 Christoph F. Mahler1
Christoph F. Mahler1 Felix Friedl1
Felix Friedl1 Christian Nusshag1
Christian Nusshag1 Claudius Speer1
Claudius Speer1 Louise Benning1
Louise Benning1 Daniel Göth1
Daniel Göth1 Matthias Schaier1Claudia Sommerer1
Matthias Schaier1Claudia Sommerer1 Markus Mieth2
Markus Mieth2 Arianeb Mehrabi2Christoph Michalski2Lutz Renders3Quirin Bachmann3
Arianeb Mehrabi2Christoph Michalski2Lutz Renders3Quirin Bachmann3 Uwe Heemann3Markus Krautter4
Uwe Heemann3Markus Krautter4 Vedat Schwenger4
Vedat Schwenger4 Fabian Echterdiek3,4
Fabian Echterdiek3,4 Martin Zeier1
Martin Zeier1 Christian Morath1
Christian Morath1 Florian Kälble1*
Florian Kälble1*- 1Department of Nephrology, University Hospital Heidelberg, Heidelberg, Germany
- 2Department of General, Visceral and Transplantation Surgery, University Hospital Heidelberg, Heidelberg, Germany
- 3Department of Nephrology, Klinikum Rechts der Isar, Technische Universität München (TUM), Munich, Germany
- 4Department of Nephrology, Hospital Stuttgart, Stuttgart, Germany
In the face of growing transplant waitlists and aging donors, sound pre-transplant evaluation of organ offers is paramount. However, many transplant centres lack clear criteria on organ acceptance. Often, previous scores for donor characterisation have not been validated for the Eurotransplant population and are not established to support graft acceptance decisions. Here, we investigated 1353 kidney transplantations at three different German centres to develop and validate novel statistical models for the prediction of early adverse graft outcome (EAO), defined as graft loss or CKD ≥4 within three months. The predictive models use generalised estimating equations (GEE) accounting for potential correlations between paired grafts from the same donor. Discriminative accuracy and calibration were determined via internal and external validation in the development (935 recipients, 309 events) and validation cohort (418 recipients, 162 events) respectively. The expert model is based on predictor ratings by senior transplant nephrologists, while for the data-driven model variables were selected via high-dimensional lasso generalised estimating equations (LassoGee). Both models show moderate discrimination for EAO (C-statistic expert model: 0,699, data-driven model 0,698) with good calibration. In summary, we developed novel statistical models that represent current clinical consensus and are tailored to the older deceased donor population. Compared to KDRI, our described models are sparse with only four and three predictors respectively and account for paired grafts from the same donor, while maintaining a discriminative accuracy equal or better than the established KDRI-score.
Introduction
Kidney transplantation is the gold-standard for patients with end-stage renal disease (1, 2). In Germany 1517 cadaveric kidney transplantations were performed in 2021, while 6593 patients remain listed for kidney transplantation (3). In view of this pressing donor shortage optimal organ acceptance strategies are essential (4).
However, despite numerous studies, particularly in western countries, the role of donor characteristics and how to best integrate them into graft acceptance strategies remains largely unknown (5). Yet, donor cues associated with an increased risk of early graft failure have been established including age, comorbidity, immunologic and genetic factors (6–8). Conversely, a registry-based study investigated the role of donor-associated risk in donor-kidney pairs and revealed that once both kidneys are considered eligible for transplantation, donor factors have minimal effect on early transplant outcome (9, 10). This indicates clinical decisions to accept or decline an organ offer are largely efficient.
Hence investigating which donor factors educate the clinical decision process and how they impact early transplant outcome is vital to understanding the role of donor characteristics and the development of standardised acceptance criteria.
Here we conducted an in-depth analysis of the deceased-donor characteristics of 1353 kidney transplantations at three German Eurotransplant centres concerning their impact on early adverse outcome (EAO) which we defined as early graft loss or impaired kidney function (CKD ≥ 4; eGFR < 30 ml/min) three months after transplantation. This approach thus eliminated the majority of bias attributed to variable and long-term environmental influences like post-transplant care and recipient behaviour (9, 11). The rationale for EOA as primarily donor- and procedure driven is echoed by transplant policies allowing recipients immediate reinstatement of accrued waiting time after graft failure within 90 days after transplantation (12).
For a baseline and comparison, we first calculated KDRI scores and performed model calibration for prediction EOA. Subsequently, we developed different new models based on previously suggested variables, data-driven variable selection and expert input from senior nephrologists. These new models were internally and externally validated for prediction of EOA within three months from transplantation.
Materials and methods
Study cohort
In this study we retrospectively included 1353 deceased kidney donor transplantations between 2006 and 2021 at our centre (605 grafts), Stuttgart transplant centre (418 grafts) as well as the transplant centre of the Technical University in Munich (330 grafts). Partner grafts were defined as transplantations where both kidneys from a single donor were transplanted in different individuals, this paired nature of the data was accounted for in the statistical models (10). We collected donor and recipient characteristics with their respective clinical outcome after transplantation. The local Ethics Committees authorised the study without a requirement for individual consent. The following inclusion criteria were applied: Recipients aged 18 years or older, offer of a kidney-organ from a deceased donor via Eurotransplant, transplantation of both kidneys from a single donor at the same centre. Exclusion criteria were combined organ offers (heart-kidney, pancreas-kidney).
Outcome
We defined early adverse outcome (EAO) as a composite of graft loss or CKD ≥4 within three months after transplantation. We reasoned that donor related graft function might be most prominent during the early phase post transplantation, whereas recipient and environmental factors mainly bias late graft failure. The CKD-EPI formula without race (13) was used for calculation of donor eGFR and recipient eGFR after transplantation.
