = 20) suffered from polymyositis and 28.6% (n = 8) suffered from dermatomyositis. Their mean age at the time of IIM diagnosis was 25.4 years. A total of 75% (n = 21) of patients had a longer history, with an average disease duration of 55.4 months, while 25% (n = 7) of women suffered from pregnancy-induced myositis. Half of the DM patients had a juvenile-onset disease. The most common clinical symptoms were muscle weakness (96%; n = 27), arthralgia (64%; n = 18), and Raynaud’s phenomenon (54%; n = 15). Skin rashes, interstitial lung disease, and dysphagia are classified as rare manifestations. Table 1 presents the basic demographic data of the cohort. There were no significant differences in clinical and serological characteristics. Multiple pregnancies were more frequent in the PM subset than in DM (70% vs. 25%; p = 0.04). No therapy refractory cases have been reported. Based on the opinion of the treating physician, mild or moderate disease activity was identified in 46% (n = 13) of cases before or after conception. Muscle enzyme levels varied from normal to slightly elevated, with no significant correlation to pregnancy outcomes. Check-ups were organized at various intervals, unfortunately lacking consistency. No mothers were on teratogenic medication before pregnancy or at the time of conception. Corticosteroids alone or in combination with azathioprine, cyclosporine A, and/or intravenous immunoglobulin (IVIg) were used. During and after pregnancy, mothers were either treatment-free (11%; n = 3), treated with corticosteroid only (64%; n = 18), or treated with corticosteroid and azathioprine combination (25%; n = 7). One mother had been on methotrexate before conception, but it was discontinued when they were planning the pregnancy. One mother was on cyclophosphamide therapy due to interstitial lung disease (ILD) at the time of conception, and this pregnancy ended in miscarriage. Due to variations in medications, we have excluded them from statistical analysis. Low-molecular-weight heparin (LMWH) and low-dose aspirin (100 mg) were also used in APL-positive cases after pregnancy pathology, as former APL guidelines suggested.
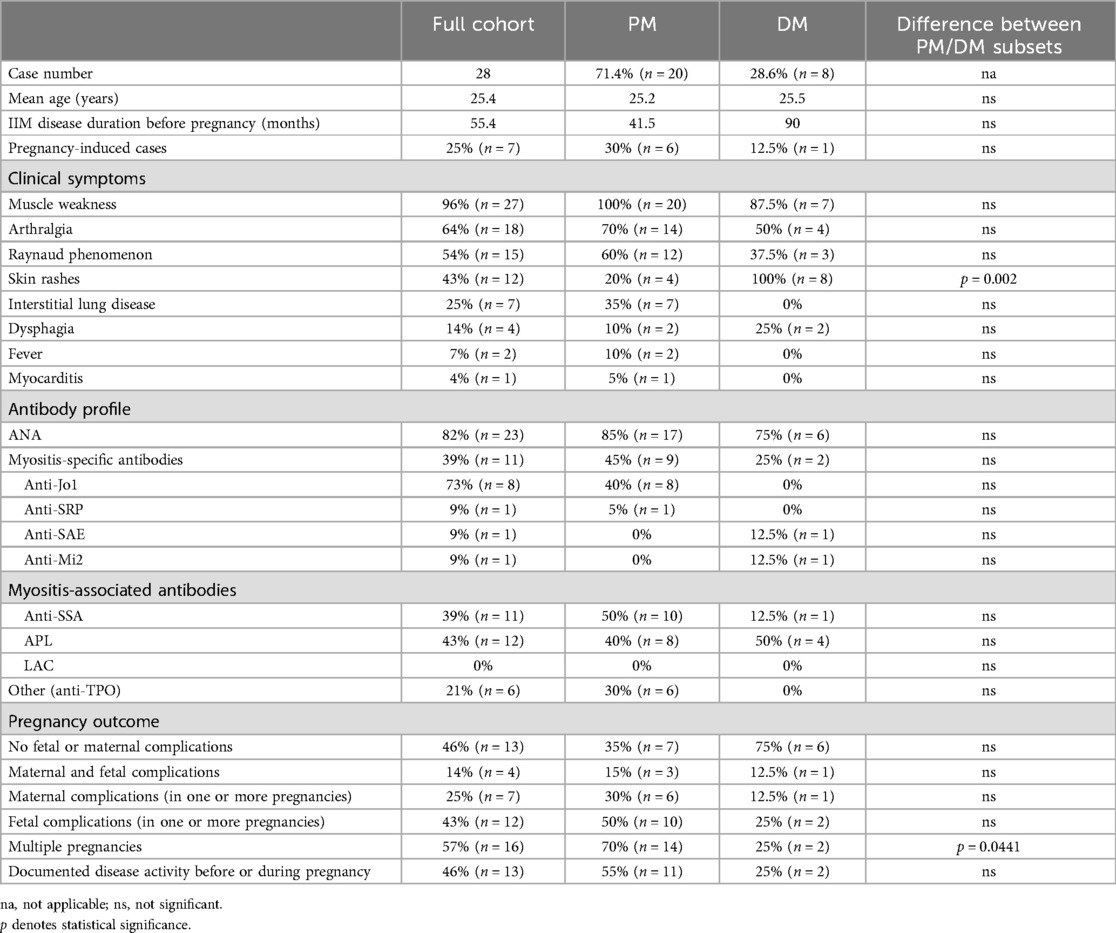
Table 1. Basic clinical and serological data of our cohort.
Immunofluorescent staining of blood samples showed that 82% (n = 23) of women with pregnancy complications were positive for antinuclear antibodies (ANAs). In total, 11% (n = 3) of women had no detectable auto-antibodies in their serum before pregnancy. A total of 36% (n = 10) of them had a single (mostly anti-phospholipid) antibody, while 54% (n = 15) showed multiple antibody positivity. Lupus anticoagulant analysis was performed in only 75% of cases (n = 21), but all results were negative. Myositis blot analysis revealed myositis-specific (39%; n = 11) and myositis-associated (50%; n = 14) antibodies. Detected IIM-specific antibodies were anti-Jo1 (73%; n = 8), anti-SAE, anti-Mi2, and anti-SRP in individual cases. Among myositis-associated antibodies, anti-SSA was detected as frequently as myositis specific antibodies (MSA) (39%; n = 11).
