 María Queralt Salas1*
María Queralt Salas1* María Teresa Solano1Mónica Baile González2Marina Acera Gómez2Laura Fox3María del Mar Pérez Artigas3Ana Santamaría4María del Carmen Quintela González4Andrés Sánchez Salinas5Joaquina M. Salmerón Camacho5Verónica Illana Álvaro6Zahra Abdallahi-Lefdil6Javier Cornago Navascues7Laura Pardo7Sara Fernández-Luis8Leddy Patricia Vega Suárez8
María Teresa Solano1Mónica Baile González2Marina Acera Gómez2Laura Fox3María del Mar Pérez Artigas3Ana Santamaría4María del Carmen Quintela González4Andrés Sánchez Salinas5Joaquina M. Salmerón Camacho5Verónica Illana Álvaro6Zahra Abdallahi-Lefdil6Javier Cornago Navascues7Laura Pardo7Sara Fernández-Luis8Leddy Patricia Vega Suárez8 Sara Villar9Patricia Beorlegui-Murillo9Albert Esquirol10Isabel Izquierdo García11Sonia Rodríguez González12
Sara Villar9Patricia Beorlegui-Murillo9Albert Esquirol10Isabel Izquierdo García11Sonia Rodríguez González12 Alberto Mussetti12
Alberto Mussetti12 Esperanza Lavilla13Javier Lopez-Marín14Silvia Filaferro15Ángel Cedillo15
Esperanza Lavilla13Javier Lopez-Marín14Silvia Filaferro15Ángel Cedillo15 Leyre Bento15,16
Leyre Bento15,16 Anna Sureda12,15
Anna Sureda12,15- 1Unidad de Trasplante de Progenitores Hematopoyéticos, Servicio de Hematología, Hospital Clínic de Barcelona, Barcelona, Spain
- 2Servicio de Hematología, Complejo Asistencial Universitario de Salamanca/IBSAL, Salamanca, Spain
- 3Departamento de Hematología, Hospital Universitari Vall d’Hebron, Barcelona, Spain
- 4Departamento de Hematología, Hospital Álvaro Cunqueiro, Vigo, Pontevedra, Spain
- 5Unidad de Trasplante de Progenitores Hematopoyéticos, H.C.U. Virgen de la Arrixaca, Murcia, Spain
- 6Departamento de Hematología, Hospital Universitario de la Princesa, Madrid, Spain
- 7Departamento de Hematología, Hospital Universitario Fundación Jiménez Díaz, Madrid, Spain
- 8Unidad de Trasplante de Progenitores Hematopoyéticos, Servicio de Hematología, Hospital Universitario Marqués de Valdecilla, Santander, Spain
- 9Departamento de Hematología, Clínica Universidad de Navarra, Pamplona, Spain
- 10Servicio de Hematología, Hospital de la Santa Creu i Sant Pau, IIB-Sant Pau and Jose Carreras Leukemia Research Institute, Universitat Autonoma of Barcelona, Barcelona, Spain
- 11Departamento de Hematología, Hospital Miguel Servet, Zaragoza, Spain
- 12Institut Català d’Oncologia - Hospital Duran i Reynals, IDIBELL, Universitat de Barcelona, Barcelona, Spain
- 13Servicio de Hematología, Hospital Universitario Lucus Augusti, Lugo, Spain
- 14Hospital Universitario de Alicante, Alicante, Spain
- 15Grupo Español de Trasplante de Progenitores Hematopoyéticos y Terapia Celular, Madrid, Spain
- 16Departamento de Hematología, Hospital Universitario Son Espases, Palma de Mallorca, Spain
Introduction: This multicenter prospective study sponsored by the Grupo Español de Transplante Hematopoyético y Terapia Celular (GETH-TC) explores the use of frailty assessments in allo-HCT candidates.
Methods: Frailty was measured using the HCT Frailty Scale at first consultation and HCT admission in 404 adults from 15 HCT programs in Spain. Based on the results, patients were classified into fit, pre-frail and frail categories. Allo-HCT outcomes were analyzed according to the results obtained from the HCT Frailty Scale. Data was collected prospectively and all patients signed informed consent.
Results: At first consultation, 102 (26.2%) patients were classified as fit, 248 (61.4%) as pre-frail, and 50 (12.4%) as frail. During the study, 62 (15.2%) patients participated in a pre-habilitation program. Among non-pre-habilitated patients (n=342), the proportion of fit patients decreased from 26.6% to 16.7%, while frail patients increased from 12.7% to 19.9%. In contrast, pre-habilitated patients (n=62) showed improvements, with fit patients increasing from 24.2% to 46.8%, and frail patients decreasing from 9.7% to 3.2%. Multivariate analysis confirmed lower OS (HR 2.52, P=0.002) and higher NRM (HR 2.69, P=0.013) in frail patients at HCT admission compared to fit ones, with a trend towards lower OS in pre-frail patients (HR 1.54, P=0.097).
Conclusion: This study highlights the feasibility of incorporating the HCT Frailty Scale into clinical practice, confirms its negative impact of frailty on transplant outcomes, and suggests that frailty is dynamic and potentially reversible through pre-transplant interventions.
Introduction
Allogeneic hematopoietic cell transplantation (allo-HCT) offers a potential cure for patients with high-risk hematologic disorders (1). Advances in the transplant methodology have substantially decreased transplant-related mortality within the first 2 years post-allo-HCT, from 40% in the late 1980s to 10-20% today (2–5). These advances have expanded the pool of patients eligible for allo-HCT, particularly including older adults and those with comorbidities (6, 7). However, despite these improvements, allo-HCT still carries risk of mortality and morbidity, underscoring the importance of meticulous patients’ selection (8–11). The frailty status of patients emerges as relevant information for the advancement in this direction.
While frailty assessment has traditionally been restricted to geriatric populations, recent research has demonstrated the usefulness of information about the frailty status of candidates in allo-HCT settings (12–14). To the advancement of frailty assessment and its use in clinical practice in the allo-HCT setting has contributed the development of frailty scales inspired in those used in geriatric settings, but adapted in a cost-effective way to the transplant ones (15–25). Frailty programs in allo-HCT settings have documented an incidence of frailty among adult candidates that ranges between 8% and 25%; have demonstrated the statistical association between patient`s frailty and the likelihood of transplant complications and mortality (15–25); and start to provide first evidence that frailty is dynamic in allo-HCT patients and eventually reversible through pre habilitation programs.
These trends in frailty research motivated the Grupo Español de Transplante Hematopoyético y Terapia Celular (GETH-TC) to initiate this study, aimed at assessing frailty in allo-HCT patients across HCT units in Spain. The study implements the HCT Frailty Scale, developed at Princess Margaret Cancer Center in Toronto, Canada (26, 27), to classify transplant candidates into three frailty levels—frail, pre-frail, and fit—at both the first consultation and HCT admission, in order to investigate the dynamics of frailty before allo-HCT. Additionally, it examines whether the association between frailty status and transplant outcomes varies depending on when frailty is evaluated, assessing the importance of its dynamic nature. Lastly, the study gathers preliminary evidence on the effectiveness of pre-habilitation programs in improving frailty before transplantation.
Methods
Study design, multicenter participation, and patient selection
GETH-TC is a non-profit scientific association that gathers all hospital units performing HCT in Spain and Portugal. All affiliates to the GETH-TC were invited to participate in the investigation, and fifteen institutions finally contributed to the project. All consecutive adults consulted for either autologous (auto-HCT) and allo-HCT between April 2022 and September 2023 were considered eligible for frailty evaluation after providing informed consent. Notably, the implementation of the HCT Frailty Scale has been a collaborative effort, utilizing the existing human and material resources of the HCT Units and without relying on external funding. This study was entirely observational, and the results from frailty assessments did not influence the determination of HCT eligibility or the design of the HCT process.
During the study period, 1023 patient candidates for auto- and allo-HCT have been evaluated and included in the study. This study selected the 404 allo-HCT candidates who were evaluated for frailty at first consultation and at HCT admission. Prospective data were updated in July 2024. The study was approved by the Ethics Committee of the Hospital Clínic de Barcelona and the GETH-TC, and conducted following the standards set forth by the Declaration of Helsinki.
Frailty assessment: implementation of the HCT Frailty Scale
The research methodology commonly applied by all participating centers is outlined in Figure 1. The frailty syndrome was consistently assessed using the HCT Frailty Scale (26, 27), and replicating the steps followed at PMCC. To standardize the assessment process, all participants in the project underwent a remote training program led by the principal investigator with experience in the Canadian study. Candidates for allo-HCT were categorized as fit, pre-frail, and frail based on the score resulting from the sum of the weighted values of the eight variables included in the HCT Frailty Scale: Clinical Frailty Score (CFS) (28), Instrumental Activities of Daily Living (IADL) test (29), grip strength score (GS) (30), Timed Up and Go Test (TUGT) (31), Self-Rated Health question (SRH-Q), falls test, and serum albumin and C-reactive protein levels (26). Additionally, cognition was assessed using the Mini-Cog test (32).
