 Ronghui Li1
Ronghui Li1 Chunjiang Wang
Chunjiang Wang Xiang Liu
Xiang Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 18 March 2025
Sec. Cancer Immunity and Immunotherapy
Volume 16 - 2025 | https://doi.org/10.3389/fimmu.2025.1563100
This article is part of the Research TopicCommunity Series in Reducing Adverse Effects of Cancer Immunotherapy: Volume IIIView all 5 articles
Background: Stevens – Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) is a life-threatening adverse reaction to nivolumab. This study investigated the clinical features of nivolumab induced SJS/TEN to provide evidence for diagnosis and treatment.
Methods: Relevant articles on nivolumab induced SJS/TEN published before December 31, 2024 were collected by searching the database, and then extracting the data for summary analysis.
Results: Thirty-one patients were enrolled with a median age of 65 years (range 43, 86). SJS/TEN appear at a median of 5.5 weeks (range, 0.9 108). Bullae/blisters (64.5%), erythema (54.8%), skin rash (54.8%), epidermal detachment (29.0%) and pain (29.0%) were the main skin symptoms. Skin biopsy showed epidermal necrosis (41.9%), keratinocytic necrosis (38.7%), interface dermatitis (29.0%) and inflammatory cell infiltration (45.2%). After stopping nivolumab and receiving treatment, 74.2% of the patients had improvement in skin symptoms, and 22.6% of the patients died of TEN.
Conclusion: As a rare immune-related adverse event of nivolumab, SJS/TEN should be closely monitored during the treatment. Nivolumab induced SJS/TEN has a long incubation period, serious clinical symptoms and poor prognosis.
Nivolumab, an immune checkpoint inhibitor (ICIs) approved in 2014, is used to treat a variety of malignancies such as melanoma, renal cell carcinoma, head and neck squamous cell carcinoma, and non-Hodgkin’s lymphoma (1). Nivolumab has demonstrated remarkable anti-tumor activity; however, it has also been associated with a significant incidence of immune-related adverse events (irAEs). Nivolumab may trigger multi-system irAEs, such as skin, gastrointestinal tract, endocrine system, hepatotoxicity, kidney and lung toxicity (2). Among them, the incidence of cutaneous immune−related adverse events (cirAEs) caused by nivolumab is the highest, which greatly affects patients’ quality of life and anti-tumor treatment decisions. Pruritus (30.1%), maculopapular rash (24.7%) and vitiligo (16.1%) were more common (3). Stevens – Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) is a life-threatening skin-mucous reaction characterized by vesicles and generalized epidermolysis, which may be associated with multiple system involvement (4). SJS/TEN is a rare irAEs of nivolumab. Unfortunately, knowledge about nivolumab-induced SJS/TEN comes mainly from case reports. The clinical regularity of nivolumab induced SJS/TEN still needs to be explored. This study summarized the clinical manifestations, treatment and prognosis of nivolumab induced SJS/TEN, and provided a reference for clinicians to diagnose and treat nivolumab induced SJS/TEN.
Case reports and case series articles on nivolumab induced SJS/TEN were included by searching the database. Databases involved in this study include PubMed, EMbase, Web of Science, Cochrane Library, WanFang Data, China National Knowledge Infrastructure, China Science and Technology Journal Database, China Biology Medicine disc. The search language is limited to Chinese and English, and the search time ends on December 31, 2024. The retrieval method is the combination of the subject heading and text word terms through the Boolean operator connection. The search regimens included “nivolumab” OR “immune checkpoint inhibitor” OR “PD1 inhibitor” AND “Stevens-Johnson syndrome/toxic epidermal necrolysis” OR “Stevens-Johnson syndrome” OR “toxic epidermal necrolysis” OR “SJS/TEN” OR “immune-related adverse events” OR “cutaneous immune−related adverse events”.
Case reports and case series of nivolumab induced SJS/TEN were included. Duplicate articles, reviews, mechanism studies, and non-nivolumab induced SJS/TEN were excluded.
The author designed the table and extracted the patient’s clinical data, including country, gender, age, incubation period, indications, disease history, concomitant medications, clinical manifestations, other autoimmune related adverse events, Nikolsky sign, SJS/TEN type, other autoimmune related adverse events, skin biopsy, treatment and outcome.
SJS is defined as the epidermolysis area < 10% body surface area, TEN is defined as the epidermolysis area > 30% body surface area, SJS/TEN overlap is defined as the epidermolysis area of 10% ~ 30% body surface area (5).
SPSS 26.0 software was used for statistical analysis of the extracted data. The counting data is represented by n (%), and the measurement data is the median value (range minimum, maximum).
