 Antonio Bustos-Merlo
Antonio Bustos-Merlo Nuria Navarrete-Navarrete
Nuria Navarrete-Navarrete Lourdes González-Navarrete
Lourdes González-Navarrete María Martín-Armada
María Martín-Armada- 1Autoimmune and Systemic Diseases Unit, Department of Internal Medicine, Hospital Universitario Virgen de las Nieves, Granada, Spain
- 2Department of Internal Medicine, Hospital Universitario de Canarias, Tenerife, Spain
Relapsing polychondritis (RP) is an immune-related condition involving inflammation of cartilaginous structures and other body tissues, especially affecting the ears, nose, eyes, joints and respiratory tract. Approximately one-third of patients with RP have an identifiable form of systemic vasculitis, connective tissue disease, other autoimmune disease, or a malignant or premalignant condition. In this report, we present the case of a 50-year-old woman who met criteria for systemic lupus erythematosus (SLE) and was diagnosed with RP several months later. The main objective was to investigate cases of overlap syndrome involving RP and SLE. A literature review of reported cases with this coexistence was conducted, examining presentation, predominant symptoms, laboratory data, complications and systemic involvement. The review included a total of 12 cases of overlap syndrome of RP and SLE, analysing the epidemiology, temporal relationship, clinical features, diagnosis, treatment and evolution of the reported cases. Although this overlapping presence is rare (less than 1%), it emphasises the importance of maintaining a high index of suspicion for RP in patients with SLE who present with recurrent episodes of scleritis, audiovestibular involvement and chondritis.
Introduction
Relapsing polychondritis (RP) is a rare inflammatory disease of unknown etiology and autoimmune basis. It is characterised by recurrent inflammatory lesions affecting cartilage, cardiovascular system and sensory organs. After its initial description by Jaksch-Wartenhorst in 1923 as polychondropathy (1), several authors have reported cases under different names, with Pearson's proposal, chronic atrophic polychondritis, being the most widely accepted (2). The epidemiology of RP is unclear, with an estimated annual incidence between 0.71 and 2.0 per million people (3, 4). It affects both sexes equally, mainly seen in the fifth decade of life. Up to one third of patients with RP have a recognisable form of systemic vasculitis, connective tissue disease or other autoimmune disorder, or a malignant or pre-malignant autoimmune disease (5, 6). A high percentage of patients with a genetic disease described in 2020 called VEXAS syndrome (vacuoles, E-1 enzyme, X-linked, autoinflammatory, somatic) have an initial clinical diagnosis of RP (7). VEXAS syndrome is characterised by manifestations such as recurrent fever, skin and lung inflammation, auricular and nasal chondritis, vasculitis, deep vein thrombosis and arthralgias, together with progressive haematological abnormalities including macrocytic anaemia and thrombocytopenia.
In this report, we describe a rare case of overlap syndrome involving PR and systemic lupus erythematosus (SLE), accompanied by a review of the literature.
Clinical case
A 50-year-old Caucasian woman presented to the outpatient clinic for review after being diagnosed with SLE during a hospital admission four months earlier. Table 1 describes her clinical and laboratory features prior to the current admission, including those that scored as criteria for SLE classification. The patient had 19 ACR/EULAR points for SLE classification, with 10 being the minimum required in addition to the presence of antinuclear antibodies (ANAs). The patient was under treatment with prednisone (7.5 mg), hydroxychloroquine (100 mg) and acetylsalicylic acid (100 mg) daily. Despite treatment, the patient returned to experience daily fever up to 38°C, which she tolerated well. In addition, she had bilateral parotid swelling and auditory symptoms such as vertigo, hearing loss and tinnitus in both ears. He also experienced hemicranial headache, with partial improvement after the use of regular analgesics. Three months prior to the current visit, the patient sought relief from her headaches through multiple punctures of both pinnae at an acupuncture centre. The day after these procedures, she experienced marked swelling in the auricular cartilages, as seen in Figure 1.