Statistical analysis
The data collection in the context of the presented project was performed with the help of an electronic database system (Microsoft Excel 2018, Microsoft Germany GmbH, Unterschleißheim). A statistical evaluation was then carried out using RStudio (R team 2021).
There was no missing data for three month graft function, graft survival or three month recipient survival. There was less than 1,5% of overall data missing. Merged multiple imputation was used to compute the mean of all imputed values of each missing value.
Variable selection and clustered analysis
Univariate Generalised Estimating Equation (GEE) (14, 15) models were employed to calculate odds ratios (OR) and confidence intervals (CI) for individual variables (16). For variable selection we applied high-dimensional lasso generalised estimating equations (LassoGee), to identify significant predictors (17). 1000-fold bootstrapping was used to ensure the stability and reliability of the selected variables. A multivariate GEE model was then fitted based on the previously selected variables. The Kidney Donor Risk Index (KDRI) was calculated using standard clinical parameters (18–20) and a cox model was re-calibrated. For internal validation we used 250-fold bootstrapping analysis, as recommended by the transparent reporting of a multivariable prediction model for individual prognosis or diagnosis guidelines.
Results
Baseline characteristics and study cohort
1353 kidney transplantations at three different Eurotransplant centres from 1184 donors were included for analysis, 605 at centre 1 (Heidelberg), 330 in centre 2 (Munich) and 418 at centre 3 (Stuttgart) between the years 2006-2021. Donor and recipient characteristics are summarised in Table 1. More recipients were male with a median of age of 62 and a median of BMI of 25. Few of them were sensitised (median/IQR of vPRA > 5% 0/5). Most patients received tacrolimus (70%) as initial immunosuppression. Patients on cyclosporine A are patients at the beginning of the study period, where cyclosporine A was more commonly used, especially within the ESP program. Within the donors, male and female was equally distributed, median age was 60 with a median BMI of 27.
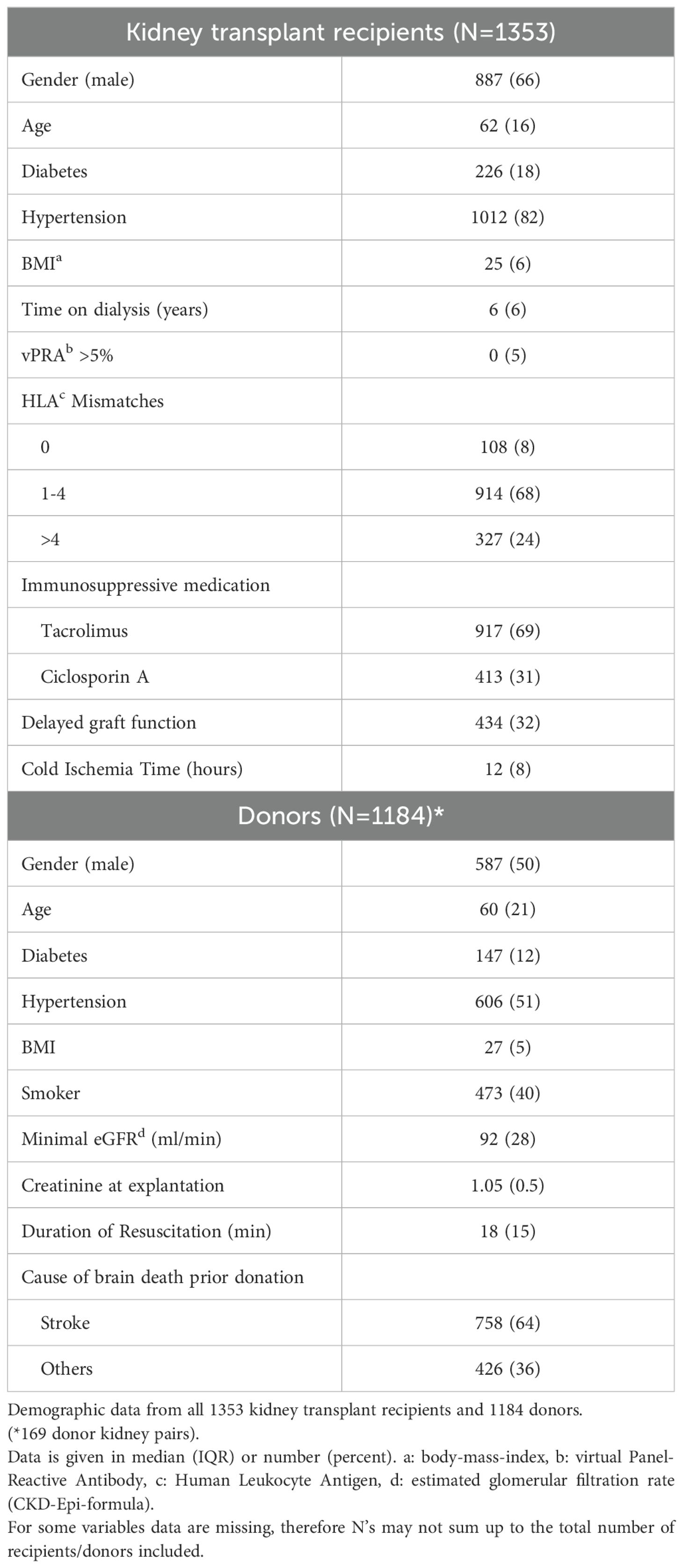
Table 1. Donor and recipient characteristics.
The data was split into separate cohorts, where 935 performed transplantations from centre 1 and 2 were used for model development and internal validation. The transplant outcomes at centre 3 were used for external validation, see Figure 1. In both cohorts, 9% (n= 83 and n=36 respectively) of the recipients experienced death censored graft failure, while impaired graft function (eGFR <30) was more common in the validation cohort (30%, n= 126) than in the development cohort (24%, n=226) at three months.