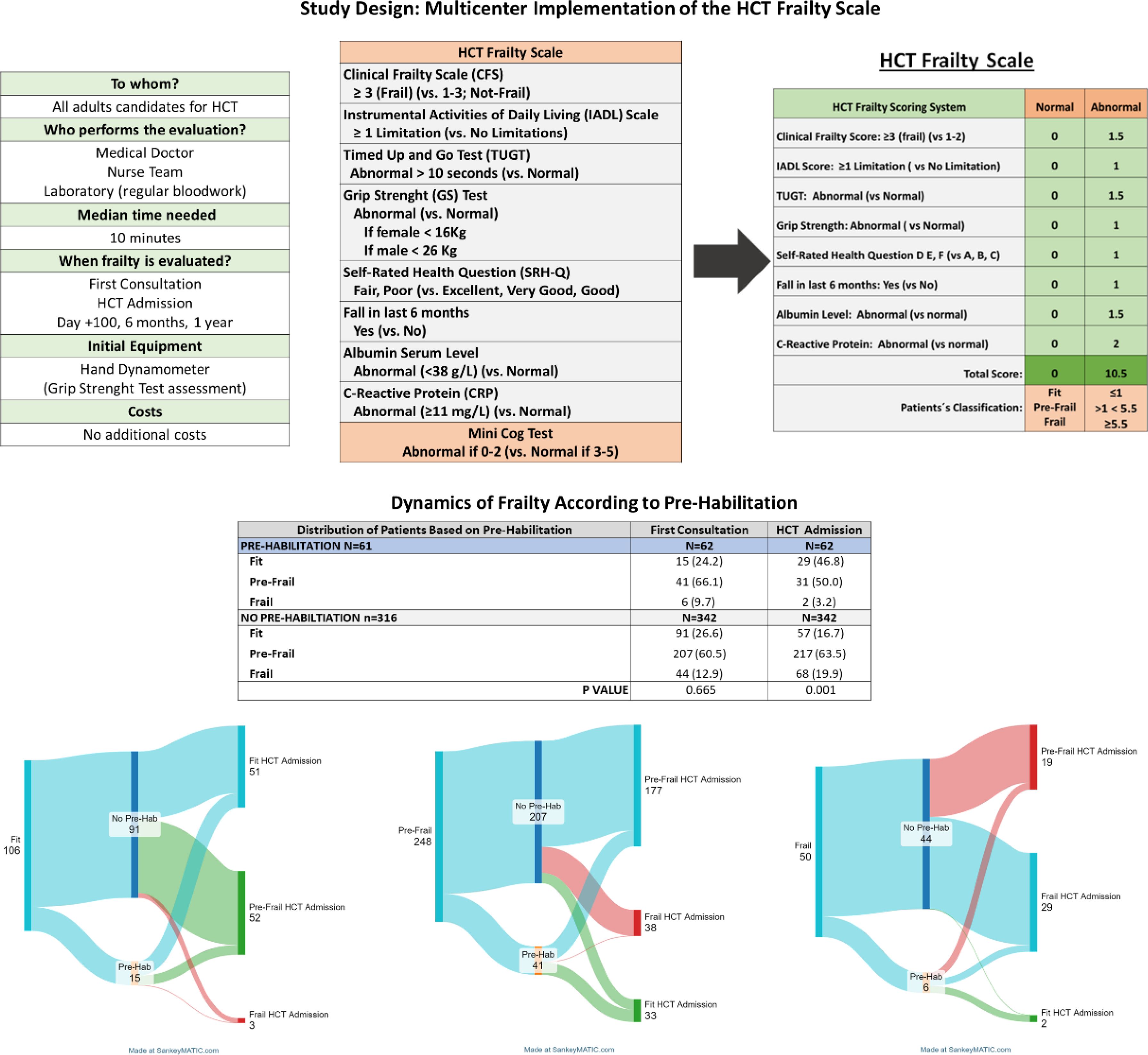
Figure 1. Study design and classification ability of the HCT Frailty Scale.
As outlined in Figure 1, the study included the longitudinal evaluation of the frailty syndrome for all patients at the first HCT consultation, at HCT admission, and during post-transplant follow-up (days +100, +180 and +1-year). The frailty assessment was conducted by hematologists and nursing teams members of the HCT units participating in the study, and typically lasted between 8 to 10 minutes.
Pre-habilitation program
In June 2022, one of the participating institutions launched a pilot pre-habilitation program for all allo-HCT candidates, regardless of age, diagnosis, or frailty status. The goal was to maintain the fitness of fit patients until HCT admission and to improve the frail or pre-frail status of those initially classified as such. The 62 adults (15.8%) consulted at this center after June 2022 were enrolled in the program. The program began within 1-7 days after the first consultation and continued until HCT admission. Pre-habilitation involved an in-person functional assessment at the Rehabilitation Service, followed by a personalized 4–8-week outpatient physical activity program monitored via telephone. To avoid delays, a dedicated clinic day was established, allowing a rehabilitation physician to schedule patients timely after their initial consultation and provide follow-up through one or two phone calls. No patient underwent in-person pre-habilitation beyond the initial assessment, and allo-HCT was never delayed to extend the program.
Pre-transplant assessment and allo-HCT practices
The first consultation for allo-HCT was performed after stem cell donor identification, and in a median of 4 weeks before HCT admission. Each HCT institution followed internal protocols for determining patients’ eligibility for allo-HCT, donor selection and designing the HCT platform. Nevertheless, conditioning regimen intensity was generally tailored to chronological age and comorbidities. With some exceptions, patients older than 55 years with significant comorbidities received reduced intensity conditioning (RIC) regimens. Grading of acute and chronic GVHD (aGVHD and cGVHD) followed established criteria (33–35).
Statistical analysis
The study analyzes data obtained from the HCT Frailty Scale at first consultation and at HCT admission, together with clinical and outcome information of patients included in the study. A statistical analysis chronogram is detailed in Supplementary Material (Section 1). Categorical and discrete variables are presented as counts and percentages, whereas continuous variables are presented as the median and range or interquartile ranges (IQR). Univariate and multivariate regression analyses (UVA and MVA) explored the impact of frailty on outcomes overall survival (OS) and non-relapse mortality (NRM). Statistical significance was set at P<0.05. EZR software was used for statistical analysis (36).
Results
Frailty assessment implementation
Of the 35 HCT units members of GETH-TC dedicated to performing allo-HCT, 13 (37%) participated on the study. During the study period, 551 adults underwent allo-HCT at the participating institutions. Of these, 404 patients (73.3%) were assessed for frailty at their initial consultation and HCT admission and included in the study.
The proportion of patients evaluated for frailty, relative to the total number consulted for allo-HCT, varied across centers. In 7 programs, more than 75% of patients were evaluated, in 4 institutions, between 50-75%, and in 2 centers, fewer than 50% of patients were assessed and included in the study. These variations were largely due to differences in the availability of resources, internal coordination, and organizational practices across centers. The median time to complete the frailty assessment was 10 minutes per patient, typically performed by hematologists or nurse coordinators from each transplant team. No external funding was provided for the study, and aside from the initial material costs (hand dynamometer required for the assessment), no additional expenses were incurred during the study period.
Frailty assessment at the first consultation
As depicted in Table 1, the median age of the cohort was 56 years (range: 18–76), with 95 (23.5%) patients aged 65 or older. A total of 260 (64.0%) patients were males, 151 (38.5%) had a KPS < 90%, and 60 (15.2) an HCT-CI > 3. The most frequent diagnoses were acute myeloid leukemia (33.7%) and myelodysplastic syndrome (20.8%), indicating that most patients had malignant hematological disorders.