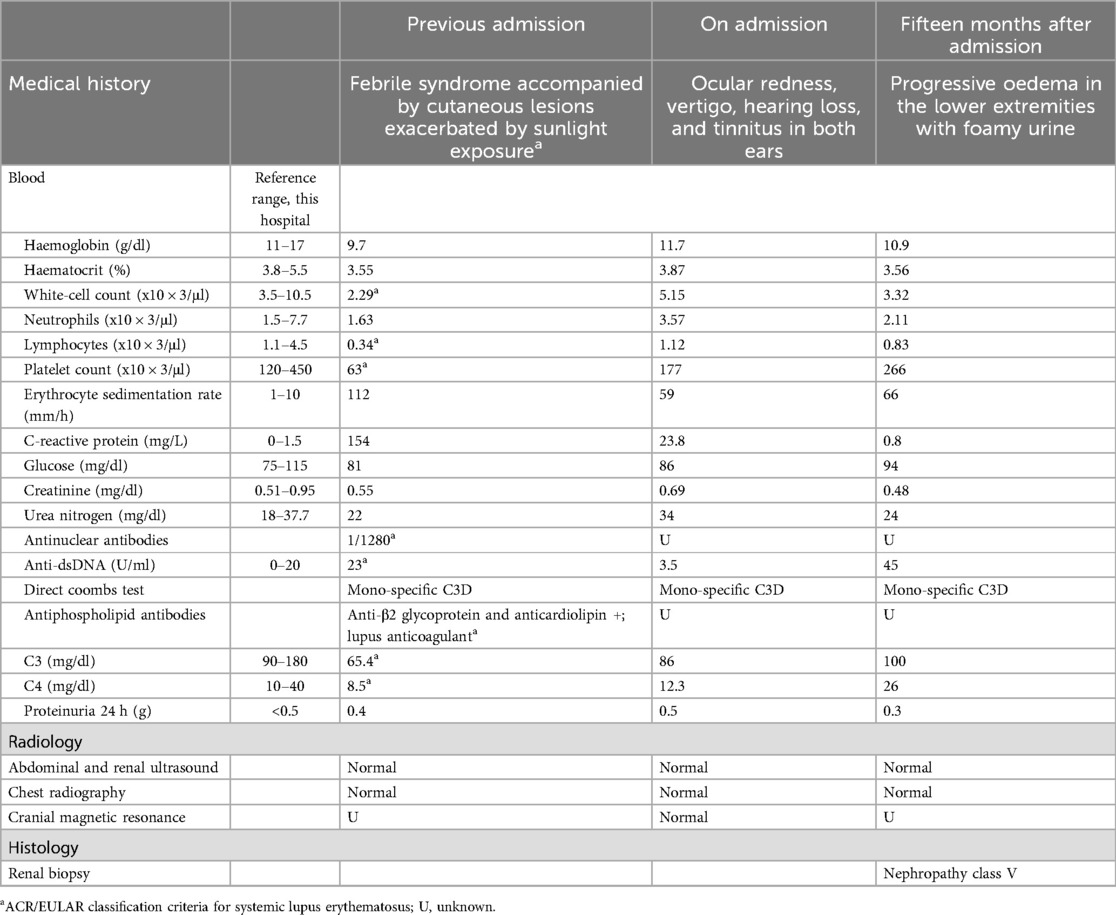
Table 1. Characteristics and laboratory data of our case patient.

Figure 1. Image of the patient, shows swelling of the left auricle.
The symptoms disappeared spontaneously two weeks after onset. On physical examination, the patient's vital signs were as follows: blood pressure 130/73 mmHg, heart rate 77 bpm and temperature 36.5°C. Ocular redness was observed left. Pupils were isochoric, normoreactive to light and accommodation, with preserved extrinsic eye movements. No alterations were detected in the cranial nerves. Sensibility and strength were preserved in all extremities. When gait was explored at, there was a tendency to fall to the left. The Romberg's test was negative. The parotid glands were enlarged and painful on palpation.
During the evaluation by the otorhinolaryngologist, a diagnosis of sudden sensorineural hearing loss in the left ear with a severe left vestibular deficit was made. Simultaneously, she was reviewed by the ophthalmologist, who diagnosed acute scleritis in the right eye. Topical ocular glucocorticoid therapy was started, together with intravenous boluses of methylprednisolone (100 mg for 3 days) and immunoglobulins (20 mg daily for 5 days). Despite ocular improvement, the audiovestibular symptomatology showed little improvement. Therefore, it was decided to administer intratympanic dexamethasone. Subsequently, oral glucocorticoid treatment was maintained, associated with subcutaneous administration of methotrexate. The patient was left with severe auditory and vestibular sequelae. During follow-up in the following months, the patient presented recurrent episodes of polychondritis (affecting the auricular pavilions, the nose and the costosternal area) and recurrent scleritis. Colchicine was added to her usual treatment, the dose of methotrexate was increased to 15 mg weekly and adalimumab was added. These episodes resulted in a saddle-shaped nasal deformity. After 15 months of follow-up, the patient experienced progressive edematisation of the lower limbs with foamy urine. Methylprednisolone 250 mg boluses were administered for 3 days and a renal biopsy was performed, with a diagnosis of class V lupus nephropathy. Treatment with adalimumab, which had successfully controlled the episcleritis, was discontinued and remission induction with cyclophosphamide 500 mg fortnightly for 3 months and subsequent maintenance with mycophenolate mofetil was performed. Subsequently, tacrolimus was added, which was ineffective. Finally, indicated treatment with rituximab (1 g/15 days, 2 doses). Two months after starting rituximab, total protein excretion was 0.45 g per day. Currently, the patient undergoes regular check-ups and maintains a residual non-nephrotic range proteinuria of about 0.3 g per day.