After screening, 29 studies were eventually included, including 31 patients (Figure 1). Table 1 summarizes the basic information of 31 patients. The median age of the 31 patients was 65 years (range 43, 86), including 18 males (58.1%) and 13 (41.9%) females. The top three reporting countries were the USA (11 cases, 35.5%), Japan (7 cases, 22.6%) and the United Kingdom (5 cases, 16.1%). The main cancer type in these patients was melanoma (9 cases, 29.0%) and lung cancer (6 cases, 19.4%). The onset time of SJS/TEN was 5.5 weeks (range 0.9,108) after the initial dose, including 7 weeks (range 0.9,108) for TEN and 6 weeks (range 1, 36) for SJS. The median cycle at the onset of SJS/TEN is 2 cycles (range 1, 77). Fifteen patients reported duration of onset of SJS/TEN after discontinuation, with a median duration of 10 days (range 2, 180). Sixteen (51.6%) patients had a history of diseases, including atrial fibrillation, hypertension, liver cirrhosis, hyperlipidemia, chronic kidney disease, follicular lymphoma, diabetes mellitus, hypersplenism, hepatitis C infection, Parkinson disease, peripheral neuropathy, hypothyroidism, hepatocellular carcinoma, gastro-esophageal reflux disease, osteoporosis. Sixteen patients were treated with other drugs, of which 7 (22.6%) received nivolumab and ipilimumab.
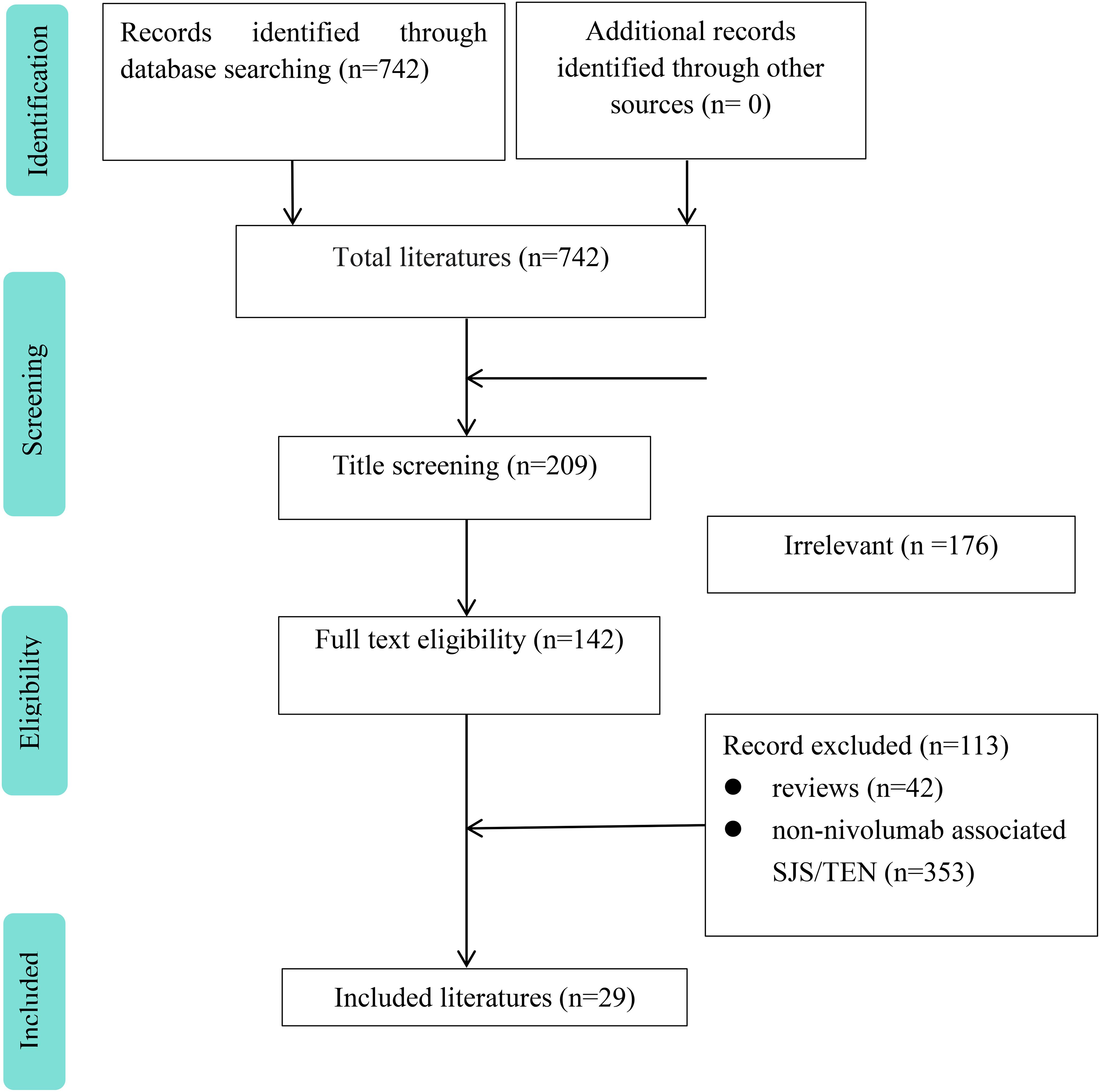
Figure 1. Flow chart of study selection process for reported cases of nivolumab-induced SJS/TEN.