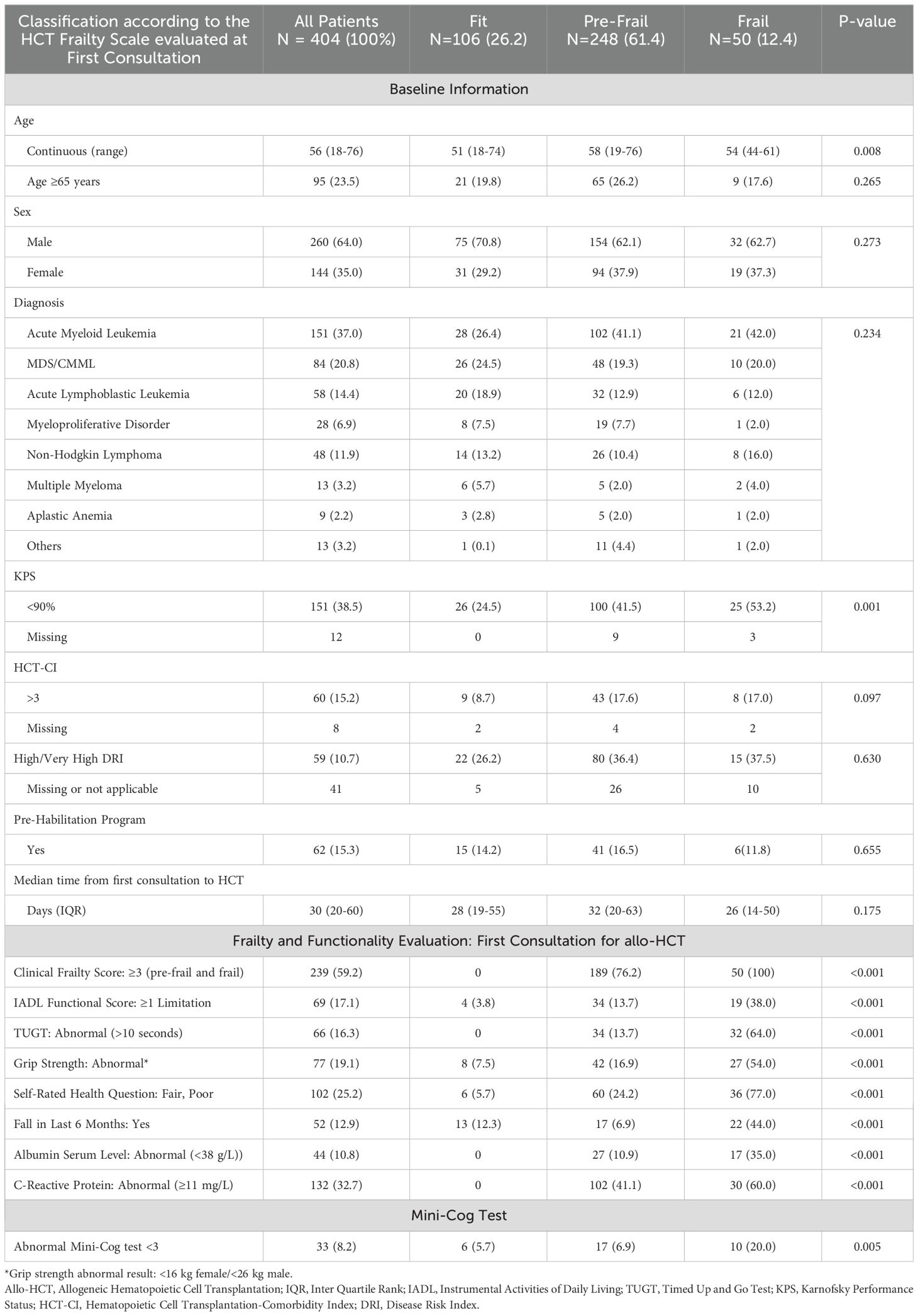
Table 1. Application of the HCT Frailty Scale at first consultation in adult candidates for Allo-HCT.
At the first consultation, 26.2% (106 patients) were classified as fit, 61.4% (248 patients) as pre-frail, and 12.4% (50 patients) as frail. As shown in Table 1, frail patients were older than fit patients, but had a similar median age to pre-frail patients (54 vs. 51 and 58, P=0.008). The proportions of frail patients with a KPS <90% (53.2% vs. 38.5% and 41.5%, P=0.001) and those scoring less than 3 on the Mini-Cog test (20.0% vs. 5.7% and 6.9%, P=0.005) were higher compared to fit and pre-frail patients. Additionally, frail and pre-frail patients tended to have more comorbidities, with HCT-CI > 3 present in 17.0% and 17.6% of frail and pre-frail patients, compared to 8.7% in fit patients (P=0.097).
Pre-habilitation and frailty evaluation at HCT admission
The median time from the first consultation to HCT admission was 30 days (range, 20-50 days). At the time of HCT admission, 21.3% (86 patients) were classified as fit, 61.4% (248 patients) as pre-frail, and 17.3% (70 patients) as frail. While these proportions appeared similar to those observed at first consultation, comparisons between the two time points revealed transitions across frailty categories for some patients, regardless of their initial status and the median time from first consultation.
As illustrated in Figure 1, among non-pre-habilitated patients (n=342), the median of time from first consultation to HCT admission was 4 weeks (range, 3-7 weeks), and the proportion of fit patients decreased from 26.6% to 16.7%, pre-frail proportions remained similar (60.5% to 63.5%) and frail patients increased from 12.7% to 19.9%. In contrast, among the 62 (15.3%) pre-habilitated patients, the median time from first consultation to admission was 7 weeks (range, 4-8) and the improvements of the frailty state of patients were evident: the percentage of fit patients increased from 24.2% to 46.8%, while the proportion of pre-frail patients decreased from 66.1% to 50.0%, and frail patients dropped from 9.7% to 3.2% (differences statistically significant, P< 0.001).
Considering the dynamics of frailty, baseline characteristics were reassessed based on the information provided by the HCT Frailty Scale at HCT admission. As shown in Table 2, patient characteristics and allo-HCT procedures were similar across frailty categories, except for higher percentage of patients in the frail and pre-frail groups receiving RIC regimens (64.3% and 54.4% vs. 43.1% in fit patients, P=0.028), likely due to the higher age distribution in these groups.
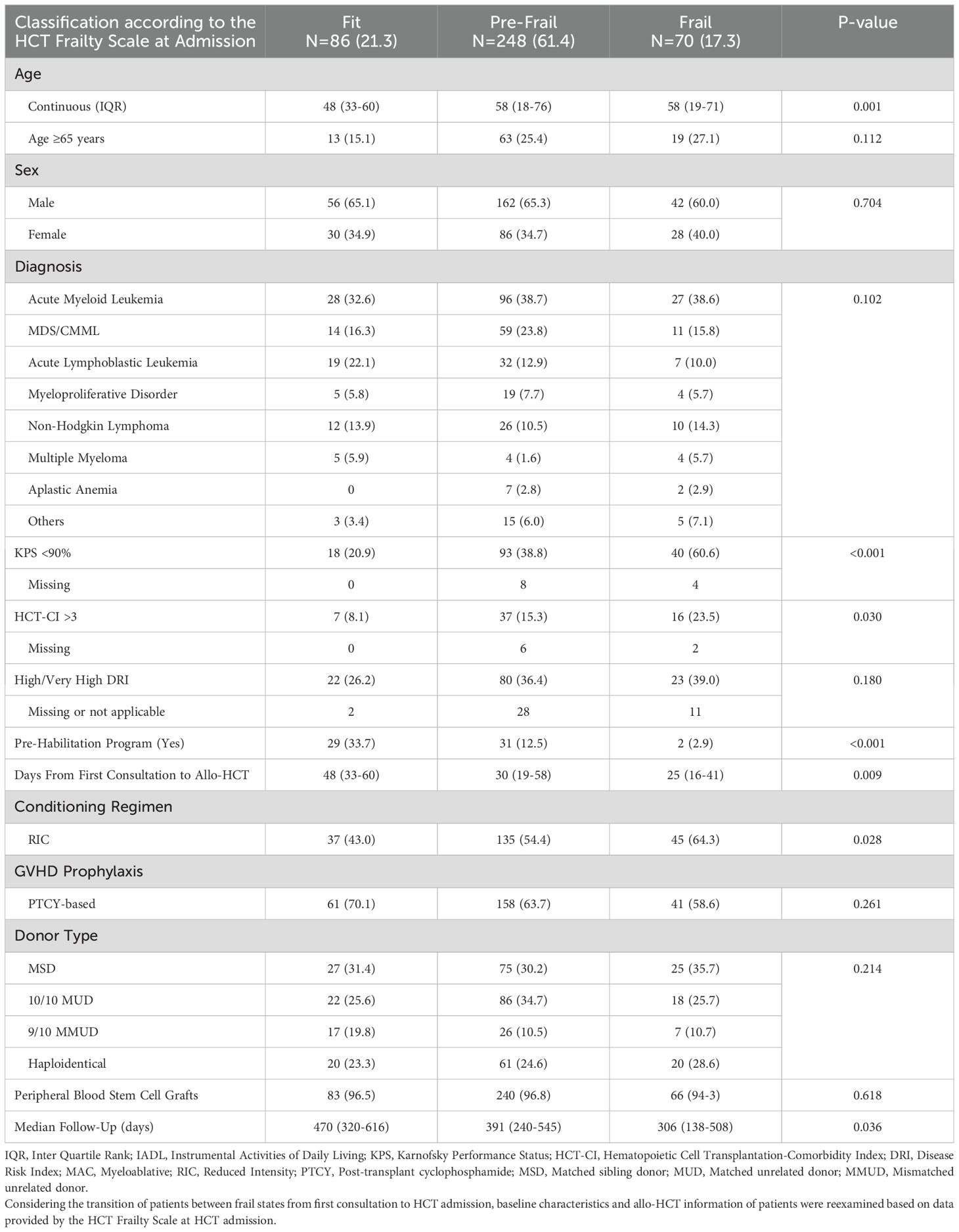
Table 2. Impact of frailty in HCT results: information based on frailty at HCT admission.
