 Hesham Abboud1*
Hesham Abboud1* Adnan Subei2Buse Sengul3Robert K. Shin4Paige Goulette5Rosemarie Walch5Jeanie Coté5Robert Pace5
Adnan Subei2Buse Sengul3Robert K. Shin4Paige Goulette5Rosemarie Walch5Jeanie Coté5Robert Pace5 Ahmed Z. Obeidat6Lisa Ferayorni7Shervin Gholizadeh7
Ahmed Z. Obeidat6Lisa Ferayorni7Shervin Gholizadeh7- 1Multiple Sclerosis and Neuroimmunology Program, University Hospitals Cleveland Medical Center, Case Western Reserve University, Cleveland, OH, United States
- 2Neurology Consultants of Dallas, Dallas, TX, United States
- 3Neurology Department, Memorial Healthcare, Hollywood, FL, United States
- 4Departments of Neurology and Ophthalmology, University of Virginia, Charlottesville, VA, United States
- 5Neurology Department, Memorial Healthcare, Owosso, MI, United States
- 6Department of Neurology, Medical College of Wisconsin, Milwaukee, WI, United States
- 7Genentech, Inc., South San Francisco, CA, United States
Objectives: This case series describes adults with aquaporin 4 immunoglobulin G–seropositive (AQP4-IgG+) neuromyelitis optica spectrum disorder (NMOSD) who switched treatment from eculizumab to satralizumab.
Methods: Case information for patients with AQP4-IgG+ NMOSD who received satralizumab for ≥6 months was obtained from US healthcare providers from April 2022 to January 2024. Patient characteristics, examination findings, diagnostic test results, treatment response, and adverse events were recorded.
Results: Among the 5 patients (4 women and 1 man) included, ages ranged from 32 to 81 years and 4 patients self-identified as Black/African American and 1 as White. Time since confirmed NMOSD diagnosis ranged from 1 to 14 years. The reasons for initiating satralizumab were route of administration/patient preference (n=3) and inadequate disease control with eculizumab (n=2). The duration of satralizumab treatment was 10 to 31 months. All 5 patients were relapse-free with satralizumab, and adverse events they experienced were primarily asymptomatic laboratory abnormalities.
Discussion: In this retrospective case series, satralizumab was effective and well tolerated in patients with NMOSD who switched from eculizumab due to route of administration/patient preference or inadequate disease control. These outcomes align with the long-term efficacy and safety outcomes with satralizumab in the phase 3 SAkura clinical trials.
1 Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is an autoimmune neuroinflammatory disease that primarily affects the optic nerves and spinal cord and may lead to vision loss, motor and sensory impairment, and permanent neurological disability (1). Four therapies have been approved by the US Food and Drug Administration for the treatment of adults with aquaporin 4 immunoglobulin G–seropositive (AQP4-IgG+) NMOSD. Eculizumab (2) and ravulizumab (3) are monoclonal antibodies targeting C5 complement protein and administered by intravenous (IV) infusion; eculizumab is administered weekly for the first 5 infusions and then every 2 weeks, and ravulizumab is administered every 2 weeks for 2 infusions and then every 4-8 weeks. Inebilizumab, an anti-CD19 B-cell–depleting antibody is administered by IV infusion every 2 weeks for 2 infusions and then every 6 months (4). Satralizumab, a humanized IgG2 monoclonal recycling antibody against the interleukin 6 receptor, is subcutaneously administered every 2 weeks for 3 injections and then every 4 weeks thereafter (5).
Satralizumab was developed specifically for the treatment of NMOSD and has demonstrated safety and efficacy in patients with AQP4-IgG+ NMOSD in 2 placebo-controlled, phase 3 clinical trials (SAkuraSky [NCT02028884] and SAkuraStar [NCT02073279]) (6, 7); long-term safety and efficacy were sustained in open-label extension periods (8, 9). The phase 3 satralizumab clinical trials excluded patients treated with eculizumab before enrollment, which limits the understanding of the safety and effectiveness of switching between approved therapies. Data on NMOSD treatment transitions are limited, particularly real-world data on switches between approved therapies with different mechanisms of action, which may have clinical implications. This case series aims to illustrate the real-world experience of US patients with AQP4-IgG+ NMOSD who transitioned from eculizumab to satralizumab and to reveal insights into clinical outcomes and safety profiles observed outside of controlled trial settings.