Figure 1. Flow chart. Flow diagram of the statistical evaluation. Deceased donor kidney transplantations at three centres between 2006 and 2021 were collected (grey boxes). Two centres were combined for model development and internal validation, the third centre was used as an external validation dataset.
Model development
To assess whether we can identify donor factors with a substantial impact on early transplant function we used EAO as a composite outcome of graft failure and CKD ≥4. Potential donor associated predictors were selected by the authors based on the existing literature, data availability and suggestions by senior nephrologists. All donor variables were included in a full statistical model (see Supplementary Table 1) for the prediction of EAO (apart from height and weight as these correlate directly with the BMI). Through Lasso GEE the coefficients for donor age, donor eGFR and cause of brain death were estimated as non-zero and therefore included in the data-driven model (see Supplementary Table 2).
An expert model (see Supplementary Table 3) was developed based on a survey among seven senior transplant nephrologists from all participating centres. They were asked to select the most valuable donor factors in predicting 90-days kidney function. Four potential donor factors (age, minimal eGFR before donation, urine output and cold ischemic time (CIT) were preselected based on clinical expert majority opinion (>50%) Figure 2. All models are summarised in Table 2.
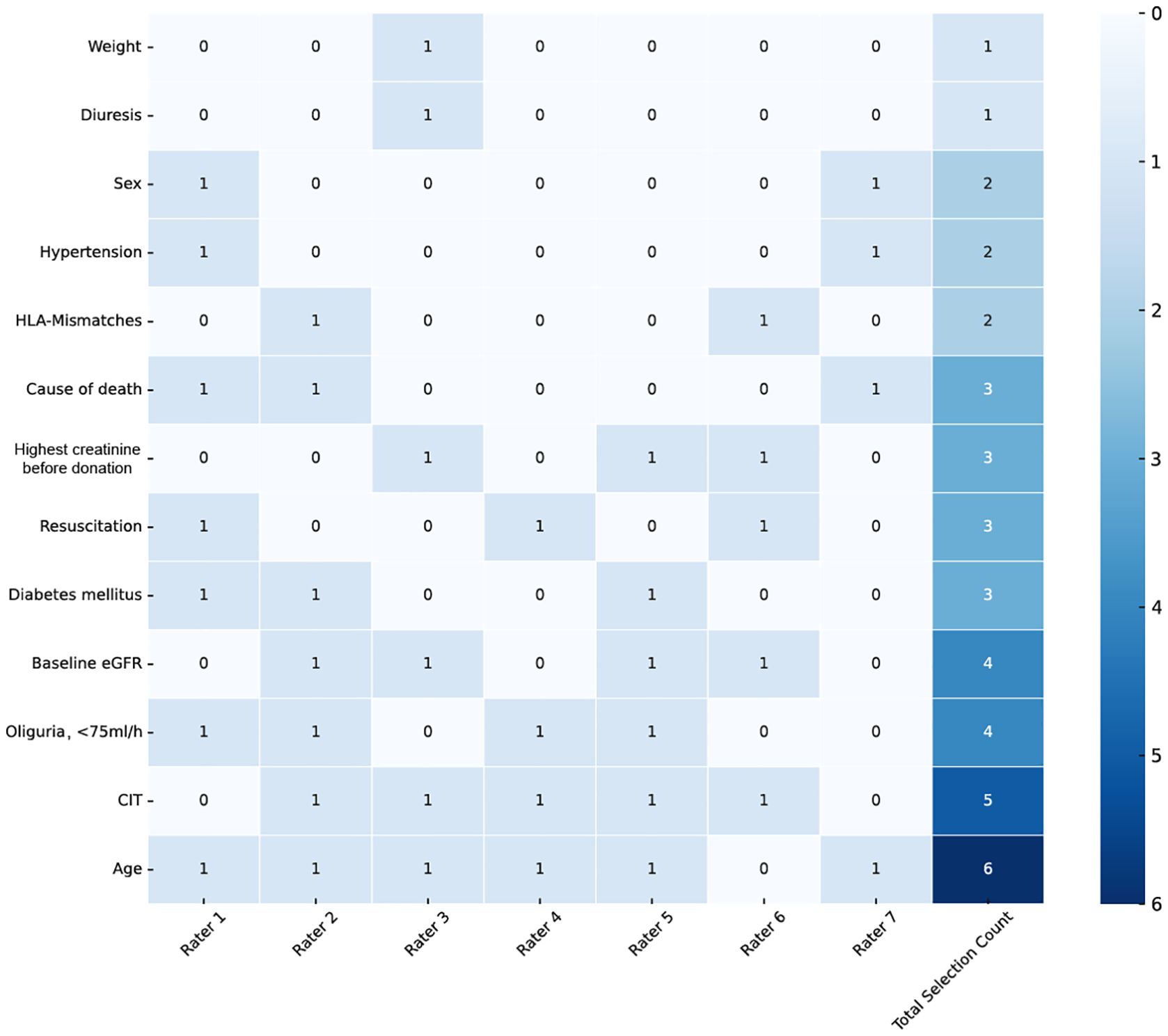
Figure 2. Expert selection. Clinical expert based variable nomination. Nominations of donor characteristics with clinical relevance for graft acceptance and presumed impact on early transplant function. Raters one to seven represent individual senior transplant nephrologists from all three centres. Variables with at four nominations were selected for further analysis. HLA, human leucocyte antigen; eGFR, estimated glomerular filtration rate; CIT, cold ischemic time.
