
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Immunol., 19 February 2025
Sec. Inflammation
Volume 16 - 2025 | https://doi.org/10.3389/fimmu.2025.1551122
This article is part of the Research TopicRole of bioinformatics and AI in understanding inflammation and immune microenvironment dynamicsView all 8 articles
 Zhe Peng
Zhe Peng Gang Zhou*
Gang Zhou*Since the emergence of COVID-19 in December 2019, the novel SARS-CoV-2 virus has primarily affected adults, with children representing a smaller proportion of cases. However, the escalation of the pandemic has led to a notable increase in pediatric cases of Multisystem Inflammatory Syndrome in Children (MIS-C). The pathogenesis of MIS-C is largely attributed to immune-mediated mechanisms, such as cytokine storms and endothelial damage, following SARS-CoV-2 infection. In this review, we comprehensively describe MIS-C, including its definitions as proposed by the CDC, WHO, and RCPCH, which emphasize persistent fever, excessive inflammatory responses, and multi-organ involvement. Additionally, we summarize current treatment approaches, prioritizing immunotherapy with intravenous immunoglobulin and corticosteroids, along with anticoagulation therapy, and monoclonal antibodies in severe cases.
Since the advent of SARS-CoV-2 in December 2019, COVID-19 has escalated swiftly, catalyzing global waves of infection and mortality. Epidemiological investigations indicate a mere 1.7% of these cases involve children (1), attributed primarily to their reduced exposure, less severe symptoms, and lack of comprehensive testing. Typically, pediatric infections manifest with respiratory symptoms and are associated with positive prognoses (2). Nonetheless, a subset of severe pediatric presentations mirroring Kawasaki disease (KD) has surfaced, marked by symptoms such as fever, gastrointestinal distress, cardiac complications, shock, multi-organ dysfunction, and heightened inflammatory markers. Initially identified in the UK during April 2020, analogous cases have subsequently been reported across Europe, the US, and other areas (3–5). Of these severe presentations, 81% demonstrate positivity for SARS-CoV-2 IgG antibodies, whereas 37% show detectable viral nucleic acids (6). Emerging evidence suggests that this syndrome, likely driven by immune responses, follows an encounter with SARS-CoV-2. In response, the World Health Organization (WHO) recognized this condition in May 2020, naming it Multisystem Inflammatory Syndrome in Children (MIS-C) (7). This review delves into the definition, pathogenesis, clinical manifestations, diagnostic criteria, therapeutic options, and prognosis of MIS-C, providing a comprehensive framework for clinicians to manage this syndrome effectively.
At present, three distinct definitions of MIS-C have been formulated by the US Centers for Disease Control and Prevention (CDC), the WHO, and the UK’s Royal College of Paediatrics and Child Health (RCPCH). Despite a lack of complete alignment among these definitions, they share several common features: fever, an intense inflammatory response, involvement of multiple organs, either direct exposure to COVID-19 or a prior infection with SARS-CoV-2, and ruling out other infectious etiologies. These criteria are designed to identify children who either fully or partially satisfy the diagnostic requirements for KD (8).
(1) Age of onset: All age groups; (2) Clinical features: Persistent fever >38.5°C, accompanied by the dysfunction of one or more organ systems (e.g., gastrointestinal, respiratory, cardiac, renal, neurological) or instances of shock; (3) Laboratory results: Increased levels of C-reactive protein (CRP) and ESR, accompanied by neutrophilia; (4) Epidemiological context: Positive reverse transcription PCR for SARS-CoV-2 (9).
(1) Age of onset: <19 years; (2) Clinical signs: Persistent fever for ≥3 days, plus at least two of the following symptoms: rash or bilateral non-purulent conjunctivitis, mucocutaneous inflammation, hypotension or shock, cardiac dysfunction, diarrhea, vomiting, or abdominal pain; (3) Laboratory indicators: Elevated ESR, CRP, PCT, coagulation abnormalities, and evidence of cardiac injury; (4) Epidemiological context: History of SARS-CoV-2 infection or exposure to COVID-19 (10).
(1) Age of onset: <21 years; (2) Clinical features: Fever >38.0°C for ≥24 hours or subjective fever for ≥24 hours, alongside dysfunction in ≥2 organ systems (gastrointestinal, respiratory, cardiovascular, renal, hematological, dermatological, or neurological); (3) Laboratory findings: Including, but not limited to, one or more of the following: elevated CRP, procalcitonin, ESR, ferritin, interleukin-6, neutrophilia, lymphopenia, and hypoalbuminemia; (4) SARS-CoV-2 infection/exposure within 4 weeks (10). A Boston Children’s Hospital study (11) revealed clinical heterogeneity under the 2020 MIS-C definition, risking misclassification of severe COVID-19 as MIS-C, particularly for cases with respiratory criteria (5, 12, 13). The updated CDC criteria exclude fever duration, renal, neurological, and respiratory involvement (5), improving specificity and aligning more closely with WHO standards (14) (Table 1).
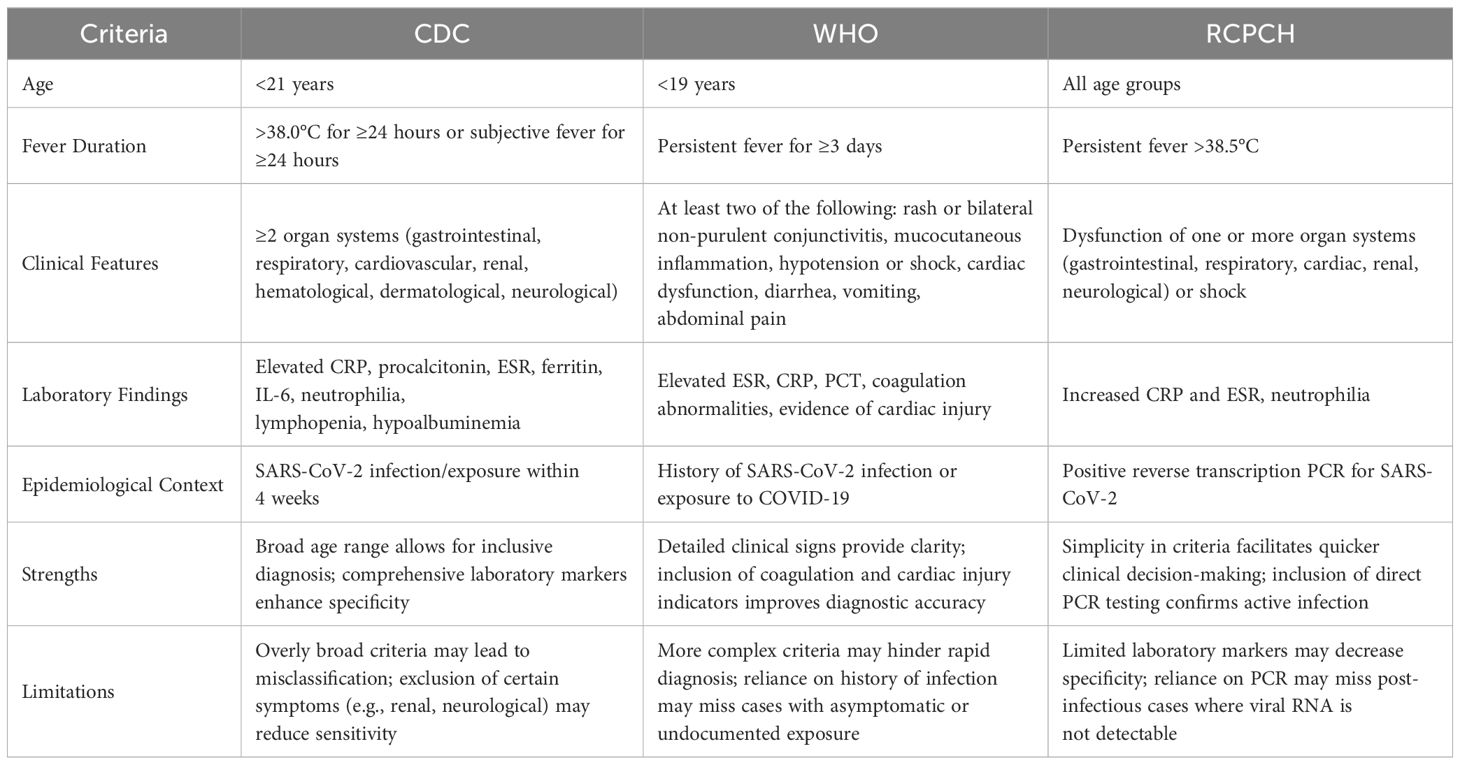
Table 1. Comparative analysis of MIS-C diagnostic criteria by CDC, WHO, and RCPCH.