Frailty at HCT admission and allo-HCT results
As described in Table 3, frail and pre-frail patients had longer median hospital stays compared to fit patients (27 and 25 days vs. 22 days, P=0.034), though no significant differences were observed in 6-month readmission rates (24.3%, 29.3%, and 28.1%, P=0.493). The cumulative incidence of aGVHD and moderate/severe cGVHD were comparable across frailty groups. For frail patients, these rates were 24.3% (P=0.236) for day +100 grade II-IV aGVHD, 8.6% (P=0.746) for day +100 grade III-IV aGVHD, and 13.0% (P=0.845) for 1-year moderate/severe cGVHD.
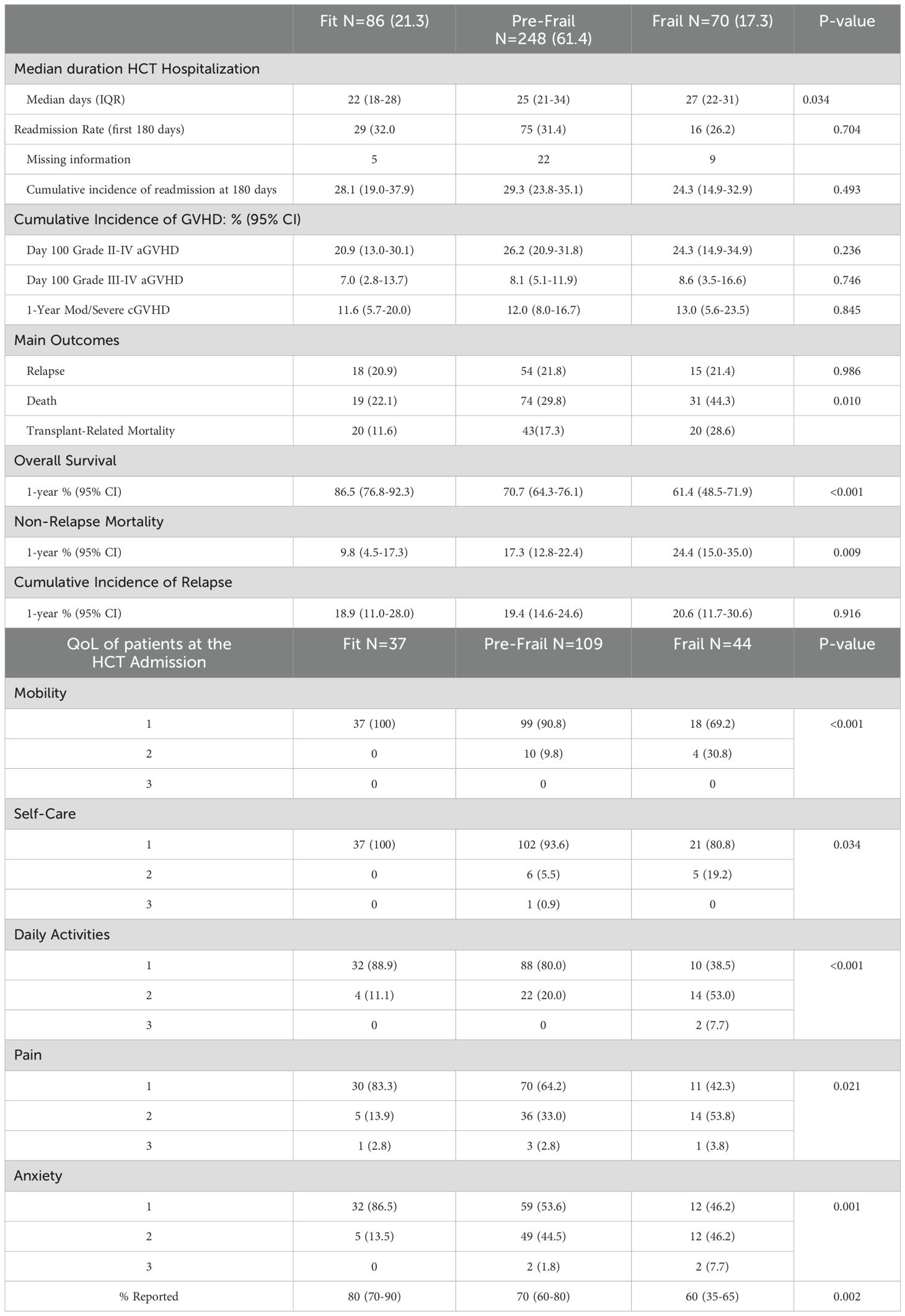
Table 3. QoL and allo-HCT results according to frailty at HCT admission.
Relapse rates at 1-year did not differ significantly by frailty status, with incidences of 18.9% (95% CI: 11.0–28.0) for fit patients, 19.4% (95% CI: 14.6–24.6) for pre-frail patients, and 20.6% (95% CI: 11.7–30.6) for frail patients (P=0.009).
Lastly, quality of life (QoL) was assessed at HCT admission in 190 patients using the EQ-5D-3L test. Fit patients reported better QoL scores compared to pre-frail and frail patients, with auto-reported rates of 80%, 70%, and 60%, respectively (P=0.002).
Frailty syndrome and transplant outcomes
With a median follow-up of 13.1 months (IQR: 7.9–18.4), 89 patients (23.2%) died, with infections and relapse being the most common causes of death. As shown in Figure 2, the estimated 1-year OS rates based on the HCT Frailty Scale at the first consultation were 78.4% (95% CI: 70.2–86.1) for fit patients, 70.6% (95% CI: 64.2–76.1) for pre-frail patients, and 66.4% (95% CI: 50.8–78.1) for frail patients (P=0.105). In contrast, at HCT admission, the estimated 1-year OS rates were 86.5% (95% CI: 76.8–92.3) for fit patients, 70.7% (95% CI: 64.3–76.1) for pre-frail patients, and 61.4% (95% CI: 48.5–71.9) for frail patients (P<0.001).
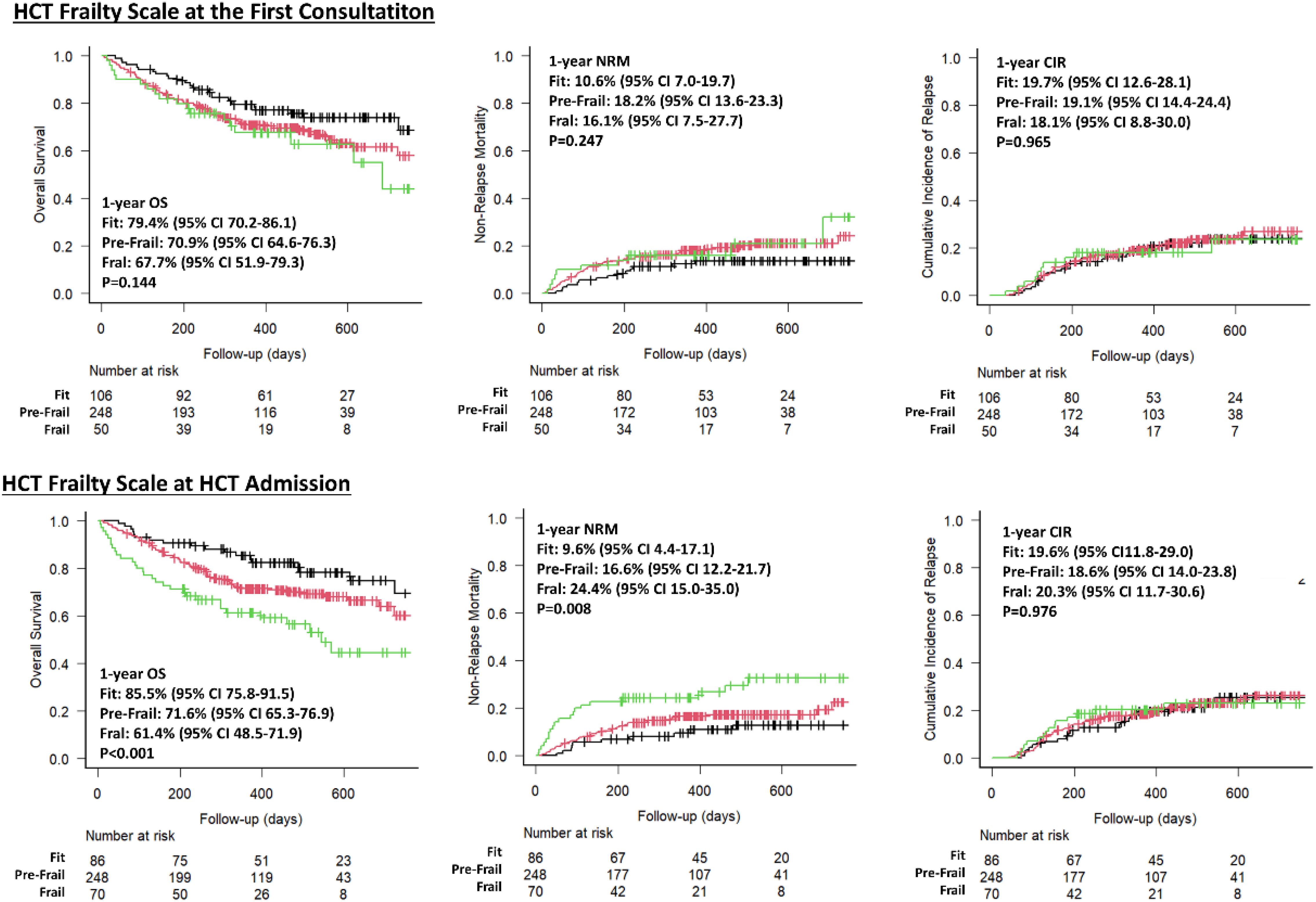
Figure 2. Outcomes of fit, pre-frail and frail adults undergoing allo-HCT.