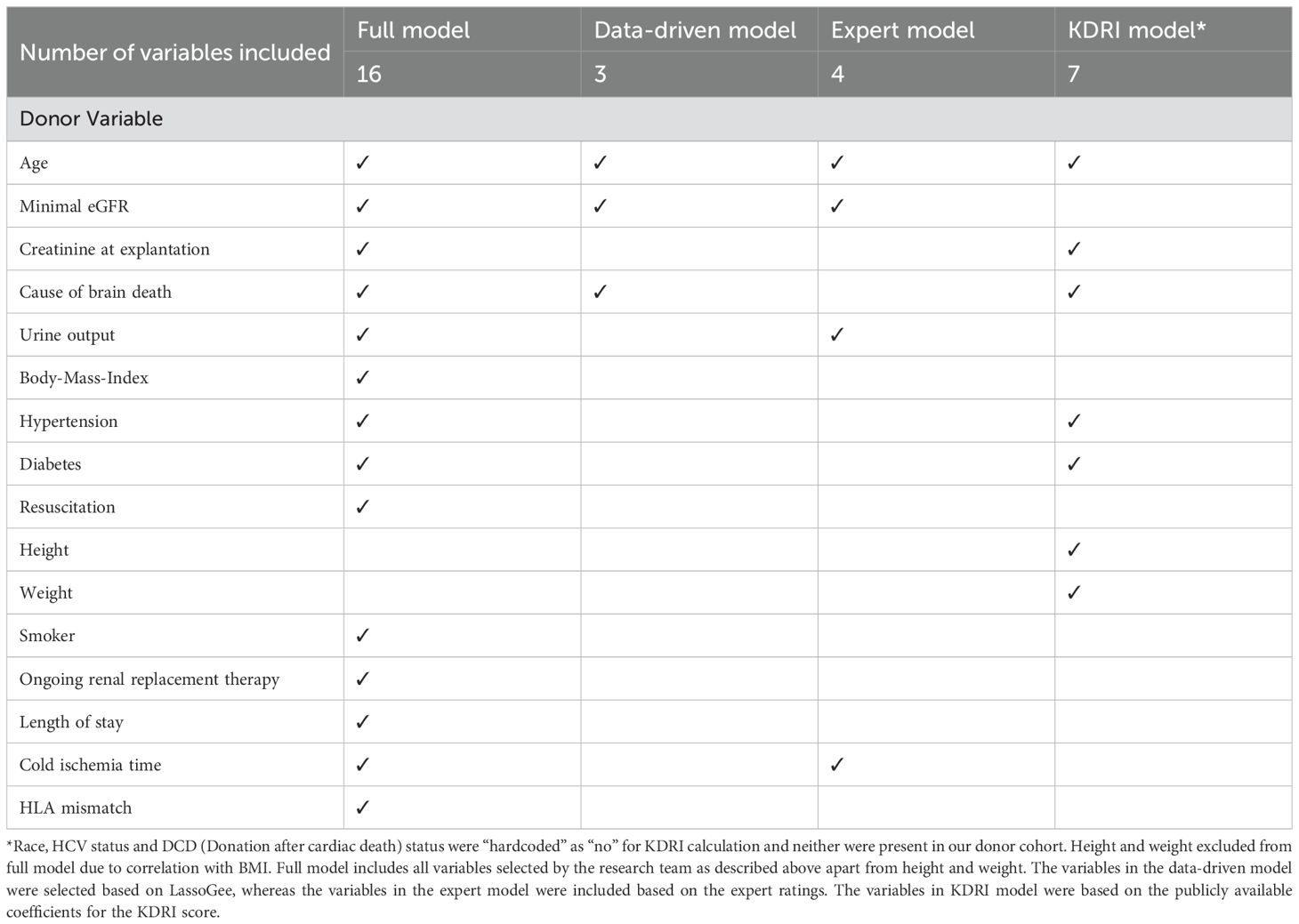
Table 2. Comparison of models and variables used.
Discriminative ability of different statistical models
All assessed models showed moderate predictive accuracy. The C-statistic of the full-model was 0.727 and 0.689 for the internal and external validation respectively, which is similar to the cox model based on KDRI scores (0.713 and 0.687). The data-driven model showed improved C-statistics of 0.728 and 0.698 respectively and had almost identical C-statistics as the expert model of 0.718 and 0.699, respectively. In both, the data-driven and the expert model calibration was generally good and improved compared to the full model, although the models showed a tendency to underpredict risk, particularly for high-risk patients (Table 3; Figure 3).