Maternal outcomes
In general, maternal outcomes in IIM were favorable. Preeclampsia was reported in only one case. Pregnancy-induced IIM was reported in 25% of all cases, with 42% (n = 3) in the first trimester, 29% (n = 2) in the third trimester of pregnancy, and 29% (n = 2) after delivery or termination. No variable showed a significant association with maternal complications in univariate testing. Interstitial lung disease was identified as an independent risk factor for maternal complications (OR: 12; 95% CI: 1.48–97.18; p = 0.02) by logistic regression analysis. All pregnancy-induced cases improved with individualized immunosuppressive treatment. The most frequently used drug was intravenous corticosteroids in these cases; high-dose IVIg was used in one severe case when the mother presented with new-onset anti-phospholipid syndrome accompanied by myositis, arthritis, fever, and interstitial lung disease.
Fetal outcomes
In the case of our 28 patients, 73 pregnancies were recorded, 60 of which were conceived after IIM onset. Patients did not report any pregnancy complications before myositis symptoms. Multiple pregnancies occurred in 57% (n = 16) of cases. In contrast to favorable maternal outcomes, depressing fetal results were found (Figure 1). Only 58% (n = 35) of pregnancies ended with delivery, with one-third of the delivered babies being born prematurely. Stillbirth was reported in 18.3% of all pregnancies and in 31.4% of labors. Early or late fetal loss was detected in 41.7% of the pregnancies (n = 25). In the first trimester, we only recorded miscarriages, along with one case of induced abortion due to high maternal disease activity. Unfortunately, no gynecological reports are available considering the potential causes of these pregnancy losses. All 12 patients who experienced miscarriages were auto-antibody-positive (anti-Jo1, anti-SRP, anti-TPO, and APL). Among patients with fetal pregnancy complications, 50% (n = 7) were APL-positive, but there were no significant differences considering fetal complications in APL-negative cases. LAC testing was performed in 75% of all patients, but all results were negative. Of the seven patients who were not tested for LAC, only one reported miscarriages. High disease activity before pregnancy was reported by the treating physician in only three cases.
