
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Immunol., 17 March 2025
Sec. Viral Immunology
Volume 16 - 2025 | https://doi.org/10.3389/fimmu.2025.1556731
This article is part of the Research TopicExploring Antiviral Immune Responses and Therapeutic Strategies Against Human CoronavirusesView all 9 articles
 Mario Framil1,2*
Mario Framil1,2* Lydia García-Serrano2
Lydia García-Serrano2 Francisco Morandeira2
Francisco Morandeira2 Juan Francisco Luchoro1
Juan Francisco Luchoro1 Arnau Antolí3,4
Arnau Antolí3,4 Jose Luis Gomez-Vazquez3Àngels Sierra-Fortuny3
Jose Luis Gomez-Vazquez3Àngels Sierra-Fortuny3 Xavier Solanich3,4
Xavier Solanich3,4During the COVID-19 pandemic, approximately 15% of patients with severe COVID-19 pneumonia were reported to have neutralizing anti-type I interferon (IFN) autoantibodies, which impaired the antiviral response and led to a poorer prognosis. However, the physiological impact of non-neutralizing autoantibodies remains unclear. In our cohort of COVID-19 patients admitted to intensive care, the presence of non-neutralizing anti-type I IFN autoantibodies increased the risk of thrombotic complications, likely via a cytokine carrier mechanism, prolonging the half-life of cytokines and dysregulating vascular endothelial function. Previous studies have associated non-neutralizing anti-type I IFN autoantibodies with an increased risk of cardiovascular complications in autoimmune diseases like systemic lupus erythematosus, but their relevance in infectious diseases remains uncertain. Stratifying anti-type I IFN autoantibodies based on their neutralizing capacity may have clinical significance not only in terms of susceptibility to infectious diseases but also in predicting cardiovascular and thrombotic events.
The COVID-19 pandemic heightened interest in anti-cytokine autoantibodies, particularly anti-type I IFN autoantibodies. Bastard et al. (1) revealed high titers of neutralizing autoantibodies against type I IFNs in up to 10% of severe COVID-19 patients. These autoantibodies compromised antiviral responses and increased the risk of severe COVID-19, especially in males over 65 years old, with a prevalence of approximately 20% in patients who died (2). Subsequent global studies confirmed these findings, emphasizing the role of neutralizing autoantibodies against type I IFNs as a significant risk factor for severe COVID-19. Anti-IFN neutralizing autoantibodies have since been linked to severe outcomes in other diseases, including severe influenza pneumonia, neurological complications associated with West Nile virus, and adverse responses to the yellow fever vaccine (2).
Most studies have focused on how neutralizing autoantibodies impair IFN signaling. However, non-neutralizing autoantibodies, which make up over 50% of detected antibodies (2, 3), have also been observed to play physiological roles. One of these roles is the stabilization of cytokines, such as IL-6, by preventing their degradation and extending their half-lives in vivo, likely through the formation of cytokine-antibody complexes (4). These complexes may subsequently recycle into the bloodstream, contributing to a dynamic equilibrium between free cytokines and those bound to antibodies. This recycling process is mediated by neonatal Fc receptors, predominantly expressed on vascular endothelial and myeloid cells, thereby ensuring the sustained presence of cytokines in circulation (5).
A similar process has been observed in systemic autoimmune diseases, such as systemic lupus erythematosus (SLE), where anti-type I IFN autoantibodies exhibit distinct roles based on their neutralizing capacity (6). Neutralizing anti-cytokine autoantibodies have been associated with decreased interferon-pathway activity and reduced disease activity in SLE patients. In contrast, non-neutralizing autoantibodies, particularly IFN-α2, have been linked to elevated cytokine concentrations in peripheral blood, which correlates with an increased risk of cardiovascular and respiratory complications (7). Given these observations, we aimed to evaluate the clinical outcomes in life-threatening COVID-19 patients based on the presence of non-neutralizing type I IFN autoantibodies.
