
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Lang. Sci., 06 January 2025
Sec. Language Processing
Volume 3 - 2024 | https://doi.org/10.3389/flang.2024.1434420
This article is part of the Research TopicRevisiting a 150-year-old conundrum on the role of Broca’s area in language processing: Embracing expected and unexpected resultsView all 4 articles
 Agnès Trébuchon1,2*
Agnès Trébuchon1,2* Alexia Fasola1Véronique Sabadell1,2†
Alexia Fasola1Véronique Sabadell1,2† Anne-Sophie Dubarry3Romain Carron1,2†
Anne-Sophie Dubarry3Romain Carron1,2† Fabrice Bartolomei1,2
Fabrice Bartolomei1,2 F.-Xavier Alario3
F.-Xavier Alario3Background: Patients with drug-resistant epilepsy involving the language network often exhibit anomic profiles in daily life due to difficulties with lexical selection processes. Very little evidence is available regarding the effects of language rehabilitation in this population.
Objective(s): We aim to induce brain plasticity combined with improvements in behavioral performance using language therapy in patients with epilepsy.
Methods: We implemented a therapy focused on phonological and semantic features of infrequent words over three treatment sessions, each targeting a specific semantic category. Intracranial signals were recorded in 10 patients during baseline and post-therapy picture-naming sessions. Response times and the percentages of correct responses during naming tests were collected. Time-frequency analyses were conducted on intracranial signals, and comparisons were made between baseline and post-therapy conditions for each patient.
Results: Half of the patients demonstrated improved naming skills following the treatment. We observed significantly different recruitment of frontotemporal areas in the left hemisphere (including Broca's area) post-therapy in patients that improved naming skills. Specifically, we found significantly different high-gamma activity in the posterior left inferior frontal gyrus 500 ms after stimulus onset in patients with improved naming skills vs. non-improved naming skills. This effect was not observed in the right hemisphere.
Conclusions: These findings suggest that enhanced performance following language therapy is associated with modifications in posterior left IFG activations during latencies closely tied to the lexical selection process.
Patients with drug-resistant epilepsy may exhibit impairments in language production alongside their pathology. Individuals with temporal lobe epilepsy (TLE) localized in the dominant hemisphere for language are particularly susceptible to experiencing language difficulties during the interictal state. These patients often demonstrate an anomia profile characterized by relatively intact semantic processing but have difficulties in accessing lexical and phonological information (Trebuchon-Da Fonseca et al., 2009; Campo et al., 2013; Bartha-doering and Trinka, 2014; Miozzo and Hamberger, 2015). This deficit is occasionally accompanied by verbal memory deficits (Trebuchon-Da Fonseca et al., 2009; Campo et al., 2013). Factors such as the duration of epilepsy, seizure frequency, antiepileptic drug, history of temporal lobe surgeries, the presence of brain lesions, and potential interictal epileptiform discharges have been identified as significantly impacting naming ability (Dodrill and Ojemann, 2007; Trimmel et al., 2021; Caciagli et al., 2023). Surgical resections performed to control seizures increase these language deficits in a sizable number of cases (Ives-Deliperi and Butler, 2012). Connectome analyses have demonstrated that naming proficiency in TLE patients is linked to the subnetworks involved in semantic memory and lexical retrieval rather than being dependent solely on discrete brain regions (Munsell et al., 2019).
Because patients with cognitive impairments encounter difficulties in daily life, rehabilitation effectiveness is a significant concern. Mazur-Mosiewicz et al. conducted a systematic review of cognitive rehabilitation programs offered to patients experiencing cognitive disorders after surgery. Evidence from the literature suggests that post-surgical rehabilitation can be effective in some cognitive domains, such as memory (Joplin et al., 2018). However, rehabilitating language or word-finding difficulties in left temporal lobe epilepsy (LTLE) patients has been understudied, and several authors have emphasized the necessity for systematic evaluation in this population (Mazur-Mosiewicz et al., 2015; Sabadell et al., 2024).
The impact of language therapy on behavior and neural activity has been extensively explored in the vascular aphasic population. Most studies utilized functional magnetic resonance imaging (fMRI) measurements, focusing on patients with an anomic profile, closely related to language production deficits observed in our target population. These investigations revealed that the alterations in brain area recruitment post-therapy vary with therapy type (Kiran and Thompson, 2019). Brain area involvement is rationalized under the dual-stream model, encompassing the ventral stream [the inferior temporal sulcus [ITS], the middle temporal gyrus [MTG], and the superior temporal gyrus [STG]] and the dorsal stream [the inferior frontal gyrus [IFG], the anterior insula, and the premotor area; Del Gaizo et al., 2017]. Therapies employing phonological exercises, particularly phonological cueing, showed a link to bilateral activation of dorsal pathways (Nardo et al., 2017). Interventions focusing on phonological and semantic exercises were associated with left ventral activation of brain regions (Bonilha et al., 2016). The engagement of areas adjacent to the classical language network might relate to using additional cognitive functions, such as executive functions, to enhance language skills (Fridriksson et al., 2022).
The research utilizing electroencephalography (EEG) or Magnetoencephalography (MEG) is less abundant and yields diverse outcomes. A common theme in these studies is the correlation between therapy effectiveness and its intensity. The success of rehabilitation is gauged using various metrics, such as latency and amplitude changes in event related potentials (ERP)/Fs (N400, P300) and modifications in sleep slow waves. Multimodal therapies, which include, for instance, phonological and semantic exercises, have demonstrated varied results (Cornelissen et al., 2003; Breier et al., 2010; Wilson et al., 2012; Sarasso et al., 2014). There is a tendency to observe changes in signal modification in the left hemisphere post-therapy (Breier et al., 2010; Wilson et al., 2012), particularly in the frontal area (Sarasso et al., 2014).
Increasing evidence suggests that therapies may induce a reorganization in the left hemisphere activation. However, the link between rehabilitation type and plasticity remains unaddressed in the context of focal epilepsy. Recently, a group of experts proposed a new paradigm through which individual treatments can be systematically characterized in terms of targets, ingredients, and mechanisms of action (Fridriksson et al., 2022). Based on their recommendations, rehabilitation in epilepsy should target naming abilities by stimulating both phonological and semantic processes through a multimodal approach, employing repetitive and intensive training.
The reorganization of brain activity in the context of TLE could manifest as either a shift in language dominance from the left hemisphere to the right hemisphere or a relocation of language processing from temporal regions to frontal regions (Tzourio-Mazoyer et al., 2017). Furthermore, studies have shown that the reorganization of the neural language network away from the seizure onset zone correlates with improved language abilities post-surgery (Perrone-Bertolotti et al., 2012a). Frontal regions involved in the language network, in particular the posterior part of the IFG, are typically preserved in surgeries for drug-resistant epilepsy, and investigating whether there is any electrophysiological plasticity in this area following rehabilitation is relevant. Due to the inconsistent anatomical definition of Broca's area (Tremblay and Dick, 2016) and the heterogeneous functional involvement of this region in either the “language network” or the domain-general network (Fedorenko and Blank, 2020), we have chosen to define Broca's area in the present study as the posterior IFG, including the posterior part of the pars triangularis and the pars opercularis (Amunts et al., 2010).
This study aims to explore the effects of naming rehabilitation on epileptic patients exhibiting anomia. A novel feature of our approach is that the therapy and its appraisal were conducted during the presurgical invasive evaluation. Specifically, we assessed how three therapy sessions may influence naming performance and neural activity, recorded via intracranial stereo-electroencephalography (SEEG) in several regions involved in naming processing, such as the posterior IFG, the MTG, the STG, and the left basotemporal area. In our research, we opted to employ the same picture-naming task for both the behavioral and neural evaluations. We anticipated that in post-therapy sessions, patients' performance would improve alongside corresponding changes in brain activity compared to the baseline condition.
We included 10 drug-refractory epileptic patients (7 females) during their presurgical investigation. Patients underwent intracranial video SEEG recording following complete or partial withdrawal of antiepileptic drugs during a period that could range between 4 and 10 days to record the patient's seizures. The strategy for electrode positioning was established in each patient based on hypotheses concerning the localization of the epileptogenic zone (EZ) to define the subsequent cortectomy. The clinical procedure for localizing the EZ included the visual and quantitative analysis of electro-clinical correlations recorded in the video SEEG. The patients were included in the study because they presented cognitive complaints concerning word retrieval in daily life during neuropsychological assessment. The details of the clinical data are summarized in Table 1. All patients were native speakers of French. For the current study, at bedside, the patients were tested collaterally using the diagnostic procedures performed during presurgical investigations. All patients signed an informed consent form before participating. This study was approved by the institutional review board of the French Institute of Health (IRB00003888).
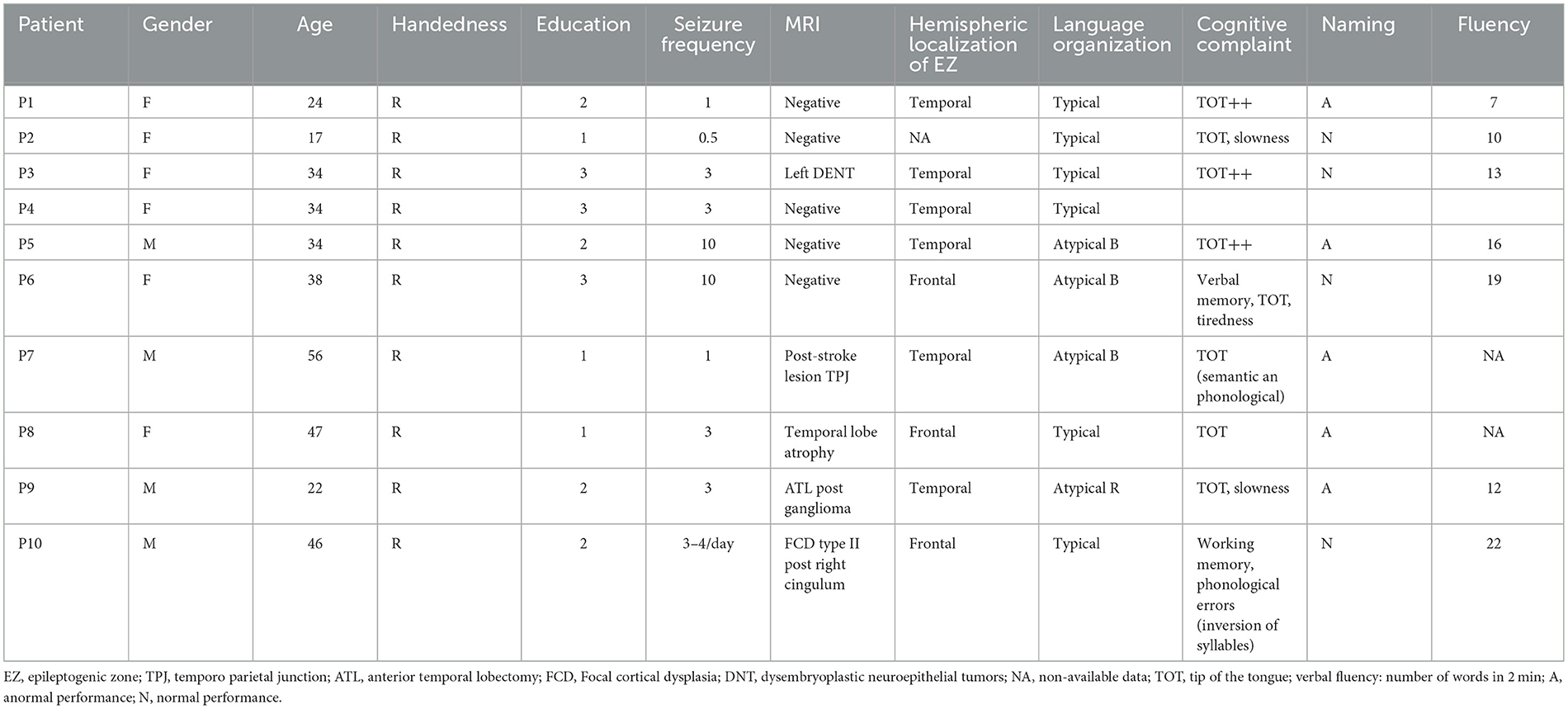
Table 1. Patients' demographic and clinical information.