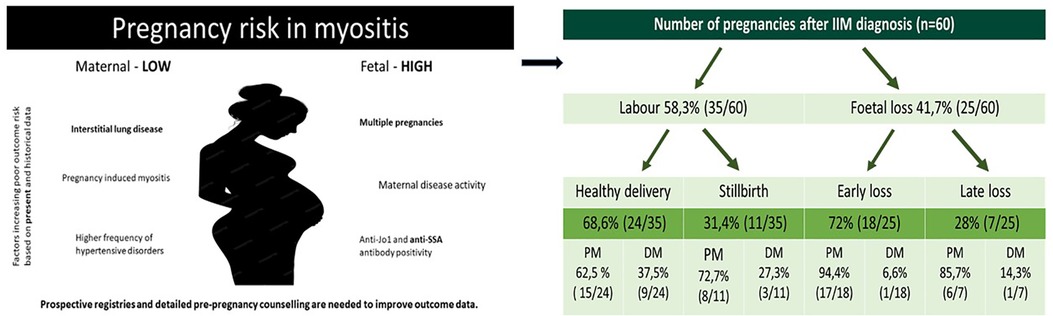
Figure 1. Main causes of maternal and fetal complications reported previously and in this study (bold); and different fetal complications during pregnancies of IIM patients in the Hungarian cohort.
Late pregnancy losses, which placed a more excessive physical and mental burden on the mothers, were reported in seven pregnancies across five women. They all were treated with proper immunosuppressive medication and had no or mild disease activity. In the cases where full gynecological descriptions were available (only four of these seven pregnancies), fetal death was associated with placental insufficiency due to early calcification or circulation issues. Late pregnancy loss was mostly observed in patients suffering from anti-synthetase syndrome (n = 3). Histopathological examination of the placenta is rare, even after fetal death. Placental insufficiency was associated with various histological findings. We also recognized a rare pathological manifestation, massive perivillous fibrinoid deposition (MPVN, Figure 2), in the placenta in the case of a woman suffering from anti-synthetase syndrome and anti-SSA antibody positivity who had experienced several pregnancy losses.
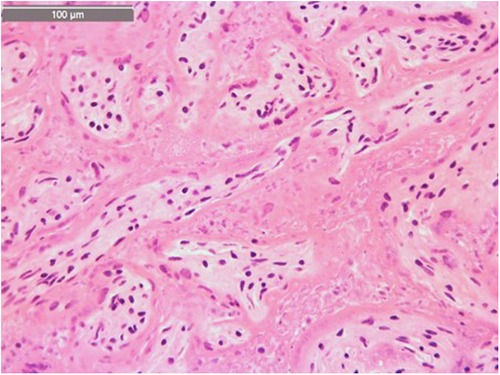
Figure 2. MPVN as a sub-phenomenon of placentitis by hematoxylin-eosin staining from the archive of our pathology institute.
In cases of pregnancy-induced myositis (n = 7), four stillbirths and two early miscarriages were reported. These mothers also experienced complications in subsequent pregnancies, regardless of disease activity.
Reviewing polymyositis patients' medical documentation fetal complication have been found twice frequent than healthy deliveries (31 complications vs. 15 healthy baby). This ratio was 9 healthy baby vs. 5 fetal complications in patients suffering from dermatomyositis. Although complications seemed more frequent in PM cases, results did not reach statistical significance. Univariate analysis showed that anti-SSA antibody positivity was significantly more frequent in patients with fetal complications (17.6% vs. 66.7%; p: 0.014). Logistic regression analysis confirmed that multiple pregnancies could be an independent risk factor for fetal complications (OR: 4.19; CI: 1.39–12.69; p = 0.0112). Based on our data, a poor outcome in a first pregnancy is associated with poor outcomes in subsequent pregnancies. The cause of repeated poor outcomes could not be revealed by our data.