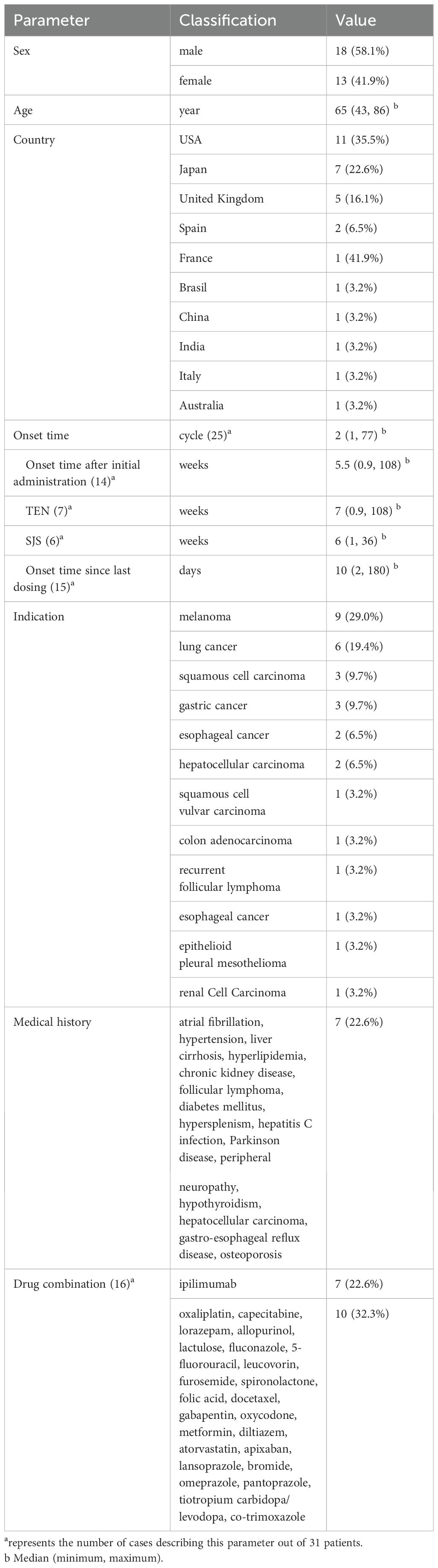
Table 1. Basic data of 31 patients with nivolumab-induced SJS/TEN.
Table 2 summarizes the clinical manifestations of 31 patients. The main skin symptoms of the patients were bullae/blisters (20 cases, 64.5%), erythema (17 cases, 54.8%), skin rash (17 cases, 54.8%), epidermal detachment (9 cases, 29.0%) and pain (9 cases, 29.0%). A small number of other patients may present with oral erosions (7 cases, 22.6%), skin erosion (6 cases, 19.4%), pruritus (6 cases, 19.4%), desquamation (6 cases, 19.4%), fever (6 cases, 19.4%). 19.4%) and lip crusting (6 cases, 19.4%) Twenty-five (80.6%) patients experienced mucosal involvement, including oral mucosa (21 patients, 67.7%), conjunctiva (10 patients, 32.3%), and genitals (8 patients, 25.8%).
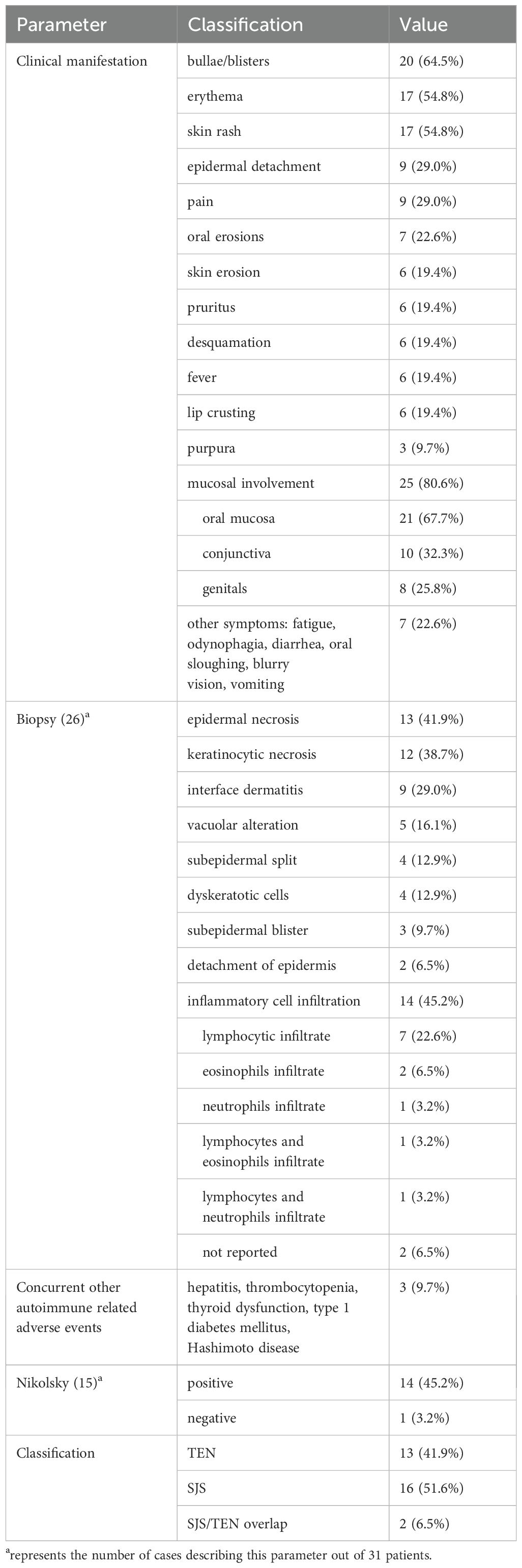
Table 2. Clinical features of 31 patients with nivolumab-induced SJS/TEN.