The experimental design was shaped by the constraint of SEEG recording durations. Patients performed two (pre-therapy) picture-naming blocks included in the functional cartography. The therapy protocol then consisted of three sessions, one per day. After each training session, patients did one post-treatment picture-naming block (Figure 1). The total duration of the procedure was 4 days.
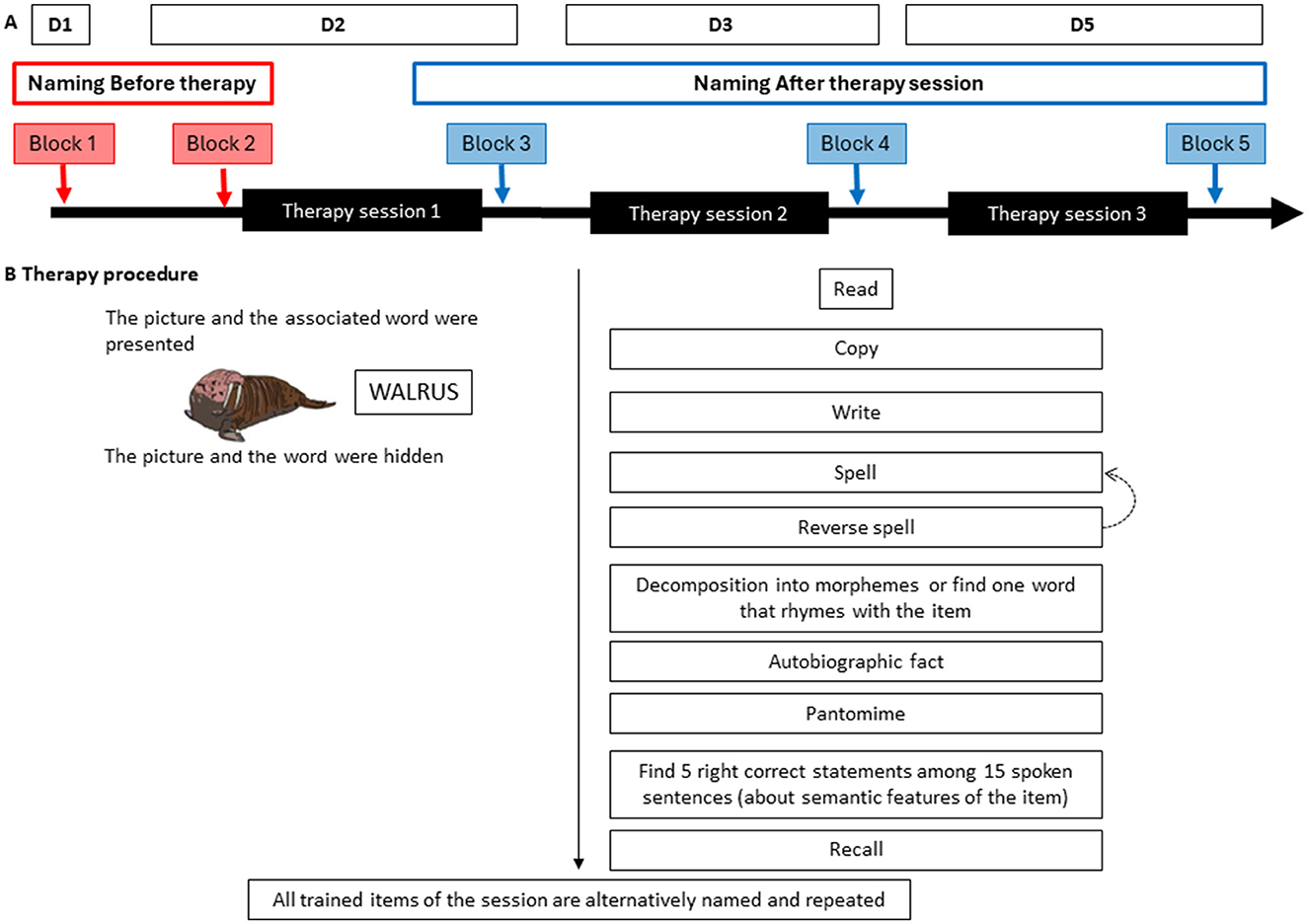
Figure 1. Experimental design and therapy procedure. (A) Experimental design: each picture-naming block is represented by an arrow, with red arrows indicating pre-therapy blocks and blue arrows the post-therapy blocks. Five naming blocks, each consisting of 100 trials, were completed over 4 days. The items in the five blocks were matched across several relevant parameters: visual complexity, the percentage of modal name usage, oral and written French lemma frequency, the number of phonemes, the number of phonological neighbors, the semantic categories, and the number of syllables. (B) Therapy procedure: the procedure was the same for each therapy session; it was divided into 10 steps. For each item, the written and spoken name was provided to the patient, who then performed different tasks: read, copy, delayed copy, spell, recall, reverse spell, analyze phonologically, recall a personal memory, answer semantic yes/no questions, gesture (if relevant), and recall. If a step was not successfully completed, the experimenter went back to the previous step (dotted arrow). Before the end of the session, the experimenter grouped all trained items and asked the patient to alternatively name and repeat them. Each therapy session lasted 45 min and was dedicated to items from a given semantic category (mammals, objects, or fruits and vegetables).
As encouraged by Fridriksson et al. (2022), we describe our language rehabilitation program according to the treatment specification system: target, active ingredients, and possible mechanisms of action of the treatment. The rehabilitation target was anomia. To select active ingredients, we drew on theoretical considerations from the fields of neuropsychology, cognitive neuroscience, and readaptation sciences. We reviewed the literature on anomia rehabilitation, primarily conducted with stroke patients but has also successfully applied in the context of other pathologies, such as primary progressive aphasia (Pagnoni et al., 2021) and, most recently, epilepsy (Sabadell et al., 2024). The ingredients were selected from a cognitive perspective while considering patients' frequent memory problems.
Finally, for the mechanisms of action, we largely adhered to Kiran and Thompson's (2019) hypothesis about brain plasticity driving language recovery after stroke. They identified general principles and factors to be incorporated into language rehabilitation. The first two principles encourage treating impaired—rather than preserved—language processes to promote underlying recovery mechanisms. The third principle highlights the need to reinforce patients' motivation and attention. Other principles call for repetition and intensity. Finally, task complexity is thought to promote learning and generalization. Given current cognitive accounts for word-finding difficulties in LTLE patients, combining semantic and phonological tasks seemed the most relevant approach for our purposes. During the procedure, items sharing semantic features were grouped to induce contextual priming (Kiran and Thompson, 2003; Boyle, 2017). In addition, the semantic complexity (operationalized in terms of atypicality in the category) was controlled to improve the generalization effects to other words (Kiran and Thompson, 2003; Gilmore et al., 2020). In a recent pilot study, we demonstrated the effectiveness of this rehabilitation program for trained items and observed encouraging results for untrained items (Sabadell et al., 2024).
The procedure was the same for each therapy session; it was divided into 10 steps (Figure 1B). For each item, the written and spoken name was provided to the patient, who then performed different tasks: read, copy, delayed copy, spell, recall, reverse spell, analyze phonologically, recall a personal memory, answer semantic yes/no questions, gesture (if relevant), and recall. If a step was not successfully completed, the experimenter went back to the previous step. Before the end of the session, the experimenter grouped all trained items and asked the patient to alternatively name and repeat them. Each therapy session lasted 45 min and was dedicated to 10 items from a given semantic category (mammals, objects, or fruits and vegetables).
We used colored pictures in a picture-naming task to quantify behavioral and neurophysiological modifications following language therapy. The pictures were selected from the MultiPic database (Duñabeitia et al., 2017). We excluded repeated words. We collected the words' features in the Lexique database (New et al., 2004). We created five lists, each comprising 100 items. These items were matched across blocks for several relevant parameters: visual complexity, percentage of modal name, oral and written French lemma frequency, number of phonemes, number of phonological neighbors, semantic categories, and number of syllables (van Casteren and Davis, 2007). The items to be trained in the therapy procedure were selected within the list of 500 words created for the naming tasks, with the inclusion criteria of being of low frequency (i.e., below an arbitrary threshold of 4 occurrences per million) and belonging to specific semantic categories.
We implemented the task on E-prime 2.0 (Psychology Software Tools, Pittsburgh, PA). Patients were tested bedside at least 2 h after a seizure, while they were comfortably seated in their hospital room. The pictures were presented on a laptop screen (size 12″ × 8″) placed on a table. The laptop was connected to the clinical SEEG/video-acquisition system Natus. The video recordings were not used in this research. One marker was written on the SEEG recording when the picture was presented. Each trial started with a fixation cross that was presented for 1,000 ms, followed by the experimental picture. The experimenter proceeded to the subsequent trial manually. The 100 trials composing each block were presented in a random order. Patients were instructed to name each picture aloud as soon as possible without time or accuracy constraints. Patients received no feedback during this naming task to ensure that any learning effect could be linked to the prehabilitation procedure. The audio responses were recorded for offline scoring.
Due to the diverse patient etiology and electrode localization, we chose a multiple-cases approach in which the data of each of the 10 patients were analyzed independently.
The responses to each trial of the picture naming task were analyzed offline using CheckVocal (Protopapas, 2007) to accurately measure the response time (RT; in ms) and assess the quality of the response. We considered a response correct if the patient provided the target word within a 12-s delay. The types of errors were classified as described in Supplementary Table 1. We excluded trained items from behavioral analyses (13 items across the 3 post-therapy blocks).