Discussion
Detailed reports on pregnancy outcomes and complications in patients with idiopathic inflammatory myopathies are scarce. Based on our large cohort, we can assume that maternal outcomes in pregnancies of IIM patients appear favorable. Neither our cohort nor previously reported ones exhibited specific maternal complications (3–9, 11–17). As an exception, Kolstad et al. published a population-based study concluding that IIM patients have longer hospitalization during delivery and an increased risk of hypertensive disorders, including preeclampsia and eclampsia, but no increased risk for fetal complications (10). In other reports, similar to our cohort, disease relapse or onset during or shortly after pregnancy was considered a risk for maternal health.
On the contrary, IIM is considered a high-risk group regarding fetal complications. A limitation of this study is the retrospective design and the heterogeneity of medical documentation. Reviewing the literature in this research field, we can state that several fetal complications have been reported, and high fetal risks are not obviously associated with maternal disease activity. A recent review also stated that only 52.8% of pregnancies in IIM patients ended with the birth of a healthy child (4). Relatively poor pregnancy outcomes have been reported, including spontaneous/induced abortion in 27.6% of pregnancies, stillbirth/neonatal death in 7.5%, preterm birth in 12.6%, intrauterine growth retardation in 4.7%, and low birth weight in 7.4%. Among 159 pregnancies occurring after DM/PM onset, only 50 involved active disease. The difference in abortion rates (36% vs. 29.5%) between pregnancies with active disease and pregnancies with inactive disease did not reach statistical significance. However, the proportion of total fetal loss (48% vs. 35%, P = 0.049) was significantly higher in pregnancies with active maternal disease. Pregnancy-induced cases have also reported more fetal complications (31.4% vs. 67.2%) (5). Previous studies also mentioned high rates of abortion/miscarriage (43%–50%) and preterm births (6, 7, 11–16), mostly in women with active IIM. Even earlier studies revealed that pregnancies in patients with juvenile-onset IIM were associated with a high percentage of at-term births, while in women with adult-onset IIM before pregnancy, this percentage decreased to 50%. Among patients diagnosed with PM–DM during pregnancy, the percentage of live births was 38% (7, 14). A Swedish population-based study revealed about a threefold increased risk of preterm birth (particularly very preterm birth) and a sixfold increased risk of low birth weight in IIM patients compared with the non-IIM group (17). Because myositis core set measures (18), manual muscle test results, and creatine kinase (CK) levels are not reported in the above-mentioned articles, judgment about disease activity and its association with fetal outcomes is heterogeneous. Detailed antibody profiles of the patients are also missing.
Our results suggest that, in addition to disease activity, multiple pregnancies and disease characteristics also influence fetal outcomes, especially in relation to late pregnancy complications. The observed late fetal losses occurred only during pregnancies of antibody-positive mothers. Massive perivillous fibrin deposition is a rare sign of severe placentitis previously associated with anti-phospholipid syndrome and infections (19, 20). We have found some case reports describing this rare pathological finding in pregnancies of IIM patients. Hung et al. presented the case of a 20-year-old anti-Jo1-positive polymyositis patient who delivered a stillborn fetus and damaged placenta with MPVN (19). Krones et al. reported the case of a new-onset MDA-5-positive DM with skin, muscle, and lung involvement. During this women's pregnancy MPVN was also reported as histopathological background of fetal complication. She delivered a premature baby at 34 weeks via an emergency cesarean section due to decreased fetal movements and a non-reassuring fetal heart rate. The maternal disease was stabilized by corticosteroid, hydroxychloroquine, and JAK inhibitor treatment. However, no information about the infant's outcome was available (20). In contrast to these cases, our patient exhibited anti-Jo1 and anti-SSA antibody positivity, showed no signs of disease activity, and was on combined immunosuppressive therapy. Unfortunately, her pregnancy ended in fetal loss due to placentitis. Her other pregnancy ended in a preterm delivery, but fortunately with a healthy infant. The placental macroscopic and histological findings were the same. Another patient with anti-Jo1 and anti-SSA antibody positivity delivered a stillborn infant at 36 weeks due to placental hypoxia and circulation issues. In this case, an autopsy was not recommended by the obstetrician.
The role of anti-phospholipid antibodies and lupus anticoagulant in pregnancy complications among myositis patients remains unknown. A limitation of our study is the lack of data; however, all tested patients were negative for LAC, while 50% of patients with fetal pregnancy complications were APL-positive. Although IIMs are rarely associated with anti-phospholipid syndrome (21), we need prospective, well-organized studies to reach further conclusions.
