 Nina Bauer
Nina Bauer Claudia Löffler3†
Claudia Löffler3†- 1Department of Internal and Integrative Medicine, Sozialstiftung Bamberg, Bamberg, Germany
- 2Department of Integrative Medicine, Medical Faculty, University of Duisburg-Essen, Bamberg, Germany
- 3Department of Internal Medicine II, University Hospital of Würzburg, Würzburg, Germany
- 4Institute of Clinical Epidemiology and Biometry, Julius Maximilians University of Würzburg, Würzburg, Germany
- 5State Institute of Health, Bavarian Health and Food Safety Authority, Erlangen, Germany
- 6Institute of Social Medicine, Epidemiology and Health Economics, Charité – Universitätsmedizin Berlin, Berlin, Germany
Introduction: Mind-body medicine (MBM) focuses on stress reduction and lifestyle changes. The primary objective of this pilot trial was to test study feasibility of a complex integrative MBM program for patients with Crohn's disease (CD), especially in rural regions, and under pandemic conditions.
Methods: Patients were stratified and randomized to the intervention group (IG) or the control group (CG). The intervention included a weekly 6-h session for 10 weeks. The CG (waiting list) received an initial 90-min workshop and started the intervention 9 months later. The primary outcome for study feasibility was recruitment and retention rates, as well as reasons for drop-out. The trial took place in Bamberg, Germany (September 2020 to December 2021).
Results: Totally 700 members of the German Crohn's and Colitis Organization—DCCV—were contacted. A total of 15% (102/700; 95% CI 12–17%) expressed interest to participate. Following screening, 41% (95% CI 32–50) were randomized to IG (n = 22) and CG (n = 20). The patients were on average (±standard deviation) 48 ± 13 years old, 67% were female, and have been suffering from CD for 20 ± 12 years. Patients traveled 71.5 ± 48.7 km (range: 9–227 km) to the intervention with no differences between IG and CG. At the 6-month follow-up, 36/42 (86%, 95% CI 74–95%) participants completed final assessment and 19/22 (86%, 95% CI 70–100%) the intervention. The most important reasons for non-responding were work-related (12/60; 20%) and for or drop-out pandemic-related anxiety (3/6). No patient and staff member became infected with SARS-CoV-2 during the study.
Conclusion: The feasibility of the MBM study was confirmed in terms of predefined recruitment and retention criteria, both despite difficult conditions (including the rural setting) and patients' fears associated with the pandemic. It was crucial to develop appropriate hygiene and safety concepts that enable chronically ill patients to participate in helpful group-based interventions even under pandemic conditions.
Clinical trial registration: ClinicalTrials.gov, identifier: NCT05182645.
Introduction
The global prevalence of inflammatory bowel disease has steadily increased within the last two decades, with an average of 1 in 200 people affected (Ng et al., 2017). Crohn's disease (CD) has an overall incidence in Germany of 6.6 new cases per 100,000 inhabitants per year, with ~25,500 patients per year who require inpatient treatment (Preiß et al., 2014; Ng et al., 2017; Sturm et al., 2022). Due to a large number of symptoms, the health-related quality of life (HRQOL) of many patients with CD is comprehensibly impaired in the most productive years of their lives. The most frequently reported symptoms with an impact on HRQOL are diarrhea, abdominal pain, fatigue, anemia, weight loss, recurrent fistulas, and extraintestinal manifestations (Romberg-Camps et al., 2010; Schirbel et al., 2010; Danese et al., 2015; Gomollón et al., 2017). Accordingly, studies have shown a statistically significant correlation between disease activity, need for retreatment, and quality of life (Casellas et al., 2000; Blondel-Kucharski et al., 2001; Bernklev et al., 2005). In addition to physical functions, emotional wellbeing, as well as social and interpersonal interactions, also play an important role in individual HRQOL. A stable social network is perceived as helpful by patients (López Blanco et al., 2005; Katz et al., 2016), while anxiety and depression, as well as dysfunctional coping with the disease, can have a negative impact on HRQOL (van der Eijk et al., 2004; Mawdsley and Rampton, 2005; Tomazoni and Benvegnú, 2018). Consequently, patients' quality of life has increasingly become focused in research on Crohn's disease and other gastrointestinal disorders (Borgaonkar and Irvine, 2000).
In line with these observations, randomized studies have shown that mind-body therapies, meditation, mindfulness, relaxation, stress management programs, and yoga may improve disease-specific quality of life and can even reduce disease-related pain in patients with IBD (Boye et al., 2011; Langhorst et al., 2013, 2015; Gerbarg et al., 2015; Neilson et al., 2016; Norton et al., 2017; Ewais et al., 2019; Torres et al., 2019). Furthermore, preliminary results from small studies suggest that patients with CD may benefit from a moderate exercise program in terms of quality of life (Ng et al., 2007), while a survey substantiated additional beneficial effects on perceived stress by exercise therapies (Torres et al., 2019). There is also some evidence that stress is associated with a higher risk of relapse in IBD (Bitton et al., 2003). In addition, Cognitive behavioral therapy (CBT) has a short-term beneficial effect on QoL in adults with IBD (Gracie et al., 2017). These first promising approaches try to explore possible psychoneuroimmunological connections between the nervous system and the immune system up to gut mucosal levels. Moreover, initial evidence also exists for further lifestyle modifications in the context of IBD (Gracie et al., 2018, 2019; Torres et al., 2019). Of particular interest is the topic of nutrition (Roda et al., 2020). Initial prospective studies have shown a substantially lower risk of later-onset CD in people following a Mediterranean diet (Khalili et al., 2020). In addition, herbal remedies are frequently used by patients as an adjunct to therapy, especially in patients with increased disease activity (Elsenbruch et al., 2005; Langhorst et al., 2005, 2007, 2015, 2020). A survey concluded that certain herbal remedies and acupuncture may reduce disease activity (Langhorst et al., 2015).
Based on these data, it is highly probable that multimodal concepts, which include mindfulness, relaxation methods, exercise, and nutrition, as well as herbal remedies, could be effective. The efficacy of such a multimodal program has already been demonstrated for patients with ulcerative colitis. In particular, there was a significant improvement in the short- and long-term quality of life and mental health (Elsenbruch et al., 2005; Langhorst et al., 2007, 2020; Labanski et al., 2020; Koch et al., 2021; Schlee et al., 2022).
However, the data available to date for patients with CD are still insufficient and some of the available studies have methodological limitations such as missing control groups, small sample size, or a too short follow-up period.
Consequently, there is a need for high-quality studies on multimodal integrative interventions. In January 2020, when recruitment was supposed to start, the first corona cases were reported in Germany.
It quickly became evident that patients with chronic diseases, in particular, that is, at higher risk for a severe COVID course, were increasingly hesitant to utilize medical treatments (Musche et al., 2020). Grunert et al. (2020) reported that patients with IBD were significantly more affected by the COVID-19 pandemic than their non-IBD peers.
Moreover, it was not until 2021 that a cross-sectional study revealed that generalized anxiety is more prevalent in rural communities, whereas COVID-19-related fear is elevated in metropoles (Diala and Muntaner, 2003; Probst et al., 2006; Schweda et al., 2021).
Taken together, we hypothesize that a holistic, comprehensive mind-body lifestyle modification program is a feasible intervention for patients with Crohn's disease even under pandemic circumstances. Therefore, the evaluation of a multimodal integrative program within the framework of this feasibility study aims on one hand to close gaps in care and on the other hand to contribute to the expansion of evidence with high methodological quality to continuously improve the treatment strategies for patients with Crohn's disease.
Materials and methods
Recruitment and patient characteristics
In addition to a call for studies in social and print media, we contacted a total of 700 members of the German Crohn's Disease/Ulcerative Colitis Association (DCCV e.V.)—a patient self-help association—from July 2020 to January 2021. Therefore, we considered a radius of 100 km from the study center to account for the population density in northern Bavaria (Upper Franconia) of 147 inhabitants per km2 (Bayerisches Landesamt für Statistik und Datenverarbeitung, 2014).