Nikolsky sign was reported in 15 patients, of whom 14 (45.2%) were positive. Three patients (9.7%) had other autoimmune related adverse events, including hepatitis, thrombocytopenia, thyroid dysfunction, type 1 diabetes mellitus, Hashimoto disease. According to the classification criteria, 16 (51.6%) patients were defined as SJS, 13 (41.9%) as TEN, and 2 (6.5%) as SJS/TEN overlap.
Table 2 summarizes the skin biopsy of 31 patients. Skin biopsy was performed in 26 of the 31 patients, and the main findings were epidermal necrosis (13 cases, 41.9%), keratinocytic necrosis (12 cases, 38.7%), interface dermatitis (9 cases, 29.0%) and inflammatory cell infiltration (14 cases, 45.2%). These inflammatory cells were mainly lymphocytes (7 cases, 22.6%), followed by neutrophils (2 cases, 6.5%).
Table 3 summarizes the treatment regimens and outcomes of 31 patients. Thirty (96.8%) patients withdrew nivolumab and one (3.2%) patient did not report nivolumab status. Twenty-seven (87.1%) patients received systemic steroid therapy and 10 (32.3%) patients received intravenous immunoglobulins (IVIG). Other treatment regimens included topical steroid (4 cases, 12.9%), cyclosporine (2 cases, 6.5%), infliximab (2 cases, 6.5%), etanercept (1 case, 3.2%), ruxolitinib (1 patient, 6.5%), ruxolitinib (1 case,6.5%). 3.2%) and plasmapheresis (1 case, 3.2%). Among patients treated with nivolumab alone, 20 (64.5%) patients experienced improvement in skin symptoms and 4 (12.9%) patients died from TEN. Of the seven patients treated with nivolumab and ipilimumab, three died of multiple organ failure, two improved symptoms, and one did not describe the outcome. The median time to improvement of skin symptoms was 28 days (range 14, 360).
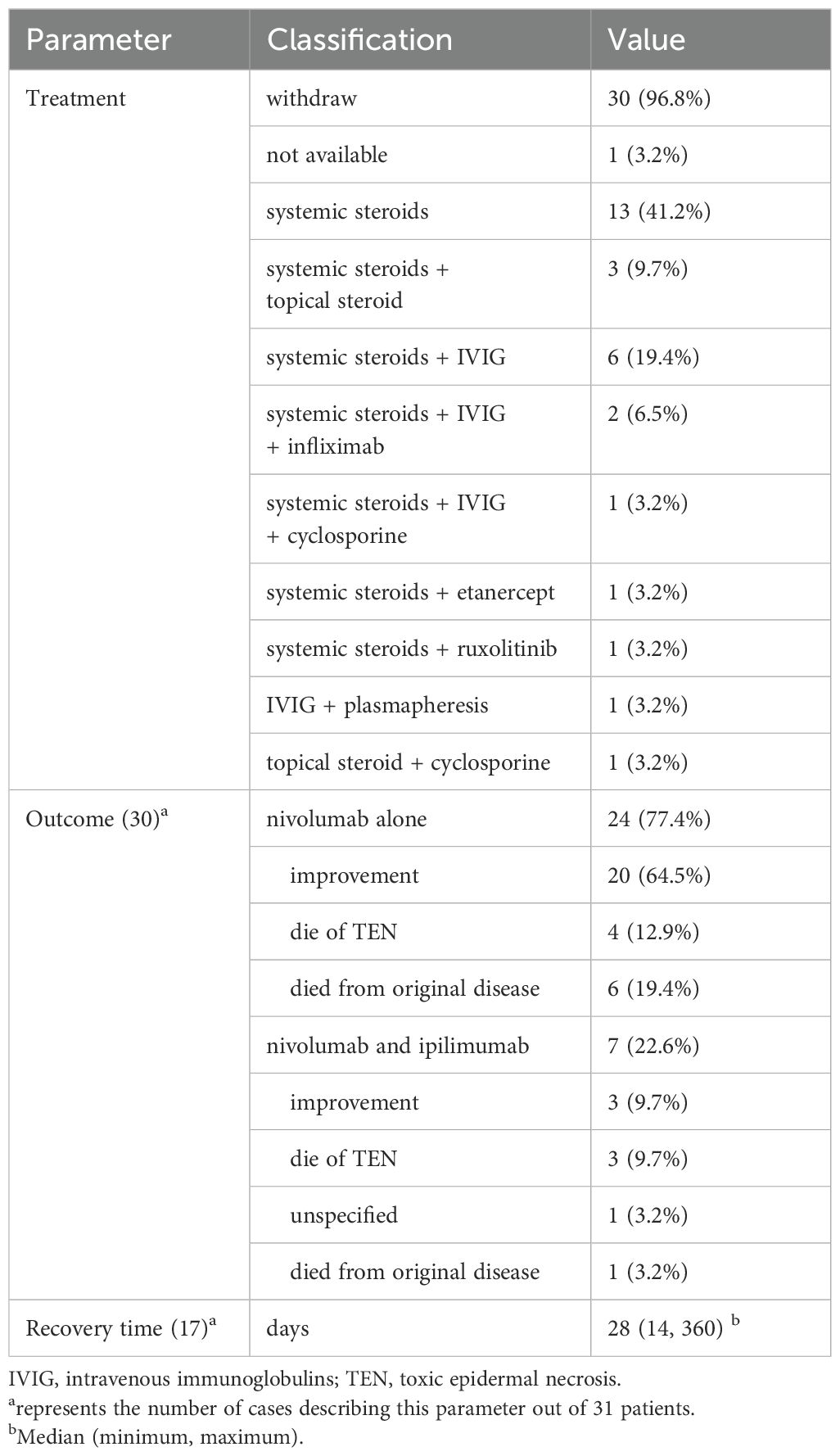
Table 3. Treatment and outcomes of 31 patients with nivolumab-induced SJS/TEN.
