 Xiaoyan Zheng1,2†
Xiaoyan Zheng1,2† Qingquan Chen
Qingquan Chen Xiaoyang Zhang
Xiaoyang Zhang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol., 31 March 2025
Sec. Viral Immunology
Volume 16 - 2025 | https://doi.org/10.3389/fimmu.2025.1533102
This article is part of the Research TopicSARS-CoV-2: Virology, Epidemiology, Diagnosis, Pathogenesis and Control, Volume IIView all 4 articles
Objective: To track the level of serum antibodies in Fuzhou residents and analyze the possible influencing factors of serum antibodies, so as to provide a scientific basis for the adjustment of population immunity and prevention and control strategies.
Methods: Residents in the Fuzhou community who had symptoms of covid-19 infection or who had tested positive for nucleic acid or antigen since December 2022 were selected for the questionnaire survey and their sera were collected to analyze the trend of antibody changes, the antibody level was divided into high antibody group and low antibody group according to the literature data. The possible influencing factors of serum antibody level was analyzed by multivariate logistic regression model.
Results: A total of 2,521 Fuzhou residents were adopted in the study, including 223 in the high antibody group and 194 in the low antibody group. A univariate analysis showed that, there were significant differences in age (Z=-4.028, P<0.00), occupation (χ2 = 18.591, P=0.005), typical symptoms after the first infection (χ2 = 9.784, P=0.002), history of surgery (χ2 = 29.542, P<0.001), symptoms lasting more than 2 weeks after the first infection (χ2 = 4.887, P=0.027), smoking (χ2 = 18.524, P<0.001) and drinking (χ2 = 19.578, P<0.001) between the high antibody group and the low antibody group. Multivariate regression models show that, age (OR= 1.011, 95%CI: 1.002~1.020, P=0.017), history of surgery (OR=4.956,95%CI: 2.606~9.423, P<0.001),smoking (OR=2.089, 95%CI: 1.002~4.355, P=0.049), drinking (OR=2.214, 95%CI: 1.066~4.600, P=0.033) were the risk factors affecting antibody level. Typical symptoms after the first infection (OR=0.224, 95%CI: 0.086~0.579, P=0.002) and symptoms lasting more than 2 weeks after the first infection (OR=0.432, 95%CI: 0.258~0.723, P=0.001) were protective factors. By observing the trend of antibody changes in 3, 6 and 9 months, we found that the level of IgG antibody showed a decreasing trend.
Conclusions: The high level of protection was more likely to occur in young adults, people without operation history, people without smoking history, people without drinking history, people with typical symptoms after the first infection and symptoms lasting more than 2 weeks after the first infection. The level of IgG antibody was decreased in general, so it is necessary to strengthen immunization.
A global health emergency resulted from the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which caused the COVID-19 infection (1, 2). As of the end of December 2022, China has steadfastly implemented the “dynamic zero” COVID-19 policy, maintaining a relatively low level of domestic cases. However, following the adjustment of COVID-19 management to a Class B infectious disease on January 8, 2023, a significant surge in cases was observed.
To determine the main elements influencing the illness process and their long-term effects on immunity, it will be essential to comprehend the intricate immunological response triggered by SARS-CoV-2 infection. The span and potency of antibody responses provide valuable insight into the resilience of post-infection immunity (3).
Previous research on the dynamic changes of specific serum antibodies in COVID-19 patients predominantly focuses on the acute phase of the disease, with most studies analyzing antibody production and decay rates within the first few months of infection. This emphasis results in a significant gap in our understanding of long-term antibody dynamics, particularly regarding the persistence and protective efficacy of antibodies beyond the acute phase (4–6). Such a deficiency in the literature highlights the critical necessity for large-scale, longitudinal prospective studies. These studies are particularly needed in the aftermath of intense virus transmission episodes in specific regions, such as Fuzhou, where community-level immunity patterns may offer unique insights into the long-term impacts of the virus on population health.
Hence, this study involves 2,521 community residents from Fuzhou, employing questionnaires and collecting serum samples every three months to investigate the determinants and trends of serum antibody changes. By applying statistical methods to analyze factors influencing antibody levels and developing predictive models for high-risk groups, this research aims to provide a scientific basis for adjusting community immunity strategies and public health policies. This approach not only addresses a crucial gap in longitudinal immunological research post-high transmission but also enhances our preparedness for potential future outbreaks.
According to the formula of sample size, the reference at the end of 2022 the China provincial new virus infection monitoring data (7), take p1 = 85%, the absolute maximum permissible error of the delta δ= 0.05, estimate the range of 80% - 90%, deff = 8.5. According to the formula, the effective sample size of our city was about 2000 people, and the loss rate of follow-up was expected to be 20%. The number of respondents was extended to 2400 people, and a total of 2521 community residents of Fuzhou were finally included as the research objects. Inclusion criteria for since December 2022, there have been SARS-CoV-2 infection symptoms or nucleic acid or antigen test is positive, different genders and all ages (≤18 years old, 18 to 59 years old, 60-79 years old, ≥80 years old) in a balanced distribution.
This prospective study employed multi-stage stratified random sampling. One street and one township were randomly selected from each county (city) district, and from each, 100 individuals were randomly chosen for a questionnaire survey and serological specimen collection. Thus, at least 200 people were surveyed in each county (city) district. These activities were conducted quarterly over a nine-month monitoring period on the community populations of the constituencies.
In Fuzhou City, the vaccination protocol comprised a three-dose regimen. The first dose served as the primary immunization, administered to individuals without prior SARS-CoV-2 infection. For those with confirmed prior infection, the initial dose was deferred until three months post-recovery to mitigate potential interference with immune response maturation. The second and third doses, designated as booster immunizations, were administered at intervals of three months following the primary dose and six months after the second dose, respectively. All vaccines utilized were inactivated SARS-CoV-2 formulations, produced by Sinopharm Beijing Institute of Biological Products Co., Ltd. (BBIBP-CorV) and Sinovac Biotech Ltd. (CoronaVac). These vaccines exhibited a documented shelf life of 24 months under standardized storage conditions.