Patients who returned received detailed information about the study. The following inclusion criteria were considered: (a) patients between 18 and 75 years, (b) with a confirmed diagnosis of Crohn's disease, (c) stable medication for at least 3 months, and (d) signed informed consent. In contrast, patients with (a) a current highly acute course, (b) complete colectomy, (c) severe mental illness (e.g., major depression, addiction, and schizophrenia), (d) severe comorbid somatic diseases (e.g., diabetes mellitus, and oncological diseases), (e) pregnant women, and (f) participants of stress reduction programs or clinical studies on psychological interventions during the time of study were not eligible to participate in the study.
Study design
To investigate the feasibility of a comprehensive mind-body lifestyle modification program in patients with Crohn's disease, we chose a prospective controlled randomized study design with four data collection points, using different data collection methods. The study was approved by the Ethics Committee of the Bavarian Medical Association (No. 19096), registered at ClinicalTrials.gov (NCT05182645), conducted according to the Declaration of Helsinki, and reported according to the CONSORT statements.
After written informed consent and baseline assessment, patients were randomized in a ratio of 1:1 to the intervention group or the control group stratified by gender, disease severity (clinical remission: mean Harvey Bradshaw Index HBI ≤ 5; mild disease HBI ≥ 6), and medication (immunomodulator yes/no) by de-aging sealed envelopes by the study management at Bamberg Hospital (out-patient department for integrative medicine) at two time points (September 2020 and January 2021). While the intervention group attended the program immediately after the first data collection point (week 0), the control group received a single psychoeducation workshop with information for self-directed application and started the full intervention 9 months later (week 36).
Following the intervention (week 12) and after 6 months (week 36), the questionnaires were again administered and laboratory parameters were collected by independent members of the research department trained in good clinical practice. In addition, the Trier Social Stress Test (TSST), which is a highly reliable method of inducing acute stress, was administered at week 12. Three months after the intervention, subjects in the intervention group were asked to participate in a partially standardized guideline-based telephone interview. Subsequently, subjects in the control group had the opportunity to participate in the intervention (Figure 1). The intervention took place on the premises of the out-patient department and the study visits on the premises of the research team, both from the Department of Internal and Integrative Medicine, Sozialstiftung Bamberg, Bamberg, Germany.
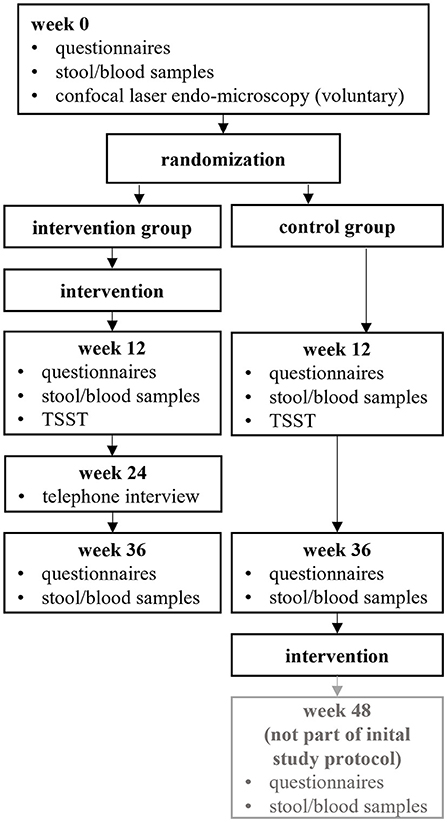
Figure 1. Illustration of the study design. TSST, Trier Social Stress Test.
Intervention
As part of the group intervention, five to seven patients per group participated in a 60-h mind-body medicine and comprehensive lifestyle modification training program over a 10-week-period (i.e., 6 h 1 day a week for 10 weeks) from 11 a.m. to 5 p.m. An experienced mind-body instructor and an experienced gastroenterologist specializing in integrative medicine guided the sessions.
Program topics focused on different procedures described above, for which scientific evidence already exists in patients with CD in an individual setting.
This includes, in particular, stress reduction and stress management, based on the Mind-Body Medical Institutes of the Harvard Medical University (Benson and Stuart, 1993) and the Mindfulness-Based Stress-Reduction (MBSR) program of the University of Massachusetts (Kabat-Zinn, 2013) as described previously in a study with CU patients (Langhorst et al., 2007; Schlee et al., 2022). Techniques taught included relaxation, mindfulness meditation, breathing, yoga, and qi gong, but also elements of cognitive behavioral therapy (CBT) and psychoeducational approaches like stress management, coping skills training, and communication. CBT techniques included perceiving and recognizing automatic thoughts and mental distortions with a focus on one's own patterns of perception and evaluation to meet them with a non-judgmental and self-kind attitude. In addition, Mediterranean whole food nutrition, as suggested by the German consensus treatment guidelines (Sturm et al., 2022), light exercise, and walking were core elements. Complementary self-care strategies, such as hydrotherapy and herbal medicine for gastrointestinal symptoms were also demonstrated and trained. In the time between the out-patient appointments, patients were asked to fill in exercise diaries daily, were given a link to audio guides for relaxation/meditation, and a variety of print information and exercises as homework to encourage 60 min home practice daily.
Participants in the control group received care as usual and a one-time 90-min workshop on mind-body medicine and complementary self-care strategies (on site respectively online). Following the measurement at Week 36, this group was also given the opportunity to participate in the intervention.
At all appointments in attendance, strict adherence to a comprehensive hygiene concept (including adherence to distance rules the obligation to wear an FFP-2 mask throughout the day) was ensured.
Outcomes and research aims
The endpoints focused on feasibility, investigations, and intervention can be find in Table 1. The following definitions of successful feasibility may serve as the basis for conducting a future large-scale confirmatory study:
1. Recruiting more than 10% of eligible patients who were contacted and invited to the study center,
2. at least 67% of the recruited study participants completed the intervention phase and the final follow-up assessment.
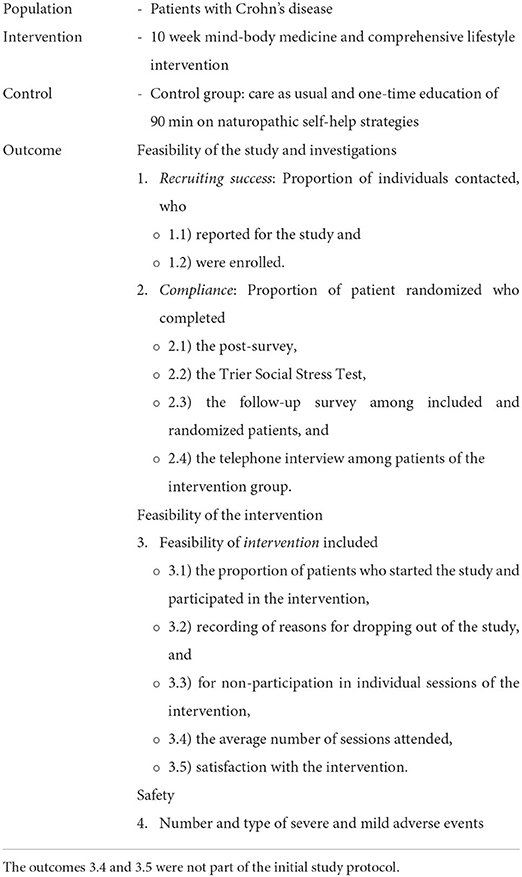
Table 1. P.I.C.O. model endpoints focused on study feasibility, investigations, and intervention.