2 Methods
Patient information was collected from US healthcare providers between April 1, 2022, and January 31, 2024. Patients with AQP4-IgG+ NMOSD who received eculizumab followed by satralizumab for ≥6 months were included. The term switch refers to the transition in maintenance treatment from eculizumab to satralizumab, with no specified minimum or maximum amount of time between treatments. All patients who met the inclusion criteria were included irrespective of the clinical outcomes or patient experience. Patients provided written consent for the publication of their case information. Patient characteristics, examination findings, diagnostic test results, treatment response, and adverse events (AEs) were recorded.
3 Case reports
Five patients (4 women and 1 man; median [range] age 56 [32-81] years) were included. Four patients self-identified as Black/African American and 1 as White (Table 1). The median (range) time from confirmed AQP4-IgG+ NMOSD diagnosis was 4 (1-14) years. The mean (SD) expanded disability scale score before receiving satralizumab was 4.6 (3.0). Before treatment with eculizumab, 3 patients received preventative maintenance therapies and 2 did not (Figure 1). The median (range) duration of eculizumab treatment was 10 (5-22) months.

Table 1. Demographic characteristics, clinical characteristics, and treatment history of patients with AQP4-IgG+ NMOSD who switched to satralizumab after eculizumaba.
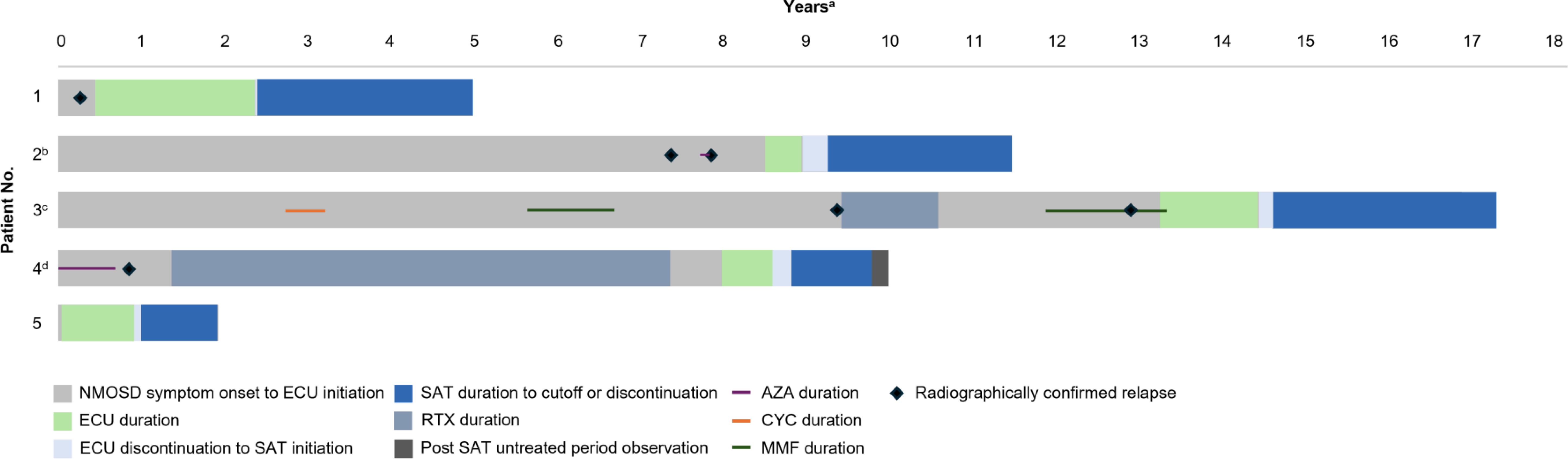
Figure 1. Timeline of NMOSD Treatments and Radiographically Confirmed Relapses. AZA, azathioprine; CYC, cyclophosphamide, ECU, eculizumab; MMF, mycophenolate mofetil; NMOSD, neuromyelitis optica spectrum disorder; RTX, rituximab; SAT, satralizumab. aLength of bar indicates time from symptom onset to data cutoff. bPatient received AZA for a brief period; the exact duration and timing are unknown. cExact date of discontinuation of ECU unknown. Patient had 4 months of interrupted SAT treatment due to insurance issues; exact timing of interruption unknown. dPatient received AZA with long-term corticosteroid taper. Patient died due to stage IV cervical cancer 2 months after last dose of SAT.