Discussion
A comprehensive search of MEDLINE databases was conducted through PubMed and EMBASE until 1 February 2023. All articles describing cases of overlap syndrome of RP and SLE were considered for inclusion. Cases that did not meet the established criteria for the diagnosis of SLE or had incomplete information were excluded. No language restrictions were applied in the search. In addition, the references of the selected articles were screened to ensure the completeness of the search. In total, 20 references were included, covering 46 cases; however, clinical and analytical features were detailed in only 11 references, totalling 12 cases. The flow chart provides a visual representation of the complete search and the articles incorporated in the review (Figure 2).
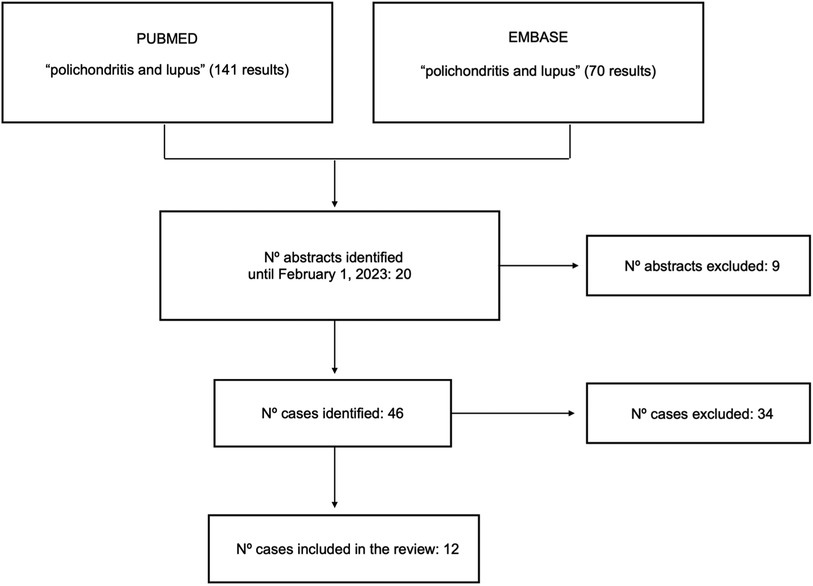
Figure 2. Flow chart of the selection of articles included in this review.
A total of 12 cases were included and analyzed, all of whom were women. Their characteristics are presented in Tables 2–4 (8–18). The mean age of the published cases with this coexistence was 37.5 years with a median of 46.5 years (range 29–75). Although in our case, RP appeared after the diagnosis of SLE, we observed that it can appear simultaneously (15–17), later (10, 11, 16), with a latency period of up to 9 years (10) or prior to (12, 14). In terms of clinical manifestations, chondritis was present in all cases, with the most frequent affected site being the outer ear, either unilaterally or bilaterally. Ocular involvement was present in 33.3%, in the form of conjunctivitis, scleritis or episcleritis (8, 12, 13, 17). Although we can see that the audiovestibular manifestations that presented in our patient are not so frequent; vestibular syndrome in 16.6% (11, 17) and sensorineural hypoacusis in 23.08% (11, 13, 17). The same applies to the involvement of the nasal cartilage, which was affected in 25% of cases (12, 16, 17). As it coincides with the series of patients with SLE, urinary alteration is seen in approximately half of the cases described. Cardiac involvement occurred in only 1 case (8). With regard to analytical parameters, which are not specified in most publications, elevated erythrocyte sedimentation rate (ESR) was found in five cases (8, 10–12, 15). Regarding the presence of published antibodies, are positive the double-stranded anti-dsDNA antibodies in five cases (8, 10, 13, 14, 18, 19). Regarding histopathology, renal biopsy was performed in four patients and skin biopsy in four other patients. The most frequently used treatment was oral corticosteroids together with hydroxychloroquine. There was only one case of rituximab administration for neurological manifestations (14). There was little information regarding patient follow-up, being unknown in most of them. Complications included, as in our patient, saddle nose deformity in 16.6% (9, 12) and one case of respiratory distress syndrome due to tracheal stenosis and the need for urgent tracheostomy (12).