Instrument design and questionnaire
The anonymous, self-administered questionnaire was compiled based on previous studies (Elsenbruch et al., 2005; Langhorst et al., 2007, 2020; Labanski et al., 2020) and tested for comprehension on three in-patients with CD. It consisted of 174 items covering demographic characteristics, disease-, quality of life- and psychological-related factors. While the focus of this paper is the evaluation of feasibility and compliance, possible treatment effects will be presented separately. Therefore, only questionnaires relevant to this paper are presented.
Disease-specific quality of life was measured using the validated German version of the Inflammatory Bowel Disease Questionnaire. This widely used and validated instrument consisting of 32 items with a 7-point-Likert-scale (1 = always to 7 = never) divided into the four subscales: bowel symptoms, systemic symptoms, social function, and emotional function. The total score can vary from 32 to 224, with higher scores indicating better quality of life (Janke et al., 2006).
The Harvey-Bradshaw Index is a simplification of the Crohn's Disease Activity Index (CDAI; correlation HBI and CDAI, r = 0.93, p < 0.001) and is composed of five items. Sum score was rated as remission (0–4), mild (5–7), moderate (8–16), and severe (>16) disease activity (Harvey and Bradshaw, 1980; Irvine et al., 1994).
Statistical analyses
Response rates and study compliance, as well as treatment adherence and drop-out rates, were calculated as the proportion of patients to whom a characteristic was applied (e.g., participation in post-survey) from the total population considered (all randomized patients) and reported as a percentage with corresponding 95% confidence interval (95% CI). Reasons for individual days of absence or study drop-out were reported qualitatively and quantitatively.
Descriptive statistics were used to report baseline characteristics, including sex, marital status, schooling, occupation, age, distance to the out-patient department, disease duration, disease activity (HBI), and quality of life (IBDQ).
The evaluation of the feasibility was not designed as a confirmatory study. We followed an exploratory approach without formal testing of hypotheses and therefore did not define a formal level of statistical significance.
Results
Sample description
The participants were on average 48 ± 13 years old and 67% were female. Most of them reported living in a stable relationship, having a medium level of education, and working part-time. Almost a quarter of the patients were retired due to age or an illness. At the start of the study, they had been suffering from a diagnosis of Crohn's disease for an average (standard deviation) of 20 ± 12 years, reported mild current disease symptoms (HBI: 6.0 ± 3.7), and a reduced quality of life (IBDQ: 147.1 ± 28.6). The distribution of sociodemographic factors was not considerably different between the two treatment groups (Table 2).
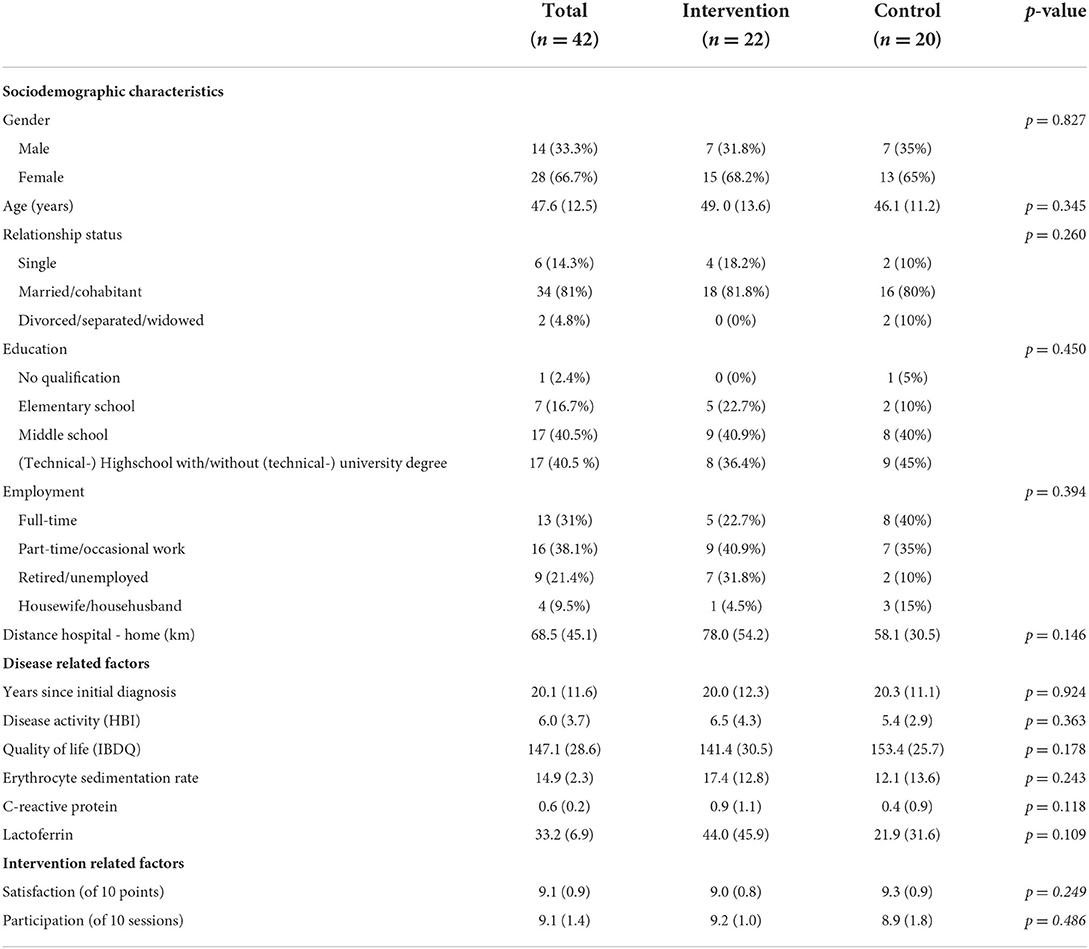
Table 2. Patient characteristics at baseline of the study and intervention related factors.
Feasibility of the study and investigations
About 102 (=15%; 95% CI 12–17%) of 700 patients, more than the predefined 10% of the contacted patients, reported back to the study center (Figure 2). Following the screening, we randomized 6% (42/700; 95% CI 4.4–8.0) of contacted patients and 41% (42/102; 95% CI 32–50%) of patients who reported back to the study center: 22 in the intervention and 20 in the control group. Eighty-six percent (95% CI 70–100%) of the patients remained in the study until the end. The compliance within the study for the investigations at defined time points was similarly high: 86% (95% CI 70–100%) and 85% (95%-CI 67–100%) of the recruited patients completed the post and follow-up surveys, and 83% (71–95%) the Trier Social Stress Test (TSST) at Week 12. Two months after the intervention, all patients in the intervention group agreed to a partially standardized guideline-based telephone interview.