Study Design and Patients: This retrospective study involved COVID-19 patients admitted to the Intensive Care Unit (ICU) of Hospital Universitari de Bellvitge from March 2020 to March 2021, with confirmed SARS-CoV-2 infection. Data were obtained from routine clinical practice and anonymized. Personal and clinical information was collected in compliance with the Spanish Data Protection Act (Ley Orgánica 3/2018, December 5, on Personal Data Protection). Informed consent was waived due to the study’s retrospective nature and the mandatory isolation measures during in-hospital care. The protocol was approved by the Ethics Committee of Hospital Universitari de Bellvitge (Barcelona, Spain; approval number PR40/21).
Clinical and Laboratory Variables: Demographic, clinical, and evolutive data during hospitalization were recorded, and laboratory variables were collected upon ICU admission. Detailed descriptions of these clinical variables can be found in the original study by Solanich et al. (3).
Autoantibodies Against Type I IFNs: Autoantibodies against IFN-α2 and IFN-ω were analyzed using an ELISA technique as described in Solanich et al. (3). In brief, NUNC MaxiSorp™ 96-well ELISA plates (Thermo Fisher Scientific) were coated with recombinant human IFN-α2 or IFN-ω (1 mg/L in 100 μL coating buffer) and incubated overnight at 4°C. After three PBS washes, plates were blocked with PBS-5% nonfat milk for 1 h at room temperature with continuous shaking at 600 rpm, washed with PBS-Tween 0.005%, and incubated with 100 μL of 1:50 diluted serum samples (patients/controls) in HPE buffer (Sanquin) for 2 h with shaking at room temperature. After washing, Fc-specific HRP-conjugated goat anti-human IgG (Nordic-MUbio, 2 mg/L) was added and incubated for 1 h. Following washes, TMB substrate was added for 10 min, and the reaction was stopped with 0.18 M H2SO4. Optical density at 450 nm was measured. Samples were considered positive if exceeding the mean value plus two standard deviations of a non-COVID-19 control group (3).
Neutralizing Autoantibodies Against Type I IFNs: The neutralizing ability of these autoantibodies at high concentrations of IFN-α2 and IFN-ω (10 ng/mL) was assessed using a functional in vitro Dual-Luciferase reporter assay, as described in Solanich et al. (3). In brief, HEK293T cells were transfected with firefly luciferase plasmids under human ISRE promoters (pGL4.45) and a constitutively expressing Renilla luciferase plasmid (pRL-SV40) for normalization. Transfection was performed with X-tremeGene 9 (Millipore-Sigma) for 36 h. Cells were then incubated in Dulbecco’s modified Eagle medium (DMEM, Thermo Fisher Scientific) with 10% healthy control or patient serum/plasma, either unstimulated or stimulated with IFN-α2 or IFN-ω (10 ng/mL) for 16 h at 37°C. Each sample was tested once. Luciferase levels were measured using Dual-Glo reagent (Promega Corp., Madison, WI, USA), according to the manufacturer’s protocol. Firefly luciferase values were normalized against Renilla luciferase values (3).
Statistical Analysis: Data are presented as median with interquartile range (IQR) for continuous variables, and as frequency rates and percentages for categorical variables. Comparisons for continuous variables were made using the Mann-Whitney U test, while comparisons for categorical variables were assessed using the chi-square test or Fisher’s exact test, as appropriate. Odds Ratios (OR) with 95% confidence intervals (CI) were calculated using logistic regression models or contingency tables, depending on the variable distribution. All tests were conducted with 95% confidence intervals and a significance level of 5%.
Serum samples from 275 patients were tested for autoantibodies against type I IFNs (IFN-α2 and IFN-ω) using ELISA. Autoantibodies were detected in 49 patients (17.8%). Among them, 23 (46.9%) had non-neutralizing autoantibodies. Within this group, 5 patients (21.7%) were positive for IFN-α2, 7 (30.4%) for IFN-ω, and 11 (47.8%) for both interferons. Male gender was more prevalent among patients with non-neutralizing autoantibodies compared to those without them (91.3% vs. 75.4%; p = 0.010). No significant difference in median age was found between groups (61 years, IQR 55–67 vs. 64 years, IQR 57–71; p = 0.112) (Table 1).