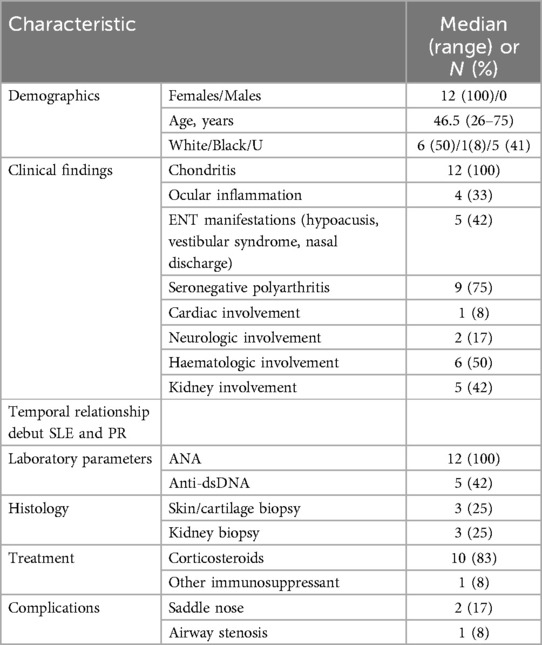
Table 2. Demographics and clinical findings of reported cases.

Table 3. Epidemiology and clinic of detailed reported cases.
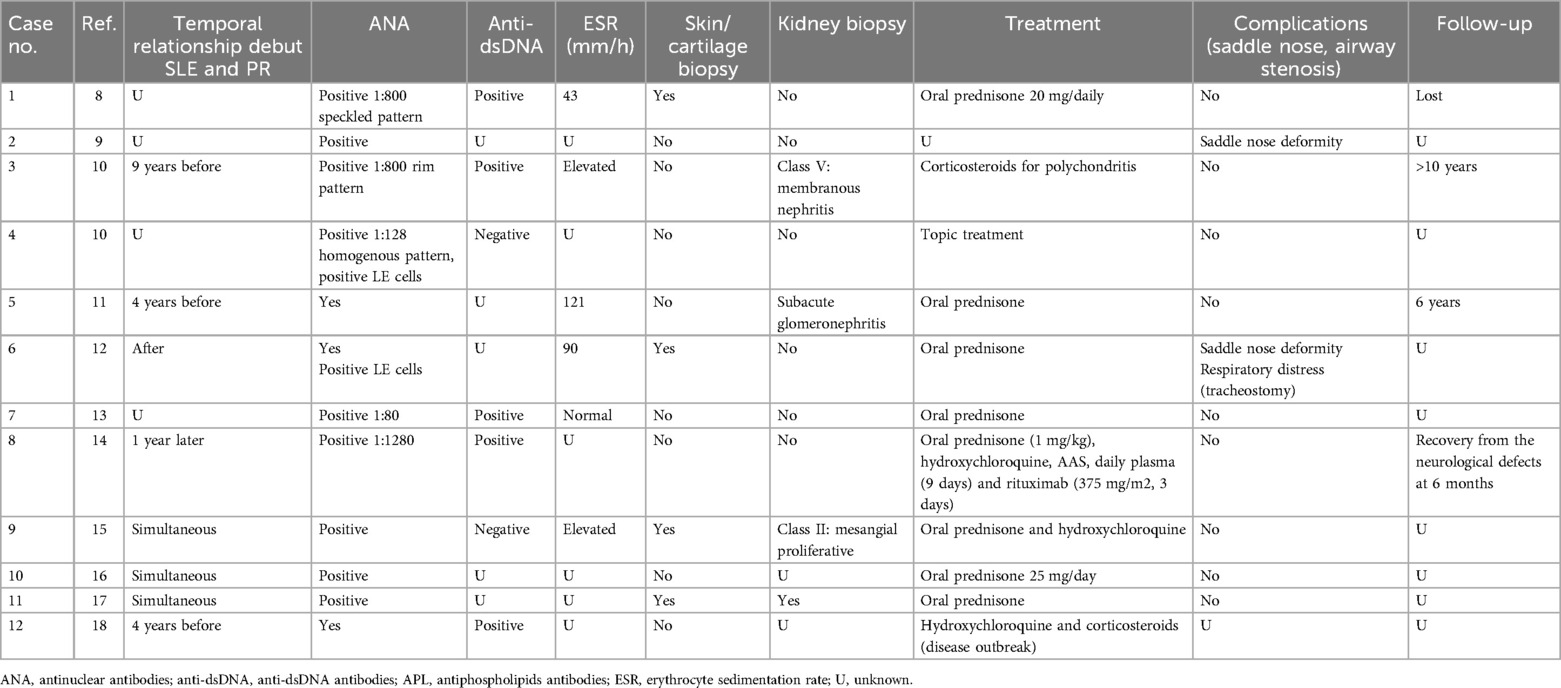
Table 4. Chronological relationship, complementary tests, treatment and evolution of the reported cases.