The effect of frailty on OS and NRM was analyzed using regression analyses. Table 4 shows that in the UVA, the hazard ratios (HR) for OS in frail versus fit patients were 1.73 (P=0.071) at the first consultation and 2.78 (P<0.001) at HCT admission, indicating that the impact of frailty on OS differed depending on the timing of the assessment. Additionally, a trend toward worse outcomes was seen in pre-frail patients compared to fit patients at HCT admission (HR 1.56, P=0.081). Although pre-habilitation influenced frailty status at HCT admission, it did not significantly affect OS (HR 0.66, P=0.146).
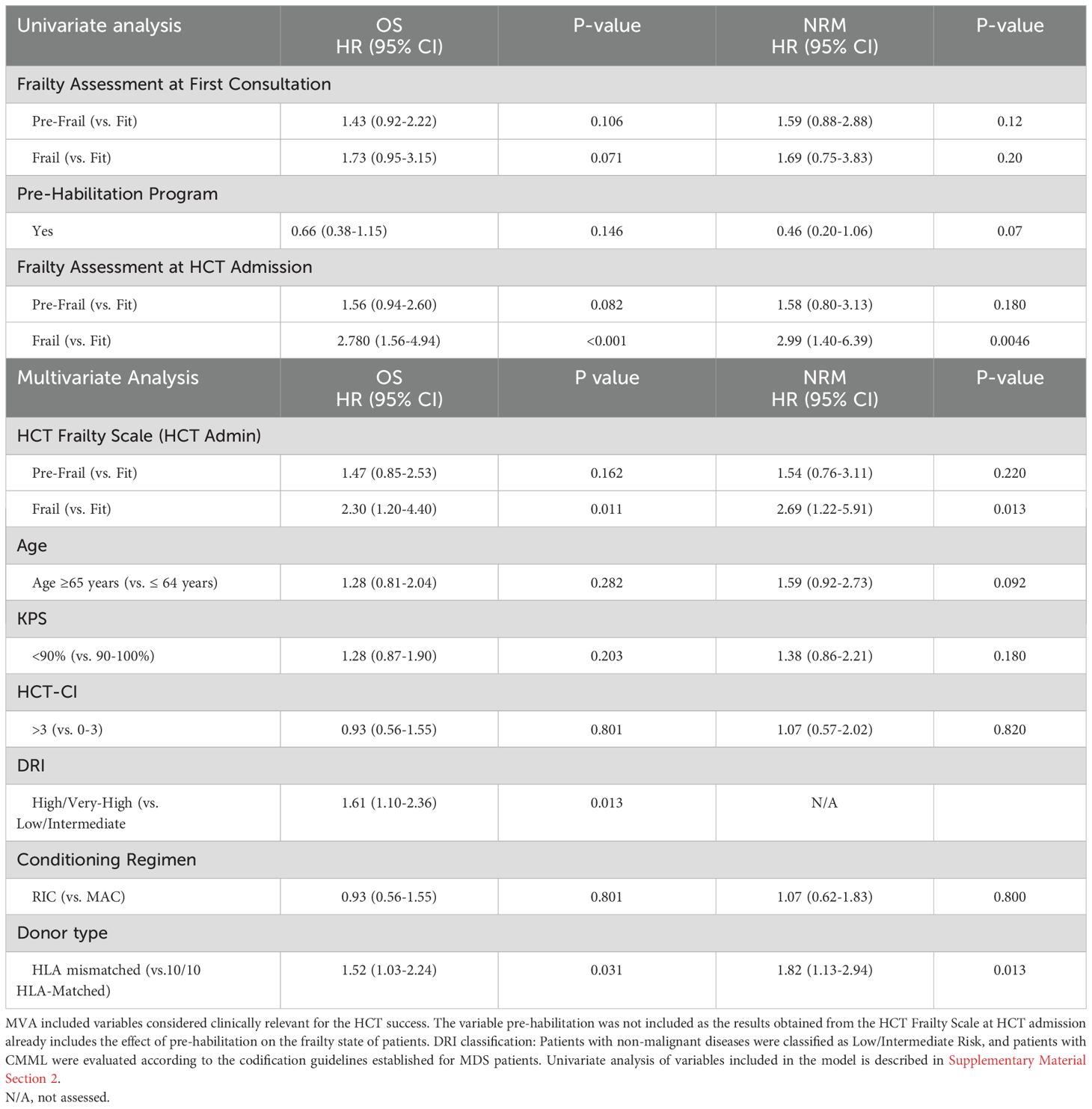
Table 4. Frailty syndrome, overall survival and non-relapse mortality.
Differences in NRM across frailty categories were also examined (Figure 2, Table 4). Similar to OS, reclassification of patients based on frailty status following pre-habilitation altered the NRM likelihood at HCT admission compared to the initial consultation. However, at HCT admission, frail patients had a significantly higher risk of NRM than fit patients (HR 2.99, P=0.004).
The MVA including variables considered clinically relevant as determinants of transplant outcomes gave similar results than the univariate one in terms of shorter OS (HR 2.30, P=0.011) and higher NRM(HR 2.69, P=0.013) in frail patients compared to fit ones. Pre-frail patients showed a non-significant trend toward shorter OS (HR 1.47, P=0.162). In addition, patients with High/Very-High DRI/HR 1.61, P=0.013) and undergoing allo-HCT from HLA-mismatched donors (HR 1.52, P=0.031) had a shorter OS than the rest. In contrast, age over 64, KPS < 90%, and an HCT-CI > 3 were not significant predictors of OS or NRM.
Pre-habilitation and transplant outcomes
The differences in the impact of frailty on outcomes, depending on when frailty was assessed, were attributed to the redistribution of pre-habilitated patients across frailty categories from first consultation to the time of HCT admission. To strengthen the findings, further analysis comparing pre-habilitated and non-pre-habilitated patients was conducted.
The baseline and allo-HCT characteristics were similar between both groups, except for median age (median age: 60 vs. 55 years, P=0.002) which was higher in the pre-habilitated group (Supplementary Table 2). As illustrated in Figure 3, frail patients at HCT admission had worse outcomes than fit and pre-frail ones irrespective of participation in the pre-habilitation program. However, in non-pre-habilitated patients, the differences in estimated OS rates across frailty categories were consistent whether frailty was assessed at the first consultation or at HCT admission. In contrast, for pre-habilitated patients, significant differences in transplant outcomes across frailty categories were observed only when frailty was assessed at admission. This suggests that the pre-habilitation program successfully improved patients’ fitness for transplant and that the improvement affected positively transplant outcomes.