The clinical presentation of MIS-C exhibit significant variability and lack specificity, with several overlapping features observed in KD. Common symptoms include persistent fever, mucocutaneous involvement (e.g., swelling of the hands and feet, conjunctivitis, cracked lips, rash), lymphadenitis, and cardiac dysfunction. Multiple organ systems are typically affected, particularly the cardiovascular and gastrointestinal systems, along with the circulatory, respiratory, and neurological systems (15, 16). Recent studies have expanded the symptom spectrum of MIS-C to include acute neurological deficits and severe dermatological reactions (17), renal involvement and hepatic dysfunction (18), and cervical inflammation (19), underscoring its heterogeneous nature.
Based on the predominant clinical manifestations, MIS-C can be categorized into three types: (I) Predominantly persistent fever and gastrointestinal symptoms, occurring in 80%–99.4% and 85.6%–90% of cases respectively, often presenting as abdominal pain, vomiting, or diarrhea. Severe cases may mimic acute appendicitis or peritonitis, occasionally leading to unnecessary surgeries (6, 20, 21). Additional complications include acute pancreatitis, hyperglycemia, acidosis, venous thrombosis, and electrolyte imbalances, likely resulting from immune dysregulation (22, 23) and ACE receptor distribution in the gastrointestinal tract (24); (II) Predominantly shock and left ventricular dysfunction, with incidence rates of 74% and 70%, respectively (6), which may require vasoactive agents or extracorporeal membrane oxygenation (ECMO) (25) due to myocardial damage and cytokine storms (26); (III) KD-like feature, including conjunctivitis, rash, and lymphadenopathy (17%) (6, 20), alongside potential acute kidney injury, liver damage, and neurological symptoms, though respiratory symptoms remain rare (15, 27).
Differentiating MIS-C from conditions with overlapping features, such as severe COVID-19 and KD, is crucial for appropriate management. Inflammatory factors are pivotal in inflammatory diseases progression and significantly influence the efficacy of therapies (28–31). MIS-C typically occurs in a post-infectious context, weeks after initial SARS-CoV-2 infection, and is characterized by elevated inflammatory markers like IL-6 and IL-18 (32). In contrast, severe COVID-19 presents predominantly with acute respiratory symptoms and viral pneumonia. Compared to KD, MIS-C patients are generally older, exhibit more pronounced gastrointestinal symptoms, and have a higher incidence of cardiac dysfunction and shock (33). Additionally, laboratory findings in MIS-C often show elevated markers of inflammation and cardiac injury, which can aid in distinguishing it from KD (34) (Figure 1).
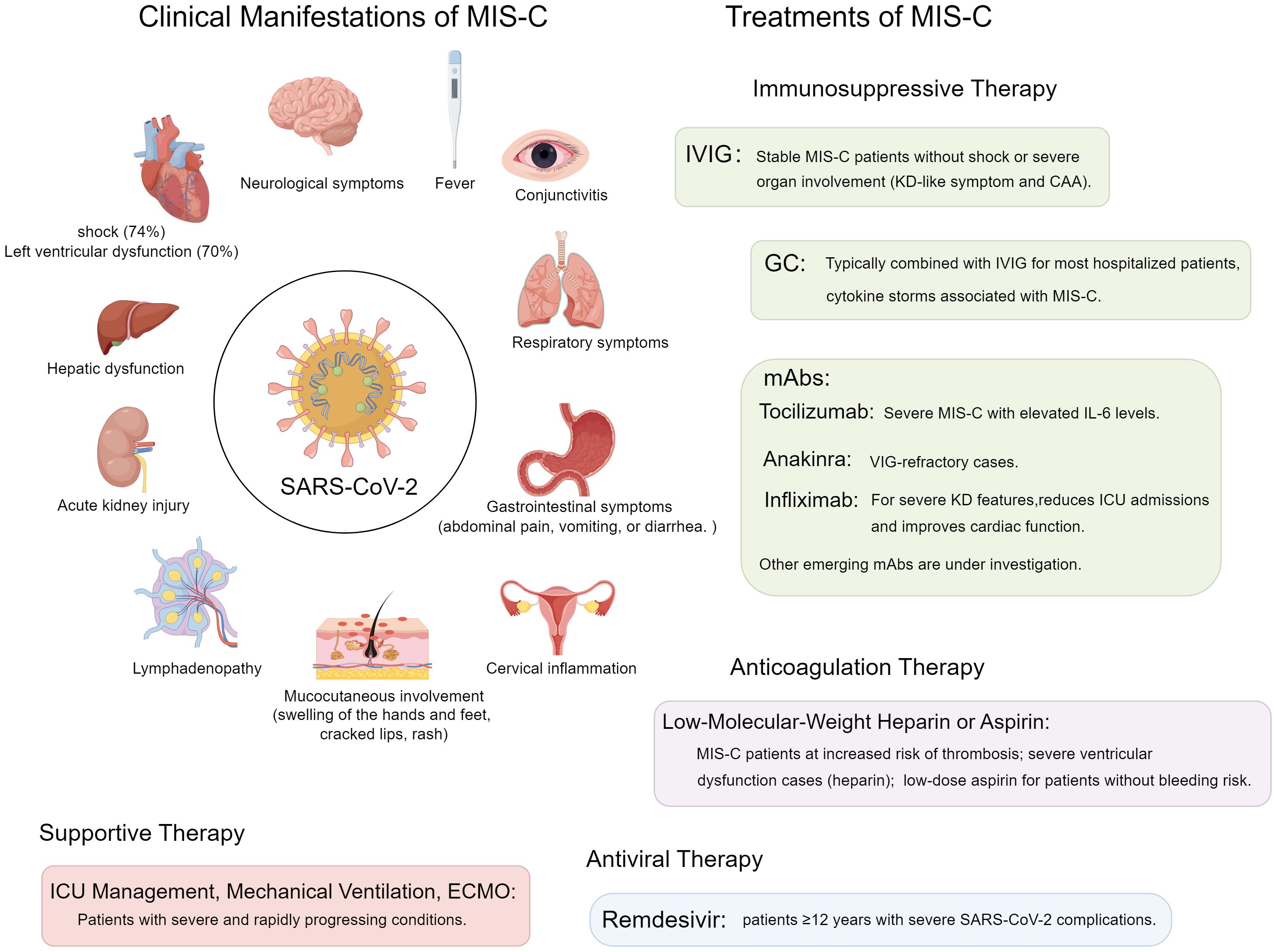
Figure 1. Clinical manifestations and treatment strategies for MIS-C.