Pre-therapy and post-therapy performance were contrasted with a bootstrap procedure. We computed single-case bootstrap estimates of the confidence interval (CI) around the mean performance at baseline [blocks 1 and 2; algorithm used by DiCiccio and Efron (1996), implemented in the R package boot version 1.3-30], separately for RT and percentage of correct responses (%CR). The performance measure at each post-therapy block (blocks 3, 4, or 5) was then compared to this 95% CI and declared significantly different from baseline whenever it lay outside the CI. For the group analysis, the same procedure was used with the whole data set. The resampling procedures preserved the hierarchical (patient and session) structure of the data. In other words, the sampling with replacement was conducted within each Patient × Session cell of the design.
Intracerebral EEG signals were recorded using intracerebral multiple contact electrodes (10–15 contacts, length: 2 mm, diameter: 0.8 mm, 1.5 mm apart edge to edge) implanted according to Talairach's stereotactic method. Neurophysiological signals were recorded continuously using a 256-channel Natus system, sampling at 512 Hz, with a low-frequency filter setting of 0.1 Hz.
The signals were extracted from the Natus software and preprocessed in Brainstorm (Tadel et al., 2011). We excluded trials in which the behavioral response was classified as incorrect. In addition, epochs containing epileptic spikes were removed by visual inspection, as were contacts with flat and noisy recorded activity. The signals were epoched in two different ways. First, epochs were extracted from 1 s before to 2 s after the onset of each picture stimulus; these were used in “stimulus-locked” analysis. Second, epochs were extracted from 1 s before to 0.5 s after each verbal response onset; these were used in “response-locked” analysis.
We focus our analysis on high-gamma activity, which has been linked to cognitive processing (Lachaux et al., 2012). We processed the data using multi intracranial analysis (MIA) (Dubarry et al., 2022). Time-frequency power was computed on consecutive 10-Hz bands between 80 and 150 Hz using a 7-cycle Morlet wavelet transform on a bipolar montage of contacts. To compensate for the 1/f distribution of power across the spectrum, a baseline correction was applied to each trial at each 10-Hz band by computing a z-score relative to activity during the baseline from 600 to 50 ms before picture onset. Then, high-gamma activity was averaged across trials for each couple of contacts. Pairs of contacts of interest were selected if they recorded high-gamma activity during the naming task, while inactivated sites were excluded.
All patients underwent a structural preoperative magnetic resonance imaging (MRI) scan and an intraoperative computed tomography (CT) scan as part of the clinical routine. An expert neurologist labeled each pair of contacts according to the brain atlas by observing the fused CT–MRI images (Mai et al., 2008). Thanks to the 3DViewer extension from Gardel software, all contact sites of each patient can be visualized in a three-dimensional representation (Villalon et al., 2018).
Because, for verbal performance, the statistical analyses contrasted pre-therapy blocks 1 and 2, grouped, with post-therapy outcome blocks, we chose to average the high-gamma activity recorded in a couple of contacts of interest during blocks 1 and 2, that is, the baseline condition, and the high-gamma activity recorded in a couple of contacts during blocks 4 and 5, that is, the post-therapy condition. For each pair of adjacent contacts, we computed paired Student's t-tests at each time sample. Thus, we obtain a time course of t-values corresponding to moments when signals significantly differ between conditions with p < 0.001 (Figure 2).
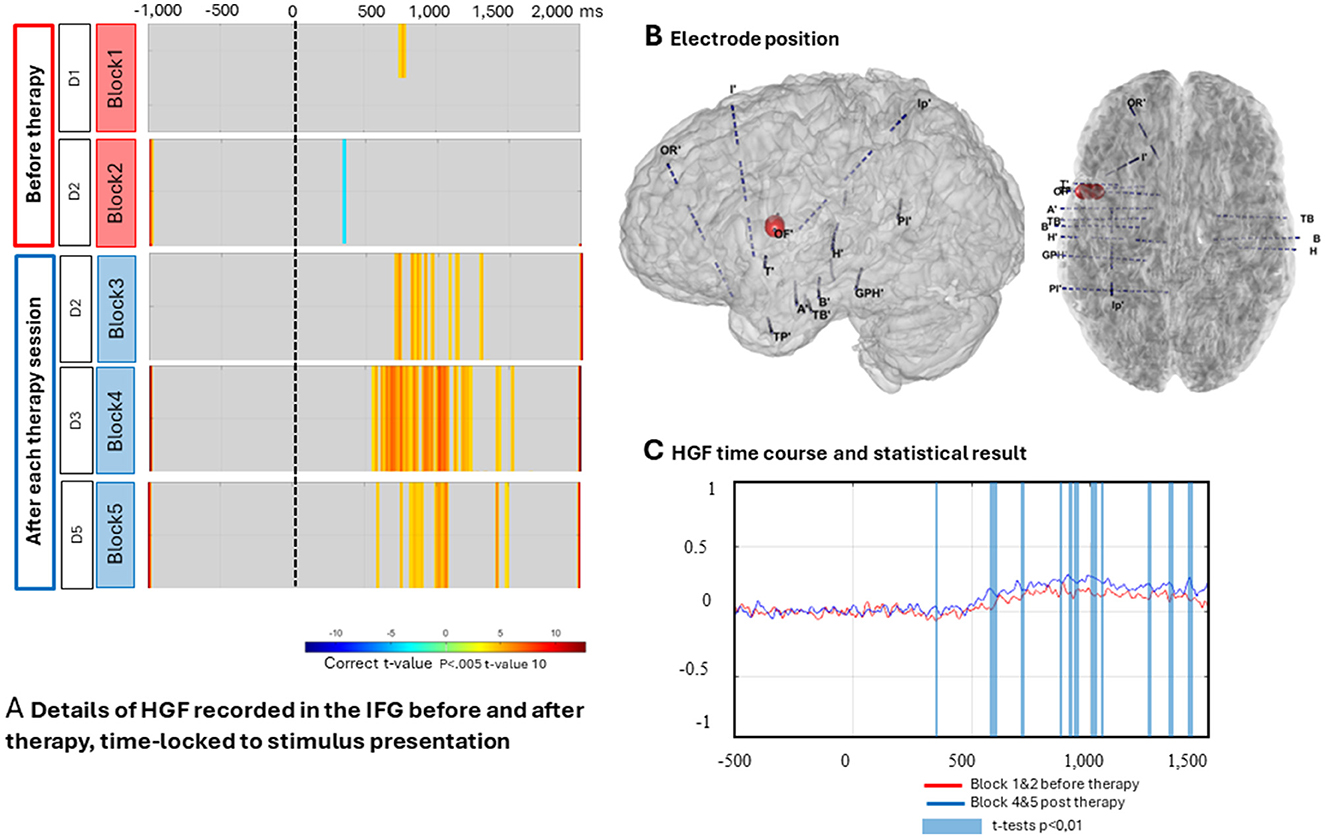
Figure 2. Representation of electrophysiological processing for one contact located in the left inferior frontal gyrus (IFG)/Broca's area of P1. (A) Details of high gamma frequency (HGF) recorded in the IFG before and after therapy, time-locked to stimulus presentation. Results of HGF analysis from P1 processed with the MIA pipeline (Dubarry et al., 2022). The colors represent the corrected t-values (bootstrap correction). We observed high-gamma activity recorded from one contact exploring the left IFG. Note that the high-gamma frequencies (orange) are sustained in blocks 3, 4, and 5 post-therapy. (B) In the three-dimensional view, all the electrodes are shown, and the red dot corresponds to the contact recorded in (A). (C) The time course of the HGF is extracted and summarized over time. Blocks 1 and 2 form the baseline condition, shown in red, while blocks 4 and 5 represent the post-therapy condition, shown in blue. The blue bar corresponds to the temporal window in which significant differences were observed.
Behavioral results before and after therapy are presented in Tables 2A, 2B. We observed a significant improvement in both speed (RT) and accuracy of naming (%CR) post-therapy in five patients (P1, P2, P3, P4, and P6), and an improvement in naming accuracy (%CR) alone in one patient (P5). These patients are classified as “good responders.” However, the pattern is not entirely consistent across all patients, particularly for the remaining four patients (P7–P10).
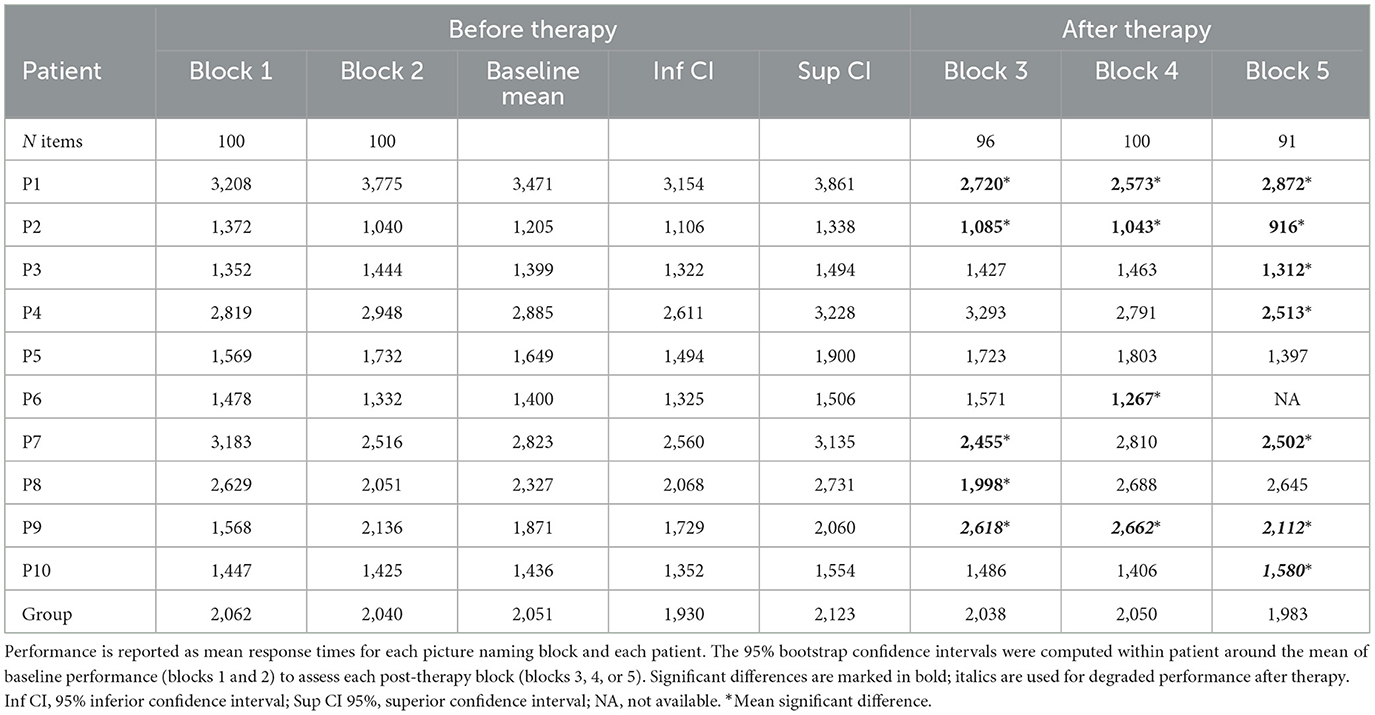
Table 2A. Behavioral results in the picture naming tests (responses times).