This review provides a comprehensive overview of the overlap of RP and SLE, highlighting the diversity of clinical manifestations and the need to consider this connection in clinical management. The differential diagnosis of RP should include granulomatosis with polyangiitis, eosinophilic granulomatosis with polyangiitis, Behçet's disease, Cogan's syndrome (interstitial keratitis and audiovestibular dysfunction) and leprosy. In the case of a male patient VEXAS, which may present with chondritis of the ear (usually unilateral) or of the nose, thrombopenia and macrocytic anaemia, should be noted. As with other immune-mediated diseases, coexistence with another immune-mediated disease, in this case SLE, is not uncommon. Interestingly, both our patient and all cases published in the literature are female. The reason for this is unknown, although we know that this prevalence of female gender is observed in most autoimmune and immune-mediated diseases in general. There are several hypotheses to explain the current gender bias. The human endosomal Toll-like receptors, TLR7 and TLR8, are important mediators of innate immunity and autoimmune pathogenesis. Their signalling promotes the earliest appearance of haematopoietic cells during development and thereafter influences the fate and function of primitive and effector immune cell types (20). TLR7 and TLR8 are encoded respectively by adjacent X-linked genes. Both evade X-chromosome inactivation in female immune cells. Cells harbouring foci of simultaneous TLR7 and TLR8 transcription are more frequent in females and males with Klinefelter syndrome than in euploid males, resulting in a sevenfold frequency difference (21). Active co-dependent transcription. In addition, it has been shown that there is a mechanism by which TLR7 and TLR8 direct monocyte fate and identify a specialised population of phagocytes responsible for inflammation and infection-associated anaemia and thrombocytopenia (22). Elevated levels of interferon gamma have also been corroborated in both murine models and human patients with SLE, systemic sclerosis and Sjögren's syndrome (23), indicating that interferon gamma may be another factor contributing to female bias in autoimmunity.
The clinical course of RP is unpredictable and variable between patients. In relation to ear involvement, unilateral or bilateral external ear inflammation is the most common presenting feature, with hearing impairment, tinnitus or vertigo being less common (24). The latter is a consequence of inner ear inflammation associated with destruction induced by Eustachian tube chondritis, endolymphatic hydrops or sensorineural hearing loss or vasculitis of the internal auditory artery or its cochlear branch. Hearing and/or vestibular involvement may occur acutely or insidiously at some point, and occurs in approximately one third of patients (25). Eye disease is a common problem, affecting about 20% of patients at presentation and up to about 60% at some point during the course of the disease (24, 26, 27). Symptoms of nasal cartilage inflammation include congestion, crusting, rhinorrhoea, epistaxis, pain, redness and swelling of the bridge of the nose, and/or nasal pressure. Nasal chondritis is present in approximately 20% of patients at presentation and in 60% over the course of the disease (24). Cartilage destruction associated with sustained or recurrent episodes of inflammation may result in a characteristic saddle-shaped deformity of the nose, seen in about 10% of patients at presentation and in 25% during the course of the disease. Arthritis is seen at presentation in up to one-third of patients, and peripheral joint involvement eventually occurs in approximately 50%–70% (24, 28). There is no predilection for large or small joints. Cardiac involvement due to clinically significant aortic or mitral valve disease occurs in approximately 10% of patients (29). Renal involvement, as determined by biopsy or the presence of hematuria and/or proteinuria, remains unclear and is probably very rare, although there are series describing renal involvement in up to 23% of cases (30). Neurological manifestations are unusual in RP (31) and neurological involvement is presumed to be due to the presence of another associated disease, as it has rarely been documented in RP due to vasculitis phenomena (32). However, at that time there was no specific test to diagnose patients with antineutrophil cytoplasmic antibody-associated vasculitis. Laboratory blood tests are not used in the absence of a specific parameter for the diagnosis of RP. Elevations of ESR or C-reactive protein (CRP), and modest leukocytosis or thrombocytosis are associated with clinical and subclinical disease activity. The appearance of ANA and antiDNA positivity are not characteristic of RP and should raise suspicion of coexisting SLE (33). Antiphospholipid antibodies are associated with obstetric complications and thrombotic events, although they have also been associated with other symptoms, including chondritis. The association is not well known and studies are needed to establish it. The coexistence or RP and antiphospholipid syndrome (APS) is very uncommon and there is no convincing evidence regarding the association between them when APS occurs in RP. It seems to be more closely related to association with SLE (34). The cases discussed in this article did not present APS and the presence of APS is not detailed in the majority of the patients. Skin biopsy is reserved for situations where the patient does not have a multi-organ cartilaginous inflammatory syndrome or does not respond to glucocorticoids (5). Due to the rarity of RP, to date there are no standardised therapeutic guidelines on treatment, which means that therapy is tailored empirically according to disease activity and the nature of organ involvement (35). Glucocorticoids may decrease disease activity and reduce the frequency of recurrence (36, 37). Immunosuppressive agents such as azathioprine, methotrexate and cyclosporine may be given in non-responders or when a corticosteroid-sparing effect is needed (38–41). Although well-designed randomised clinical trials are lacking and the evidence for their use is mainly based on expert opinion, biologic agents are also showing a role in the therapeutic approach to these patients. However, data on rituximab administration are controversial and this agent is not recommended as a first-line biologic in the treatment of patients with RP (42).