In this study, the following information was collected by means of a questionnaire: gender, age, occupation, height, weight, whether there were typical symptoms after the initial infection, history of surgery, whether they had been vaccinated in the last three months, length of time to cure, whether they still had symptoms two weeks after the initial infection, history of drinking, history of smoking, and the presence of background diseases. The background diseases were referred to Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Professionals published by the Centers for Disease Control, included diabetes mellitus, hypertension, autoimmune diseases, coronary atherosclerotic heart disease, tumors, and renal insufficiency, which were classified as underlying medical conditions.
We collected venous blood samples in March, June, and September, using procoagulant tubes. Each sample, consisting of 3-5 ml of blood, was barcoded to correlate with its corresponding questionnaire. Samples were gently mixed, allowed to settle, and then centrifuged at 3000 rpm for 5-10 minutes. They were transported to the Centers for Disease Control within 24 hours. If not analyzed within 24 hours, samples were stored at 4°C. The serum IgG antibody levels were detected using the MAGLUMI IgG antibody detection kit based on chemiluminescence immunoassay. This involved centrifuging the samples at 2000 rpm for 10 minutes, labeling the antigen with a chemiluminescent agent, incubating for 20 minutes, and then performing the test on the machine. Results were exported to an Excel file for subsequent analysis.
Based on serum antibody test values, subjects were categorized into high and low antibody level groups. Initially, a one-way analysis was performed. Measurement data were analyzed using either the t-test or the rank-sum test, while count data were evaluated with the chi-squared test. Significant variables identified through univariate screening were further analyzed to determine the influencing factors of serum antibody levels using a multifactorial logistic regression model. A two-sided p-value of less than 0.05 was considered statistically significant. All data were analyzed using SPSS 26.0 software.
It was calculated that at least 2400 samples were needed, and ultimately, 2521 samples were collected. Literature review indicates that antibody levels ≥65 AU/mL are considered to represent high protection, while levels ≤20 AU/mL are considered low. Given that IgM appears earliest and decays fastest, it was excluded from the main analysis due to its large variability. After a significant infection wave in January 2023, antibody levels were naturally decaying by March; hence, the March IgG levels were analyzed to identify factors influencing serum antibody concentrations. From this analysis, 223 individuals were categorized into the high antibody group, and 194 into the low antibody group. In the high antibody group, the median age was 40 years (range: 15-65), and the median BMI was 22.27 (range: 19.60-24.97). Age did not follow a normal distribution (D=0.124, P<0.001), whereas BMI did (D=0.056, P=0.087). The group comprised 98 males (43.9%) and 125 females (56.1%). In the low antibody group, the median age was 57 years (range: 34.75-74), and the median BMI was 23.04 (range: 20.20-25.17), with both age and BMI not following a normal distribution (Age: D=0.091, P<0.001; BMI: D=0.095, P<0.001). This group included 93 males (47.9%) and 101 females (52.1%). In both groups, age and BMI were normally distributed as shown in Table 1. Information on the assignment of independent variables is shown in Table 2.
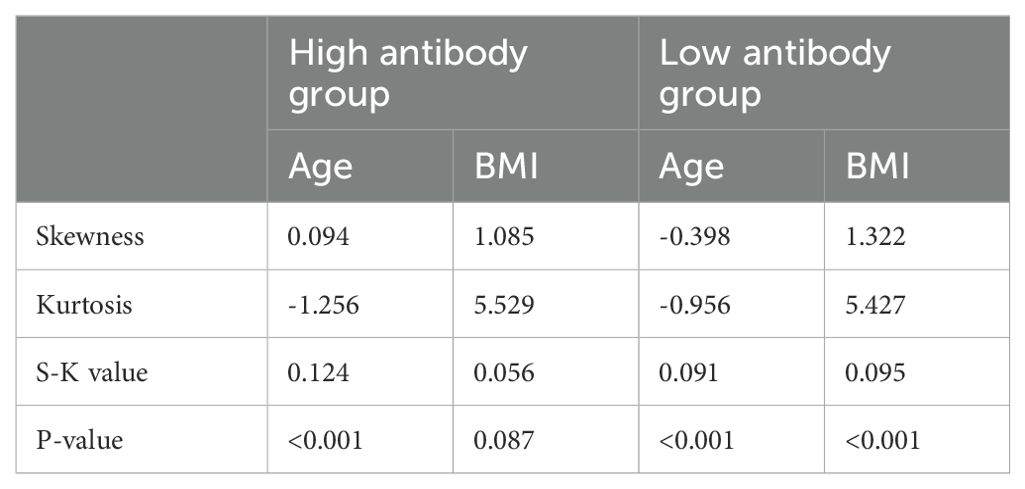
Table 1. Normality test of age and BMI.