The primary reasons for transitioning from eculizumab to satralizumab included patient preference for administration route or frequency of satralizumab or loss of venous access (Patients 1, 2, 5) and inadequate disease control (Patients 3, 4) (Table 1). Patient 3 received eculizumab for 14 months, during which they experienced a progression in right arm dysfunction and a lack of appetite. The patient perceived right arm dysfunction as inadequate disease control; however, a relapse was not confirmed through radiographic evidence. Patient 4 exhibited symptoms of optic neuritis 5 months after initiating eculizumab. An MRI could not be conducted, and an ophthalmological evaluation was not obtained to confirm this as a relapse.
Median (range) time between discontinuation of eculizumab and initiation of satralizumab was 9 (2-17) weeks (Figure 1). The median (range) duration of satralizumab treatment was 25 (10-31) months. At the analysis cutoff date, all 5 patients had been treated with satralizumab for a duration at least as long as they had received eculizumab (Patient 5) or longer (Patients 1-4). No patients received bridging corticosteroids during the transition to satralizumab treatment, and all 5 patients received satralizumab as a monotherapy.
Patients 1, 2, 3, and 4 had ≥1 radiographically confirmed relapse before receiving eculizumab (Figure 1). Patient 4 experienced optic neuritis symptoms while receiving eculizumab, but this possible relapse was not confirmed with objective measures. After switching to satralizumab, all 5 patients were relapse-free and clinically stable or improved (Table 2).
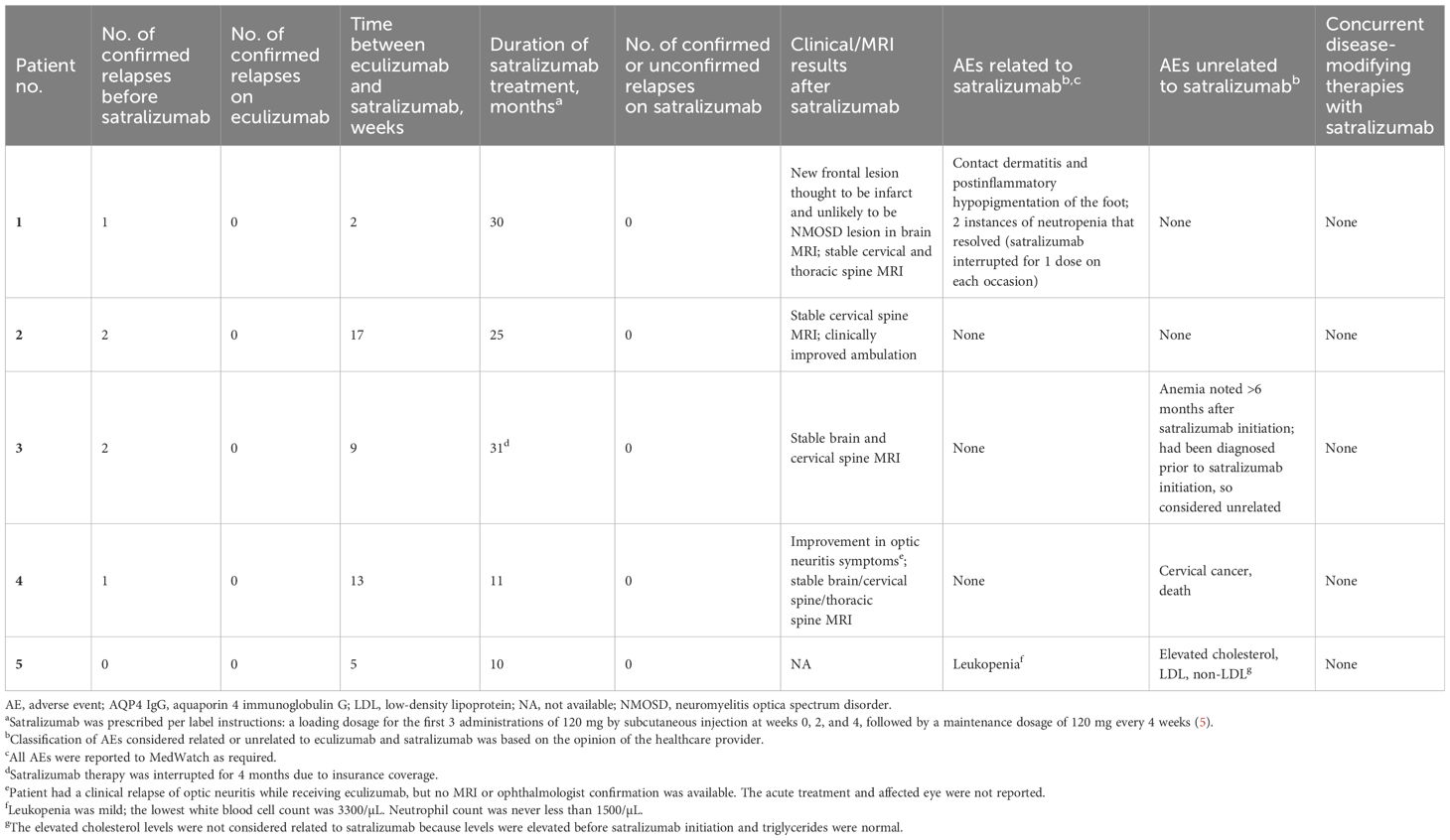
Table 2. Effectiveness and safety data for satralizumab in patients with AQP4-IgG+ NMOSD who switched to satralizumab after eculizumab.