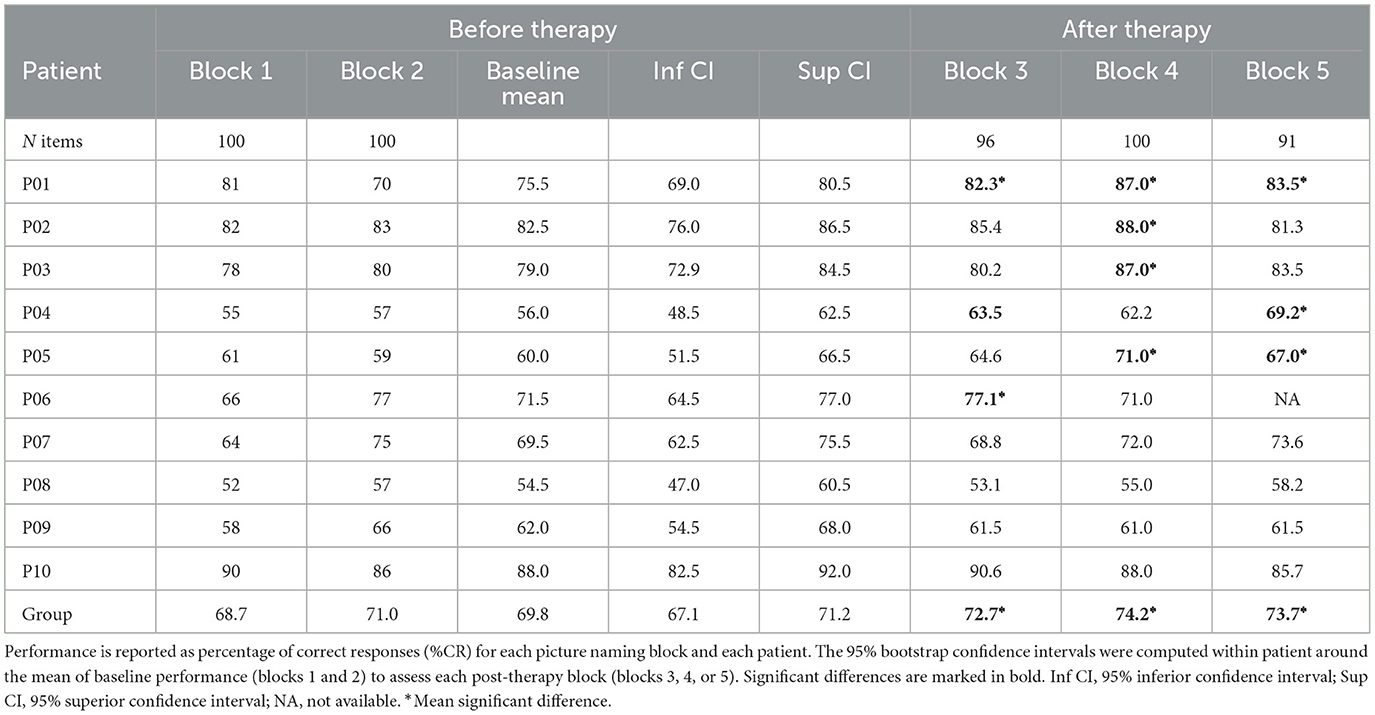
Table 2B. Behavioral results in the picture naming tests (% correct responses).
All patients exhibited similar language errors, particularly semantic paraphasia and omissions, as described in Supplementary Table 2.
In the group analysis, RTs in post-therapy sessions lay within the bootstrapped CI; in contrast, correct response rates lay outside this confidence interval. In other words, overall, the group was not faster post-therapy, but it was more accurate. This average increase in accuracy overlooks the large inter-patient variability we observed.
Figure 2 presents the detailed electrophysiological results for one patient (P1), while Figures 3, 4 summarize the electrophysiological results across all patients. Due to clinical constraints, not all patients underwent the same exploration, and because the temporal frontal areas were not investigated in P10, we decided to exclude this patient from the electrophysiological analyses. However, the left posterior IFG was sampled in all nine remaining patients.
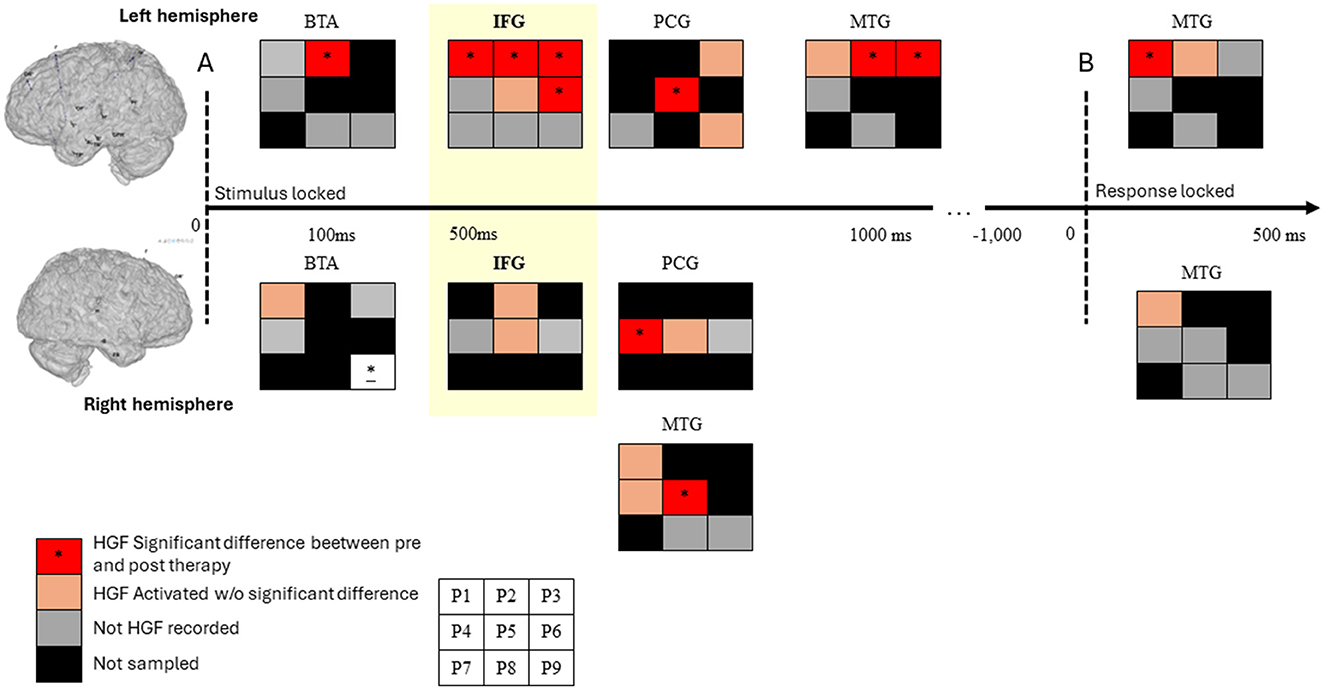
Figure 3. Summary and schematic representation of high-gamma changes in patients over time in the basal temporal area (BTA), the middle temporal gyrus (MTG), the inferior frontal gyrus (IFG), and the postcentral gyrus. Each square represents the outcome for one patient. Since not all patients have the same implantation sites or recorded HGF, we present the results as follows: black square = region not sampled in this patient; gray square = recorded region with no significant HGF compared to baseline; orange square = significant HGF recorded during the naming task; red square = significant HGF differences between pre- and post-therapy (as shown in Figure 2). (A) Results of the stimulus-locked analysis during the naming task are presented. The left and right hemispheres are represented at the top and bottom, respectively. We highlight our main result in the IFG in yellow. This region was sampled in all patients, and in five patients, we found HGF during the naming task. For four patients (P1, P2, P3, and P6), we observed significant differences between pre- and post-therapy. Note that for two of these patients, we recorded from the contralateral IFG and found no changes in HGF on the right side. On the left side, we also found HGF in the left BTA and later in the left MTG. Note that the significantly different activity in the right BTA of P9 is challenging to interpret because he presents an atypical hemispheric representation of language (with right specialization). (B) The results of the response-locked analysis are presented, focusing only on the MTG. All individual results are available in the Supplementary material.
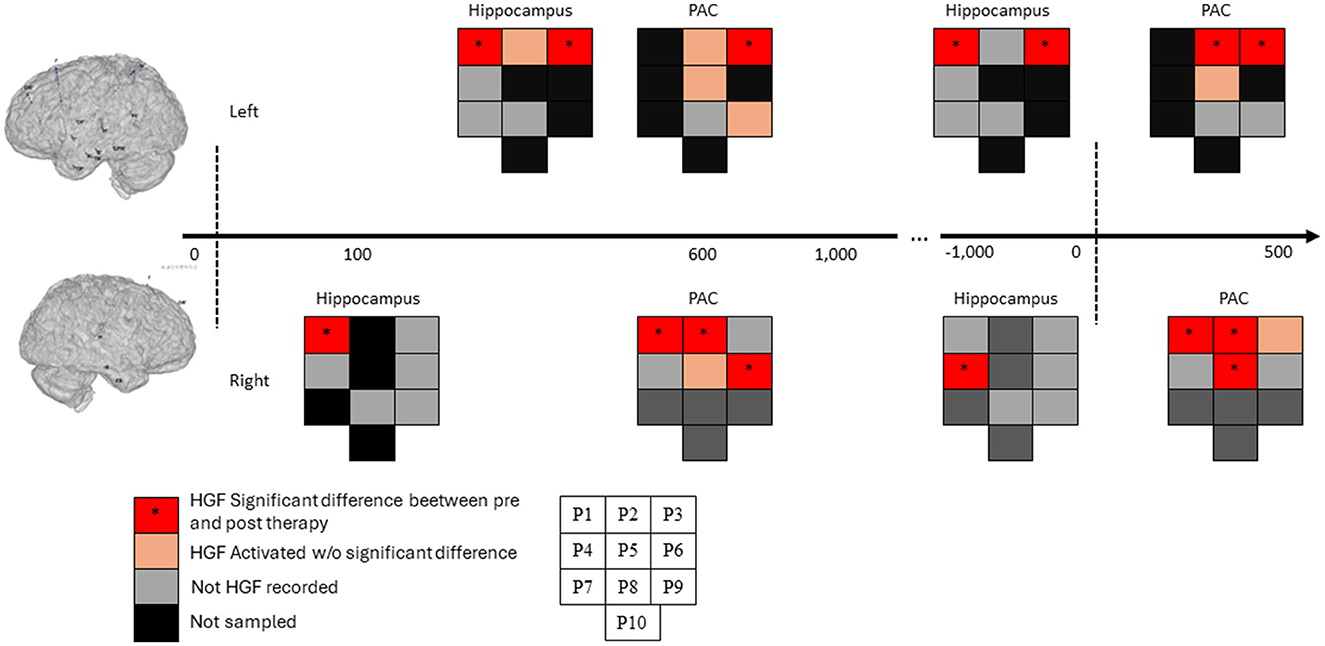
Figure 4. Summary and schematic representation of high-gamma changes in patients in the hippocampus and primary auditory cortex (PAC). Each square represents the outcome for one patient. Because the same implantation sites or recorded HGF were not the same for all patients, we present the results as follows: black square = region not sampled in this patient; gray square = recorded region with no significant HGF compared to baseline; orange square = significant HGF recorded during the naming task; red square = significant HGF differences between pre- and post-therapy. The PAC and the hippocampi in both hemispheres showed significantly different activations between pre- and post-therapy conditions in the stimulus locked activities and responses locked activities mainly in “good responders” patients (P1–P6). These results are less left-lateralized and can be explain by the improvement in response time.