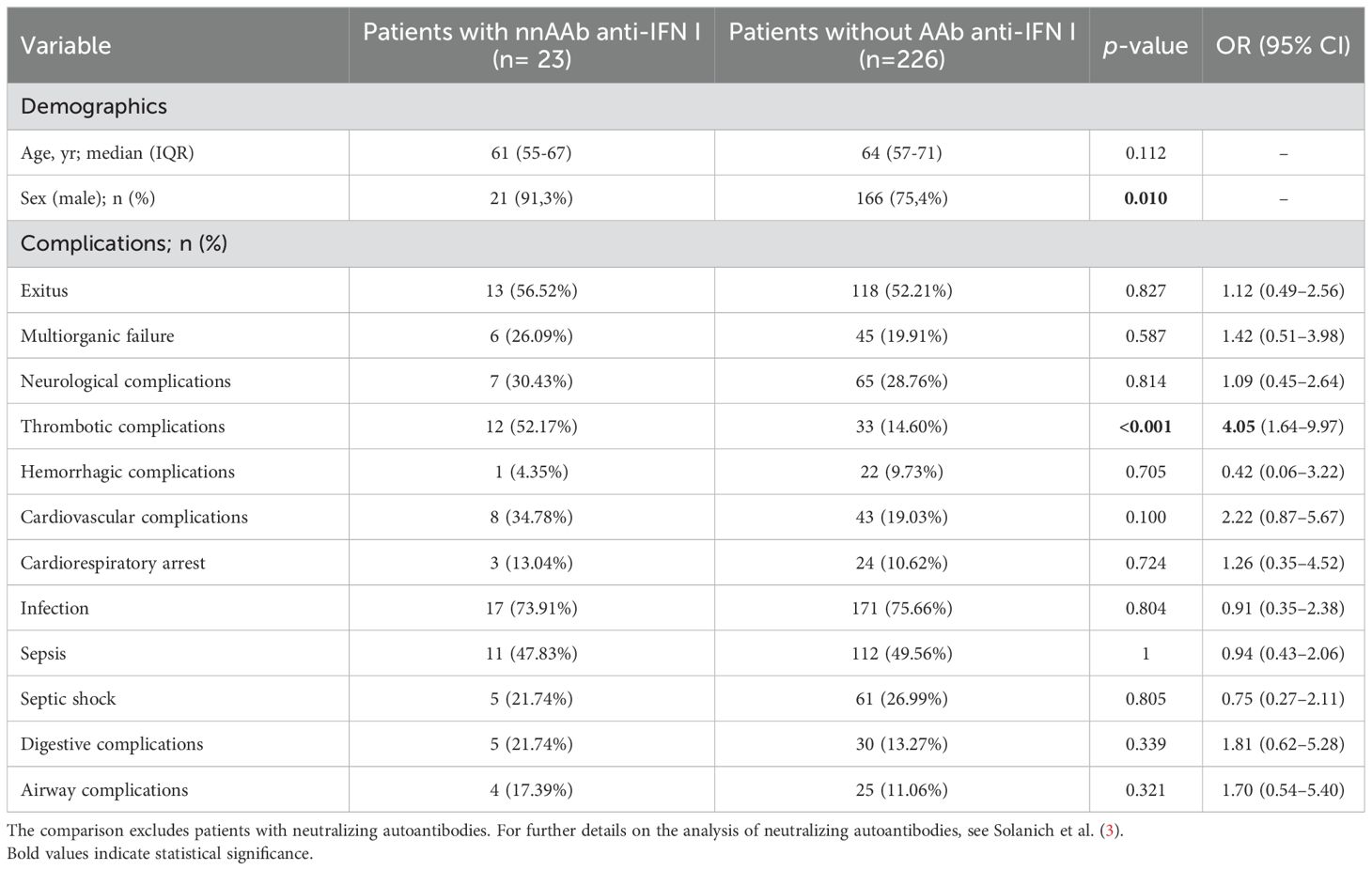
Table 1. Main demographics and clinical complications of severe COVID-19 patients with non-neutralizing anti-type I IFN autoantibodies compared to patients without anti-type I IFN autoantibodies.