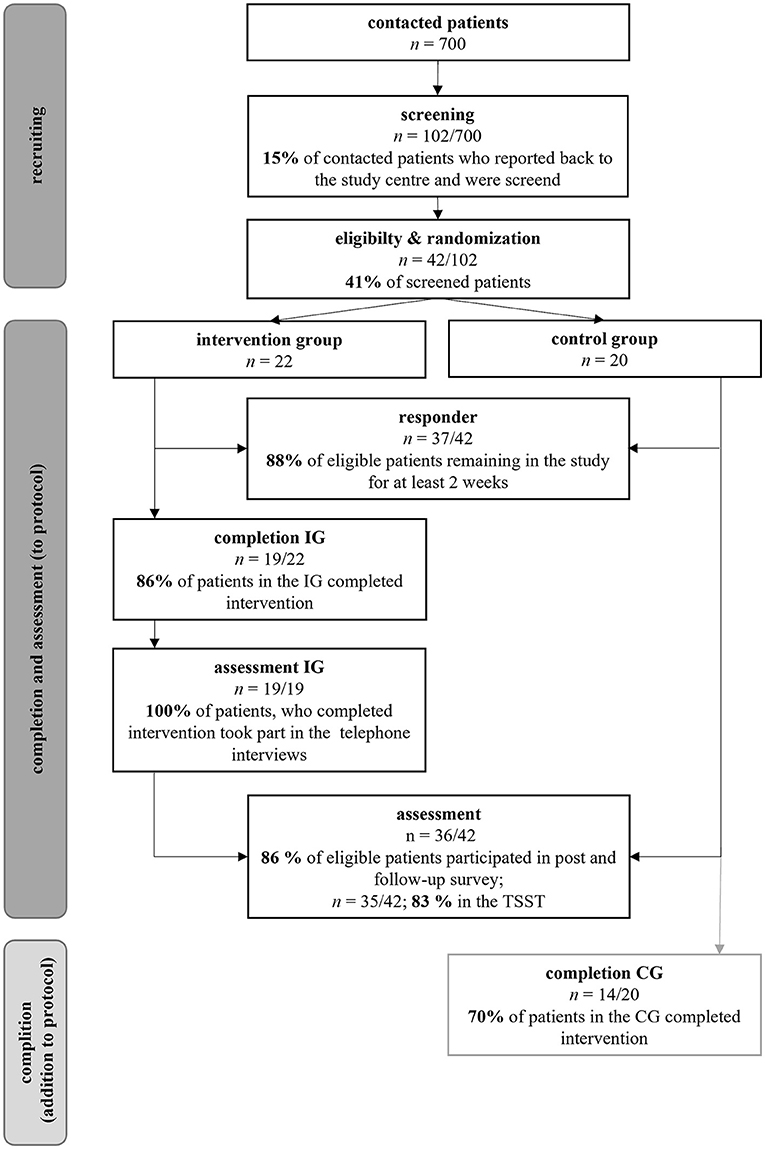
Figure 2. Recruitment success, compliance and feasibility of the intervention. Reasons for non-response and drop-out see Figure 3.
Drop-out rates and feasibility of the intervention
One-third of the patients, who contacted the study center, did not meet the inclusion criteria or met one or more exclusion criteria. Reasons for non-response are listed in Figure 3. Twelve percent of the recruited patients (95% CI 2–23%) dropped out of the study within 2 weeks (IG: 3, CG: 2). Two patients (IG) had hoped to be assigned to the spring/summer waiting control group. For them, participation in a group intervention was not an option due to the high restriction of the measures related to the pandemic (e.g., lock-down) at the time of randomization. Further reasons are reported in Figure 3. The drop-out rates did not differ (95% CI −0.30–0.32) between IG (14%) and CG (15%). With 86% (95% CI 70–100%), the required participation rate of 67% in the intervention group was met.
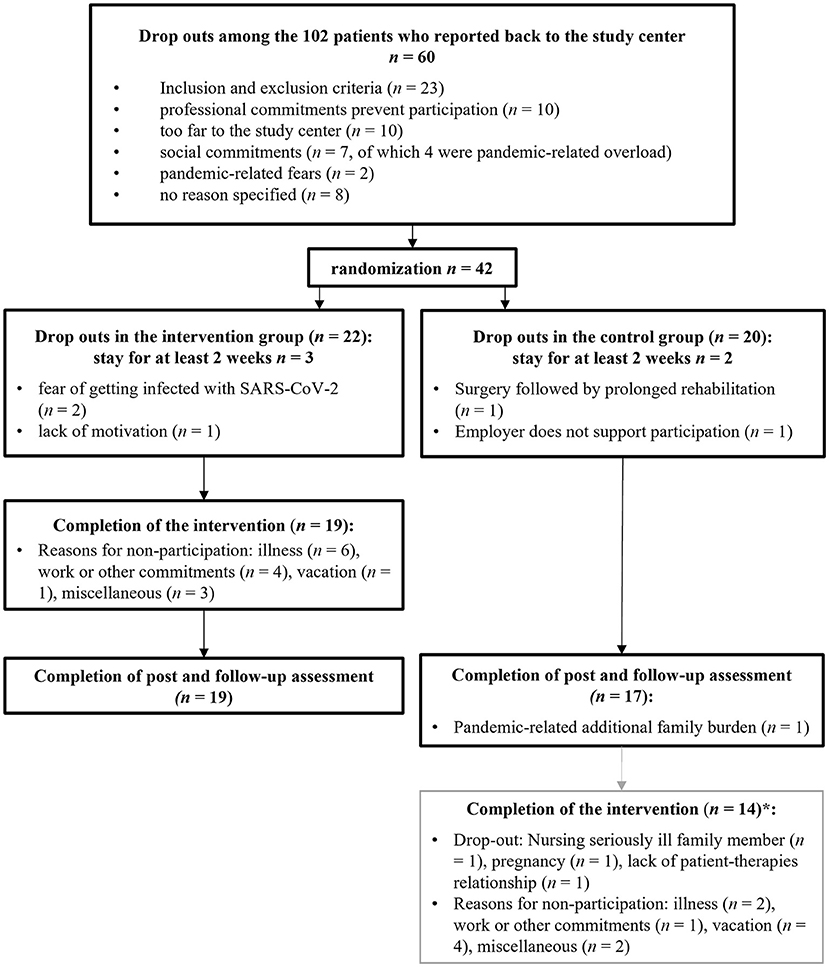
Figure 3. Reasons for study discontinuation. *Completion of the intervention was not part of the initial study protocol.
The following complementary findings are made with regard to feasibility and compliance. Of the 20 patients in the control group, 14 participated in the intervention (70%, 95% CI 48–90%). Patients participated in an average of 9.1 ± 1.4 of the 10 sessions, with no differences between the two groups (95% CI −0.67–1.40). Symptoms of a common cold were reported more frequently in the intervention group (winter months) and vacation more often in the control group (summer months). Patients covered an average distance of 71.5 ± 48.7 km to the intervention (25%-percentile: 37 km; 50%-percentile: 59 km, 75%-percentile: 103 km). The longest distance traveled one way was 227 km. However, patients with a further journey were more likely to skip a session (95% CI −0.66 to −0.04).
The satisfaction with the intervention was high at 9.1 ± 0.9 (95% CI −0.99–0.27), out of a possible 10 points (best score).
Safety of the study under pandemic conditions
During the entire study period, two severe (SAE) and four mild adverse events occurred, which were presumably not causally related to the study. One SAE patient in the control group developed an episode of her Crohn's disease 2 months after baseline measurement and was admitted to the hospital as an inpatient. The second SAE patient suffered pancreatitis after elective endoscopic retrograde cholangiopancreatography (ERCP) shortly after baseline measurement, which kept her from participating in the intervention for the first 2 days of intervention. The four mild adverse events all occurred in the intervention group. For safety reasons, these patients with symptoms typical of a respiratory infection remained at home to avoid infecting other group members in case of (corona) virus infection. Due to this respectful interaction of the group members in the pandemic, as well as the high hygiene standards, no patient and no member of the therapeutic or scientific team became infected with SARS-CoV-2.
Discussion
This paper provides three findings we believe to be important. This study proves for the first time the feasibility of a randomized controlled trial with a long observation period and a comprehensive mind-body lifestyle modification program in patients with Crohn's disease. As the recruitment rate and compliance were achieved according to predefined criteria, the feasibility of such a trial is also given in rural regions and under pandemic conditions. Second, a high level of adherence to the program appointments could be demonstrated. Third, a high level of patient satisfaction with the multi-modal intervention was shown, although this required a strong and continuous commitment.