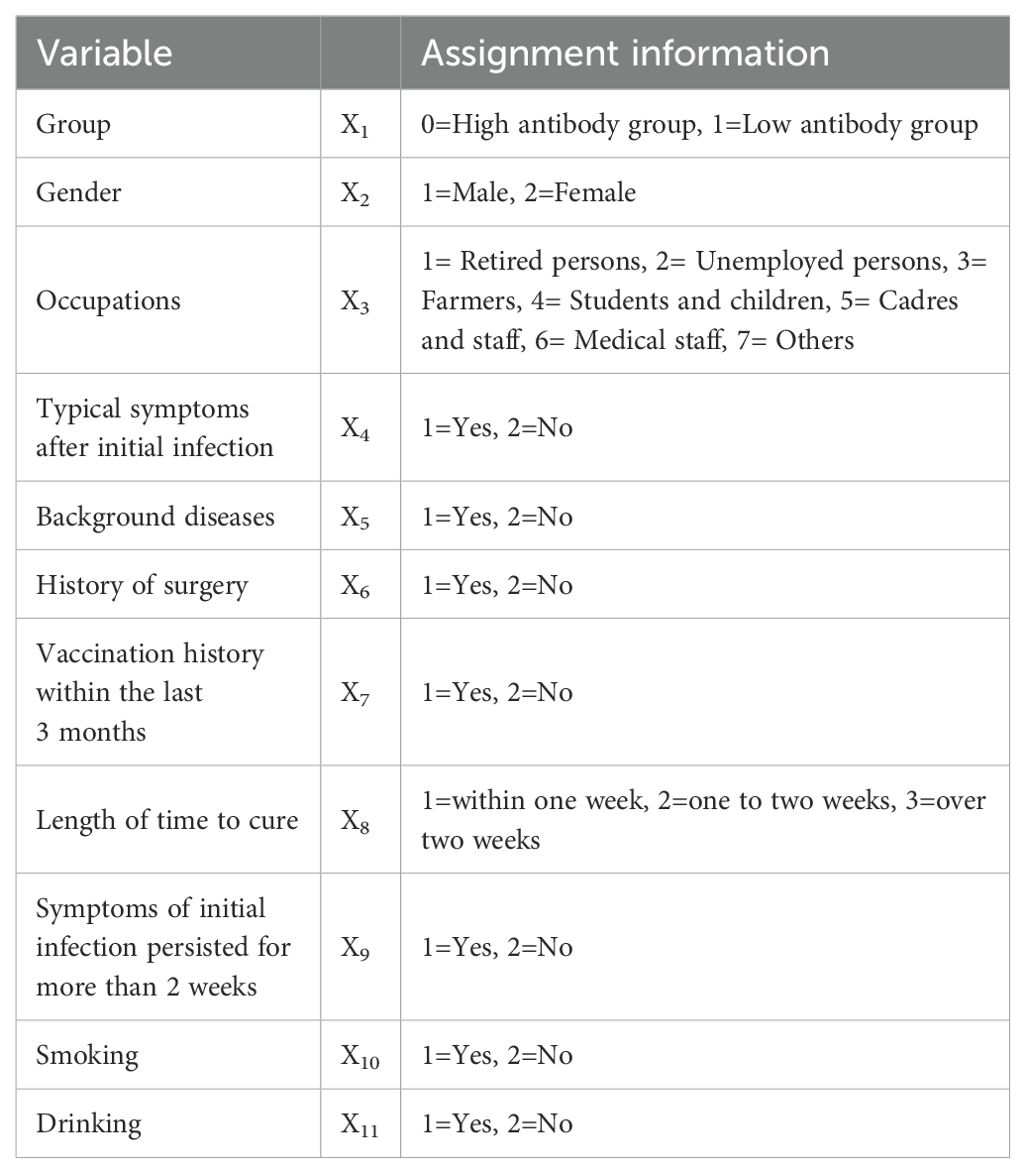
Table 2. Independent variable assignment information.
In the high antibody group and the low antibody group were significantly different in age (Z=-4.028,P<0.001), occupation (χ2 = 18.591, P=0.005), typical symptoms after the first infection (χ2=9.784, P=0.002), history of surgery (χ2 = 29.542, P<0.001), symptoms lasting more than 2 weeks after the first infection (χ2 = 4.887, P=0.027), smoking history (χ2 = 18.524, P<0.001), drinking history (χ2 = 19.578, P<0.001). There were significant differences in BMI (Z=-1.241, P=0.215), gender (χ2 = 0.666, P=0.414), background diseases (χ2 = 2.929, P=0.087), vaccination history in the last three months (χ2 = 0.312, P=0.576), length of cure (χ2 = 3.011, P=0.222), and the incidence of adverse reactions (Z=-1.241, P=0.215). P=0.222). The distribution of related factors and the analysis results are shown in Table 3.
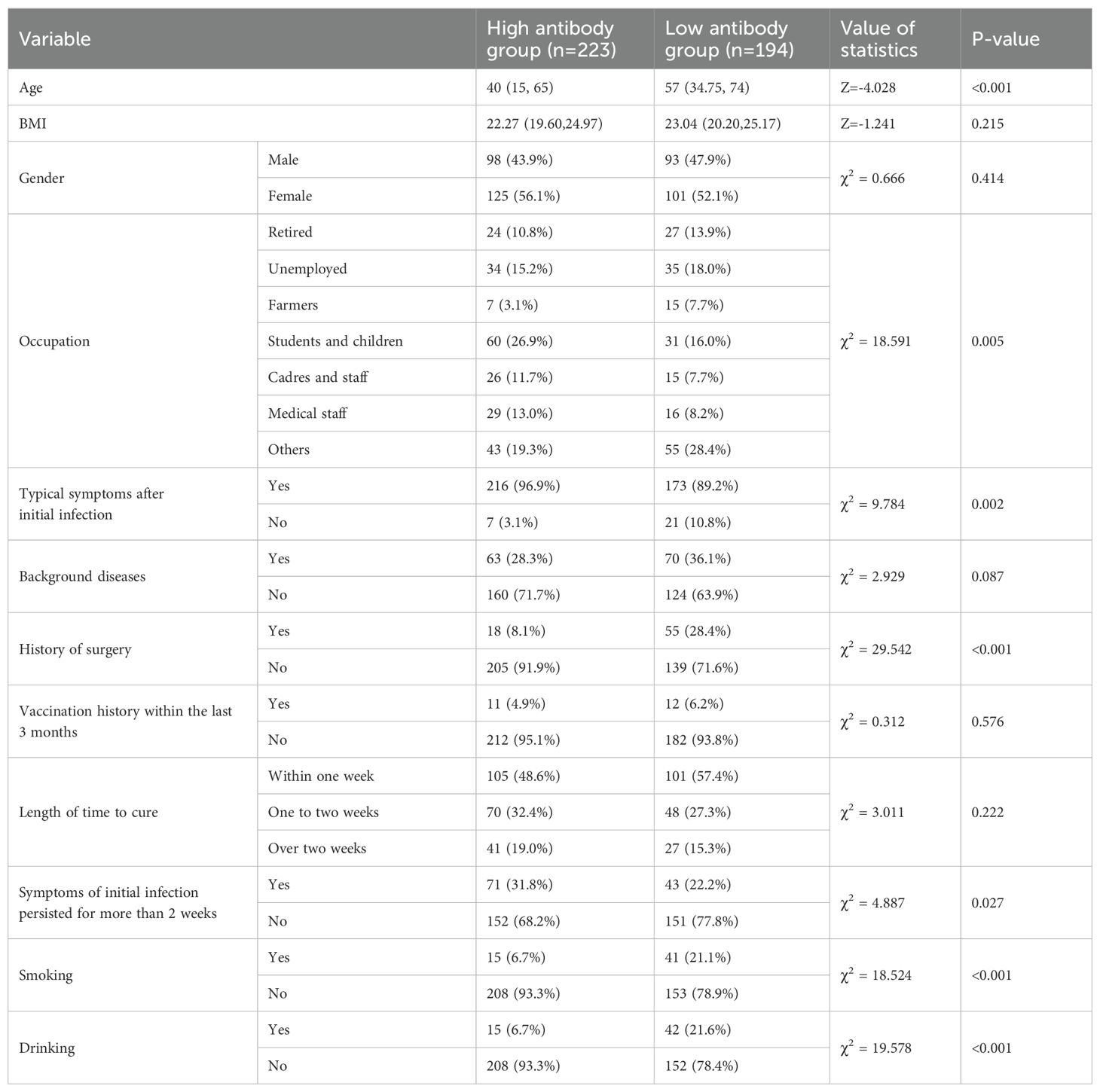
Table 3. Distribution and analysis results of related factors in the two groups.