AEs related to satralizumab, as determined by their healthcare providers, were reported by 2 patients (Table 2). Patient 1 had neutropenia twice, at 2 months and at 1 year after initiation; on each occasion, satralizumab was temporarily interrupted for 1 dose, the neutrophil count increased at repeat testing 1 month later, and satralizumab was resumed. This patient also had contact dermatitis with postinflammatory hypopigmentation. Patient 5 had leukopenia at 1 month and 3 months after satralizumab initiation without interruption in satralizumab dosing. Patient 4 received satralizumab for 11 months with no AEs; however, the patient died 2 months after discontinuation of satralizumab due to stage IV cervical cancer.
4 Discussion
This case series presents the clinical courses of 5 US patients with AQP4-IgG+ NMOSD who switched from eculizumab to satralizumab in real-world practice because of preferred route/frequency of administration (including loss of venous access) or inadequate disease control with eculizumab. After switching to satralizumab monotherapy, all patients were relapse-free, and AEs were primarily asymptomatic laboratory abnormalities. At data cutoff, 4 patients were receiving satralizumab, 3 for ≥25 months. These results are consistent with a case report of a patient who had no reported relapses or AEs after switching from eculizumab to satralizumab (10).
Patients with NMOSD may switch from one treatment to another due to lack of effective disease control or AEs as well as route of administration preference, medical insurance coverage, and real-world access (11). Uncontrolled disease activity is important in predicting treatment change in patients with NMOSD (12). Switching between NMOSD treatments due to disease activity, tolerability, or nonmedical reasons is common, with reason for switch influencing risk of disease advancement (11). Understanding reasons for and outcomes after switching between approved therapies may aid in developing optimum treatment strategies in the clinical management of NMOSD.
Among a panel of NMOSD experts, the most common considerations for choosing therapies after efficacy and safety were disease or relapse severity and patient preference for treatment administration (13). Additionally, these panel experts agreed that the choice between the NMOSD therapies may be informed by patient preferences for dosing frequency and route of administration, along with acceptance of safety risks (13). In this case series, patients 1 and 5 switched to satralizumab due to a preference for the less-frequent treatment and self-administered therapy, respectively. In a US cross-sectional survey of people with NMOSD, the highest proportions of patients were concerned with treatment effectiveness and AEs; administration concerns were also reported, including discomfort during administration and treatment inconvenience (14).
High rates of disease reactivation and relapse have been documented in the first 3 months following discontinuation of eculizumab (15). In our case series, the interval between eculizumab discontinuation and satralizumab initiation ranged from 2 to 17 weeks, yet no relapses were observed after discontinuation of eculizumab. Literature suggests that when switching between approved therapies, the new treatment can be started immediately after cessation of the previous one, taking into account the mechanism and onset of efficacy of the new treatment (13). In this series, satralizumab was effective, regardless of the duration between eculizumab discontinuation and satralizumab initiation and whether patients were clinically stable or had experienced a possible relapse during eculizumab treatment. It is important to note that patient 3 switched due to their subjective sense of disease progression but without objective evidence of relapse. In that case, measuring serum CH50 may have been helpful to evaluate the biological efficacy of eculizumab but it was not done, limiting a definitive conclusion regarding disease activity. Future eculizumab switches due to efficacy concerns could benefit from such measurement. Importantly, switching from eculizumab to satralizumab did not increase infection risk or cause unexpected AEs.