Feasibility of the study
A particular challenge with regard to the feasibility of studies for patients with chronic diseases, such as CD, is the pandemic. A large cross-sectional German study including almost 17,000 participants could demonstrate elevated levels of generalized anxiety, COVID-19-related fear, adherent/dysfunctional safety behavior, and subjective risk perception in participants with high-risk conditions, such as diabetes or conditions of immunodeficiency (Kohler et al., 2021). In consequence, rates of mental distress and disorders increased significantly (Bäuerle et al., 2020; Mehrotra et al., 2020). Until a vaccine was developed, it was therefore recommended that risk groups, in particular, isolate themselves. However, studies have clearly shown that the COVID-19 pandemic has led to a decrease in the utilization of many medical care services (Mehrotra et al., 2020). This can be reported particularly for chronic conditions (Hacker et al., 2021). For example, in the first summer of the pandemic, 4 in 10 adults surveyed reported that they had postponed or avoided routine or emergency care because of the pandemic (Czeisler et al., 2020). Therefore, treatment teams increasingly focused on transferring face-to-face group therapy to online group chats during the early months of the COVID-19 pandemic (Scholl et al., 2021). However, since multimodal concepts can only be partially adapted to a virtual format, the next challenge was now to develop appropriate hygiene and safety concepts that enable chronically ill patients to participate in helpful programs even under pandemic conditions and to feel safe and in good hands. Even before the S-3 guideline supplement on the COVID-19 pandemic for patients with inflammatory bowel disease was published in October 2020 (Stallmach et al., 2020), the Bamberg study team, therefore, decided to start recruitment.
Against this background, the unexpectedly high interest of the contacted patients with 15% contacting the study center is remarkable. On one hand, this could be due to the many years of very good cooperation with the national patient organization for IBD (“Deutsche Morbus Crohn/Colitis Ulcerosa Vereinigung,” DCCV e.V.), whose members were probably familiar with the expertise and commitment of the study center. Moreover, the role of the self-help group in studies could be very important, as members trust their patient organization, which communicates respectfully with its members and provides information to the best of its knowledge. On the other hand, it could also have played an important role to convey the mitigation efforts to ensure that this mind-body medicine program is safe [e.g., small groups (nmax = 7), large rooms, regularly ventilate, mask requirements, and social distancing] and to explain clearly how to safely access care in the invitation to participate.
If we look at the patients who contacted the study center but then decided against participation before the randomization, it is noticeable that, in particular, professional or social commitments were the most frequently cited reasons for deciding against participation, in addition to a perceived too far journey. This is in line with the results of the recently published qualitative study on patients with ulcerative colitis (Schlee et al., 2022). Less than 4% of eligible patients decided not to participate due to pandemic concerns or fears, which again may indicate that patients felt safe in the study setting presented.
The feasibility of the study was also quantified by the compliance within the study, which was determined as the proportion of subjects who completed the scheduled assessments at different time points. Eighty-six percent of randomized patients completed both the post-survey directly after the intervention and the 6-month follow-up. This figure is comparable to other studies (Berrill et al., 2014; Neilson et al., 2016). However, these studies were not conducted under pandemic conditions, which must be considered.
In addition, 83% of the participants in both study groups carried out the Trier Social Stress Test (TSST), and all patients in the intervention group agreed to a partially standardized guideline-based telephone interview 2 months after the intervention. The fact that patients were even willing to undergo a stress-triggering test, which tends to be perceived as rather unpleasant, as well as a time-intensive telephone interview, speaks for a very good identification with the study and strong patient commitments.
In the control group, only three drop-outs were recorded after randomization, most of which could not be related to study design or waiting time. The fact that, at the end of the actual study, 14 of the 17 patients remaining in the control arm also took the opportunity to participate in an intervention suggests that a multimodal comprehensive mind-body lifestyle modification program addresses the unmet needs of the patients. Moreover, the one-time 90-min workshop on mind-body medicine and complementary self-care strategies in the control group might have been a motivation to stay.
Feasibility of the intervention
To examine the feasibility of the stress-management and comprehensive lifestyle-modification program, we studied patient adherence to appointments with a focus on reasons for non-participation in individual sessions and for dropping out of the study. In addition, we asked the participants about their satisfaction with the intervention.
Three of five patients, who terminated the study early, dropped out in the first 2 weeks after randomization. Although more patients in the intervention group dropped out of the study directly, verbally reported back dissatisfaction with the outcome of randomization was higher in the control group, which may reflect patients' need for a multimodal, multi-week approach. Even though long observation periods are important from a scientific point of view and the patients in the control group received a single psychoeducation workshop, the patients' desire to be allowed to participate in a potentially helpful intervention in a timely manner is understandable.
Because studies have shown that non-compliance is a barrier to learning mindfulness, which is a key element in the investigated comprehensive mind-body lifestyle modification program, it is especially important to examine and understand the reasons for drop-outs and lack of compliance after the start of the intervention (Lymeus et al., 2019; Zhang et al., 2021). Unfortunately, drop-out rates of 25% or higher have been reported in representative studies (Abbott et al., 2014; Lamothe et al., 2016). Adherence to mindfulness-based interventions in patients with inflammatory bowel disease in randomized trials published to date ranged from 55% (Schoultz et al., 2015, 2016) to 58% (Berrill et al., 2014) and remained below the values achieved here even in a study with free group choice (82%) (Neilson et al., 2016).
Adherence from randomization to the end of the holistic integrative medicine intervention was 86%, the same as in a meta-analysis for yoga interventions in Europe (Cramer et al., 2016). However, compared to study data showing that drop-out rates increase with underlying medical conditions and even nearly double as the number of sessions increases (under 8 vs. over 12 sessions) (Cramer et al., 2016), adherence in the context of this study appears unexpectedly high, even more so under pandemic conditions. In this study, although the number of face-to-face sessions is in the middle range at 10 weeks, individual yoga sessions, as in the meta-analysis mentioned above, were considerably shorter at 1–2 h than a duration of 6 h in the out-patient department.
Despite the comprehensive hygiene concept of the hospital, SARS-CoV-2-related fears or anticipated pandemic-related challenges were a major issue for patients already in the recruitment phase and were responsible for half of the study drop-outs in the further course (n = 3 out of 6). On the other hand, this study showed that Crohn's disease patients are motivated to participate in a comprehensive mind-body lifestyle modification program even under pandemic conditions and that its implementation is possible under high hygiene standards without endangering the health of the partly immunosuppressed participants. Not a single SARS-CoV-2 positive patient or therapist during the intervention periods was recorded. In addition, virtual sessions may not appear to be an equivalent alternative to face-to-face sessions. In a systematic review of Internet-based interventions focusing on mindfulness, adherence ranged from 38 to 78% (mean 40%) (Christensen et al., 2009), well below the adherence in the present study.
The patients participated very regularly in the group intervention itself and were extremely satisfied, although a high degree of cooperation (including no sick leave possible) was also required outside the program. The high participation rate is particularly remarkable because many patients travel long distances to take part. To relieve the patients and to make it easier to reconcile the intervention with work, it would be of central importance here to have the intervention recognized as a health insurance benefit with the consequence of the possibility of issuing a certificate of incapacity for work. This is particularly important because a program for building-up personal health competence could be interesting not only for the patients' quality of life but also from an economic point of view.
The results must be interpreted carefully considering several potential limitations. First, a weakness is the small case number, although this is in the nature of feasibility studies. Second, a self-selection bias is likely due to the voluntary character of the intervention and the overrepresentation of women. For example, studies concluded that women use different coping strategies than men and that emotional coping strategies, in particular, may play a greater role. Women might therefore have felt more addressed by the holistic approach (Sarid et al., 2017). Furthermore, it is possible that individuals with an interest in integrative medicine, naturopathy, and/or mindfulness-based exercises, as well as patients who are motivated for group interventions, in general, were more likely to contact the study center. The strengths of the study are the high-quality study design, the data assessment by “good-clinical-practice” certified researcher, and the discussion of drop-out rates and reasons against the background of planning and feasibility of studies under challenging conditions (rural region and pandemic). Where appropriate and necessary (e.g., assessment of disease activity and quality of life), standardized, established, and validated questionnaires were used to allow meaningful classification and, if necessary, subsequent comparison of results in reviews and meta-analyses. Both survey waves, starting September 2020 and January 2021, were conducted identically and strictly according to the study protocol.