We found significant differences in high-gamma activity (p ≤ 0.001) between baseline and post-therapy conditions for patients who showed improvements in both %CR and RTs during post-therapy blocks (P1, P2, P3, and P6) in the posterior left IFG between 400 and 1,000 ms. Additionally, no significant differences were found in patients with posterior right IFG exploration (P2 and P6). No such changes were observed in other patients, despite all being sampled in this region. The time course of high-gamma activity and the specific time points of significant differences are detailed for each area in the Supplementary material.
In addition, our analyses time-locked to stimulus presentation revealed three other brain areas in the left hemisphere (Figure 3) that were engaged during picture-naming tasks, showing significant differences between baseline and post-therapy conditions: the basal temporal area (BTA), the MTG, and the postcentral gyrus (PCG). Two additional areas, the primary auditory cortex (PAC) and the hippocampi in both hemispheres, also showed significantly different activations between conditions (Figure 4).
Time-locked to response onset, significant modifications in high-gamma activity were recorded in the left MTG (Figure 3) and the bilateral PAC and hippocampi (Figure 4).
Patients with drug-resistant epilepsy that disorganizes the language network are likely to display an anomia profile with verbal memory impairments between seizures; these deficits may increase after surgery (Bartha-doering and Trinka, 2014; Busch et al., 2016). Our study is the first to assess behavioral and neural changes induced by language therapy in this population. Furthermore, we assessed brain activity using SEEG recordings during the intracerebral presurgical evaluation. In four patients, we observed improvements in behavioral performance following therapy, which were associated with electrophysiological modifications in Broca's area (the left posterior IFG).
First, behavioral assessments show that all patients presented the same kind of language errors, especially semantic paraphasia and omissions, which have been previously reported (Trebuchon-Da Fonseca et al., 2009; Minkina et al., 2013; Bartha-doering and Trinka, 2014). Accuracy (%CR) is typically used in the literature to compare behavioral performance before and after therapy. We observed heterogeneous accuracy patterns across patients (Table 2). To provide a more comprehensive description of the behavioral patterns, we also assessed RTs. Notably, five patients demonstrated significantly faster post-therapy naming RTs and significantly improved accuracy. As depicted in Table 2, the improved %CR is not always combined with shorter RTs and vice versa. However, the increased %CR, along with shorter RTs, does not reflect the same behavioral strategy as the increased %CR along with longer RTs. We can assume that the behavioral compensatory mechanisms would be different. For these reasons, we believe adding RT measurements more systematically in further studies is important. The RT variable has been neglected for quite some time (Crerar, 2004; Conroy et al., 2009), despite its potential significance. Although considerable interest in analyzing naming speed in anomic patients exists, the rehabilitation effects on this aspect present several methodological challenges. The interindividual variability of the success of therapy has already been documented (Wisenburn and Mahoney, 2009).
Effects reported in the literature mainly focus on trained items. In our study, we excluded trained items from our data set; thus, we analyzed therapy effects on unexposed words. Additionally, considering the decrease in naming speed with practice (Levelt, 1999), whether the effects on untrained items result from the intervention or merely from task repetition remains unclear (Basso et al., 2013). In our study, we exclusively collected RT data for untrained items across five distinct blocks that had never been named previously, thereby eliminating the risk of retest effects. We can attribute the modifications of behavioral performance to a generalization effect to other categories. In the literature, the effect size of semantic therapy seems to be relatively small but larger than for other therapy types (Wisenburn and Mahoney, 2009). In general, most of the gains after language therapy are reported for exposed/trained words (Wisenburn and Mahoney, 2009). Generalization is the targeted effect of a therapy because it is a sign that training some items from some semantic categories has an extended impact on other categories. In our study, the behavioral performance we recorded demonstrated a generalization effect, meaning that they extended to untrained words, a result often difficult to measure consistently (Mayer et al., 2024). We hypothesize that this generalization effect occurred because post-therapy assessments were conducted immediately after the therapy. Generalization effects may have been facilitated by several ingredients of our therapy, including utilizing a semantic task, incorporating an orthographic model, the high frequency of repetitions within each session, and the frequency of sessions within the same week (Sze et al., 2021).
The weakness of the behavioral results, specifically the lack of significant group improvement in accuracy, can be explained by the experimental design of our study. Our study was focused on short-term effects through the administration of three sessions that lasted 45 min each (for a total of 135 min). These constraints were imposed by the clinical setting where the therapy took place. Indeed, patients included were involved in presurgical investigations for localizing the EZ; they were admitted for a 4- to 10-day period. It is possible that some patients needed more time for training to present positive effects, given that a better recovery is associated with 8.8 h of therapy per week for 11.2 weeks in treatment in poststroke aphasia (Bhogal et al., 2003). It also has been demonstrated that the intensity of the therapy is an essential component of its efficiency (Jacquemot et al., 2012; Kiran and Thompson, 2019). A higher dosage and a higher number of repetitions of items have been associated with the short-term effects of therapy (Sze et al., 2021).
In addition, the location of the EZ may be a factor linked to the benefit of this therapy. P1, P4, and P5 are patients with temporal lobe epilepsy; in contrast, a higher proportion of individuals have frontal lobe epilepsy who have more varied behavioral evolutions after therapy. Neural networks involved in language deficits and those that can be engaged in plasticity induced by the therapy are potentially different between these patients. Furthermore, the location of the EZ has been shown to be a factor involved in reorganizing language representation in the brain (Perrone-Bertolotti et al., 2012b; Baciu and Perrone-Bertolotti, 2015).
In contrast to other neuroimaging techniques, intracranial recordings give the opportunity to investigate brain activity with an optimal signal-to-noise ratio. The major inconvenience is the limited spatial sampling guided by clinical assumptions. Thus, SEEG allows us to make time-frequency analyses in high frequencies (high-gamma) known to be closely linked to cognitive processing (Lachaux et al., 2012). In parallel to behavioral changes, electrophysiological analyses show modifications of high-gamma activity elicited by the naming task in the posterior IFG (Broca's area) in the left hemisphere.
We found significant differences in high-gamma activity in the left posterior IFG/Broca's area before and after therapy only in the four patients who showed improvements in their naming skills. No significant differences were observed in patients where the right IFG was sampled and engaged during the task. These results suggest that the effectiveness of rehabilitation may be linked to changes in the recruitment of the left posterior IFG.
Neural changes following a language therapy reported in the case of post-stroke aphasia show two main kinds of neuroplasticity: the engagement of left perilesional areas and/or the recruitment of homologous controlateral regions. Some studies about patients with vascular aphasia have demonstrated that gains in naming ability following early intensive therapy are correlated with increased activation of the posterior left IFG/Broca's Area (Mattioli et al., 2014; Crosson et al., 2019). The main implication of the left hemisphere in language treatment effects is in line with EEG and MEG studies of neural plasticity induced by language therapy (Cornelissen et al., 2003; Meinzer et al., 2004; Wilson et al., 2012; MacGregor et al., 2014; Sarasso et al., 2014; Singh et al., 2018). Cornelissen et al. observed training-specific effects in the left inferior parietal cortex, close to the impaired areas, without changes in the right hemisphere after therapy (Cornelissen et al., 2003). Mohr and collaborators measured mismatch negativity (MMNm) changes after intensive language-action therapy. They found a therapy-related increase of MMNm amplitudes over the left language-dominant hemisphere ~200 ms after the words could first be recognized as meaningful words in contrast to pseudowords (Mohr et al., 2016). They proposed that the left frontotemporal topography of the pre–post MMNm change may reflect better functionality of lexical semantic networks, which may be the basis for the observed improvement of language processing. Singh et al. (2018) observed that ERPs' source analysis post-rehabilitation revealed that the ability to recruit left frontal areas within a 300- to 550-ms time window after stimulus onset contributed to correct responses (Singh et al., 2018).
In the context of brain tumors, functional reorganization appears to follow a hierarchical sequence, initially engaging peri- and intralesional areas and subsequently involving regions in the opposite hemisphere for compensation (Nieberlein et al., 2023). Interestingly, the region most frequently reported to exhibit plasticity, whether perilesional or contralateral, is Broca's area (Gunal et al., 2018; Nieberlein et al., 2023). Closer to the population studied here, a case study of a patient with temporal lobe epilepsy shows that phonological tasks activated the left IFG and the right MTG with impaired behavioral performances before surgery. After surgery, phonological tasks activated the left IFG and left temporal regions, with behavioral performance revealing average scores. The authors concluded that the right hemisphere is less efficient than the left for phonological processing (Perrone-Bertolotti et al., 2012b). However, we must be cautious with our asymmetric result of brain plasticity given the clinical implantation schemas; the left hemisphere is more sampled than the right in our patients (35 recorded sites in the left vs. 28 in the right hemisphere in all patients).