This study’s limitations include the small number of patients, partially missing data, lack of a control group, and retrospective design. The aim of this report was to enhance real-world data on treatment options in NMOSD; our findings should not be construed or interpreted as evidence of superiority or inferiority of either treatment in the absence of head-to-head clinical trials. We understand the importance of larger data sets in strengthening the conclusions drawn. Currently, there are no publications regarding switches from eculizumab to satralizumab or from eculizumab to any other treatment in NMOSD. Given the rarity of these switches—owing largely to the success of eculizumab in managing the disease—we believed it was imperative to report these cases. This information could potentially assist treating physicians in making informed decisions. We intend to report additional cases as they occur, though such switches remain uncommon. Future studies should also evaluate biomarker changes during treatment switches. Nevertheless, this case series provides valuable real-world data on patients with AQP4-IgG+ NMOSD who switched from eculizumab to satralizumab.
5 Conclusions
In this retrospective case series, satralizumab was effective and well tolerated in patients with NMOSD who switched from eculizumab treatment. All patients were relapse-free, and no major AEs related to satralizumab were reported. These outcomes align with the long-term efficacy and safety outcomes observed in satralizumab clinical trials.
Data availability statement
The datasets presented in this article are not readily available because of ethical and privacy restrictions. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants or patients/participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
HA: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. AS: Data curation, Investigation, Writing – review & editing. BS: Data curation, Investigation, Writing – review & editing. RS: Data curation, Investigation, Writing – review & editing. PG: Data curation, Investigation, Writing – review & editing. RW: Data curation, Investigation, Writing – review & editing. JC: Data curation, Investigation, Writing – review & editing. RP: Data curation, Investigation, Writing – review & editing. AO: Data curation, Investigation, Writing – review & editing. LF: Conceptualization, Data curation, Formal analysis, Writing – original draft, Writing – review & editing. SG: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Open access fees were funded by Genentech/Roche.
Acknowledgments
We would like to thank the patients who participated in this case series as well as Chris Drahaim, Vanessa Di Felice, Jasmin Graziano, Idan Hannawa, Kerri Lucia, Kaylan Fenton, and Lynn Wheeler for their assistance in obtaining case information.
Conflict of interest
HA: Consultant for Biogen, Genentech, Inc., Bristol Myers Squibb, Alexion, Horizon, Cycle Pharma, and Alpine Pharma. Receives research support from Novartis, Sanofi-Genzyme, Bristol Myers Squibb, Genentech, Inc., UCB, and the Guthy-Jackson Charitable Foundation. Served as an assistant editor for the Neurology Journal. Receives royalties from UpToDate. AS: Speaker for TG Therapeutics, Bristol Myers Squibb. BS: Served on advisory boards for Genentech, EMD Serono, and Horizon. Dr. Sengul has received personal compensation for serving on speakers bureaus for Biogen and EMD Serono and served on the steering committee for EMD Serono. RS: Received personal compensation as a consultant or speaker for Alexion, Biogen, Bristol Myers Squibb, EMD Serono, Genentech, Horizon, Novartis, Sanofi Genzyme, and TG Therapeutics. PG, RW, JC, and RP: Consultant for Genentech/Roche, Bristol Myers Squibb, Sanofi, Horizon, Alexion. Speakers bureau for Alexion, Horizon, Biogen, Bristol Myers Squibb, EMD Serono. The institution of Drs. Walch, Goulette, Cote, and Pace has received research support from Genentech/Roche, Sanofi, EMD Serono, and Novartis. Research support from TG Therapeutics. AO: Speaker or consultant for Alexion Pharmaceuticals, Amgen, Banner Life Sciences, BD Biosciences, Biogen, Biologix, Bristol Myers Squibb, Celgene, EMD Serono, Genentech, Inc., GW Pharma, Jazz Pharmaceuticals, Horizon Therapeutics, Novartis, Sandoz Pharmaceuticals, Sanofi/Genzyme, TG Therapeutics, and Viela Bio and honoraria from Medscape, WebMD, and MJH Life Sciences. LF and SG: Employees of Genentech, Inc., and shareholders in F. Hoffmann-La Roche Ltd.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Wingerchuk DM, Lucchinetti CF. Neuromyelitis optica spectrum disorder. N Engl J Med. (2022) 387:631–9. doi: 10.1056/NEJMra1904655
2. Soliris (eculizumab). Prescribing information (2024). Alexion Pharmaceuticals. Available online at: https://alexion.com/Documents/Soliris_USPI.pdf (Accessed July 29, 2024).
3. Ultomiris (ravulizumab-cwvz). Prescribing information (2024). Alexion Pharmaceuticals. Available online at: https://alexion.com/Documents/Ultomiris_USPI.pdf (Accessed July 29, 2024).