Overlap syndrome between SLE and RP is extremely rare (<1%). Since the diagnosis of RP is based on clinical findings, it is crucial to maintain a high index of suspicion for RP in the presence of recurrent scleritis, audiovestibular involvement and chondritis in patients with SLE, especially those in the fourth-fifth decade of life. This case highlights the importance of early diagnosis and immediate therapeutic intervention, especially in situations of severe manifestations of RP, due to the sequelae damage that can result from severe and recurrent inflammation and deterioration in the patient's quality of life. The management of patients with 2 potentially aggressive diseases such as SLE and RP requires a treat-to-target strategy. The multidisciplinary approach and a very close follow-up will determine whether the treatment is adequate or whether dose adaptations, treatment changes or even non pharmacological interventions are required, e.g., assessment by a psychologist, control of anxiety or depression symptoms, indication of hearing aids, surgical interventions for aesthetic deformities or others. Undoubtedly, this work has some limitations, as it deals with a series of non-homogeneous cases. We have made an effort to compare them and to highlight the relevance of considering the diagnosis of relapsing polychondritis in patients with suggestive symptoms, despite the fact that SLE may also have similar chronic inflammatory signs. Specialists who treat patients with autoimmune diseases are well aware that no two patients are alike, and that the diseases can present in different ways. We also know that several of them can coexist in the same patient, a common finding in patients with immune-mediated diseases. The differentiating features of both diseases, SLE and RP, are what will lead to the suspicion of their coexistence. Only persistent study and updating of knowledge by specialists will allow suspicion, diagnosis and appropriate treatment of these patients. Under-diagnosis of one of the entities can have fatal consequences.
Patient perspective
A Story of Resilience: Living with Relapsing Polychondritis and Systemic Lupus Erythematosus.
The first symptoms of my illness started with tiredness, when it was seven o'clock in the evening I had to lie down and sleep, I didn't think anything of it, I put it down to work. The first episode of inflammation of the ears was with fever and a lot of pain for about 2 weeks, but since then I always had the feeling of having hard ears. After about a month, I began to have a severe headache every day, which was worse at night, as was the fever. As the days went by I had a very annoying noise in my left ear, and my eyes, alternately, became very red and very painful, I began to feel dizzy and had a very strange sensation when I walked. I went to my internal medicine specialist and was hospitalised, during which time I lost my hearing for about 8–10 days, but after treatment I recovered a little, which still allows me to hear with the help of hearing aids. For the first few months I needed a cane to walk as I had no balance. C ith the help of vestibular rehabilitation at home and in the hospital, as well as walking every day and doing yoga, I managed to improve partially. At first the episodes of red eyes were recurrent, with a lot of pain, accompanied by fever and headache quite often. Later I was diagnosed with lupus nephritis. The sun harms me a lot, it causes reddening of the skin and itching, I always wear sun protection.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
AB-M: Writing – review & editing, Writing – original draft. NN-N: Writing – review & editing. LG-N: Writing – original draft. MM-A: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
APS, antiphospholipid antibodies; ANA, antinuclear antibodies; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; RP, relapsing polychondritis; SLE, systemic lupus erythematosus; TLR, toll-like receptors; VEXAS, vacuoles, E-1 enzyme, X-linked, autoinflammatory, somatic.