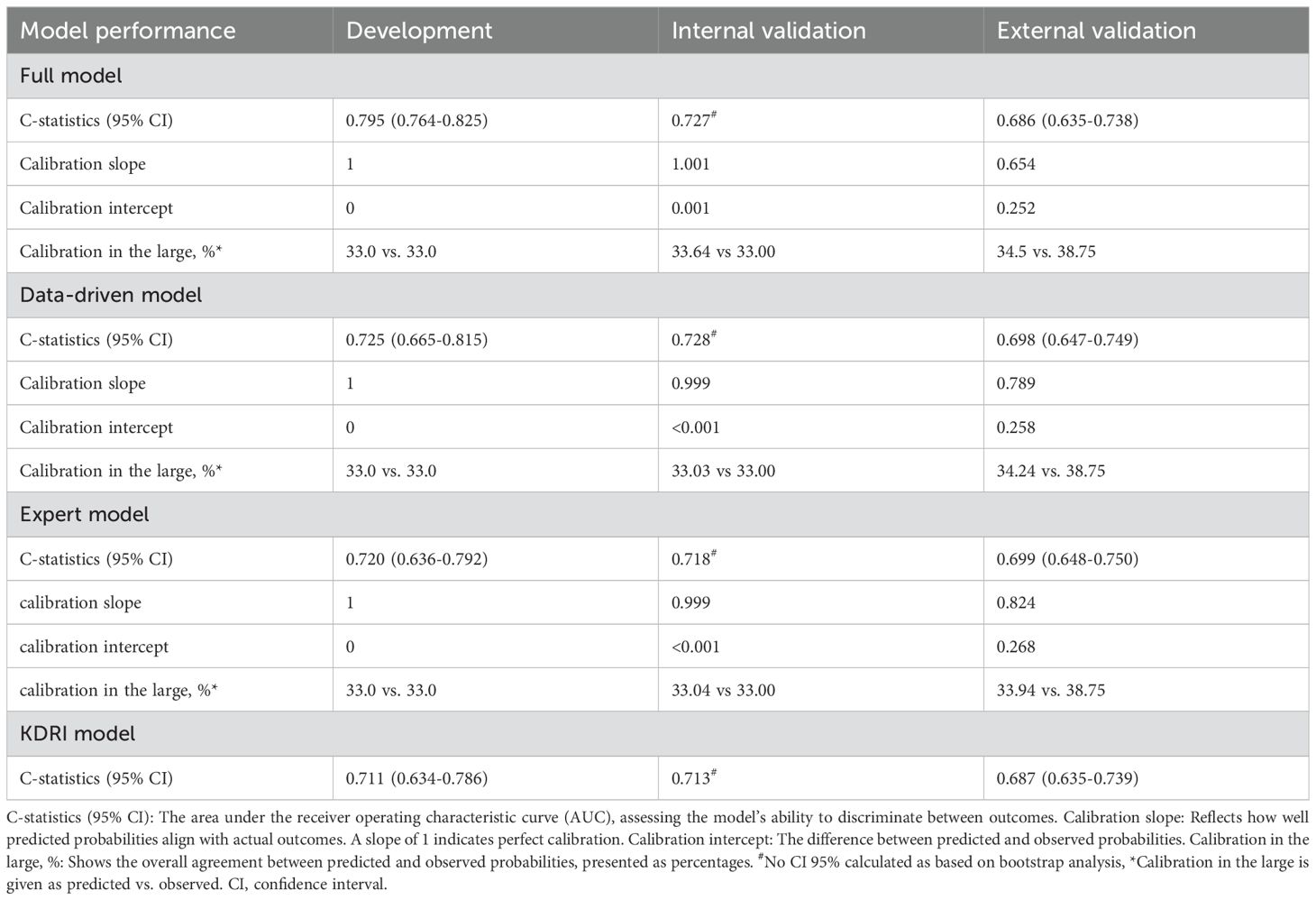
Table 3. Comparison of models in external and internal validation.
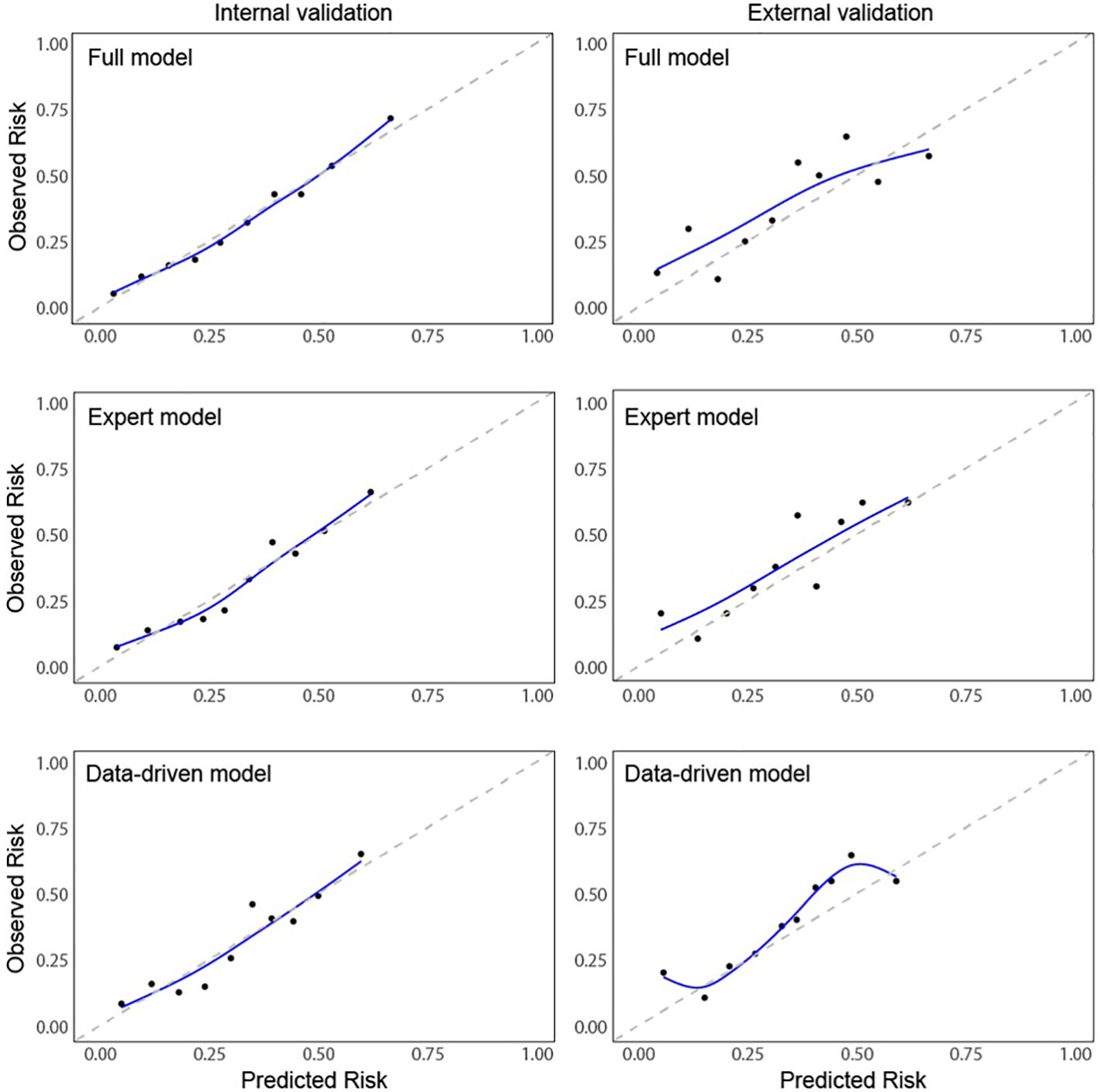
Figure 3. Calibration plots of early adverse outcome (EAO). Calibration Curves of Early Adverse Outcomes (EAO) for Internal and External Validation. This figure displays calibration plots comparing predicted versus observed risks for kidney transplant failure across three different models (Full, Expert and Data-driven) using both internal and external validation data. The left column shows calibration curves for internal validation, while the right column shows calibration curves for external validation. Each plot presents decile-based calibration points: Mean predicted risk (x-axis) and mean observed risk (y-axis) within each decile. Smoothed line (blue): A Generalized Additive Model (GAM) fit, providing a smooth approximation of the calibration relationship. Dashed diagonal line (gray): Represents perfect calibration, where predicted and observed risks are equal. Each curve illustrates the agreement between predicted and observed outcomes, with better calibration reflected by points and the blue line aligning closely with the diagonal reference line.