The left posterior IFG activity significantly increased ~500 ms after stimulus onset. According to various models, the left posterior IFG is involved at the end of lexical selection and the beginning of syllabification and preparing the articulation of the word in subjects without language impairments (Indefrey and Levelt, 2004; discussed by Laganaro, 2016; Munding et al., 2016). The temporal dynamics of processing stages might be different in patients who present language production deficits with an offset of stages linked to longer RTs. In addition to the left posterior IFG's role in linguistic features of word production, our results do not exclude a potential impact of neuroplasticity in this area on executive functions. It has been demonstrated that the left IFG, among other regions, is involved in inhibitory control over motor responses (Swick et al., 2008). In addition, a study on Parkinson's disease patients showed that linguistic and executive function processes interact in the left posterior IFG during word production tasks involving selection with cortical asymmetries between patients with left- vs. right-sided Parkinson's disease (Di Tella et al., 2018; MacPherson et al., 2019).
In addition to left IFG activity changes, we found early increased high-gamma activity in the left BTA, which has been previously linked to the lexical selection process (Llorens et al., 2016; Munding et al., 2016; Dubarry et al., 2017). Such activity modification in this area, along with better performance mainly measured in naming speed, may reflect better and faster lexical selection after the language therapy.
We recorded MTG activities at later latencies than those documented in the literature; it is usually recruited from 200 to 400 ms after picture onset, whereas in our data, its activity begins from 600 to 1,500 ms. The MTG is known to be part of the ventral stream and is engaged in combining information provided by different temporal areas. Thus, it has the potential to monitor the response through an internal loop (Hickok and Poeppel, 2007). Finally, the left PCG engagement was significantly different before and after therapy from 600 to 1,500 ms post-stimulus onset, suggesting a possible effect on motor preparation of the response induced by therapy protocol. Around 600 ms, this area may also be engaged in phonological processing (Cornelissen et al., 2003). Electrophysiological changes recorded in the hippocampi and the PAC are likely linked to the duration of RTs. It has been demonstrated that the latency of hippocampal high-gamma activity predicts naming latency (Hamamé et al., 2014); however, our data do not allow us to link activity modifications in this area to an effect of the therapy. Similarly, PAC activity is significantly different between conditions at latencies close to the RTs. It has been reported that the two STGs are involved in the external loop of self-monitoring (Indefrey and Levelt, 2004). These changes may be more related to the moment of word production than to the effect of rehabilitation.
We also find minor changes in the right hemisphere. The involvement of a widespread inter-hemispheric network after language therapy has been demonstrated in similar studies, depending on the language task performed by patients (Pulvermüller et al., 2005; Meinzer et al., 2008). Studies interested in investigating abnormal electrophysiological markers in aphasic patients have demonstrated shifts between the right and left hemispheres in a specific time window, suggesting an effect on a particular encoding process (Laganaro et al., 2008). In addition, the authors proposed that variability in right-hemisphere activations in different recovery stages indicates changes occurring between hemispheres during recovery. Also, right-hemisphere activation may be linked to the hemispheric complementarily properties and, more generally, the idea of a dynamic continuum involving both hemispheres in language production (and language processing; Lindell, 2006; Tzourio-Mazoyer et al., 2017).
This study is the first to investigate the neural modifications related to language therapy in epileptic patients using the SEEG exploration method. The small number of patients involved limits the strength of the conclusions that can be drawn from the study. Also, the inherent variability in etiology, EZ localization, lesions, and behavioral profiles across the participants warranted all the behavioral and electrophysiological data to be analyzed at the individual participant level. The explicit attempt to account for and detail the inherent variability across the patients (i.e., multiple-cases approach) is a clear strength of this study (Jacquemot et al., 2012).
More generally, the results of this study support the promotion of Enhanced Recovery After Surgery (ERAS) protocols. Several reviews report specific protocols proven to optimize the pre-, peri-, and postoperative care of patients undergoing surgery. ERAS protocols now exist for several neurosurgical procedures and populations (Greisman et al., 2022; Liu et al., 2022) but have not been established in the epilepsy surgery literature. The idea of prehabilitation to improve cognitive reserve can help patients cope with post-surgery cognitive decline (Mazur-Mosiewicz et al., 2015; Baxendale, 2020). To date, few data are available in this field. Two studies report the benefits of prehabilitation before surgery. One study showed improved memory performance supported by the right hemisphere, thus reducing the risk of the surgical procedure (Verentzioti et al., 2017). Another case study (n = 3) reported a rehabilitation of 20 proper names before surgery and showed that some progress on trained items post-surgery was preserved (Kendall et al., 2016). According to these authors, shifting critical functions for naming (i.e., from left temporal lobe neural networks) to language networks distributed in the left hemisphere is possible through multimodal training involving dimensions supported by other networks (e.g., semantic, phonological, orthographic, and articulatory dimensions).
Finally, the link between improved naming performance and brain activity changes provides an argument for using specific neuromodulation procedures in targeted regions to improve cognitive performance before surgery, particularly for low-grade gliomas (Barcia et al., 2012; Rivera-Rivera et al., 2017). This procedure has also been used in the context of epilepsy surgery. In the reported case, 6 days of stimulation were sufficient to induce the neuroplasticity needed to extend the surgical procedure (Serrano-Castro et al., 2020).
Boccuni et al. (2024) reported a case in which a patient underwent 20 days of non-invasive inhibitory repetitive Transcranial magnetic stimulation (rTMS) and Transcranial direct current stimulation (tDCS) stimulation over the language network, coupled with intensive cognitive training before brain tumor surgery (Boccuni et al., 2024). Prehabilitation increased the distance between the tumor and the eloquent language network. Furthermore, enhanced functional connectivity within the language circuit was observed. This positive result confirmed the feasibility of a larger trial (Boccuni et al., 2023).
The emerging evidence regarding prehabilitation is based primarily on isolated case studies. Although the target and type of stimulation have been well-documented, the type of procedure and the training target are rarely specified or are under-described. We hope that the results of the present study will help advance such preoperative care for patients undergoing surgery.
We must note that the limit of our investigation lies in the sampling of SEEG, which does not permit comprehensive coverage of the entire neocortical surface as is possible with awake surgery. We did not show a specific effect in all the regions described that are involved in naming with direct electrical stimulation (Rofes et al., 2024).
In conclusion, we found improved naming performance and brain activity changes in patients with drug-resistant epilepsy after short-term language therapy administrated during presurgical SEEG exploration. We observed a main neuroplasticity effect in the left IFG/Broca's area, which is not included in the possible resection of the anterior part of the left temporal lobe proposed to patients with temporal lobe epilepsy. This could imply that the network involved in the success of the therapy should be preserved after surgery. Given that 34% of patients show a decline in naming abilities after left temporal lobe resection, further studies including measurement of long-term language therapy effects should be interesting (Mazur-Mosiewicz et al., 2015; Sabadell et al., 2024).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Institutional Review Board of the French Institute of Health (IRB00003888, FWA00005831). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
AT: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization. AF: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. VS: Conceptualization, Methodology, Validation, Writing – review & editing. A-SD: Software, Writing – review & editing, Investigation, Methodology, Validation. RC: Data curation, Investigation, Resources, Writing – review & editing, Methodology. FB: Conceptualization, Formal analysis, Investigation, Methodology, Validation, Writing – review & editing. F-XA: Conceptualization, Formal analysis, Investigation, Methodology, Software, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work, carried out within the Labex BLRI (ANR-11-LABX-0036) and the Institut Convergence ILCB was supported by grants from France 2030 (ANR-16-CONV-0002) and the Excellence Initiative of Aix-Marseille University (A*MIDEX). AF was supported by a Ph. D. grant from the French Ministry of Research and Higher Education. The project leading to this publication has received funding from the French Government under the “France 2030” investment plan managed by the French National Research Agency (reference: ANR-16-CONV000X/ANR-17-EURE-0029) and from Excellence Initiative of AixMarseille University - A*MIDEX (AMX-19-IET-004).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/flang.2024.1434420/full#supplementary-material
Amunts, K., Lenzen, M., Friederici, A. D., Schleicher, A., Morosan, P., Palomero-Gallagher, N., et al. (2010). Broca's region : novel organizational principles and multiple receptor mapping. PLoS Biol. 8:e1000489. doi: 10.1371/journal.pbio.1000489
Baciu, M., and Perrone-Bertolotti, M. (2015). What do patients with epilepsy tell us about language dynamics? a review of fMRI studies. Rev. Neurosci. 26, 323–341. doi: 10.1515/revneuro-2014-0074
Barcia, J. A., Sanz, A., Balugo, P., Alonso-Lera, P., Brin, J. R., Yus, M., et al. (2012). High-frequency cortical subdural stimulation enhanced plasticity in surgery of a tumor in Broca's area. NeuroReport 23, 304–309. doi: 10.1097/WNR.0b013e3283513307
Bartha-doering, L., and Trinka, E. (2014). The interictal language profile in adult epilepsy. Epilepsia 55, 1512–1525. doi: 10.1111/epi.12743
Basso, G., Magon, S., Reggiani, F., Capasso, R., Monittola, G., Yang, F. J., et al. (2013). Distinguishable Neurofunctional Effects of Task Practice and Item Practice in Picture Naming: a BOLD fMRI Study in Healthy Subjects. Amsterdam: Elsevier.