Post-marketing data analysis showed that the average incidence of cirAEs was about 25.1%, with a higher proportion of cirAEs in patients receiving anti-CTLA-4 treatment than anti-PD-1/PD-L1 treatment (6, 7). The incidence of cirAEs was higher when different ICIs were combined (8). The incidence of pruritus in patients treated with PD-1 inhibitors ranges from 13% to 20%, while the incidence of SJS/TEN is lower, but the mortality is higher (9). Compared with other drug-induced SJS/TEN, nivolumab induced SJS/TEN tended to have a longer incubation period, with a median time of 5.5 weeks. The different pharmacokinetics may explain the different onset time of drug-induced SJS/TEN. Nivolumab has a half-life of 25 days, and steady-state plasma concentrations are achieved at 12 weeks with biweekly dosing regimens (10). Other drugs, such as lamotrigine, have a half-life of about 23 to 37 hours, with peak blood concentrations 3 hours after administration. Therefore, the mean time of onset of lamotrigine-induced SJS/TEN was 2.8 weeks (11). An alternative explanation is that PD-1 inhibition activates T cells directed against self-antigens, leading to progressive loss of peripheral tolerance in the skin and later development of SJS/TEN (12). SJS/TEN may even occur up to 6 months after withdrawal of nivolumab (13). This is a delayed immune-related event (14). Nivolumab has an approximately 85% occupancy rate on circulating T cells for 85 days and is dose-independent (15).
The ratio of nivolumab induced SJS/TEN was about 1.4 to 1, and the incidence was higher in males than in females. There was no significant sex difference in classical drug-induced SJS/TEN (16). Considering the limited number of included cases, whether gender is related to the occurrence of SJS/TEN needs to be further verified. In addition, patients often have multiple underlying diseases that require a combination of multiple drugs. These drugs are related to SJS/TEN, such as proton pump inhibitors and allopurinol (17). However, based on the time correlation and the improvement of patients’ symptoms after discontinuation of nivolumab, the cause can be identified as nivolumab. However, whether the combination of multiple drugs increases the incidence of SJS/TEN needs further investigation.