Analysis of Variance (ANOVA) statistics for model comparison revealed that the data-driven model provides the best balance between prediction capability and complexity with significant improvements over the KDRI model which performed worst in our cohort. Correspondingly the Bayesian Information Criteria (BIC) for KDRI was significantly increased compared to the data-driven model (1146.8, 1072.8 respectively). The statistical model with all parameters had good discriminative accuracy, however being the most complex model, it may overfit the data as indicated by the lower calibration slope of 0.654 versus 0.824 for the expert model and 0.789 for the data driven model.
For sensitivity analysis we leveraged a separate validation cohort with an equal number of patients from each centre to exclude centre specific factors that contribute to EAO. The performance of the tested models remained comparable, with C-statistics of 0.753 and 0.722 in the data-driven and expert model respectively and 0.732 for KDRI.
Taken together, concerning the prediction of EAO, our study thus indicates that the new sparse data-driven and expert-based models tend to perform better in our cohort compared to a KDRI based model. Both the data-driven model with only three donor factors (age, eGFR and cause of brain death) and an expert model with four donor characteristics (age, eGFR, urine output and CIT) reveal moderate prediction accuracy and robust calibration that supports differentiation of favourable from unfavourable donor profiles.
Discussion
In view of an increasing donor shortage optimal organ acceptance strategies are essential. Efforts to enhance organ utilization are currently made through multiple approaches and at a large scale. Especially in the US, the Organ Procurement Transplantation Network and the United Network for Organ Sharing have introduced several strategies. One was the implementation of the KDPI which is derived from the KDRI.
Despite its widespread use in the United States, its application is debated within the Eurotransplant region. The score may fail to capture the full complexity of the organ allocation process, leaving out important factors such as procedural details, immunological profiles, or recipient-specific characteristics. Furthermore, it has been suggested that the KDRI contributes to higher organ discard rates in the U.S., raising concerns about the effectiveness of this donor-based index (21, 22). A Canadian study by Rose et al. found that donor age alone offers predictive performance similar to the full KDRI (23).
This is in line with the present results. In this multicentric study with a cohort of 1353 transplant recipients of three different transplant centres in Germany, we investigated which donor factors can be used to predict or model the early outcome after transplantation, i.e. EAO. To this end, various models were developed and validated regarding performance and tested against each other. We performed a survey among seven senior nephrologists with years of experience within transplantation and organ allocation. Here, we found that for donor age, donor kidney function (minimal eGFR prior to donation and urine output) and for CIT there is good consensus among senior transplant nephrologists at the different centres concerning their impact on graft acceptance and early transplant outcome. Subsequent data-driven analysis with Lasso revealed that mainly donor age, minimal eGFR prior donation and the cause of brain death were the most relevant in predicting EAO. The data-driven and the expert model performed equally well. A third model used was integrating a variety of more donor factors (14 factors) with similar performance compared to the expert model but the most complexity (16 factors versus 4 (expert) and 3 (data-driven) factors. As a fourth model, the KDRI was calculated for comparison and showed a tendency for worse outcome differentiation. Likewise, European studies have highlighted the limitations of using the KDRI (24–27).
This study confirmed and refined the findings of previous studies assessing donor associated risk factors (28). The observation, that some of the findings revealed in this study have previously been reported in retrospective analysis of graft failure (for example the strong effect of donor age on early graft loss) (21), highlights the importance of a clinically guided characterisation of the graft over purely statics driven algorithms (9, 29).
This study has important limitations as this is a retrospective analysis of outcome after transplantation of donated and transplanted kidney grafts. This necessarily results in some degree of bias, as the study is restricted to the variables collected during the organ allocation process and declined or discarded grafts could not be analysed. A second limitation is the comparably high percentage of kidneys with EAO, which echoes the proportion of old donors and recipients in the German Eurotransplant population, specifically the Eurotransplant senior program (ESP). This underlines the importance of further study in a larger, but equally well characterised transplantation cohort. Also, as this is a study at German Eurotransplant centres with a mostly Caucasian and aging patient population our conclusions may not apply to patient cohorts with a different distribution of these factors. Finally, this study is potentially biased by confounders of clinical decisions at the centres and allocation criteria specific to the Eurotransplant system, such as the ESP.
One of the strengths of this study is the use of a well-curated dataset with minimal missing entries, enhancing the reliability of the analysis. This cohort closely represents the current Eurotransplant donor population, as reflected by a median donor age of 60. Additionally, the models were developed using generalised estimating equations (GEE) to account for paired data, addressing the potential correlation between grafts from the same donor transplanted into different recipients, further strengthening the robustness of the findings.