Baxendale, S. (2020). Cognitive rehabilitation and prehabilitation in people with epilepsy. Epilepsy Behav. 106:107027. doi: 10.1016/j.yebeh.2020.107027
Bhogal, S. K., Teasell, R., and Speechley, M. (2003). Intensity of aphasia therapy, impact on recovery. Stroke 34, 987–992. doi: 10.1161/01.STR.0000062343.64383.D0
Boccuni, L., Abellaneda-Pérez, K., Martín-Fernández, J., Leno-Colorado, D., Roca-Ventura, A., Bisbe, A. P., et al. (2023). Neuromodulation-induced prehabilitation to leverage neuroplasticity before brain tumor surgery: a single-cohort feasibility trial protocol. Front. Neurol. 14:1243857. doi: 10.3389/fneur.2023.1243857
Boccuni, L., Roca-Ventura, A., Buloz-Osorio, E., Leno-Colorado, D., Martín-Fernández, J., Cabello-Toscano, M., et al. (2024). Exploring the neural basis of non-invasive prehabilitation in brain tumour patients: an fMRI-based case report of language network plasticity. Front. Oncol. 14:1390542. doi: 10.3389/fonc.2024.1390542
Bonilha, L., Gleichgerrcht, E., Nesland, T., Rorden, C., and Fridriksson, J. (2016). Success of anomia treatment in aphasia is associated with preserved architecture of global and left temporal lobe structural networks. Neurorehabil. Neural Repair 30, 266–279. doi: 10.1177/1545968315593808
Boyle, M. (2017). Semantic treatments for word and sentence production deficits in Semantic treatments for word and sentence production deficits in aphasia. Semin. Speech Lang. 38, 52–61. doi: 10.1055/s-0036-1597256
Breier, J. I., Randle, S., Maher, L. M., and Papanicolaou, A. C. (2010). Changes in maps of language activity activation following melodic intonation therapy using magnetoencephalography: two case studies. J. Clin. Exp. Neuropsychol. 32, 309–314. doi: 10.1080/13803390903029293
Busch, R. M., Floden, D. P., Prayson, B., Chapin, J. S., Kim, K. H., Ferguson, L., et al. (2016). Estimating risk of word-finding problems in adults undergoing epilepsy surgery. Neurology 87, 2363–2369. doi: 10.1212/WNL.0000000000003378
Caciagli, L., Paquola, C., He, X., Vollmar, C., Centeno, M., Wandschneider, B., et al. (2023). Disorganization of language and working memory systems in frontal versus temporal lobe epilepsy. Brain 146, 935–953. doi: 10.1093/brain/awac150
Campo, P., Poch, C., Toledano, R., Igoa, J. M., Belinchón, M., García-Morales, I., et al. (2013). Anterobasal temporal lobe lesions alter recurrent functional connectivity within the ventral pathway during naming. J. Neurosci. 33, 12679–12688. doi: 10.1523/JNEUROSCI.0645-13.2013
Conroy, P., Sage, K., and Lambon Ralph, M. A. (2009). The effects of decreasing and increasing cue therapy on improving naming speed and accuracy for verbs and nouns in aphasia. Aphasiology 23, 707–730. doi: 10.1080/02687030802165574
Cornelissen, K., Laine, M., Tarkiainen, A., Järvensivu, T., Martin, N., and Salmelin, R. (2003). Adult brain plasticity elicited by anomia treatment. J. Cogn. Neurosci. 15, 444–461. doi: 10.1162/089892903321593153
Crerar, M. A. (2004). Aphasia rehabilitation and the strange neglect of speed. Neuropsychol. Rehabil. 14, 173–206. doi: 10.1080/09602010343000174
Crosson, B., Rodriguez, A. D., Copland, D., Fridriksson, J., Krishnamurthy, L. C., Meinzer, M., et al. (2019). Neuroplasticity and aphasia treatments: new approaches for an old problem. J. Neurol. Neurosurg. Psychiat. 90, 1147–1155. doi: 10.1136/jnnp-2018-319649
Del Gaizo, J., Fridriksson, J., Yourganov, G., Hillis, A. E., Hickok, G., Misic, B., et al. (2017). Mapping language networks using the structural and dynamic brain connectomes. eNeuro 4:ENEURO.0204-17.2017. doi: 10.1523/ENEURO.0204-17.2017
Di Tella, S., Baglio, F., Cabinio, M., Nemni, R., Traficante, D., and Silveri, M. C. (2018). Selection processing in noun and verb production in left- and right-sided Parkinson's disease patients. Front. Psychol. 9, 1–13. doi: 10.3389/fpsyg.2018.01241
DiCiccio, T., and Efron, B. (1996). Bootstrap confidence intervals. Statist. Sci. 11, 189–228. doi: 10.1214/ss/1032280214
Dodrill, C. B., and Ojemann, G. A. (2007). Do recent seizures and recent changes in antiepileptic drugs impact performances on neuropsychological tests in subtle ways that might easily be missed? Epilepsia 48, 1833–1841. doi: 10.1111/j.1528-1167.2007.01140.x
Dubarry, A.-S., Liégeois-Chauvel, C., Trébuchon, A., Bénar, C., and Alario, F.-X. (2022). An open-source toolbox for Multi-patient Intracranial EEG Analysis (MIA). NeuroImage 257:119251. doi: 10.1016/j.neuroimage.2022.119251
Dubarry, A.-S., Llorens, A., Trébuchon, A., Carron, R., Liégeois-Chauvel, C., Bénar, C.-G., et al. (2017). Estimating parallel processing in a language task using single-trial intracerebral electroencephalography to cite this version : HAL Id : hal-01495041. Psychol. Sci. 28, 1–13. doi: 10.1177/0956797616681296
Duñabeitia, J. A., Crepaldi, D., Meyer, A. S., New, B., Pliatsikas, C., Smolka, E., et al. (2017). MultiPic: a standardized set of 750 drawings with norms for six European languages. Quart. J. Exp. Psychol. 71, 808–816. doi: 10.1080/17470218.2017.1310261
Fedorenko, E., and Blank, I. A. (2020). Broca's area is not a natural kind. Trends Cogn. Sci. 24, 270–284. doi: 10.1016/j.tics.2020.01.001
Fridriksson, J., Basilakos, A., Boyle, M., Cherney, L. R., DeDe, G., Gordon, J. K., et al. (2022). Demystifying the complexity of aphasia treatment: application of the rehabilitation treatment specification systemx. Archiv. Phys. Med. Rehabil. 103, 574–580. doi: 10.1016/j.apmr.2021.08.025
Gilmore, N., Meier, E. L., Johnson, J. P., and Kiran, S. (2020). Typicality-based semantic treatment for anomia results in multiple levels of generalisation. Neuropsychol. Rehabil. 30, 802–828. doi: 10.1080/09602011.2018.1499533
Greisman, J. D., Olmsted, Z. T., Crorkin, P. J., Dallimore, C. A., Zhigin, V., Shlifer, A., et al. (2022). Enhanced Recovery After Surgery (ERAS) for cranial tumor resection: a review. World Neurosurg. 163, 104–122.e2. doi: 10.1016/j.wneu.2022.03.118
Gunal, V., Savardekar, A. R., Devi, B. I., and Bharath, R. D. (2018). Preoperative functional magnetic resonance imaging in patients undergoing surgery for tumors around left (dominant) inferior frontal gyrus region. Surg. Neurol. Int. Sci. Schol. 9:126. doi: 10.4103/sni.sni_414_17
Hamamé, C. M., Alario, F.-X., Llorens, A., Liégeois-Chauvel, C., and Trébuchon-Da Fonseca, A. (2014). High frequency gamma activity in the left hippocampus predicts visual object naming performance. Brain Lang. 135, 104–114. doi: 10.1016/j.bandl.2014.05.007
Hickok, G., and Poeppel, D. (2007). The cortical organization of speech processing. Nat. Rev. Neurosci. 2007:nrn2113. doi: 10.1038/nrn2113
Indefrey and Levelt W. J. M. (2004). The spatial and temporal signatures of word production components. Cognition 92, 101–144. doi: 10.1016/j.cognition.2002.06.001
Ives-Deliperi, V. L., and Butler, J. T. (2012). Naming outcomes of anterior temporal lobectomy in epilepsy patients: a systematic review of the literature. Epilepsy Behav. 24, 194–198. doi: 10.1016/j.yebeh.2012.04.115
Jacquemot, C., Dupoux, E., and Robotham, L. (2012). Specificity in rehabilitation of word production : a meta-analysis and a case study. Behav. Neurol. 25, 73–101. doi: 10.1155/2012/418920
Joplin, S., Stewart, E., Gascoigne, M., and Lah, S. (2018). Memory rehabilitation in patients with epilepsy: a systematic review. Neuropsychol. Rev. 7, 88–110. doi: 10.1007/s11065-018-9367-7
Kendall, D. L., Minkina, I., Bislick, L., Grabowski, T. J., Phatak, V., Silkes, J. P., et al. (2016). Language treatment prior to anterior temporal lobe surgery: can naming skills be preserved? J. Rehabilit. Res. Dev. Rehabilit. Res. Dev. Serv. 53, 813–826. doi: 10.1682/JRRD.2014.12.0310
Kiran, S., and Thompson, C. K. (2003). The role of semantic complexity in treatment of naming deficits: training semantic categories in fluent aphasia by controlling exemplar typicality. J. Speech Lang. Hear. Res. 46:773. doi: 10.1044/1092-4388(2003/061)
Kiran, S., and Thompson, C. K. (2019). Neuroplasticity of language networks in aphasia: advances, updates, and future challenges. Front. Neurol. 2019:295. doi: 10.3389/fneur.2019.00295
Lachaux, J.-P., Axmacher, N., Mormann, F., Halgren, E., and Crone, N. E. (2012). High-frequency neural activity and human cognition: past, present and possible future of intracranial EEG research. Progr. Neurobiol. 98, 279–301. doi: 10.1016/j.pneurobio.2012.06.008
Laganaro, M. (2016). Dynamics of word production and processing speed. Lang. Cogn. Neurosci. 31, 463–464. doi: 10.1080/23273798.2015.1096402
Laganaro, M., Morand, S., Schwitter, V., Zimmermann, C., and Schnider, A. (2008). Normalisation and increase of abnormal ERP patterns accompany recovery from aphasia in the post-acute stage. Neuropsychologia 46, 2265–2273. doi: 10.1016/j.neuropsychologia.2008.02.013
Levelt, W. J. M. (1999). Models of word production. Trends Cogn. Sci. 3, 223–232. doi: 10.1016/S1364-6613(99)01319-4
Lindell, A. K. (2006). In your right mind: right hemisphere contributions to language processing and production. Neuropsychol. Rev. 16, 131–148. doi: 10.1007/s11065-006-9011-9
Liu, B., Liu, S., Zheng, T., Lu, D., Chen, L., Ma, T., et al. (2022). Neurosurgical enhanced recovery after surgery ERAS for geriatric patients undergoing elective craniotomy: a review. Medicine 101:E30043. doi: 10.1097/MD.0000000000030043
Llorens, A., Dubarry, A.-S., Trébuchon, A., Chauvel, P., Alario, F.-X., and Liégeois-Chauvel, C. (2016). Contextual modulation of hippocampal activity during picture naming. Brain Lang. 159, 92–101. doi: 10.1016/j.bandl.2016.05.011
MacGregor, L. J., Difrancesco, S., Pulvermüller, F., Shtyrov, Y., and Mohr, B. (2014). Ultra-rapid access to words in chronic aphasia: the effects of intensive language action therapy (ILAT). Brain Topogr. 28, 279–291. doi: 10.1007/s10548-014-0398-y
MacPherson, S. E., Gillebert, C. R., Robinson, G. A., and Vallesi, A. (2019). Editorial: intra- and inter-individual variability of executive functions: determinant and modulating factors in healthy and pathological conditions. Front. Psychol. 10, 1–7. doi: 10.3389/fpsyg.2019.00432
Mai, J. K., Paxinos, G., and Voss, T. (2008). Atlas of the Human Brain. Amsterdam: Academic Press; Elsevier.