Our findings suggest that nivolumab induced SJS/TEN is clinically distinct from that classical drug-induced SJS/TEN. Drug-induced SJS/TEN develops rashes in the first few days of rapid progression, whereas ICI-related skin outbreaks occur weeks to months earlier (18). In our study, about 55% of the cases had a rash prior to blistering and skin sloughing. Nivolumab-induced SJS/TEN is similar to classical drug-induced SJS/TEN in more than 80% of patients with mucosal involvement. Different mucosal involvement of SJS/TEN induced by nivolumab was significantly lower than that of classical SJS/TEN. However, the involvement of different mucous membranes varies, 90% of classical SJS/TEN involve the oral mucosa, 84% involve the eyes, and 60-70% involve the genitals (19, 20). Another note is that there may be a lack of mucosal involvement in patients with extensive epidermal detachment. These may be a unique feature of nivolumab induced SJS/TEN (21). Drug-induced SJS/TEN histology showed epidermal necrosis, keratinocyte apoptosis, basal vacuolar change, subepidermal bullae, subepidermal clefting, and Inflammatory cell infiltration. 1 These inflammatory cells were mainly infiltrated by lymphocytes, followed by eosinophils and neutrophils. Skin biopsies of nivolumab induced SJS/TEN were similar to classical ones. However, nivolumab induced SJS/TEN was found to have less inflammatory cell infiltration than classical SJS/TEN. Wetter et al. reported that 85% of patients had inflammatory cell infiltration, while we found that only about 54% of patients had inflammatory cell infiltration (16). Nivolumab-induced SJS/TEN needs to be distinguished from other skin diseases, such as bullous lichenoid dermatitis, bullous radiation recall dermatitis, bullous pemphigoid, and paraneoplastic pemphigus. This requires a comprehensive judgment based on different clinical manifestations and pathological findings. Immunofluorescence and circulating autoantibody testing may be critical for some patients with atypical clinical features.
The exact mechanism of nivolumab induced SJS/TEN is not fully understood. PD-1/PD-L1 is involved in maintaining the structural and functional integrity of the skin mucosa by protecting keratinocytes (22, 23). The antagonism of PD-1 leads to the imbalance of T cell homeostasis in the skin, which leads to cytotoxic reactions and inflammatory responses. T cell overactivation can synthesize and secrete a variety of effector molecules, such as perforin/granase, FAS ligand, tumor necrosis factor. These effector molecules enter the mucosa, skin and subcutaneous tissues to activate the apoptosis process, causing the apoptosis and necrosis of keratinocytes (24, 25). Anti-pd-1/PD-L1 treatment significantly upregulate the expression of PD-L1, inflammatory chemokines (such as CXCL9, CXCL10, and CXCL11), cytotoxic factors (such as PRF1 and GZMB), and pro-apoptotic molecules FASLG in lymphocyte and keratinocytes (12).
For patients diagnosed with SJS/TEN, immediate discontinuation of the offending medication is a top priority. Effective treatment should be taken as early as possible according to the severity of the lesion, especially the area of epidermolysis. In addition to supportive treatment, systemic steroids are the primary drug of concern for STS/TEN. Systemic steroids should be given orally as 1 to 2 mg·kg-1·d-1 prednisone or methylprednisolone (26, 27). Most patients can improve their skin symptoms after receiving systemic steroids. Cyclosporin, TNF-α inhibitors, and IVIG are also used as additional treatments for poor systemic steroid response. Given the long half-life of nivolumab, plasma exchange can be an effective treatment, especially in cases where other treatments are not effective or contraindicated (28). Nivolumab induced SJS/TEN patients may have water and electrolyte disturbance, severe infection, sepsis and even septic shock. Therefore, water and electrolyte balance should be maintained during treatment, and multiple organ failure should be closely monitored and prevented. The overall mortality rate for SJS/TEN was 22%, with 4.8% for SJS, 19.4% for SJS-TEN, and 14.8% for TEN (29, 30). The overall mortality rate of nivolumab -induced SJS/TEN was 22.6%, similar to that reported. It should be noted that these seven deaths were all TEN patients. This means that the mortality rate of 13 patients with TEN is as high as 53.8%. According to our findings, the mortality rate of patients during steroid treatment alone was 7.7%, while the mortality rate during steroid combination treatment was 28.6%. However, the efficacy and safety of different treatment options still need more clinical practice to prove. Previously reported risk factors for SJS/TEN mortality include elderly patients, comorbidities, hematological cancers, sepsis, pneumonia, and renal impairment (31). In these nivolumab-induced SJS/TEN deaths, the main causes of death were infection and tumor progression. Zhou et al. believed that the degree of epidermal detachment was a key prognostic factor for ICI induced SJS/TEN (30). Three patients affected at least 80% or more of the body surface area.
The limitations of the study need to be discussed. First, the patients in this article were mainly from case reports, leading to reporting bias. This leads to the possibility that the findings may not be representative of all nivolumab-induced SJS/TEN patients. Second, we used two language searches, which resulted in a limited number of cases. Third, not all clinical data are reported in every article. Despite its limitations, this study is useful in providing insights into the clinical features, diagnosis, management, and outcomes of nivolumab -induced SJS/TEN. More research is needed to confirm the findings in future studies.