IgG antibody level and age (P<0.001), whether there were typical symptoms after the first infection (P=0.041), surgical history (P<0.001), duration of cure (P=0.030), symptoms lasting more than 2 weeks after initial infection (P=0.005), smoking history (P<0.001), drinking history (P<0.001), but not with gender (P=0.576), BMI (P=0.342), occupation (P=0.788), vaccination history in the past three months (P=0.486) and underlying diseases (P=0.102). Among the variables related to antibody levels in this study, age (r=-0.194), typical symptoms after the first infection (r=-0.082), and symptoms lasting more than 2 weeks after the first infection (r=-0.114) were negatively correlated with antibody levels. History of surgery (r=0.182), length of cure (r=0.086), history of smoking (r=0.157), and history of drinking (r=0.174) were positively correlated with antibody levels, and the results are shown in Table 4.
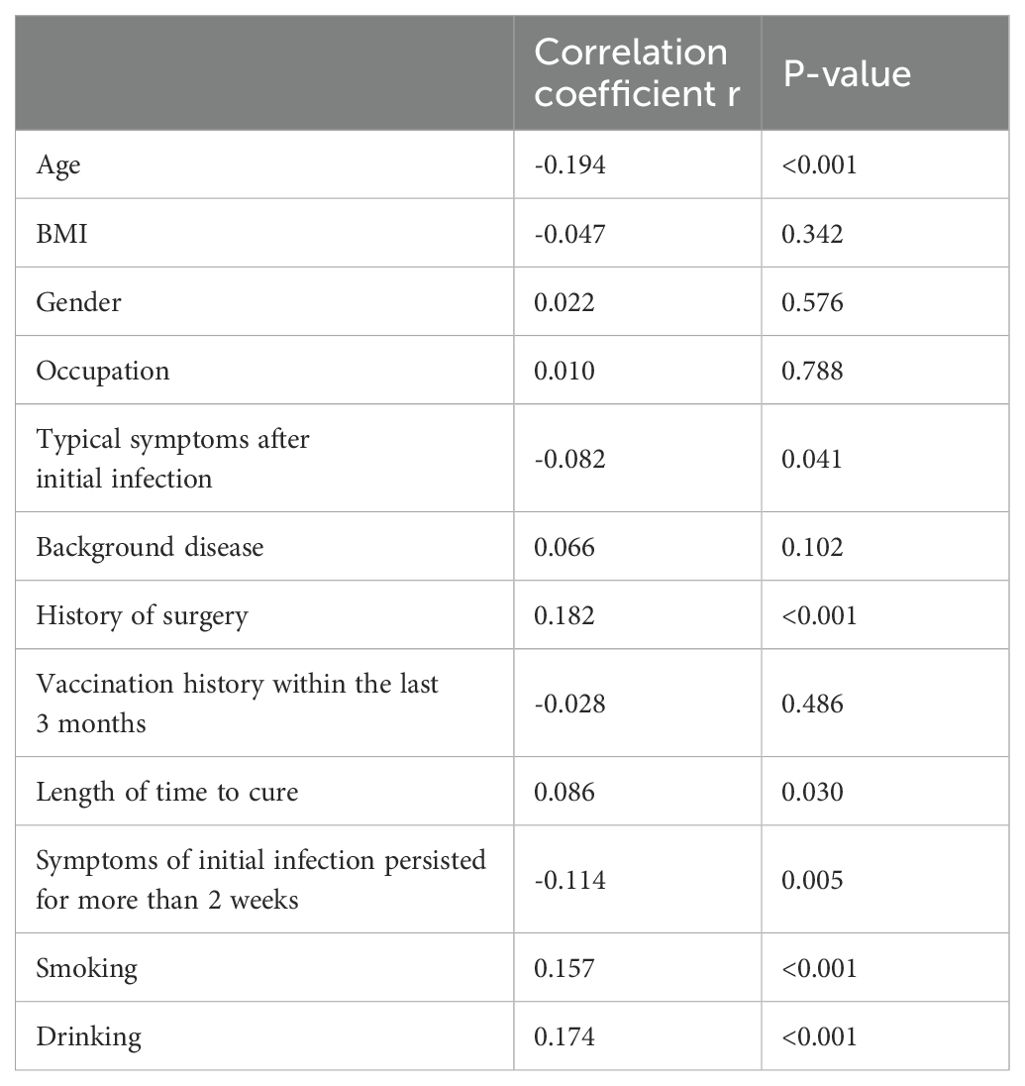
Table 4. Correlation analysis of antibody levels (raw values).