References
2. Pearson CM, Kline HM, Newcomer VD. Relapsing polychondritis. N Engl J Med. (1960) 263:51–8. doi: 10.1056/NEJM196007142630201
3. Hazra N, Dregan A, Charlton J, Gulliford MC, D'Cruz DP. Incidence and mortality of relapsing polychondritis in the UK: a population-based cohort study. Rheumatology (Oxford). (2015) 54:2181. doi: 10.1093/rheumatology/kev240
4. Horváth A, Páll N, Molnár K, Kováts T, Surján G, Vicsek T, et al. A nationwide study of the epidemiology of relapsing polychondritis. Clin Epidemiol. (2016) 8:211. doi: 10.2147/CLEP.S91439
5. Francès C, el Rassi R, Laporte JL, Rybojad M, Papo T, Piette J. Dermatologic manifestations of relapsing polychondritis. A study of 200 cases at a single center. Medicine (Baltimore). (2001) 80:173. doi: 10.1097/00005792-200105000-00003
6. Letko E, Zafirakis P, Baltatzis S, Voudouri A, Livir-Tallatos C, Foster CS. Relapsing polychondritis: a clinical review. Semin Arthritis Rheum. (2002) 31:384. doi: 10.1053/sarh.2002.32586
7. Beck DB, Ferrada MA, Sikora KA, Ombrello AK, Collins JC, Wuhong Pei NB, et al. Somatic mutations in UBA1 and severe adult-onset autoinflammatory disease. N Engl J Med. (2020) 383:2628. doi: 10.1056/NEJMoa2026834
8. Harisdangkul V, Johnson WW. Association between relapsing polychondritis and systemic lupus erythematosus. South Med J. (1994) 87:753–7. doi: 10.1097/00007611-199407000-00017
9. Job-Deslandre C, Delrieu F, Delbarre F, Carilioz A. Relapsing polychondritis and systemic lupus erythematosus. J Rheumatol. (1983) 10:666–8.6620269
10. Small P, Frenkiel S. Relapsing polychondritis. A feature of systemic lupus erythematosus. Arthritis Rheum. (1980) 23:361–3. doi: 10.1002/art.1780230317
11. Cody DT, Sones DA. Relapsing polychondritis: audiovestibular manifestations. Laryngoscope. (1971) 81:1208–22. doi: 10.1288/00005537-197108000-00004
12. Kaye RL, Sones DA. Relapsing polychondritis. Clinical and pathologic features in fourteen cases. Ann Intern Med. (1964) 60:653–64. doi: 10.7326/0003-4819-60-4-653
13. Aflaki E, Nazarinia MA, Habib Agahi Z, Shenavandeh S, Jahanbani MR, Zahedi Kashkooli L, et al. Systemic lupus erythematosus associated with relapsing polychondritis. Shiraz E Med J. (2008) 9:163–5.
14. Bellon N, Anguel N, Vandendries C, Goujard C, Lambotte O. Auricular chondritis and thrombotic microangiopathy: an unusual combination revealing systemic lupus erythematosus. Joint Bone Spine. (2013) 80:424–5. doi: 10.1016/j.jbspin.2012.11.002
15. Nguyen MA, Rahnama-Moghadam S, Gilson RT. An uncommon presentation of an uncommon disease: relapsing polychondritis overlap with systemic lupus erythematosus. Dermatol Online J. (2016) 22:13030. doi: 10.5070/D3222030091
16. Suyama Y, Ishimoto SI, Hagiwara K. Clinical images: arytenoid chondritis. Arthritis Rheumatol. (2017) 69:1193. doi: 10.1002/art.4008810.1002/art.40088
17. Rogers PH, Boden G, Tourtellotte CD. Relapsing polychondritis with insulin resistance and antibodies to cartilage. Am J Med. (1973) 55:243–8. doi: 10.1016/0002-9343(73)90175-7
18. Le Brun M, Koubi M, Gomes De, Pinho Q, Raguin E, Benyamine A, Granel B. Une oreille boursoufflée [A swollen ear]. Rev Med Interne. (2022) 43:690–1. doi: 10.1016/j.revmed.2022.06.002
19. Snyder JM, Treuting PM, Nagy L, Yam C, Yi J, Brasfield A, et al. Humanized TLR7/8 expression drives proliferative multisystem histiocytosis in C57BL/6 mice. PLoS One. (2014) 9:E107257. doi: 10.1371/journal.pone.0107257
20. Youness A, Cenac C, Faz-López B, Grunenwald S, Barrat FJ, Chaumeil J, et al. TLR8 escapes X chromosome inactivation in human monocytes and CD4(+) T cells. Biol Sex Differ. (2023) 14:60. doi: 10.1186/s13293-023-00544-5
21. Akilesh HM, Buechler MB, Duggan JM, Hahn WO, Matta B, Sun X, et al. Chronic TLR7 and TLR9 signaling drives anemia via differentiation of specialized hemophagocytes. Science. (2019) 363(6423):eaao5213. doi: 10.1126/science.aao5213
22. Theofilopoulos AN, Koundouris S, Kono DH, Lawson BR. The role of IFN-gamma in systemic lupus erythematosus: a challenge to the Th1/Th2 paradigm in autoimmunity. Arthritis Res. (2001) 3:136–41. doi: 10.1186/ar290