Summarising, our study demonstrates the limited benefit of the KDRI within the Eurotransplant region, where most donors fall into the highest quartile (30) and KDRI usage could lead to an unnecessarily high decline rate. Correspondingly, similar statistical models derived from multiple donor factors for prediction of early graft function are often complex. Here, we show the relevant donor factors can be reduced to a few, while maintaining similar or better accuracy in outcome prediction. Together, the clinically driven nomination of donor characteristics and the penalised regression analysis estimated donor age and the baseline donor kidney function as variables that may well be part of the donor associated substrate for EAO and could be leveraged for the development of clinical criteria for the acceptance of deceased-donor kidney grafts.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethikkommision d. med. Fakultät d. Uni Heidelberg, Alte Glockengießerei 11/1, 69115 Heidelberg. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
CFM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. FF: Data curation, Formal analysis, Methodology, Supervision, Writing – review & editing. CN: Data curation, Methodology, Supervision, Writing – review & editing. CSp: Data curation, Methodology, Supervision, Writing – review & editing. LB: Data curation, Methodology, Supervision, Writing – review & editing. DG: Writing – review & editing, Data curation. MS: Supervision, Writing – review & editing. CSo: Resources, Supervision, Writing – review & editing. MM: Supervision, Writing – review & editing, Resources. AM: Supervision, Writing – review & editing. CMi: Supervision, Writing – review & editing. LR: Supervision, Writing – review & editing. QB: Writing – review & editing, Data curation. UH: Supervision, Writing – review & editing. MK: Supervision, Writing – review & editing. VS: Supervision, Writing – review & editing. FE: Supervision, Writing – review & editing, Data curation, Project administration, Validation. MZ: Conceptualization, Supervision, Writing – review & editing. CMo: Conceptualization, Methodology, Supervision, Writing – review & editing. FK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. CFM is funded by the Clinician Scientist Program of the Heidelberg Faculty of Medicine.
Acknowledgments
We thank Lukas Baumann and Johannes Vey from the Institute for Medical Biometry, Heidelberg, Germany for statistical consulting and review of the statistical methods.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. We acknowledge the use of ChatGPT 4.0 for code generation in Python and R.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1511368/full#supplementary-material
References
1. Tonelli M, Wiebe N, Knoll G, Bello A, Browne S, Jadhav D. Systematic review: kidney transplantation compared with dialysis in clinically relevant outcomes. Am J Transplant. (2011) 11:2093–109. doi: 10.1111/j.1600-6143.2011.03686.x
2. Hariharan S, Israni AK, Danovitch G. Long-term survival after kidney transplantation. New Engl J Med. (2021) 385:729–43. doi: 10.1056/NEJMra2014530
3. Organtransplantation, D. S. Jahresbericht. Frankfurt/Main: Deutsche Stiftung Organtransplantation (2021).
4. Childress JF. Organ donor research: overcoming challenges, increasing opportunities. JAMA. (2017) 318:2177–8. doi: 10.1001/jama.2017.16442
5. Wu DA, Watson CJ, Bradley JA, Johnson RJ, Forsythe JL, Oniscu GC, et al. Global trends and challenges in deceased donor kidney allocation. Kidney Int. (2017) 91:1287–99. doi: 10.1016/j.kint.2016.09.054
6. von Moos S, Akalin E, Mas V, Mueller TF. Assessment of organ quality in kidney transplantation by molecular analysis and why it may not have been achieved, yet. Front Immunol. (2020) 11:833. doi: 10.3389/fimmu.2020.00833
7. Morath C, Döhler B, Kälble F, da Silva LP, Echterdiek F, Schwenger V, et al. Pre-transplant HLA antibodies and delayed graft function in the current era of kidney transplantation. Freiburg: Universität (2020).
8. Steers NJ, Li Y, Drace Z, D'Addario JA, Fischman C, Liu L. Genomic mismatch at LIMS1 locus and kidney allograft rejection. New Engl J Med. (2019) 380:1918–28. doi: 10.1056/NEJMoa1803731
9. Schaapherder AF, Kaisar M, Mumford L, Robb M, Johnson R, de Kok MJC. Donor characteristics and their impact on kidney transplantation outcomes: Results from two nationwide instrumental variable analyses based on outcomes of donor kidney pairs accepted for transplantation. EClinicalMedicine. (2022) 50:101516. doi: 10.1016/j.eclinm.2022.101516
10. Mahler CF, Friedl F, Nusshag C, Speer C, Benning L, Göth D, et al. Impact of deceased-donor characteristics on early graft function: outcome of kidney donor pairs accepted for transplantation. Front Immunol. (2024) 15:1303746. doi: 10.1016/j.kint.2020.11.016
11. de Kok MJ, Schaapherder AF, Mensink JW, de Vries AP, Reinders ME, Konijn C, et al. A nationwide evaluation of deceased donor kidney transplantation indicates detrimental consequences of early graft loss. Kidney Int. (2020) 97:1243–52. doi: 10.1016/j.kint.2020.01.043
12. Swinarska JT, Stratta RJ, Rogers J, Chang A, Farney AC, Orlando G, et al. Early graft loss after deceased-donor kidney transplantation: what are the consequences? J Am Coll Surgeons. (2021) 232:493–502. doi: 10.1016/j.jamcollsurg.2020.12.005