Since occupation had statistical significance in the 2 test, but had no statistical significance in the correlation analysis; The length of cure time was not statistically significant in the 2 test, but was statistically significant in the correlation analysis. The results of the two tests were inconsistent, so it was not included in the multivariate regression analysis. Multivariate logistic regression analysis showed that age (P=0.017), typical symptoms after the first infection (P=0.002), symptoms after 2 weeks after the first infection (P=0.001), history of surgery (P< 0.001), drinking history (P=0.033) and smoking history (P=0.049) were correlated with IgG antibody levels. Age (OR=1.011, 95%CI: 1.002-1.020, P=0.017), history of surgery (OR=4.956, 95%CI: 2.606-9.423, P< 0.001), smoking history (OR=2.089,95%CI: 1.002-4.355, P=0.049) and drinking history (OR=2.214,95%CI: 1.066-4.600, P=0.033) were risk factors affecting antibody levels. Typical symptoms after the first infection (OR=0.224, 95%CI: 0.086-0.579, P=0.002) and symptoms lasting for more than 2 weeks after the first infection (OR=0.432, 95%CI: 0.258-0.723, P=0.001) were protective factors affecting the antibody level. The results are shown in Table 5.

Table 5. Logistic regression analysis.
Fuzhou experienced the first wave of infection peak from December 2022 to January 2023, and the antibody level had a natural decay process from January to March. After that, the second wave and the third wave of infection occurred in May and August of 2023. After one month, serum samples were collected again in June and September of this study. According to the test statistics, although the antibody level of some people increased slightly, the overall IgG antibody level in March, June and September still showed a downward trend, and the results are shown in Figure 1.
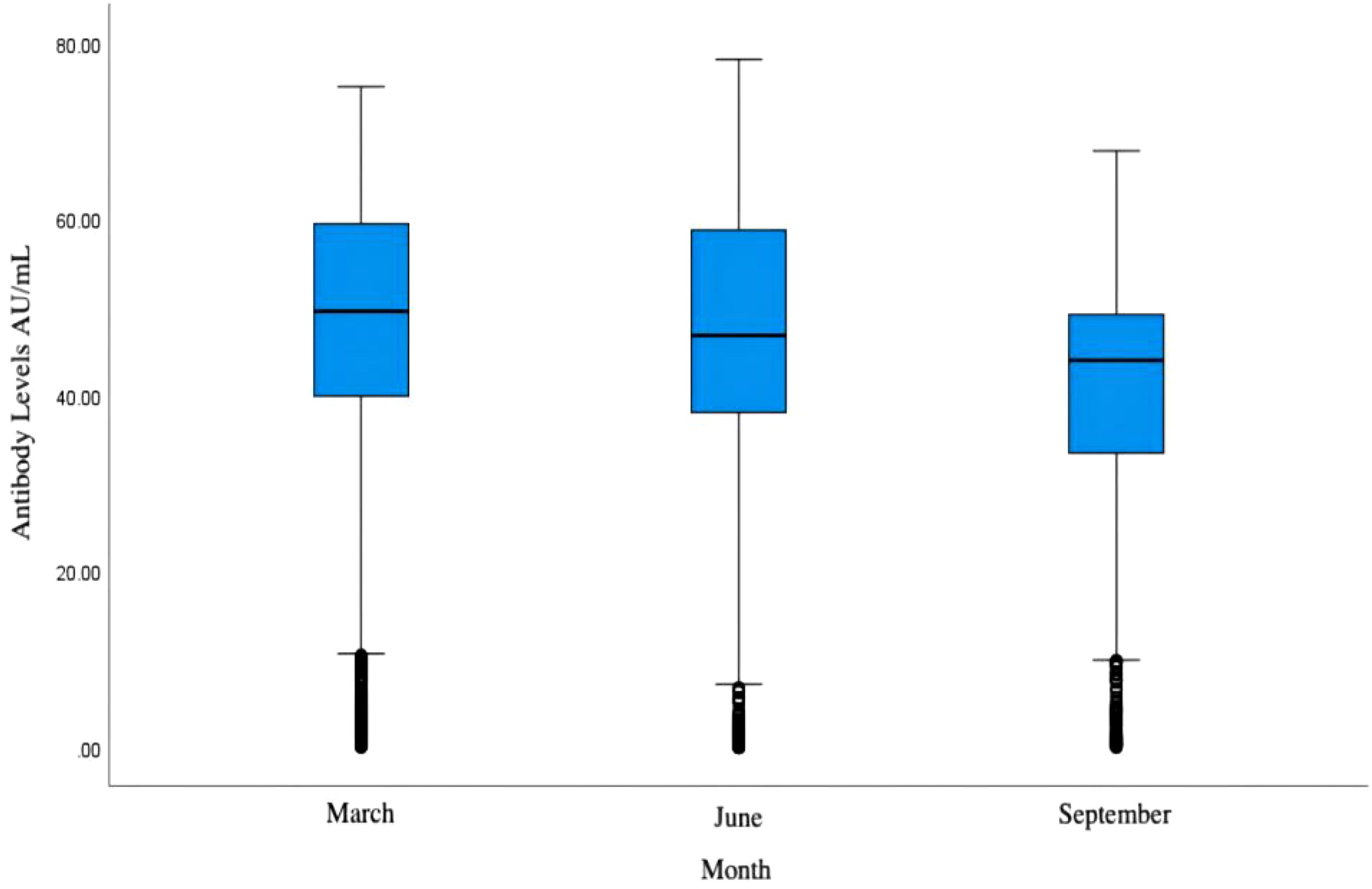
Figure 1. Overall IgG antibody levels of participants in March, June, and September.