Interestingly, the presence of non-neutralizing autoantibodies against type I IFNs was significantly associated with thrombotic complications compared to their absence (12 [52.2%] vs. 33 [14.6%]; p < 0.001) (Table 1), having four times higher odds of developing thrombotic complications (OR 4.054 [95% CI 1.638-9.972]) (Figure 1). Additionally, there was also a higher tendency of cardiovascular complications (8 [34.8%] vs. 43 [18.8%]; p = 0.098), especially among fatal cases (6 [46.2%] vs. 26 [21.7%]; p = 0.081). No other clinical complications did reach statistical significance.
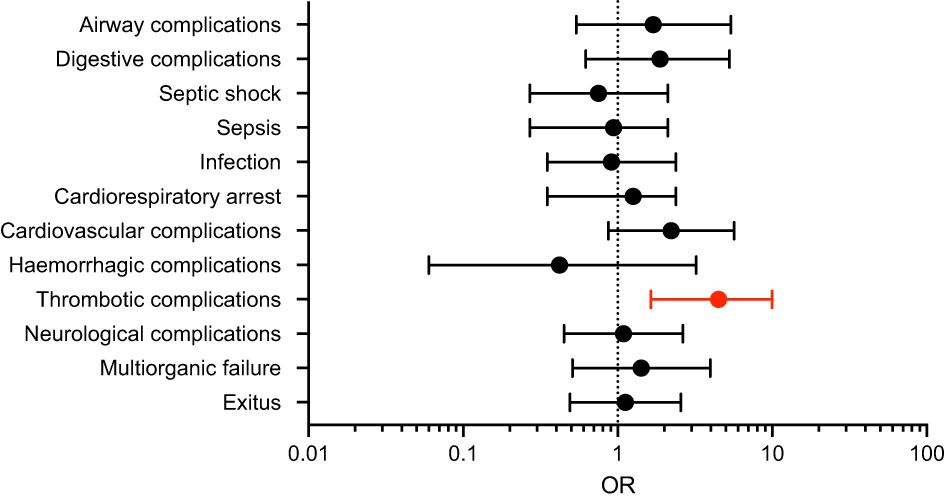
Figure 1. Odds of complications in severe COVID-19 patients with non-neutralizing anti-type I IFN autoantibodies. Forest plot showing the Odds Ratios (OR) with 95% confidence intervals (CI) for different complications. The dotted line represents an OR of 1 (no association). Thrombotic complications show significantly higher odds (highlighted in red). Error bars represent confidence intervals.
Our study underscores the significant association between non-neutralizing autoantibodies against type I interferons and an increased risk of thrombotic complications in critically ill COVID-19 patients. The role of non-neutralizing autoantibodies remains unclear, particularly regarding their physiological significance or potential impact on disease progression.
Previous studies have reported the presence of anti-type I interferon autoantibodies in approximately 10% of patients with SLE and primary Sjögren’s syndrome (6, 7). In these cohorts, patients with neutralizing autoantibodies experienced better clinical outcomes, showing less severity and fewer relapses compared to those without autoantibodies. Notably, patients with non-neutralizing antibodies exhibited higher levels of IFN-α2 than those without, presenting clinical symptoms as severe or even more pronounced. Furthermore, this group showed a higher percentage of cardiovascular and respiratory complications.
Moreover, type I interferons play a crucial role in vascular endothelial homeostasis by maintaining a balance between procoagulant and fibrinolytic factors. Sustained elevation of type I IFN levels in the vascular endothelium can disrupt this balance, leading to a hypercoagulable state (8, 9). This dysregulation has been linked to endothelial dysfunction and an increased risk of thrombosis, with prolonged exposure to type I interferons contributing to microangiopathy and impaired endothelial cell functions (8,9). In our cohort, the presence of non-neutralizing autoantibodies was significantly associated with a high incidence of thrombotic complications. This may be due to non-neutralizing autoantibodies extending cytokine half-life in circulation, further disrupting endothelial homeostasis.