Conclusion
In summary, an expansion of the offer of comprehensive mind-body lifestyle modification programs is desirable for patients with Crohn's disease, since this offer is very well accepted by the patients even under rural and pandemic circumstances. Patients showed high adherence, were highly satisfied with the intervention, traveled long distances to the out-patient department, and even participated without a sick leave certificate for the days of the study.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee of the Bavarian Medical Association: No. 19096. The patients/participants provided their written informed consent to participate in this study.
Author contributions
JL and TK contributed to the conception and design of the study. NB, CU, ÖÖ, and JL managed the project administration and the data collection. NB performed the statistical analysis. NB and CL wrote the first draft of the manuscript. All authors have reviewed and edited the manuscript and agreed to the submitted version.
Funding
This study was supported by the Bavarian State Ministry for Health and Care (Germany) by means of the funding program Gesund.Leben.Bayern (in English: Healthy.Living.Bavaria), Reference Number GE7-2497-GLB-19-V4. The sponsors of the present study had no role in the design, execution, interpretation, or writing of the study.
Acknowledgments
We are very grateful for the opportunity to conduct this study. In addition, we wish to thank the German Crohn's and Colitis Association (DCCV e.V.) for their financial and administrative support throughout the study and the funding for the Chair of Integrative Medicine, and the individual participants who donated their time to complete the intervention and study, as well as Beate von Busch, Sina Herberich, Andrea Langhorst, Katrin Pfuhlmann, Ralf Reißmann, Maike Rist, Christoph Schlee, Jessica Schnitker, and Katrin Wagner for their commitment and support and the students Ms. Marie Groh, Ms. Stefanie Kropac, Ms. Luise Leithäuser, and Ms. Verena Thomann for their assistance.
Conflict of interest
CL received lecture fees from Celgene GmbH, Roche GmbH, Novartis Pharma GmbH, BMS GmbH & Co. KGaA, Mundipharma GmbH Co. KG, Merck KGaA. JL was a speaker for Repha GmbH, Techlab Inc., Falk Foundation, Takeda, Celegene GmbH and Willmar Schwabe and received research funding from Repha GmbH, Techlab Inc., Falk Foundation and Willmar Schwabe.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor SS declared a shared affiliation with the author TK at the time of review.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abbott, R. A., Whear, R., Rodgers, L. R., Bethel, A., Thompson Coon, J., Kuyken, W., et al. (2014). Effectiveness of mindfulness-based stress reduction and mindfulness based cognitive therapy in vascular disease: a systematic review and meta-analysis of randomised controlled trials. J. Psychosom. Res. 76, 341–351. doi: 10.1016/j.jpsychores.2014.02.012
Bäuerle, A., Teufel, M., Musche, V., Weismüller, B., Kohler, H., Hetkamp, M., et al. (2020). Increased generalized anxiety, depression and distress during the COVID-19 pandemic: a cross-sectional study in Germany. J. Public Health 42, 672–678. doi: 10.1093/pubmed/fdaa106
Bayerisches Landesamt für Statistik und Datenverarbeitung. (2014). Bayern in Zahlen Ausgabe 11: Zensus 2011. Munich: Bayerisches Landesamt für Statistik und Datenverarbeitung.
Benson, H., and Stuart, E. M. (1993). The Wellness Book. Boston, MA: Harvard Medical School; Mind-Body Medicine.
Bernklev, T., Jahnsen, J., Schulz, T., Sauar, J., Lygren, I., Henriksen, M., et al. (2005). Course of disease, drug treatment and health-related quality of life in patients with inflammatory bowel disease 5 years after initial diagnosis. Eur. J. Gastroenterol. Hepatol. 17, 1037–1045. doi: 10.1097/00042737-200510000-00006
Berrill, J. W., Sadlier, M., Hood, K., and Green, J. T. (2014). Mindfulness-based therapy for inflammatory bowel disease patients with functional abdominal symptoms or high perceived stress levels. J. Crohn's Colitis 8, 945–955. doi: 10.1016/j.crohns.2014.01.018
Bitton, A., Sewitch, M. J., Peppercorn, M. A., deB Edwardes, M. D., Shah, S., Ransil, B., et al. (2003). Psychosocial determinants of relapse in ulcerative colitis: a longitudinal study. Am. J. Gastroenterol. 98, 2203–2208. doi: 10.1111/j.1572-0241.2003.07717.x
Blondel-Kucharski, F., Chircop, C., Marquis, P., Cortot, A., Baron, F., Gendre, J. P., et al. (2001). Health-related quality of life in Crohn's disease: a prospective longitudinal study in 231 patients. Am. J. Gastroenterol. 96, 2915–2920. doi: 10.1111/j.1572-0241.2001.04681.x
Borgaonkar, M. R., and Irvine, E. J. (2000). Quality of life measurement in gastrointestinal and liver disorders. Gut 47, 444–454. doi: 10.1136/gut.47.3.444
Boye, B., Lundin, K. E. A., Jantschek, G., Leganger, S., Mokleby, K., Tangen, T., et al. (2011). INSPIRE study: does stress management improve the course of inflammatory bowel disease and disease-specific quality of life in distressed patients with ulcerative colitis or Crohn's disease? A randomized controlled trial. Inflamm. Bowel Dis. 17, 1863–1873. doi: 10.1002/ibd.21575
Casellas, F., López-Vivancos, J., Badia, X., Vilaseca, J., and Malagelada, J. R. (2000). Impact of surgery for Crohn's disease on health-related quality of life. Am. J. Gastroenterol. 95, 177–182. doi: 10.1111/j.1572-0241.2000.01681.x
Christensen, H., Griffiths, K. M., and Farrer, L. (2009). Adherence in internet interventions for anxiety and depression. J. Med. Internet Res. 11, e13. doi: 10.2196/jmir.1194
Cramer, H., Haller, H., Dobos, G., and Lauche, R. (2016). A systematic review and meta-analysis estimating the expected dropout rates in randomized controlled trials on yoga interventions. Evid. Based Complement. Alternat. Med. 2016, 5859729. doi: 10.1155/2016/5859729
Czeisler, M. É., Marynak, K., Clarke, K. E. N., Salah, Z., Shakya, I., Thierry, J. M., et al. (2020). Delay or avoidance of medical care because of COVID-19-related concerns - United States, June 2020. MMWR Morb. Mortal. Wkly. Rep. 69, 1250–1257. doi: 10.15585/mmwr.mm6936a4
Danese, S., Fiorino, G., Mary, J.-Y., Lakatos, P. L., D'Haens, G., Moja, L., et al. (2015). Development of red flags index for early referral of adults with symptoms and signs suggestive of Crohn's disease: an IOIBD initiative. J. Crohn's Colitis 9, 601–606. doi: 10.1093/ecco-jcc/jjv067
Diala, C. C., and Muntaner, C. (2003). Mood and anxiety disorders among rural, urban, and metropolitan residents in the United States. Commun. Ment. Health J. 39, 239–252. doi: 10.1023/A:1023342307323
Elsenbruch, S., Langhorst, J., Popkirowa, K., Müller, T., Luedtke, R., Franken, U., et al. (2005). Effects of mind-body therapy on quality of life and neuroendocrine and cellular immune functions in patients with ulcerative colitis. Psychother. Psychosom. 74, 277–287. doi: 10.1159/000086318
Ewais, T., Begun, J., Kenny, M., Chuang, K.-H., Barclay, J., Hay, K., et al. (2019). Protocol for a pilot randomised controlled trial of mindfulness-based cognitive therapy in youth with inflammatory bowel disease and depression. BMJ Open 9, e025568. doi: 10.1136/bmjopen-2018-025568
Gerbarg, P. L., Jacob, V. E., Stevens, L., Bosworth, B. P., Chabouni, F., DeFilippis, E. M., et al. (2015). The effect of breathing, movement, and meditation on psychological and physical symptoms and inflammatory biomarkers in inflammatory bowel disease: a randomized controlled trial. Inflamm. Bowel Dis. 21, 2886–2896. doi: 10.1097/MIB.0000000000000568
Gomollón, F., Dignass, A., Annese, V., Tilg, H., van Assche, G., Lindsay, J. O., et al. (2017). 3rd European evidence-based consensus on the diagnosis and management of Crohn's disease 2016: part 1: diagnosis and medical management. J. Crohn's Colitis 11, 3–25. doi: 10.1093/ecco-jcc/jjw168