Mattioli, F., Ambrosi, C., Mascaro, L., Scarpazza, C., Pasquali, P., Frugoni, M., et al. (2014). Early aphasia rehabilitation is associated with functional reactivation of the left inferior frontal gyrus a pilot study. Stroke 45, 545–552. doi: 10.1161/STROKEAHA.113.003192
Mayer, J. F., Madden, E. B., Mozeiko, J., Murray, L. L., Patterson, J. P., Purdy, M., et al. (2024). Generalization in aphasia treatment: a tutorial for speech-language pathologists. Am. J. Speech-Lang. Pathol. 33, 57–73. doi: 10.1044/2023_AJSLP-23-00192
Mazur-Mosiewicz, A., Carlson, H. L., Hartwick, C., Dykeman, J., Lenders, T., Brooks, B. L., et al. (2015). Effectiveness of cognitive rehabilitation following epilepsy surgery: current state of knowledge. Epilepsia 56, 735–744. doi: 10.1111/epi.12963
Meinzer, M., Elbert, T., Wienbruch, C., Djundja, D., Barthel, G., and Rockstroh, B. (2004). Intensive language training enhances brain plasticity in chronic aphasia. BMC Biol. 2, 1–9. doi: 10.1186/1741-7007-2-20
Meinzer, M., Flaisch, T., Breitenstein, C., Wienbruch, C., Elbert, T., and Rockstroh, B. (2008). Functional re-recruitment of dysfunctional brain areas predicts language recovery in chronic aphasia. NeuroImage 39, 2038–2046. doi: 10.1016/j.neuroimage.2007.10.008
Minkina, I., Ojemann, J. G., Grabowski, T. J., Silkes, J. P., Phatak, V., and Kendall, D. L. (2013). Treatment of proper name retrieval deficits in an individual with temporal lobe epilepsy. Am. J. Speech-Lang. Pathol. 22, 250–256. doi: 10.1044/1058-0360(2012/12-0048)
Miozzo, M., and Hamberger, M. J. (2015). Preserved meaning in the context of impaired naming in temporal lobe epilepsy. Neuropsychology 29, 274–281. doi: 10.1037/neu0000097
Mohr, B., MacGregor, L. J., Difrancesco, S., Harrington, K., Pulvermüller, F., and Shtyrov, Y. (2016). Hemispheric contributions to language reorganisation: an MEG study of neuroplasticity in chronic post stroke aphasia. Neuropsychologia 93, 413–424. doi: 10.1016/j.neuropsychologia.2016.04.006
Munding, D., Dubarry, A. S., and Alario, F. X. (2016). On the cortical dynamics of word production: a review of the MEG evidence. Lang. Cogn. Neurosci. 31, 441–462. doi: 10.1080/23273798.2015.1071857
Munsell, B. C., Wu, G., Fridriksson, J., Thayer, K., Mofrad, N., Desisto, N., et al. (2019). Relationship between neuronal network architecture and naming performance in temporal lobe epilepsy: a connectome based approach using machine learning. Brain Lang. 193, 45–57. doi: 10.1016/j.bandl.2017.08.006
Nardo, D., Holland, R., Leff, A. P., Price, C. J., and Crinion, J. T. (2017). Less is more: neural mechanisms underlying anomia treatment in chronic aphasic patients. Brain 140, 3039–3054. doi: 10.1093/brain/awx234
New, B., Pallier, C., Brysbaert, M., and Ferrand, L. (2004). Lexique 2: a new French lexical database. Beha. Res. Methods Instr. Comput. 36, 516–524. doi: 10.3758/BF03195598
Nieberlein, L., Rampp, S., Gussew, A., Prell, J., and Hartwigsen, G. (2023). Reorganization and plasticity of the language network in patients with cerebral gliomas. NeuroImage 37:103326. doi: 10.1016/j.nicl.2023.103326
Pagnoni, I., Gobbi, E., Premi, E., Borroni, B., Binetti, G., Cotelli, M., et al. (2021). Language training for oral and written naming impairment in primary progressive aphasia: a review. Transl. Neurodegener. 10, 1–34. doi: 10.1186/s40035-021-00248-z
Perrone-Bertolotti, M., Yvert, G., Baciu, M., and David, O. (2012a). Dynamic causal modeling of spatiotemporal integration of phonological and semantic processes : an electroencephalographic study dynamic causal modeling indicated this increase of activation of the anterior temporal lobe in the semantic condition as a cons. J. Neurosci. 32, 4297–4306. doi: 10.1523/JNEUROSCI.6434-11.2012
Perrone-Bertolotti, M., Zoubrinetzky, R., Yvert, G., Bas, J. F. L., and Baciu, M. (2012b). Functional MRI and neuropsychological evidence for language plasticity before and after surgery in one patient with left temporal lobe epilepsy. Epilepsy Behav. 23, 81–86. doi: 10.1016/j.yebeh.2011.11.011
Protopapas, A. (2007). CheckVocal: a program to facilitate checking the accuracy and response time of vocal responses from DMDX. Behav. Res. Methods 39, 859–862. doi: 10.3758/BF03192979
Pulvermüller, F., Hauk, O., Zohsel, K., Neininger, B., and Mohr, B. (2005). Therapy-related reorganization of language in both hemispheres of patients with chronic aphasia. NeuroImage 28, 481–489. doi: 10.1016/j.neuroimage.2005.06.038
Rivera-Rivera, P. A., Rios-Lago, M., Sanchez-Casarrubios, S., Salazar, O., Yus, M., González-Hidalgo, M., et al. (2017). Cortical plasticity catalyzed by prehabilitation enables extensive resection of brain tumors in eloquent areas. J. Neurosurg. Am. Assoc. Neurol. Surg. 126, 1323–1333. doi: 10.3171/2016.2.JNS152485
Rofes, A., D'Agata, F., Guerrini, F., and Spena, G. (2024). Speech and lexico-semantic errors during direct cortical stimulation mapping of the language-dominant hemisphere: effects of object and action naming. J. Neurosurg. Am. Assoc. Neurol. Surg. 140, 1641–1659. doi: 10.3171/2023.10.JNS231493
Sabadell, V., Trébuchon, A., and Alario, F. X. (2024). An exploration of anomia rehabilitation in drug-resistant temporal lobe epilepsy. Epilepsy Behav. Rep. 27:100681. doi: 10.1016/j.ebr.2024.100681
Sarasso, S., Määttä, S., Ferrarelli, F., Poryazova, R., Tononi, G., and Small, S. L. (2014). Plastic changes following imitation-based speech and language therapy for aphasia: a high-density sleep EEG study. Neurorehabil. Neural Repair 28, 129–138. doi: 10.1177/1545968313498651
Serrano-Castro, :J, Ros-López, B., Fernández-Sánchez, V. E., García-Casares, N., Muñoz-Becerra, L., Cabezudo-Garcia, P., et al. (2020). Neuroplasticity and epilepsy surgery in brain eloquent areas: case report. Front. Neurol. 11:549172. doi: 10.3389/fneur.2020.00698
Singh, T., Phillip, L., Behroozmand, R., Gleichgerrcht, E., Piai, V., Fridriksson, J., et al. (2018). Pre-articulatory electrical activity associated with correct naming in individuals with aphasia. Brain Lang. 177–178, 1–6. doi: 10.1016/j.bandl.2018.01.002
Swick, D., Ashley, V., and Turken, A. U. (2008). Left inferior frontal gyrus is critical for response inhibition. BMC Neurosci. 9, 1–11. doi: 10.1186/1471-2202-9-102
Sze, W. P., Hamaeu, S., Warren, J., and Best, W. (2021). Identifying the components of a successful spoken naming therapy: a meta-analysis of word-finding interventions for adults with aphasia. Aphasiology 35, 33–72. doi: 10.1080/02687038.2020.1781419
Tadel, F., Baillet, S., Mosher, J. C., Pantazis, D., and Leahy, R. M. (2011). Brainstorm: a user-friendly application for MEG/EEG analysis. Comput. Intell. Neurosci. 2011:879716. doi: 10.1155/2011/879716
Trebuchon-Da Fonseca, A., Guedj, E., Alario, F. X., Laguitton, V., Mundler, O., Chauvel, P., et al. (2009). Brain regions underlying word finding difficulties in temporal lobe epilepsy. Brain 132, 2772–2784. doi: 10.1093/brain/awp083
Tremblay and Dick A. S. (2016). Broca and Wernicke are dead, or moving past the classic model of language neurobiology. Brain Lang. 162, 60–71. doi: 10.1016/j.bandl.2016.08.004
Trimmel, K., Caciagli, L., Xiao, F., van Graan, L. A., Koepp, M. J., Thompson, P. J., et al. (2021). Impaired naming performance in temporal lobe epilepsy: language fMRI responses are modulated by disease characteristics. J. Neurol. 268, 147–160. doi: 10.1007/s00415-020-10116-x
Tzourio-Mazoyer, N., Perrone-Bertolotti, M., Jobard, G., Mazoyer, B., and Baciu, M. (2017). Multi-factorial modulation of hemispheric specialization and plasticity for language in healthy and pathological conditions: a review. Cortex 86, 314–339. doi: 10.1016/j.cortex.2016.05.013
van Casteren, M., and Davis, M. (2007). Match: a program to assist in matching the conditions of factorial experiments. Behav. Res. Methods 39, 973–978. doi: 10.3758/BF03192992
Verentzioti, A., Patrikelis, P., Lucci, G., Alexoudi, A., Kosmidis, M., Siatouni, A., et al. (2017). Can neuro-optimization determine the candidacy for epilepsy surgery? J. Neurol. 8:446. doi: 10.4172/2155-9562.1000446
Villalon, S. M., Paz, R., Roehri, N., Lagarde, S., Pizzo, F., Colombet, B., et al. (2018). EpiTools, A software suite for presurgical brain mapping in epilepsy: intracerebral EEG. J. Neurosci. Methods 303, 7–15. doi: 10.1016/j.jneumeth.2018.03.018
Wilson, K. R., O'Rourke, H., Wozniak, L. A., Kostopoulos, E., Marchand, Y., and Newman, A. J. (2012). Changes in N400 topography following intensive speech language therapy for individuals with aphasia. Brain Lang. 123, 94–103. doi: 10.1016/j.bandl.2012.06.005
Keywords: anomia profile, intracranial EEG, rehabilitation, epilepsy, inferior frontal gyrus (IFG)
Citation: Trébuchon A, Fasola A, Sabadell V, Dubarry A-S, Carron R, Bartolomei F and Alario F-X (2025) Exploring post-rehabilitation plasticity with intra-cerebral recordings on anomic profiles. Front. Lang. Sci. 3:1434420. doi: 10.3389/flang.2024.1434420
Received: 17 May 2024; Accepted: 13 November 2024;
Published: 06 January 2025.
Edited by:
Maria V. Ivanova, University of California, Berkeley, United StatesReviewed by:
Adrià Rofes, University of Groningen, NetherlandsCopyright © 2025 Trébuchon, Fasola, Sabadell, Dubarry, Carron, Bartolomei and Alario. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Agnès Trébuchon, YWduZXMudHJlYnVjaG9uQHVuaXYtYW11LmZy
†ORCID: Véronique Sabadell orcid.org/0000-0002-6707-3023
Romain Carron orcid.org/0000-0002-4723-7406
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.