The pathophysiological mechanisms of MIS-C remain inadequately understood. It may arise from direct damage induced by SARS-CoV-2, an exaggerated immune response in genetically predisposed individuals (35). SARS-CoV-2 infection can provoke endothelial damage, leading to multi-organ dysfunction (36). MIS-C onset occurs 4–5 weeks post-infection, with antibodies and viral nucleic acids absent, indicating an adaptive immune response rather than direct viral invasion (28) (15). Multiple studies (15, 37–39) demonstrate that severe immune dysregulation induces cytokine storms, causing systemic inflammation and organ failure (30–32). Alunno et al. (40) attribute MIS-C to massive inflammatory mediator release and cytokine storm activation, while Rowley et al. (39) link cytokine storms to endothelial dysfunction. The efficacy of anti-inflammatory and immunomodulatory treatments over antiviral treatment underscore excessive immune activation as the primary mechanism (40).
Although a definitive causal relationship between MIS-C and SARS-CoV-2 remains unconfirmed, the occurrence of MIS-C during COVID-19 outbreaks and its temporal correlation with SARS-CoV-2 infection suggest a strong association. The MIS-C inflammatory response resembles severe COVID-19 in adults (41–43), characterized by dysregulated cell-mediated or humoral immunity. MIS-C patients have neutralizing antibodies against SARS-CoV-2 (37), correlating with activation of IL-18, IL-16, myeloid chemotaxis, lymphocytes, monocytes, and NK cells. Autoantibodies targeting endothelial, gastrointestinal, and immune cells in MIS-C patients suggest a role in pathogenesis. In addition, SARS-CoV-2 spike protein may act as a superantigen (44), intensifying immune responses and contributing to multi-organ damage. Moreover, genetic factors may also be involved. Immunogenomic studies have identified genetic variants increasing MIS-C susceptibility, including mutations in viral recognition and antigen presentation pathways (45), and polymorphisms in immune response genes, such as those encoding cytokines and their receptors, which heighten MIS-C risk (46).
All children with MIS-C test positive for serum COVID-19-specific immunoglobulin (Ig) G and IgM. In some cases, nasopharyngeal samples also test positive for COVID-19 nucleic acid (15, 47–49).
In conjunction with the diagnostic criteria and clinical data for MIS-C, patients must meet at least three of the following criteria: (1) Complete blood count abnormalities, including mild to moderate anemia, decreased absolute lymphocyte count, and thrombocytosis; (2) Elevated inflammatory markers such as CRP, SF, ESR, and PCT; (3) Coagulation disturbances, including prolonged APTT/PT and increased fibrinogen; (4) Inflammatory markers; (5) Increased IL-6, IL-8, and TNF levels (47).
Electrocardiogram findings include ST-segment depression, flattened T waves, and arrhythmias. Echocardiogram results show a reduced ejection fraction, ventricular enlargement, pericardial effusion, and coronary abnormalities; however, the severe coronary changes characteristic of KD are uncommon. Compared to KD, diminished systolic and diastolic function is observed (50). Cardiac MRI reveals hyperemia and edema without evidence of necrosis or fibrosis. Chest CT scans indicate pulmonary alterations such as decreased translucency, ground-glass opacities, or pleural effusion in approximately 50% of cases, with some patients presenting without any noticeable abnormalities (15, 49, 51). Abdominal imaging frequently detects hepatosplenomegaly, ascites or pelvic effusion, appendiceal or gallbladder enlargement, enteritis, mesenteric lymphadenitis, and thickening of the intestinal wall in 77% of cases (27). Neurological imaging often shows high-intensity T2/FLAIR signals, suggesting possible inflammatory edema (52). Echocardiography is a primary diagnostic tool for MIS-C, assessing cardiac function and coronary abnormalities with good sensitivity, though limited for subtle myocardial changes. Cardiac MRI offers higher sensitivity and specificity for inflammation and structural issues, useful when echocardiography is inconclusive. Emerging technologies like 3D echocardiography and advanced MRI enhance cardiac assessment (53).
Currently, immunosuppressive therapies are broadly recommended as the primary pharmacological treatment for MIS-C worldwide. These are typically supplemented with anticoagulants such as heparin or aspirin and administered in medical facilities with ICU capabilities, mechanical ventilation, and ECMO, among other advanced therapeutic technologies (47–49, 54, 55).
The administration of intravenous immunoglobulin (IVIG) and/or glucocorticoids (GC) for treating multisystem inflammatory syndrome in MIS-C is based on the condition’s post-infectious origins, its immunological features, the elevated inflammation levels, and its clinical resemblance to KD (56). Current clinical guidelines advocate for IVIG, GC, or a combination of both as viable first-line treatments for MIS-C, but evidence remains insufficient to determine the most effective approach (57, 58). A retrospective study by Jonat et al. revealed that early administration of IVIG and GC was linked to reduced hospital stay durations, underscoring the importance of early intervention (59). Close monitoring is essential for patients receiving multiple immunomodulators, particularly those with immunodeficiencies or on immunosuppressive therapy, to balance therapeutic benefits against infection risks.
Given the clinical similarities between MIS-C and KD, IVIG, which is a standard treatment for KD, has also been utilized in the management of MIS-C (60). Coronary artery aneurysms (CAA) are observed in approximately 9% to 24% of MIS-C cases (47, 61, 62), and IVIG has been shown to effectively reduce CAA incidence in KD (40). A survey of MIS-C treatment practices revealed that IVIG is administered as the first-line therapy in 98% of cases (63). IVIG exerts anti-inflammatory effects by depleting neutrophils, inhibiting IL-1β, reducing complement deposition, suppressing T-cell activity, and modulating endothelial function (64, 65). Additionally, IVIG plays a crucial role in neutralizing autoantibodies, thereby facilitating their clearance from the bloodstream (66, 67).
In stable MIS-C patients without shock or severe organ involvement, IVIG monotherapy is often effective, particularly when GC are contraindicated. However, due to diagnostic challenges associated with MIS-C and the risk of delayed treatment leading to cardiogenic shock (68), IVIG is especially recommended for KD-like presentations with CAA. The typical IVIG dosing regimen involves a single infusion of 2 g/kg (with a maximum dose of 100 g), adjusted for body weight (57, 69). Repeated dosing is generally not recommended due to potential for adverse effects (57, 69). IVIG’s role in immune modulation is vital in autoimmune diseases, including MIS-C. A study from South Africa reported that most children with MIS-C received both IVIG and corticosteroids, while a smaller group required additional IVIG doses (11). For severe cases involving shock or organ failure, the combination of IVIG and corticosteroids is recommended (70, 71).
GC are effective immunomodulators that inhibit cytokine production through nuclear trans-repression of pro-inflammatory genes. Their non-genomic effects on both immune and endothelial cells involve modulation of membrane permeability and T-cell signaling (72, 73). GC play a crucial role in managing the cytokine storm associated with MIS-C, thereby reducing disease severity and mitigating tissue damage (74, 75). Early GC administration within 48 hours of hospitalization has been associated with shorter stays, suggesting that prompt initiation is critical (59).
The standard GC regimen typically consists of short-term treatment with methylprednisolone at a dose of 1–2 mg/kg/day for 3–5 days (76, 77). In some cases, high-dose protocols, such as 30 mg/kg/day for three days, can be tapered over a period of two weeks (76). Licciardi et al. reported a 67.7% response rate in children treated exclusively with intravenous methylprednisolone (78). GC combined with IVIG is standard for most hospitalized MIS-C patients unless there are contraindications to GC use (79), with tapering over 2–3 weeks or longer (57). In severe cardiovascular involvement, combined IVIG and GC therapy may resolve complications rapidly (14). For cases resistant to standard treatments, GC pulse therapy or biologic agents may be necessary (57).