4. Uplizna (inebilizumab-cdon). Prescribing information (2021). Horizon Therapeutics. Available online at: https://www.hzndocs.com/Uplizna-Prescribing-Information.pdf (Accessed July 29, 2024).
5. Enspryng (satralizumab-mwge). Prescribing information (2022). Genentech, Inc. Available online at: https://www.gene.com/download/pdf/enspryng_prescribing.pdf (Accessed July 29, 2024).
6. Yamamura T, Kleiter I, Fujihara K, Palace J, Greenberg B, Zakrzewska-Pniewska B, et al. Trial of satralizumab in neuromyelitis optica spectrum disorder. N Engl J Med. (2019) 381:2114–24. doi: 10.1056/NEJMoa1901747
7. Traboulsee A, Greenberg BM, Bennett JL, Szczechowski L, Fox E, Shkrobot S, et al. Safety and efficacy of satralizumab monotherapy in neuromyelitis optica spectrum disorder: a randomised, double-blind, multicentre, placebo-controlled phase 3 trial. Lancet Neurol. (2020) 19:402–12. doi: 10.1016/S1474-4422(20)30078-8
8. Kleiter I, Traboulsee A, Palace J, Yamamura T, Fujihara K, Saiz A, et al. Long-term efficacy of satralizumab in AQP4-IgG-seropositive neuromyelitis optica spectrum disorder from SAkuraSky and SAkuraStar. Neurol Neuroimmunol Neuroinflamm. (2023) 10(1):e200071. doi: 10.1212/NXI.0000000000200071
9. Yamamura T, Weinshenker B, Yeaman MR, De Seze J, Patti F, Lobo P, et al. Long-term safety of satralizumab in neuromyelitis optica spectrum disorder (NMOSD) from SAkuraSky and SAkuraStar. Mult Scler Relat Disord. (2022) 66:104025. doi: 10.1016/j.msard.2022.104025
10. Funakoshi K, Suzuki K. A safe change from eculizumab to satralizumab in a patient with neuromyelitis optica spectrum disorder. Neurol Sci. (2023) 44:1097–8. doi: 10.1007/s10072-022-06495-w
11. Okuda DT, Moog TM, McCreary M, Cook K, Burgess KW, Smith AD. Treatment transitions in neuromyelitis optica spectrum disorder increase risk for disease advancement. Mult Scler Relat Disord. (2023) 79:105041. doi: 10.1016/j.msard.2023.105041
12. Gholizadeh S, Exuzides A, Lewis KE, Palmer C, Waltz M, Rose JW, et al. Clinical and epidemiological correlates of treatment change in patients with NMOSD: insights from the CIRCLES cohort. J Neurol. (2023) 270:2048–58. doi: 10.1007/s00415-022-11529-6
13. Paul F, Marignier R, Palace J, Arrambide G, Asgari N, Bennett JL, et al. International Delphi consensus on the management of AQP4-IgG+ NMOSD: recommendations for eculizumab, inebilizumab, and satralizumab. Neurol Neuroimmunol Neuroinflamm. (2023) 10(4):e2000124. doi: 10.1212/NXI.0000000000200124
14. Beekman J, Keisler A, Pedraza O, Haramura M, Gianella-Borradori A, Katz E, et al. Neuromyelitis optica spectrum disorder: patient experience and quality of life. Neurol Neuroimmunol Neuroinflamm. (2019) 6:e580. doi: 10.1212/NXI.0000000000000580
Keywords: NMOSD, satralizumab, eculizumab, AQP4, case series
Citation: Abboud H, Subei A, Sengul B, Shin RK, Goulette P, Walch R, Coté J, Pace R, Obeidat AZ, Ferayorni L and Gholizadeh S (2025) Switch from eculizumab to satralizumab in aquaporin 4 immunoglobulin G–seropositive neuromyelitis optica spectrum disorder: a case series report. Front. Immunol. 15:1526563. doi: 10.3389/fimmu.2024.1526563
Received: 12 November 2024; Accepted: 26 December 2024;
Published: 10 January 2025.
Edited by:
Moussa Antoine Chalah, GHU Paris Psychiatrie et Neurosciences, FranceReviewed by:
Manabu Araki, Kawakita General Hospital, JapanTomoko Okamoto, National Center of Neurology and Psychiatry, Japan
Copyright © 2025 Abboud, Subei, Sengul, Shin, Goulette, Walch, Coté, Pace, Obeidat, Ferayorni and Gholizadeh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hesham Abboud, SGVzaGFtLmFiYm91ZEB1aGhvc3BpdGFscy5vcmc=