With the widespread use of nivolumab in the cancer field, physicians should be aware of the serious skin adverse effects of nivolumab. When SJS/TEN is clinically suspected, patients should stop nivolumab immediately. Nivolumab-induced SJS/TEN is characterized by long latency, severe clinical symptoms and poor prognosis. Therefore, close monitoring, identification and treatment should be paid attention to during clinical use and after withdrawal.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
RL: Conceptualization, Formal Analysis, Investigation, Project administration, Resources, Software, Visualization, Writing – original draft, Writing – review & editing. HL: Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing. CW: Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. XL: Conceptualization, Data curation, Formal Analysis, Investigation, Software, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by Natural Science Foundation of Hunan Province (No. 2023JJ30847).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Paik J. Nivolumab plus relatlimab: first approval. Drugs. (2022) 82:925–31. doi: 10.1007/s40265-022-01723-1
2. Dougan M, Luoma AM, Dougan SK, Wucherpfennig KW. Understanding and treating the inflammatory adverse events of cancer immunotherapy. Cell. (2021) 184:1575–88. doi: 10.1016/j.cell.2021.02.011
3. Ramos-Casals M, Brahmer JR, Callahan MK, Flores-Chávez A, Keegan N, Khamashta MA, et al. Immune-related adverse events of checkpoint inhibitors. Nat Rev Dis Primers. (2020) 6:38. doi: 10.1038/s41572-020-0160-6
4. Charlton OA, Harris V, Phan K, Mewton E, Jackson C, Cooper A. Toxic epidermal necrolysis and steven-johnson syndrome: A comprehensive review. Adv Wound Care (New Rochelle). (2020) 9:426–39. doi: 10.1089/wound.2019.0977
5. Estrella-Alonso A, Aramburu JA, González-Ruiz MY, Cachafeiro L, Sánchez MS, Lorente JA. Toxic epidermal necrolysis: a paradigm of critical illness. Rev Bras Ter Intensiva. (2017) 29:499–508. doi: 10.5935/0103-507X.20170075
6. Wongvibulsin S, Pahalyants V, Kalinich M, Murphy W, Yu KH, Wang F, et al. Epidemiology and risk factors for the development of cutaneous toxicities in patients treated with immune-checkpoint inhibitors: A United States population-level analysis. J Am Acad Dermatol. (2022) 86:563–72. doi: 10.1016/j.jaad.2021.03.094
7. Apalla Z, Nikolaou V, Fattore D, Fabbrocini G, Freites-Martinez A, Sollena P, et al. European recommendations for management of immune checkpoint inhibitors-derived dermatologic adverse events. The EADV task force ‘Dermatology for cancer patients’ position statement. J Eur Acad Dermatol Venereol. (2022) 36:332–50. doi: 10.1111/jdv.17855
8. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. (2015) 373:23–34. doi: 10.1056/NEJMoa1504030
9. Belum VR, Benhuri B, Postow MA, Hellmann MD, Lesokhin AM, Segal NH, et al. Characterisation and management of dermatologic adverse events to agents targeting the PD-1 receptor. Eur J Cancer. (2016) 60:12–25. doi: 10.1016/j.ejca.2016.02.010
10. Centanni M, Moes DJAR, Trocóniz IF, Ciccolini J, van Hasselt JGC. Clinical pharmacokinetics and pharmacodynamics of immune checkpoint inhibitors. Clin Pharmacokinet. (2019) 58:835–57. doi: 10.1007/s40262-019-00748-2
11. Hui LLY, Loke C, Aw DCW, Tan L, Limenta LMG, Shen M, et al. Lamotrigine-induced Stevens-Johnson syndrome and toxic epidermal necrolysis in Singapore: A case series. Ann Acad Med Singap. (2021) 50:915–8. doi: 10.47102/annals-acadmedsg.2021326
12. Goldinger SM, Stieger P, Meier B, Micaletto S, Contassot E, French LE, et al. Cytotoxic cutaneous adverse drug reactions during anti-PD-1 therapy. Clin Cancer Res. (2016) 22:4023–9. doi: 10.1158/1078-0432.CCR-15-2872
13. Potts J, Lee RR, Hilliard CA. Lichenoid dermatitis preceding Stevens-Johnson syndrome in a patient treated with nivolumab. BMJ Case Rep. (2022) 15:e251233. doi: 10.1136/bcr-2022-251233
14. Couey MA, Bell RB, Patel AA, Romba MC, Crittenden MR, Curti BD, et al. Delayed immune-related events (DIRE) after discontinuation of immunotherapy: diagnostic hazard of autoimmunity at a distance. J Immunother Cancer. (2019) 7:165. doi: 10.1186/s40425-019-0645-6