Gracie, D. J., Guthrie, E. A., Hamlin, P. J., and Ford, A. C. (2018). Bi-directionality of brain-gut interactions in patients with inflammatory bowel disease. Gastroenterology 154, 1635–1646.e3. doi: 10.1053/j.gastro.2018.01.027
Gracie, D. J., Hamlin, P. J., and Ford, A. C. (2019). The influence of the brain–gut axis in inflammatory bowel disease and possible implications for treatment. Lancet Gastroenterol. Hepatol. 4, 632–642. doi: 10.1016/S2468-1253(19)30089-5
Gracie, D. J., Irvine, A. J., Sood, R., Mikocka-Walus, A., Hamlin, P. J., and Ford, A. C. (2017). Effect of psychological therapy on disease activity, psychological comorbidity, and quality of life in inflammatory bowel disease: a systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2, 189–199. doi: 10.1016/S2468-1253(16)30206-0
Grunert, P. C., Reuken, P. A., Stallhofer, J., Teich, N., and Stallmach, A. (2020). Inflammatory bowel disease in the COVID-19 pandemic: the patients' perspective. J. Crohn's Colitis 14, 1702–1708. doi: 10.1093/ecco-jcc/jjaa126
Hacker, K. A., Briss, P. A., Richardson, L., Wright, J., and Petersen, R. (2021). COVID-19 and chronic disease: the impact now and in the future. Prev. Chronic Dis. 18, E62. doi: 10.5888/pcd18.210086
Harvey, R. F., and Bradshaw, J. M. (1980). A simple index of Crohn's-disease activity. Lancet 315, 514. doi: 10.1016/S0140-6736(80)92767-1
Irvine, E., Feagan, B., Rochon, J., Archambault, A., Fedorak, R. N., Groll, A., et al. (1994). Quality of life: a valid and reliable measure of therapeutic efficacy in the treatment of inflammatory bowel disease. Gastroenterology 106, 287–296. doi: 10.1016/0016-5085(94)90585-1
Janke, K.-H., Klump, B., Steder-Neukamm, U., Hoffmann, J., and Häuser, W. (2006). Validierung der Deutschen Version (Kompetenznetz “Chronisch entzündliche Darmerkrankungen”) des Inflammatory Bowel Disease Questionnaire IBDQ-D. Psychother. Psychosom. Med. Psychol. 56, 291–298. doi: 10.1055/s-2006-932661
Kabat-Zinn, J. (2013). Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness. New York, NY: Bantam Books Trade Paperbacks.
Katz, L., Tripp, D. A., Ropeleski, M., Depew, W., Curtis Nickel, J., Vanner, S., et al. (2016). Mechanisms of quality of life and social support in inflammatory bowel disease. J. Clin. Psychol. Med. Settings 23, 88–98. doi: 10.1007/s10880-015-9431-x
Khalili, H., Håkansson, N., Chan, S. S., Chen, Y., Lochhead, P., Ludvigsson, J. F., et al. (2020). Adherence to a Mediterranean diet is associated with a lower risk of later-onset Crohn's disease: results from two large prospective cohort studies. Gut 69, 1637–1644. doi: 10.1136/gutjnl-2019-319505
Koch, A. K., Schöls, M., Haller, H., Anheyer, D., Cinar, Z., Eilert, R., et al. (2021). Comprehensive lifestyle modification influences medium-term and artificially induced stress in ulcerative colitis-A sub-study within a randomized controlled trial using the trier social stress test. J. Clin. Med. 10, 5070. doi: 10.3390/jcm10215070
Kohler, H., Bäuerle, A., Schweda, A., Weismüller, B., Fink, M., Musche, V., et al. (2021). Increased COVID-19-related fear and subjective risk perception regarding COVID-19 affects behavior in individuals with internal high-risk diseases. J. Prim. Care Commun. Health 12, 2150132721996898. doi: 10.1177/2150132721996898
Labanski, A., Langhorst, J., Engler, H., and Elsenbruch, S. (2020). Stress and the brain-gut axis in functional and chronic-inflammatory gastrointestinal diseases: a transdisciplinary challenge. Psychoneuroendocrinology 111, 104501. doi: 10.1016/j.psyneuen.2019.104501
Lamothe, M., Rondeau, É., Malboeuf-Hurtubise, C., Duval, M., and Sultan, S. (2016). Outcomes of MBSR or MBSR-based interventions in health care providers: a systematic review with a focus on empathy and emotional competencies. Complem. Therap. Med. 24, 19–28. doi: 10.1016/j.ctim.2015.11.001
Langhorst, J., Anthonisen, I. B., Steder-Neukamm, U., Lüdtke, R., Spahn, G., Michalsen, A., et al. (2005). Amount of systemic steroid medication is a strong predictor for the use of complementary and alternative medicine in patients with inflammatory bowel disease: results from a German national survey. Inflamm. Bowel Dis. 11, 287–295. doi: 10.1097/01.MIB.0000160771.71328.6c
Langhorst, J., Hofstetter, A., Wolfe, F., and Häuser, W. (2013). Short-term stress, but not mucosal healing nor depression was predictive for the risk of relapse in patients with ulcerative colitis: a prospective 12-month follow-up study. Inflamm. Bowel Dis. 19, 2380–2386. doi: 10.1097/MIB.0b013e3182a192ba
Langhorst, J., Mueller, T., Luedtke, R., Franken, U., Paul, A., Michalsen, A., et al. (2007). Effects of a comprehensive lifestyle modification program on quality-of-life in patients with ulcerative colitis: a twelve-month follow-up. Scand. J. Gastroenterol. 42, 734–745. doi: 10.1080/00365520601101682
Langhorst, J., Schöls, M., Cinar, Z., Eilert, R., Kofink, K., Paul, A., et al. (2020). Comprehensive lifestyle-modification in patients with ulcerative colitis-A randomized controlled trial. J. Clin. Med. 9, 3087. doi: 10.3390/jcm9103087
Langhorst, J., Wulfert, H., Lauche, R., Klose, P., Cramer, H., Dobos, G. J., et al. (2015). Systematic review of complementary and alternative medicine treatments in inflammatory bowel diseases. J. Crohn's Colitis 9, 86–106. doi: 10.1093/ecco-jcc/jju007
López Blanco, B., Moreno-Jiménez, B., Devesa Múgica, J. M., and Rodríguez Muñoz, A. (2005). Relationship between socio-demographic and clinical variables, and health-related quality of life in patients with inflammatory bowel disease. Rev. Esp. Enferm Dig. 97, 887–898. doi: 10.4321/S1130-01082005001200005
Lymeus, F., Lindberg, P., and Hartig, T. (2019). A natural meditation setting improves compliance with mindfulness training. J. Environ. Psychol. 64, 98–106. doi: 10.1016/j.jenvp.2019.05.008
Mawdsley, J. E., and Rampton, D. S. (2005). Psychological stress in IBD: new insights into pathogenic and therapeutic implications. Gut 54, 1481–1491. doi: 10.1136/gut.2005.064261
Mehrotra, A., Chernew, M. E., Linetsky, D., Hatch, H., Cutler, D. A., and Schneider, E. C. (2020). The Impact of the COVID-19 Pandemic on Outpatient Care: Visits Return to Prepandemic Levels, But Not for All Providers and Patients. Common Health Fund. doi: 10.26099/41xy-9m57
Musche, V., Bäuerle, A., Steinbach, J., Schweda, A., Hetkamp, M., Weismüller, B., et al. (2020). COVID-19-related fear and health-related safety behavior in oncological patients. Front. Psychol 11, 1984. doi: 10.3389/fpsyg.2020.01984
Neilson, K., Ftanou, M., Monshat, K., Salzberg, M., Bell, S., Kamm, M. A., et al. (2016). A controlled study of a group mindfulness intervention for individuals living with inflammatory bowel disease. Inflamm. Bowel Dis. 22, 694–701. doi: 10.1097/MIB.0000000000000629
Ng, S. C., Shi, H. Y., Hamidi, N., Underwood, F. E., Tang, W., Benchimol, E. I., et al. (2017). Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet 390, 2769–2778. doi: 10.1016/S0140-6736(17)32448-0
Ng, V., Millard, W., Lebrun, C., and Howard, J. (2007). Low-intensity exercise improves quality of life in patients with Crohn's disease. Clin. J. Sport Med. 17, 384–388. doi: 10.1097/JSM.0b013e31802b4fda
Norton, C., Czuber-Dochan, W., Artom, M., Sweeney, L., and Hart, A. (2017). Systematic review: interventions for abdominal pain management in inflammatory bowel disease. Aliment. Pharmacol. Therap. 46, 115–125. doi: 10.1111/apt.14108
Preiß, J. C., Bokemeyer, B., Buhr, H. J., Dignaß, A., Häuser, W., Hartmann, F., et al. (2014). Aktualisierte S3-Leitlinie— “Diagnostik und Therapie des Morbus Crohn” 2014. Zeitschrift für Gastroenterologie 52, 1431–1484. doi: 10.1055/s-0034-1385199
Probst, J. C., Laditka, S. B., Moore, C. G., Harun, N., Powell, M. P., and Baxley, E. G. (2006). Rural-urban differences in depression prevalence: implications for family medicine. Fam. Med. 38, 653–660.