The pathophysiology of MIS-C involves elevated pro-inflammatory cytokines, particularly IL-6 (80–83). Coronaviruses upregulate IL-6 via enhanced mRNA transcription and stabilization (84, 85), contributing to cytokine storm syndromes (86) and adverse outcomes like prolonged viral shedding and respiratory failure (87–89). Tocilizumab, an IL-6 inhibitor, is the preferred therapy, administered initially at 4–8 mg/kg or 400 mg in 100 ml saline intravenously over >1 hour, with a possible second dose after 2 hours, not exceeding 800 mg or two doses total (90). This treatment demonstrates substantial effectiveness and safety (84, 85, 91). Severe MIS-C often requires combined IVIG, GC, and tocilizumab (15, 92).
Anakinra, an IL-1 inhibitor, was initially used due to MIS-C’s association with KD but is now reserved for IVIG-refractory cases (15, 91). SARS-CoV infection induces IL-1 production by alveolar type II cells (85, 93), and MIS-C patients exhibit increased IL-1β gene expression (94). Anakinra can block IL-1 (95), benefiting patients with severe sepsis and macrophage activation syndrome (96, 97), serving as an alternative therapy for IVIG-refractory MIS-C (57, 98). It is typically administered at 2–3 mg/kg subcutaneously (69) or intravenously if necessary (97). If no response within 24–48 hours, switching to tocilizumab or infliximab is recommended (69). TNF-α is implicated in severe KD (99, 100), and infliximab, a TNF-α mAb (5–10 mg/kg IV) (47, 101, 102) reduces ICU admissions, enhances cardiac function (58), and facilitates corticosteroid tapering (57, 103). Eculizumab, an anti-C5 mAb, inhibits terminal complement activation (104), improving MIS-C-related thrombotic microangiopathy (105). Emapalumab blocks IFN-γ and tadekinig alfa inhibits IL-18 (106), but current data on these agents remain limited. Emerging therapies, including new mAbs targeting various cytokines and immune pathways such as baricitinib and JAK inhibitors, are under investigation to mitigate cytokine signaling and reduce inflammation in MIS-C patients (107, 108).
The hypercoagulable state in MIS-C requires careful anticoagulation management (109, 110). Early heparin therapy is essential for children with severe ventricular dysfunction, and low-molecular-weight heparin or aspirin is recommended for those at high risk of thrombosis (110, 111). For MIS-C patients without bleeding risks, low-dose aspirin is advised unless contraindicated, continuing for at least one month post-diagnosis or until inflammatory markers normalize (35, 57, 112–115). Antiviral agents such as ribavirin, interferon, and lopinavir/ritonavir have uncertain efficacy for MIS-C, as it is immune-mediated rather than viral cytopathic (77, 116). Remdesivir is used for severe SARS-CoV-2 cases in patients ≥12 years but has unclear relevance in MIS-C; consultation with specialists is recommended for refractory cases (117). Chloroquine phosphate’s efficacy in MIS-C is unproven (47). Due to the severity of MIS-C, ICU admission for respiratory, cardiac, and circulatory support is often necessary, with ECMO in critical cases (15, 47–49) (Figure 1).
Despite severe presentations, the MIS-C mortality is low (1.9%), and most patients recover with timely treatment (20, 118). Coronary artery abnormalities (9%-24%) warrant regular follow-up (2, 119). Additionally, MIS-C may lead to long-term neurodevelopmental impacts, including cognitive and behavioral changes (120), and chronic inflammatory conditions that cause sustained immune dysregulation, increasing risks for autoimmune disorders and prolonged systemic inflammation (121). Consequently, long-term monitoring and management are essential for comprehensive patient care. Furthermore, IL-18 and TNF-α serve as prognostic markers for disease severity and the efficacy of IVIG therapy in MIS-C (122). Endothelial-cell-specific molecule-1 is a valuable diagnostic and prognostic biomarker, aiding in identifying MIS-C patients at higher cardiovascular risk and guiding treatment strategies (123).
In conclusion, MIS-C is a severe complication of SARS-CoV-2 in children, marked by systemic inflammation and multi-organ involvement. Its pathogenesis involves immune dysregulation, with delayed antibody and cytokine responses. Early recognition and a multidisciplinary approach, including IVIG, corticosteroids, and biologics, are critical for effective management. Prognosis is generally favorable with timely treatment, though long-term monitoring for cardiovascular sequelae is essential. Future research should focus on understanding its immunopathology, refining diagnostics, and optimizing therapies to improve outcomes.
ZP: Writing – original draft. GZ: Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We appreciate the support from the Chongqing University Three Gorges Hospital for this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Team CC-R. Coronavirus disease 2019 in children - United States, February 12-April 2, 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:422–6. doi: 10.15585/mmwr.mm6914e4
2. Sperotto F, Friedman KG, Son MBF, VanderPluym CJ, Newburger JW, Dionne A. Cardiac manifestations in SARS-CoV-2-associated multisystem inflammatory syndrome in children: a comprehensive review and proposed clinical approach. Eur J Pediatr. (2021) 180:307–22. doi: 10.1007/s00431-020-03766-6
3. Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet. (2020) 395:1607–8. doi: 10.1016/S0140-6736(20)31094-1
4. Radia T, Williams N, Agrawal P, Harman K, Weale J, Cook J, et al. Multi-system inflammatory syndrome in children & adolescents (MIS-C): A systematic review of clinical features and presentation. Paediatr Respir Rev. (2021) 38:51–7. doi: 10.1016/j.prrv.2020.08.001
5. Melgar M, Lee EH, Miller AD, Lim S, Brown CM, Yousaf AR, et al. Council of state and territorial epidemiologists/CDC surveillance case definition for multisystem inflammatory syndrome in children associated with SARS-coV-2 infection - United States. MMWR Recomm Rep. (2022) 71:1–14. doi: 10.15585/mmwr.rr7104a1
6. Zou H, Lu J, Liu J, Wong JH, Cheng S, Li Q, et al. Characteristics of pediatric multi-system inflammatory syndrome (PMIS) associated with COVID-19: a meta-analysis and insights into pathogenesis. Int J Infect Dis. (2021) 102:319–26. doi: 10.1016/j.ijid.2020.11.145
7. Loke YH, Berul CI, Harahsheh AS. Multisystem inflammatory syndrome in children: Is there a linkage to Kawasaki disease? Trends Cardiovasc Med. (2020) 30:389–96. doi: 10.1016/j.tcm.2020.07.004
8. Yang MC, Tsai CC, Su YT, Wu JR. The emergence of a new cytokine storm during the COVID-19 pandemic: Multisystem inflammatory syndrome in children. Kaohsiung J Med Sci. (2021) 37:255–6. doi: 10.1002/kjm2.12347