Although the community residents in Fuzhou experienced three infection peaks in January, May and August, the total IgG antibody level in March, June and September still showed a downward trend. According to the literature, the median time of specific IgG antibody seroconversion was 12 to 14 days after onset, rapidly increased and reached the peak in the third to fourth weeks, and decreased significantly 8 weeks after discharge (8).
Previous studies focused on antibody responses across different populations, time frames, and vaccination contexts. Our study reported a decline in IgG antibody levels in Fuzhou’s community after infection peaks, with demographic and clinical factors, such as age and smoking, influencing antibody levels. Protective factors included the presence of typical symptoms and prolonged symptoms post-infection. However, Wolszczak-Biedrzycka et al. (9) explored the effect of a third BNT162b2 dose on healthcare workers, showing higher antibody levels in previously infected individuals. This highlighted the booster’s role in enhancing immunity, in contrast to our study, which focused on natural immunity (9). This conclusion was strengthened by another study, showing a stronger antibody response in individuals who received the Pfizer/BioNTech booster compared to AstraZeneca, emphasizing vaccine-induced immunity over natural infection (10).In addition, one study examined the persistence of antibodies in healthcare workers 10 months post-vaccination, finding that prior infection leaded to more stable antibody levels (11). Prior infection and vaccination together resulted in stronger immunity (12). In conclusion, these findings all suggested the importance of considering individual vaccination history in immunity strategies.
Based on the results showing a downward trend in overall antibody levels, the newly produced immune antibodies are not sufficient to compensate for the declining antibody levels, suggesting that without the second and third waves of infection, antibody levels may have fallen more rapidly. Moreover, studies have shown that the duration of natural immunity is not long enough to resist the next variant (13). However, a moderate level of antibodies can protect people from severe damage caused by SARS-CoV-2, so it is necessary to strengthen immunization regularly to maintain the level of immunity (14).
The results of univariate analysis showed that gender, BMI, underlying disease, vaccination history in the past three months, and cure time had no significant effect on the level of antibody protection. The people with old age, history of surgery, smoking history, drinking history, no typical symptoms after the first infection, and symptoms did not last for more than 2 weeks after the first infection in the low antibody group were higher than those in the high antibody group. Although some studies have shown that compared with the vaccination of two doses of the inactivated SARS-CoV-2 vaccine, the vaccination of the third dose of the inactivated SARS-CoV-2 vaccine can significantly increase the levels of IgG antibodies and neutralizing antibodies and induce a higher level of immune protection (15, 16). However, due to the two years of COVID-19 epidemic, according to the national policy, the Chinese people have been generally vaccinated against COVID-19, and the number of people who have received booster shots is currently small. Moreover, the data collected in this study are from December 2022 onwards (because the body does not produce antibodies immediately after COVID-19 vaccine injection, and because of individual differences, Antibodies do not develop 100% of the time after vaccination.) “, while experiencing a large area of infection in January, which may account for the small effect of vaccination on antibody levels in this study.” In addition, some studies have shown that gender, BMI and underlying diseases can affect the antibody level (17–21), but in this study, there is no obvious correlation between gender, BMI and underlying diseases and the antibody level and change of community residents in Fuzhou, which may be confounded by other factors such as age. Whether gender, BMI and underlying diseases are the influencing factors of antibody level needs further detailed analysis.
Multivariate logistic regression model analysis showed that age, surgery history, drinking history, and smoking history were risk factors affecting antibody levels. Age is a risk factor, which may be related to lymphopenia, neutrophilia, inflammation and coagulation related indicators in elderly patients (≥65 years old). Increased neutrophils can lead to the formation of more significant neutrophil extracellular traps in the microvessels of critically ill patients (22, 23), which may be an enhancement factor in the pathogenesis of COVID-19 infection. These activated neutrophils and monocytes can accumulate in multiple organs (lung, heart, kidney, small intestine and liver, etc.), and increase the expression of related pro-inflammatory factors and inflammatory chemokines, thereby causing “cytokine storm” related inflammatory storm and aggravating pathological damage (24). In addition, the levels of IFN-γ and IL-2 in patients with acute COVID-19 (≥55 years old) are low, and the activation of T cells derived from dendritic cells is impaired, which will also lead to a reduced adaptive immune response (25). Surgical trauma has an impact on the immune system: studies have shown that the immunoglobulin level of patients decreases after surgery, and the degree of reduction is closely related to the level of surgical trauma (26). Long-term drinking, alcohol affects the function of adaptive immune response by acting on dendritic cells, T cells and other ways, and weakens the body’s immune response to pathogens on the whole (27). Moreover, alcohol has been shown to affect the signal of IFN and inhibit the body’s immune response to pathogens (28). Cigarette smoke can damage the maturation and function of dendritic cells, including the decreased ability to stimulate T cells and the inhibition of immune response (29). It can also reduce major histocompatibility class I antigen presentation and inhibit the immune response against virus-infected cells by inhibiting the activity of immunoproteasomes (30). Moreover, tobacco contains a variety of harmful chemicals such as nicotine, which can regulate innate and adaptive immune responses by interacting with acetylcholine receptors on the surface of immune cells (31).