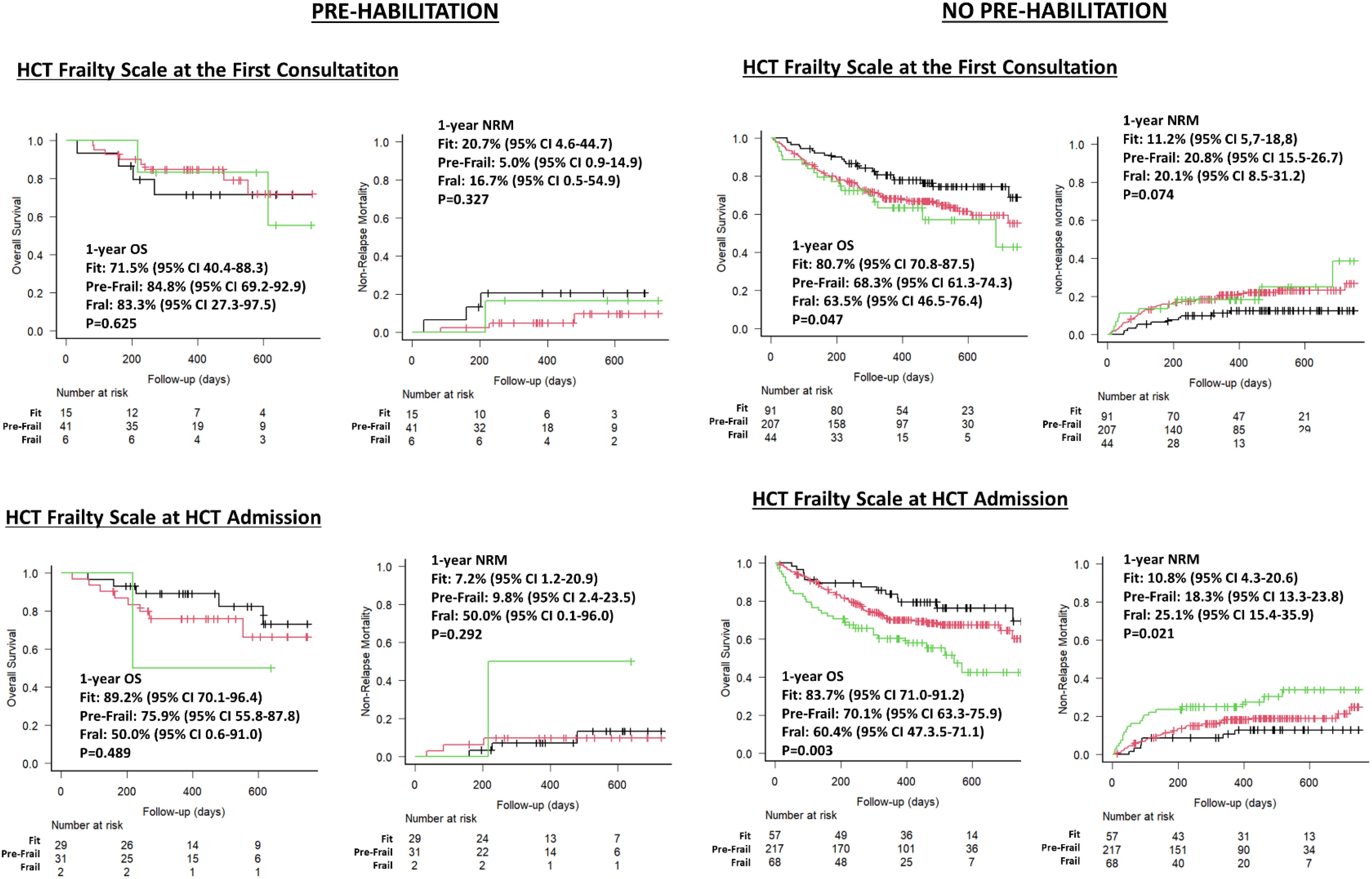
Figure 3. Impact of frailty and pre-Habilitation on HCT Frailty Scale classification and outcomes.
Discussion
This multicenter study reports the results of a frailty assessment project in the allo-HCT setting, involving 15 HCT units across Spain. It confirms that the HCT Frailty Scale, initially implemented at PMCC (26, 27), can be successfully integrated into routine clinical practice through coordinated team efforts, without requiring additional resources. Overall, 404 Spanish allo-HCT candidates were classified in fit, pre-frail, or frail categories, in proportions similar to those seen in the Canadian study. Importantly, patients’ frailty status at admission was strongly associated with transplant outcomes, with fit patients showing a higher likelihood of positive results compared to frail patients. In addition, the longitudinal evaluation of frailty documented that is dynamic and eventually reversible through individualized pre-habilitation programs.
Despite efforts to homogeneously applying the HCT Frailty Scale across the participant HCT units, there was variability across them in their engagement with the project. For example, some centers successfully evaluated over 75% of allo-HCT candidates, while others assessed fewer than 40% of potential patients. These differences mainly stemmed from the fact that not all the units had the same resources to implement the evaluation, and alert about the importance of timing coordinating efforts for the successful integration of frailty evaluations into clinical practice. This results also underscore the importance of using cost-effective tools like the HCT Frailty Scale to enable consistent application across transplant centers.
Differences were observed in the baseline characteristics of patients across various frailty levels, including comorbidities, KPS<90%, and abnormal values on the Mini-Cog test. As anticipated, given that KPS is a subjective and unidimensional measure of performance status, and considering that cognitive impairment—a key aspect of cognitive frailty—often coexists with physical frailty, the proportions of patients with KPS<90% and abnormal Mini-Cog tests were higher in frail patients (37, 38).
The analysis of the association between frailty and transplant outcomes, revealed lower likelihood of OS and higher likelihood of NRM among frail and pre-frail patients than among those classified as fit. These results did not change when including additional explanatory variables such as comorbidities, chronological age, and KPS. These results align with previously published ones on the negative impact of frailty on allo-HCT outcomes (15–25), as well as results from PMCC (26, 27). In addition, highlight the importance of implementing frailty assessments in allo-HCT practice for better patient counselling, decision making, and desiging better allo-HCT platforms.
The study further emphasizes the dynamic nature of frailty in allo-HCT candidates suggesting that frailty can potentially be reversed through pre-transplant interventions (39–42). Patients who participated in pre-habilitation showed a trend toward either improving their frailty status or maintaining their fit condition before transplantation. In contrast, some non-pre-habilitated patients experienced a decline in fitness during the pre-transplant phase. This decline was unexpected, as many patients had been discharged from prior treatments when undergo their first allo-HCT consultation.
It is presumed that consolidation therapies administered while awaiting allo-HCT, along with the cumulative toxicity of these treatments, contributed to the minimal spontaneous improvement and even worsened frailty in some non-pre-habilitated patients (Figure 1). Unfortunately, clinical events during this period were not collected, limiting our ability to identify specific factors influencing the negative progression of frailty in some individuals.
As shown in Figure 3, frailty data collected at first consultation correlated with early transplant outcomes in non-pre-habilitated patients, suggesting the transition between frailty states was not clinically significant. However, in pre-habilitated patients, frailty assessments at admission had a stronger correlation with outcomes than those at first consultation, as the variability in the frailty stages of these patients during the two time points was significantly relevant. These results highlighting the importance of tracking frailty over time and support pre-habilitation for all allo-HCT candidates to improve pre-frail and frail conditions and prevent fit patients from deteriorating (21, 43–45).
QoL at HCT admission was influenced by the patient’s frailty status. While the results in this area should be considered preliminary due to the limited number of patients evaluated, they remain significant, as QoL impairments may affect patients’ ability to cope with potential medical issues occurring during the post-transplant phase. QoL is a multifaceted concept, and the association between frailty and QoL has been minimally explored in existing studies (46).
This study primarily focused on evaluating physical frailty and QoL. However, the expansion of allo-HCT to a more diverse patients’ population together with the refinement of pre-transplant assessments underway, recommend exploring the addition of other related variables as predictors of transplant outcomes. In this respect, sarcopenia, reflecting patients’ muscle mass and strength and a key indicator of patients´ physical resilience and recovery potential, has been linked to higher likelihood of post-transplant complications and reduced OS (47, 48). Another issue that has not been considered yet in our investigation is the social dimension of frailty of transplanted patients, including economic status, caregiver availability, social support, and familial dynamics. Previous research has documented the association between patient’s ecosystem and transplant outcomes (49, 50) and more should be done in the investigation of this topic in the near future
The follow-up period in this study limited the analysis of frailty’s impact on outcomes to the first year after allo-HCT. Furthermore, while the improvement in frailty observed among pre-habilitated patients is promising, the fact that pre-habilitation was implemented at only one participating HCT unit restricts the generalizability of these findings across other institutions. Notice additionally that the information provided by the HCT Frailty Scale was not used to adjust transplant protocols or modify supportive care strategies. Future research should include longer follow-up, multicenter pre-habilitation programs, and explore how integrating frailty data into clinical decision-making and transplant planning to further improve patient outcomes.