9. Tam H, El Tal T, Go E, Yeung RSM.Pediatric inflammatory multisystem syndrome temporally associated with COVID-19: a spectrum of diseases with many names. CMAJ. (2022) 192(38):E1093. doi: 10.1503/cmaj.201600
10. Patel JM. Multisystem inflammatory syndrome in children (MIS-C). Curr Allergy Asthma Rep. (2022) 22:53–60. doi: 10.1007/s11882-022-01031-4
11. Geva A, Patel MM, Newhams MM, Young CC, Son MBF, Kong M, et al. Data-driven clustering identifies features distinguishing multisystem inflammatory syndrome from acute COVID-19 in children and adolescents. EClinicalMedicine. (2021) 40:101112. doi: 10.1016/j.eclinm.2021.101112
12. Feldstein LR, Tenforde MW, Friedman KG, Newhams M, Rose EB, Dapul H, et al. Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS-C) compared with severe acute COVID-19. JAMA. (2021) 325:1074–87. doi: 10.1001/jama.2021.2091
13. LaRovere KL, Riggs BJ, Poussaint TY, Young CC, Newhams MM, Maamari M, et al. Neurologic involvement in children and adolescents hospitalized in the United States for COVID-19 or multisystem inflammatory syndrome. JAMA Neurol. (2021) 78:536–47. doi: 10.1001/jamaneurol.2021.0504
14. Melgar M, Seaby EG, McArdle AJ, Young CC, Campbell AP, Murray NL, et al. Treatment of multisystem inflammatory syndrome in children: understanding differences in results of comparative effectiveness studies. ACR Open Rheumatol. (2022) 4:804–10. doi: 10.1002/acr2.11478
15. Feldstein LR, Rose EB, Horwitz SM, Collins JP, Newhams MM, Son MBF, et al. Multisystem inflammatory syndrome in U.S. Children and adolescents. N Engl J Med. (2020) 383:334–46. doi: 10.1056/NEJMoa2021680
16. Godfred-Cato S, Bryant B, Leung J, Oster ME, Conklin L, Abrams J, et al. COVID-19-associated multisystem inflammatory syndrome in children - United States, March-July 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:1074–80. doi: 10.15585/mmwr.mm6932e2
17. Day-Lewis M, Berbert L, Baker A, Dionne A, Newburger JW, Son MBF. Updated case definition of MIS-C and implications for clinical care. Pediatrics. (2024) 153(2):e2023063259. doi: 10.1542/peds.2023-063259
18. Meneghel A, Masenello V, Alfier F, Giampetruzzi S, SemBenini C, Martini G, et al. Renal involvement in multisystem inflammatory syndrome in children: not only acute kidney injury. Children (Basel). (2023) 10(10):1661. doi: 10.3390/children10101661
19. Brooks R, Fisher R, Glicksman C, Pollak U, Simanovsky N, Berkun Y. Multisystem inflammatory syndrome in children associated with COVID-19 presenting as cervical inflammation. Acta Paediatr. (2023) 112:477–82. doi: 10.1111/apa.v112.3
20. Hoste L, Van Paemel R, Haerynck F. Multisystem inflammatory syndrome in children related to COVID-19: a systematic review. Eur J Pediatr. (2021) 180:2019–34. doi: 10.1007/s00431-021-03993-5
21. Alotaibi MA, Alhumaidan W, Alotaibi A, Alotaibi AM. Pediatric appendicitis in times of COVID-19: Think MIS-C. J Pediatr Surg Case Rep. (2022) 77:102151. doi: 10.1016/j.epsc.2021.102151
22. Distel H, Hutchins K, Purohit PJ, Begue RE. Multisystem inflammatory syndrome in children presenting as acute severe necrotizing pancreatitis: A case report. JPGN Rep. (2024) 5:567–71. doi: 10.1002/jpr3.12113
23. Petrea Cliveti CL, Ciortea DA, Candussi IL, Gurau G, Matei NM, Berghes SE, et al. A study of hydroelectrolytic and acid-base disturbances in MIS-C patients: A perspective on antidiuretic hormone secretion. Curr Issues Mol Biol. (2024) 46:11438–59. doi: 10.3390/cimb46100681
24. Sharifkashani S, Bafrani MA, Khaboushan AS, Pirzadeh M, Kheirandish A, Yavarpour Bali H, et al. Angiotensin-converting enzyme 2 (ACE2) receptor and SARS-CoV-2: Potential therapeutic targeting. Eur J Pharmacol. (2020) 884:173455. doi: 10.1016/j.ejphar.2020.173455
25. Schwartz SP, Walker TC, Kihlstrom M, Isani M, Smith MM, Smith RL, et al. Extracorporeal membrane oxygenation for COVID-19-associated multisystem inflammatory syndrome in a 5-year-old. Am Surg. (2022) 88:174–6. doi: 10.1177/0003134820983198
26. Inciardi RM, Lupi L, Zaccone G, Italia L, Raffo M, Tomasoni D, et al. Cardiac involvement in a patient with coronavirus disease 2019 (COVID-19). JAMA Cardiol. (2020) 5:819–24. doi: 10.1001/jamacardio.2020.1096
27. Dufort EM, Koumans EH, Chow EJ, Rosenthal EM, Muse A, Rowlands J, et al. Multisystem inflammatory syndrome in children in new york state. N Engl J Med. (2020) 383:347–58. doi: 10.1056/NEJMoa2021756
28. Zhai X, Zhang H, Xia Z, Liu M, Du G, Jiang Z, et al. Oxytocin alleviates liver fibrosis via hepatic macrophages. JHEP Rep. (2024) 6:101032. doi: 10.1016/j.jhepr.2024.101032
29. Xiao J, Lin H, Liu B, Xia Z, Zhang J, Jin J. Decreased S1P and SPHK2 are involved in pancreatic acinar cell injury. biomark Med. (2019) 13:627–37. doi: 10.2217/bmm-2018-0404
30. Xiao J, Huang K, Lin H, Xia Z, Zhang J, Li D, et al. Mogroside II(E) inhibits digestive enzymes via suppression of interleukin 9/interleukin 9 receptor signalling in acute pancreatitis. Front Pharmacol. (2020) 11:859. doi: 10.3389/fphar.2020.00859
31. Zhang H, Xia T, Xia Z, Zhou H, Li Z, Wang W, et al. KIF18A inactivates hepatic stellate cells and alleviates liver fibrosis through the TTC3/Akt/mTOR pathway. Cell Mol Life Sci. (2024) 81:96. doi: 10.1007/s00018-024-05114-5
32. Peart Akindele N, Kouo T, Karaba AH, Gordon O, Fenstermacher KZJ, Beaudry J, et al. Distinct cytokine and chemokine dysregulation in hospitalized children with acute coronavirus disease 2019 and multisystem inflammatory syndrome with similar levels of nasopharyngeal severe acute respiratory syndrome coronavirus 2 shedding. J Infect Dis. (2021) 224:606–15. doi: 10.1093/infdis/jiab285
33. Mauro A, Di Mari C, Casini F, Giani T, Sandini M, Biondi L, et al. Neurological manifestations of Kawasaki disease and multisystem inflammatory syndrome in children associated with COVID-19: A comparison of two different clinical entities. Front Pediatr. (2022) 10:1088773. doi: 10.3389/fped.2022.1088773
34. Tong T, Yao X, Lin Z, Tao Y, Xu J, Xu X, et al. Similarities and differences between MIS-C and KD: a systematic review and meta-analysis. Pediatr Rheumatol Online J. (2022) 20:112. doi: 10.1186/s12969-022-00771-x
35. Consiglio CR, Cotugno N, Sardh F, Pou C, Amodio D, Rodriguez L, et al. The immunology of multisystem inflammatory syndrome in children with COVID-19. Cell. (2020) 183:968–981 e967. doi: 10.1016/j.cell.2020.09.016
36. Colmenero I, Santonja C, Alonso-Riano M, Noguera-Morel L, Hernandez-Martin A, Andina D, et al. SARS-CoV-2 endothelial infection causes COVID-19 chilblains: histopathological, immunohistochemical and ultrastructural study of seven paediatric cases. Br J Dermatol. (2020) 183:729–37. doi: 10.1111/bjd.v183.4