In addition, the results of multivariate logistic regression model analysis showed that typical symptoms after the first infection and symptoms 2 weeks after the first infection were protective factors affecting the antibody level. This may be related to the severity of the disease, with typical symptoms after the first infection and symptoms lasting for more than two weeks indicating more severe disease. However, multiple relevant studies have shown that the level of IgG antibodies in patients with severe COVID-19 is higher, and the sustained high levels of specific IgM and IgG antibodies may be closely related to the severity of the disease (32, 33).
Finally, the inconsistency between the chi-square test and the correlation analysis of occupation and length of time to cure may be due to the loss of a part of the data information in the chi-square test analysis, which divided the antibody levels into high and low antibody groups.
This study also has certain limitations. First, the collected samples were randomly selected from community residents in Fuzhou. Although the sample size was large, there was loss to follow-up, incomplete data, and a certain degree of bias. Second, when analyzing the single factor, there were several confounding factors, and there was bias. Thirdly, although this study monitored the dynamic changes of antibody in March, June and September, the monitoring time was not enough. At the same time, only the data of IgG antibody in March were used to analyze the factors affecting serum antibody, which needs to be constantly summarized and improved in the follow-up related research.
Age, history of surgery, smoking and drinking are risk factors for antibody levels. The presence of typical symptoms after the first infection and symptoms 2 weeks after the first infection were protective factors affecting antibody levels. The level of IgG antibody showed a downward trend. Therefore, it is necessary to strengthen immunization against COVID-19 infection regularly.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The ethical research board committee of Fuzhou Center for Disease Control and Prevention (Approval No. IRB2023002) approved the research. The need for individual informed consents is waived by the institution/review board due to the fact that exclusively utilized anonymized aggregated data was used and did not involve any individual subjects.
XZhe: Formal Analysis, Validation, Writing – original draft. QC: Writing – original draft. QL: Writing – review & editing. XZha: Conceptualization, Methodology, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Special Fund for Fujian Province Major Scientific Research Special Project (2022ZD01001), Fujian Province Science and Technology Plan Guiding Project (2022D021) and Major Scientific Research on Health of Fujian (2021ZD0101).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sadeghi Dousari A, Taati Moghadam M, Satarzadeh N. COVID-19 (Coronavirus disease 2019): A new coronavirus disease. Infect Drug Resist. (2020) 13:2819–28. doi: 10.2147/IDR.S259279
2. Hu B, Guo H, Zhou P, Shi ZL. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol. (2021) 19:141–54. doi: 10.1038/s41579-020-00459-7
3. Movsisyan M, Truzyan N, Kasparova I, Chopikyan A, Sawaqed R, Bedross A, et al. Tracking the evolution of anti-SARS-CoV-2 antibodies and long-term humoral immunity within 2 years after COVID-19 infection. Sci Rep. (2024) 14:13417. doi: 10.1038/s41598-024-64414-9
4. Long QX, Tang XJ, Shi QL, Li Q, Deng HJ, Yuan J, et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat Med. (2020) 26:1200–4. doi: 10.1038/s41591-020-0965-6
5. Gaebler C, Wang Z, Lorenzi JCC, Muecksch F, Finkin S, Tokuyama M, et al. Evolution of antibody immunity to SARS-CoV-2. Nature. (2021) 591:639–44. doi: 10.1038/s41586-021-03207-w
6. Lumley SF, O'Donnell D, Stoesser NE, Matthews PC, Howarth A, Hatch SB, et al. Antibody status and incidence of SARS-CoV-2 infection in health care workers. N Engl J Med. (2021) 384:533–40. doi: 10.1056/NEJMoa2034545
7. Available online at: https://weekly.chinacdc.cn/fileCCDCW/cms/news/info/upload/ccdcw-surveillance-202212-202301-cn.pdf (Accessed January 25, 2023).
8. Seow J, Graham C, Merrick B, Acors S, Pickering S, Steel KJA, et al. Longitudinal observation and decline of neutralizing antibody responses in the three months following SARS-CoV-2 infection in humans. Nat Microbiol. (2020) 5(12):1598–601. doi: 10.1038/s41564-020-00813-8
9. Wolszczak-Biedrzycka B, Bieńkowska A, Cieślikiewicz B, Smolińska-Fijołek E, Biedrzycki G, Dorf J. The effect of the third dose of the BNT162b2 vaccine on anti-SARS-CoV-2 spike antibody levels in healthcare workers with and without COVID-19 infection. Ann Med. (2023) 55(1):722–32. doi: 10.1080/07853890.2023.2182907
10. Wolszczak Biedrzycka B, Bieńkowska A, Smolińska-Fijołek E, Biedrzycki G, Dorf J. The influence of two priming doses of different anti-COVID-19 vaccines on the production of anti-SARS-CoV-2 antibodies after the administration of the pfizer/bioNTech booster. Infect Drug Resist. (2022) 15:7811–21. doi: 10.2147/IDR.S390351
11. Wolszczak-Biedrzycka B, Bieńkowska A, Zaborowska JE, Smolińska-Fijołek E, Biedrzycki G, Dorf J. Anti-SARS-CoV-2S antibody levels in healthcare workers 10 months after the administration of two BNT162b2 vaccine doses in view of demographic characteristic and previous COVID-19 infection. Vaccines (Basel). (2022) 10:741. doi: 10.3390/vaccines10050741
12. Wolszczak-Biedrzycka B, Bieńkowska A, Dorf J. Assessment of post-vaccination antibody response eight months after the administration of BNT1622b2 vaccine to healthcare workers with particular emphasis on the impact of previous COVID-19 infection. Vaccines (Basel). (2021) 9:1508. doi: 10.3390/vaccines9121508
13. Brits E, Adepoju P. Omicron potential under close scrutiny. Nature. (2021) 10:197–9. doi: 10.1038/d44148-021-00119-9
14. World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19 6 January 2022. Geneva: World Health Organization (2022). Available at: https://www.who.int/multi-media/details/whopress-conference-on-coronavirus-disease.