23. Willeke P, Schluter B, Schotte H, Domschke W, Gaubitz M, Becker H. Interferon-gamma is increased in patients with primary Sjogren’s syndrome and Raynaud’s phenomenon. Semin Arthritis Rheum. (2009) 39:197–202. doi: 10.1016/j.semarthrit.2008.04.002
24. Kent PD, Michet C Jr, Luthra HS. Relapsing polychondritis. Curr Opin Rheumatol. (2004) 16:56–61. doi: 10.1097/00002281-200401000-00011
25. Clark LJ, Wakeel RA, Ormerod AD. Relapsing polychondritis–two cases with tracheal stenosis and inner ear involvement. J Laryngol Otol. (1992) 106:841. doi: 10.1017/s002221510012105x
26. Isaak BL, Liesegang TJ, Michet CJ Jr. Ocular and systemic findings in relapsing polychondritis. Ophthalmology. (1986) 93:681. doi: 10.1016/s0161-6420(86)33695-9
27. Fukuda K, Mizobuchi T, Nakajima I, Kishimoto T, Miura Y, Taniguchi Y. Ocular involvement in relapsing polychondritis. J Clin Med. (2021) 10:4970. doi: 10.3390/jcm10214970
28. Mathew SD, Battafarano DF, Morris MJ. Relapsing polychondritis in the department of defense population and review of the literature. Semin Arthritis Rheum. (2012) 42:70. doi: 10.1016/j.semarthrit.2011.12.007
29. Lang-Lazdunski L, Hvass U, Paillole C, Pansard Y, Langlois J. Cardiac valve replacement in relapsing polychondritis. A review. J Heart Valve Dis. (1995) 4:227. PMID: 7655680.7655680
30. Chang-Miller A, Okamura M, Torres VE, Michet CJ, Wagoner R, Donadio J, et al. Renal involvement in relapsing polychondritis. Medicine (Baltimore). (1987) 66:202. doi: 10.1097/00005792-198705000-00004
31. Massry GG, Chung SM, Selhorst JB. Optic neuropathy, headache, and diplopia with MRI suggestive of cerebral arteritis in relapsing polychondritis. J Neuroophthalmol. (1995) 15:171. doi: 10.1097/00041327-199509000-00009
32. Cañas CA, Díaz-Martínez JC, Tobón GJ. Combination of hypertrophic pachymeningitis, PR3-ANCA-positive vasculitis, and relapsing polychondritis. J Rheumatol. (2011) 38:966. doi: 10.3899/jrheum.101238
33. Piette JC, El-Rassi R, Amoura Z. Antinuclear antibodies in relapsing polychondritis. Ann Rheum Dis. (1999) 58:656. doi: 10.1136/ard.58.10.656
34. Zeuner M, Straub RH, Schlosser U, Rauh G, Schmitz G, Schòlmerich J, et al. Anti-phospholipid-antibodies in patients with relapsing polychondritis. Lupus. (1998) 7:12–4. doi: 10.1191/096120398678919615
35. Dolan DL, Lemmon GB Jr, Teitelbaum SL. Relapsing polychondritis. Analytical literature review and studies on pathogenesis. Am J Med. (1966) 41:285. doi: 10.1016/0002-9343(66)90023-4
36. Lipnick RN, Fink CW. Acute airway obstruction in relapsing polychondritis: treatment with pulse methylprednisolone. J Rheumatol. (1991) 18:98. PMID: 2023206.2023206
37. Damiani JM, Levine HL. Relapsing polychondritis–report of ten cases. Laryngoscope. (1979) 89:929. doi: 10.1288/00005537-197906000-00009
38. Trentham DE, Le CH. Relapsing polychondritis. Ann Intern Med. (1998) 129:114. doi: 10.7326/0003-4819-129-2-199807150-00011
39. Park J, Gowin KM, Schumacher HR Jr. Steroid sparing effect of methotrexate in relapsing polychondritis. J Rheumatol. (1996) 23:937. PMID: 8724312.8724312
40. Stewart KA, Mazanec DJ. Pulse intravenous cyclophosphamide for kidney disease in relapsing polychondritis. J Rheumatol. (1992) 19:498. PMID: 1578473.1578473
41. Mellado F, Talesnik E, Castiglione E. Azathioprine as monotherapy for scleritis in relapsing polychondritis. Ocul Immunol Inflamm. (2012) 20:235. doi: 10.3109/09273948.2012.659369
Keywords: relapsing polychondritis, systemic lupus erythematosus, chondritis, audiovestibular involvement, overlap syndrome
Citation: Bustos-Merlo A, Navarrete-Navarrete N, González-Navarrete L and Martín-Armada M (2024) Case Report: Overlap syndrome of relapsing polychondritis and systemic lupus erythematosus observed in women: a comprehensive review and unique case presentation. Front. Lupus 2:1334214. doi: 10.3389/flupu.2024.1334214
Received: 6 November 2023; Accepted: 2 August 2024;
Published: 21 August 2024.
Edited by:
Elena Massarotti, Brigham and Women's Hospital and Harvard Medical School, United StatesReviewed by:
Naomi I. Maria, Northwell Health, United StatesOzge Basaran, Hacettepe University, Türkiye
Copyright: © 2024 Bustos-Merlo, Navarrete-Navarrete, González-Navarrete and Martín-Armada. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Bustos-Merlo, YW50b25pb2J1c3Rvc21lcmxvQGdtYWlsLmNvbQ==