37. Gruber CN, Patel RS, Trachtman R, Lepow L, Amanat F, Krammer F, et al. Mapping systemic inflammation and antibody responses in multisystem inflammatory syndrome in children (MIS-C). Cell. (2023) 186:3325. doi: 10.1016/j.cell.2023.06.012
38. Belot A, Antona D, Renolleau S, Javouhey E, Hentgen V, Angoulvant F, et al. SARS-CoV-2-related paediatric inflammatory multisystem syndrome, an epidemiological study, France, 1 March to 17 May 2020. Euro Surveill. (2020) 25(22):2001010. doi: 10.2807/1560-7917.ES.2020.25.22.2001010
39. Weisberg SP, Connors TJ, Zhu Y, Baldwin MR, Lin WH, Wontakal S, et al. Distinct antibody responses to SARS-CoV-2 in children and adults across the COVID-19 clinical spectrum. Nat Immunol. (2021) 22:25–31. doi: 10.1038/s41590-020-00826-9
40. Tong T, Jin YH, Wang M, Gong FQ. Treatment of multisystem inflammatory syndrome in children. World J Pediatr. (2024) 20:325–39. doi: 10.1007/s12519-024-00798-y
41. Goyal P, Choi JJ, Pinheiro LC, Schenck EJ, Chen R, Jabri A, et al. Clinical characteristics of covid-19 in new york city. N Engl J Med. (2020) 382:2372–4. doi: 10.1056/NEJMc2010419
42. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
43. Qin C, Zhou L, Hu Z, Zhang S, Yang S, Tao Y, et al. Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clin Infect Dis. (2020) 71:762–8. doi: 10.1093/cid/ciaa248
44. Cheng MH, Zhang S, Porritt RA, Noval Rivas M, Paschold L, Willscher E, et al. Superantigenic character of an insert unique to SARS-CoV-2 spike supported by skewed TCR repertoire in patients with hyperinflammation. Proc Natl Acad Sci U.S.A. (2020) 117:25254–62. doi: 10.1073/pnas.2010722117
45. Barreto TMM, Souza RS, Sao Pedro RB, Paiva IM, Silva AS, Nogueira AL, et al. Rare genetic variants of NLRP12 in admixed latino-american children with SARS-coV-2-related multisystem inflammatory syndrome. J Infect Dis. (2024) 230:1400–9. doi: 10.1093/infdis/jiae480
46. Yang CA, Huang YL, Chiang BL. Innate immune response analysis in COVID-19 and kawasaki disease reveals MIS-C predictors. J Formos Med Assoc. (2022) 121:623–32. doi: 10.1016/j.jfma.2021.06.009
47. Whittaker E, Bamford A, Kenny J, Kaforou M, Jones CE, Shah P, et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-coV-2. JAMA. (2020) 324:259–69. doi: 10.1001/jama.2020.10369
48. Moraleda C, Serna-Pascual M, Soriano-Arandes A, Simo S, Epalza C, Santos M, et al. Multi-inflammatory syndrome in children related to severe acute respiratory syndrome coronavirus 2 (SARS-coV-2) in Spain. Clin Infect Dis. (2021) 72:e397–401. doi: 10.1093/cid/ciaa1042
49. Belhadjer Z, Méot M, Bajolle F, Khraiche D, Legendre A, Abakka S, et al. Acute heart failure in multisystem inflammatory syndrome in children in the context of global SARS-CoV-2 pandemic. Circulation. (2020) 142:429–36. doi: 10.1161/CIRCULATIONAHA.120.048360
50. Matsubara D, Kauffman HL, Wang Y, Calderon-Anyosa R, Nadaraj S, Elias MD, et al. Echocardiographic findings in pediatric multisystem inflammatory syndrome associated with COVID-19 in the United States. J Am Coll Cardiol. (2020) 76:1947–61. doi: 10.1016/j.jacc.2020.08.056
51. Blondiaux E, Parisot P, Redheuil A, Tzaroukian L, Levy Y, Sileo C, et al. Cardiac MRI in children with multisystem inflammatory syndrome associated with COVID-19. Radiology. (2020) 297:E283–8. doi: 10.1148/radiol.2020202288
52. Imataka G, Kuwashima S, Yoshihara S. A comprehensive review of pediatric acute encephalopathy. J Clin Med. (2022) 11:5921. doi: 10.3390/jcm11195921
53. Wong J, Theocharis P, Regan W, Pushparajah K, Stephenson N, Pascall E, et al. Medium-term cardiac outcomes in young people with multi-system inflammatory syndrome: the era of COVID-19. Pediatr Cardiol. (2022) 43:1728–36. doi: 10.1007/s00246-022-02907-y
54. Sanders JM, Monogue ML, Jodlowski TZ, Cutrell JB. Pharmacologic treatments for coronavirus disease 2019 (COVID-19): A review. JAMA. (2020) 323:1824–36. doi: 10.1001/jama.2020.6019
55. Xu Y, Li X, Zhu B, Liang H, Fang C, Gong Y, et al. Characteristics of pediatric SARS-CoV-2 infection and potential evidence for persistent fecal viral shedding. Nat Med. (2020) 26:502–5. doi: 10.1038/s41591-020-0817-4
56. Feleszko W, Okarska-Napierala M, Buddingh EP, Bloomfield M, Sediva A, Bautista-Rodriguez C, et al. Pathogenesis, immunology, and immune-targeted management of the multisystem inflammatory syndrome in children (MIS-C) or pediatric inflammatory multisystem syndrome (PIMS): EAACI Position Paper. Pediatr Allergy Immunol. (2023) 34:e13900. doi: 10.1111/pai.13900
57. Henderson LA, Canna SW, Friedman KG, Gorelik M, Lapidus SK, Bassiri H, et al. American college of rheumatology clinical guidance for multisystem inflammatory syndrome in children associated with SARS-coV-2 and hyperinflammation in pediatric COVID-19: version 3. Arthritis Rheumatol. (2022) 74:e1–e20. doi: 10.1002/art.42062
58. Algarni AS, Alamri NM, Khayat NZ, Alabdali RA, Alsubhi RS, Alghamdi SH. Clinical practice guidelines in multisystem inflammatory syndrome (MIS-C) related to COVID-19: a critical review and recommendations. World J Pediatr. (2022) 18:83–90. doi: 10.1007/s12519-021-00499-w
59. Jonat B, Geneslaw AS, Capone CA, Shah S, Bartucca L, Sewell TB, et al. Early treatment of multisystem inflammatory syndrome in children. Pediatrics. (2023) 152(3):e2023061297. doi: 10.1542/peds.2023-061297
60. Cannon L, Campbell MJ, Wu EY. Multisystemic inflammatory syndrome in children and kawasaki disease: parallels in pathogenesis and treatment. Curr Allergy Asthma Rep. (2023) 23:341–50. doi: 10.1007/s11882-023-01083-0
61. Bautista-Rodriguez C, Sanchez-de-Toledo J, Clark BC, Herberg J, Bajolle F, Randanne PC, et al. Multisystem inflammatory syndrome in children: an international survey. Pediatrics. (2021) 147(2):e2020024554. doi: 10.1542/peds.2020-024554
62. Jongsma MLM, de Waard AA, Raaben M, Zhang T, Cabukusta B, Platzer R, et al. The SPPL3-defined glycosphingolipid repertoire orchestrates HLA class I-mediated immune responses. Immunity. (2021) 54:132–150 e139. doi: 10.1016/j.immuni.2020.11.003
63. Dove ML, Jaggi P, Kelleman M, Abuali M, Ang JY, Ballan W, et al. Multisystem inflammatory syndrome in children: survey of protocols for early hospital evaluation and management. J Pediatr. (2021) 229:33–40. doi: 10.1016/j.jpeds.2020.10.026
64. Ganigara M, Sharma C, Bayry J. Unraveling the mechanisms of IVIG immunotherapy in MIS-C. Cell Rep Med. (2021) 2:100431. doi: 10.1016/j.xcrm.2021.100431
65. Ramaswamy A, Brodsky NN, Sumida TS, Comi M, Asashima H, Hoehn KB, et al. Post-infectious inflammatory disease in MIS-C features elevated cytotoxicity signatures and autoreactivity that correlates with severity. medRxiv. (2021) 54:1083–95. doi: 10.1101/2020.12.01.20241364