15. Brahmer JR, Drake CG, Wollner I, Powderly JD, Picus J, Sharfman WH, et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol. (2010) 28:3167–75. doi: 10.1200/JCO.2009.26.7609
16. Wetter DA, Camilleri MJ. Clinical, etiologic, and histopathologic features of Stevens-Johnson syndrome during an 8-year period at Mayo Clinic. Mayo Clin Proc. (2010) 85:131–8. doi: 10.4065/mcp.2009.0379
17. Frey N, Bodmer M, Bircher A, Jick SS, Meier CR, Spoendlin J. Stevens-johnson syndrome and toxic epidermal necrolysis in association with commonly prescribed drugs in outpatient care other than anti-epileptic drugs and antibiotics: A population-based case-control study. Drug Saf. (2019) 42:55–66. doi: 10.1007/s40264-018-0711-x
18. Dodiuk-Gad RP, Chung WH, Valeyrie-Allanore L, Shear NH. Stevens-johnson syndrome and toxic epidermal necrolysis: an update. Am J Clin Dermatol. (2015) 16:475–93. doi: 10.1007/s40257-015-0158-0
19. Bequignon E, Duong TA, Sbidian E, Valeyrie-Allanore L, Ingen-Housz-Oro S, Chatelin V, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: ear, nose, and throat description at acute stage and after remission. JAMA Dermatol. (2015) 151:302–7. doi: 10.1001/jamadermatol.2014.4844
20. Gulanikar A, Abrol A, Sagar S. Study of genital manifestations of Stevens Johnson Syndrome/Toxic Epidermal Necrolysis. Indian J Sex Transm Dis AIDS. (2022) 43:39–42. doi: 10.4103/ijstd.IJSTD_61_19
21. Koshizuka K, Sakurai D, Sunagane M, Mita Y, Hamasaki S, Suzuki T, et al. Toxic epidermal necrolysis associated with nivolumab treatment for head and neck cancer. Clin Case Rep. (2020) 9:848–52. doi: 10.1002/ccr3.3695
22. Alexandris D, Alevizopoulos N, Gakiopoulou H, Stavrinou N, Vourlakou C. Cutaneous stevens johnson - toxic epidermal necrolysis immunotherapy related toxicities in lung cancer patients. J Oncol Pharm Pract. (2022) 28:1276–82. doi: 10.1177/10781552221074623
23. Saw S, Lee HY, Ng QS. Pembrolizumab-induced Stevens-Johnson syndrome in non-melanoma patients. Eur J Cancer. (2017) 81:237–9. doi: 10.1016/j.ejca.2017.03.026
24. Dasanu CA. Late-onset Stevens-Johnson syndrome due to nivolumab use for hepatocellular carcinoma. J Oncol Pharm Pract. (2019) 25:2052–5. doi: 10.1177/1078155219830166
25. Noe MH, Micheletti RG. Diagnosis and management of Stevens-Johnson syndrome/toxic epidermal necrolysis. Clin Dermatol. (2020) 38:607–12. doi: 10.1016/j.clindermatol.2020.06.016
26. Thompson JA, Schneider BJ, Brahmer J, Achufusi A, Armand P, Berkenstock MK, et al. Management of immunotherapy-related toxicities, version 1.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2022) 20:387–405. doi: 10.6004/jnccn.2022.0020
27. Kuo AM, Markova A. High grade dermatologic adverse events associated with immune checkpoint blockade for cancer. Front Med (Lausanne). (2022) 9:898790. doi: 10.3389/fmed.2022.898790
28. Watanabe Y, Yamaguchi Y, Takamura N, Takahashi Y, Aihara M. Toxic epidermal necrolysis accompanied by several immune-related adverse events developed after discontinuation of nivolumab. Eur J Cancer. (2020) 131:1–4. doi: 10.1016/j.ejca.2020.02.044
29. Creamer D, Walsh SA, Dziewulski P, Exton LS, Lee HY, Dart JKG, et al. UK guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. J Plast Reconstr Aesthet Surg. (2016) 69:e119–53. doi: 10.1016/j.bjps.2016.01.034
30. Hsu DY, Brieva J, Silverberg NB, Silverberg JI. Morbidity and mortality of stevens-johnson syndrome and toxic epidermal necrolysis in United States adults. J Invest Dermatol. (2016) 136:1387–97. doi: 10.1016/j.jid.2016.03.023
Keywords: nivolumab, toxic epidermal necrolysis, Stevens-Johnson syndrome, cutaneous adverse reactions, immune-related adverse events
Citation: Li R, Lei H, Wang C and Liu X (2025) Clinical features of nivolumab-induced Stevens-Johnson syndrome/toxic epidermal necrolysis: retrospective analysis based on case reports. Front. Immunol. 16:1563100. doi: 10.3389/fimmu.2025.1563100
Received: 19 January 2025; Accepted: 05 March 2025;
Published: 18 March 2025.
Edited by:
Cleber Machado-Souza, Pelé Pequeno Príncipe Research Institute, BrazilReviewed by:
Smrity Sahu, Post Graduate Institute of Medical Education and Research (PGIMER), IndiaCopyright © 2025 Li, Lei, Wang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiang Liu, eHkzeXkyMDIxMTJAMTI2LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.