In conclusion, this study highlights the importance of assessing frailty in clinical practice within allo-HCT settings. Frailty can be evaluated using cost-effective frailty scales such as the HCT Frailty Scale, after appropriate training and coordination (26, 27). Frailty assessment provides valuable prognostic insights into transplant outcomes, underscoring the potential benefits of pre-habilitation programs to enhance patients’ fitness before transplantation.
Data availability statement
Anonymized data would be shared only after specific request and internal consideration. Requests to access these datasets should be directed to MQS, bXFzYWxhc0BjbGluaWMuY2F0.
Ethics statement
The studies involving humans were approved by CEIC Hospital Clinic de Barcelona. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MQS: Conceptualization, Formal analysis, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing. MTS: Investigation, Validation, Writing – review & editing. MB: Investigation, Validation, Writing – review & editing. MA: Investigation, Validation, Writing – review & editing. LF: Investigation, Validation, Writing – review & editing. MP: Investigation, Validation, Writing – review & editing. ASa: Investigation, Validation, Writing – review & editing. MQ: Investigation, Validation, Writing – review & editing. ASS: Investigation, Validation, Writing – review & editing. JS: Investigation, Validation, Writing – review & editing. VI: Investigation, Validation, Writing – review & editing. ZA-L: Investigation, Validation, Writing – review & editing. JC: Investigation, Validation, Writing – review & editing. LP: Investigation, Validation, Writing – review & editing. SFL: Investigation, Validation, Writing – review & editing. LV-S: Investigation, Validation, Writing – review & editing. SV: Investigation, Validation, Writing – review & editing. PB-M: Investigation, Validation, Writing – review & editing. AE: Investigation, Validation, Writing – review & editing. II: Investigation, Validation, Writing – review & editing. SG: Investigation, Validation, Writing – review & editing. AM: Investigation, Validation, Writing – review & editing. EL: Investigation, Validation, Writing – review & editing. JL-M: Investigation, Validation, Writing – review & editing. SF: Investigation, Validation, Writing – review & editing. ÁC: Investigation, Validation, Writing – review & editing. LB: Investigation, Validation, Writing – review & editing. ASu: Investigation, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We thank our patients and the Grupo Español de Trasplante Hematopoyético y Terapia Celular (GETH-TC) for the support provided during the study development. In addition, the principal investigator is grateful to Dr. Anna Sureda, Dr. Rajat Kumar, and Dr. Shabbir Alibhai for their support during the study period. We additionally thank REDCap (Research Electronic Data Capture) service for permitting the use of their service without costs. REDCap is a secure, web-based software platform designed to support data capture for research studies.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1512154/full#supplementary-material
References
1. Copelan EA. Hematopoietic stem-cell transplantation. N Engl J Med. (2006) 354:1813–26. doi: 10.1056/NEJMra052638
2. McDonald GB, Sandmaier BM, Mielcarek M, Sorror M, Pergam SA, Cheng GS, et al. Survival, nonrelapse mortality, and relapse-related mortality after allogeneic hematopoietic cell transplantation: comparing 2003-2007 versus 2013-2017 cohorts. Ann Intern Med. (2020) 172:229–39. doi: 10.7326/M19-2936
3. Penack O, Peczynski C, Mohty M, Yakoub-Agha I, Styczynski J, Montoto S, et al. How much has allogeneic stem cell transplant-related mortality improved since the 1980s? A retrospective analysis from the EBMT. Blood Adv. (2020) 4:6283–90. doi: 10.1182/bloodadvances.2020003418
4. Salas MQ, Pasic I, Remberger M, Novitzky-Basso I, Law AD, Lam W, et al. Improving safety and outcomes after allogeneic hematopoietic cell transplantation: A single-center experience. Transplant Cell Ther. (2022) 28:265.e1– e9. doi: 10.1016/j.jtct.2022.02.001
5. Gooley TA, Chien JW, Pergam SA, Hingorani S, Sorror ML, Boeckh M, et al. Reduced mortality after allogeneic hematopoietic-cell transplantation. N Engl J Med. (2010) 363:2091–101. doi: 10.1056/NEJMoa1004383
6. Duarte RF, Sanchez-Ortega I. HSCT in elderly patients. In: Carreras E, Dufour C, Mohty M, Kroger N, editors. The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies. Cham (CH (2019). p. 499–503.
7. Passweg JR, Baldomero H, Chabannon C, Basak GW, de la Camara R, Corbacioglu S, et al. Hematopoietic cell transplantation and cellular therapy survey of the EBMT: monitoring of activities and trends over 30 years. Bone Marrow Transplant. (2021) 56:1651–64. doi: 10.1038/s41409-021-01227-8
8. Majhail NS, Farnia SH, Carpenter PA, Champlin RE, Crawford S, Marks DI, et al. Indications for Autologous and allogeneic hematopoietic cell transplantation: guidelines from the American society for blood and marrow transplantation. Biol Blood Marrow Transplant. (2015) 21:1863–9. doi: 10.1016/j.bbmt.2015.07.032
9. Snowden JA, Sanchez-Ortega I, Corbacioglu S, Basak GW, Chabannon C, de la Camara R, et al. Indications for haematopoietic cell transplantation for haematological diseases, solid tumours and immune disorders: current practice in Europe, 2022. Bone Marrow Transplant. (2022) 57:1217–39. doi: 10.1038/s41409-022-01691-w
10. Kanate AS, Majhail NS, Savani BN, Bredeson C, Champlin RE, Crawford S, et al. Indications for hematopoietic cell transplantation and immune effector cell therapy: guidelines from the American society for transplantation and cellular therapy. Biol Blood Marrow Transplant. (2020) 26:1247–56. doi: 10.1016/j.bbmt.2020.03.002
11. Kanate AS, Perales MA, Hamadani M. Eligibility criteria for patients undergoing allogeneic hematopoietic cell transplantation. J Natl Compr Canc Netw. (2020) 18:635–43. doi: 10.6004/jnccn.2020.7559
12. Abel GA, Klepin HD. Frailty and the management of hematologic Malignancies. Blood. (2018) 131:515–24. doi: 10.1182/blood-2017-09-746420
13. Hegde A, Murthy HS. Frailty: the missing piece of the pre- hematopoietic cell transplantation assessment? Bone Marrow Transplant. (2018) 53:3–10. doi: 10.1038/bmt.2017.192
14. Morley JE, Vellas B, van Kan GA, Anker SD, Bauer JM, Bernabei R, et al. Frailty consensus: a call to action. J Am Med Dir Assoc. (2013) 14:392–7. doi: 10.1016/j.jamda.2013.03.022
15. Jayani R, Rosko A, Olin R, Artz A. Use of geriatric assessment in hematopoietic cell transplant. J Geriatr Oncol. (2019) 11:225–36. doi: 10.1016/j.jgo.2019.09.012
16. Klepin HD, Wildes TM. Fighting for the integration of geriatric principles into oncology. J Geriatr Oncol. (2018) 9:705–6. doi: 10.1016/j.jgo.2018.05.013
17. Williams GR, Deal AM, Jolly TA, Alston SM, Gordon BB, Dixon SA, et al. Feasibility of geriatric assessment in community oncology clinics. J Geriatr Oncol. (2014) 5:245–51. doi: 10.1016/j.jgo.2014.03.001
18. Hamaker ME, Wildes TM, Rostoft S. Time to stop saying geriatric assessment is too time consuming. J Clin Oncol. (2017) 35:2871–4. doi: 10.1200/JCO.2017.72.8170
19. Muffly LS, Kocherginsky M, Stock W, Chu Q, Bishop MR, Godley LA, et al. Geriatric assessment to predict survival in older allogeneic hematopoietic cell transplantation recipients. Haematologica. (2014) 99:1373–9. doi: 10.3324/haematol.2014.103655
20. Deschler B, Ihorst G, Schnitzler S, Bertz H, Finke J. Geriatric assessment and quality of life in older patients considered for allogeneic hematopoietic cell transplantation: a prospective risk factor and serial assessment analysis. Bone Marrow Transplant. (2018) 53:565–75. doi: 10.1038/s41409-017-0021-4
21. Derman BA, Kordas K, Ridgeway J, Chow S, Dale W, Lee SM, et al. Results from a multidisciplinary clinic guided by geriatric assessment before stem cell transplantation in older adults. Blood Adv. (2019) 3:3488–98. doi: 10.1182/bloodadvances.2019000790