66. Ballow M. The IgG molecule as a biological immune response modifier: mechanisms of action of intravenous immune serum globulin in autoimmune and inflammatory disorders. J Allergy Clin Immunol. (2011) 127:315–323; quiz 324-315. doi: 10.1016/j.jaci.2010.10.030
67. Norris PAA, Kaur G, Lazarus AH. New insights into IVIg mechanisms and alternatives in autoimmune and inflammatory diseases. Curr Opin Hematol. (2020) 27:392–8. doi: 10.1097/MOH.0000000000000609
68. Bichali S, Bonnet M, Lampin ME, Baudelet JB, Reumaux H, Domanski O, et al. Impact of time to diagnosis on the occurrence of cardiogenic shock in MIS-C post-COVID-19 infection. World J Pediatr. (2023) 19:595–604. doi: 10.1007/s12519-022-00681-8
69. Schlapbach LJ, Andre MC, Grazioli S, Schobi N, Ritz N, Aebi C, et al. Best practice recommendations for the diagnosis and management of children with pediatric inflammatory multisystem syndrome temporally associated with SARS-coV-2 (PIMS-TS; multisystem inflammatory syndrome in children, MIS-C) in Switzerland. Front Pediatr. (2021) 9:667507. doi: 10.3389/fped.2021.667507
70. Crosby L, Balasubramanian S, Ramanan AV. Steroids or intravenous immunoglobulin as first line in MIS-C in LMICs. Lancet Rheumatol. (2021) 3:e615–6. doi: 10.1016/S2665-9913(21)00223-X
71. Villacis-Nunez DS, Jones K, Jabbar A, Fan L, Moore W, Peter AS, et al. Short-term outcomes of corticosteroid monotherapy in multisystem inflammatory syndrome in children. JAMA Pediatr. (2022) 176:576–84. doi: 10.1001/jamapediatrics.2022.0292
72. Sinha A, Bagga A. Pulse steroid therapy. Indian J Pediatr. (2008) 75:1057–66. doi: 10.1007/s12098-008-0210-7
73. Stahn C, Buttgereit F. Genomic and nongenomic effects of glucocorticoids. Nat Clin Pract Rheumatol. (2008) 4:525–33. doi: 10.1038/ncprheum0898
74. Son MBF, Murray N, Friedman K, Young CC, Newhams MM, Feldstein LR, et al. Multisystem inflammatory syndrome in children - initial therapy and outcomes. N Engl J Med. (2021) 385:23–34. doi: 10.1056/NEJMoa2102605
75. Ouldali N, Toubiana J, Antona D, Javouhey E, Madhi F, Lorrot M, et al. Association of intravenous immunoglobulins plus methylprednisolone vs immunoglobulins alone with course of fever in multisystem inflammatory syndrome in children. JAMA. (2021) 325:855–64. doi: 10.1001/jama.2021.0694
76. Verdoni L, Mazza A, Gervasoni A, Martelli L, Ruggeri M, Ciuffreda M, et al. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. Lancet. (2020) 395:1771–8. doi: 10.1016/S0140-6736(20)31103-X
77. Sahu KK, Mishra AK, Lal A. COVID-2019: update on epidemiology, disease spread and management. Monaldi Arch Chest Dis. (2020) 90(1). doi: 10.4081/monaldi.2020.1292
78. Licciardi F, Baldini L, Dellepiane M, Covizzi C, Mogni R, Pruccoli G, et al. MIS-C treatment: is IVIG always necessary? Front Pediatr. (2021) 9:753123. doi: 10.3389/fped.2021.753123
79. In Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Bethesda (MD): National Institutes of Health (US) (2021).
80. Carter MJ, Fish M, Jennings A, Doores KJ, Wellman P, Seow J, et al. Peripheral immunophenotypes in children with multisystem inflammatory syndrome associated with SARS-CoV-2 infection. Nat Med. (2020) 26:1701–7. doi: 10.1038/s41591-020-1054-6
81. Gruber CN, Patel RS, Trachtman R, Lepow L, Amanat F, Krammer F, et al. Mapping systemic inflammation and antibody responses in multisystem inflammatory syndrome in children (MIS-C). Cell. (2020) 183:982–995 e914. doi: 10.1016/j.cell.2020.09.034
82. Zhu YP, Shamie I, Lee JC, Nowell CJ, Peng W, Angulo S, et al. Immune response to intravenous immunoglobulin in patients with Kawasaki disease and MIS-C. J Clin Invest. (2021) 131(20):e147076. doi: 10.1172/JCI147076
83. Toraih EA, Hussein MH, Elshazli RM, Kline A, Munshi R, Sultana N, et al. Multisystem inflammatory syndrome in pediatric COVID-19 patients: a meta-analysis. World J Pediatr. (2021) 17:141–51. doi: 10.1007/s12519-021-00419-y
84. Schmidt W, Pawlak-Bus K, Jozwiak B, Leszczynski P. Identification of clinical response predictors of tocilizumab treatment in patients with severe COVID-19 based on single-center experience. J Clin Med. (2023) 12(6):2429. doi: 10.3390/jcm12062429
85. Yoshikawa T, Hill T, Li K, Peters CJ, Tseng CT. Severe acute respiratory syndrome (SARS) coronavirus-induced lung epithelial cytokines exacerbate SARS pathogenesis by modulating intrinsic functions of monocyte-derived macrophages and dendritic cells. J Virol. (2009) 83:3039–48. doi: 10.1128/JVI.01792-08
86. Crayne CB, Albeituni S, Nichols KE, Cron RQ. The immunology of macrophage activation syndrome. Front Immunol. (2019) 10:119. doi: 10.3389/fimmu.2019.00119
87. Stone JH, Frigault MJ, Serling-Boyd NJ, Fernandes AD, Harvey L, Foulkes AS, et al. Efficacy of tocilizumab in patients hospitalized with covid-19. N Engl J Med. (2020) 383:2333–44. doi: 10.1056/NEJMoa2028836
88. Herold T, Jurinovic V, Arnreich C, Lipworth BJ, Hellmuth JC, von-Bergwelt-Baildon M, et al. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J Allergy Clin Immunol. (2020) 146:128–136 e124. doi: 10.1016/j.jaci.2020.05.008
89. Del Valle DM, Kim-Schulze S, Huang HH, Beckmann ND, Nirenberg S, Wang B, et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat Med. (2020) 26:1636–43. doi: 10.1038/s41591-020-1051-9
90. Nasim S, Hashmi SH, Azim D, Kumar S, Nasim J. Tocilizumab for COVID-19: a real ‘miracle drug’? Infect Dis (Lond). (2020) 52:681–2. doi: 10.1080/23744235.2020.1780307
91. Xu X, Han M, Li T, Sun W, Wang D, Fu B, et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci U.S.A. (2020) 117:10970–5. doi: 10.1073/pnas.2005615117
92. Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, et al. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics. (2020) 145:e20200702. doi: 10.1542/peds.2020-0702
93. Schett G, Manger B, Simon D, Caporali R. COVID-19 revisiting inflammatory pathways of arthritis. Nat Rev Rheumatol. (2020) 16:465–70. doi: 10.1038/s41584-020-0451-z
94. Ghosh P, Katkar GD, Shimizu C, Kim J, Khandelwal S, Tremoulet AH, et al. An Artificial Intelligence-guided signature reveals the shared host immune response in MIS-C and Kawasaki disease. Nat Commun. (2022) 13:2687. doi: 10.1038/s41467-022-30357-w
95. Bhat CS, Shetty R, Ramesh D, Banu A, Ramanan AV. Anakinra in refractory multisystem inflammatory syndrome in children (MIS-C). Indian Pediatr. (2021) 58:994–6. doi: 10.1007/s13312-021-2340-1
96. Shakoory B, Carcillo JA, Chatham WW, Amdur RL, Zhao H, Dinarello CA, et al. Interleukin-1 receptor blockade is associated with reduced mortality in sepsis patients with features of macrophage activation syndrome: reanalysis of a prior phase III trial. Crit Care Med. (2016) 44:275–81. doi: 10.1097/CCM.0000000000001402
97. Caglayan S, Sonmez HE, Otar Yener G, Baglan E, Ozturk K, Ulu K, et al. Anakinra treatment in multisystemic inflammatory syndrome in children (MIS-C) associated with COVID-19. Front Pediatr. (2022) 10:942455. doi: 10.3389/fped.2022.942455