13. Inker LA, Eneanya ND, Coresh J, Tighiouart H, Wang D, Sang Y, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. New Engl J Med. (2021) 385:1737–49. doi: 10.1056/NEJMoa2102953
14. Buch G, Schulz A, Schmidtmann I, Strauch K, Wild PS. A systematic review and evaluation of statistical methods for group variable selection. Stat Med. (2023) 42:331–52. doi: 10.1002/sim.9620
15. Hui FKC, Maestrini L, Welsh AH. Homogeneity pursuit and variable selection in regression models for multivariate abundance data. Biometrics. (2024) 80. doi: 10.1093/biomtc/ujad001
16. Pavlou M, Ambler G, Seaman SR, Guttmann O, Elliott P, King M, et al. How to develop a more accurate risk prediction model when there are few events. BMJ (Clinical Res ed.). (2015) 351:h3868. doi: 10.1136/bmj.h3868
17. Huang T, He W, Xie Y, Lv W, Li Y, Li H, et al. A LASSO-derived clinical score to predict severe acute kidney injury in the cardiac surgery recovery unit: a large retrospective cohort study using the MIMIC database. BMJ Open. (2022) 12:e060258. doi: 10.1136/bmjopen-2021-060258
18. Bikbov BR. Open source programming code for calculation of the kidney donor profile index and kidney donor risk index. Kidney Dis (Basel Switzerland). (2018) 4:269–72. doi: 10.1159/000492427
19. Rao PS, Schaubel DE, Guidinger MK, Andreoni KA, Wolfe RA, Merion RM, et al. A comprehensive risk quantification score for deceased donor kidneys: the kidney donor risk index. Transplantation. (2009) 88:231–6. doi: 10.1097/TP.0b013e3181ac620b
20. Lehner LJ, Kleinsteuber A, Halleck F, Khadzhynov D, Schrezenmeier E, Duerr M, et al. Assessment of the kidney donor profile index in a European cohort. Nephrology dialysis Transplant. (2018) 33:1465–72. doi: 10.1093/ndt/gfy030
21. Hamed MO, Chen Y, Pasea L, Watson CJ, Torpey N, Bradley JA, et al. Early graft loss after kidney transplantation: risk factors and consequences. Am J Transplant. (2015) 15:1632–43. doi: 10.1111/ajt.13162
22. Stewart DE, Garcia VC, Rosendale JD, Klassen DK, Carrico BJ. Diagnosing the decades-long rise in the deceased donor kidney discard rate in the United States. Transplantation. (2017) 101:575–87. doi: 10.1097/TP.0000000000001539
23. Rose C, Sun Y, Ferre E, Gill J, Landsberg D, Gill J, et al. An examination of the application of the kidney donor risk index in British Columbia. Can J Kidney Health Dis. (2018) 5:2054358118761052. doi: 10.1177/2054358118761052
24. Dahmen M, Becker F, Pavenstädt H, Suwelack B, Schütte-Nütgen K, Reuter S, et al. Validation of the Kidney Donor Profile Index (KDPI) to assess a deceased donor's kidneys' outcome in a European cohort. Sci Rep. (2019) 9:11234. doi: 10.1038/s41598-019-47772-7
25. Ramspek CL, El Moumni M, Wali E, Heemskerk MBA, Pol RA, Crop MJ, et al. Development and external validation study combining existing models and recent data into an up-to-date prediction model for evaluating kidneys from older deceased donors for transplantation. Kidney Int. (2021) 99:1459–69. doi: 10.1016/j.kint.2020.11.016
26. Arias-Cabrales C, Pérez-Sáez MJ, Redondo-Pachón D, Buxeda A, Burballa C, Bermejo S, et al. Usefulness of the KDPI in Spain: A comparison with donor age and definition of standard/expanded criteria donor. Nefrologia. (2018) 38:503–13. doi: 10.1016/j.nefro.2018.03.003
27. Peters-Sengers H, Heemskerk MBA, Geskus RB, Kers J, van der Heide JJH, Berger SP, et al. Validation of the prognostic kidney donor risk index scoring system of deceased donors for renal transplantation in the Netherlands. Transplantation. (2018) 102:162–70. doi: 10.1097/TP.0000000000001889
28. Querard A-H, Foucher Y, Combescure C, Dantan E, Larmet D, Lorent M, et al. Comparison of survival outcomes between Expanded Criteria Donor and Standard Criteria Donor kidney transplant recipients: a systematic review and meta-analysis. Transplant Int. (2016) 29:403–15. doi: 10.1111/tri.12736
29. Stallone G, Grandaliano G. To discard or not to discard: transplantation and the art of scoring. Clin Kidney J. (2019) 12:564–8. doi: 10.1093/ckj/sfz032
Keywords: kidney transplantation, donor selection criteria, graft loss, donor score, kidney donor risk index (KDRI)
Citation: Mahler CF, Friedl F, Nusshag C, Speer C, Benning L, Göth D, Schaier M, Sommerer C, Mieth M, Mehrabi A, Michalski C, Renders L, Bachmann Q, Heemann U, Krautter M, Schwenger V, Echterdiek F, Zeier M, Morath C and Kälble F (2025) Evaluation of deceased-donor kidney offers: development and validation of novel data driven and expert based prediction models for early transplant outcomes. Front. Immunol. 15:1511368. doi: 10.3389/fimmu.2024.1511368
Received: 14 October 2024; Accepted: 06 December 2024;
Published: 07 January 2025.
Edited by:
Guido Moll, Charité University Medicine Berlin, GermanyReviewed by:
Yoshiko Matsuda, National Center for Child Health and Development (NCCHD), JapanBrian Shaw, Duke University, United States
Copyright © 2025 Mahler, Friedl, Nusshag, Speer, Benning, Göth, Schaier, Sommerer, Mieth, Mehrabi, Michalski, Renders, Bachmann, Heemann, Krautter, Schwenger, Echterdiek, Zeier, Morath and Kälble. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Florian Kälble, Zmxvcmlhbi5rYWVsYmxlQG1lZC51bmktaGVpZGVsYmVyZy5kZQ==