22. Holmes HM, Des Bordes JK, Kebriaei P, Yennu S, Champlin RE, Giralt S, et al. Optimal screening for geriatric assessment in older allogeneic hematopoietic cell transplantation candidates. J Geriatr Oncol. (2014) 5:422–30. doi: 10.1016/j.jgo.2014.04.004
23. Lin RJ, Elko TA, Devlin SM, Shahrokni A, Jakubowski AA, Dahi PB, et al. Impact of geriatric vulnerabilities on allogeneic hematopoietic cell transplantation outcomes in older patients with hematologic Malignancies. Bone Marrow Transplant. (2019) 55:157–64. doi: 10.1038/s41409-019-0654-6
24. Nawas MT, Andreadis C, Martin TG, Wolf JL, Ai WZ, Kaplan LD, et al. Limitation in patient-reported function is associated with inferior survival in older adults undergoing autologous hematopoietic cell transplantation. Biol Blood Marrow Transplant. (2019) 25:1218–24. doi: 10.1016/j.bbmt.2019.01.028
25. Salas MQ, Atenafu EG, Bascom O, Wilson L, Lam W, Law AD, et al. Pilot prospective study of Frailty and Functionality in routine clinical assessment in allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. (2021) 56:60–9. doi: 10.1038/s41409-020-0979-1
26. Salas MQ, Atenafu EG, Pasic I, Al-Shaibani E, Bascom O, Wilson L, et al. Impact of hematopoietic cell transplant frailty scale on transplant outcome in adults. Bone Marrow Transplant. (2023) 58:317–24. doi: 10.1038/s41409-022-01892-3
27. Salas MQ, Atenafu EG, Pasic I, Bascom O, Wilson L, Lam W, et al. HCT frailty scale for younger and older adults undergoing allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. (2023) 58:1237–46. doi: 10.1038/s41409-023-02088-z
28. Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. (2005) 173:489–95. doi: 10.1503/cmaj.050051
29. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. (1969) 9:179–86. doi: 10.1093/geront/9.3_Part_1.179
30. Bohannon RW. Hand-grip dynamometry predicts future outcomes in aging adults. J Geriatr Phys Ther. (2008) 31:3–10. doi: 10.1519/00139143-200831010-00002
31. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. (1991) 39:142–8. doi: 10.1111/j.1532-5415.1991.tb01616.x
32. Olin RL, Fretham C, Pasquini MC, Arora M, Bhatt VR, Derman B, et al. Geriatric assessment in older alloHCT recipients: association of functional and cognitive impairment with outcomes. Blood Adv. (2020) 4:2810–20. doi: 10.1182/bloodadvances.2020001719
33. Schoemans HM, Lee SJ, Ferrara JL, Wolff D, Levine JE, Schultz KR, et al. EBMT-NIH-CIBMTR Task Force position statement on standardized terminology & guidance for graft-versus-host disease assessment. Bone Marrow Transplant. (2018) 53:1401–15. doi: 10.1038/s41409-018-0204-7
34. Harris AC, Young R, Devine S, Hogan WJ, Ayuk F, Bunworasate U, et al. International, multicenter standardization of acute graft-versus-host disease clinical data collection: A report from the Mount Sinai acute GVHD international consortium. Biol Blood Marrow Transplant. (2016) 22:4–10. doi: 10.1016/j.bbmt.2015.09.001
35. Jagasia MH, Greinix HT, Arora M, Williams KM, Wolff D, Cowen EW, et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. the 2014 diagnosis and staging working group report. Biol Blood Marrow Transplant. (2015) 21:389–401 e1. doi: 10.1016/j.bbmt.2014.12.001
36. Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. (2013) 48:452–8. doi: 10.1038/bmt.2012.244
37. Dartigues JF, Amieva H. Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J Nutr Health Aging. (2014) 18:95. doi: 10.1007/s12603-013-0437-5
38. Artz AS, Pollyea DA, Kocherginsky M, Stock W, Rich E, Odenike O, et al. Performance status and comorbidity predict transplant-related mortality after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. (2006) 12:954–64. doi: 10.1016/j.bbmt.2006.05.015
39. Hale M, Shah S, Clegg A. Frailty, inequality and resilience. Clin Med (Lond). (2019) 19:219–23. doi: 10.7861/clinmedicine.19-3-219
40. Chen X, Mao G, Leng SX. Frailty syndrome: an overview. Clin Interv Aging. (2014) 9:433–41. doi: 10.2147/CIA.S45300
41. Gill TM, Gahbauer EA, Allore HG, Han L. Transitions between frailty states among community-living older persons. Arch Intern Med. (2006) 166:418–23. doi: 10.1001/archinte.166.4.418
42. Lang PO, Michel JP, Zekry D. Frailty syndrome: a transitional state in a dynamic process. Gerontology. (2009) 55:539–49. doi: 10.1159/000211949
43. Cheng JT, Obaisi O, Yadav R, Gupta E, Fu JB, Bruera E, et al. The role of outpatient physical medicine and rehabilitation in a multidisciplinary prehabilitation program for older adults before allogeneic hematopoietic stem cell transplant. Am J Phys Med Rehabil. (2024) 103:710–5. doi: 10.1097/PHM.0000000000002428
44. Mawson S, Keen C, Skilbeck J, Ross H, Smith L, Dixey J, et al. Feasibility and benefits of a structured prehabilitation programme prior to autologous stem cell transplantation (ASCT) in patients with myeloma; a prospective feasibility study. Physiotherapy. (2021) 113:88–99. doi: 10.1016/j.physio.2021.08.001
45. Wingard JR, Wood WA, Martens M, Le-Rademacher J, Logan B, Knight JM, et al. Pretransplantation exercise and hematopoietic cell transplantation survival: A secondary analysis of blood and marrow transplant clinical trials network (BMT CTN 0902). Biol Blood Marrow Transplant. (2017) 23:161–4. doi: 10.1016/j.bbmt.2016.10.007
46. Crocker TF, Brown L, Clegg A, Farley K, Franklin M, Simpkins S, et al. Quality of life is substantially worse for community-dwelling older people living with frailty: systematic review and meta-analysis. Qual Life Res. (2019) 28:2041–56. doi: 10.1007/s11136-019-02149-1
47. Nagayama T, Fujiwara SI, Kikuchi T, Onda K, Murahashi R, Nakashima H, et al. Impact of muscle mass loss assessed by computed tomography on the outcome of allogeneic stem cell transplantation. Leuk Lymphoma. (2022) 63:1694–700. doi: 10.1080/10428194.2022.2034159
48. DeFilipp Z, Troschel FM, Qualls DA, Li S, Kuklinski MW, Kempner ME, et al. Evolution of body composition following autologous and allogeneic hematopoietic cell transplantation: incidence of sarcopenia and association with clinical outcomes. Biol Blood Marrow Transplant. (2018) 24:1741–7. doi: 10.1016/j.bbmt.2018.02.016
49. Preussler JM, Mau LW, Majhail NS, Bevans M, Clancy E, Messner C, et al. Caregiver availability and patient access to hematopoietic cell transplantation: social worker perspectives inform practice. Support Care Cancer. (2019) 27:4253–64. doi: 10.1007/s00520-019-04696-2
Keywords: frailty syndrome, HCT Frailty Scale, allogeneic-HCT, pre-habilitation, survival
Citation: Salas MQ, Solano MT, Baile González M, Acera Gómez M, Fox L, Pérez Artigas MdM, Santamaría A, Quintela González MdC, Sánchez Salinas A, Salmerón Camacho JM, Illana Álvaro V, Abdallahi-Lefdil Z, Cornago Navascues J, Pardo L, Fernández-Luis S, Vega Suárez LP, Villar S, Beorlegui-Murillo P, Esquirol A, Izquierdo García I, Rodríguez González S, Mussetti A, Lavilla E, Lopez-Marín J, Filaferro S, Cedillo Á, Bento L and Sureda A (2025) Frailty assessment in adults undergoing allogeneic hematopoietic cell transplantation: insights from a multicenter GETH-TC study to optimize outcomes and care. Front. Immunol. 15:1512154. doi: 10.3389/fimmu.2024.1512154
Received: 16 October 2024; Accepted: 12 December 2024;
Published: 07 January 2025.
Edited by:
Sina Naserian, Hôpital Paul Brousse, FranceReviewed by:
Roberto Crocchiolo, Niguarda Ca’ Granda Hospital, ItalyElisa Sala, Ulm University Medical Center, Germany
Copyright © 2025 Salas, Solano, Baile González, Acera Gómez, Fox, Pérez Artigas, Santamaría, Quintela González, Sánchez Salinas, Salmerón Camacho, Illana Álvaro, Abdallahi-Lefdil, Cornago Navascues, Pardo, Fernández-Luis, Vega Suárez, Villar, Beorlegui-Murillo, Esquirol, Izquierdo García, Rodríguez González, Mussetti, Lavilla, Lopez-Marín, Filaferro, Cedillo, Bento and Sureda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Queralt Salas, cXVlcmFsdC5zYWxhczg3QG91dGxvb2suZXM=; bXFzYWxhc0BjbGluaWMuY2F0