98. Lee JY, Kim J, Choi SH, Kim DH, Yun KW, Kim YJ, et al. Clinical effectiveness of biological immunomodulators in SARS-coV-2-associated multisystem inflammatory syndrome in children: A systematic review. Children (Basel). (2024) 11(10):1180. doi: 10.3390/children11101180
99. Pouletty M, Borocco C, Ouldali N, Caseris M, Basmaci R, Lachaume N, et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): a multicentre cohort. Ann Rheum Dis. (2020) 79:999–1006. doi: 10.1136/annrheumdis-2020-217960
100. Diorio C, Henrickson SE, Vella LA, McNerney KO, Chase J, Burudpakdee C, et al. Multisystem inflammatory syndrome in children and COVID-19 are distinct presentations of SARS-CoV-2. J Clin Invest. (2020) 130:5967–75. doi: 10.1172/JCI140970
101. Mori M, Hara T, Kikuchi M, Shimizu H, Miyamoto T, Iwashima S, et al. Infliximab versus intravenous immunoglobulin for refractory Kawasaki disease: a phase 3, randomized, open-label, active-controlled, parallel-group, multicenter trial. Sci Rep. (2018) 8:1994. doi: 10.1038/s41598-017-18387-7
102. Abdel-Haq N, Asmar BI, Deza Leon MP, McGrath EJ, Arora HS, Cashen K, et al. SARS-CoV-2-associated multisystem inflammatory syndrome in children: clinical manifestations and the role of infliximab treatment. Eur J Pediatr. (2021) 180:1581–91. doi: 10.1007/s00431-021-03935-1
103. Dolinger MT, Person H, Smith R, Jarchin L, Pittman N, Dubinsky MC, et al. Pediatric crohn disease and multisystem inflammatory syndrome in children (MIS-C) and COVID-19 treated with infliximab. J Pediatr Gastroenterol Nutr. (2020) 71:153–5. doi: 10.1097/MPG.0000000000002809
104. Jodele S, Dandoy CE, Lane A, Laskin BL, Teusink-Cross A, Myers KC, et al. Complement blockade for TA-TMA: lessons learned from a large pediatric cohort treated with eculizumab. Blood. (2020) 135:1049–57. doi: 10.1182/blood.2019004218
105. Aurora T, Joseph N, Bhoopalan SV, Caniza MA, Flerlage T, Ghafoor S, et al. The successful use of eculizumab for treatment of thrombotic microangiopathy in pediatric acute SARSCoV2 infection and multisystem inflammatory syndrome in children. Haematologica. (2022) 107:2517–22. doi: 10.3324/haematol.2022.280603
106. Canna SW, Girard C, Malle L, de Jesus A, Romberg N, Kelsen J, et al. Life-threatening NLRC4-associated hyperinflammation successfully treated with IL-18 inhibition. J Allergy Clin Immunol. (2017) 139:1698–701. doi: 10.1016/j.jaci.2016.10.022
107. Wurm J, Ritz N, Zimmermann P. Coronavirus disease 2019 (COVID-19) in children: Evolving epidemiology, immunology, symptoms, diagnostics, treatment, post-COVID-19 conditions, prevention strategies, and future directions. J Allergy Clin Immunol. (2024) 6749:01216–8. doi: 10.1016/j.jaci.2024.11.012
108. Zhu F, Ang JY. COVID-19 infection in children: diagnosis and management. Curr Infect Dis Rep. (2022) 24:51–62. doi: 10.1007/s11908-022-00779-0
109. Varga Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, Zinkernagel AS, et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet. (2020) 395:1417–8. doi: 10.1016/S0140-6736(20)30937-5
110. Riollano-Cruz M, Akkoyun E, Briceno-Brito E, Kowalsky S, Reed J, Posada R, et al. Multisystem inflammatory syndrome in children related to COVID-19: A New York City experience. J Med Virol. (2021) 93:424–33. doi: 10.1002/jmv.26224
111. Shah SK, Munoz AC. Multisystem inflammatory syndrome in children in COVID-19 pandemic. Indian J Pediatr. (2020) 87:671–3. doi: 10.1007/s12098-020-03440-7
112. McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment, and long-term management of kawasaki disease: A scientific statement for health professionals from the american heart association. Circulation. (2017) 135:e927–99. doi: 10.1161/CIR.0000000000000484
113. Harwood R, Allin B, Jones CE, Whittaker E, Ramnarayan P, Ramanan AV, et al. A national consensus management pathway for paediatric inflammatory multisystem syndrome temporally associated with COVID-19 (PIMS-TS): results of a national Delphi process. Lancet Child Adolesc Health. (2021) 5:133–41. doi: 10.1016/S2352-4642(20)30304-7
114. Merzon E, Green I, Vinker S, Golan-Cohen A, Gorohovski A, Avramovich E, et al. The use of aspirin for primary prevention of cardiovascular disease is associated with a lower likelihood of COVID-19 infection. FEBS J. (2021) 288:5179–89. doi: 10.1111/febs.v288.17
115. Rowley AH. Understanding SARS-CoV-2-related multisystem inflammatory syndrome in children. Nat Rev Immunol. (2020) 20:453–4. doi: 10.1038/s41577-020-0367-5
116. Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. (2020) 30:269–71. doi: 10.1038/s41422-020-0282-0
117. Waseem M, Shariff MA, Lim CA, Nunez J, Narayanan N, Patel K, et al. Multisystem inflammatory syndrome in children. West J Emerg Med. (2022) 23:505–13. doi: 10.5811/westjem
118. Jiang L, Tang K, Levin M, Irfan O, Morris SK, Wilson K, et al. COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet Infect Dis. (2020) 20:e276–88. doi: 10.1016/S1473-3099(20)30651-4
119. Toubiana J, Poirault C, Corsia A, Bajolle F, Fourgeaud J, Angoulvant F, et al. Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: prospective observational study. BMJ. (2020) 369:m2094. doi: 10.1136/bmj.m2094
120. Abbati G, Attaianese F, Rosati A, Indolfi G, Trapani S. Neurological involvement in children with COVID-19 and MIS-C: A retrospective study conducted for more than two years in a pediatric hospital. Children (Basel). (2022) 9(12):1809. doi: 10.3390/children9121809
121. Dourdouna MM, Tatsi EB, Syriopoulou V, Michos A. Proteomic signatures of multisystem inflammatory syndrome in children (MIS-C) associated with COVID-19: A narrative review. Children (Basel). (2024) 11(10):1174. doi: 10.3390/children11101174
122. Bartha-Tatar A, Sinkovits G, Schnur J, Maraczi V, David M, Zsigmond B, et al. Prognostic value of baseline serum pro-inflammatory cytokines in severe multisystem inflammatory syndrome in children. J Clin Med. (2024) 13(23):7177. doi: 10.3390/jcm13237177
Keywords: MIS-C, COVID-19, SARS-CoV-2, multisystem inflammatory syndrome, pediatric, Kawasaki disease, immunotherapy, diagnosis
Citation: Peng Z and Zhou G (2025) Progress on diagnosis and treatment of multisystem inflammatory syndrome in children. Front. Immunol. 16:1551122. doi: 10.3389/fimmu.2025.1551122
Received: 24 December 2024; Accepted: 24 January 2025;
Published: 19 February 2025.
Edited by:
Jibin Liu, Nantong Tumor Hospital, ChinaReviewed by:
Jing Zhang, University of South Dakota, United StatesCopyright © 2025 Peng and Zhou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gang Zhou, emhvdWdhbmcxMTI3QDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.