Summarizing previous and current results, we can conclude that the risk of fetal complications in patients with myositis is high. Although the stillbirth rate in the general population in Hungary is considered high (8%–9%) (22), this rate is even higher (31.4%) in our IIM cohort. There is an unmet need for prospective, detailed studies to identify the causal relationships between disease activity, organ involvement, auto-antibody profiles, and maternal outcomes. Close monitoring of pregnancies in IIM patients, even without disease activity and placenta autopsies after healthy or complicated pregnancies, could help explore the pathomechanism of placental insufficiency and decrease fetal complication rates. Prospective studies are needed to evaluate the connection between disease activity, serology profiles, myositis symptoms, and pregnancy outcomes. Family planning for these patients should be well organized and counseled by myositis experts, with multi-disciplinary collaborations and consensus guidelines to improve worrying fetal outcomes.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics statement
This study involving human participants was approved by the Regional and Institutional Ethics Committee, University of Debrecen (RKEB 6144-2022). The study was conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired primarily isolated as part of our previous study for which ethical approval was obtained. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
MN-V: Writing – original draft. DS: Data curation, Investigation, Writing – review & editing. KS: Data curation, Investigation, Writing – review & editing. SM: Visualization, Writing – review & editing. LB: Methodology, Writing – review & editing. TB: Data curation, Investigation, Methodology, Writing – review & editing. ZG: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lundberg IE, Fujimoto M, Vencovsky J, Aggarwal R, Holmqvist M, Christopher-Stine L, et al. Idiopathic inflammatory myopathies. Nat Rev Dis Primers. (2021) 7(1):86. doi: 10.1038/s41572-021-00321-x
2. Oldroyd A, Lilleker JB, Amin T, Aragon O, Bechman K, Cuthbert V, et al. British Society for Rheumatology guideline on management of paediatric, adolescent and adult patients with idiopathic inflammatory myopathy. Rheumatology. (2022) 61:1760–1. doi: 10.1093/rheumatology/keac115
4. Papapetropoulos T, Kanellakopoulou N, Tsibri E, Paschalis C. Polymyositis and pregnancy: report of a case with three pregnancies. J Neurol Neurosurg Psychiatry. (1998) 64:406. doi: 10.1136/jnnp.64.3.406
5. Tang K, Zhou J, Lan Y, Zhang H, Jin H. Pregnancy in adult-onset dermatomyositis/polymyositis: a systematic review. Am J Reprod Immunol. (2022) 88(5):e13603. doi: 10.1111/aji.13603
6. Mino R, Shimada H, Wakiya R, Nakashima S, Miyagi T, Sugihara K, et al. Pregnancy course and outcomes of patients with polymyositis and dermatomyositis (PM/DM) managed in a single center. Medicine (Baltimore). (2023) 102(14):e33462. doi: 10.1097/MD.0000000000033462
7. Gutiérrez G, Dagnino R, Mintz G. Polymyositis/dermatomyositis and pregnancy. Arthritis Rheum. (1984) 27(3):291–4. doi: 10.1002/art.1780270307
8. Nagy-Vincze M, Vencovsky J, Lundberg IE, Dankó K. Pregnancy outcome in idiopathic inflammatory myopathy patients in a multicenter study. J Rheumatol. (2014) 41(12):2492–4. doi: 10.3899/jrheum.140438
9. Pinal-Fernandez I, Selva-O’Callaghan A, Fernandez-Codina A, Martinez-Gomez X, Rodrigo-Pendas J, Perez-Lopez J, et al. Pregnancy in adult-onset idiopathic inflammatory myopathy: report from a cohort of myositis patients from a single center. Semin Arthritis Rheum. (2014) 44(2):234–40. doi: 10.1016/j.semarthrit.2014.05.004