Understanding the mechanisms underlying the association between non-neutralizing autoantibodies and thrombotic complications could significantly enhance outcomes in high-risk patients, not only in COVID-19 but also in other infectious diseases driven by anti-type I interferon autoantibodies, as well as in systemic autoimmune diseases. Further research is needed to validate these findings and explore whether similar associations are observed in other conditions, helping to clarify the role of non-neutralizing autoantibodies in disease progression and their potential as therapeutic targets.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Ethics Committee of the Hospital Universitari de Bellvitge (Barcelona, Spain; approval number PR40/21). The studies were conducted in accordance with the local legislation and institutional requirements. The human samples used in this study were acquired from a by- product of routine care or industry. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
MF: Conceptualization, Writing – original draft, Writing – review & editing. LG-S: Conceptualization, Writing – review & editing. FM: Writing – review & editing. JL: Writing – review & editing. AA: Writing – review & editing. JG-V: Writing – review & editing. ÀS-F: Writing – review & editing. XS: Conceptualization, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that Generative AI was used in the creation of this manuscript. This manuscript was revised for clarity using AI-assisted tools. The author assumes full responsibility for its final content.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bastard P, Rosen LB, Zhang Q, Michailidis E, Hoffmann HH, Zhang Y, et al. Autoantibodies against type I IFNs in patients with life-threatening COVID-19. Science. (2020) 370:eabd4585. doi: 10.1126/science.abd4585
2. Bastard P, Gervais A, Le Voyer T, Philippot Q, Cobat A, Rosain J, et al. Human autoantibodies neutralizing type I IFNs: From 1981 to 2023. Immunol Rev. (2024) 322:98–112. doi: 10.1111/imr.13304
3. Solanich X, Rigo-Bonnin R, Gumucio VD, Bastard P, Rosain J, Philippot Q, et al. Pre-existing autoantibodies neutralizing high concentrations of type I interferons in almost 10% of COVID-19 patients admitted to intensive care in Barcelona. J Clin Immunol. (2021) 41:1733–44. doi: 10.1007/s10875-021-01136-x
4. Kärner J, Pihlap M, Ranki A, Krohn K, Trebusak Podkrajsek K, Bratanic N, et al. IL-6-specific autoantibodies among APECED and thymoma patients. Immun Inflammation Dis. (2016) 4:235–43. doi: 10.1002/iid3.109
5. Shulgin B, Helmlinger G, Kosinsky Y. A generic mechanism for enhanced cytokine signaling via cytokine-neutralizing antibodies. PloS One. (2016) 11:e0149154. doi: 10.1371/journal.pone.0149154
6. Gupta S, Tatouli IP, Rosen LB, Hasni S, Alevizos I, Manna ZG, et al. Distinct functions of autoantibodies against interferon in systemic lupus erythematosus: A comprehensive analysis of anticytokine autoantibodies in common rheumatic diseases. Arthritis Rheumatol. (2016) 68:1677–87. doi: 10.1002/art.39607
7. Bradford HF, Haljasmägi L, Menon M, McDonnell TCR, Särekannu K, Vanker M, et al. Inactive disease in patients with lupus is linked to autoantibodies to type I interferons that normalize blood IFNα and B cell subsets. Cell Rep Med. (2023) 4:100894. doi: 10.1016/j.xcrm.2022.100894
8. Kavanagh D, McGlasson S, Jury A, Williams J, Scolding N, Bellamy C, et al. Type I interferon causes thrombotic microangiopathy by a dose-dependent toxic effect on the microvasculature. Blood. (2016) 128:2824–33. doi: 10.1182/blood-2016-05-715987
Keywords: non-neutralizing autoantibodies, type I interferon, COVID-19, thrombotic complications, endothelial dysfunction, ICU patients
Citation: Framil M, García-Serrano L, Morandeira F, Luchoro JF, Antolí A, Gomez-Vazquez JL, Sierra-Fortuny À and Solanich X (2025) Non-neutralizing anti-type I interferon autoantibodies could increase thrombotic risk in critical COVID-19 patients. Front. Immunol. 16:1556731. doi: 10.3389/fimmu.2025.1556731
Received: 07 January 2025; Accepted: 26 February 2025;
Published: 17 March 2025.
Edited by:
Pengfei Wang, Fudan University, ChinaReviewed by:
Kai Kisand, University of Tartu, EstoniaCopyright © 2025 Framil, García-Serrano, Morandeira, Luchoro, Antolí, Gomez-Vazquez, Sierra-Fortuny and Solanich. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mario Framil, ZnJhbWlsQGNsaW5pYy5jYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.