15. Zhang H, Jia Y, Ji Y, Cong X, Liu Y, Yang R, et al. Inactivated vaccines against SARS-CoV-2: neutralizing antibody titers in vaccine recipients. Front Microbiol. (2022) 13:816778. doi: 10.3389/fmicb.2022.816778
16. Ng HM, Lei CL, Fu S, Li E, Leong SI, Nip CI, et al. Heterologous vaccination with inactivated vaccine and mRNA vaccine augments antibodies against both spike and nucleocapsid proteins of SARS-CoV-2: a local study in Macao. Front Immunol. (2023) 14:1131985. doi: 10.3389/fimmu.2023.1131985
17. Nie J, Li Q, Wu J, Zhao C, Hao H, Liu H, et al. Quantification of SARS-CoV-2 neutralizing antibody by a pseudotyped virus-based assay. Nat Protoc. (2020) 15:3699–715. doi: 10.1038/s41596-020-0394-5
18. Hastert FD, Henss L, von Rhein C, Gerbeth J, Wieters I, Borgans F, et al. Longitudinal analysis of coronavirus-neutralizing activity in COVID-19 patients. Viruses. (2022) 14:882. doi: 10.3390/v14050882
19. Muecksch F, Wise H, Batchelor B, Squires M, Semple E, Richardson C, et al. Longitudinal serological analysis and neutralizing antibody levels in coronavirus disease 2019 convalescent patients. J Infect Dis. (2021) 223:389–98. doi: 10.1093/infdis/jiaa659
20. Yung CF, Saffari SE, Mah SYY, Tan NWH, Chia WN, Thoon KC, et al. Analysis of neutralizing antibody levels in children and adolescents up to 16 months after SARS-CoV-2 infection. JAMA Pediatr. (2022) 176:1142–3. doi: 10.1001/jamapediatrics.2022.3072
21. Lei Q, Hou H, Yu C, Zhang Y, Ndzouboukou JB, Lin X, et al. Kinetics of neutralizing antibody response underscores clinical COVID-19 progression. J Immunol Res. (2021) 2021:9822706. doi: 10.1155/2021/9822706
22. Ren SY, Wang WB, Gao RD, Zhou AM. Omicron variant ( B.1.1. 529) of SARS-CoV-2: Mutation, infectivity, transmission, and vaccine resistance. World J Clin cases. (2022) 10(1):1–11. doi: 10.12998/wjcc.v10.i1.1
23. Liao M, Liu Y, Yuan J, Wen Y, Xu G, Zhao J, et al. Single-cell landscape of bronchoalveolar immune cells in patients with COVID-19. Nat Med. (2020) 26:842–4. doi: 10.1038/s41591-020-0901-9
24. Zhou R, To KK, Wong YC, Liu L, Zhou B, Li X, et al. Acute SARS-CoV-2 infection impairs dendritic cell and T cell responses. Immunity. (2020) 53:864–77. doi: 10.1016/j.immuni.2020.07.026
25. Lu DB, Liu XP, Hu LZ. Effect of laparoscopic and open surgery on rectal cancer and its effect on the stress response,immune function and life quality of patients. J Hainan Med Univ. (2016) 22:289–291+295. doi: 10.13210/j.cnki.jhmu.20151030.001
26. Xu GL, Wang X, Zhang WH. Research progress of lung immune cell injury induced by alcohol exposure. J Toxicol. (2017) 31:314–7. doi: 10.16421/j.cnki.1002-3127.2017.04.014
27. Edsen-Moore MR, Fan J, Ness KJ, Marietta JR, Cook RT, Schlueter AJ. Effects of chronic ethanol feeding on murine dendritic cell numbers, turnover rate, and dendropoiesis. Alcoholism: Clin Exp Res. (2010) 32(7):1309–20. doi: 10.1111/j.1530-0277.2008.00699.x
28. Robbins CS, Franco F, Mouded M, Cernadas M, Shapiro SD. Cigarette smoke exposure impairs dendritic cell maturation and T cell proliferation in thoracic lymph nodes of mice. J Immunol. (2008) 180(10):6623–8. doi: 10.4049/jimmunol.180.10.6623
29. Kammerl IE, Dann A, Mossina A, Brech D, Lukas C, Vosyka O, et al. Impairment of immunoproteasome function by cigarette smoke and in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. (2016) 193(11):1230–41. doi: 10.1164/rccm.201506-1122OC
30. Sopori M. Effects of cigarette smoke on the immune system. Nat Rev Immunol. (2002) 2:372–7. doi: 10.1038/nri803
31. Hou H, Wang T, Zhang B, Luo Y, Mao L, Wang F, et al. Detection of IgM and IgG antibodies in patients with coronavirus disease 2019. Clin Transl Immunol. (2020) 9:e01136. doi: 10.1002/cti2.1136
32. Azkur AK, Akdis M, Azkur D, Sokolowska M, van de Veen W, Brüggen MC, et al. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy. (2020) 75:1564–81. doi: 10.1111/all.14364
Keywords: SARS-CoV-2, community residents, serum antibody, influencing factors, logistic regression
Citation: Zheng X, Chen Q, Liao Q and Zhang X (2025) Tracking the evolution of serum antibody levels and influencing factors post-SARS-CoV-2 infection among community residents in Fuzhou City. Front. Immunol. 16:1533102. doi: 10.3389/fimmu.2025.1533102
Received: 23 November 2024; Accepted: 12 March 2025;
Published: 31 March 2025.
Edited by:
Ronaldo Celerino Da Silva, Oswaldo Cruz Foundation, BrazilReviewed by:
Stelvio Tonello, University of Eastern Piedmont, ItalyCopyright © 2025 Zheng, Chen, Liao and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoyang Zhang, ZGF3bnN1bnpAMTI2LmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.