10. Kolstad KD, Fiorentino D, Li S, Chakravarty EF, Chung L. Pregnancy outcomes in adult patients with dermatomyositis and polymyositis. Semin Arthritis Rheum. (2018) 47(6):865–9. doi: 10.1016/j.semarthrit.2017.11.005
11. Gupta L, Zanwar A, Ahmed S, Aggarwal A. Outcomes of pregnancy in women with inflammatory myositis: a cohort study from India. J Clin Rheumatol. (2020) 26(5):165–8. doi: 10.1097/RHU.0000000000000996
12. Gomes V, Mesquita A, Capela C. Autoimmune diseases and pregnancy: analysis of a series of cases. BMC Res Notes. (2015) 8:216. doi: 10.1186/s13104-015-1177-x
13. Zhong Z, Lin F, Yang J, Zhang F, Zeng X, You X. Pregnancy in polymyositis or dermatomyositis: retrospective results from a tertiary centre in China. Rheumatology. (2017) 56:1272–5. doi: 10.1093/rheumatology/kex070
14. Doria A, Iaccarino L, Ghirardello A, Briani C, Zampieri S, Tarricone E, et al. Pregnancy in rare autoimmune rheumatic diseases: UCTD, MCTD, myositis, systemic vasculitis and Beçhet disease. Lupus. (2004) 13:690–5. doi: 10.1191/0961203304lu1098oa
15. Silva CA, Sultan SM, Isenberg DA. Pregnancy outcome in adult-onset idiopathic inflammatory myopathy. Rheumatology. (2003) 42:1168–72. doi: 10.1093/rheumatology/keg318
16. Akiyama C, Shirai T, Sato H, Fujii H, Ishii T, Harigae H. Association of various myositis-specific autoantibodies with dermatomyositis and polymyositis triggered by pregnancy. Rheumatol Int. (2022) 42:1271–80. doi: 10.1007/s00296-021-04851-1
17. Che WI, Hellgren K, Stephansson O, Lundberg IE, Holmqvist M. Pregnancy outcomes in women with idiopathic inflammatory myopathy, before and after diagnosis—a population-based study. Rheumatology. (2020) 59:2572–80. doi: 10.1093/rheumatology/kez666
18. Miller FW, Rider LG, Chung YL, Cooper R, Danko K, Farewell V, et al. Proposed preliminary core set measures for disease outcome assessment in adult and juvenile idiopathic inflammatory myopathies. Rheumatology. (2001) 40(11):1262–73. doi: 10.1093/rheumatology/40.11.1262
19. Hung NA, Jackson C, Nicholson M, Highton J. Pregnancy-related polymyositis and massive perivillous fibrin deposition in the placenta: are they pathogenetically related? Arthritis Rheum. (2006) 55(1):154–6. doi: 10.1002/art.21710
20. Krones C, Vu M, Popp B, Scardamaglia L. New onset MDA-5 positive dermatomyositis and massive perivillous fibrin deposition in third trimester of pregnancy: a case report. J Obstet Gynaecol Res. (2023) 49:1620–3. doi: 10.1111/jog.15625
21. de Souza FH, Levy-Neto M, Shinjo SK. Antiphospholipid syndrome and dermatomyositis/polymyositis: a rare association. Rev Bras Reumatol. (2012) 52(4):642–4.22885428
22. Statistical Yearbook of Hungarian Central Statistical Office (2016). www.ksh.hu/docs/hun/xftp/idoszaki/pdf/koraszul16.pdf
Keywords: polymyositis, dermatomyositis, pregnancy, outcome, miscarriages, internal organ involvement
Citation: Nagy-Vincze M, Szinay D, Szabó K, Molnár Deliné S, Balkay L, Béldi T and Griger Z (2024) High fetal risk in pregnancies of myositis patients—a Hungarian cohort study. Front. Lupus 2:1449390. doi: 10.3389/flupu.2024.1449390
Received: 14 June 2024; Accepted: 11 November 2024;
Published: 4 December 2024.
Edited by:
Angela Tincani, ASST-Spedali Civili and University of Brescia, ItalyReviewed by:
Amanda Eudy, Duke University, United StatesMaddalena Larosa, University Hospital of Padua, Italy
Copyright: © 2024 Nagy-Vincze, Szinay, Szabó, Molnár Deliné, Balkay, Béldi and Griger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Melinda Nagy-Vincze, bmFneS12aW5jemUubWVsaW5kYUBtZWQudW5pZGViLmh1
†ORCID:
Tibor Béldi
orcid.org/0000-0003-4972-1370