Roda, G., Chien Ng, S., Kotze, P. G., Argollo, M., Panaccione, R., Spinelli, A., et al. (2020). Crohn's disease. Nat. Rev. Dis. Primers 6, 22. doi: 10.1038/s41572-020-0193-x
Romberg-Camps, M. J. L., Bol, Y., Dagnelie, P. C., Hesselink-van de Kruijs, M. A. M., Kester, A. D. M., Engels, L. G. J. B., et al. (2010). Fatigue and health-related quality of life in inflammatory bowel disease: results from a population-based study in the Netherlands: the IBD-South Limburg cohort. Inflamm. Bowel Dis. 16, 2137–2147. doi: 10.1002/ibd.21285
Sarid, O., Slonim-Nevo, V., Pereg, A., Friger, M., Sergienko, R., Schwartz, D., et al. (2017). Coping strategies, satisfaction with life, and quality of life in Crohn's disease: a gender perspective using structural equation modeling analysis. PLoS ONE 12, e0172779. doi: 10.1371/journal.pone.0172779
Schirbel, A., Reichert, A., Roll, S., Baumgart, D. C., Büning, C., Wittig, B., et al. (2010). Impact of pain on health-related quality of life in patients with inflammatory bowel disease. World J. Gastroenterol. 16, 3168–3177. doi: 10.3748/wjg.v16.i25.3168
Schlee, C., Uecker, C., Bauer, N., Koch, A. K., and Langhorst, J. (2022). Multimodal stress reduction and lifestyle modification program for patients with ulcerative colitis: a qualitative study. BMC Complement. Med. Ther. 22, 60. doi: 10.1186/s12906-021-03478-w
Scholl, J., Kohls, E., Görges, F., Steinbrecher, M., Baldofski, S., Moessner, M., et al. (2021). Acceptability and feasibility of the transfer of face-to-face group therapy to online group chats in a psychiatric outpatient setting during the COVID-19 pandemic: longitudinal observational study. JMIR Form. Res. 5, e27865. doi: 10.2196/27865
Schoultz, M., Atherton, I., and Watson, A. (2015). Mindfulness-based cognitive therapy for inflammatory bowel disease patients: findings from an exploratory pilot randomised controlled trial. Trials 16, 379. doi: 10.1186/s13063-015-0909-5
Schoultz, M., Macaden, L., and Hubbard, G. (2016). Participants' perspectives on mindfulness-based cognitive therapy for inflammatory bowel disease: a qualitative study nested within a pilot randomised controlled trial. Pilot Feasibility Stud. 2, 3. doi: 10.1186/s40814-015-0041-z
Schweda, A., Weismüller, B., Bäuerle, A., Dörrie, N., Musche, V., Fink, M., et al. (2021). Phenotyping mental health: age, community size, and depression differently modulate COVID-19-related fear and generalized anxiety. Compr. Psychiatry 104, 152218. doi: 10.1016/j.comppsych.2020.152218
Stallmach, A., Sturm, A., Blumenstein, I., Helwig, U., Koletzko, S., Lynen, P., et al. (2020). Addendum zu den S3-Leitlinien Morbus Crohn und Colitis ulcerosa: Betreuung von Patienten mit chronisch entzündlichen Darmerkrankungen in der COVID-19-Pandemie – offene Fragen und Antworten. Zeitschrift für Gastroenterologie 58, 982–1002. doi: 10.1055/a-1234-8079
Sturm, A., Atreya, R., Bettenworth, D., Bokemeyer, B., Dignaß, A., Ehehalt, R., et al. (2022). Aktualisierte S3-Leitlinie “Diagnostik und Therapie des Morbus Crohn” der Deutschen Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankheiten (DGVS) – August 2021 – AWMF-Registernummer: 021-004. Zeitschrift für Gastroenterologie 60, 332–418. doi: 10.1055/a-1713-3941
Tomazoni, E. I., and Benvegnú, D. M. (2018). Symptoms of anxiety and depression, and quality of life of patients with Crohn's disease. Arq. Gastroenterol. 55, 148–153. doi: 10.1590/s0004-2803.201800000-26
Torres, J., Ellul, P., Langhorst, J., Mikocka-Walus, A., Barreiro-de Acosta, M., Basnayake, C., et al. (2019). European Crohn's and colitis organisation topical review on complementary medicine and psychotherapy in inflammatory bowel disease. J. Crohn's Colitis 13, 673–685e. doi: 10.1093/ecco-jcc/jjz051
van der Eijk, I., Vlachonikolis, I. G., Munkholm, P., Nijman, J., Bernklev, T., Politi, P., et al. (2004). The role of quality of care in health-related quality of life in patients with IBD. Inflamm. Bowel Dis. 10, 392–398. doi: 10.1097/00054725-200407000-00010
Keywords: Crohn's disease, lifestyle modification, mind-body medicine, pandemic, inflammatory bowel disease, stress management, rural conditions, feasibility
Citation: Bauer N, Löffler C, Öznur Ö, Uecker C, Keil T and Langhorst J (2022) Mind-body-medicine and comprehensive lifestyle-modification in patients with Crohn's disease—Feasibility of a randomized controlled trial under pandemic circumstances. Front. Integr. Neurosci. 16:960301. doi: 10.3389/fnint.2022.960301
Received: 02 June 2022; Accepted: 08 July 2022;
Published: 23 August 2022.
Edited by:
Steffen Schulz, Charité Universitätsmedizin Berlin, GermanyReviewed by:
Mohamed Hassan Elnaem, International Islamic University Malaysia, MalaysiaLeila Itani, Beirut Arab University, Lebanon
Milena Peruhova, Lozenetz Hospital, Bulgaria
Copyright © 2022 Bauer, Löffler, Öznur, Uecker, Keil and Langhorst. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jost Langhorst, am9zdC5sYW5naG9yc3RAc296aWFsc3RpZnR1bmctYmFtYmVyZy5kZQ==
†These authors have contributed equally to this work and share first authorship